Embed Size (px)
Citation preview

Ventilator-Ventilator-Associated Associated PneumoniaPneumonia

IntroductionDefinition
48 hours after intubation mechanically ventilatedNo clinical evidence of pneumonia prior to intubation
Time of onset of pneumonia is importantspecific pathogens and outcomes
Early-onset VAP (<4 days) better prognosis, antibioticsensitive
Late-onset VAP (5 days or more) MDR pathogensincreased patient mortality and morbidity.
ATS/IDSA Guidelines: Guidelines for the management of adults with VAP

Pathogenic mechanisms

Diagnosis and Epidemiology DifficultBased on clinical indicators such as new or persistent infiltrates and purulent sputum Invasive bronchoscopic quantitative methods ( brush and bronchoalveolar lavage) : more precisely
invasive, expensive, and may be less useful in patients with antibiotics quantitative cultures are not available in all hospitals.

ATS/IDSA Guidelines: Guidelines for the management of adults with VAP
Evidence-based guidelineEarly, appropriate antibiotics in adequate dosesAvoiding excessive antibioticsBased on microbiologic cultures, clinical response, shortening the duration to the minimum effective period.

Major epidemiologic points
Polymicrobial; especially in ARDS (Level I) Aerobic
G(-) bacilli (P. aeruginosa, K. P, and Acinetobacter species) G(+) cocci (S. aureus, much of which is MRSA)
Anaerobes are an uncommon cause (Level II) Nosocomial virus and fungus are uncommon in immunocompetent patients. (Level I) MDR pathogens:
severe, chronic underlying disease, late-onsetvaries by patient population, and type of ICU (Level II)
ATS/IDSA Guidelines: Guidelines for the management of adults with VAP

Risk factors for VAPDuration of mechanical ventilationAspiration of gastric contentsCOPDUse of PEEPReintubationDuration of hosptalizationSupine head positioning
(head of bed not elevated)Fall or winter seasonNasal intubation or sinusitis

Modifiable Risk Factors and Recommendation
Intubation and mechanical ventilation
Aspiration, body position and enteral feeding
ATS/IDSA Guidelines: Guidelines for the management of adults with VAP

Modifiable Risk Factors and Recommendation
Modulation of colonization: oral antiseptics and antibiotics
Stress bleeding prophylaxis, transfusion and glucose control

Recommendations for the clinical strategy. Tracheal aspirate Gram stain can be direct initial therapy A negative tracheal aspirate has a strong value (94 %) progressive radiographic infiltrate + 2~3 clinical features represent the most accurate clinical criteria.Re-evaluation of using antibiotics based on the results of semi-quantitative, by Day 3 or sooner (Level II)
ATS/IDSA Guidelines: Guidelines for the management of adults with VAP

Recommendations for initial antibiotic therapy
Select an initial empiric therapy based on risk factors for MDR Local microbiology, cost, availability, and formulary restrictionsFor patients who have recently received an antibiotic→ a different antibiotic class
ATS/IDSA Guidelines: Guidelines for the management of adults with VAP

Initial antibiotic therapy MDR risk factor

Initial antibiotic therapy

Recommendations Recommendations for optimal antibiotic for optimal antibiotic therapytherapy
Aerosolized antibiotics: not been proven (Level I)
MDR with poor response : as adjunctive therapy (Level III)
Combination therapy at initialThough no data compared with monotherapyaminoglycoside regimen, stopped after 5-7 days (Level III)
If appropriate antibiotic, shorten the duration of therapy as 7 days (not P. aeruginosa !) (Level I).

Recommendations for selected MDR pathogens Combination therapy is recommended.
Resistance ↑on monotherapy Appropriate and effective (Level II)
Acinetobacter: carbapenems, sulbactam, colistin, polymyxin. ESBL+ Enterobacteriaceae: monotherapy of carbapenems (Level II)Adjunctive therapy ( inhaled aminoglycoside or polymyxin) for MDR G(-) (Level III) Linezolid is an alternative to vancomycin
MRSA, renal insufficiency, nephrotoxic agents (Level III).

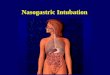
Ventilator Circuit ChangVentilator Circuit Change and VAPe and VAP
UpToDate November 16, 2005

Ventilator circuit change Most important routes of bacterial invasion
aspiration of oropharyngeal secretions inhalation of aerosols containing bacteria
Common colonization of circuits with large numbers of microorganisms. Circuits were changed daily? 2~3 days?
not a benign procedure, particularly for critically ill patients. Cost and time !!

Summary of Studies Interval Number Results Referenc
e
8 hrs/24hrs 213/271 1.5 % in both groups Am Rev Respir Dis 1978; 118:
493
24 hrs/48 hrs
44/51 No difference N Engl J Med 1982;306:150
5
24 hrs/48 hrs
106/127 29 % / 14% Am Rev Respir Dis 1991:143:
738
48 hrs/no change
35/28 No significant difference
Am Rev Respir Dis
1995;82:903
48 hrs/7 days
1708/1715
No significant difference
Anesthesiology
1995:82:903
7 days/no routine change
147/153 No significant difference
Ann Intern Med
1995:123:168
7 days/14 days
31/48 0.195/0163 Respir Care 1996;41:601

RecommendationsRecommend that ventilator circuits can be changed at weeklyLess frequent intervals without increasing the risk of VAP Required if gross soiling with blood or vomitus occursThe impact upon VAP is presently unclear for issues
heated versus unheated circuitsartificial noses versus heated humidifiers.

SummerySummery

Summery
MDR pathogensA lower respiratory tract culture needs to be collectedNegative cultures: stop antibiotic therapy An empiric therapy regimen should include agents that are from a different antibiotic class than the patient has recently received.

Summery
Combination therapy and short-duration (5 days) P. aeruginosa: aminoglycoside + ß-lactam Linezolid is an alternative to vancomycin, for proven MRSA. Aerosolized antibiotics to MDR pathogens. Ventilator circuits changed at weekly

ReferencesATS/IDSA Guidelines: Guidelines for the management of adults with HAP, VAP, and HCAP American Thoracic Society, Am J Respir Crit Care Med 2005; 171:388. Ventilator circuit change and ventilator-associated pneumonia UpToDate November 16, 2005

Thanks for attention!Thanks for attention!