Embed Size (px)
Citation preview

29D.C. Madoff et al. (eds.), Venous Embolization of the Liver,DOI 10.1007/978-1-84882-122-4_5, © Springer-Verlag London Limited 2011
Liver Anatomy: Variant Venous Anatomy and Implications for Resection
Ajay V. Maker, William R. Jarnagin, and Anne M. Covey
5
Surgical resection remains the most effective therapy for patients with primary and metastatic liver tumors. All techniques for partial hepatectomy ultimately rely on control and transection of the vascular inflow and the biliary and venous outflow of the segments to be resected. Variations in portal venous anatomy are not uncommon and have important implications for both hepatic resection and for interventional procedures including preoperative portal vein embolization and TIPS. With an increase in complex surgical resections and percutaneous hepatobiliary interventions, a thor-ough understanding of variant hepatic venous anatomy is critical. This chapter addresses the congenital and acquired anomalies of the portal vein, the implications
these have on biliary ductal anatomy and portal vein embolization, and the variations of the hepatic veins.
5.1 Congenital Anomalies of the Portal Vein
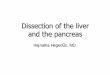
The splenic and superior mesenteric veins join to form the main portal vein posterior to the head of the pan-creas. The main portal vein typically divides at the hilum into the left and right portal branches. The right portal vein typically has a short extrahepatic course and then divides into the right anterior sectoral trunk, which feeds segments V and VIII, and the right posterior sec-toral trunk, which supplies segments VI and VII. The left portal vein has a longer extrahepatic course along the dorsocaudal aspect of segment IV before it curves ventrally into the umbilical fissure to supply the cau-date and segments II, III, and IV (Fig. 5.1).
Embryologically, the portal vein is formed between the 4th and 10th weeks of gestation.1-3 By the fourth
A.M. Covey (*)Department of Diagnostic Radiology, Memorial Sloan-Kettering Cancer Center,1275 York Avenue, New York, NY 10021, USAe-mail: [email protected]
Abstract
The complexity of radiologic and surgical interventions on the liver has increased in the last decade. Knowledge of anatomical variants is crucial for safe hepatic resection and for preservation of adequate inflow and outflow to the functional remnant liver tissue. There are many congenital and acquired anomalies of the portal vein that need to be identified preoperatively, and their presence may indicate concomitant variations in biliary ductal anatomy.
Keywords
Congenital anomalies of the liver • Hepatic anatomy variants • Hepatic vein variations • Liver anatomy • Venous anatomy variants

30 A.V. Maker et al.
week, there are three paired venous systems: the cardinal veins, the vitelline veins from the yolk sac, and the umbilical veins from the chorion. By the end of the fourth week, the right and left vitelline veins are
cross-linked, with the superior anastomoses forming the intrahepatic portal veins. The extrahepatic portal veins are formed by selective involution of the right and left vitelline veins.3 Alterations in the pattern of obliteration of these anastomoses can result in several variants, and failure to form these anastomoses results in complete or partial absence of the portal system.4
Major congenital portal vein variants include total or partial agenesis, duplication, a single main portal vein, and venous malposition, including a prepancre-atic portal vein.5-8 These variants are often accompa-nied by cardiac and other congenital malformations.9 With modern preoperative cross-sectional imaging, these anomalies are often obvious, and surgical and interventional planning can be tailored based on the specific anatomy. For patients with congenital absence of the portal vein, the treatment of liver tumors, such as in hepatocellular carcinoma, remains radical resec-tion,10 and patients who have undergone resection have had uncomplicated postoperative courses despite a lack of portal blood and the associated hepatotropic factors.1,11-14
Far more common variations, however, involve the branching pattern of the portal vein. These can range from anomalies at the main portal vein bifurcation, to far more subtle intrahepatic variations, all of which can have significant clinical consequences during hepatic resection. Failure to properly identify the origin of the portal inflow to the remaining functional liver remnant and inadvertent ligation can result in a necrotic liver segment, or even hepatic failure and death.
5.1.1 Branching Patterns of the Portal Vein
In our experience, there are five major branching pat-terns of the portal vein. The most common, type 1, is the standard portal venous anatomy in which the main portal vein divides into the right and left por-tal branches. The right portal vein then gives rise to anterior and posterior sectoral branches that supply Couinaud segments V/VIII and segments VI/VII, respectively (Fig. 5.1). We found this pattern present in 65% of 200 patients studied with CT portography.15
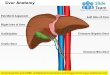
Trifurcation of the main portal vein into the right anterior, right posterior, and left portal vein branches, or type 2 anatomy, occurred in 9% of our patients (Fig. 5.2). This is important to recognize in right-sided resections where instead of controlling inflow via the main right portal vein, both the anterior and posterior sectoral branches would need to be separately controlled.
RASa
IVB
IVAIII
II
Ligamentum teres
LPV
SV
IMV
RPS
RPV
CV
SMV
b
Fig. 5.1 (a, b) In standard anatomy, the portal vein is formed by the confluence of the splenic vein (SV) and the superior mesen-teric vein (SMV). The inferior mesenteric vein (IMV) ends in the splenic vein. The main portal vein typically divides at the hilum into the left and right portal branches. The right portal vein (RPV) typically has a short extrahepatic course and then divides into the right anterior sectoral trunk (RAS), which feeds segments V and VIII, and the right posterior sectoral trunk (RPS), which supplies segments VI and VII. The left portal vein (LPV) has a longer extrahepatic course along the inferior aspect of segment IV before it curves cranially into the umbilical fissure to supply the caudate and segments II, III, and IV

315 Liver Anatomy: Variant Venous Anatomy and Implications for Resection
Likewise, preoperative portal vein embolization, which is performed most commonly on the right side, would require separate embolization of both branches.
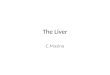
The most common variation on the standard anat-omy is the “Z-type” anatomy, type 3, seen in 13% of patients in our study and in 6–11.4% by others.16-18 It is referred to as “the portal vein variation” by Kitani and colleagues, who encountered it almost 10% of the time in 478 consecutive patients.19 In this variation, the first branch of the main portal vein is the right posterior portal vein, and the right anterior portal vein and the left portal vein bifurcate (Fig. 5.3). In right hepatec-tomy, the right portal vein is often controlled extrahe-patically. However, in this anatomic configuration, ligation of what may appear to be the right branch of the main portal vein for the right-sided resections may actually be the right posterior portal vein or the trunk to the right anterior sector and the left lobe. Similarly, for left-sided resections, the approach to the left portal vein will not be in its standard position. Thus, ligation of this venous trunk of the right anterior and the left portal veins would leave a wide nonperfused liver rem-nant, and risk of hepatic failure and death.
In less than 10% of patients, we found that the seg-ment VII or VI branch was the first branch of the right portal vein (types 4 and 5, respectively) and that the right anterior portal vein trifurcated to supply the anterior sec-tor and one segment of the posterior sector (Fig. 5.4). This is important to note in extended left hepatic resec-tion, where if the right anterior sectorial branch with one segmental branch of the posterior sector is ligated, a large portion of the remnant liver would be without portal flow, possibly resulting in hepatic failure. Similarly, for any resection of the posterior sector, each individual pedicle would need to be identified and ligated since there is no common posterior sectorial pedicle. It is well known that intrahepatic vessel ramification of the right posterior sector is extremely variable, and careful plan-ning with preoperative imaging and intraoperative ultra-sound is critical in these patients.20,21
In addition to the five main types of portal vein branching patterns described, “other” portal vein vari-ants were identified in 6% of patients. Half of these had trifurcation of the right portal vein into the right anterior sectorial portal trunk, segment VI, and seg-ment VII branches. One patient each had the following anomalies: quadrification of the main portal vein into segment VI, segment VII, the right anterior portal vein, and the left portal vein; trifurcation of the right portal vein into branches supplying segment V, segment VIII, and the right posterior sectoral trunk; trifurcation of
RAS
LPV
RPS
PV
a
b
c
Fig. 5.2 (a–c) Type 2 portal vein anatomy: trifurcation of the main portal vein (MPV) into the right anterior sector (RAS), right posterior sector (RPS), and left portal vein (LPV) branches

32 A.V. Maker et al.
the main portal vein into segment VI, segment VII, and the left main and right anterior sectoral branch; the segment IV and VII branches originating from the right anterior portal vein; and an accessory segment VI branch from the right portal vein in a patient with type 5 portal vein branching.
Older sonographic literature identifies variant por-tal vein anatomy in 10–15% of patients; however, in recent studies utilizing portography, the incidence is closer to one-third of the patients studied.15,22-24 Variants of the left portal vein are rare, but, when variations of the right portal vein exist and the main portal branch-ing pattern is anomalous, the left vein may not be found in its standard position, and it must be clearly identified and controlled prior to left-sided resections.
5.2 Acquired Anomalies
Acquired portal vein anomalies of clinical significance to the interventionalist arise from venous collaterals. These collaterals can be secondary to portal hyperten-sion, splenic or splenomesenteric venous stenosis, or portal vein obstruction due to pancreatitis, tumor, or surgery. Multiple patterns of venous collaterals are described, the most common being gastroesophageal, paraumbilical, splenorenal, and inferior mesenteric. Gastric collateral veins most often present on imaging in patients with portal hypertension, and associated esophageal varices are a clinically important source of upper gastrointestinal hemorrhage. Obliteration of the splenic vein is also the source of gastric collaterals.
RPSPV
RASa
LPV
c d
b
Fig. 5.3 (a–d) Type 3 anatomy: the most common variation on the standard anatomy. The first branch of the main portal vein is the right posterior sector portal vein (RPS) leaving a common
trunk that divides into the right anterior sector portal vein (RAS) and the left portal vein (LPV)

335 Liver Anatomy: Variant Venous Anatomy and Implications for Resection
Paraumbilical varices arise from the left portal vein via the umbilical vein. Although this vein is obliterated in patients with normal portal pressure, it has the poten-tial to recanalize and serve as a conduit via the epigas-tric veins to the external iliac veins25 or course subcutaneously, forming a caput medusa.26,27 It is for this reason that the ligamentum teres must be securely ligated during mobilization of the liver. Similarly, care must be taken when dividing the triangular ligaments of the liver, as small vessels within these structures can become prominent with venous congestion. Sharp dis-section without ligation or diathermy will result in hemorrhage from these vessels. Furthermore, in a stenosed or occluded portal vein, cavernous transfor-mation can occur within 1 week of the event.28 This
results in the formation of venous channels within and around the affected portal vein (Fig. 5.5).
Major resection in the setting of portal hypertension is hazardous and predisposes the liver to even higher portal pressures postoperatively, thereby inhibiting nor-mal liver regeneration and increasing the risk of life-threatening bleeding. Evidence of varices on preoperative radiography and endoscopy may be the only findings to alert the surgeon of hepatic dysfunction in the absence ICG testing or other hepatic function tests.
5.3 Implications on Ductal Anatomy
Of interest to the surgeon and interventionalist, espe-cially when biliary cannulation or reconstruction is necessary, is the fact that portal vein variations are
RAPVV
VI
VII
VIII
IVII
III
LPV
a
b
Fig. 5.4 (a, b) An uncommon but surgically relevant anomaly occurs when the first branch of the portal vein is the segment VI (type 5) or VII branch (type 4). In this situation, the segment VI or VII branch, respectively, and the right anterior portal vein (RAPV) share a common trunk. Inadvertent ligation of the RAPV during left trisegmentectomy can result in hepatic failure due to insufficient portal flow to the remnant
a
b
Fig. 5.5 (a, b) Contrast-enhanced CT images from a patient with cavernous transformation of the portal vein. There are extensive varices as a result and a large splenorenal shunt

34 A.V. Maker et al.
associated with distinct bile duct variations. This has been identified in studies of liver cast specimens and by conventional cholangiography.16,29,30 In patients with type 3 portal vein anatomy, a classic bile duct branching pattern is found significantly less fre-quently than in patients with standard anatomy. These patients often have a right posterior sectoral duct draining into the left hepatic duct with a supraportal course, or into the common bile duct with an infra-portal course (Fig. 5.6). Furthermore, these patients have a higher incidence of left lateral segment ducts coursing caudal to the umbilical portion of the left portal vein.19 As in cases of variant portal anatomy, variant biliary anatomy must be investigated prior to ligation, as biliary congestion of the functional rem-nant can lead to liver dysfunction. Evidence of portal vein anomalies should alert the surgeon to possible biliary variation and careful dissection during liver resection. The safest course of action in these patients is to address the biliary radicals during parenchymal transection and to avoid extrahepatic dissection of the ducts. Other ways to avoid biliary complications are to perform magnetic resonance cholangiopancreatog-raphy (MRCP) or intraoperative cholangiography.
5.4 Implications for Portal Vein Embolization
A healthy, non-cirrhotic individual requires a functional hepatic reserve of at least approximately 20% the origi-nal liver volume. The regenerative capacity of the liver
should enable full functional compensation within weeks of resection. Once greater than 50% of liver volume is resected, the risk of clinically significant liver insufficiency does exist, and particular care must be taken, especially with extended right hepatectomy. In patients who are otherwise candidates for hepatic resec-tion, the lack of adequate functional liver remnant may be the only obstacle to curative resection.
In cases where liver function may be impaired due to steatohepatitis, hepatitis, or cirrhosis, or when extended resection is necessary to gain tumor-free margins, portal vein embolization is frequently employed to induce hypertrophy of the proposed liver remnant in an effort to increase the number of patients who are candidates for hepatic resection.31,32 Portal vein embolization was described in humans in the 1980s,33,34 more than 50 years after it was discovered that rabbit portal vein ligation induced contralateral lobar hypertrophy.35,36 Knowledge of the portal venous anatomy for each patient determines the success of the forced liver hypertrophy, and more importantly, spares the functional liver remnant from inadvertent embolization.
5.4.1 Hepatic Vein Variations
Although there are multiple small veins that drain the right lobe and segment I directly into the retrohepatic vena cava, the majority of hepatic blood flow drains into the inferior vena cava (IVC) via the left, middle, and right hepatic veins. In major hepatectomy, extrahepatic control of these vessels is preferred, especially when the tumor is large and near the confluence of the hepatic veins, or is attached to the IVC or the dia-phragm. Standard anatomy consists of a single right hepatic vein entering the vena cava, and left and mid-dle hepatic veins that join the vena cava as a single trunk. Autopsy studies of the left and middle hepatic venous trunk have elucidated at least five types of middle and hepatic vein trunk variants37 (Fig. 5.7). Type I has no branching within 1 cm of the IVC, type II has two branches within 1 cm of IVC (most com-mon), type III is a trifurcation, type IV is a quadrifica-tion, and type V has independent middle and left hepatic veins draining into the IVC. When the left and middle hepatic veins form a common trunk, control of the left hepatic vein alone is often not possible extra-hepatically. Complete exposure generally requires full mobilization of the left liver, and division of the
Fig. 5.6 Catheter cholangiogram shows the most common anatomic variant of the bile ducts associated with variant portal vein anatomy in which the right posterior bile duct (RPBD) drains into the left bile duct (LBD).

355 Liver Anatomy: Variant Venous Anatomy and Implications for Resection
ligamentum venosum allows a tunnel to be dissected between the IVC and the middle and left hepatic veins. It is important to identify the hepatic venous anatomy preoperatively and realize if there are variations in the branching patterns since bleeding in this area can be difficult to control.
5.5 Conclusion
The complexity of radiologic and surgical interven-tions on the liver has increased in the last decade. Knowledge of anatomical variants is crucial for safe hepatic resection and for preservation of adequate
inflow and outflow to the functional remnant liver tissue. There are many congenital and acquired anom-alies of the portal vein that need to be identified preop-eratively, and their presence may indicate concomitant variations in biliary ductal anatomy.
References
1. Joyce AD, Howard ER. Rare congenital anomaly of the por-tal vein. Br J Surg. 1988;75(10):1038-1039.
2. Marks C. Developmental basis of the portal venous system. Am J Surg. 1969;117(5):671-681.
3. Massin M, Verloes A, Jamblin P. Cardiac anomalies associ-ated with congenital absence of the portal vein. Cardiol Young. 1999;9(5):522-525.
4. Walsh G, Williams MP. Congenital anomalies of the portal venous system – CT appearances with embryological con-siderations. Clin Radiol. 1995;50(3):174-176.
5. Gallego C, Velasco M, Marcuello P, Tejedor D, De Campo L, Friera A. Congenital and acquired anomalies of the portal venous system. Radiographics. 2002;22(1):141-159.
6. Hu GH, Shen LG, Yang J, Mei JH, Zhu YF. Insight into congenital absence of the portal vein: Is it rare? World J Gastroenterol. 2008;14(39):5969-5979.
7. Laverdiere JT, Laor T, Benacerraf B. Congenital absence of the portal vein: case report and MR demonstration. Pediatr Radiol. 1995;25(1):52-53.
8. Zhang JS, Wang YP, Wang MQ, et al. Diagnosis of an acces-sory portal vein and its clinical implications for portosystemic shunts. Cardiovasc Interv Radiol. 1996;19(4):239-241.
9. Parisato FO, Pataro EF. Anomalous portal vein. Vena porta anomalia. Angiologia. 1965;17(3):119-123.
10. Lundstedt C, Lindell G, Tranberg KG, Svartholm E. Congenital absence of the intrahepatic portion of the portal vein in an adult male resected for hepatocellular carcinoma. Eur Radiol. 2001;11(11):2228-2231.
11. Guariso G, Fiorio S, Altavilla G, et al. Congenital absence of the portal vein associated with focal nodular hyperplasia of the liver and cystic dysplasia of the kidney. Eur J Pediatr. 1998;157(4):287-290.
12. Marois D, van Heerden JA, Carpenter HA, Sheedy PF 2nd. Congenital absence of the portal vein. Mayo Clin Proc. 1979;54(1):55-59.
13. Matsuoka Y, Ohtomo K, Okubo T, Nishikawa J, Mine T, Ohno S. Congenital absence of the portal vein. Gastrointest Radiol. 1992;17(1):31-33.
14. Nakasaki H, Tanaka Y, Ohta M, et al. Congenital absence of the portal vein. Ann Surg. 1989;210(2):190-193.
15. Covey AM, Brody LA, Getrajdman GI, Sofocleous CT, Brown KT. Incidence, patterns, and clinical relevance of variant portal vein anatomy. AJR Am J Roentgenol. 2004; 183(4):1055-1064.
16. Cheng YF, Huang TL, Chen CL, et al. Anatomic dissociation between the intrahepatic bile duct and portal vein: risk factors for left hepatectomy. World J Surg. 1997;21(3):297-300.
17. Ko S, Murakami G, Kanamura T, Sato TJ, Nakajima Y. Cantlie’s plane in major variations of the primary portal vein ramification at the porta hepatitis: cutting experiment using cadaveric livers. World J Surg. 2004;28(1):13-18.
a
b
Fig. 5.7 (a) Coronal oblique reformatted CT demonstrates type II hepatic vein anatomy. (b) Axial contrast-enhanced CT show-ing type III hepatic vein anatomy in which the right (RHV), middle (MHV), and left (LHV) hepatic veins trifurcate from the IVC. Incidental note is made of a small accessory RHV

36 A.V. Maker et al.
18. Yamane T, Mori K, Sakamoto K, Ikei S, Akagi M. Intrahepatic ramification of the portal vein in the right and caudate lobes of the liver. Acta Anat. 1988;133(2):162-172.
19. Kitami M, Takase K, Murakami G, et al. Types and frequen-cies of biliary tract variations associated with a major portal venous anomaly: analysis with multi-detector row CT cho-langiography. Radiology. 2006;238(1):156-166.
20. Goldsmith NA, Woodburne RT. The surgical anatomy pertain-ing to liver resection. Surg Gynecol Obstet. 1957;105:310-318.
21. Hata F, Hirata K, Murakami G, Mukaiya M. Identification of segments VI and VII of the liver based on the ramification patterns of the intrahepatic portal and hepatic veins. Clin Anat. 1999;12(4):229-244.
22. Atri M, Bret PM, Fraser-Hill MA. Intrahepatic portal venous variations: prevalence with ultrasound. Radiology. 1992;184: 523-526.
23. Cheng YF, Huang TL, Chen CL, Chen YS, Lee TY. Variations of the intrahepatic bile ducts: application in living related liver transplantation and splitting liver transplanta-tion. Clin Transplant. 1997;11(4):337-340.
24. Filly RA, Laing FC. Anatomic variation of portal venous anatomy in the porta hepatitis: ultrasonographic evaluation. J Clin Ultrasound. 1978;6(2):83-89.
25. Williams PL. Veins of the abdomen and pelvis: hepatic por-tal system. In: Williams PL, ed. Gray’s Anatomy. 38th ed. New York: Churchill Livingstone; 1999:1602-1604.
26. Cho KC, Patel YD, Wachsberg RH, Seeff J. Varices in portal hypertension: evaluation with CT. Radiographics. 1995;15(3):609-622. A review publication of the Radiological Society of North America, Inc.
27. Ito K, Higuchi M, Kada T, et al. CT of acquired abnormalities of the portal venous system. Radiographics. 1997;17(4):897-917.
28. De Gaetano AM, Lafortune M, Patriquin H, De Franco A, Aubin B, Paradis K. Cavernous transformation of the portal
vein: patterns of intrahepatic and splanchnic collateral circu-lation detected with Doppler sonography. Am J Roentgenol. 1995;165(5):1151-1155.
29. Ishiyama S, Yamada Y, Narishima Y, Yamaki T, Kunii Y, Yamauchi H. Surgical anatomy of the hilar bile duct. Tan Sui J Biliary Tract Pancreas. 1999;20:811-820.
30. Kumon M, Matsuhima M, Itahara T. Gross anatomy of the liver hilus and caudate lobe using corrosion casts of the liver. Tan Sui Biliary Tract Pancreas. 1989;10:1417-1422.
31. Abulkhir A, Limongelli P, Healey AJ, et al. Preoperative portal vein embolization for major liver resection: a meta-analysis. Ann Surg. 2008;247(1):49-57.
32. Covey AM, Brown KT, Jarnagin WR, et al. Combined portal vein embolization and neoadjuvant chemotherapy as a treat-ment strategy for resectable hepatic colorectal metastases. Ann Surg. 2008;247(3):451-455.
33. Kinoshita H, Sakai K, Hirohashi K. Preoperative portal vein embolization for hepatocellular carcinoma. World J Surg. 1986;10(5):803-808.
34. Makuuchi M, Thai BL, Takayasu K, et al. Preoperative por-tal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery. 1990;107(5):521-527.
35. Bax HR, Mansens BJ, Schalm L. Atrophy of the liver after occlusion of the bile ducts or portal vein and compensatory hypertrophy of the unoccluded portion and its clinical importance. Gastroenterology. 1956;31(2):131-155.
36. Makuuchi M et al. Preoperative transcatheter embolization of the portal venous branch for patients receiving extended lobectomy due to the bile duct carcinoma. J Jpn Soc Clin Surg. 1984;45:1558.
37. Nakamura S, Tsuzuki T. Surgical anatomy of the hepatic veins and the inferior vena cava. Surg Gynecol Obstet. 1981; 152(1):43-50.