Embed Size (px)
Citation preview

The Journal of Pathology
Vol. 119 No. 2
VENOUS I N F A R C T I O N O F THE A D R E N A L GLANDS
B. Fox Department of Histopathology, Charing Cross Hospital Medical School, London
PLATES XVI-XXII
THE pathogenesis of adrenal haemorrhage and necrosis in man is often obscure. In a recent personal study of 78 cases it was possible to clarify the pathogenesis by emphasising the role of vascular damage (Fox, 1973). There were 32 cases, which are reported here, of adrenal infarction due to thrombosis of the venous supply. It has not previously been appreciated that in this type of case there is not only thrombosis of the central veins but also of the capsular veins. It has been suggested &at adrenal vein thrombosis is secondary to the parenchymal changes (Sheehan, 1955; Thrash and Iri, 1963; Greendyke, 1965), but in this series it appears to be primary. It is apparent that until an explanation is found for adrenal vein thrombosis the pathogenesis of haemorrhage and necrosis will remain obscure. A hypothesis is presented to account for thrombosis of the adrenal venous supply.
MATERIALS AND METHODS
The cases are summarised in table I. In 21 cases the whole of both adrenal glands were examined. In one case the whole of the left and half of the right gland were available, and in one case the right gland only. The glands with surrounding connective tissue were fixed in 4 per cent. neutral formaldehyde saline. After fixation the whole gland was cut trans- versely into blocks of tissue about 4 mm thick; serial sections from all the blocks were pre- pared. There were single cases in which eight, six, five, four and three blocks were examined and three cases in which there were two blocks. Serial sections through the whole of all the paraffin blocks were prepared. In all cases at least every tenth section was stained with hae- malum and eosin (HE). Other sections were stained with Mallory’s phosphotungstic acid- haematoxylin (PTAH) by the Picro-Mallory technique, the modified Picro-Mallory technique for platelets (Carstairs, 1965), Martius-scarlet-blue (MSB) for fibrin (Lendrum et al., 1962), James’ (1967) silver impregnation method for reticulin, Moore’s and Gomori’s aldehyde fuschin stains for elastic, Perls’ reaction and the van Gieson (VG), periodic acid-Schiff (PAS), Giemsa, and Gram-Weigert methods. All tissues from other organs obtained at necropsy were fixed in 4 per cent, neutral formaldehyde saline. Sections were prepared and stained with HE, PTAH and occasionally with MSB and Giemsa and Gram-Weigert methods.
Received 9 January 1975; accepted 22 July 1975. J. PATH.-VOL. 119 (1976) 65 E

TA
BL
E
I V
enous infarction of adrenal glands; clinical findings
Blood
pressure (m
m H
g) Shock
lo5P inrecordable
I40/60
+ -
140/80 -
110/70 N
o
record
Case
Clinical
diagnosis M
ode of death
Significant investigations
Treatm
ent O
ther significant inform
ation O
rganisms
isolated
...
Ps. pyocyaneus in sputum
S. pneum
oniae in sputum
" C
olifo~m
", organism
s in urine
Age
Cyanosis
+ + -
I- 1
64M
Bronchopneum
onia C
hronic bronchitis E
mphysem
a
Sudden collapse Serum
sodium
131 mE
q/l. Serum
potassium
5.2 mE
q/l
Chloram
phenicol M
ephentermine
Pain and guarding right subcostal
region one
day before death
78M
Acute
on chronic
bronchitis C
or pulmonale
Auricular fibrillation
Sudden collapse Serum
sodium
132 mE
q/l. Serum
potassium
4.6 mE
q/l
Penicillin Streptom
ycin
Tetracycline
Digoxin
Tracheostom
y
71F Sudden collapse
Serum sodium
135 m
Eq/l.
Serum potasyium
4.2 m
Eq/l
Choline
Theophyl!jnate Franol
Chronic bronchial asthm
a 165/120
1 -
Tetracycline
Am
inophylline D
igoxin
80M
Bronchopneum
onia Steatorrhoea of un-
Congestive
cardiac know
n cause
failure
Gradually
deterio- rated over 3 days during w
hich time
pyrexia present
E.
Coli
in urine
Blood
urea 240
mg/100 m
l after
operation falling to 82 m
g/100 ml
Nitrofurantoin
Streptomycin
Prednisolone 10 m
g qds for 1 day, 3 days be- fore death
I- 140/75
Laparotom
y 40
days before death
86M
Renal failure due to urinary tract infection
Urethral stricture w
ith bladder calculi
Gradually deterio- rated
Pr. vulgaris in urine
Blood urea 11 1 m
gjl00 ml
rising to 330 m
g/100 ml
Serum sodium
120 m
Eq/l and
serum potas-
sium 5.5
mE
q/l
Nitrofurantoin
...
I- 54M
G
angrene of ileum
due to adhesions
Gradually
deterio- rated for
4 days
after 2nd
oper- ation
E. Coli in
wound sw
ab and sputum
Blood urea 200 m
g/lM) m
l; fel to 66 m
gllOO
m
l
Resection of ileum
H
ydrocortisone 100 m
g i.v. once
following 2nd
operation
2 days after 1st operation collapsed
BP
130/70, falling
to 80160.
2 days
later 2nd
oper- ation for breakdow
n of anastom
osis

.-
Shoc
k
__
+
__
Cya
nosi
__
+
Sign
ifica
nt
inve
stig
atio
ns
Tre
atm
ent
Oth
er s
igni
fica
nt
info
rmat
ion
Cas
e C
linic
al
diag
nose
s M
ode
of
deat
h B
lood
pr
essu
re
(mm
Hg)
O
rgan
ism
s is
olat
ed
...
Blo
od c
hole
ster
ol
295
mg/
100
ml
Peni
cilli
n T
riio
doth
yron
ine
Hyp
othe
rmia
with
com
a Fo
r 3
days
. R
ecta
l te
mpe
ratu
re 3
5-35
6°C
7 C
ereb
rova
scul
ar
Myx
oede
ma,
com
a B
ronc
hopn
eum
onia
acci
dent
lrn
f1O
0 in
reco
rdab
le
7%
+ +
S. fa
ecal
is
in u
rine
On a
res
pira
tor
...
8 Po
lyne
uriti
s with
re
spir
ator
y di
ffic
ulty
Sudd
en c
olla
pse:
di
ed i
n If
hours
9 G
angr
ene
of s
mal
l in
test
ine
due
to
adhe
sion
s C
onge
stiv
e ca
rdia
c fa
ilure
B
ronc
hopn
eum
onia
Sudd
en c
olla
pse :
di
ed a
bout
12
hr
late
r
lZ0/
50
100/
50
1 +
Nil
Peni
cilli
n ...
Seru
m c
hlor
ide
93 m
Eq/
L
Blo
od u
rea
80
mg/
100
ml on
day
of c
olla
pse
inte
stin
e
Adm
itted
in s
emi-
com
a an
d di
ed
abou
t 12
hr
late
r
No
reco
rd
No
reco
rd
-
+
-
-
No
reco
rd
__
+
__
-
No
reco
rd
No
reco
rd
A k
now
n tr
amp.
R
ecta
l te
mpe
ratu
re on
ad
- m
issi
on 2
66°C
ri
sing
to
36°
C
10
Hyp
othe
rmia
M
alnu
triti
on
Pla
sma a
l bum
in
1.7
g/lW
ml
Blo
od c
hole
ster
ol
98 m
g/10
0 m
l Se
rum
pot
assi
um
4.4
dq
ll
Seru
m s
odiu
m
130
da
/l
...
... In
test
inal
obs
truc
- tio
n C
arci
nom
atos
is
? pr
imar
y tr
ans-
ve
rse c
olon
Sudd
en c
olla
pse :
di
ed 1
3 hr
late
r 15
0/10
0
106/
60
.I- 60
/40
190/
100
12
Car
cino
mat
osis
, pr
imar
y si
te n
ot
know
n B
ronc
hopn
eum
onia
Gra
dual
ly
dete
rior
ated
for
3
days
Peni
cilli
n ...
...

TA
BL
E
I (c
ontin
ued)
-. _
_
Cas
e C
linic
al
diag
nose
s M
ode
of
deat
h Sh
ock
Org
anis
ms
isol
ated
Si
gnif
ican
t in
vest
igat
ions
T
reat
men
t O
ther
sig
nifi
cant
in
form
atio
n B
lood
pr
essu
re
(mm
Hg)
Not
re
cord
ed
6010
13
-
14
1M
.-
78M
Infa
ntile
ecz
ema
Oed
ema
Rap
id d
eter
iora
tion
over
16
hr: d
ied
in
com
a
S. a
ureu
s fr
on
fing
er
WB
C 2
3,00
0 pe
r
Plat
elet
s 48
1,00
0 eu
mm
per
cu m
m
Top
ical
gen
tian
viol
et
Boi
ls
on
scal
p tr
eate
d w
ith
peni
cilli
n an
d pr
edni
solo
ne
Bro
ncho
pneu
mon
ia
Con
gest
ive c
ardi
ac
Shoc
k fa
ilure
Sudd
en c
olla
pse:
di
ed 3
hr
late
r ...
100m
gHyd
ro-
cort
ison
e 1V
14
-day
his
tory
of
pneu
- m
onia
tr
eate
d w
ith
antib
iotic
s
...
15
66F
Bro
ncho
pneu
mon
ia
Myo
card
ial i
nfar
c-
Rhe
umat
oid
arth
riti
s tio
n
Die
d af
ter
14 d
ays
in c
oma
I20/
80
80/5
0 1
+ K
I. a
erog
enes
fr
om t
ra-
chea
l sw
ab
Seru
m s
odiu
m
130
mE
o/l
Am
oici
llin
Hyd
roeo
rtio
sne
IV a
nd I
M
Dig
oxin
ca
rdia
l inf
arct
16
6OM
C
arci
nom
atos
is,
prim
ary
site
not
kn
own
Gra
dual
ly d
eter
io-
rate
d N
o re
cord
N
o re
cord
N
<
reco
...
Pl
eura
l bio
psy
show
ed m
eta-
st
atic
tubu
lar
aden
ocar
- ei
nom
a
Pres
ente
d w
ith
scia
tica
and
then
de
velo
ped
left-
side
d pl
eura
l ef
fu-
sion
...
17
60M
H
ypot
herm
ia d
ue to
Bro
ncho
pneu
mon
ia
Bila
tera
l “tr
ench
expo
sure
foot
”
Die
d af
ter
24 h
r of
se
mi-
cons
ciou
snes
s 10
0/80
J.
7010
j.
1101
90
+ P
r. v
ulga
ris
from
spu
tu
and
leg
H. i
nflu
enm
e fr
om sp
utui
Seru
m so
dium
14
1 m
Eol
l A
mpi
cilli
n C
loxa
cilli
n A
va
gran
t fo
und
col-
la
psed
. R
ecta
l tem
per-
at
ure
24°C
whi
ch r
ose
over
a p
erio
d of
3 d
ays
to 3
7.8”
C
Seru
m p
otaS
.sium
3.
8 m
Eq/
l B
lood
ure
a 53
mg/
100
ml
2 da
ys b
efor
e 8
hour
ly
deat
h -_
_
...
18
2M
Fa
mili
al n
ephr
otic
sy
ndro
me
Gra
dual
ly d
eter
io-
rate
d Su
dden
col
laps
e w
ith d
eath
in
min
utes
1201
85
AC
TH
unt
il 3
mth
Aza
thio
prin
e Py
rido
xine
befo
re d
eath
...
U
rina
ry p
rote
in
7.0
g da
ily
Seru
m p
rote
ins
Seru
m a
lbum
in
2.2
g/lO
O m
l
4.4 g/
loo
‘?I
...
19
4SF
Rap
id d
eter
iora
tion
over
10
days
. Su
dden
dea
th f
ol-
low
ing
aspi
ratio
n of
vom
itus
Mis
t te
nt
Oxy
gen
Clo
xaci
llin
Col
istin
A
min
ophy
lline
Rec
urre
nt r
espi
rato
ry i
n-
fect
ions
from
1 y
r on-
war
ds
Bro
ncho
pneu
mon
ia
Bro
nchi
ecta
sis
Fibr
ocys
tic d
isea
se
of p
ancr
eas
No
reco
rd

Clin
ical
di
agno
ses
Mod
e of
de
ath
Org
anis
ms
isol
ated
Si
gnif
ican
t in
vest
igat
ions
T
reat
men
t O
ther
sig
nifi
cant
in
form
atio
n C
ase
Shoc
k C
yano
sis
__
--
+ No
reco
rd
+ + No
reco
rd
20
~
21
56M
~
66M
__
51
F
~
55M
Sudd
en c
olla
pse
follo
win
g gr
adua
l de
teii
oral
ion
I2Ol
7O
60/3
0 +
Pred
niso
ne
Hyd
roco
rtis
one
IV
Am
pici
llin
IV
Met
aram
inol
26
days
be
fore
de
ath
pigm
enta
tion
in m
outh
no
ticed
. D
ay
befo
re
deat
h,
colla
psed
, th
ough
t to
be
due
to
gram
-neg
ativ
e ba
cter
- ae
mic
sho
ck
Ren
al f
ailu
re d
ue
rapi
dly
prog
res!
ty
pe o
f gl
omer
h ne
phri
tis
Ren
al b
iops
y B
lood
ure
a up
to
552
mg/
lI+l
ml
Seru
m
sodi
um
134
mE
oll
No
reco
rd
~
+
...
Sudd
en
oper
atio
n co
llaps
e B
P. a
fter
8010 m
m
Hg
whi
ch
resp
onde
d to
Hyd
roco
rtis
one
Peri
toni
tis d
ue t
o pe
rfor
ated
duo
- de
nal u
lcer
B
ronc
hopn
eum
on
1201
90
110/
60
j. H
ydro
cort
ison
e IV
an
d IM
IV S
alin
e A
chro
mvc
in 1V
Am
pici
llin
Bec
ame
drow
sy a
nd t
hen
deep
ly c
omat
ose
22 h
r af
ter
acci
dent
22
__
23
Shoc
k M
ultip
le fr
actu
res
ribs
170/
100
...
...
acci
dent
No
reco
rd
+ ...
A
min
ophy
lline
D
igita
lis
Chr
onic
21
yr
. br
onch
itis
On
day
of fo
r
colla
pse
resp
irat
ory
acid
osis
fou
nd
Acu
te o
n ch
roni
c br
onch
itis
Em
phys
ema
Con
gest
ive c
ardi
at
failu
re
Sudd
en c
olla
pse
Die
d w
ithin
min
utes
24
85M
N
o re
cord
N
o re
cord
-
Pr.
vul
sari
s in
uri
ne
Blo
od u
rea
114
mg/
100
ml
ris-
in
g to
295
mg/
10
0 m
l fa
ll-
ing
to 1
51 m
g/
100
ml.
Hb
7.4
gll0
0 m
l. W
BC
24,
200
per
cu m
m.
96p&
neut
ro-
phils
2 d
ays
befo
re d
eath
Tet
racy
clin
e A
mpi
cilli
n
Nal
idix
ic a
cid
Ope
ratio
n fo
r du
oden
al
ulce
r 8
yr
prev
ious
ly
Ura
emia
H
aem
orrh
agic
cy
stiti
s
Sudd
en c
olla
pse
Die
d w
ithin
min
utes

TA
BL
E
1 (c
ontin
ued)
Rem
aine
d in
com
a fo
r 4
days
and
di
ed
100/
80
7016
0
Sudd
enly
die
d 40
+i
n.
afte
r adm
is-
sion
80/5
0
Col
laps
ed a
nd d
ied
in I
f hr
U
nrec
orda
ble
Sudd
en c
olla
pse
Die
d in
10
min
. 17
01 10
0
Org
anis
ms
isol
ated
Si
gnif
ican
t in
vest
igat
ions
O
ther
sig
nifi
cant
in
form
atio
n B
lood
pr
essu
re
Mod
e of
de
ath
(m
Hg)
C
linic
al
diag
nose
s C
ast
Shoc
k
__
_
-
-
+
Cya
nosi
s T
reat
men
t
25
59F
Hyp
othe
rmia
M
yxoe
dem
a co
ma
No
reco
rd
...
Rec
tal
tem
pera
ture
on
adm
issi
on 3
0°C
gra
d-
ually
ri
sing
to
33
°C.
Rem
aine
d in
com
a
Seru
m p
rote
in-
boun
d io
dine
0.
4 m
g/10
0 m
l B
lood
cho
les-
te
ro14
17 m
g/
100
ml ...
IV fl
uids
T
riio
do-t
hyro
nine
26
-
27
81M
__
79
F
Bum
s in
volv
ing
60%
bo
dy s
urfa
ce
Det
erio
rate
d an
d 13
0/80
di
ed in
36
hr
Blo
od
pres
sure
m
ain-
ta
ined
at
norm
al l
evel
IV fl
uids
and
pl
asm
a ...
Lef
t ven
tric
ular
fa
ilure
t
+ ...
...
A
min
ophy
lline
4-
day
hist
ory
of
dysp
- no
ea.
28
45M
...
R
lood
urea
Rec
tal t
empe
ratu
re
353°
C.
Impr
oved
the
ne
xt
2 da
ys b
ut c
ol-
laps
ed o
n 4t
h da
y
Hyp
othe
rmia
Sc
hizo
phre
nia
Seru
m p
otas
sium
5.
1 m
Eq/
l 2+
days
bef
ore
deat
h
Ben
zhex
ol
29
-
30
60M
~
71M
? M
enin
gitis
C
onge
stiv
e ca
rdia
c fa
ilure
Cer
ebro
spin
al
flui
d cl
oudy
80
WB
C p
er cu
mm
Pr
otei
n 10
0 m
g/
l00m
l Se
rum
sod
ium
13
5 m
Eq/
l Se
rum
pot
assi
um
3.2
mE
q/l
Dig
italis
B
ariu
m
mea
l 2
yr
pre-
vi
ousl
y sh
owed
ir
re-
gula
rity
on
less
er cu
rve
? ca
rcin
oma.
G
astr
o-
scop
y ap
pear
ed n
orm
al
Sudd
en c
olla
pse
1151
65
Die
d in
3 h
ours
I
Foun
d de
ad i
n be
d B
ronc
hitis
2 y
r ...
...
...
...
31
67M
B
ronc
hopn
eum
onia
C
hron
ic b
ronc
hitis
E
mph
ysem
a
+ +
...
...
Am
pici
llin
Oxy
gen
36 h
r be
fore
dea
th c
om-
plai
ned
of
cons
tant
ac
he in
lef
t hy
poch
on-
driu
m
32
70M
B
ronc
hitis
man
y
Foun
d de
ad in
cha
ir
year
s ...
...
...

ADRENAL GLAND INFARCTION 71
RESULTS 1. Pathological Findings
a. Necropsy Jindings The necropsy findings including the macroscopic changes in the adrenal
glands are summarised in table 11. In the cases with massive haemorrhage there was a central area of haemorrhage surrounded by pale necrotic-looking cortex (fig. 1) and there was often haemorrhage and oedema of the surrounding connective tissue. In only three cases were thrombi seen in the main adrenal veins.
b. Histological findings in the adrenal glands The findings are summarised in table I11 which includes an estimate of the
amount of adrenal gland involved in those cases in which the whole gland was examined, and an estimate of the age of the lesions. The age of the lesions was estimated by comparing them with cases where the maximum time the adrenal lesions could have been present was known, that is postoperative cases previously described (Fox, 1969) and case 22 which followed trauma.
There are two main types of adrenal lesions: Type I-Adrenal venous thrombosis with mainly central haemorrhage and extensive ischaemic necrosis, cases 1, 3, 6, 8, 9, 10, 11, 12, 13, 16, 17, 20, 21, 23, 25, 26, 28, 29, 31, 32; 14, 22,24 right gland only; 27 left gland only. Type 2-Adrenal venous thrombosis with mainly extensive ischaemic necrosis and minimal haemorrhage, cases 2, 4, 5, 7, 15, 18, 19, 30; 14 and 24 left gland only; 27 right gland only.
A. Parenchymal changes Type 1
(i) Haemorrhage The haemorrhage involves the medulla, the alar raphe, and often extends
in an irregular way into the cortex, usually involving the zona reticularis and inner zona fasciculata, and occasionally reaching the capsule and periadrenal connective tissue. The haemorrhage usually has a uniform appearance, although occasionally there are areas, mainly around the centre, in which the red cells have lost their normal staining characterictics. There are thin and thick bands of fibrin scattered throughout the haemorrhage and occasionally there are large masses of fibrin around the edges, particularly in the region of the vascular dam.
In cases 9, 11 left gland, and 26, of apparently recent haemorrhage, there is a close relationship between the haemorrhage and thrombosed venous sinuses or intra-adrenal veins. Within the areas of haemorrhage there is marked disruption of the reticulin pattern with fragmentation and loss of reticulin fibres. There is necrosis and loss of individual medullary and cortical cells in the areas of haemorrhage.
(ii) Necrosis (a) Extensive ischaemic necrosis-The term " extensive " is used to dis-
tinguish the lesion from those of focal and segmental necrosis (Fox, 1969).

Cas
e
Enl
arge
d an
d ha
emor
rhag
ic
1
Gen
eral
ised
faec
ulen
t per
itoni
tis, l
eaka
ge o
f ile
al a
nast
omos
is, g
angr
ene
of i
leum
, old
ren
al tu
bula
r ne
cros
is a
nd s
ubca
psul
ar a
bsce
ss in
live
r
2 3 4 5 6 7
TA
BL
E I1
Ven
ous i
nfar
ctio
n of
adr
enal
gla
nds;
nec
rops
y fin
ding
s
Mac
rosc
opic
al fi
ndin
gs in
adr
enal
s I
Rig
ht
Mas
sive
hae
mor
rhag
e
Hae
mor
rhag
ic
(6x
5 x
2 cm
)
Hae
mor
rhag
ic
(7x5
x3.5
cm)
Nor
mal
Hae
mor
rhag
ic
(5.5
x 2
3 x
2 cm
)
Enl
arge
d an
d ha
emor
rhag
ic
Are
a of
hae
mor
rhag
e (2
x I x
0.5
cm
)
Lef
t
Mas
sive
hae
mor
rhag
e
Oth
er s
igni
fican
t fin
ding
s
~-
Supp
urat
ive
bron
chop
neum
onia
. C
or p
ulm
onal
e, a
cute
on
chro
nic
bron
chiti
s an
d em
phys
ema.
B
ronc
hiec
tasi
s.
Nec
rotis
ing
ulce
ratio
n of
oes
opha
gus
with
fib
rin
thro
mbi
in
vein
s an
d ca
pilla
ries
Hae
mor
rhag
ic
(45
x4
x2
cm)
Em
pyem
a (r
ight
), m
ultip
le l
ung
absc
esse
s an
d br
onch
opne
umon
ia.
Fibr
in t
hrom
bi i
n ve
in o
f th
yroi
d Le
ft ve
ntri
cula
r hy
pert
roph
y.
glan
d
Are
a of
hae
mor
rhag
e Su
ppur
ativ
e br
onch
opne
umon
ia a
nd
emph
ysem
a.
Sube
ndoc
ardi
al
(2
~2
~0
.8
cm
) ha
emor
rhag
e in
nor
mal
-siz
ed he
art.
Fibr
in i
n al
veol
i I I
Nor
mal
Su
ppur
ativ
e br
onch
itis
and
orga
nisi
ng b
ronc
hopn
eum
onia
. M
icro
- ab
sces
ses
in k
idne
ys, h
eart
and
spl
een.
B
enig
n ne
phro
scle
rosi
s with
ol
d tu
bula
r ne
cros
is.
Foca
l ne
cros
is i
n liv
er.
Fibr
in i
n w
alls
of
sple
nic
arte
ries
, alv
eoli,
and
ulc
er in
tong
ue
Hae
mor
rhag
ic
(5.5
x 2
.8 x
23
cm
) U
reth
ral
stri
ctur
e, w
ith
chro
nic
uret
hral
ab
sces
s,
hype
rtro
phy
of
blad
der,
necr
otis
ing
cyst
itis,
ves
ical
cal
culi,
pro
stat
ic h
yper
trop
hy
andc
hron
icpy
elon
ephr
itis.
Sup
pura
tiveb
ronc
hopn
eum
onia
. Fi
brin
in
vei
ns o
f bl
adde
r
Are
a of
hae
mor
rhag
e (1
x 1
~0
.5
cm)
Dif
fuse
su
ppur
ativ
e br
onch
opne
umon
ia,
atro
phy
of
thyr
oid,
ol
d fi
broc
aseo
us p
ulm
onar
y tu
berc
ulos
is,
fibr
osis
of
hear
t an
d ch
roni
c pe
rica
rdi ti
s

Mac
rosc
opic
al fi
ndin
gs in
adr
enal
s C
ase
Oth
er s
igni
fican
t fin
ding
s Le
ft R
ight
Mas
sive
hae
mor
rhag
e N
orm
al
8 A
trop
hy o
f pe
riphe
ral
nerv
es a
nd m
usci
es.
Thre
e sh
allo
w u
lcer
s in
sm
all i
ntes
tine.
B
ronc
hopn
eum
onia
. Fi
brin
in v
eins
and
arte
ries
in
ileal
ulc
er
Are
a of
hae
mor
rhag
e A
rea
of h
aem
orrh
age
Gen
eral
ised
fae
cule
nt p
erito
nitis
, br
eakd
own
of s
utur
e lin
e in
sm
all
inte
stin
e.
Bro
ncho
pneu
mon
ia w
ith a
bsce
ss fo
rmat
ion
9 10
Nor
mal
N
orm
al
Myo
card
ial
fibro
sis
and
brow
n at
roph
y.
Bro
ncho
pneu
mon
ia.
Car
- ci
noid
tum
our
of s
mal
l int
estin
e
Sphe
roid
al c
ell c
arci
nom
a of
sto
mac
h w
ith i
nvol
vem
ent o
f tra
nsve
rse
colo
n an
d pe
riton
eum
. A
ctiv
e ch
roni
c ch
olan
gitis
. Tu
bula
r de
gene
ratio
n an
d ne
cros
is in
the
kidn
eys.
Fibr
in in
wal
ls o
fpan
crea
tic
arte
ries,
vei
ns a
nd ca
pilla
ries,
and
sple
nic a
rterie
s
Con
gest
ion
11
Con
gest
ion
Cen
tral l
ique
fact
ion
Met
asta
tic c
arci
nom
a (5
x 3
x 2
5 cm
) 12
M
etas
tatic
car
cino
ma
(4x3
x3cm
) A
deno
carc
inom
a of
tai
l of
pan
crea
s w
ith i
nvol
vem
ent
of s
tom
ach,
sp
leen
, le
ft ad
rena
l gl
and
and
right
kid
ney.
M
etas
tatic
dep
osits
in
ceo
liac
lym
ph n
odes
, liv
er a
nd k
idne
y.
Isch
aem
ic in
farc
tion
of
sple
en w
ith fi
brin
in a
rterie
s
Nor
mal
Tw
o ar
eas
of in
farc
tion
(1 x
05
x 0.
2 cm
and
(0
5 x
02.x
0.2
cm)
Thro
mbu
s in
ext
ra-a
dren
al
vein
(1.6
x 0
.5 x
0.3
cm)
Wid
espr
ead
ecze
ma,
ulc
ers o
n fin
gers
and
bron
chop
neum
onia
13
Smal
l hae
mor
rhag
e Su
ppur
ativ
e br
onch
opne
umon
ia,
bron
chie
ctas
is
and
emph
ysem
a.
Fibr
in i
n al
veol
i of
lung
s an
d w
alls
of
sple
nic
arte
ries
14
Hae
mor
rhag
ic
(4 x
3 x
2 cm
)
15
Nor
mal
N
orm
al
Bro
ncho
pneu
mon
ia,
myo
card
ial
infa
rctio
n an
d co
rona
ry a
ther
oma.
R
heum
atoi
d ar
thri
tis a
nd n
odul
ar c
ollo
id g
oitre
. Fi
brin
in
wal
ls o
f pu
lmon
ary
vein
s

TA
BL
E I1 (c
ontin
ued)
Mac
rosc
opic
al fi
ndin
gs in
adr
enal
s C
ase
Oth
er s
igni
fican
t fin
ding
s R
ight
Nor
mal
Left
16
Nor
mal
bu
t su
rrou
nded
by
tu
mou
r tis
sue
Ade
noca
rcin
oma
of b
ody
of p
ancr
eas,
with
met
asta
tic d
epos
its in
live
r, ab
dom
inal
lym
ph n
odes
, lu
mba
r ve
rtebr
ae a
nd p
leur
a.
Infa
rct
of
sple
en.
Acu
te u
lcer
s in
duod
enum
and
sto
mac
h
17
Con
gest
ion
Supp
urat
ive
bron
chop
neum
onia
, pe
tech
ial
haem
orrh
ages
in
lu
ngs,
st
omac
h an
d pe
lves
of
kidn
eys.
C
ellu
litis
of
legs
with
gan
gren
e of
rig
ht f
oot.
Nec
rosi
s of
pan
crea
s.
Fibr
in in
wal
ls o
f sp
leni
c, th
yroi
d an
d re
nal a
rterie
s, re
nal v
eins
and
bra
in c
apill
arie
s
Hae
mor
rhag
e
18
Nor
mal
C
hron
ic g
lom
erul
onep
hriti
s, h
orse
-sho
e sh
aped
kid
ney
and
thro
mbo
sis
of in
ferio
r ven
a ca
va a
nd re
nal
vein
s N
orm
al
19
Nor
mal
N
orm
al
Fibr
ocys
tic d
isea
se o
f pa
ncre
as w
ith c
ystic
bro
nchi
ecta
sis a
nd b
ronc
ho-
pneu
mon
ia.
Fibr
in in
glo
mer
ular
tufts
, spl
enic
arte
ries a
nd al
veol
i
20
Enla
rged
(5
~3
~5
x3
cm
with
ce
ntra
l ha
emor
rhag
e (2
.5 x
1.5
x 1
cm
)
Enla
rged
(5 x
3.5
x 3
cm
) with
ce
ntra
l ha
emor
rhag
e (
2x
15
~1
cm
)
Rap
idly
pro
gres
sive
typ
e of
glo
mer
ulon
ephr
itis.
In
farc
tion
of t
este
s.
Bro
ncho
pneu
mon
ia.
Chr
onic
pe
ricar
ditis
an
d m
yoca
rdia
l de
- ge
nera
tion.
Fi
brin
in
glom
erul
ar t
ufts
and
inte
rstit
ium
of
kidn
ey;
arte
ry i
n te
stis
, ve
in i
n ile
um,
wal
ls o
f sp
leni
c ar
terie
s, i
n sp
leni
c fo
llicl
es, v
ein
in th
yroi
d an
d al
veol
i
Gro
ssly
hae
mor
rhag
ic
Gro
ssly
hae
mor
rhag
ic
Sutu
red
perf
orat
ed c
hron
ic
duod
enal
ul
cer,
gene
ralis
ed p
erito
nitis
an
d br
onch
opne
umon
ia
21
22
Larg
e ha
emor
rhag
e Fr
actu
res
of p
elvi
s, le
ft cl
avic
le, r
ight
upp
er e
ight
ribs
and
all
left
ribs.
H
aem
orrh
ages
in
lung
s an
d la
cera
tion
of li
ver
Loca
lised
hae
mor
rhag
e
23
Mas
sive
hae
mor
rhag
e.
Adr
enal
vei
n oc
clud
ed b
y th
rom
bus
(fig
. 1)
Mas
sive
hae
mor
rhag
e
~
Cor
pul
mon
ale
and
bron
chop
neum
onia

Mac
rosc
opic
al fi
ndin
gs in
adr
enal
s C
ase
24
25
26
27
28
29
30
31
32
Rig
ht
Mas
sive
cen
tral
hae
mor
rhag
e
Hae
mor
rhag
ic
Con
gest
ion
Hae
mor
rhag
e (3
cm
dia
met
er)
Gro
ssly
hae
mor
rhag
ic
Mas
sive
hae
mor
rhag
e
Hae
mor
rhag
e
Mas
sive
hae
mor
rhag
e
Hae
mor
rhag
e
Left
Nor
mal
Hae
mor
rhag
ic
Con
gest
ion
Hae
mor
rhag
e (5
cm d
iam
eter
)
Gro
ssly
hae
mor
rhag
ic
Mas
sive
hae
mor
rhag
e
Hae
mor
rhag
e
Mas
sive
hae
mor
rhag
e.
Adr
enal
ve
in
occl
uded
by
th
rom
bus
Hae
mor
rhag
e
Oth
er s
igni
fican
t fin
ding
s
Perf
orat
ed a
nast
omot
ic u
lcer
at
site
of
gast
ro-je
juno
stom
y.
Gas
tro-
in
test
inal
hae
mor
rhag
e
Chr
onic
atr
ophi
c th
yroi
ditis
w
ith
fibro
sis.
A
cute
br
onch
itis
and
pulm
onar
y oe
dem
a.
Fibr
in in
wal
ls o
f sp
leni
c ar
terie
s
Seco
nd-d
egre
e bu
rns
invo
lvin
g 60
per
cen
t. of
sur
face
are
a of
bod
y.
Rec
ent a
nd o
ld m
yoca
rdia
l inf
arct
ion
Supp
urat
ive
bron
chop
neum
onia
an
d fo
cal
myo
card
itis.
Fi
brin
in
re
nal a
rterie
s, g
lom
erul
i and
pul
mon
ary
arte
ries
Chr
onic
pye
lone
phrit
is
Ana
plas
tic c
arci
nom
a of
sto
mac
h w
ith s
econ
dary
dep
osits
in
brai
n,
men
inge
s an
d ly
mph
nod
es.
Bro
ncho
pneu
mon
ia a
nd p
ulm
onar
y in
farc
t. C
hron
ic p
yelo
neph
ritis
. Fi
brin
in c
apill
arie
s of
brai
n, w
alls
of
arte
ries
in ly
mph
nod
e an
d sp
leen
Supp
urat
ive
bron
chop
neum
onia
and
car
cino
ma
of tr
ache
a.
Fibr
in i
n gl
omer
ular
tufts
Bro
ncho
pneu
mon
ia,
chro
nic
bron
chiti
s an
d em
phys
ema.
Fo
cal
peric
ardi
tis.
Fibr
in i
n w
alls
of p
ancr
eatic
vei
ns
Myo
card
ial
infa
rctio
n, c
oron
ary
athe
rom
a.
Chr
onic
bro
nchi
tis a
nd
emph
ysem
a

76 B. FOX
W V
A N
00 wlwl I
+ I ++ I i-+- I +
+ I 1 ++ + I -t i- ++ ++ ++ + I ++
+ I ++ ++ + + ++ ++ ++ i- I ++
+ I ++ ++ + i- ++ ++ +i + I ++
+ I ++ ++ ++ ++ __
++ __
+ I
++ + I ++
z ~
I /
!&& z z __
++
+ I
-
+
/ I
~
++
+ i- ~
++
I I
__
++ + I ++
+ ++ + -t + + ++ ++ ++ -t I ++
I I 1 I I
I
+ + __
dcl
I I + I I I I I
* &el del d+l del del d-l d-l
N d wl W p.

ADRENAL GLAND INFARCTION
++
77
W v
A N
++
A _ _ ~
I I
+i- + I
+ - I - ++
W v
A N
~
zi?
E? A
__
I I
N V
W v
A N
__
v i m m a
__
++
~
4
~
I
I I
~
I I
viln a m
I I I I I I I 1 I I / I I +
I
.- D l
~ / I
-
L. m - 2 4 U
.-
I
~
I
1 1 I I I / / I
__
I I
I I
__
++
I I- l l
+ I 1 I + .!. + ++ t ++ -1- +
P
.- M I + + ++ I ++ I + ++ __
++
++ ++ ++ ++ t +
++ ++ I + ++ ++ ++ ++ __
++
+ +
1 1 ++ i ++ I ++ t+ ++ I + ++ +
I I
-
++
I / ++ I + ++ __
If + + +
I + + + ++ ++ ++ __
++
++ i+
++ ++ ++ I + -t + ++
I I ++ I 1 I I I I
dcl d-1
2 W ,-, 1 I

78
nn m m
-
++
B. FOX
I I
-
++
++ -
+ i-
00 a m
__
I I
I /
__
++
++ __
I 1
w w v v N N A A
/ I I 1
W V
A N
W V
A N
El V
A W
W V
A N
__
nvI m m
__
I +
-
I I
__
++
W V
A N
W V
A N N
V
I
nn
__
I 1
00 m m
-
I I I I
I I
-
+ I
I I
-
++
I I
___
++
I I I /
++ ++ ++ ++ __
++ __
++
+’- I ++ ++ ++ ++ ++ ++ ++ -
++
++ ~
++ ++ ++ ++ ++ ++ ++ ++
++ 1 ++
I
++ -
+ I
__
++
++ -
+ I
~
++
++ ++ ++ -
+ I
__
++
++ ++ -
+ I
-
++
++ __
++
++ __
++ ++
++ I ++ I
++ ++ ++
++ ++ ++ ++ ++ ++ ++ ++
l + i I I I / I I I I / I
dcl
- N N
dcl
- R
dcl dd I
x 1 2 4

ADRENAL GLAND INFARCTION 79
Extensive lesions are clearly defined areas of necrosis involving the cortex which extend from the areas of haemorrhage, often to the capsular surface (fig. 2), but occasionally there is a rim of surviving zona glomerulosa or of outer zona fasciculata (fig. 3). There is usually a clear line of demarcation between the haemorrhage and the necrotic area, but occasionally they merge. When this occurs the red cells within the necrotic areas lose their staining characteristics and are usually only discernible in the inner third. In most other cases the only red cells within the necrotic areas are those in sinusoids, and these usually lose their staining characteristics. Around the areas of necrosis there is a zonal arrangement of three irregular bands : (a) of degenerate cortex; (b) of neutrophils, nuclear debris and basophilic material; and (c) an outer band of haemorrhage (fig. 4). The structure of the necrotic areas varies according to the apparent age of the lesions but is fairly uniform within one adrenal gland. The ageing of the histological changes is given within a time range of less than 2 days, greater than 2 but less than 6, greater than 6 and less than 10, and greater than 10 days.
Less than 2 days. There is coagulative necrosis with loss of cellular outline and partly vacuolated homogenous cytoplasm. The nuclei are often pale and become ghost-like and there is some pyknosis and karyorrhexis (fig. 5). In the very early lesions there is usually no neutrophil infiltration, but occasionally there are neutrophils throughout the necrotic area. In the band of degenerate cortex which is usually present on the outer side of the necrotic area there is vacuolation of the cytoplasm with occasional pyknosis of nuclei. The band of neutrophils varies from 50-250 pm thick around the edges of the necrotic areas but is absent or slight on the inner surface. When the necrotic area extends to the capsule (fig. 2) the band of neutrophils usually extends into the periadrenal connective tissue, but when there is a surviving rim of cortex the band of neutrophils is usually on the inner side of the surviving cortex. The band of neutrophils is separated from normal cortex by an irregular band of haemor- rhage (fig. 4). The reticulin pattern within the cortex is normal; there is no iron present.
Greater than 2 and less than 6 days. There is usually complete loss of normal parenchymal structure which is replaced by vacuolated eosinophilic tissue in which there are usually no surviving nuclei (fig. 6). The bands of neutrophils are marked and they contain nuclear debris and basophilic tissue (fig. 2). The older the lesion the less recognisable are the neutrophils and the denser the nuclear debris and basophilic tissue. The cytoplasm of the cells in the degenerate zone become more vacuolated and the nuclei pyknotic. There is little alteration in the haemorrhagic zone. The reticulin pattern is altered, usually to a honeycomb type (Fox, 1969), but there is also collapse of reticulin network. There are often areas of inflammatory granulation tissue in the areas of surviving cortex and pericapsular connective tissue adjacent to the necrotic areas.
Greater than 6 and less than 10 days. The cortical tissue becomes more vacuolated, the neutrophils have mainly disappeared but there is often a thick band of basophilic tissue with some nuclear debris. The cells in the degenerate

80 B. FOX
zone become more structureless, the nuclei disappear and around 10 days the degenerate zone becomes less well-defined and in areas disappears. There are areas of fibrosis on the capsular surface with bands extending into the necrotic areas and occasionally there is fibrosis around the edges of the necrotic areas. The inflammatory granulation tissue in the periadrenal fat becomes organised.
Greater than 10 days. The necrotic areas become more structureless, with occasional clefts, and there is no evidence of nuclear debris or basophilic tissue (fig. 7). Fibrous tissue is thicker on the capsular surface and may extend in thick bands into the necrotic areas. There is often a clear line of demarcation between the necrotic areas and adjacent normal cortex. There is no evidence of recent or old haemorrhage within the areas of necrosis.
(b) Focal ischaemic necrosis-These lesions are identical to those spheroidal areas of necrosis found in the outer cortex in patients with polyarteritis nodosa (Balb and Nachtnebel, 1929). They are occasionally infiltrated by neutrophils, nuclear debris and basophilic material similar to that seen in extensive ischaemic necrosis. The reticulin pattern may be normal or show similar changes to those seen in extensive ischaemic necrosis.
(iii) Other parenchymal changes In most of the cases there were varying degrees of compact cell change and
tubule formation in the surviving areas of cortex, but there is no recognisable pattern of these changes in relation to the haemorrhage or necrosis.
B. Vascular changes There is thrombosis of the extra-adrenal main vein (fig. S), intra-adrenal
muscular veins (fig. 9), emissary veins, venous sinuses and capsular veins (fig. 10). Although thrombi in the intra-adrenal veins are usually related to areas of haemorrhage and necrosis they sometimes occur in normal parts of the gland. Thrombosed capsular veins are usually near to the capsule but they do occasionally occur in vessels some distance from the gland and are occa- sionally well-organised (fig. 11). It is possible to recognise a pattern of organisation of the thrombi, mainly in the intra-adrenal veins. In the early stages, up to 2 days, the thrombi are composed of masses of platelets (fig. 12), in places forming fairly homogenous clumps with irregular bands of fibrin, and scattered groups of white and red cells (fig. 12). Some of the thrombi, particularly in the capsular veins, are composed only of fibrin and red cells. Over 2 and less than 6 days the platelets become homogenous, there is lamination of thrombi with thin and thick strands of fibrin, red and white cells. Fissures form and endothelial cells from the wall of the vessel infiltrate the thrombus, and vascular channels begin to appear (fig. 13). Over 6 and up to 10 days organisation continues ; more endothelial lined vascular channels are formed and reticulin fibres appear. There are masses of fibrin and pink homogenous tissue but very few cells are seen (fig. 8).

Fox ADRENAL GLAND INFARCTION
PLATE XVI
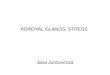
FIG. 1.-Case 23. Massive central haemorrhage in both adrenals with necrosis of the surrounding cortices.
FIG. 2.-Case 3. Extensive ischaemic necrosis extending to capsule with a band of neutrophils and nuclear debris in periadrenal connective tissue. Haemalum and eosin. x 150.

Fox
ADRENAL GLAND INFARCTION
PLATE XVII
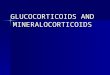
FIG. 3.-Case 5. Extensive ischaemic necrosis with a rim of surviving outer cortex. HE. x 50.
FIG. 4.-Case 3. Venous infarct with necrotic cortex surrounded by bands of neutrophils, haemorrhage and degenerate cortex. Picro-Mallory. x 70.

Fox
ADRENAL GLAND INFARCTION
PLATE XVlII
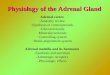
FIG. 5.-Case 22. Early coagulative necrosis with FIG. 6.-Case 4. Cortex replaced by vacuolated, mainly structureless, eosinophilic tissue. HE. loss of staining characteristics of nuclei and
cytoplasm and someloss of nuclei. HE. x 225. x 150.
FIG. 7.-Case 18. Old ischaemic necrosis in alar raphe with no evidence of cellular reaction. There is a rim of surviving outer cortex. HE. x 56.

Fox
ADRENAL GLAND INFARCTION
PLATE XIX
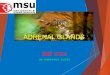
FIG. 8.-Case 4. Organised thrombus occluding extra-adrenal main vein. Picro-Mallory. X 40.
FIG. 9.-Case 22. Organised laminated thrombus with attached mass of conglomerated red cells and fibrin occluding main central adrcnal vein. HE. X 40.

Fox PLATE XX
ADRENAL GLAND INFARCTION
FIG. 10.-Case 1. Fairly well-organised thrombi in capsular veins. HE. x 48.
FIG. 11 .-Case 5. Organised adherent thrombus with early formation of new vascular channels in capsular vein. HE. x 100.

Fox PLATE XXI
ADRENAL GLAND INFARCTION
FIG. 12.-Case 32. Thrombus composed of platelets with scattered white cells, some red cells and fibrin, in extra-adrenal main vein. Picro-Mallory. x 120.
FIG. 13.-Case 5. Organised adherent thrombus with formation of new vascular channels in intra- adrenal vein. HE. x 100.

Fox
ADRENAL GLAND INFARCTION
PLATE XXII
FIG. I4.-Case 22. Fibrin thrombi in sinusoids in inner part of necrotic cortex. PTAH. x 80.
FIG. 15.-Case 23. Fibrinous vasculosis in capsular and intra-adrenal arteries. PTAH. x 110.

ADRENAL GLAND INFARCTION 81
There is often variation in the structure of the thrombi within the glands and the descriptions given are of the most organised areas. As far as can be ascertained the thrombi in the intra-adrenal muscular veins are older than those in the sinuses and occasionally the thrombi in the extra-adrenal vein are the most well organised. Though the thrombi in the venous sinuses occasionally appear to be about the same age as those in the muscular veins, in none of the cases do the thrombi in the venous sinuses appear older than those in the muscular veins. The cortical sinusoids are often lined and occluded by fibrin, mainly in the areas of haemorrhage and necrosis but occasionally in the uninvolved parts of the gland. Fibrin thrombi are sometimes particularly prominent on the inner surface of the areas of extensive ischaemic necrosis (fig. 14). Many of the capsular veins, including those containing thrombi, are lined by fibrin. The capsular and intra-adrenal arteries are not thrombosed but many of them are lined by fibrin and some have deposits of fibrin in the media (fibrinous vasculosis) (fig. 15). The muscle walls of the extra-adrenal main vein appear normal but the walls of some of the intra-adrenal veins are necrotic when they are included in the areas of infarction.
Type 2
In this group of cases the main parenchymal change is extensive ischaemic necrosis, structurally identical to that in Type 1, but haemorrhage when present is slight and usually confined to the centre of the gland. In some of these cases there is evidence of old haemorrhage with deposits of iron, mainly around the necrotic areas. The alar raphe and parts of the medulla, as well as the cortex, are necrotic. Even though the necrosis is very marked, often involving the whole gland, there are occasionally areas of surviving outer cortex
The vascular changes are identical to those in Type 1 but in case 19, in which the parenchymal changes appear to be over 10 days old, there is very marked organisation and recanalisation of the thrombus in the central adrenal vein.
(fig. 3).
Histological examination of other tissues
All the tissues available were examined histologically, particularly for the presence of thrombi and deposits of fibrin. The significant histological findings are summarised in table 11.
Clinical findings
The main findings are summarised in table I. In all cases except cases 1 and 20 the terminal hypotension and shock was thought to be due to the main diseases present. In case 1 adrenal failure and in case 20 Gram-negative bacteraemic shock were considered as possible causes for the collapse and death.
I . PATH.-VOL. 119 (1976) F

82 B. FOX
DISCUSSION In these 32 cases of adrenal haemorrhage and necrosis there were thrombi
in the intra-adrenal veins, venous sinuses, cortical sinuses, capsular veins and often the main extra-adrenal veins. Although venous thrombosis has often been regarded as the main cause of adrenal haemorrhage and necrosis (Simmonds, 1902; Hall and Hemkin, 1936; Keele and Keele, 1942; Botteri and Orell, 1964; Namiki, 1964) it has been suggested that it is secondary to the parenchymal changes (Sheehan, 1955; Thrash and Iri, 1963; Greendyke, 1965). However, the evidence in this series of cases is that venous thrombosis is the primary change. The histological findings are of infarction (fig. 4) and are similar to those found in venous infarction of the adrenals occurring during abdominal operation in which there is little doubt that venous thrombosis is primary (Fox, 1969). That adrenal vein thrombosis is primary is also suggested by the cases 2, 7, 13, 24, 25, 26 and 28, in which there is venous thrombosis with haemorrhage and necrosis in one gland and venous thrombosis without parenchymal changes in the other (Botteri and Orell). Greendyke, with the same evidence in his cases, thought that this indicated that venous thrombosis could not be the cause of adrenal changes. It is possible that Greendyke did not appreciate that adrenal thrombosis can occur without causing haemorrhage and necrosis. In most large series of cases of adrenal haemorrhage and necrosis not associated with pregnancy (Plaut, 1955; Botteri and Orell; Greendyke), adrenal venous thrombosis was nearly always present and, apart from Green- dyke and Plaut, it was thought to have been the cause of the parenchymal lesions. Greendyke suggested that adrenal venous thrombosis was probably secondary to parenchymal necrosis or haemorrhage and quoted as evidence Sevitt (1955) who found venous thrombosis in only one of 14 cases, and Berte (1953) who, in a review of 24 cases, found only seven with venous thrombosis. Sevitt’s cases were due to trauma in which adrenal haemorrhage was mainly due to direct injury to the gland. The cases reviewed by Berte were single case reports and in none of them did it appear that the adrenal glands had been thoroughly examined. It is apparent from this series that, unless blocks of the whole of the adrenal gland are examined, adrenal vein thrombosis will be missed. Venous thrombosis is often patchy, so that there are sections in which there is massive haemorrhage around apparently patent veins, whereas in other sections from the same gland the veins are thrombosed.
It has been suggested that because adrenal vein thrombosis can occur without parenchymal changes, venous thrombosis is unlikely to be the main cause of adrenal haemorrhage and necrosis (Plaut ; Greendyke; Thrash and Iri). However, in three cases of adrenal vein thrombosis, without any paren- chymal changes (Fox, 1973), the capsular veins were patent, whereas, in nearly all of the 32 cases in this paper of adrenal haemorrhage and necrosis, there is thrombosis of the capsular veins (table 111) and usually of the emissary veins. It is probable that, when adrenal vein thrombosis occurs without haemorrhage or necrosis, blood is able to leave the gland by the alternate venous supply through the emissary and capsular veins (Dobbie and Symington, 1966).

ADRENAL GLAND INFARCTION 83
It has not previously been realised that thrombosis of the capsular veins is of great significance in the production of adrenal infarction. In most descrip- tions of adrenal haemorrhage and necrosis, including reports of a large number of cases (Crawford, 1951 ; Plaut; Sheehan; Namiki; Greendyke; Bove, 1965), the capsular veins are not mentioned but, in a few (Botteri and Orell; Thrush and Iri), thrombosis of the capsular veins had been described but the significance of them missed.
Adrenal vein thrombosis was associated with fibrin thrombi in the cortical sinusoids in all the cases. It has been suggested that adrenal vein thrombosis is secondary to sinusoidal thrombosis (Simmonds; Bove; McKay, 1965, p. 440), but the evidence in this paper is mainly against this hypothesis. There is often no definite continuity between the sinusoidal thrombi and the throm- bosed central veins, particularly in cases in which there is central haemorrhage. In case 19, in which thrombosed central veins are in continuity with thrombosed sinusoids, the central vein thrombosis is well organised; thus, it seems more probable that the central vein thrombosis had resulted in sinusoidal thrombosis. If central venous thrombosis were due to propagation of thrombus from the sinusoids, one would expect the thrombi in the smaller venous sinuses to be better organised than those in the larger veins, but in these cases this was not so. It has been suggested that sinusoidal fibrin thrombosis in cases of adrenal haemorrhage in humans (Hjort and Rapaport, 1965; McKay, 1965, p. 85) and in animals (Wong, 1962; Galton, 1964; McKay, 1965, p. 260) is due to disseminated intravascular coagulation (DIC). There is convincing evidence in cases 8, 11, 13, 19,27, 30 and 31 that DIC had occurred and may have been the cause of the fibrin thrombi in the sinusoids. It is significant that in these cases there were thrombi in the normal cortex as well as in the areas of haemor- rhage and necrosis. It is possible that adrenal sinusoids may be directly damaged by exotoxins or endotoxins which are known to cause injury to endothelium (McGrath and Stewart, 1969). Another possible mechanism is that stasis with anoxia occurs in the sinusoids, resulting in damage to the wall with subsequent thrombosis.
There were no thrombi in the capsular arteries in any of the 32 cases, but in 12 (table 11) there was marked fibrinous vasculosis and occasional deposits of fibrin on the endothelial surface of the capsular arteries and occasionally in the intra-adrenal arteries (fig. 15). Fibrinous vasculosis has previously been described in only five cases (Falconer, 1953; Botteri and Orell), but in view of the high incidence in this series it would appear that it has frequently been missed. It is probable that fibrinous vasculosis in these cases is due to local hypoxia which may have occurred as a result of adrenal venous infarction. It is possible that in two of the cases DIC caused damage of the vessel wall with subsequent deposition of fibrin.
In these cases of venous infarction there are two main types of necrosis- focal and extensive. The changes in focal necrosis are identical to those found when capsular arteries are occluded (Ba16 and Nachtnebel, 1929; Namiki). However, in extensive necrosis it is unlikely that the lesions could be due to blockage of capsular arteries. When a large number of capsular arteries are

84 B. FOX
damaged the areas of necrosis are cylindrical in shape, they involve the outer part of the cortex and extend to the capsule and there is usually no rim of surviving outer cortex (Fox, 1973). In extensive necrosis there is usually a band of surviving outer cortex, even where the area of necrosis is very large (fig. 3), which suggests that these necrotic areas are not due to damage to capsular arteries. It is probable that extensive necrosis is due to blockage of cortical sinusoids primarily on the inner surface of the area of necrosis, usually adjacent to the area of haemorrhage.
One of the puzzling features of adrenal infarction are those cases in Type 2 in which the parenchymal lesions are principally those of ischaemic necrosis with only minimal haemorrhage. There are no apparent differences in the vascular changes between the cases in Types 1 and 2, and no obvious differences in the age of the lesions. In cases 14, 24 and 26 the changes in one gland are those seen in Type 1 and in the other gland are those of Type 2, which does suggest that venous thrombosis is the cause of both parenchymal changes. It is possible that necrosis is due solely to blockage of sinusoids secondary to adrenal vein thrombosis, but it is difficult to see why haemorrhage is so slight. Case 18 is important because there can be little doubt that adrenal vein thrombosis was secondary to thrombosis of the inferior vena cava and of the left renal vein. In this case adrenal vein thrombosis has produced large areas of ischaemic necrosis, mainly with a rim of surviving outer cortex (fig. 8), and although there is evidence of old haemorrhage it is mainly around the edges of the necrotic areas. It is of interest that in this case the external capsular veins were patent: thus, although the blood could not drain into the adrenal veins, it presumably could drain into the inferior phrenic, diaphragmatic and perirenal fat veins. Another possible explanation is that adrenal vein thrombosis can cause spasm of capsular arteries which results in cortical necrosis without haemorrhage (Thrash and Iri). However, there is no experimental or other evidence available to suggest that such a mechanism does occur.
Although DIC had been thought to be the cause of adrenal haemorrhage and necrosis, particularly in cases occurring in pregnancy (McKay et al., 1953; Bohle and Krecker, 1959), the role that it plays in cases of venous infarction has not previously been carefully assessed, although McKay (1965, p. 422) thought that DIC was probably the cause of adrenal haemorrhage in " sponta- neous '' adrenal haemorrhage. The main clinical criteria used to assess whether DIC may have been present in this series was hypotension, shock or cyanosis when there was no obvious respiratory or circulatory cause to explain the cyanosis. The main pathological evidence is the presence of fibrin thrombi in the microcirculation, particularly in the renal glomeruli and the adrenal glands ; fibrinous vasculosis in arteries, and scattered foci of necrosis (tables I1 and 111). Although fibrin thrombi in adrenal sinusoids are seen in cases of focal necrosis (Fox, 1973) and in cases associated with abdominal operations (Fox, 1969), the presence of such thrombi in areas of apparently normal cortex was used as evidence in favour of DIC. In cases 11, 17,19,29 and 30 there is unequivocal evidence that DIC has occurred; in cases 1, 4, 8, 13 and 31 it is probable, and in cases 2, 9, 12 and 14 it is possible that DIC occurred.

ADRENAL GLAND INFARCTION 85
In cases 19 and 30, with definite DIC, and all of the cases which probably had DIC, there was severe bacterial infection and, although in case 4 only was there evidence of bacteraemia, it is probable that bacterial endotoxins which are known to cause DIC experimentally (Hjort and Rapaport) and in humans (McGehee, Rapaport and Hjort, 1967; Goldenfarb et al., 1970) were the cause of DIC. Hypoxia may have played a part in causing DIC in cases with severe, acute and chronic respiratory diseases (Garvey et al., 1969). Cases 11 and 29 with definite DIC were patients with mucin-secreting gastric carcinomas in which DIC is well recognised (Dumont et al., 1965; Boulard et al., 1971).
Hypothermia was present in three of the cases with definite DIC, an association which has not previously been reported in humans, although it has been described in dogs (Johansson and Nilsson, 1964).
Although there is a good deal of evidence that DIC is responsible for focal cortical haemorrhage and necrosis, particularly in cases associated with pregnancy (McKay et al., Hjort and Rapaport), it is probable that it is coinci- dental in cases of venous infarction, but it could play a part in inducing adrenal vein thrombosis.
Apart from the cases of venous infarction in which adrenal thrombosis is due to metastatic carcinoma there is no obvious explanation for adrenal vein thrombosis. It is apparent that the pathogenesis of venous infarction will only be clarified further if an explanation is found for venous thrombosis. In these cases there is the unusual situation in which thrombi are virtually restricted to the adrenal veins. The main adrenal vein is anatomically and physiologically different from any other vein in the body. It has thick bundles of muscle fibres which are arranged along the long axis of the vessel (Dobbie and Symington) and the concentration of adrenocortical and medullary hormones is greater than in any other vein. It is possible that the localisation of thrombi to the adrenal vein is mainly due to these two separate factors. The striking feature of the structure of the thrombi in the main adrenal vein, particularly in the early stages of development, is the large number of platelets (fig. 12) and later the large amount of fibrin (fig. 9). This suggests the possibility that platelets play an important role in the early stages of adrenal vein thrombosis. Recently, the steps involved in the production of platelet thrombus and the role of platelets in haemostasis and thrombosis have been clarified (Holmsen, 1972).
There are many substances which are able to induce platelet thrombosis; the ones which may be of particular significance in adrenal vein thrombosis are adrenaline and noradrenaline (Mitchell and Sharp, 1964; O'Brien, 1964), thrombin (Grette, 1962) and endotoxin (Des Prez, Horowitz and Hook, 1961). Another factor whi'ch may be of importance in these cases, particularly those with DIC, is the formation of fibrin which also plays a vital role in platelet aggregation (Born, 1965; Niewiarowski, Ream and Thomas, 1970).
It is important to establish why the thrombi are localised in the adrenal veins. In most cases there is no microscopic evidence that the walls of the veins are damaged, so that other factors must be involved. Two factors to be considered are turbulence of blood flow, and stasis, both of which may cause

86 B. FOX
platelet thrombosis (Wells, 1969) even without apparent damage to the vessel wall (Thomas, 1972). Stasis probably occurs in the adrenal vein when it contracts and prevents blood entering the venous sinuses as the result of stimulation by catecholamines (Miller and Lewis, 1969). Turbulent flow may occur if there are irregularities in the vessel wall or sudden changes in the direction of blood flow. When the muscle fibres of adrenal vein contract they increase in girth (Dobbie and Symington), which could result in sufficient irregularity of the lumen to cause turbulence. Another possible site of turbu- lence is the junction of muscular adrenal veins which often occur at an acute angle (Dobbie and Symington).
Once the platelet nidus has been formed and it has become stabilised by fibrin there will be successive layering of aggregated platelets and fibrin with inclusion of red and white cells and the formation of a laminated thrombus. When the blood flow through the main adrenal vein has been reduced blood will leave the gland by the alternative venous circulation, which in turn will become involved in the thrombotic process.
The most common condition associated with venous infarction was bronchopneumonia which was present in 21 cases and in eight of these there was also chronic respiratory disease. There have been only occasional reports of adrenal haemorrhage associated with chronic respiratory diseases (Maclean and Ironside, 1958; Bove), but this is probably not a true reflection of the incidence of this association. Adrenal haemorrhage and necrosis are often missed at post-mortem examination; in six cases in this series the adrenal glands at necropsy appeared normal and there are many cases which are not published (Dr R. A. B. Drury, 1969, personal communication; Dr M. 0. Skelton, 1969, personal communication). Adrenal haemorrhage and necrosis has previously been reported in only two patients with hypothermia (Le Marquand, Hausmann and Hemsted, 1953; Dent, Stokes and Carpenter, 1961) but it is probable that cases are missed and there are also cases which have not been published (Professor Dorothy S. Russell, 1964, personal communica- tion).
The clinical diagnosis of adrenal infarction is difficult but it should be suspected in any patient with severe infections, particularly in patients with bronchopneumonia and chronic respiratory disease, and in cases of hypothermia. The sudden onset of upper abdominal pain, particularly associated with hypotension, is strongly suggestive of adrenal infarction (Keele and Keele). The estimation of serum electrolytes will probably not be of value, but the estimation of plasma cortisol can be useful. If there is complete block of adrenal veins, with infarction of the gland, one would expect the level of cortisol to be very low.
SUMMARY
An investigation of 78 cases of adrenal haemorrhage and necrosis disclosed that 32 were examples of adrenal venous infarction. In all these cases there was thrombosis of the main adrenal vein and in most there was also thrombosis of the capsular veins, a finding which has not been well established. In a number

ADRENAL GLAND INFARCTION 87
of cases with venous infarction there was clinical and pathological evidence that disseminated intravascular coagulation (DIC) had occurred, but it appears that it was not the direct cause of venous thrombosis. The majority of cases of venous infarction occur in patients with severe infection, frequently of the respiratory tract. Venous infarction was found in five cases with hypothermia an association which had rarely been described, and in three of these there was evidence of DIC. This is apparently the first occasion on which DIC has been demonstrated in cases of hypothermia in man. The cause of venous thrombosis in the adrenal glands is obscure in most cases of venous infarction, although in three it was due to involvement by metastatic carcinoma. It is suggested that the factors responsible for the initiation of thrombosis in the adrenal veins are catecholamines, thrombin, fibrin and endotoxin. Localisation of the thrombi to the adrenal vein is due to the unique anatomical structure of the vein which, under certain circumstances, results in the local stasis of blood.
I wish to thank Mr F. D. Humberstone, Miss P. Naidoo and Mr C. Pancham for technical assistance, Mr R. Barnett for the photomicrographs and Dr D. A. L. Bowen, of the Depart- ment of Forensic Medicine, who supplied some of the cases. I am also grateful to the many clinicians who allowed me access to their records.
REFERENCES B A L ~ , J., AND NACHTNEBEL, 0. 1929. Periarteritis nodosa and internal secretions. Orv.
He‘til., 73, 33. BERTE, S. J. 1953. Spontaneous adrenal haemorrhage in the adult: literature review and
report of two cases. Ann. intern. Med., 38, 28. BOHLE, A., AND KRECKER, H. J. 1959. Uber des Sanarelli-Shwartzman Phenomenon
(S.G.O. Generalisierte Shwartzman-Phenomenon) des Menschen. Klin. Wschr., 37, 803. BORN, G. V. R. 1965. Platelets in thrombogenesis: mechanism and inhibition of platelet
aggregation. Ann. Roy. Coll. Surg., 36, 200. BOTTERI, A., AND ORELL, S. R. 1964. Adrenal haemorrhage and necrosis in the adult. A
clinicopathological study of 23 cases. Acta med. scand, 175, 409. BOULARD, CI., FABRE, J., BIERME, R., PRIS, J., GOLDBERGER, E., AND BELSOL, G. 1971.
Anemie hemolytique micro-angiopathique et coagulation intravasculaire disseminee au cours des cancers metastatiques. Presse rned., 79, 1347.
BOVE, K. E. 1965. Thrombosis of the medullary adrenal vein. Arch. Path., 80, 418. CARSTAIRS, K. C. 1965. The identification of platelets and platelet antigens in histological
sections. J. Path. Bact., 90, 225. CRAWFORD, MARGARET D. 1951. Suprarenal haemorrhage and necrosis in pregnancy. J.
Path. Bact., 63, 365. DENT, C. E., STOKES, J. F., AND CARPENTER, M. E. 1961. Death from hypothermia in
steatorrhoea. Lancet, 1, 748. DES PREZ, R. M., HOROWITZ, H. I., AND HOOK, E. W. 1961. Effects of bacterial endotoxin
on rabbit platelets. J. exp. Med., 114, 857. DOBBIE, J. W., AND SYMINGTON, T. 1966. The human adrenal gland with special reference
to the vasculature. J. Endocr., 34, 479. DUMONT, J., BOIRON, M., LEDUC, D., FRESSINAUD, L., AND BERNARD, J. 1965. Association
d’une anemic hemolytique et d’un purpura thrombopenique a un cancer de l’estomac. Presse med., 73, 877.
FALCONER, C. D. 1953. Adrenal apoplexy: case of unilateral haemorrhage simulating tumour of kidney. Brit. J. Urol., 25, 183.

88 B. FOX
Fox, B. 1969. Unilateral adrenal necrosis and haemorrhage following operations on the stomach. J. Path. Bact., 97, 127
Fox, B. 1973. The pathogenesis of adrenal haemorrhage and necrosis in man; a clinico- pathological study. M.D. Thesis, Univ. London.
GALTON, M. 1964. Studies of the generalised Shwartzman reaction in the pregnant golden hamster. Amer. J . Path., 44, 613.
GARVEY, M. B., DENNIS, L. H., HILDEBRANDT, P. K., AND CONRAD, M. E. 1969. Hypobaric erythraemia; pathology and coagulation studies. Brit. J. Haemat., 17, 275.
GOLDENFARB, P. B., ZUCKER, S., CORRIGAN, J. J., JR., AND CATHEY, M. H. 1970. The coagu- lation mechanism in acute bacterial infection. Brit. J. Haemat., 18, 643.
GREENDYKE, R. M. 1965. Adrenal haemorrhage. Amer. J. Clin. Path., 43, 210. GRETTE, K. 1962. Studies on the mechanism of thrombin catalyzed hemostatic reactions in
blood platelets. Acta Phyisol. scand., Suppl. 195, 1. HALL, E. M., AND HEMKEN, LOUISA. 1936. The adrenal glands. A clinical and pathologic
study. Archs. intern. Med., 58, 448. HJORT, P. F., AND RAPAPORT, S. I. 1965. Shwartzman reaction: pathogenetic mechanisms
and clinical manifestations. Ann. Rev. Med., 16, 135. HOLMSEN, H. 1972. The platelet, its membrane, physiology and biochemistry. Clins.
Haematol., 1, 235. JAMES, K. R. 1967. A simple silver method for the demonstration of reticulin fibres. J.
Med. Lab. Technol., 24,49. JOHANSSON, B. W., AND NILSSON, I. M. 1964. The effects of heparin and epsilon amino-
caproic acid on the coagulation in hypothemic dogs. Acta physiol. scand, 60, 267. KEELE, DORIS V., AND KEELE, K. D. 1942. Syndrome of haemorrhagic suprarenal infarction.
Brit. med. J., 2, 687. LE MARQUAND, H. S., HEUSMANN, W., AND HEMSTED, H. E. 1953. Myxoedema as a cause of
death; report of two cases. Brit. rned. J., 1, 704. LENDRUM, A. C., FRASER, D. S., SLIDDERS, W., AND HENDERSON, R. 1962. Studies on the
character and staining of fibrin. J. Clin. Path., 15, 401. MCGEHEE, W. G., RAPAPORT, S. I., AND HJORT, P. F. 1967. Intravascular coagulation in
fulminant meningococcemia. Ann. intern. Med., 67, 250. MCGRATH, J. M., AND STEWART, G. J. 1969. The effects of endotoxin on vascular endo-
thelium. J. exp. Med., 129, 833. MCKAY, D. G. 1965. Disseminated intravascular coagulation; an intermediary mechan-
ism of diseases. New York. MCKAY, D. G., MERRILL, S. J., WEINER, A. E., HERTIG, A. T., AND REID, D. E. 1953. The
pathologic anatomy of eclampsia, bilateral renal cortical necrosis, pituitary necrosis and other acute fatal complications of pregnancy, and its possible relationship to the gen- eralised Shwartzman phenomenon. Amer. J. Obstet. Gynec., 66, 507.
MACLEAN, N., AND IRONSIDE, J. J. 1958. Adrenal apoplexy. Brit. med. J., 1, 1162. MILLER, J. W., AND LEWIS, J. E. 1969. Drugs affecting smooth muscle. Ann. Rev. Pharmacol.
MITCHELL, J. R., AND SHARP, A. A. 1964. Platelet clumping in vitro. Brit. J. Haemat., 10,
NAMIKI, H. 1964. Vascular lesions of the adrenal gland. Actapath. jap., 14, 435. NEWISROWSKI, S., REAM, V. J., AND THOMAS, D. P. 1970. Effect of fibrinogen derivatives on
O'BRIEN, J. R. 1964. A comparison of platelet aggregation produced by seven compounds
PLAUT, A. 1955. Adrenal necrosis and thrombosis in routine necropsies. Amer. J. Path., 31,
SEVITT, S . 1955. Post-traumatic adrenal apoplexy. J. din. Path., 8, 185. SHEEHAN, H. L. 1955. Infarctus hemorragique du cortex surrenal dans le grossesse. Ann.
SIMMONDS, M. 1902. Nebennierenblutungen. Virchows Arch. path. Anat., 170, 242.
9, 147.
78
platelet aggregation. Thrombos. Diathes. Haemorrh. (Stuttg.), Suppl. 42, 49.
and a comparison of their inhibitors. J . Clin. Path., 17, 275.
93.
Endocr. (Paris), 16, 687.

ADRENAL GLAND INFARCTION 89
THOMAS, D. P. 1972. The platelet contribution to arterial and venous thrombosis. Clins.
THRASH, AGATHA M., AND IRI, H. 1963. Adrenal infarction. Archs. Path., 75, 538. WELLS, R. E. 1969. Rheologic aspects of stasis in thrombus formation. In Thrombosis, ed.
WONG, T-C. 1962. A study on the generalised Shwartzman reaction in pregnant rats in-
Haematol., 1, 267.
Sherry et al., Washington D.C., p. 469.
duced by bacterial endotoxin. Amer. J. Obstet. Gynec., 84, 786.