Embed Size (px)
Citation preview
Ventilator Waveforms &
Loops: A Beginners
Approach
DAVID WATERS RN, MA, PGDIP ED, BA(HONS)
MARCIA BIXBY RN, MS, CCRN, APRN-BC
Welcome
Class code: C60M393
Contact hours: 1.00
CERP A credits: 1.00
Faculty Disclosures: None
Learning Outcomes
1. Evaluate the role of waveforms and loops associated with ventilation and respiratory failure of the critically ill patient.
2. Outline the components and their clinical significance of normal and abnormal waveforms and loops.
3. List patient care considerations and safety issues associated with monitoring ventilator waveforms and loops.
David Waters
Oxford,
United Kingdom

Marcia Bixby
Case Study – in the Beginning
Alison
38 yo female with history of asthma since
childhood
Presents to the ED with status asthmaticus
Ralph
• 56 yo with history of hypertension and DM
• Smoked 1PPD – 40 years
• Construction worker
• Traumatic fall - 20 feet off of a scaffolding
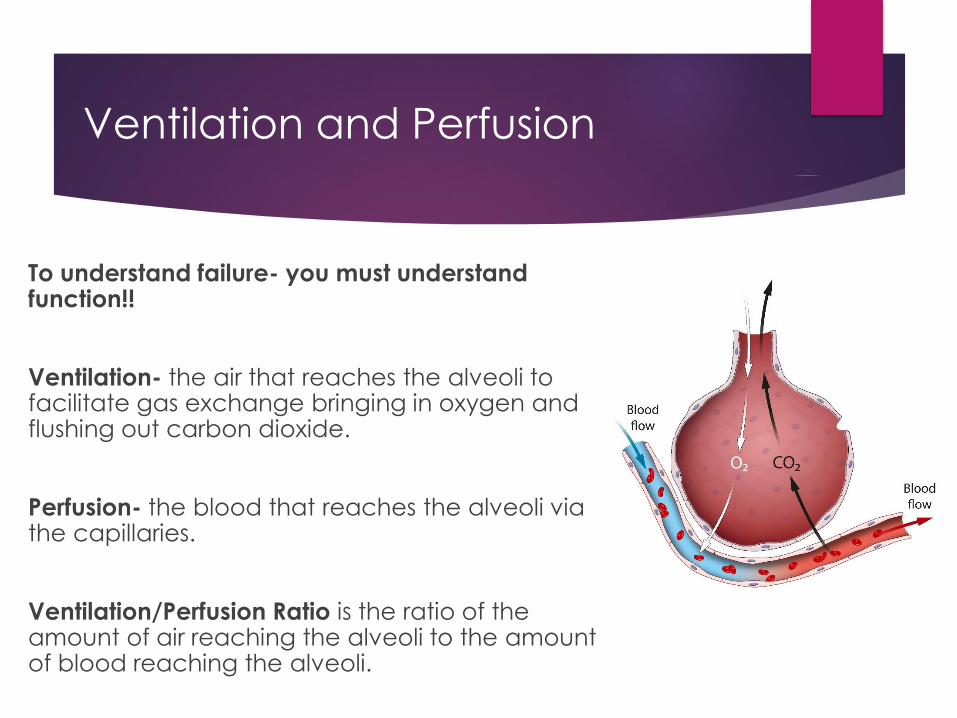
Ventilation and Perfusion
To understand failure- you must understand function!!
Ventilation- the air that reaches the alveoli to facilitate gas exchange bringing in oxygen and flushing out carbon dioxide.
Perfusion- the blood that reaches the alveoli via the capillaries.
Ventilation/Perfusion Ratio is the ratio of the amount of air reaching the alveoli to the amount of blood reaching the alveoli.
Capillary Membrane
Permeability
Increased interstitial volume > increased pressure Lungs – NCPE > ITP
Bowel – bowel edema – > IAP
Brain – cerebral edema - > ICP
Extremities – compartment syndrome
Identify and relieve cause of increased pressure
Restoration of perfusion
Restoration of oxygenation
Allow for restoration of organ function

Compliance and Resistance
Lung Compliance- measure of the lung’s ability
to stretch and expand.
Low Compliance- high elastic recoil-stiff lung
High Compliance- low elastic recoil-pliable lung
Lung Resistance- the resistance of the
respiratory tract to airflow during inspiration and
expiration
Respiratory Failure
Hypoventilation – narcotics, muscular
Airway obstruction/Asthma - RESISTANCE
ARDS/Pneumonia - COMPLIANCE
Pulmonary Embolus
Neuro injury
Burns – Inhalation
Aspiration
Chest/pulmonary trauma
Congestive Heart Failure
Diagnosis – Respiratory Failure
Vitals – tachycardia, tachypnea, dyspnea
Confusion and extreme tiredness
Perfusion deficits
Sats dropping
ABG – hypercarbia , hypoxia despite increase O2 delivery
mixed resp/-metabolic acidosis uncompensated
CXR - CT scan
COMPLIANCE (elasticity) reduced-stiff lung
Case Study - continued
How do you anticipate your assessment of Alison and Ralph to look like?
Vital signs
HR- normal or tachy?
RR – normal or increased?
BP – normal, hypo or hyper?
ABG
PaO2
PaCO2
Mental status
Case Study continued
Because this is a ventilation session – you know Alison and Ralph
will be intubated and mechanically ventilated. HOWEVER:
Alison – unresponsive to nebs and steroids in the ED
What is your threshold for intubation
Why would you intubate her
What mode and pressures do you anticipate to start
Ralph – pneumothorax, fx right ribs, head injury, fx femur
What is your threshold for intubation
Why would you intubate him
What mode and pressures do you anticipate to start
Modes of Ventilation
Basic Concepts
Respiratory rate
Tidal Volume
Oxygen level
PEEP
Minute ventilation – adjust rate and tidal volume
to maintain steady minute ventilation
If lung volume decreases – rate must increase,
PEEP adjusted for compliance/resistance
BiPAP – CPAP - NiPPV
Used as therapy to increase alveolar recruitment
Can be adjusted to patients response
May prevent intubation
Face mask or nasal mask
Uncomfortable
Monitor for aspiration
BiPAP - Bilevel Positive Airway Pressure
CPAP - Continuous Positive Airway Pressure
NiPPV - NonInvasive Positive Airway Pressure
Modes of Ventilation
Non-Invasive :
BiPAP, CPAP, NiPPV
Invasive:
Spontaneous – Assisted – Controlled
Volume - Volume or Pressure
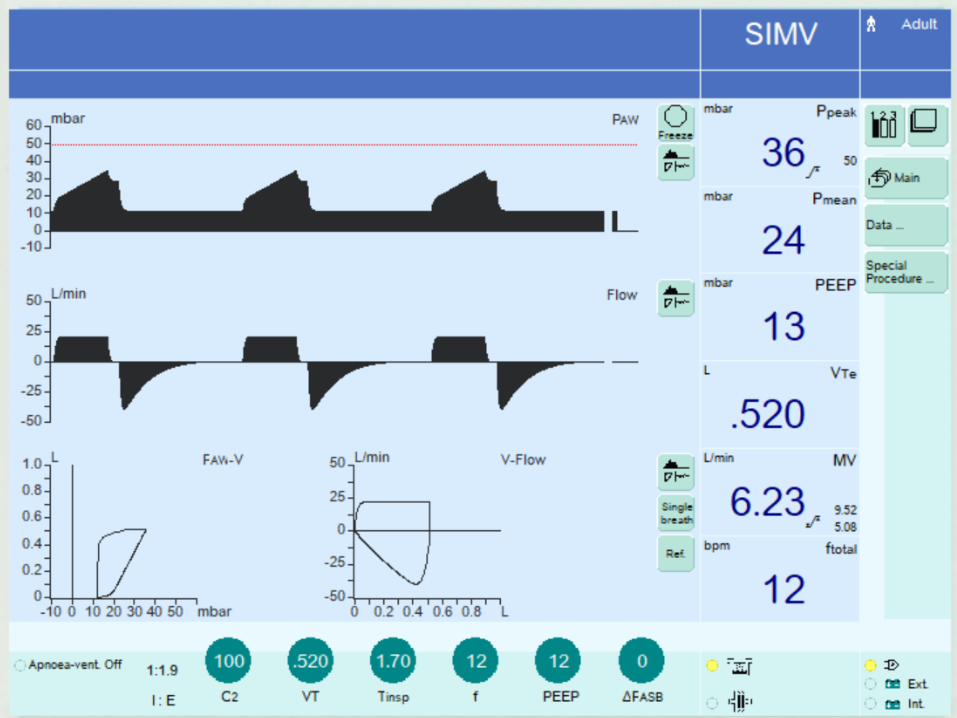
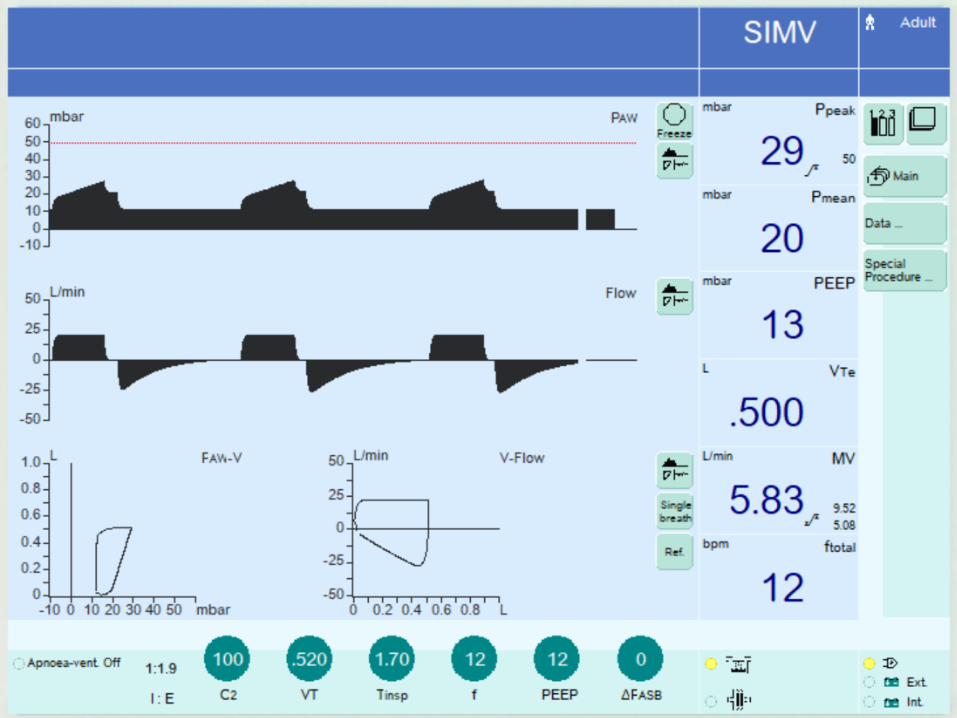
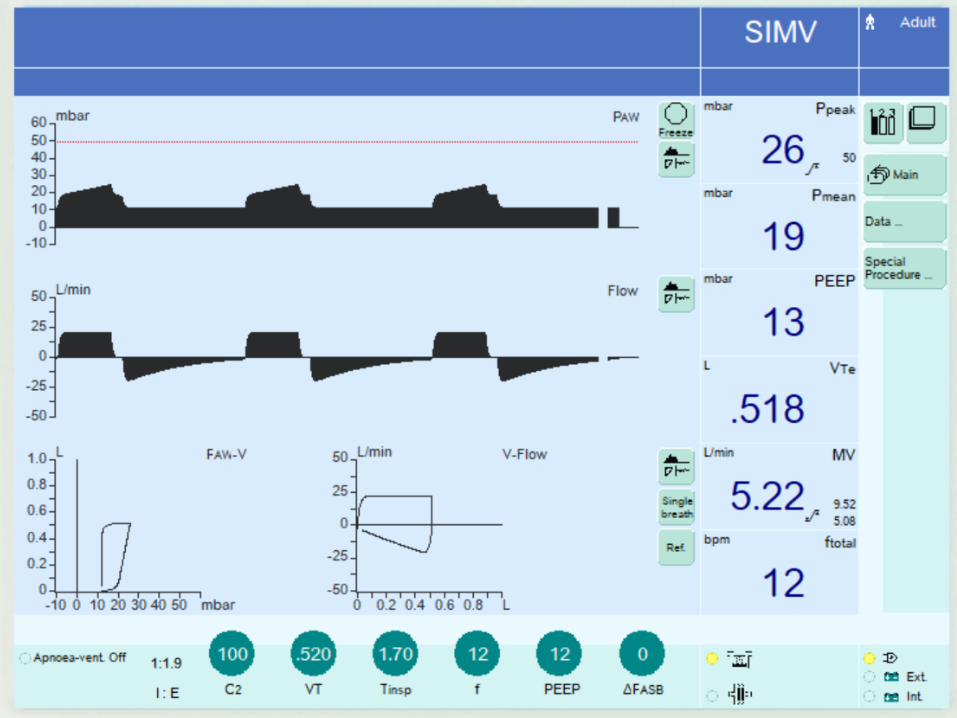
SIMV Assist Control
Pressure Control Pressure Support
APRV HFOV
PEEP and PRESSURE Ventilation
Helps to keep alveoli open
Prevents alveolar collapse on expiration
Higher levels of PEEP increase ITP
Can interfere with cardiac output
Prevents preload
Increases afterload
Monitor hemodynamic response to PEEP
Esophageal pressure monitoring
MONITOR WAVEFORMS
Critical Care Ventilation Detective
Signifies top clues in
ventilation graphic
interpretation
Scalars & Loops – the Basics
Graphical representations of data collated by the
mechanical ventilator
Can be divided into 2 categories
Those measuring 1 parameter over time – scalar, or waveform
Pressure
Flow
Volume
Those measuring 2 parameters over time – loop
Pressure-Volume
Flow-Volume
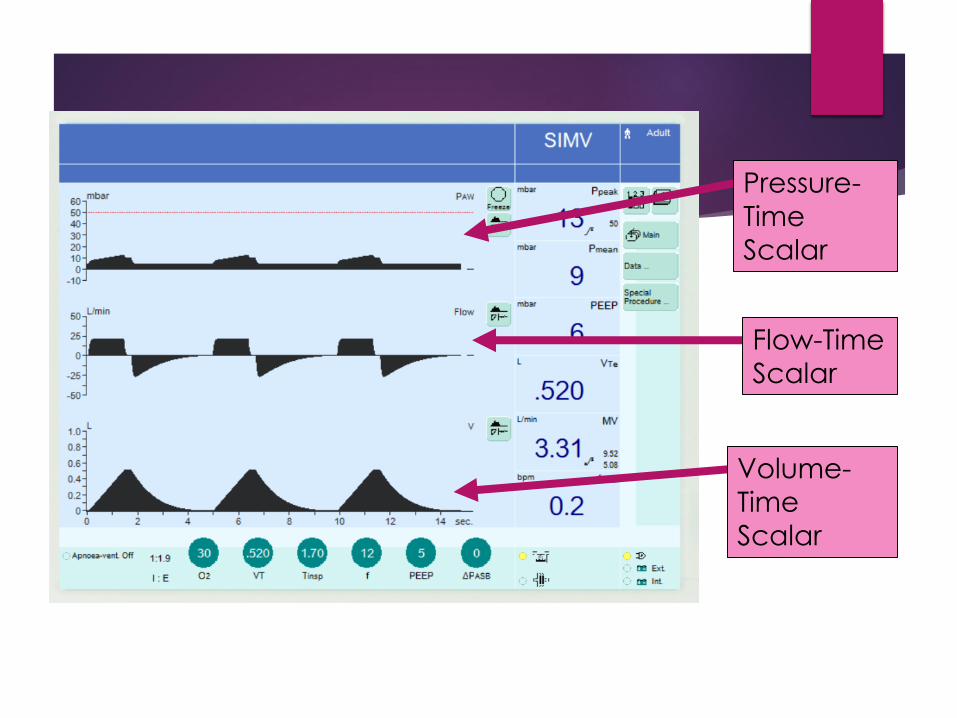
Pressure-
Time
Scalar
Flow-Time
Scalar
Volume-
Time
Scalar
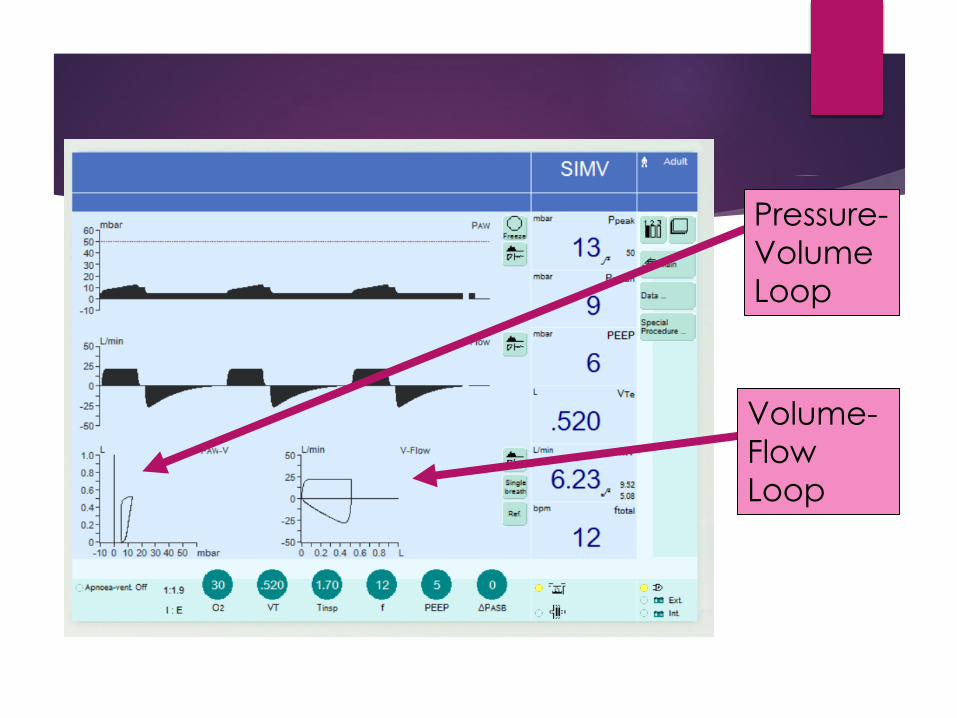
Pressure-
Volume
Loop
Volume-
Flow
Loop
Scalar:
Pressure-
Time
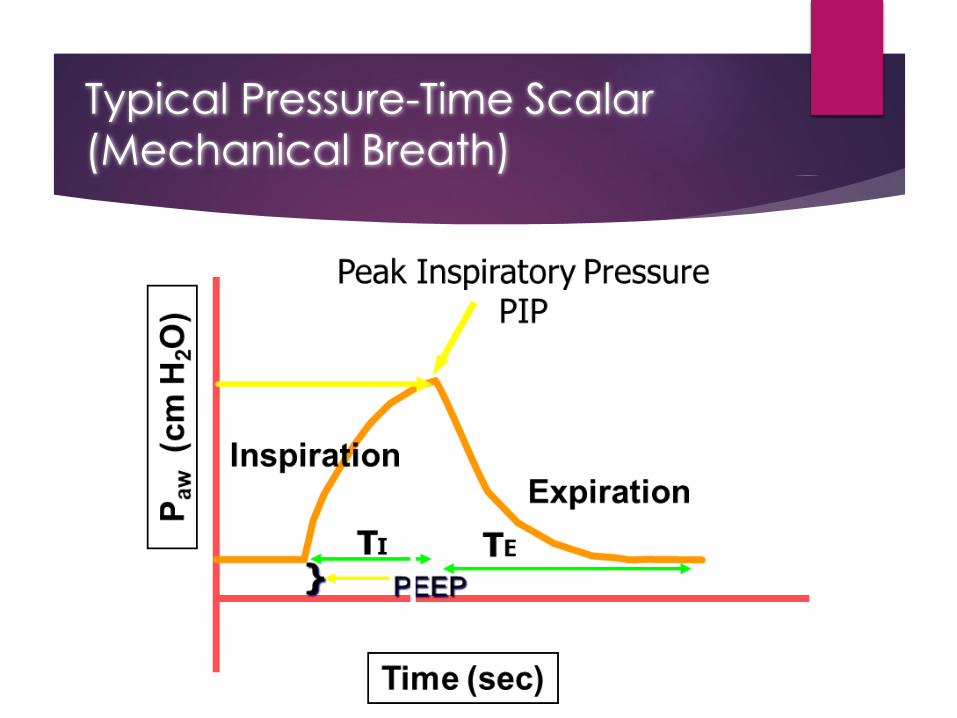
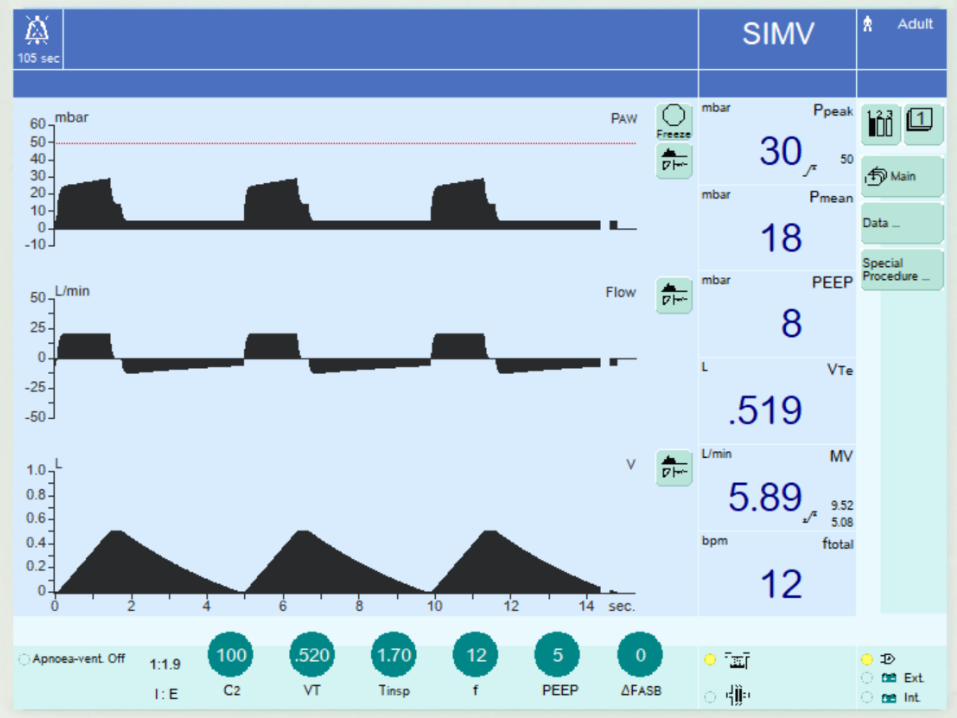
Typical Pressure-Time Scalar
(Mechanical Breath)
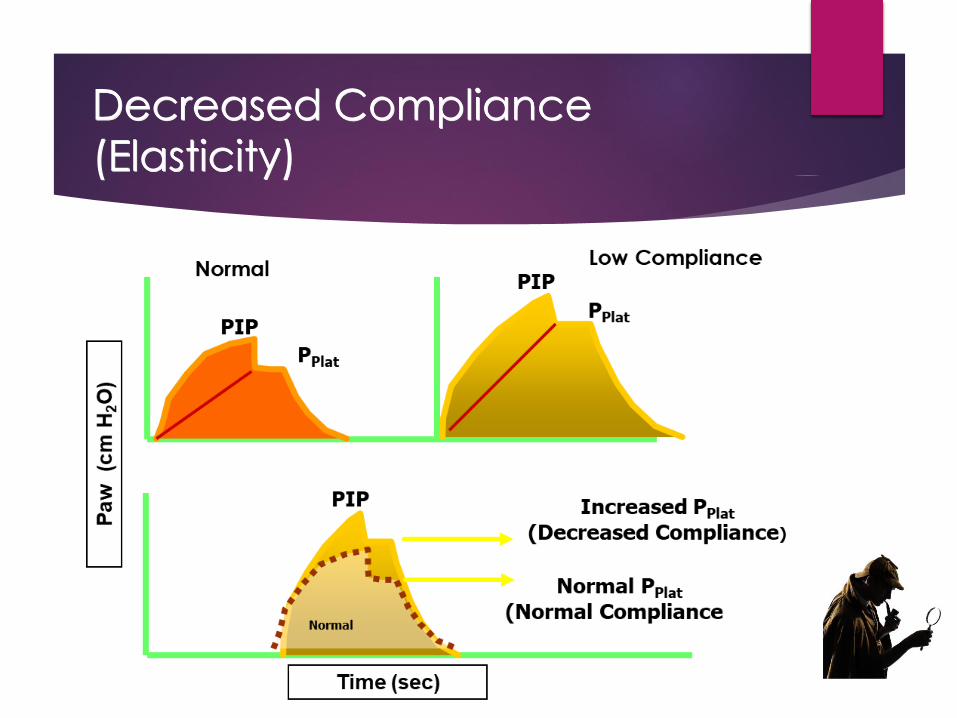
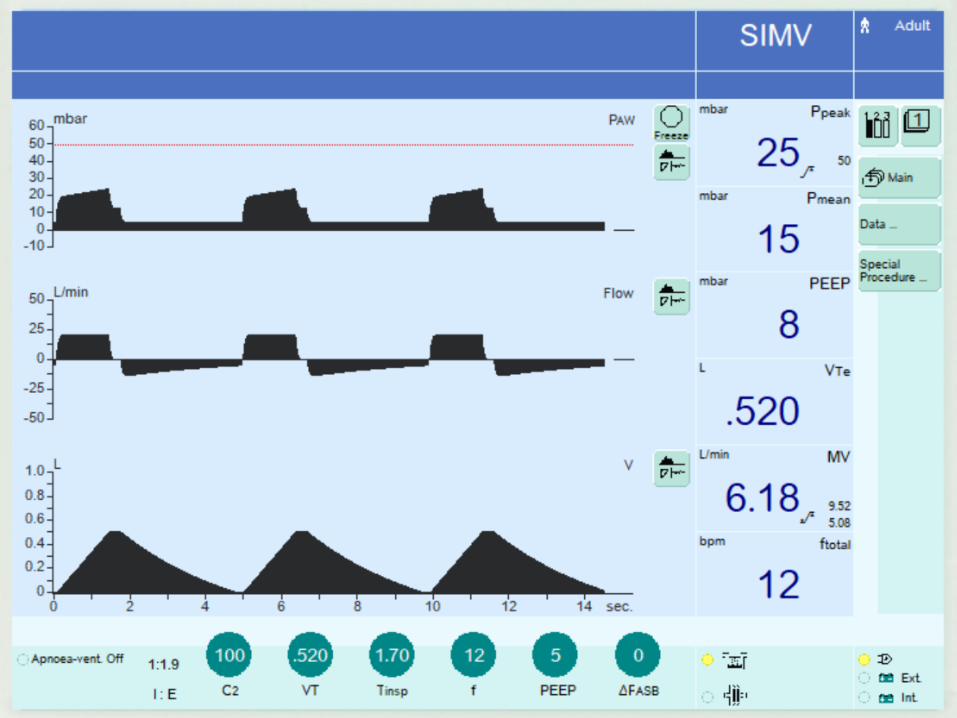
Decreased Compliance
(Elasticity)
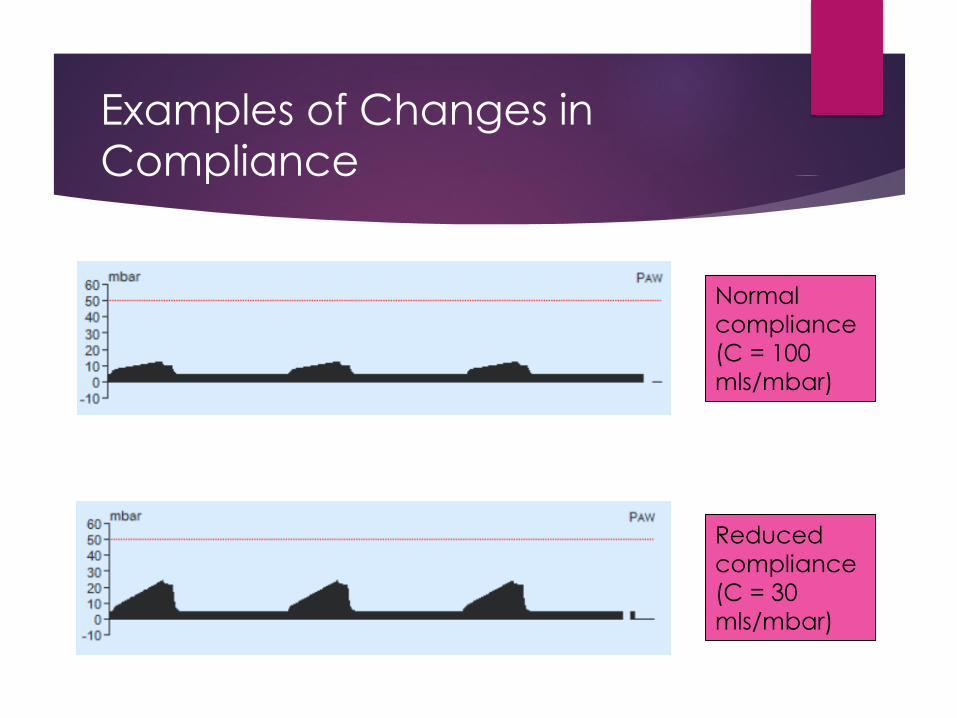
Normal
compliance
(C = 100
mls/mbar)
Reduced
compliance
(C = 30
mls/mbar)
Examples of Changes in
Compliance
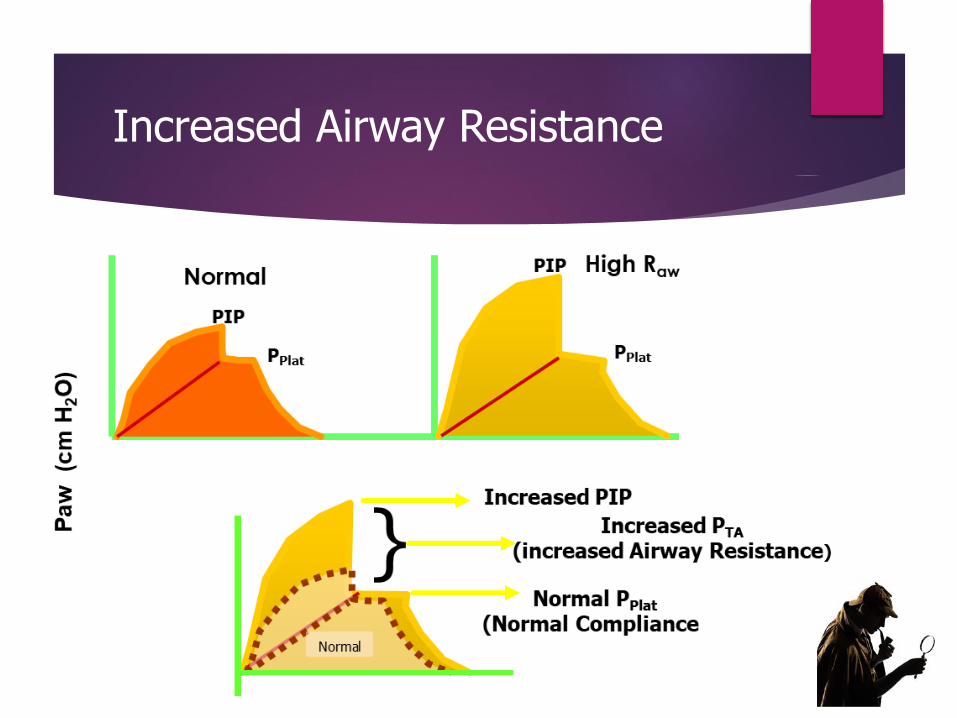
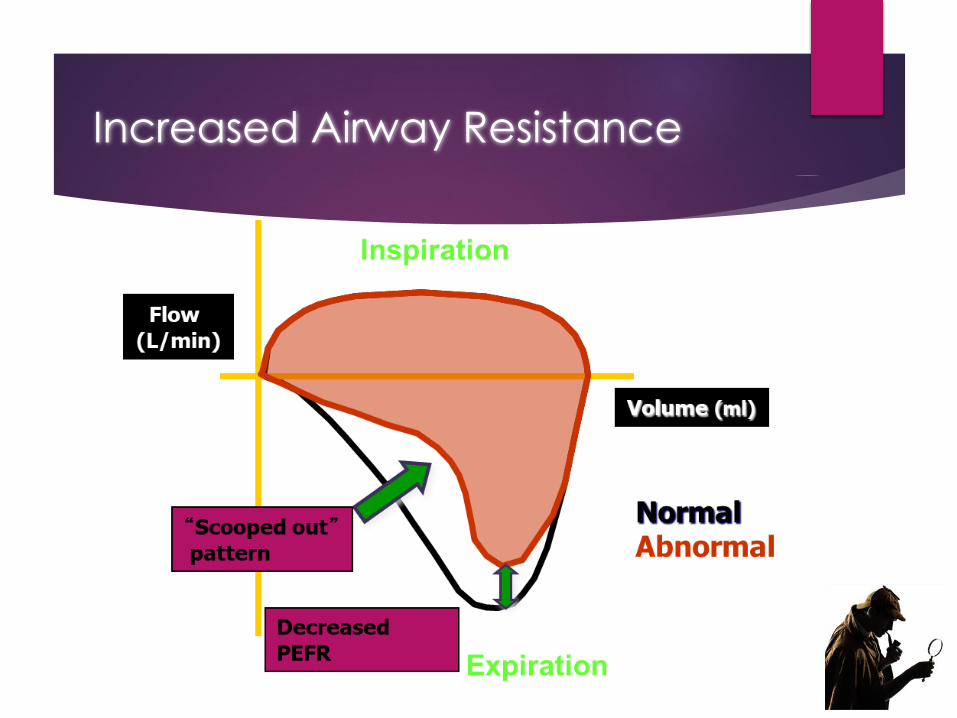
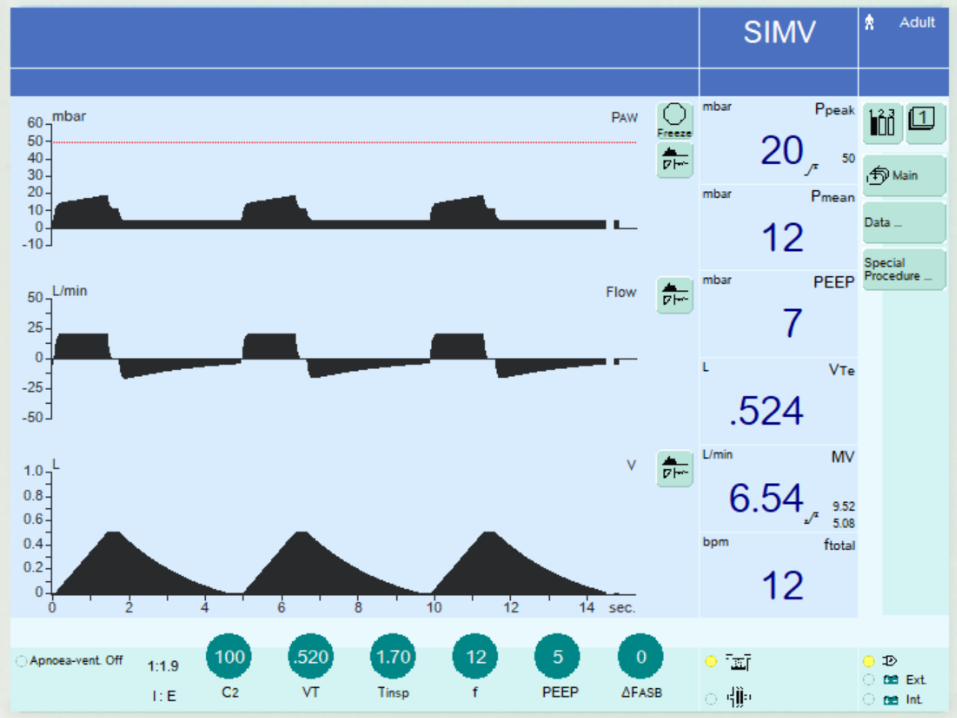
Increased Airway Resistance
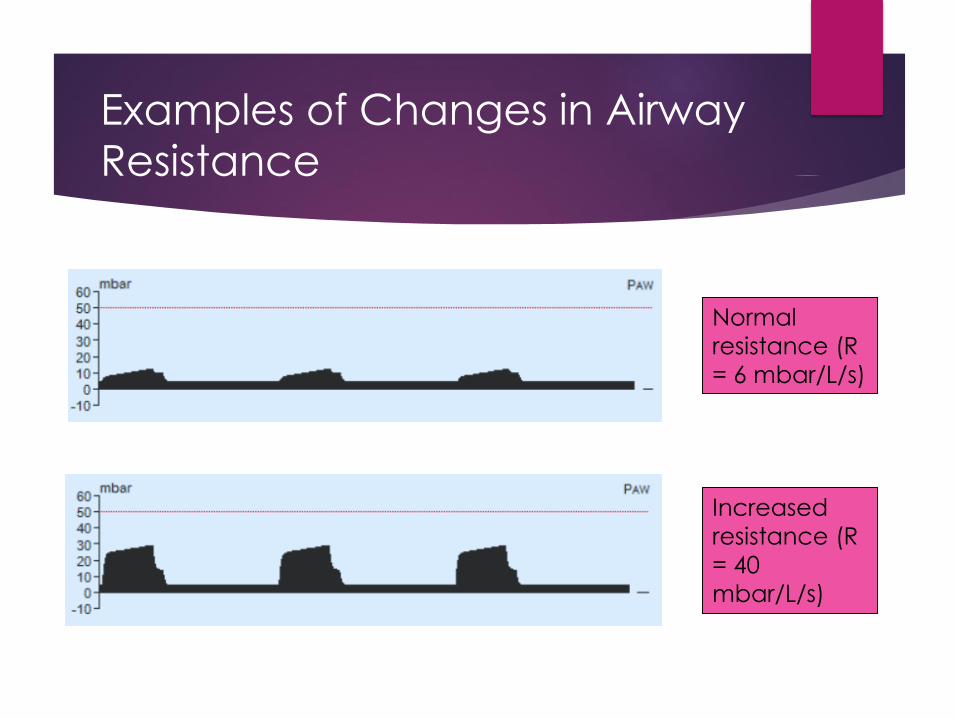
Normal
resistance (R
= 6 mbar/L/s)
Increased
resistance (R
= 40
mbar/L/s)
Examples of Changes in Airway
Resistance
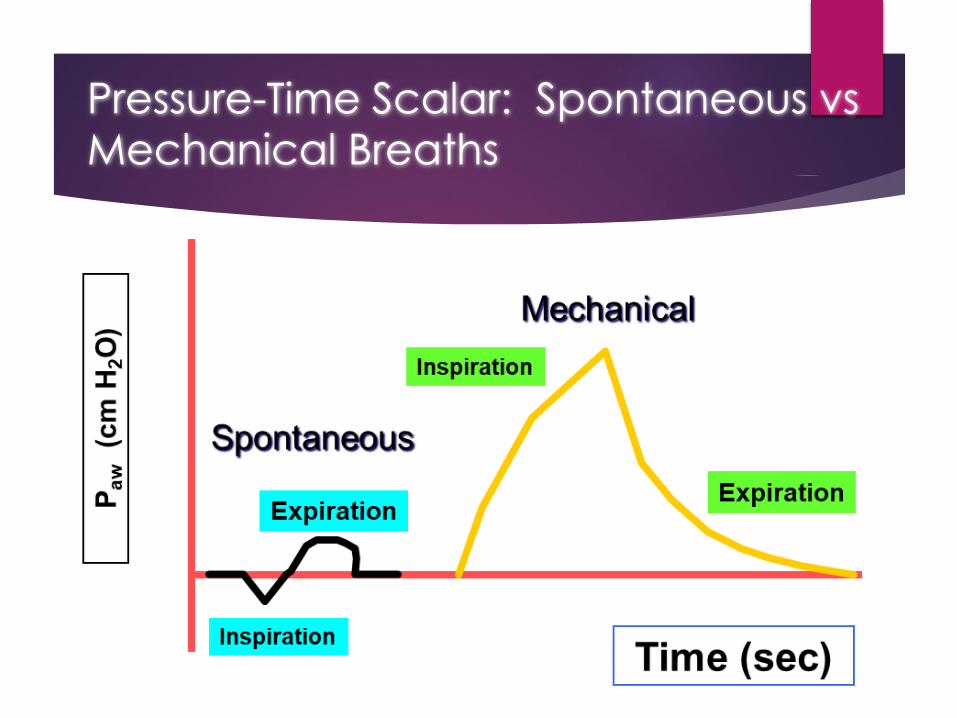
Pressure-Time Scalar: Spontaneous vs
Mechanical Breaths
Scalar:
Flow-
Time
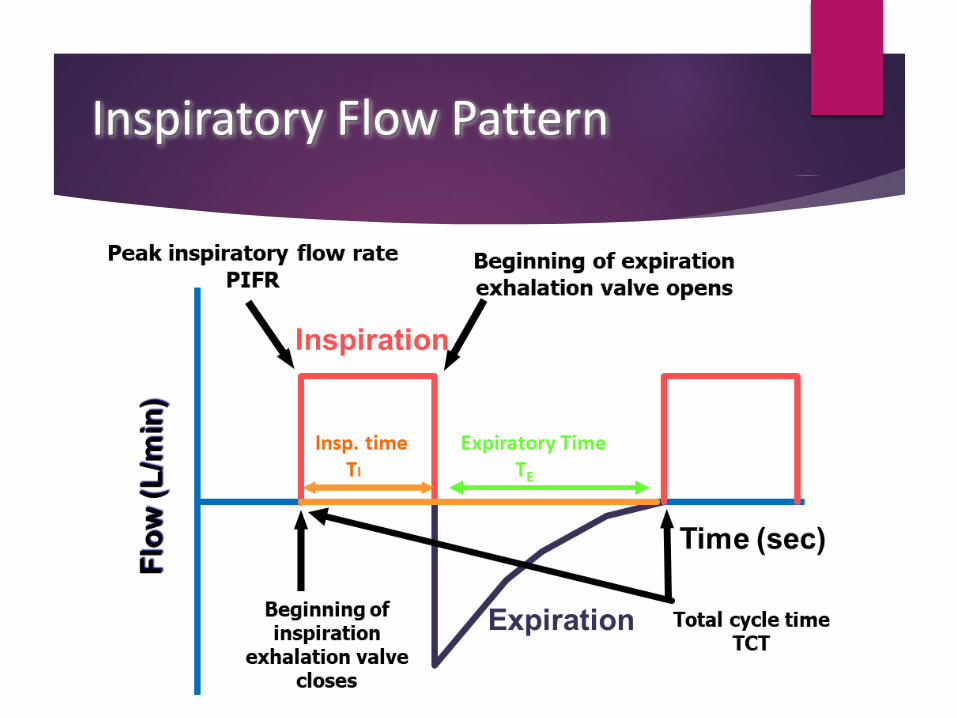
Inspiratory Flow Pattern
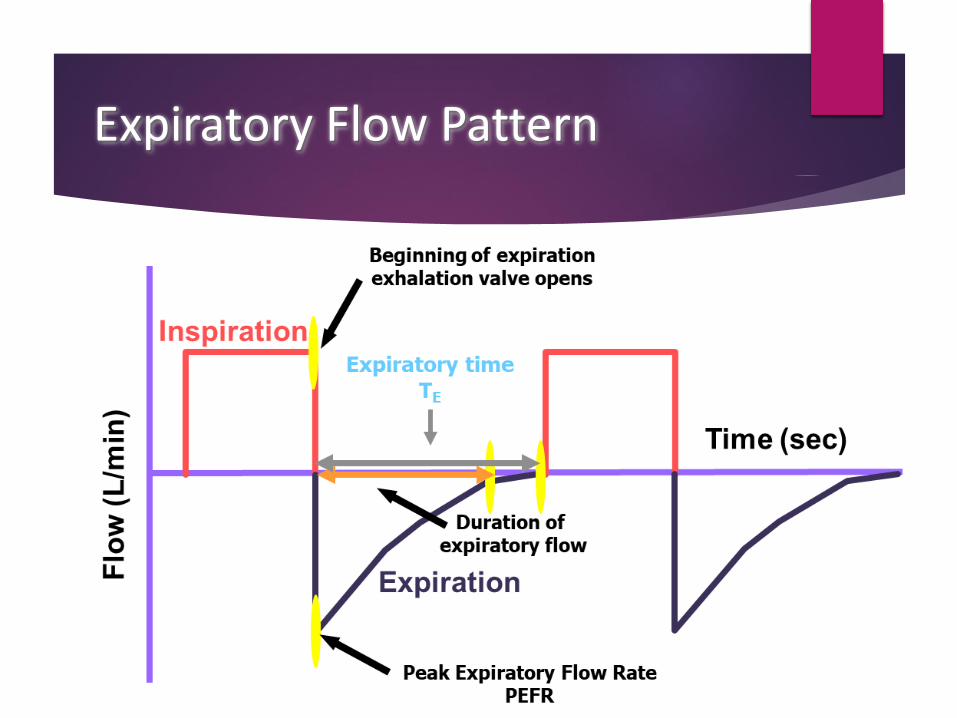
Expiratory Flow Pattern
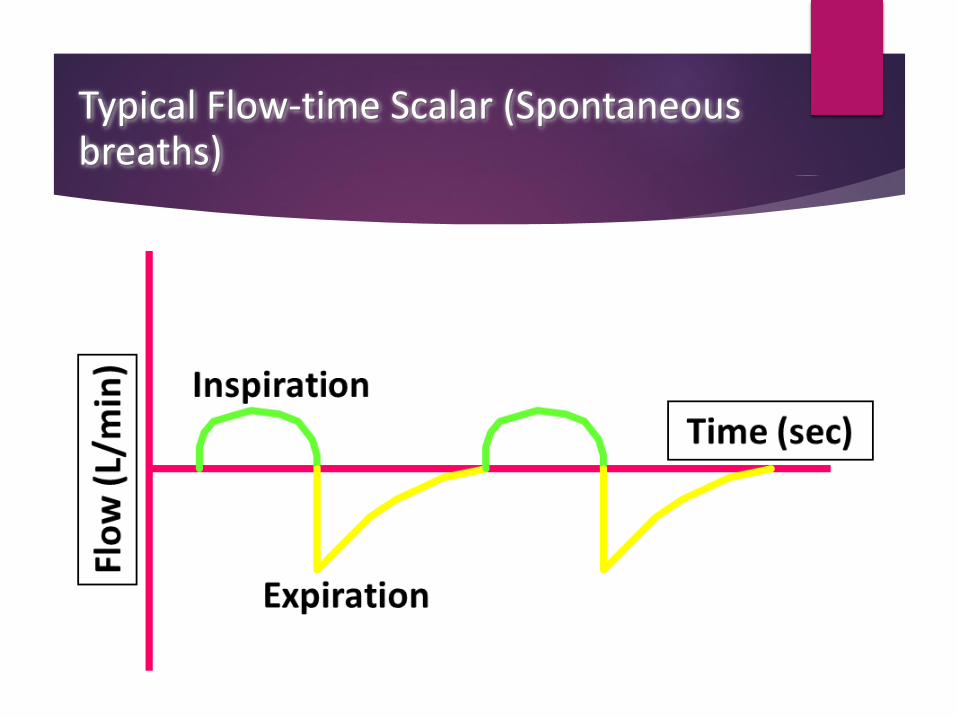
Typical Flow-time Scalar (Spontaneous breaths)
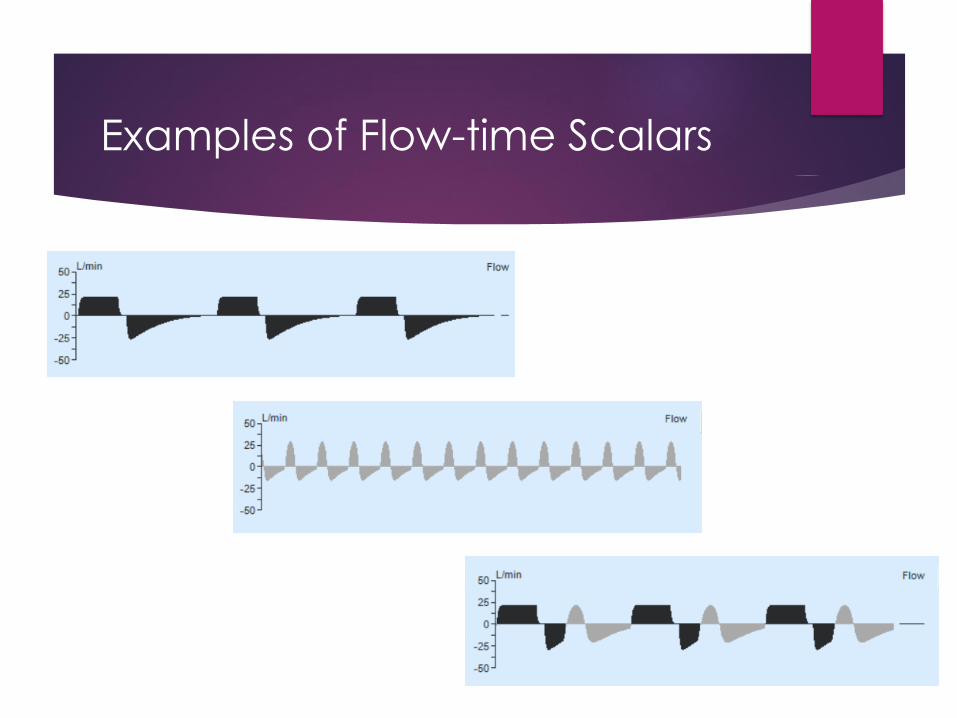
Examples of Flow-time Scalars
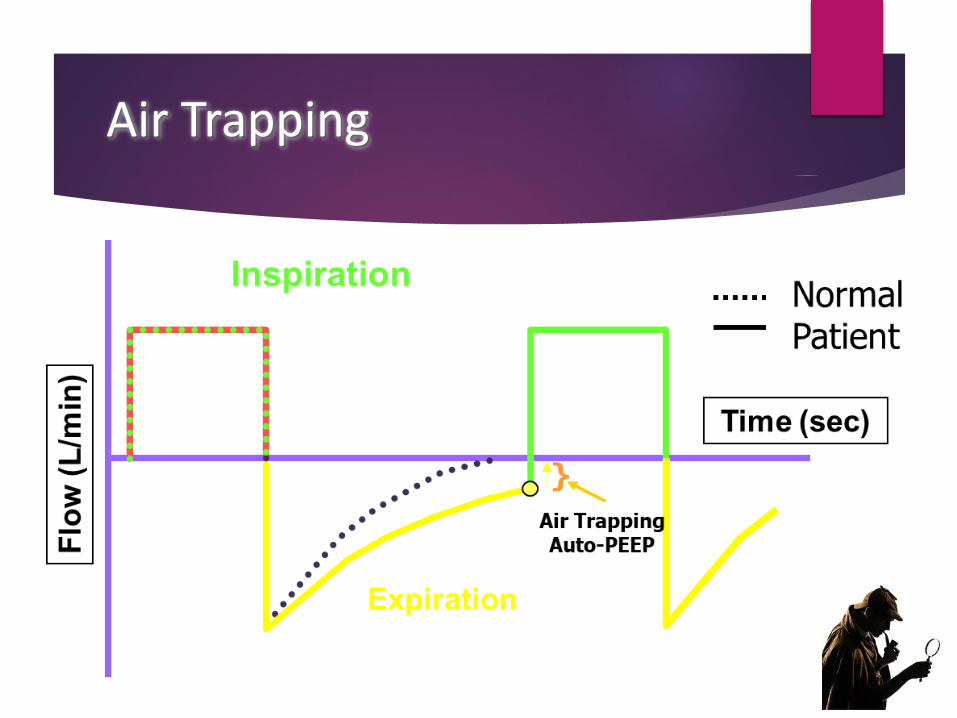
Air Trapping
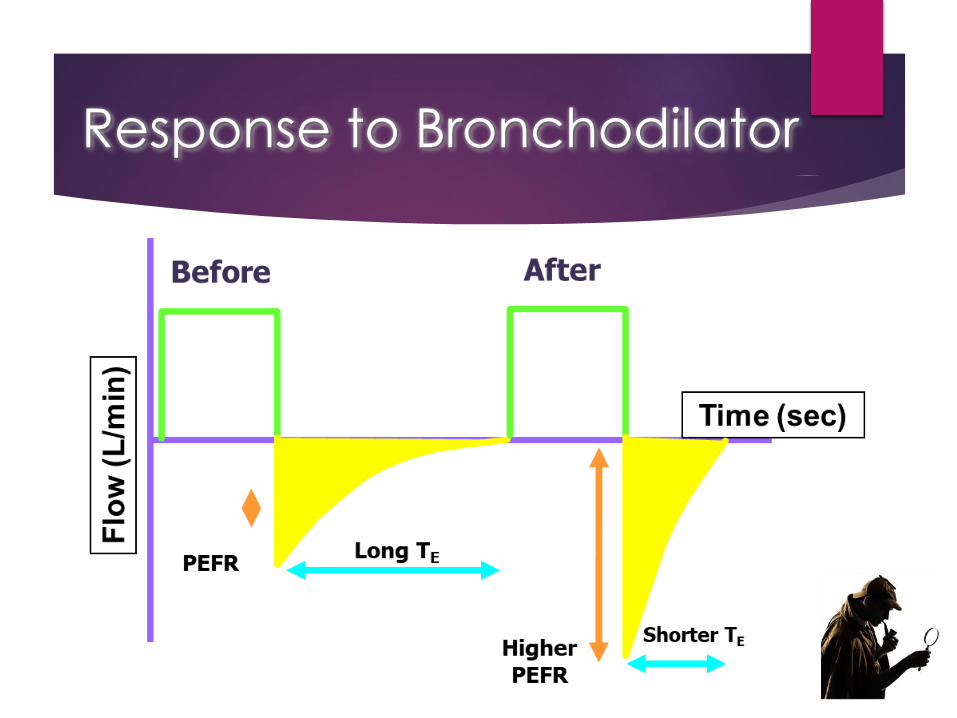
Response to Bronchodilator
Scalar:
Volume-
Time
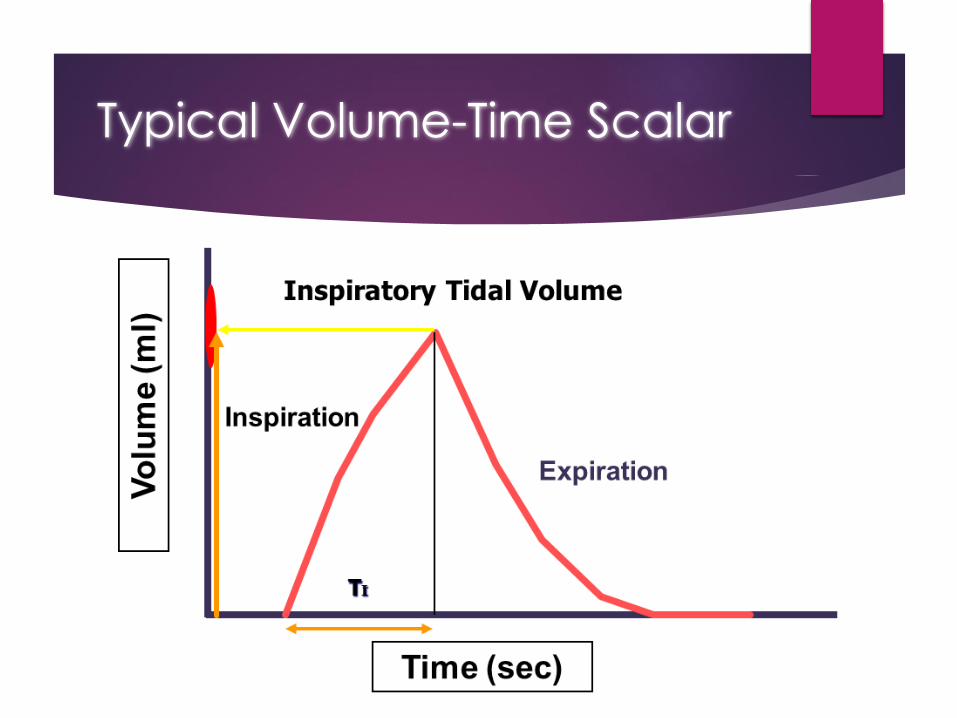
Typical Volume-Time Scalar
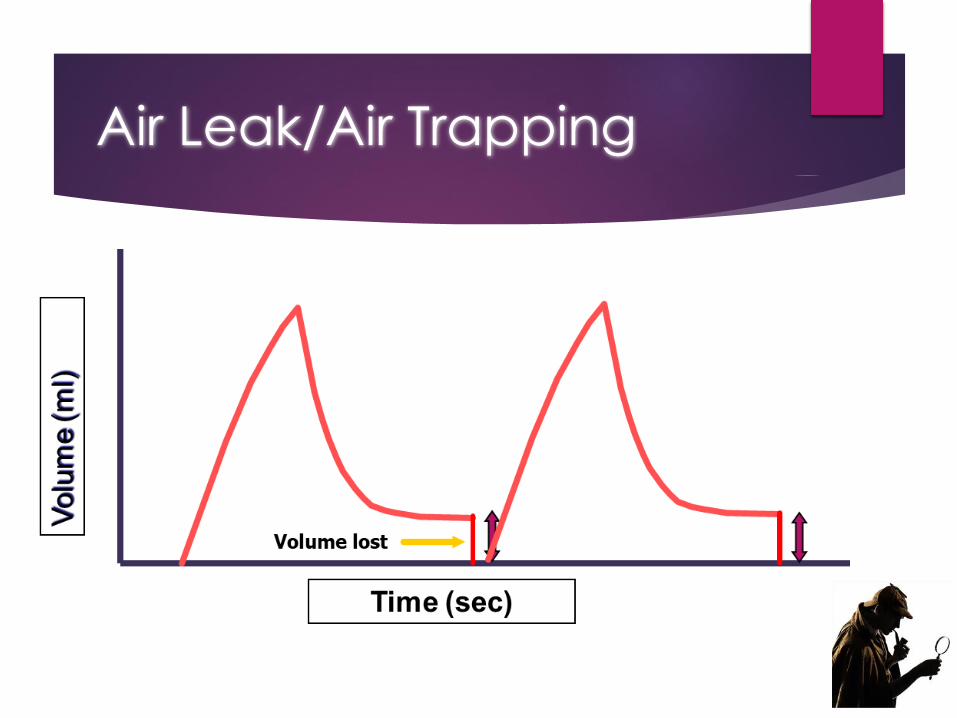
Air Leak/Air Trapping
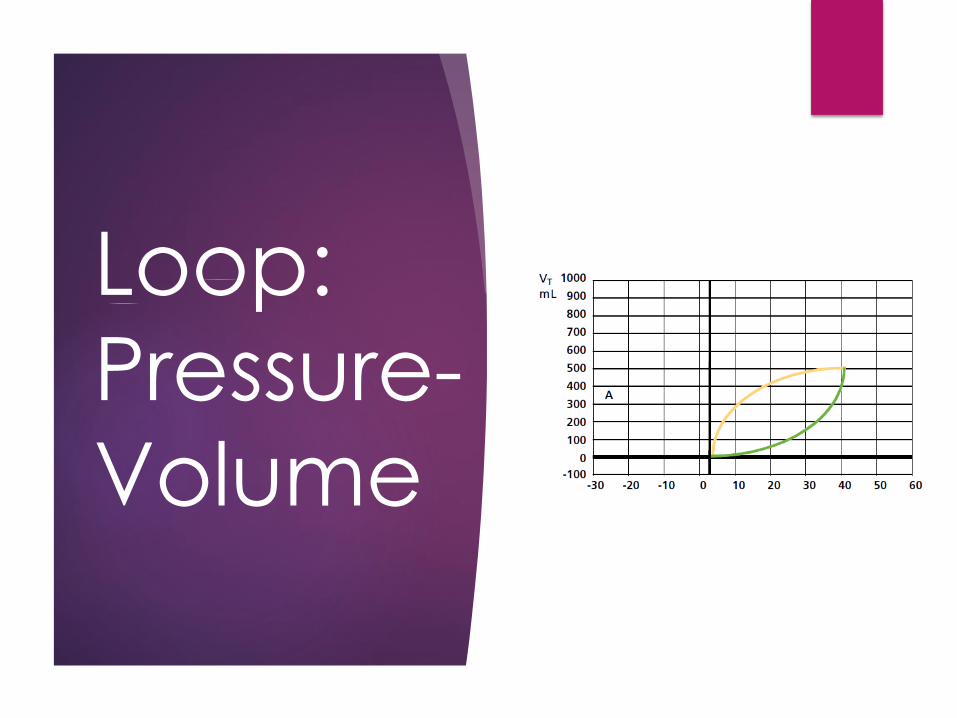
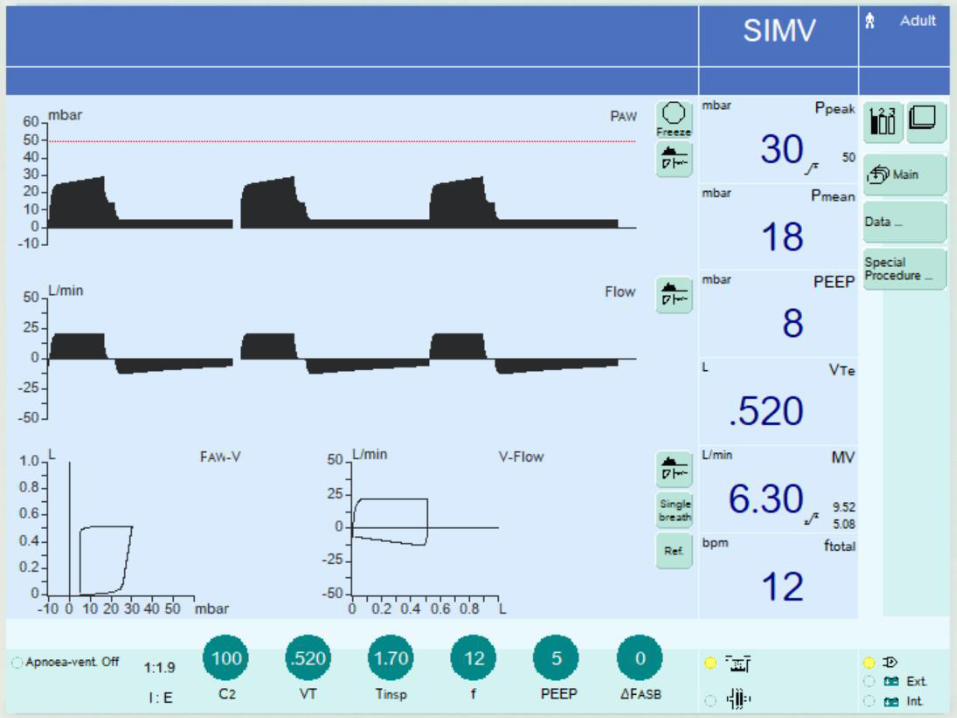
Loop:
Pressure-
Volume
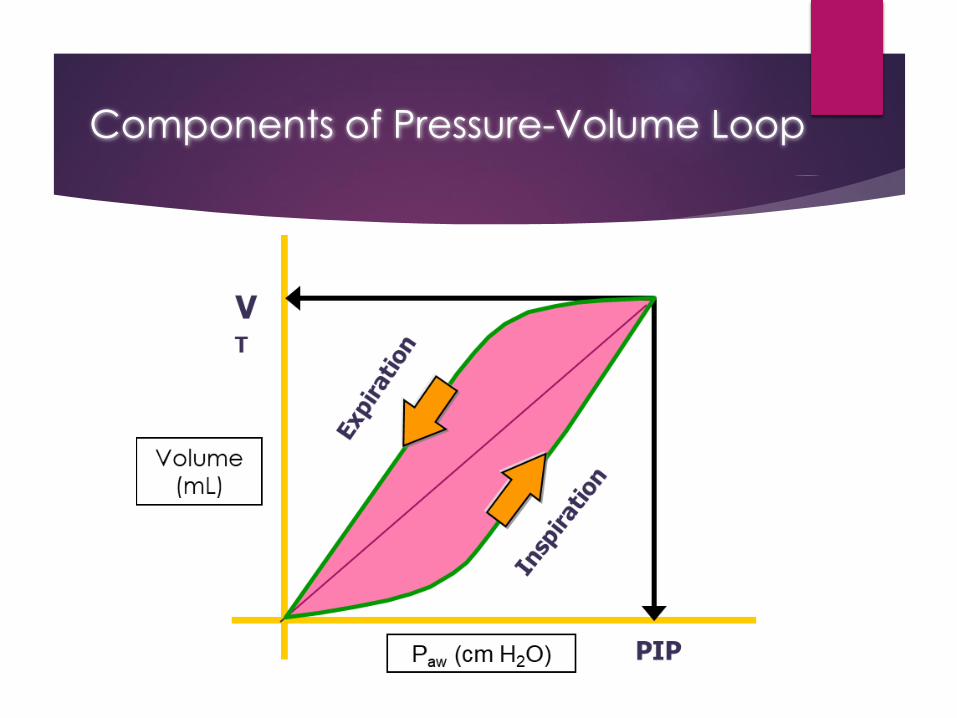
Components of Pressure-Volume Loop
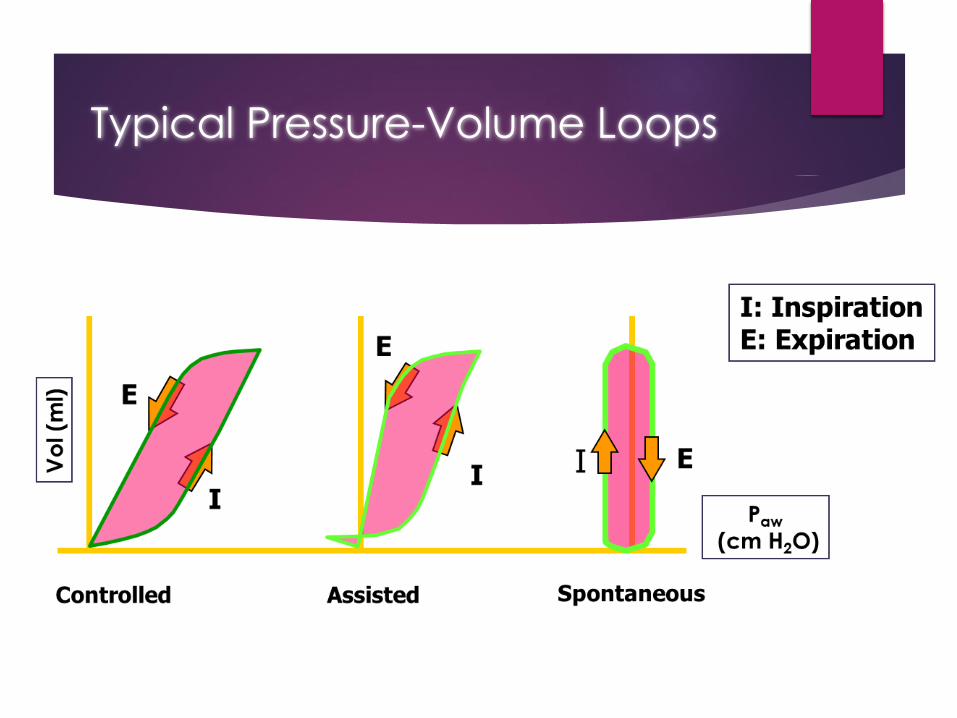
Typical Pressure-Volume Loops
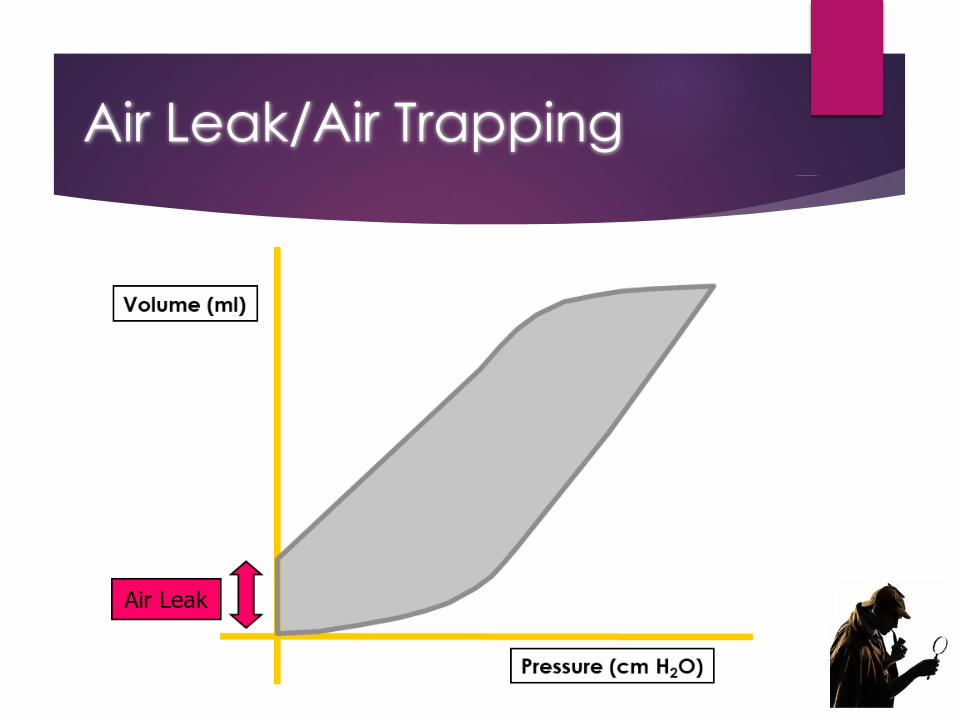
Air Leak/Air Trapping
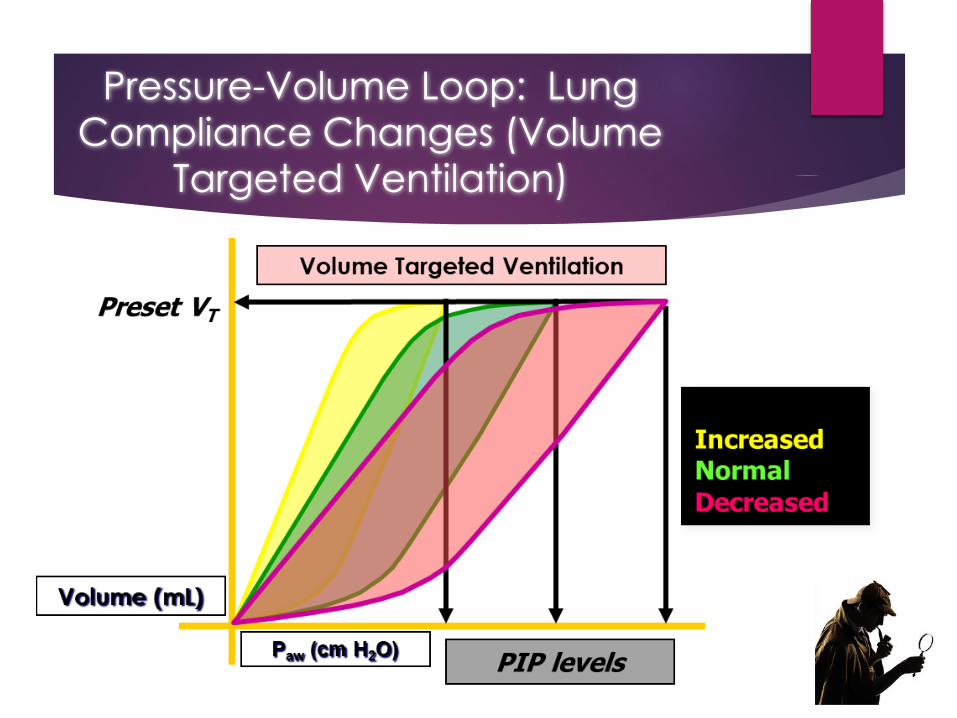
Pressure-Volume Loop: Lung
Compliance Changes (Volume
Targeted Ventilation)
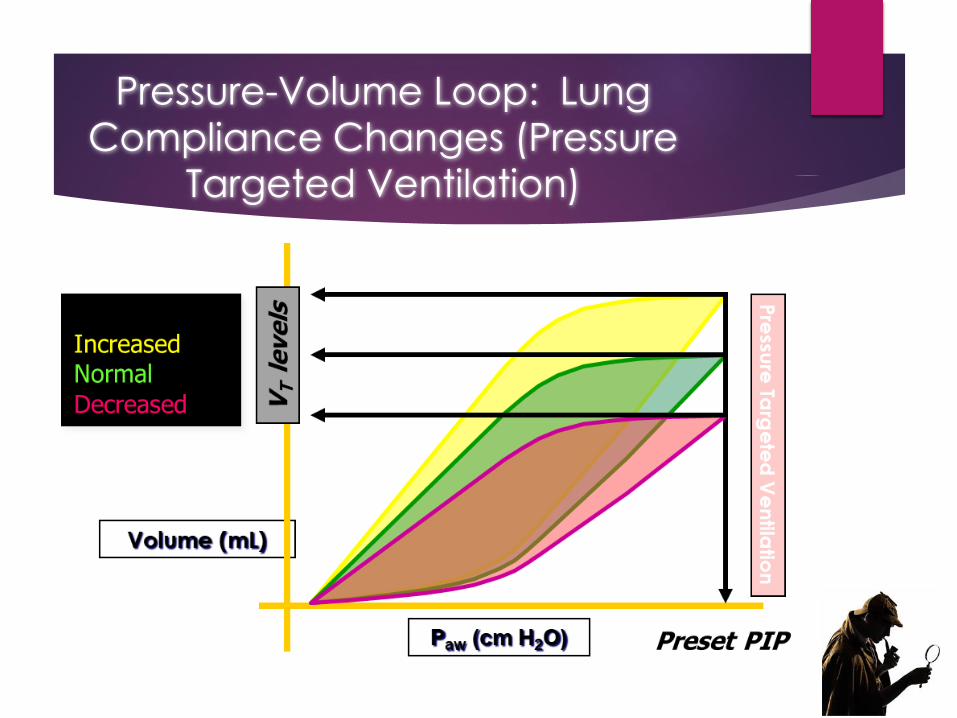
Pressure-Volume Loop: Lung
Compliance Changes (Pressure
Targeted Ventilation)
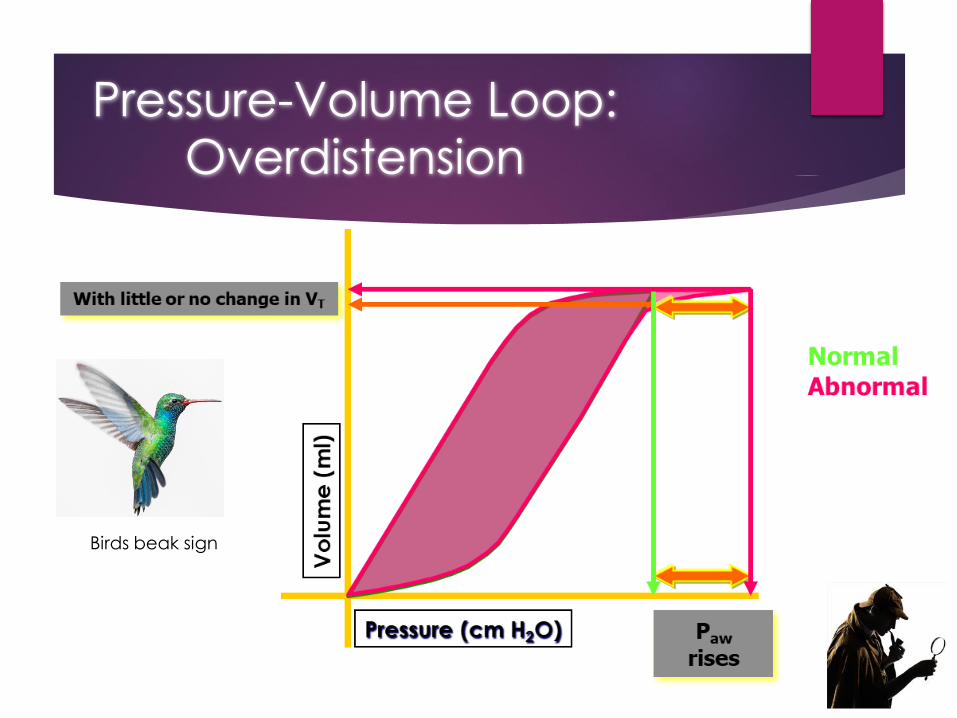
Pressure-Volume Loop:
Overdistension
Birds beak sign

Loop:
Flow-
Volume
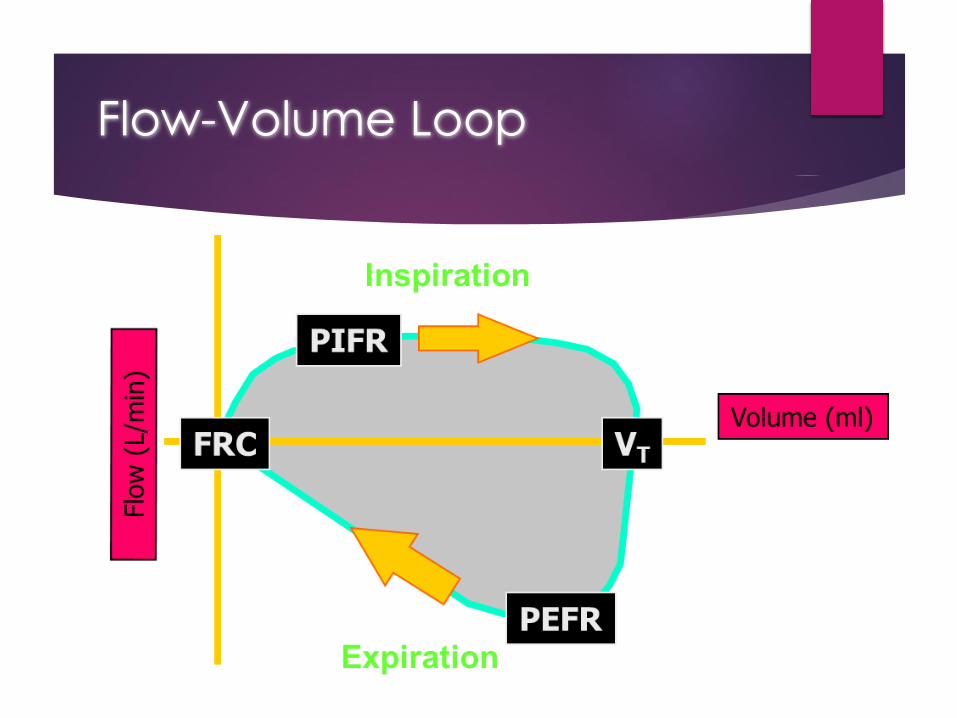
Flow-Volume Loop
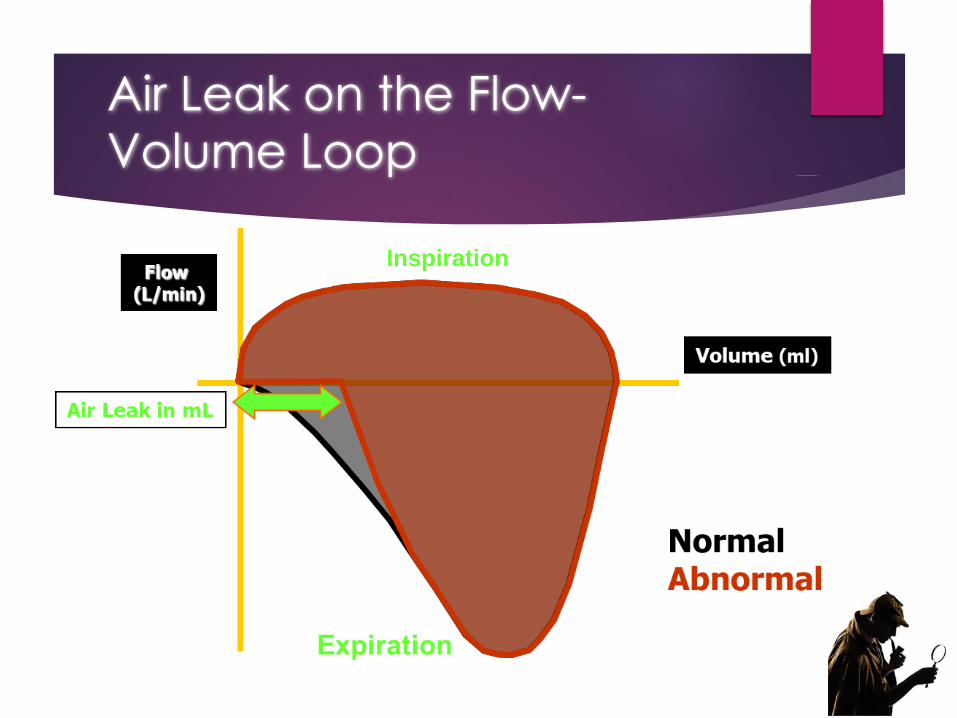
Air Leak on the Flow-
Volume Loop
Inspiration
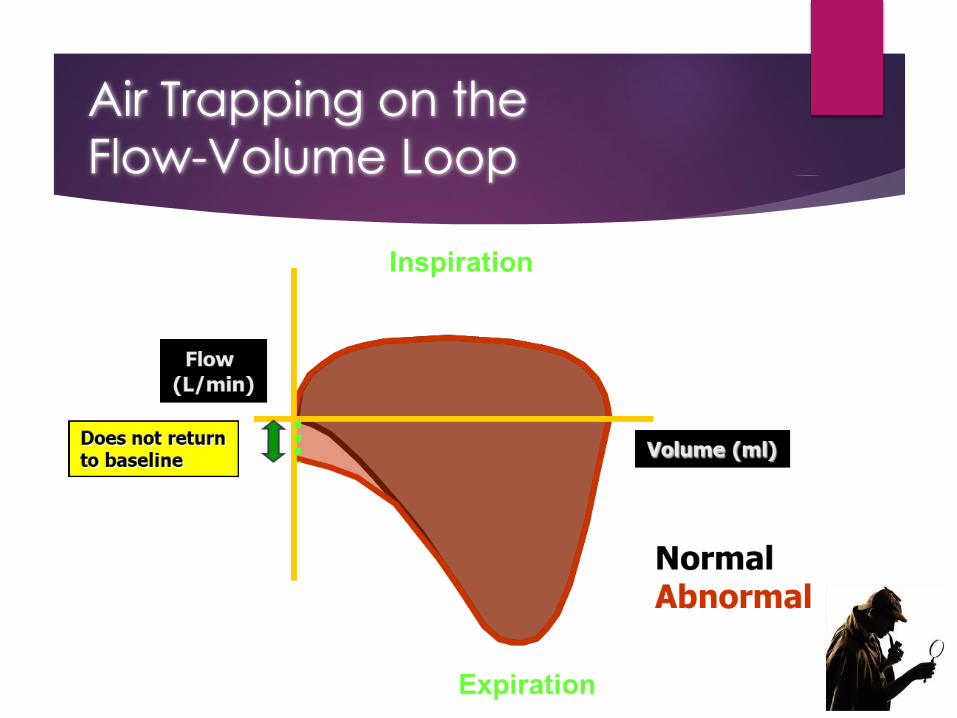
Air Trapping on the
Flow-Volume Loop
Increased Airway Resistance
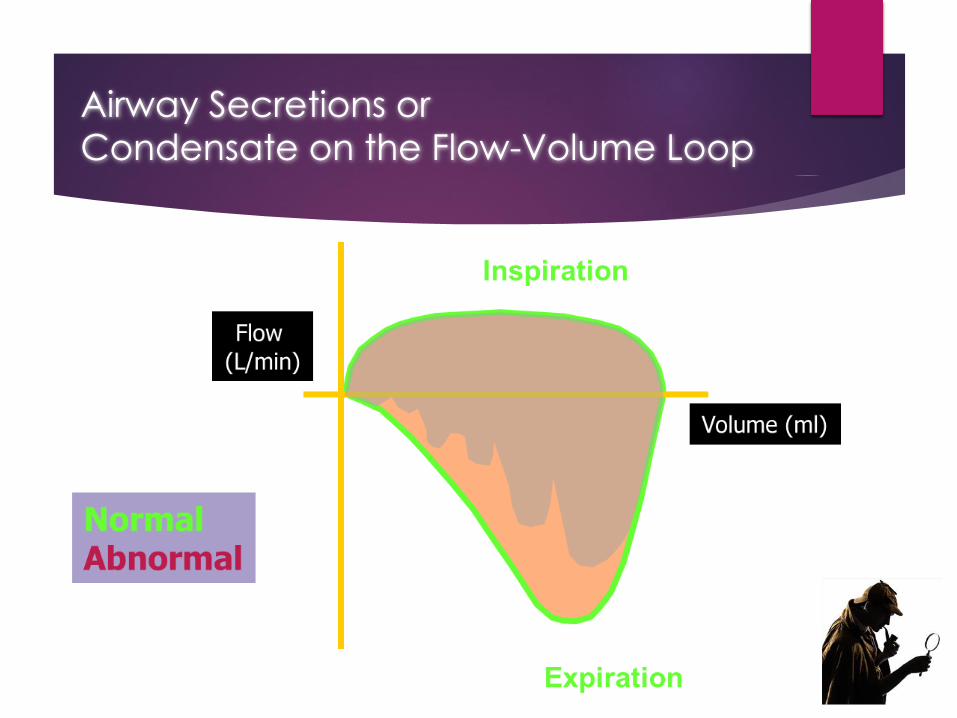
Airway Secretions or
Condensate on the Flow-Volume Loop
Real-time Scenarios:
Interpretation of
Mechanical Ventilation
Graphics
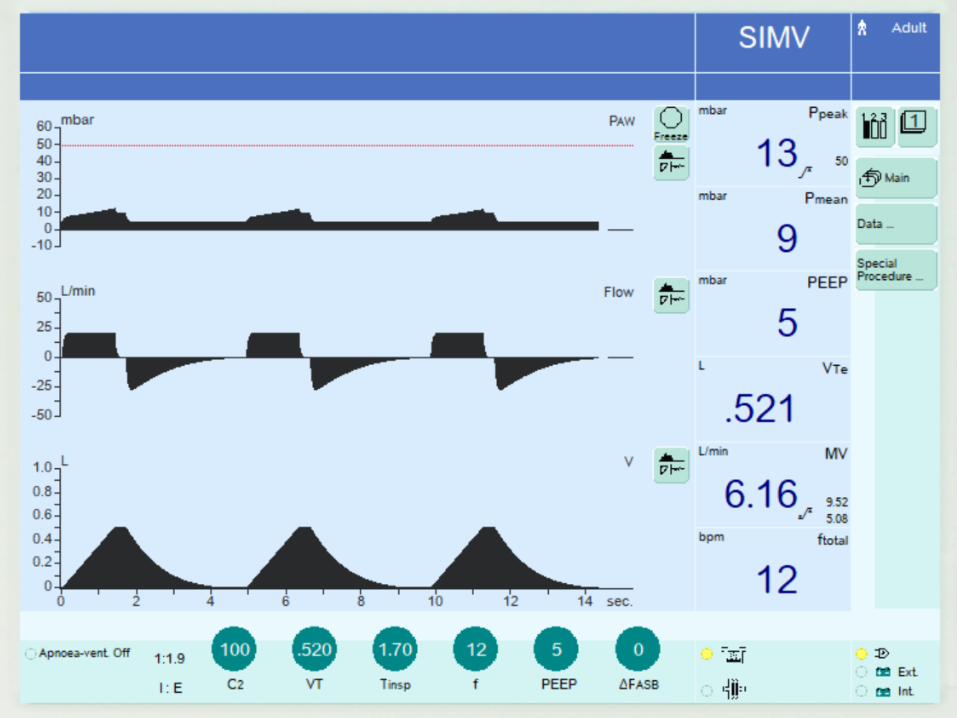
Alison
BP 94/68 mmHg, HR 122 bpm, RR 28 rpm, SpO2
93% on room air & 95% on 4L, afebrile –64
inches, 140 lbs/ 63 kg
Her ABG on 60% venturimask: pH 7.18, PaO2
64, PaCO2 70, HCO3 12 – using accessory
muscles
Intubated and placed on - 100% x 20, TV
6cc/kg – 381 cc , PEEP 5 cm– is this
appropriate at this time?
Should she be sedated ?
How would you sedate her ?
Paralytics?
Ralph – a complicated
patient
Hypoxic – why? Pain from rib fractures, altered MS from concussion/hypoxia
Atelectasis from hypoventilation due to pain, pulmonary contusions?
CXR reveals ground glass appearance bilateral lower lung fields – PTX right resolved, CT good position
ABG: Ph 7.47, PaO2 70 mmHg, PaCO2 33 mmHg, HCO3 18
HCT 9 from 10.3
PF ratio 175
What do you want to do – you can not switch your assignment……
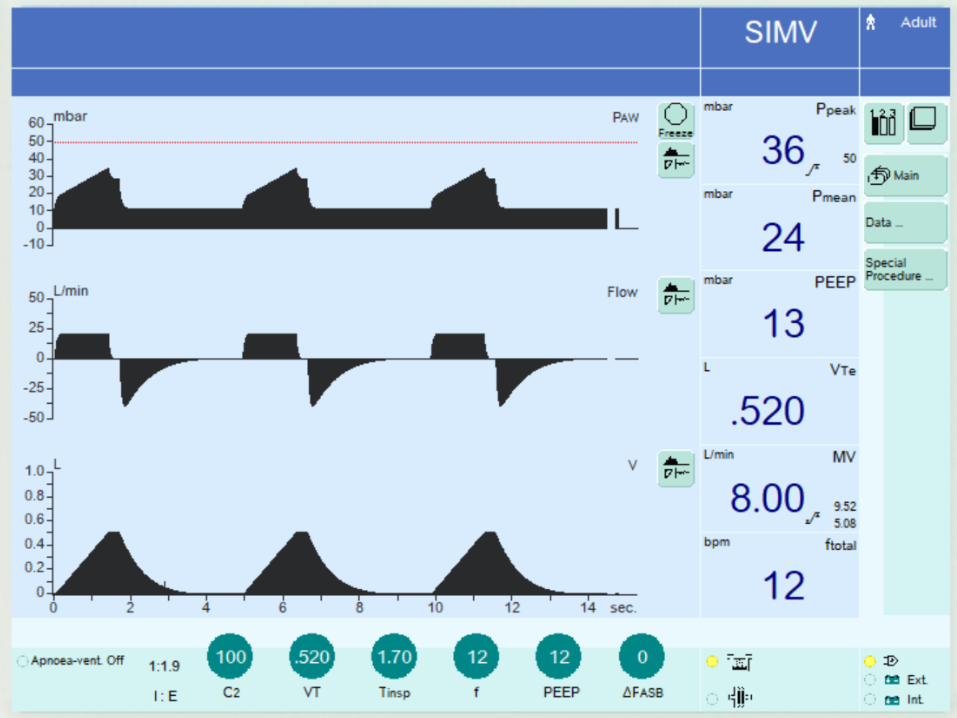
Ralph – a complicated
patient
6 hours later BP 150/78 mmHg, HR 114 bpm, RR 38 rpm, SpO2 85% on 15L
CXR reveals opacities bilateral lower lung fields – PTX right resolved, Chest tube in good position
Intubated due to worsening respiratory status
Breath sounds diminished bilaterally, rales bilat 1/3 up both lung fields
What is happening?
Learning Outcomes
1. Evaluate the role of waveforms and loops associated with ventilation and respiratory failure of the critically ill patient.
2. Outline the components and their clinical significance of normal and abnormal waveforms and loops.
3. List patient care considerations and safety issues associated with monitoring ventilator waveforms and loops.
Resources
Simulated ventilator screen images available from Draeger Medical (2020) https://www.draeger.com/en_uk/Hospital/Downloads
Emrath, E. (2021) The basics of ventilator waveforms. Current Pediatrics Reports. 9, p9-11.
Hess, D. & Kacmarek, R. (2014) Essentials of Mechanical Ventilation. 3rd Ed. McGraw-Hill Education.
Lian, J. (2009) Understanding ventilator waveforms –and how to use them in patient care. Nursing Critical Care. 4(1), p43-55.
Mackenzie, I. (2008) Core topics in mechanical ventilation. Cambridge University Press: Cambridge.


























![Pneumonia (Ventilator-associated [VAP] and non-ventilator](https://img.pdfslide.net/doc/110x75/61c3dfa934191a172140c0d5/pneumonia-ventilator-associated-vap-and-non-ventilator-.jpg)

