Embed Size (px)
Citation preview
J. Stomat. Occ. Med. (2009) 2: 147–159DOI 10.1007/s12548-009-0027-7Printed in Austria© Springer-Verlag 2009
Vertical dimension of occlusion: the keys to decisionWe may play with the VDO if we know some game’s rulesM. Rebibo1, L. Darmouni2, J. Jouvin3, J. D. Orthlieb2
1Nice, France2Faculté de Chirurgie-Dentaire de Marseille, Unité d’Occlusodontologie, Université de la Méditerranée, Marseille, France3Faculté de Chirurgie-Dentaire de Marseille, Unité de Prothèse, Université de la Méditerranée, Marseille, France
Received July 29, 2009; Accepted July 30; 2009
During an extensive prosthetic reconstruction, the choice ofthe vertical dimension of occlusion (VDO) is frequently pres-ented as the main point to obtain a success of treatment.
Probably, it is a sensible opinion to think that there is anoptimal adaptive space concerning the vertical dimension(VD) rather than a magic point. The practitioner may playwith the VD, if a strict rotation around the hinge axis is utilized,if the facial type is not worsened and if lip closure is kept in anatural position. In case of temporomandibular osteoarthritis,non progressive large changes of VD have to be avoided.
The decision making will be described in relation todifferent factors, such as overjet, overbite, prosthetic space,mandibular morphology, profile, vertical and horizontal skel-etal type.
Adecision-making table is proposed to visualize the trendof these different factors.
Keywords: Vertical dimension, vertical dimension of occlu-sion, decision making, prosthodontic, cephalometry
Introduction
For an extensive prosthetic reconstruction, the choice of thevertical dimension of occlusion (VDO) is often referred to asthe central issue, the essential problem.
Paradoxically, many arguments are frequently used tojustify the changes of the VDO in both direction, increasing ordecreasing. Mechanical reasons (retention, prosthetic space,and corono-root arm), aesthetic (profile and wrinkles), neu-romuscular (resting posture and muscle strength) and evenarticular (decompression) arguments are quite often used inthe debate on this particular subject.
Gaspard in 1985 concluded: “There is no accurate andreproducible method for determining VD” [6]. Palla in 1995[17], after a thorough literature’s review, confirms “Unfortu-nately, despite our knowledge about the mechanisms that
govern the different vertical dimensions and free way space,their determination remains a process primarily based onclinical experience of clinical practitioner”. At the time ofevidence-based dentistry, and despite 50 years of publicationon the subject, these findings place the practitioner still in asituation with more or less hazardous decisions based on theclinical experience.
Based on these facts, it seems to be quite important tohave proper tools in clinical decision making. How to verifythat the therapeutic VD will be in harmony with all theanatomical and neuro-physiological determinants?
Furthermore, what are the objective criteria’s, which letus determine to increase or decrease VD?
It is reasonable to believe that there is an optimal spacefor the VDO and not a single point miraculous [19].The newfree way space and VD rest are the results of a phenomenon ofneuromuscular adaptation [7].
This area of adaptation of vertical closure is defined by anupper limit, a lower limit and an amplitude, that remains to bedefined in terms of the potential for neuromuscular adapta-tion to each and mechanical parameters to evaluate.
Having sought to identify relevant criteria, benchmarksand insufficient unfounded beliefs, this article aims to proposea method of comparing the critical reflection involved andleading to a maintenance or modification of the quantizedVDO (in the sense of reduction or enlargement).
Myths or limits?
“The VDO could not be increased”
“Conserve the VDO corresponding to the ICP and don’tincrease it” [4]. The belief, that an increase in the verticaldimension causes temporomandibular disorders (TMD), de-rived from the following hypothesis: an elevation induces anincrease in the tonicity of elevator muscles, with a possibleonset of muscle pain, increased tooth mobility and finallythe intrusion of teeth. This ingression would generate adecrease in VDO and a return to its initial value. Palla, onthe contrary, remarks, that this assumption, has not beenconfirmed [17]:
Correspondence: Pr. Jean-Daniel Orthlieb, DDS, PhD, Faculté deChirurgie-Dentaire de Marseille, Unité d’Occlusodontologie, Universitéde la Méditerranée, 27 bd Jean Moulin 13555Marseille cedex 7, France.E-mail: [email protected]
position paper
J. Stomat. Occ. Med. � Springer-Verlag Vertical dimension of occlusion: the keys to decision 3/2009 147
– A degree of relapse sometimes occurs after increasingocclusal height, but it is not constant, and VDO is not theoriginal value when it is increased in one step of severalmillimeters (e.g. in orthognathic surgery or in animalexperiments).
– This degree of relapse caused by bone remodeling and in-gression of the teeth cannot only be connected to thedegree of increase and occurs especially in the earlymonths.
– An increased VDO does not appear to disrupt the chewingfunction. It has been shown that the increase of VD results inmost cases a relaxation of closing muscles [20], which is
found clinically on a daily practice with the wear of anocclusal splint.
The opinion of the authors on relapses of VD is that thecontrol of functions (e.g. Tongue interposition, clenching)could be a more important factor of avoiding a relapse thanthe proper initial variation of VDO:
Increase the VDO: A skeletal open bite type is not acomplete obstacle to increase VDO, but the relaxed closedlip posture could represent a limit. In case of a relapse with theresult of a decreased lower facial height few years aftertreatment, there is at least the strong possibility to link thisrelapse to an uncontrolled behavioural factor (e.g. dentalintrusions due to clenching or bruxism)?
Decrease the VDO: In some anterior open bite cases, adecrease of the VDO must be accompanied by a strongcoaching of functional reeducation of nasal breathing, restposture of the tongue and swallowing.
“VDO could not be reduced” or the confusionbetween loss of VD and subsequent lossof occlusal posterior support
On the topic of reducing the VDO, we find contradictoryand unjustified opinions as: “Any grinding cusps inevitably
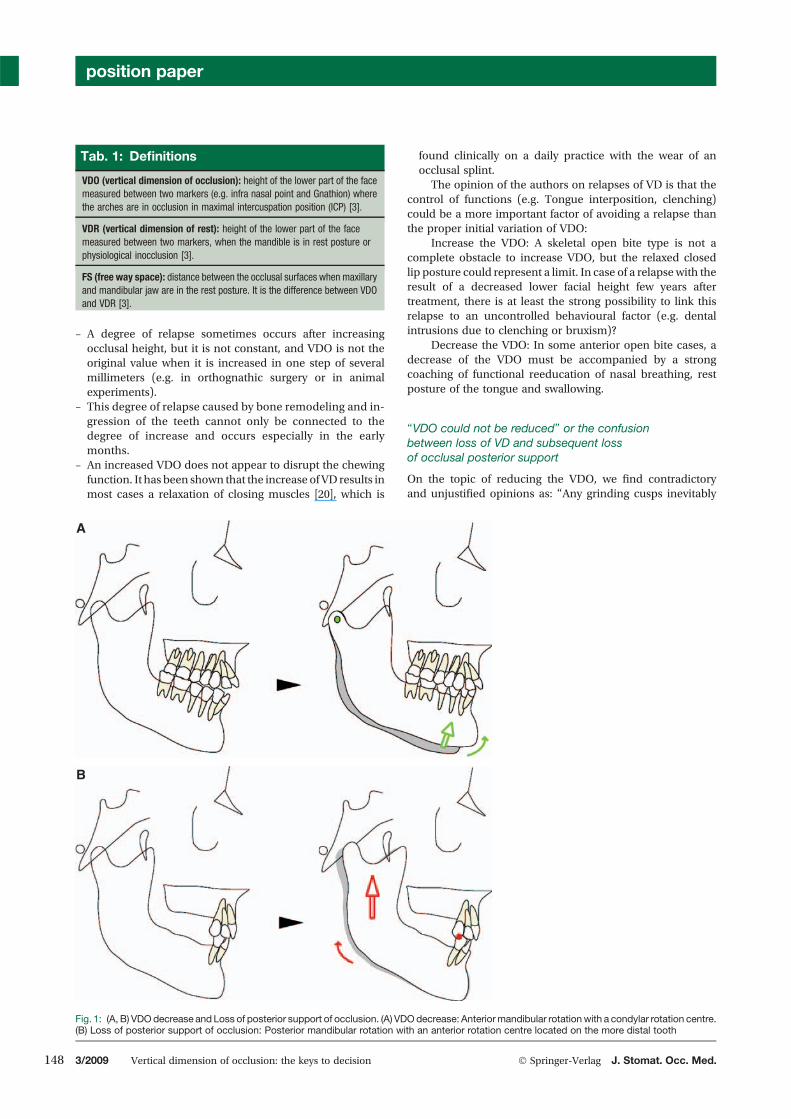
Tab. 1: Definitions
VDO (vertical dimension of occlusion): height of the lower part of the facemeasured between two markers (e.g. infra nasal point and Gnathion) wherethe arches are in occlusion in maximal intercuspation position (ICP) [3].
VDR (vertical dimension of rest): height of the lower part of the facemeasured between two markers, when the mandible is in rest posture orphysiological inocclusion [3].
FS (free way space): distance between the occlusal surfaces when maxillaryand mandibular jaw are in the rest posture. It is the difference between VDOand VDR [3].
A
B
Fig. 1: (A, B) VDOdecrease and Loss of posterior support of occlusion. (A) VDOdecrease: Anteriormandibular rotationwith a condylar rotation centre.(B) Loss of posterior support of occlusion: Posterior mandibular rotation with an anterior rotation centre located on the more distal tooth
position paper
148 3/2009 Vertical dimension of occlusion: the keys to decision � Springer-Verlag J. Stomat. Occ. Med.
causes a reduction in VD” [6], “Few cases warrant a reductionin VD”; “There is no apparent problem associated with thedecrease in VD” [4]. This latter view seems to be confirmed byMagnusson [9].
If, in the past, it has often stated that the TMD arecorrelated with loss of VD, probably due to the frequentconfusion between loss of VDO and subsequent loss of occlu-sal posterior support [14].
From a geometrical and mechanical point of view, adecrease of the VD is completely different to the loss ofposterior occlusal support. The VDO corresponds to thelimit of rotation of mandibular elevation, which meansthat its variations corresponds to the situation of the“vertical occlusal stop” of rotation of mandibular elevationwhich means that the variations of VDO are carried outaround the mandibular hinge axis, defining an angle ofrotation.
It is thus aberrant to speak about posterior verticaldimension and anterior vertical dimension. Perhaps the termsposterior and anterior “dental space” or “available prosthetic
height” should be used instead. There is only one VD for themandible; variations of this VD are related to angular rotationin regards to the mandibular hinge axis.
On the contrary, the loss of posterior occlusal supportcorresponds to a posterior mandibular rotation around ananterior dental point of support (centre of rotation), thissituation could be critical for the TMJ [24].
“Dental abrasion would mean loss of VDO”
In fact, generally dental abrasion does not mean loss of VDO.Since Niswonger in 1938 [11], we should know, that thepresence of abraded teeth does not mean that the VD is
BA
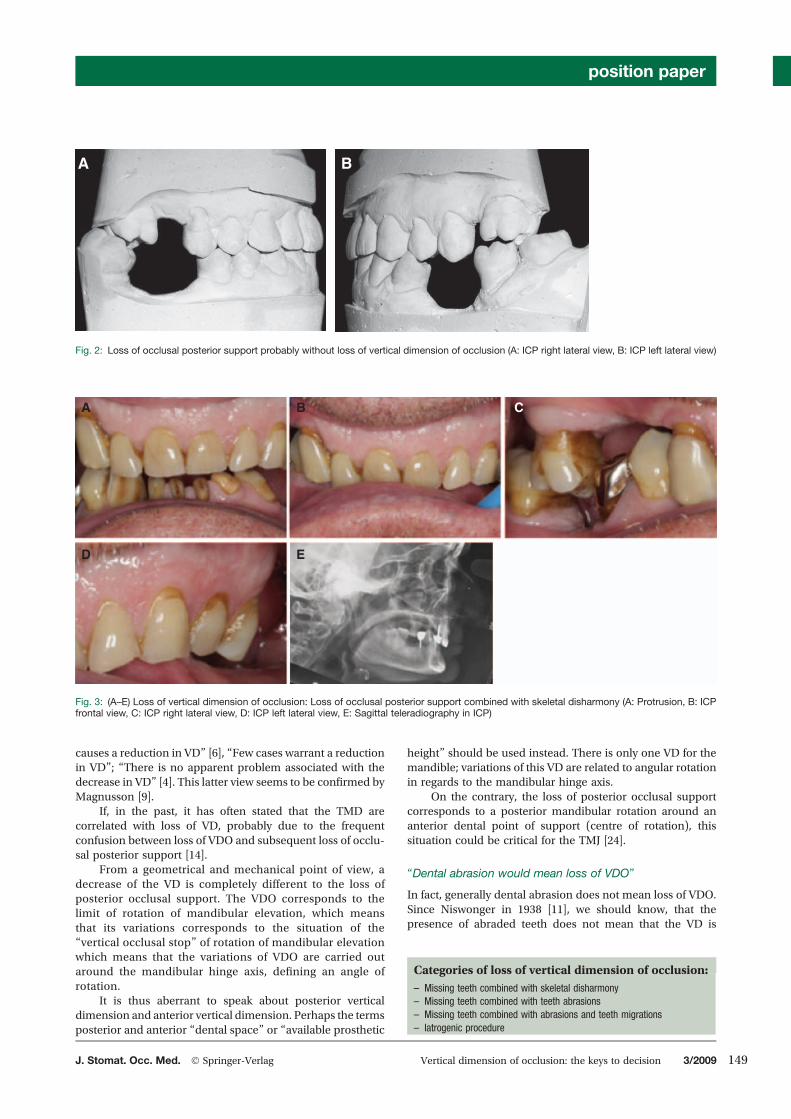
Fig. 2: Loss of occlusal posterior support probably without loss of vertical dimension of occlusion (A: ICP right lateral view, B: ICP left lateral view)
A C
D E
B
Fig. 3: (A–E) Loss of vertical dimension of occlusion: Loss of occlusal posterior support combined with skeletal disharmony (A: Protrusion, B: ICPfrontal view, C: ICP right lateral view, D: ICP left lateral view, E: Sagittal teleradiography in ICP)
Categories of loss of vertical dimension of occlusion:
– Missing teeth combined with skeletal disharmony– Missing teeth combined with teeth abrasions– Missing teeth combined with abrasions and teeth migrations– Iatrogenic procedure
position paper
J. Stomat. Occ. Med. � Springer-Verlag Vertical dimension of occlusion: the keys to decision 3/2009 149

A B C
Fig. 4: (A–C) Anterior teeth abrasion: probably no loss of VDO (A: occlusal view, B: ICP frontal view, C: Sagittal teleradiography in ICP)
A B C
D E F
Fig. 5: (A–C) Missing teeth combined with teeth migrations (A: ICP right lateral view, B: ICP frontal view, C: ICP left lateral view, D: maxillar arch,E: mandibular arch, F: Sagittal teleradiography in ICP)
A
D E F
B C
Fig. 6: (A–C) Loss of vertical dimension of occlusion: Loss of occlusal posterior support combinedwith teeth abrasions (A: ICP right lateral view, B: ICPfrontal view, C: ICP left lateral view, D: occlusal view, E: mounting cast in centric relation, F: Sagittal teleradiography to test an increased VDO)
position paper
150 3/2009 Vertical dimension of occlusion: the keys to decision � Springer-Verlag J. Stomat. Occ. Med.
systematically reduced, a compensatory egress, especially inthe anterior teeth, is very frequently observed.
The presence of anterior dental migration, with re-cent diastemas, associated with a subsequent loss ofposterior support seems to be a more obvious clinicalsituation [12].
“Posture of rest and free way space would be stableclinical references”
Rivera-Morales [19], Rugh and Drago [20], amongst manyothers, have reported the lack of reproducibility of thevertical dimension of rest (VDR) evaluations (electromyo-graphic or clinical), the large variability of the free wayspace and its adaptability to VDO variations. From ahypothetical clinical measurement of the inter-occlusalfree way space, what is the basis to evaluate the level ofthe VDO?
Phonetic tests are clinical stable references
Although Silverman [21] thought, minimum vertical phoneticspace as immutable, but clinical experiences generaly foundthat there is a large capacity of adaptation in this area.
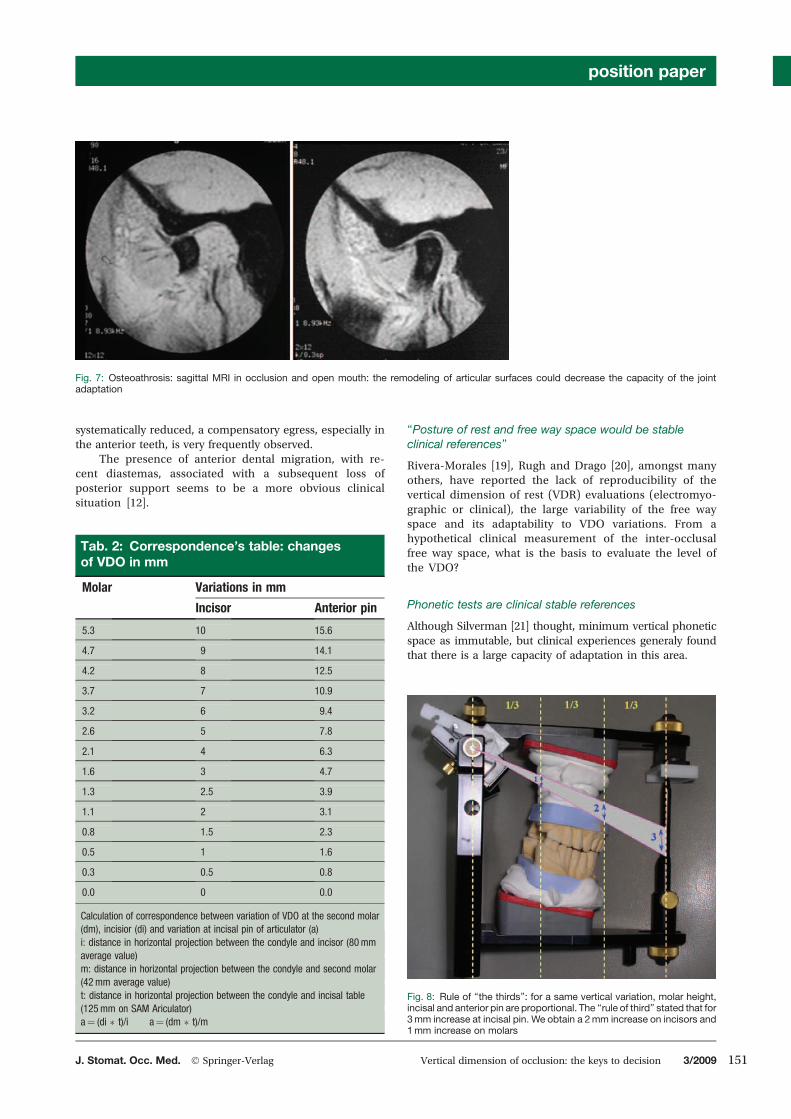
Fig. 7: Osteoathrosis: sagittal MRI in occlusion and open mouth: the remodeling of articular surfaces could decrease the capacity of the jointadaptation
Tab. 2: Correspondence’s table: changesof VDO in mm
Variations in mmMolar
Incisor Anterior pin
5.3 10 15.6
4.7 9 14.1
4.2 8 12.5
3.7 7 10.9
3.2 6 9.4
2.6 5 7.8
2.1 4 6.3
1.6 3 4.7
1.3 2.5 3.9
1.1 2 3.1
0.8 1.5 2.3
0.5 1 1.6
0.3 0.5 0.8
0.0 0 0.0
Calculation of correspondence between variation of VDO at the second molar(dm), incisior (di) and variation at incisal pin of articulator (a)i: distance in horizontal projection between the condyle and incisor (80mmaverage value)m: distance in horizontal projection between the condyle and second molar(42mm average value)t: distance in horizontal projection between the condyle and incisal table(125mm on SAM Ariculator)a¼ (di � t)/i a¼ (dm � t)/m
Fig. 8: Rule of “the thirds”: for a same vertical variation, molar height,incisal and anterior pin are proportional. The “rule of third” stated that for3mm increase at incisal pin. We obtain a 2mm increase on incisors and1mm increase on molars
position paper
J. Stomat. Occ. Med. � Springer-Verlag Vertical dimension of occlusion: the keys to decision 3/2009 151
Using “wheezing whistling (sibilant) sound or “S”would be the most reliable method, provided that thepatient is wearing the prosthesis approximately 1 week(at least 1 day).
If the patient has phonetic difficulties after 4 weeks, anequilibration is indicated by placing amarker on themaxillaryteeth, whilst the patient articulates “66” “[23]”, or pronouncesounds such as S, Che, Z and F [2].
But the above-mentioned tests are meaningless, incase the anterior dental arrangement is disturbed! Thus,these phonetic tests are only “a posteriori” verification, i.e.after the fitting of provisional dental elements truly infunction.
Changes in VDO could affect TMJ
Strict variationofVDOcauses amandibular rotationaround thehinge axis. This rotational condylar movement is completelyphysiological and induces a very limited intra-capsular move-ment:Anincreaseby1mmonthe incisors levelcausesacondylerotation of approximately 1, which is equivalent to a shift of thecondylo-disc interfaceof0.1mm.So,withhealthyTMJ, increaseor decrease in VDO will not cause any joint changes.
A
B
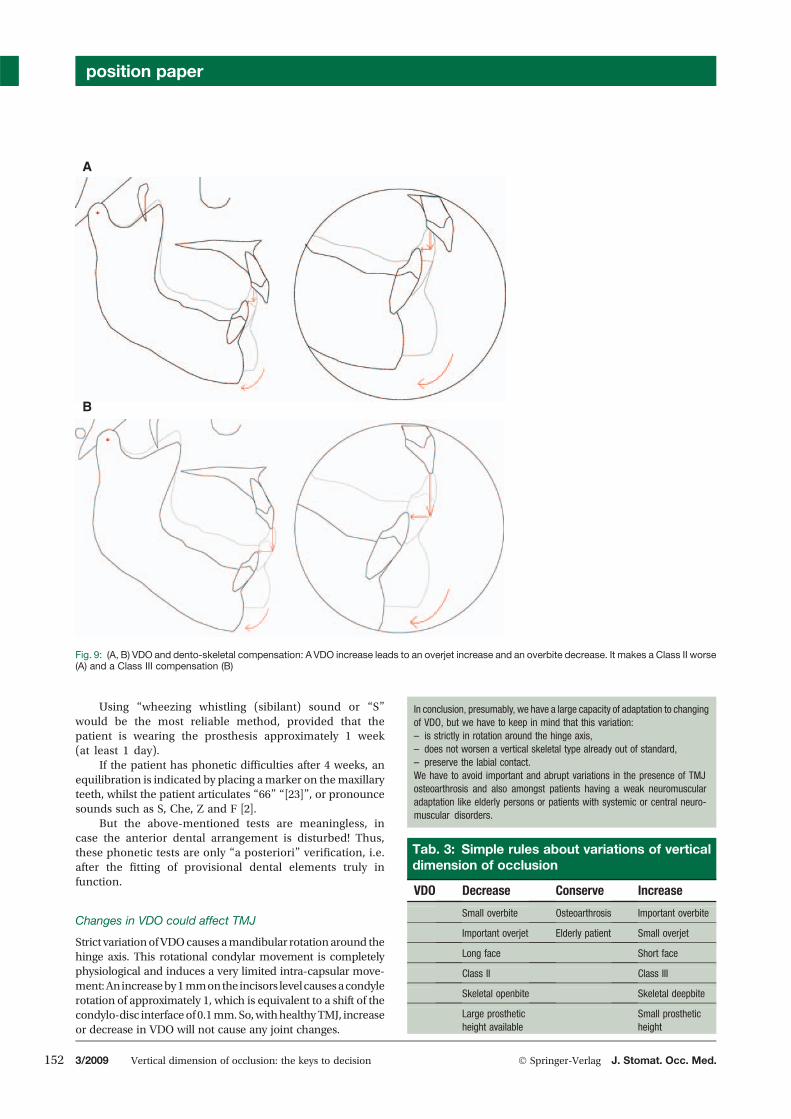
Fig. 9: (A, B) VDO and dento-skeletal compensation: AVDO increase leads to an overjet increase and an overbite decrease. It makes a Class II worse(A) and a Class III compensation (B)
In conclusion, presumably, we have a large capacity of adaptation to changingof VDO, but we have to keep in mind that this variation:– is strictly in rotation around the hinge axis,– does not worsen a vertical skeletal type already out of standard,– preserve the labial contact.We have to avoid important and abrupt variations in the presence of TMJosteoarthrosis and also amongst patients having a weak neuromuscularadaptation like elderly persons or patients with systemic or central neuro-muscular disorders.
Tab. 3: Simple rules about variations of verticaldimension of occlusion
VDO Decrease Conserve Increase
Small overbite Osteoarthrosis Important overbite
Important overjet Elderly patient Small overjet
Long face Short face
Class II Class III
Skeletal openbite Skeletal deepbite
Large prostheticheight available
Small prostheticheight
position paper
152 3/2009 Vertical dimension of occlusion: the keys to decision � Springer-Verlag J. Stomat. Occ. Med.
Only in the case of severe TMJ osteoarthrosis(flat condyle), a variation of the VDO (greater than 3mmon incisor) could cause a situation of constraint in theTMJ [22].
Vertical dimension of occlusion: the decision’scriteria
The classical presence of an inter-occlusal space in restingposture and the lack of contact between the dental arches
A
C
F
I
HG
D E
B
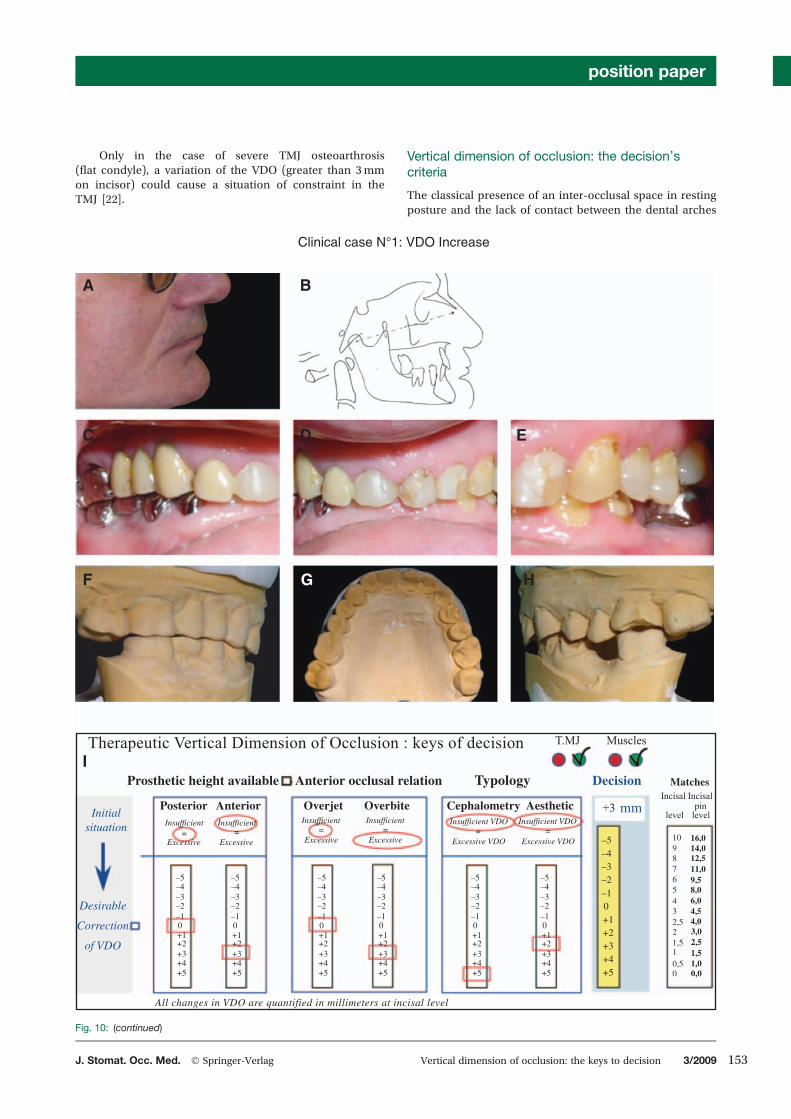
Clinical case N°1: VDO Increase
Therapeutic Vertical Dimension of Occlusion : keys of decision
Prosthetic height available
PosteriorInsufficient
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5
1098765432,5
1,5
0,5
2
1
0 0,01,01,52,53,04,04,56,08,09,511,012,514,016,0
–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
Initialsituation
Desirable
Correction
of VDO
= = = = = =Excessive
All changes in VDO are quantified in millimeters at incisal level
Excessive Excessive Excessive Excessive VDO Excessive VDO
Insufficient Insufficient Insufficient Insufficient VDO Insufficient VDO
Anterior Overjet Overbite Cephalometry Aesthetic
Anterior occlusal relation Typology MatchesIncisal
level level
Incisalpin
Decision
mm
T.MJ Muscles
+3
Fig. 10: (continued)
position paper
J. Stomat. Occ. Med. � Springer-Verlag Vertical dimension of occlusion: the keys to decision 3/2009 153

during phonation are indicators for a VDO treatment.But, it seems, that they are usually acquired by spontane-ous adaptation of the patient. These muscular referencesappear too much unreliable. From our actual opinion,the objective criteria, which will influence really our deci-sion, are:
. Prosthetic height available
. Anterior occlusal relation: Overjet and overbite.
After this two essential criteria’s, we have to control in thenext step, if they are in harmony with:
. Skeletal typology and morphology of the mandible
. TMJ and neuromuscular coordination
. Aesthetic and facial heights.
Prosthetic height available
Retention is a mechanical factor influencing directly theprognosis of our fixed restorations, it is therefore impera-tive. We can consider that the height of an abutment forcrowns should be greater than 4mm. By contrast, crownheight does not exceed the height of the root anchorage.The crown height is also depending from the occlusalplane.
Finally, once VDO and occlusion plan are designed, theprosthetic height available can be increased at the expense ofthe periodontium by surgical coronary elongation.
The choice will be between sufficient retention andfavourable crown-root ratio.
To facilitate the analysis, we have to discern the posteriorprosthetic height and the anterior prosthetic height.
The graduated anterior pin of articulator allows thenecessary quantitative assessment, taking into accountthe variations related to the proportional variation angle of
themandible. This calculation is generally allowed by the ruleof thirds, or by trigonometric calculation.
Overjet and overbite
Overbite is an average of 3–4mm and overjet average is2–3mm in the current populations [12]. Obtaining or main-taining functional anterior contact and anterior cinematiccontrol is one of the main objectives of the prosthetic treat-ment. Changes in the VDOdirectly influence occlusal anteriorrelations, so the anterior objectiveswill dominate the choice ofVDO.
Increase VDOreduces anterior overbite and increases theoverjet. So we could use an increase of the VDO in case ofexcessive overbite or insufficient overjet.
Conversely a decrease VDO leads to an increase of theoverbite and to a decrease of the overjet. So, it is interesting todecrease VDO in case of excessive overjet or insufficientoverbite.
Skeletal typology and mandibular morphology
Classical cephalometric analysis can identify skeletal verti-cal type of patient (hyper-, hypo- or normo-divergent) andthe sagittal skeletal type (skeletal Class I, II or III). It seemslogical that VDO generated by the therapeutic treatmentdoes not worse a dysgnathy. But tends rather to compen-sate it [1].
By the way of the mandibular rotation around the con-dyles, an increase in VDO aggravates skeletal class II andcompensates skeletal Class III. In contrast, a decrease of VDOaggravates skeletal class III and compensates some Class IIskeletal.
J K L
M N
Fig. 10: (A) Extra oral view. (B) Initial Sagittal telepradiography. (C–E) Initial ICP views. (F–H) Initial casts in centric relation. (I) Decision algorithm. Thepatient does not present a gum smile; surgical coronorary elongation is not considered. DECISION: VDO needs a 3mm increase, in order to obtaina sufficient anterior prosthetic height. VDO increase value is limited here by excessive overjet and posterior prothetic height. (J) Corrected VDO oncephalometry. (K, L) Wax-up. (M) Temporary teeth. (N) Final prosthesis
position paper
154 3/2009 Vertical dimension of occlusion: the keys to decision � Springer-Verlag J. Stomat. Occ. Med.
Edwards showed the great variability generated by usingas a reference for simple angle average of the angle AnteriorNasal Spine point-Xi point-suprapogonion point (ANS-Xi-pm) [5].
In addition, a statistical study on 450 sagittal cephalo-grams showed correlations between the height of the lowerfacial height and mandibular morphology measured by thegonial angle and mandibular arch angle. A correlation table
D
H
G
E F
Therapeutic Vertical Dimension of Occlusion : keys of decision T.MJ Muscles
Prosthetic height available Anterior occlusal relation Typology MatchesIncisal Incisal
Decision
Posterior Anterior Overjet Overbite Cephalometry AestheticInitial
situation
Desirable
Correction
of VDO
Insufficient=
Excessive
Insufficient=
Excessive
Insufficient=
Excessive
Insufficient=
Excessive=
Excessive VDO
Insufficient VDO=
Excessive VDO
Insufficient VDOmm+2
level levelpin
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
1098765432,5
1,5
0,5
2
1
0 0,01,01,52,53,04,04,56,08,09,511,012,514,016,0
All changes in VDO are quantified in millimeters at incisal level
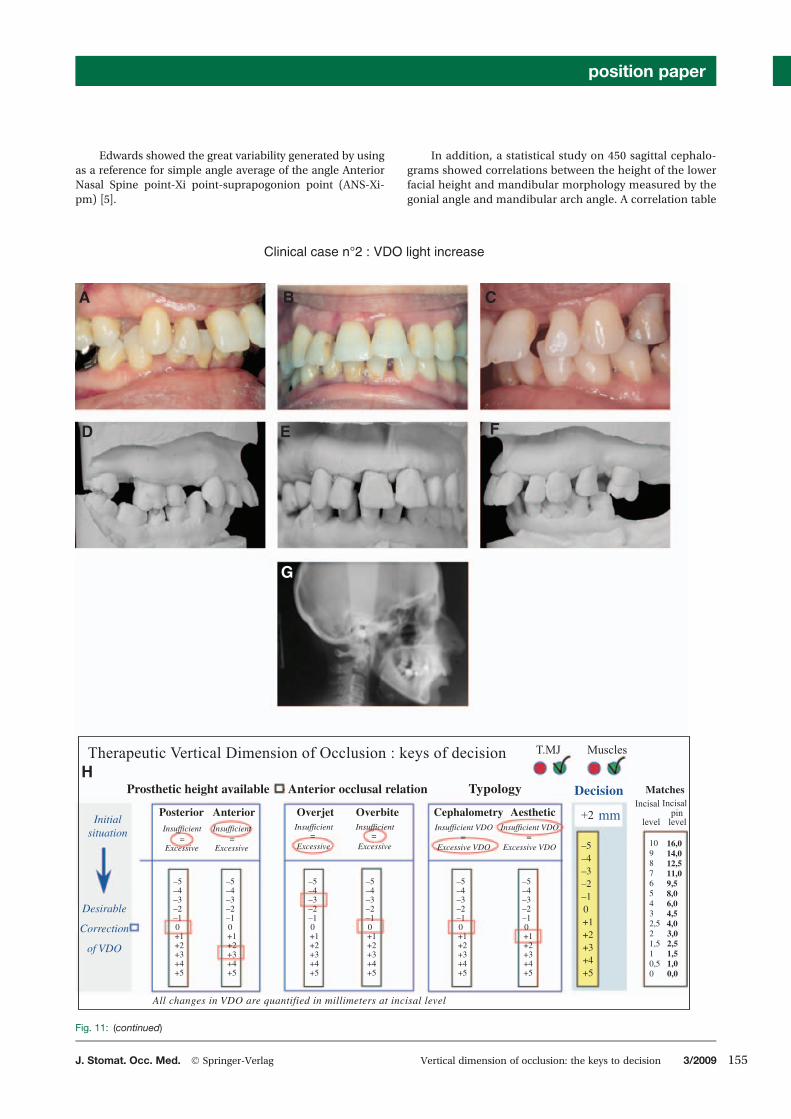
Clinical case n°2 : VDO light increase
A B C
Fig. 11: (continued)
position paper
J. Stomat. Occ. Med. � Springer-Verlag Vertical dimension of occlusion: the keys to decision 3/2009 155
based on measurements of these angles, allows us to offerVDO in harmonywith the bony structures [16]. However, thismore precise approach does not allow us to define the VDOwith a sufficient precision (millimeter) because of the indi-vidual variability. The cephalometric analysis does not giveprecisely the ideal value of VDO. But it shows the direction ofthe treatment.
TMJ and neuro-muscular coordination
A careful clinical examination (intra-auricular palpationshowing difficulties of rotation. auscultation of crepitations)associated with a careful anamnesis and the observation of apanoramic radiography (flat condyle) is used most often todiscern a healthy subject to a TMJ advanced osteoarthrosicphenomena.
In this case, it is advisable to avoid significant abruptvariation of VDOaswell as in patients, suspected to have a lowpotential for neuromuscular adaptation (such as elderlypatient).
In other cases under physiological situation, we will havea green light to changes of VDO as we need from mechanicalor aesthetic point of view.
Aesthetic and facial heights
The therapeutic VDO targets a harmonious facial appearancewith a pleasant appearance of the lower facial height inocclusion.
Except for the subjective visual assessment, anthropo-metric measurements from photography allow quantifica-tion and comparison to previous documents. Ravon [18]following McGee [8] researched measurements of the height
of the lower face in correlation to the distances Glabella-Nasion, Nasion-Gnation, line bi-pupillary-cleft lip, interpupillary. This is to have an approximate value of VDO,which seems more valid than the proportional analysis toovariable as the ratio of Wilie betweenmiddle and lower facialheight [15].
But the impact of a vertical variation of 1 or 2mm is verylow in regards to facial aesthetics, but is very important frommechanical or occlusal aspects.
The rational decision
The practitioner can play with the VDO in the area of adapta-tion according to the biological, mechanical or aestheticspecific requirements.
The study on articulator is irreplaceable to assess directlythe influence of variations of VDO on the posterior and anteriorprosthetic heights available and back, and on the anteriorocclusal relations (overbite and overjet).
The previous decision criteria do not play an equal rolefrom the decision point of view.
Some of them are more determinants.A rational of decision can be proposed in 5 phases:
1 – Anterior and posterior heights available will be evaluatedtaking into account the mechanic requirements (stabilityand resistance).
2 – The importance of creating or maintaining anterior oc-clusal contacts gives a principal role to the value ofanterior overjet and overbite.
3 – Then the skeletal typology and mandibular morphologymust be observed and understood.
I
L
J K
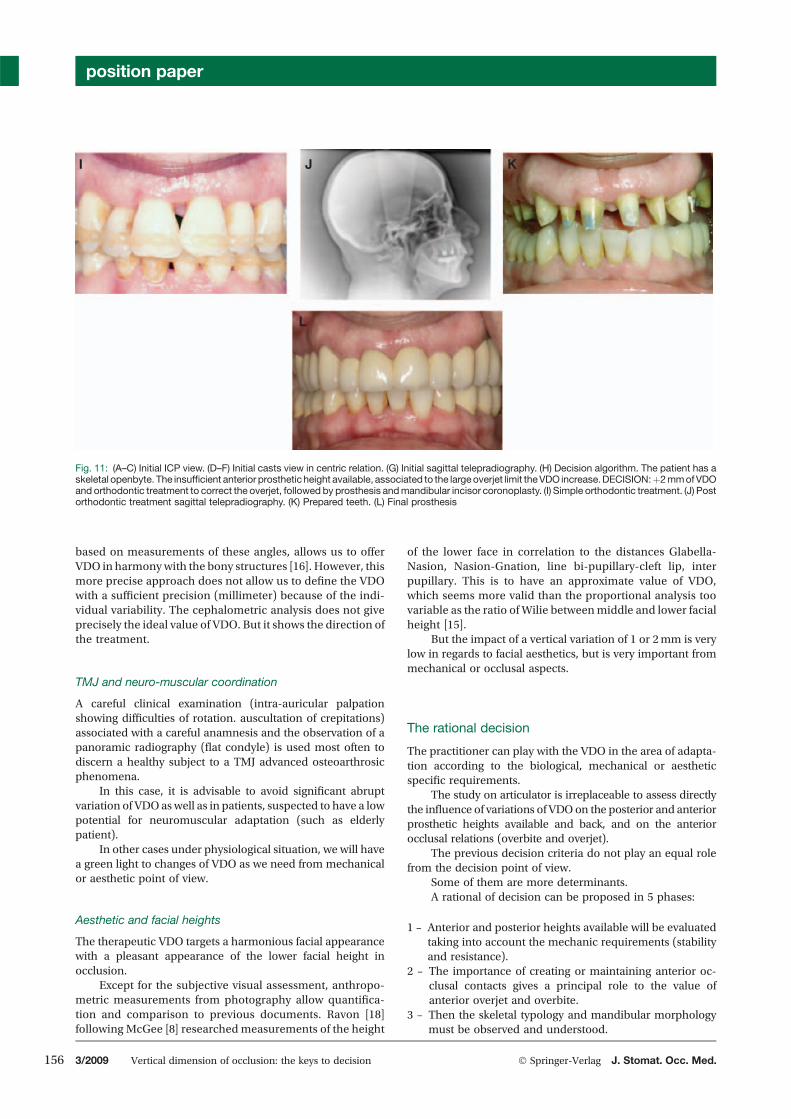
Fig. 11: (A–C) Initial ICP view. (D–F) Initial casts view in centric relation. (G) Initial sagittal telepradiography. (H) Decision algorithm. The patient has askeletal openbyte. The insufficient anterior prosthetic height available, associated to the largeoverjet limit theVDO increase.DECISION:þ2mmofVDOand orthodontic treatment to correct the overjet, followed by prosthesis andmandibular incisor coronoplasty. (I) Simple orthodontic treatment. (J) Postorthodontic treatment sagittal telepradiography. (K) Prepared teeth. (L) Final prosthesis
position paper
156 3/2009 Vertical dimension of occlusion: the keys to decision � Springer-Verlag J. Stomat. Occ. Med.
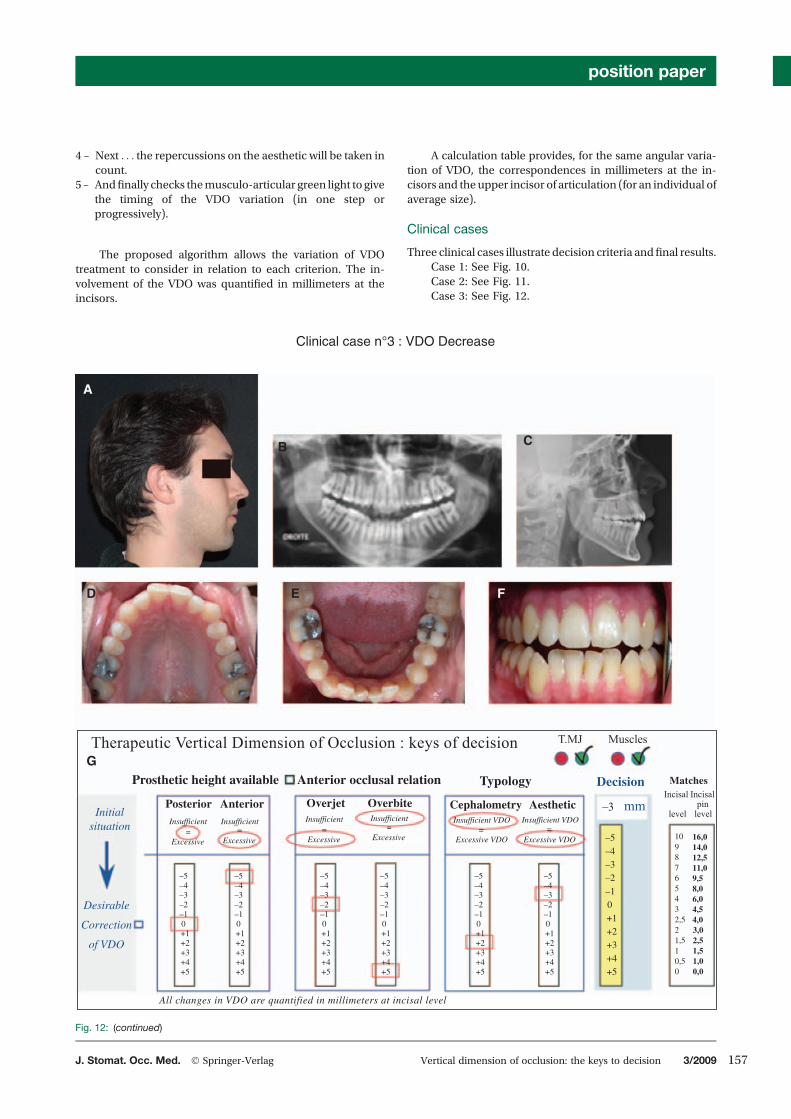
4 – Next . . . the repercussions on the aesthetic will be taken incount.
5 – Andfinally checks themusculo-articular green light to givethe timing of the VDO variation (in one step orprogressively).
The proposed algorithm allows the variation of VDOtreatment to consider in relation to each criterion. The in-volvement of the VDO was quantified in millimeters at theincisors.
A calculation table provides, for the same angular varia-tion of VDO, the correspondences in millimeters at the in-cisors and the upper incisor of articulation (for an individual ofaverage size).
Clinical cases
Three clinical cases illustrate decision criteria andfinal results.Case 1: See Fig. 10.Case 2: See Fig. 11.Case 3: See Fig. 12.
Clinical case n°3 : VDO Decrease
A
B
D
G
E F
C
Therapeutic Vertical Dimension of Occlusion : keys of decision T.MJ Muscles
Prosthetic height available Anterior occlusal relation Typology MatchesDecision
Posterior Anterior Overjet Overbite Cephalometry Aesthetic –3Incisal
level level
IncisalpinmmInitial
situation
Desirable
Correction
of VDO
Insufficient= =
Excessive Excessive
Insufficient Insufficient= =
Excessive Excessive
Insufficient= =
Excessive VDO Excessive VDO
Insufficient VDO Insufficient VDO
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
–5–4–3–2–1
+1+2+3+4+5
0
1098765432,5
1,5
0,5
2
1
0 0,01,01,52,53,04,04,56,08,09,511,012,514,016,0
All changes in VDO are quantified in millimeters at incisal level
Fig. 12: (continued)
position paper
J. Stomat. Occ. Med. � Springer-Verlag Vertical dimension of occlusion: the keys to decision 3/2009 157
Conclusions
Practitioner can play with the VDO but have to be aware of therules, e.g. optimize occlusal relationships earlier, themechan-ical aspects of retention and the crown-root offset, slightlyskeletal types and promote the aesthetic and the potentialbenefits of adaptation, when they exist.
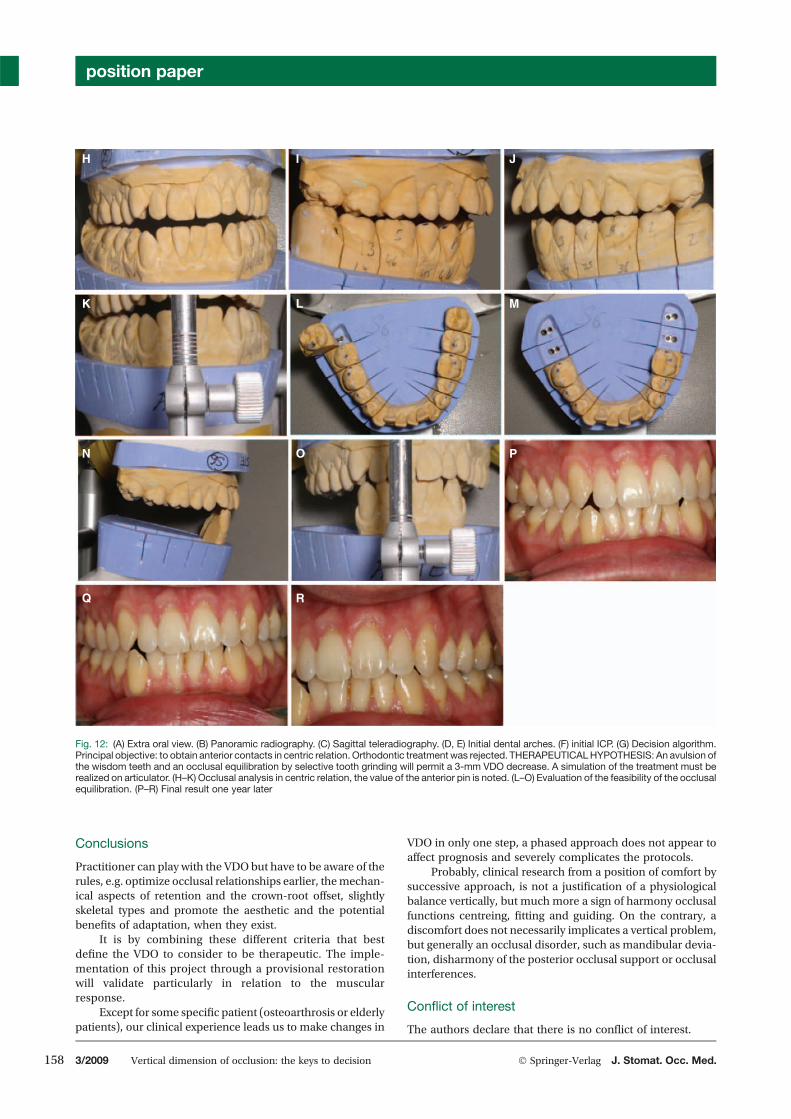
It is by combining these different criteria that bestdefine the VDO to consider to be therapeutic. The imple-mentation of this project through a provisional restorationwill validate particularly in relation to the muscularresponse.
Except for some specific patient (osteoarthrosis or elderlypatients), our clinical experience leads us to make changes in
VDO in only one step, a phased approach does not appear toaffect prognosis and severely complicates the protocols.
Probably, clinical research from a position of comfort bysuccessive approach, is not a justification of a physiologicalbalance vertically, but much more a sign of harmony occlusalfunctions centreing, fitting and guiding. On the contrary, adiscomfort does not necessarily implicates a vertical problem,but generally an occlusal disorder, such as mandibular devia-tion, disharmony of the posterior occlusal support or occlusalinterferences.
Conflict of interest
The authors declare that there is no conflict of interest.
P
I J
K
H
L M
N O
Q R
Fig. 12: (A) Extra oral view. (B) Panoramic radiography. (C) Sagittal teleradiography. (D, E) Initial dental arches. (F) initial ICP. (G) Decision algorithm.Principal objective: to obtain anterior contacts in centric relation. Orthodontic treatmentwas rejected. THERAPEUTICALHYPOTHESIS: An avulsion ofthe wisdom teeth and an occlusal equilibration by selective tooth grinding will permit a 3-mm VDO decrease. A simulation of the treatment must berealized on articulator. (H–K) Occlusal analysis in centric relation, the value of the anterior pin is noted. (L–O) Evaluation of the feasibility of the occlusalequilibration. (P–R) Final result one year later
position paper
158 3/2009 Vertical dimension of occlusion: the keys to decision � Springer-Verlag J. Stomat. Occ. Med.

References
[1] Avril CM. The transfert of the information received by staticmandibular position analysis in the latero-lateral cephalometrictracing. J gnatho 1988;1:105–16.
[2] Berteretche MV, et Hue O. Dimensions verticales. In:Occlusodontie pratique. d’Occlusodontologie CN (ed) Cdp.Paris, 2000;31–40.
[3] Collège National d’Occlusodontologie (CNO). Occlusodontologie:lexique. Quintessence International. Paris, 2001;55.
[4] Dawson PE. Les problèmes de l’occlusion. Evaluation diagnostic ettraitement. Julien Prélat; Paris, 1977.
[5] Edwards CL, Richards MW, Billy EJ, Neilans LC. Using computerisedcephalometrics to analyse the vertical dimension of occlusion. Int JProsthodont 1993;6:371–6.
[6] GaspardM. Troubles de l’occlusiondentaire et SADAM. InCollectiondu chirurgien-Dentiste. Procodif editeur. Sévres, 1985.
[7] Lee RL. Anterior guidance. In: Lundeen HC, Gibbs CH (eds)Advances in occlusion. J Wright Ed Boston 1982;51–79.
[8] MacGee GF. Use of facial measurements in determining verticaldimension. J am Dent Assoc 1947;35:342–7.
[9] Magnusson T. Signs and symptoms of mandibular dysfunction incomplete denture wearers five years after receiving new dentures.Cranio 1985;3:267–72.
[10] McHorris WH. Ajustement Occlusal par meulage sélectif (I). Rev IntParodont Dentist Restaur 1985;5:9–25.
[11] Niswonger ME. Obtaining the vertical relation in edentulouscases that existed prior to extraction. J Am Dent Asssoc 1938;25:1842–7.
[12] Okeson JP. Management of temporomandibular disorders andocclusion. The CV Mosby Cy. St Louis, 1998;637.
[13] Orthlieb J-D. Bezzina S et Preckel EB. OCTA: Concept d’aide au plande traitement en prothèse. Synergie prothétique 2001;3:87–97.
[14] Orthlieb J-D, Laplanche O et Preckel EB. La fonction occlusale et sesdysfonctionnements. Réalités cliniques 1996;7:131–43.
[15] Orthlieb JD. Diagnostic occluso-céphalométrique assisté parordinateur (Occluso-cephalometric computerised diagnosis). InOdontologie. Thesis Université de la Meditérranée; Marseille, 1990.
[16] Orthlieb JD, Laurent M et Laplanche O. Cephalometric estimation ofocclusal vertical dimension. J Oral Rehabilitation 2000;9:802–7.
[17] Palla S. LaDimensionVerticale: Les connaissances et les incertitudes.In La dimension verticale: mythes et limites. Collége Nationald’Occlusodontologie, Paris, 1995;3–12.
[18] Ravon P. Rapports Morphologiques entre les organes dentaires et laface. Etude Statistique. Université de Montpellier, Montpellier, 1986.
[19] Rivera-Morales WC et Mohl ND. Relationship of occlusal verticaldimension to the health of the masticatory system. J Prosthet Dent1991;65:547–3.
[20] Rugh JD et Drago CJ. Vertical dimension: a study of clinical restposition and jaw muscle activity. J Prosth Dent 1981;45:670–5.
[21] Silverman M. Occlusion in prosthodontics and in the naturaldentition. Mutual Publishing Company, Washington, 1962.
[22] Slavicek R, Lucchini V. et Laplanche O. Vingt questions à RudolfSLAVICEK. In: Provence C (ed) CNO Provence Marseille, 1994;62.
[23] Spear FM. Occlusal consideration for complex restorative therapy.In: Mc neill C (ed) Science and practice of occlusion. QuintessencePublishing Co. Inc., Chicago, 1997;437–56.
[24] Tallents RH, Macher DJ, Kyrkanides S, Katzberg RW et Moss ME.Prevalence of missing posterior teeth and intraarticulartemporomandibular disorders. J Prosthet Dent 2002;87:45–50.
[25] Valentin C et Martineau C. La consultation en odontologie. SNPMD,Paris, 1984.
position paper
J. Stomat. Occ. Med. � Springer-Verlag Vertical dimension of occlusion: the keys to decision 3/2009 159





























