Embed Size (px)
Citation preview

y
Analysis of 50 patients with atypical odontalgia A preliminary report on pharmacological procedures for diagnosis and treatment
E. Russell Vickers, MDSc, BDS, a Michael J. Cousins, MD, FANZCA, b Suellen Walker, MBBS, FANZCA, c and Ken Chisholm, MD, FRCPC, d Sydney, Australia, and Halifax, Nova Scotia UNIVERSITY OF SYDNEY, ROYAL NORTH SHORE HOSPITAL, AND VICTORIA GENERAL HOSPITAL
Atypical odontalgia is a distressing and unusual chronic 0rofacial pain condition. It is often difficult to diagnose because it is associated with a lack of clinical and radiographic abnormalities. The condition is poorly understood on a pathophysiological basis, and patients often undergo repetitive and unnecessary dental procedures in attempts to alleviate pain. In this study, 50 patients diagnosed with odontalgia were evaluate d by pharmacological procedures, including topical anesthetic application and phentolamine infusion. Results of these pharmacological procedures suggest that atypical odontalgia is a neuropathic pain of the oral cavity that may have a component of sympathetically maintained pain. Therapeutic trials of topical capsaicin were carried out to assess its efficacy for pain reduction. Topical capsaicin was effective in most patients. (Oral Surg Oral Meal Oral Pathol Oral Radiol Fndod 1998;85:24-32)
Atypical odontalgia (AO) is a chronic pain condition that is poorly understood and inconsistently presented in the literature and for which there is a paucity of information regarding diagnostic, treatment, and man- agement procedures. The purpose of this study was twofold. First, we wanted to analyze patient self-report data to gather more information on epidemiological variables (gender, age, and socioeconomic status), potential causal factors, and pain descriptors. Second, we wanted to evaluate a number of pharmacological interventions designed to aid in the diagnosis and man- agement of AO: applications of a topical anesthetic to intraoral pain sites for the purpose of reducing allody- nia and hyperalgesia (see Table I for definitions of terms); blinded, placebo-controlled sympathetic block- ade (to assess any sympathetic component to AO); and topical capsaicin therapy.
AO was first described as a painful and unusual con- dition that occurs in the dentoalveolar structures and oral mucosa. 1 The pain is moderate to severe in intensi- ty and has a pattem of referral that can cross the midline of the mandible and maxilla and may involve the face. The pain can occur in single or multiple sites, and it can be particularly difficult to diagnose for dental and med-
aOral Surgeon, Pain Management and Research Centre, University of Sydney, Royal North Shore Hospital. bprofessor and Head, Pain Management and Research Centre, University of Sydney, Royal North Shore Hospital. cConsultant Anaesthetist, Pain Management and Research Centre, University of Sydney, Royal North Shore Hospital. dConsultant Anaesthetist, Department of Anaesthesia, Victoria General Hospital, Halif~tx, Nova Scotia. Received for publication Dec. 3, 1996; returned for revision Apr. 7, 1997; accepted for publication May 27, 1997. Copyright © 1998 by Mosby, Inc. 1079-2104/98/$5.00 + 0 7/12/83610
ical practitioners. It has been described as "phantom tooth pain" because of insufficient data for a physiolog- ical explanation of it, and its similarities to phantom limb pain have been noted. 2,3 The differential diagnosis of AO has included cracked tooth syndrome, atypical facial pain, migrainous neuralgia, and sinusitis. The condition occurs infrequently; when it does, dental sur- geons and specialists often confidently try to alleviate it by operative means, only to find that the various (and often numerous) procedures undertaken fail to abolish it. 4 Perhaps the greatest difficulty for the general practi- tioner and the specialist is the absence of clinical and radiographic evidence to establish a diagnosis pertain- ing to organic pathology--an absence suggesting pain of psychological origin. The International Association for the Study of Pain (IASP) has defined AO as a "severe throbbing pain in the tooth without major pathology. ''5
While other chronic orofacial pain conditions, such as temporomandibular disorder (TMD), have had exten- sive documentation, relatively few studies investigating AO have been published. Complicating our understand- ing of AO has been the limited number of patients ana- lyzed: for Rees and Harris 1 in 1979, the sample size was 44; for Marbach 6 (investigating "phantom tooth pain") in 1978, it was 25; for Brooke 7 in 1980, 22; for Kreisberg 8 in 1982, 2; for P611man in 1993, 44. 9 However, most of this published data is epidemiologi- cal; there are few data available for clinicians with respect to diagnostic tests and treatment modalities. The cause of AO has been linked with vascular changes to local tissues 1 and to psychological factors. 1,1° The accepted treatment has usually included long-term anti- depressant therapy, although not all sufferers respond with a reduction in pain. Thermographic studies u,12
24

ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Volume 85, Number 1
and other clinical trials 13 suggest that AO is a neuro- pathiC pain condition of the oral cavity, and this sug- gestion is endorsed by the compelling arguments of Marbach, 2,3 an experienced clinician in the field of AO.
A clinical characteristic of AO has been the variable pain reduction response from local anesthetic blocks; there were, for example, instances of complete, partial, and no relief in a limited study of 13 patients) 4 Adding to the confusion of this clinical feature, there have been anecdotal reports with conflicting views on pain relief from somatosensory blockade) ,15 An investigation of this potentially important diagnostic characteristic was thus warranted, and for this study, the first stage of sequential analgesic blockade was assessed. This stage consisted of an application of a topical anesthetic cream, EMLA, to the peripheral pain sites. EMLA cream 5% (Astra Pharmaceuticals Pry. Ltd., Sydney, Australia) is a eutectic mixture of lidocaine and prilo- caine bases, and tile agent has been shown to have rapid oral mucosal absorption and to penetrate deep into the oral tissues. 16,17
Studies using thermography u,12 and stellate ganglion block 18 have implicated sympathetically maintained pain (SMP) as playing a role in AO. Stellate ganglion block has been used as a diagnostic test for SMP in head, neck, and upper limb. 19 However, the limitations of stellate block include false-positive responses (because of spread of the local anesthetic to somatic fibers), false-negative responses (because of incorrect placement of the local anesthetic), and an inability to allow for blinded, placebo-controlled injections. 2° More recently, intravenous administration of phentolamine (an t~-i and ct-2 adrenoceptor antagonist) has been used as a diagnostic test for SMP, and a positive response (pain relief) may be predictive of the success of subse- quent sympathetic blocks. 2L22 In addition, the phento- lamine test has the advantages of being less invasive, less painful, and capable of allowing for the administra- tion of blinded, placebo-controlled infusions.
Early evidence-based treatment of AO used long4erm tricyclic antidepressant medication with adjunct psy- chological interventions. 1 More recently, Epstein 13 assessed the efficacy of topical applications of capsaicin in treating oral neuropathic pain and had promising results. Capsaicin (8-methyl-N-vanillyl-6-noneamide) is derived from capsicum fruit (cayenne pepper) and has recently elicited interest among pain researchers. As far as medical applications are concerned, its principal role has been in the treatment of dermal lesions from post- herpetic neuralgia in humans. 23 It has both algesic and analgesic properties, and topical application of the sub- stance reduces inflammation by depleting potent algogens (pain-producing agents) such as bradykinin
Vickers et al. 25
Table I. Glossary of terms
AO AO-TMD
CGRP CRPS EMLA IASP SMP TMD allodynia hyperalgesia neuropathy
Atypical odontalgia Atypical odontalgia with secondary temporomandibu-
lax disorder Calcitonin gene-related pepfide Complex regional pain syndrome Eutectic mixture of local anesthetics International Association for the Study of Pain Sympathetically maintained pain Temporomandibulax disorder pain from stimulus that does not usually cause pain increased response to a painful stimuli nerve pathology (nerve sprouting, demyelination)
and histamine. 24 Capsaicin causes a reduction in unmyelinated capsaicin-sensitive fibers (fibers imbued with substance P or with calcitonin gene-related peptide [CGRP]), 25 which are restricted to afferent neurons (C and At-fibers).26
METHODS Patients complaining of chronic orofacial pain were
referred by dental and medical practitioners to the authors' institution, a multidisciplinary pain center (the University of Sydney's Pain Management and Research Centre, at the Royal North Shore Hospital in Sydney).
Pain questionnaire and multidisciplinary pain center assessment
Each subject completed a comprehensive pain ques- tionnaire that included a section for demographic and socioeconomic data, a section for data on pain variables (Visual Analogue Scale [VAS] scores, McGill Pain Questionnaire descriptors, 27 and temporal qualities), and a section specifically for evaluation of TMD. Each patient was diagnosed by the pain center oral surgeon (E.R.V.), in collaboration with other pain center person- nel (anesthetist/pain specialist, psychologist, psychia- trist, physiotherapist). A diagnosis of AO was based on the general criteria previously reported. 3a4
Topical application of EMLA EMLA cream 5%, on a cotton bud, was liberally
applied to the mucosal or gingival tissues where the patient complained of intraoral pain. The test site was wiped free of excess saliva before the placement of EMLA, with the agent well localized for a standardized 5-minute application time. The patient was asked to indicate the degree of reduction in pain intensity, expressing it as a percent of the baseline pain level (before the EMLA application). Where a patient had multiple sites of pain, EMLA was placed on the origi- nal site of pain only.

26 Vickers et aL ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY January 1998
Sympathetic blockade Twelve patients were randomly selected throughout
the study to undergo patient-blinded, placebo-con- trolled sympathetic blockade by phentolamine infusion. Patients were monitored with electrocardiograph, pulse oximetry, and noninvasive blood pressure measure- ments. Initially, 500 ml of intravenous normal saline (0.9%) was administered to limit potential hypotension from phentolamine. VAS scores were recorded at base- line and at 5-minute intervals. The trial involved a placebo infusion of saline over 10 minutes, followed by 15 mg of phentolamine over 10 minutes. If no analgesic response was reported by the patient, and if cardiovas- cular side effects (tachycardia and hypotension) were minimal, further 5-mg bolus doses of phentolamine were administered until a response (pain relief or side effects) was seen.
Treatment efficacy of topical capsaicin Patients were instructed to complete a diagnostic trial
of capsaicin 0.025% (Capsig, Sigma Co., Clayton, Australia), applied topically for 4 weeks. The procedure of the trial involved the application of a proprietary top- ical anesthetic mouthwash (benzocaine 15%, ametho- caine 1.7%) for 3 minutes before capsaicin placement to achieve a pain-free application of the agent. Capsaicin was applied for 3 minutes every morning and every evening for 4 weeks. Cases were reviewed, and changes in pain intensity (in terms of VAS) from the 4-week trial were reported. Long-term pain relief was recorded at least 3 months after the trial was completed to minimize any pain reduction by placebo effect.
Statistical analyses A chi-squared test with Yates correction factor was
used to assess any significant change in pain reduction from the EMLA application, the phentolamine infusion, and the 4-week trial of capsaicin. Student's t test was used to assess any significant difference between the pain ratings from the 4-week trial of capsaicin and the pain ratings at long-term review.
RESULTS Over a 3-year period (from 1992 to 1995), 50 patients
(34 females and 16 males), with an age range of 21 to 82 years (mean = 51 _ 15 years [SD]), were diagnosed with AO among the pain center population. Most of the referrals were from dental practitioners (n = 37), with 13 patients referred by their medical practitioners.
Demographic data showed that 33 of the 50 subjects had been born in Australia, 12 in Europe, 3 in Asia, and 2 in Africa. Forty-eight of the subjects were Caucasian; the other two were Oriental. Most of the people in the
group (n = 49) were married (n = 33); the rest were sep- arated or divorced (n = 6), single (n = 6), or widowed (n = 4). Forty patients lived with their families, two patients lived with friends, and eight patients lived alone. The breakdown for occupational status was as follows: employment, 22; domestic duties, 16, pension, 10; unemployed, 2. Twenty-nine patients claimed that their pain had significantly affected their work perfor- mance or social life, and 17 patients reported that it had had little or no effect. Most of patients were non-smok- ers (n = 38), and 10 of the 50 consumed alcohol on a daily basis.
The duration of pain experienced in the group ranged from 3 months to 32 years (mean = 4.9 +_ 6.7 years [SD]). The causes of pain for the group (n = 50) were reported as follows: after dental treatment, 37; after dental infection, 3; because of dental trauma, 1; and of idiopathic onset, 9. When the patients were asked to complete a statement concerning the intensity of their pain (mild, medium, or severe), most of them reported it as severe (n = 23), with 16 patients reporting medium levels of pain and 5 indicating that their pain was mild. A 10-cm VAS completed by patients (n = 45), with "no pain" anchored at the 0-cm end and "worst pain imag- inable" at the 10-cm end, showed a range of pain scores from 3 to 10 (mean = 7 _+ 2 [SD]), with five patients claiming that theirs was the "worst pain imaginable." On a 3-point scale assessing the temporal quality (con- stant, periodic, or transient) of their pain, 40 patients indicated constant pain and 10 patients reported period- ic pain.
According to data provided by the patients, the num- ber of practitioners (medical specialists, dental special- ists, and other health practitioners) consulted before referral and specifically for orofacial pain ranged from 1 to 17 (mean = 5 -+ 3 [SD]). Of 43 respondents, 60% indicated that cure of their condition was "uncertain" (n = 17), "unlikely" (n = 8), or "impossible" (n = 1). The questionnaire showed 66% of the patients reporting "stress" concurrent with the pain (27 of 41), with the stress predominantly due to family, financial, work, bereavement, health, or pain-related factors.
Clinical examination showed that 15 of the patients were suffering solely from AO, while 35 had AO with an accompanying temporomandibular disorder (TMD). The large majority of AO patients with an associated TMD (patients with AO-TMD) claimed that TMD signs and symptoms occurred after the onset of intraoral pain (from AO).
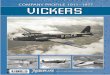
Results of the 5-minute diagnostic trials of EMLA application to the area of intraoral pain (n = 38) showed a significant reduction in pain, ranging from 0% to 100% (mean = 60 _+ 29 [SD]; p < 0.0001) (Fig. 1). Results of the phentolamine infusion to assess a sympa-

ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Volume 85, Number I
100 ® ~ ® o 100 -
Vickers et aI. 27
e- o
-1
e -
80
60
40
20
® Q ®
® © @ ® ® ®
®
Q
©
O
0
I I I I I I I I
0 5 10 15 20 25 30 35
patient study number
Fig. l. Percentage of pain reduction from a 5-minute appli- cation of EMLA 5% topical anesthetic cream to pain site (n = 38). Results of the diagnostic trial of EMLA showed a sig- nificant reduction in pain ranging from 0-100% (mean = 60 _+ 29 SD; p < 0.0001). Only one patient reported no dis- cernible change in pain intensity from application of the top- ical anesthetic agent.
thetic component (n = 12) showed a significant reduc- tion in pain, ranging from 0% to 80% (mean = 31 +_ 27 [SD]; p < 0.02), with no noticeable pain reduction from the saline infusions (Fig. 2). Results of the 4-week trial of 0.025% capsaicin (n = 30) also showed significant pain reduction: 11 subjects claimed no benefit (nil pain reduction), but 19 subjects responded positively, with the reduction in pain ranging from 10% to 100% (mean = 58 + 25 [SD]; p < 0.01). At long-term follow-up (mean = 13 months), there was no significant change in pain compared with results from the 4-week capsaicin trial; the positive responders had maintained a mean pain reduction of 50% (_+ 34 [SD]; p = 0.25). Table II gives the individual patient response for each diagnos- tic trial.
DISCUSSION Data analysis showed that AO did not have an
increased prevalence in any particular target group with respect to ethnic origin or socioeconomic status. The condition was seen to occur over the adult age range. Younger age groups (children and teenagers) were not seen to suffer from the condition--unlike TMD, which can be more frequent in these groups. P611mann 9 reported a correlation between age and duration of "phantom sensations" of the oral cavity; however, no
C 0
C
80
60
40
20
I I I I I I I I I I I t I
0 1 2 3 4 5 6 7 8 9 10 11 12
patient study number
Fig. 2. Percentage of pain reduction from phentolamine infu- sion assessing sympathetic contribution (n = 12) showed a significant reduction in pain ranging from 0-80% (mean = 31 +_ 27 SD; p < 0.02).
correlation was noted in our study. A greater percentage of patients were female, although no clear reason was evident; similar gender differences have been reported in other chronic orofacial pain studies. 28,29 Results showed that most of the patients experienced "constant" and "severe" pain. Several patients claimed to have con- sidered (and one claimed to have attempted) suicide as an option to end their pain, which underlies the serious nature of this condition. Two disturbing findings in this study were the mean pain duration and the number of practitioners consulted before referral to the pain center. Many patients were relieved when informed that their pain had been diagnosed, despite being advised that there were few controlled studies indicating successful outcomes from definitive treatment. Indeed, several patients had complained that referring practitioners had alluded to the patients' pain as "imaginary," based on the lack of any abnormalities in their clinical and radi- ographic examinations. Clearly, lack of knowledge about AO, complicated by scant understanding of chronic pain pathophysiology, resulted in lengthy delays before pain center referral by the patients' respective dental practitioners (and specialists). The authors found that AO, far from being a rare condition, is relatively frequently encountered, as previously sug- gested; patients diagnosed with AO comprised 25% of the chronic orofacial pain group that was referred to the pain center. 4,30

28 Vickers et aL ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY January 1998
Table II. Summary of pain data for each patient (n = 50)
EMLA trial* Phentolamine Capsaicin Capsaicin Gender Age (yr) Duration (yr) Sites of pain Diagnosis pain reduction (%) infusion trialf review (too)
Female 57 5 33-43 AO-TMD 20 0,(8) Male 66 4 35-37 AO 75 100 50,(24) Female 55 5 All quadrants AO-TMD 0 0 NA Female 75 7.5 All quadrants AO 50 NA Female 60 1 13-28 AO 50 50,(4) Male 23 3 28,37-8 AO-TMD 100 0 0 Female 41 0.8 Right quadrants AO-TMD 40 80 90,(20) Female 38 0.8 26 AO-TMD 80 NA Female 53 30 34,23-26 AO-TMD 50 NA Male 49 4 14-22 AO-TMD 50 NA Female 29 1 27-28 AO 20 NA Female 46 0.8 37-38 AO 100 20 0 0 Male 52 3.5 All quadrants AO-TMD i00 NA Female 54 8 16,44 AO-TMD 30 30 50 0,(12) Male 32 0.5 17-18,28 AO-TMD 100 10 ** Male 46 1.5 15-16 AO-TMD 50 20 * * Female 37 6 28,37-38 AO-TMD 100 20 NA Female 76 7 24-26,35-6 AO 80 0 70 100,(4) Female 45 1.5 All quadrants AO-TMD NA Female 57 32 12 AO-TMD 75 25 15,(3) Female 64 2 35-36 AO-TMD 50 50 0 0 Female 41 3 21-28 AO 50 50 50,(3) Female 62 2 11 - 13 AO 10 0 0 Female 50 4 12 AO 100 0 0 Male 21 0.8 48 AO-TMD 0 0 Male 54 10 16-8,45-8 AO-TMD 100 N A Female 45 2 41-38 AO-TMD 20 20 (<3)* Female 82 1.5 34 AO 100 80,(6) Female 46 0.8 26 AO-TMD 10 NA Female 77 3 15-16 AO 75 66 25 0,(6) Male 66 1 13-23 AO-TMD 80 80 30 30,(12) Female 33 3 All molars AO-TMD 60 100,(6) Male 63 11 14-5,44-8 AO-TMD 75 NA Male 66 0.3 32 AO-TMD 50 50 75 ,(30) Female 44 1.3 24-8,38 AO-TMD 75 NA Male 73 1.4 18-28 AO-TMD 60 30,(3) Female 57 16 45-7 AO-TMD 60 0 0 Female 30 0.6 46 AO-TMD NA Female 62 10 All quadrants AO-TMD 50 50 25,(24) Male 53 2 44-46 AO 50 NA Female 60 2 38,48 AO-TMD 50 95 50,(24) Female 46 0.9 14-6,24-6 AO-TMD 50 50 NA Male 39 3 16 AO-TMD 0 NA Female 61 5 13-23,33-43 AO-TMD 50 80 50,(3) Male 27 0.3 23 AO 50 ** Male 25 0.2 16-8 AO 50 50,(12) Female 45 4 16-7,25-7 AO-TMD 75 NA Female 50 3 16 AO 20 50 95,(36) Female 58 10 32-42 AO-TMD 50 NA Female 51 20 23-8,34-8 AO-TMD 90 10 NA
AO, Atypical odontalgia (single condition); AO-TMD, AO with secondary temporomandibular disorder; NA, capsaicin not available from manufacturer (discontinued); LE patient lost to follow-up. *5-minute application to pain site t4-week trial (topical capsaicin) *No long-term review; less than 3 months
The cause of AO was attributed to dental treatment in a high proportion of patients. The initiating factor in dental treatment varied from the drilling of dentine for a simple restoration to root canal therapy and periodon-
tal scaling. The highly enervated and vascular dental pulp, gingival tissues, and mucosal tissues are frequent- ly subjected to repetitive stimuli--thermal, mechanical, chemical, and biological--that can elicit pain; thus, a

ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Volume 85, Number 1
mechanism for peripheral nerve sensitization is clearly feasible for the development of neuropathic pain. Marbach 2 has provided strong arguments that pulp extirpation serves as the initiating factor for AO through the development of peripheral and central nervous sys- tem lesions. In our study, however, for at least some patients, relatively innocuous dental procedures had resulted in AO--a fact that suggests other, or addition- al, mechanisms. In the presence of nerve injury or chronic inflammation, sensitized C-polymodal nocicep- tots may be activated by norepinephrine31,32; hence, norepinephrine (and epinephrine) in a dental local anes- thetic cartridge may potentially exacerbate pain. This may be relevant in the case of the patients in this study who reported short episodes of higher pain intensity after local anesthetic injection during previous dental treatments. The authors propose that neurogenic or bio- chemical sensitization, with potential exacerbation by pharmacologic agents, may be an additional causal fac- tor in AO. It is likely that the cause of AO is multifacto- rial; pharmacologic, biochemical/neural, environmen- tal, and genetic factors probably all contribute.
This study showed topical capsaicin to have an effi- cacy in pain reduction similar to that reported recently by Epstein and Marcoe 13 in the treatment of "oral neu- ropathic pain". While 37% of our patients received no benefit from capsaicin, 63% had a positive, and fre- quently a substantial, response to the treatment. Review of the positive responders showed that mean pain reduc- tion was maintained, although there was wide individ- ual variation. The reason for this variable response is unclear from the data obtained in our study; however, different underlying pathophysiological mechanisms would most probably be responsible. 33 While peripher- al nervous system effects of topical capsaicin are evi- dent, additional benefit from the agent by axonal trans- port to the central nervous system would be likely. Three patients who came to the center for treatment were being treated with low-dose tricyclic antidepres- sant medication and subsequently underwent concur- rent capsaicin therapy. However, from this initial uncontrolled report, conclusions as to the efficacy of a single therapy, capsaicin or tricyclic, as opposed to a regimen combining them, cannot be drawn at this stage.
A difficulty encountered in assessing capsaicin effica- cy during this study was the ethical requirement to treat the TMD component when it was present. TMD thera- py consisted of intensive physiotherapy (ultrasound mad laser) and extension exercises for the involved muscle groups. Patients were advised to postpone the start of their physiotherapy until after the capsaicin trial, if pos- sible. However, some patients underwent physiotherapy before or during the capsaicin trial, and this limited the accuracy of capsaicin evaluation. It should be noted that
Vickers et al. 29
strictly controlled long-term studies assessing treatment procedures for chronic pain are fraught with difficulty, inasmuch as some patients (and referring doctors) embark on their own treatment protocols during a long- term study. Fortunately, in our study, most patients claimed they could distinguish between the benefit from physiotherapy for TMD (facial/extraoral pain reduction) and the benefit from capsaicin treatment for AO (intraoral pain reduction). Topical capsaicin, which offers itself as a simple and non-invasive technique, should be considered an important therapeutic regimen in the treatment of AO, as long as controlled, blinded studies confirm this preliminary data.
One of the difficulties in diagnosing AO may be attributed to the presence of the secondary TMD; this association has been noted by others in studies of oral neuropathic pain and facial pain. 18 Most of the patients with AO in this study also showed signs and symptoms of TMD, a condition which is generally considered by dental practitioners to be straightforward to diagnose and treat. Without corresponding treatment for AO, lit- tle relief is obtained by patients with AO-TMD, and this would account for the failure of conventional TMD treatment in such cases. Consequently, the problem continues to bewilder the dental practitioner. Nearly all of the patients with AO-TMD stated that the TMD signs and symptoms occurred after the onset of intraoral pain (AO). The appearance of TMD in such a patient could certainly be accounted for by the tooth extractions that were performed in an attempt to alleviate the intraoral pain--pain exacerbated by the patient's inability to tol- erate a denture or occlusal splint because of tissue hyperalgesia of the extraction sites. Often, patients had whole quadrants of teeth that had been decimated by dental treatments (multiple restorations followed by root canal therapy, apicectomies, extractions, and exploration and curettage). This treatment rationale is based on the outdated Cartesian model of pain, accord- ing to which the removal of an area peripheral to a pain site is expected to "amputate" the pain along with the body part. Several patients claimed that "jaw clench- ing" and "grinding my teeth" helped them cope with the constant intraoral pain, Hypothetically, activation of low-threshold mechanoreceptors by bmxism may mod- ulate nociception through gate-control mechanisms; bruxism may thus be a potential pain-coping mecha- nism for AO. However, bruxism results in a worsening of the overall pain state on account of the appearance of secondary myofascial pain. Table III lists the McGill pain descriptors selected by our AO patients (including those with secondary TMD), and Table IV shows the frequency of TMD signs and symptoms present in the AO-TMD group.
Results of the phentolamine infusion (0% to 80%

30 Vickers et al.
Table III. Frequencies of pain word descriptors marked on the MPQ by the combined group of patients (AO, n = 8; AO-TMD, n = 32)*
Sensory descriptor Frequency
Sensory Throbbing 18 Aching 15 Tender 15 Sharp 11 Pulsing 10 Shooting 10 Stabbing 9 Burning 9 Gnawing 8
Other Nagging 16 Tiring 12 Annoying 12 Intense 10 Sickening 9 Exhausting 8 Miserable 8
*MPQ descriptors represent sensory qualifies or other (affective/evaluative/rniscellaneous) qualities. Only descriptors selected by more than 20% of patients are listed in this table.
pain reduction), which was only performed in a limited number of patients, indicated that SMP is a frequent but variable component of AO. Lynch and Elgeneidy 18 recently reported, in their study of oral neuropathic pain, a similar variable pain reduction response of SMP from stellate ganglion block. This provides further evi- dence that either AO is a form of oral neuropathic pain or they are the same condition. 3,12,13,18 SMP is defined as pain that is maintained by sympathetic efferent ener- vation or by circulating catecholamines. Pathophysiology of SMP involves coupling between sympathetic and somatosensory pathways; this cou- pling has been postulated to occur at peripheral noci- ceptors, at the dorsal root ganglion with sprouting of noradrenergic perivascular axons, 34 and at central spinal cord sites. 35 Both direct and indirect methods of excitation of peripheral nociceptors by norepinephrine have been proposed. Some C-polymodal nociceptors have been shown to develop sensitivity to sympathetic stimulation after nerve damage or chronic inflamma- tion 31,32 and may thus be directly stimulated by norepi- nephrine. Alternatively, norepinephrine may act indi- rectly via release of prostaglandins, which in turn
36 37 stimulate the nociceptor. , There is now an increased awareness of the role of the sympathetic nervous system in a variety of neuropathic pain states, such as post-her- petic neuralgia, central nervous system lesions, and "amputation syndromes" (phantom pain syndromes). 2° Histological studies of neural enervation of the orofa- cial region have suggested sympathetic involvement in
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY January 1998
Table IV. Frequencies of signs and symptoms of TMD in patients diagnosed with AO-TMD (n = 30)
Sign~symptom Frequency (%)
Facial/jaw pain 87 Neck pain 70 Bruxism 60 Headaches/earaches 57 Temporomandibular joint pain 50 Clicking of TMJ 50 Difficulty in chewing 47 Facial/masticatory muscle tension 47 Restricted oral opening 43 Tinnitus 37 Teeth chipping/wearing down 37 Dizziness 33 Unpleasant taste 33 Difficulty in breathing through nose 30 Tingling sensation in face 27 Numbness in face 13 Locking of jaw 7
"causalgia". 38-4° In the past, SMP was linked with "reflex sympathetic dystrophy" and "cansalgia," now designated Complex Regional Pain Syndrome (CRPS) Type I and CRPS Type II, respectively. 5 CRPS is a clin- ical diagnosis that may include, but that does not imply, an underlying component of SMP. The main feature of CRPS is pain (with associated allodynia/hyperalgesia) that is disproportionate in severity to the inciting event and that is regionally distributed beyond the territory of a single peripheral nerve. In CRPS there may be associ- ated edema, changes in blood flow, and abnormal sudo- motor activity. Although SMP may be a component of a particular patient's pain syndrome, it is often impossible to predict, on the basis of presenting symptoms alone, whether that patient will benefit from sympatholysis.
Over 82% of our patients experienced pain migration from a single tooth site to multiple sites and widely dif- fuse pain throughout the gingivae and mucosa. The tra- ditional representation of the afferent nervous system depicts "hard wiring," with pain unable to cross anatomic boundaries such as the midline. However, recent data have shown that "peripheral sensitization" is associated with localized or "primary" hyperalgesia and that "central sensitization" is associated with "sec- ondary" hyperalgesia. The latter may spread vertically and may cross the midline, because afferent pathways have the potential to exhibit "plasticity" after peripher- al nerve damage. 41,42 Chronic pain states usually have both peripheral and central nervous system compo- nents. This would explain the partial success in previous trials of tricyclic antidepressants I for the central com- ponent and the similarly partial success in our study of local topical applications of capsaicin for the peripheral

ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY Volume 85, Number 1
component. The peripheral pain component varied markedly from 0% to 100%, based on the results of EMLA application. However, pain reduction from the EMLA application did not necessarily predict the suc- cess of capsalcin treatment. The variable results of the phentolamine test showed that a sympathetic contribu- tion is present in some (but not all) patients, adding to the complexity of AO and suggesting that optimum treatment would require several diagnostic procedures.
Further complicating matters since AO was first reported has been the issue of nomenclature. Originally, the condition was described by some authors as atypical odontalgia, in response to its "atypical" nature; this term was subsequently listed in the Taxonomy of Chronic Pain Syndromes by the IASR 5 Some of the other terms used for AO have been idiopathic odontal- gia, 43 neurovascular odontalgia, 44 phantom tooth pain, 6 and, more recently, oral neuropathic pain. 2,3,13,18 However, for some patients AO could arguably be termed CRPS Type II. Diagnostic criteria for CRPS (Types I and II) include edema, changes in skin blood flow, and abnormal sudomotor activity. While thermo- graphic data may support the classification of AO as CRPS according to some of the criteria, AO does not satisfy other criteria, such as increased sudomotor activ- ity (sweating), and so cannot currently be classified as CRPS in the oral cavity. Researchers who undertake further studies of this condition, particularly practition- ers unfamiliar with AO, may be confused by these changes in terminology, some recent and some not so recent. Clearly, there is a need for consensus among researchers and clinicians as to a suitable term for the designation of AO.
The group of patients with AO that this study ana- lyzed is the largest reported in the literature to date. The study illustrates the complexity of chronic pain, partic- ularly in the orofacial region. Because of our current lack of understanding of AO, further studies in the epi- demiology and causation of this distressing condition are warranted. Judging from this initial uncontrolled report, capsaicin appears to be a promising agent in the treatment of AO; concurrent treatment regimens (such as tricyclic antidepressants) were restricted for most of the patients in this study to provide some measure of control. However, blinded, controlled studies of cap- saicin are still needed to assess its definitive therapeutic effect. The current treatment for other types of neuro- pathic pain, such as phantom-limb pain and post-her- petic neuralgia, includes membrane-stabilizing drugs such as mexiletine and drug combinations of anticon- vulsants and tricyclic antidepressants. 45 Recent pilot data have also indicated the usefulness of mexiletine for treating oral neuropathic pain and the usefulness of the lidocaine infusion as a diagnostic procedure. 46
Vickers et aI. 31
Unfortunately, patient noncompliance due to drug side effects is common, and it reduces the efficacy of these regimens. Future modalities for the treatment of severe neuropathic pain of body and limbs (and possibly of oral neuropathic pain) will probably include spinal cord stimulation and long-term matrix formulations of drugs via intrathecal administration. This study and previous work show AO to have multiple components, including hyperalgesia (primary and secondary), allodynia, SMR and myofascial pain. In addition, psychological factors that are associated with chronic pain, such as depression and "stress" (which affected 66% of the patients in this study), are usually associated with the condition. Associated pain behaviors and variable pain-coping skills further complicate the evaluation of patients and their respective individual responses to treatment. Further studies of AO are warranted, and because of the multifactorial nature of this pain condition, it is highly desirable that a multidisciplinary approach to diagnosis and treatment be taken with patients who are experi- encing it.
REFERENCES 1. Rees RT, Harris M. Atypical odontalgia. Br J Oral Surg 1979;
16:212-8. 2. Marbach JJ. Is phantom tooth pain a deafferentation (neuropath-
ic) syndrome? (part 1): evidence derived from pathophysiology and treatment. Oral Snrg Oral Med Oral Pathol 1993;75:95-105.
3. Marbach JJ. Is phantom tooth pain a deafferentation (neuropath- ic) syndrome? (part 2): psychosocial considerations. Oral Surg Oral Med Oral Pathol 1993;75:225-32.
4. Campbell RL, Parks KW, Dodds RN. Chronic facial pain asso- ciated with endodontic therapy. Oral Surg Oral Med Oral Pathol 1990;69:287-90.
5. Merskey H, Bogduk N, editors. Classification of chronic pain: descriptions of chronic pain syndromes and. definitions of pain terms. Seattle: IASP Press; 1994. p. 53-6.
6. Marbach JJ. Phantom tooth pain. J Endodont 1978;12:362-72. 7. Brooke RI. Atypical odontalgia. Oral Snrg Oral Med Oral Pathol
1980;49:196-9. 8. Kreisberg MK. Atypical odontalgia: differential diagnosis and
treatment. J Am Dent Assoc 1982;104:852-4. 9. P611mann L. Determining factors of the phantom tooth. New
York State Dental Journal 1993;59:42-5. 10. Graff-Radford SB, Solberg WK. Is atypical odontalgia a psy-
chological problem? Oral Surg Oral Med Oral Pathol 1993;75: 579-82.
11. Gratt BM, Sickles EA, Graff-Radford SB, Solberg WK. Electronic thermngraphy in the diagnosis of atypical odontalgia: a pilot study. Oral Surg Oral Med Oral Pathnl 1989;68:472-81.
12. Graff-Radford SB, Ketelaer M-C, Gratt BM, Solberg WK. Thermographic assessment of nenropathic facial pain. J Orofacial Pain 1995;9:138-45.
13. Epstein JB, Marcoe JH. Topical application of capsaicin for treatment of oral neuropathic pain and trigeminal neuralgia. Oral Surg Oral Med Oral Pathol 1994;77:135-40.
14. Bates RE, Stewart CM. Atypical odontalgia: phantom tooth pain. Oral Surg Oral Med Oral Pathol 1991 ;72:479-83.
15. Graff-Radford SB, Solberg WK. Atypical odontalgia. J Craniomandibular Disorders, Oral Facial Pain 1992;6:260-6.
16. Vickers ER, Punnia-Moorthy A. A comparison of the efficacy of three topical anaesthetic agents. Aust Dent J 1992;37:266-70.
17. Vickers ER, Punnia-Moorthy A. Pulpal anesthesia from an

32 Vickers et aL
application of a topical anesthetic. Quintessence International 1993;24:547-51.
18. Lynch ME, Elgeneidy AK. The role of sympathetic activity in neuropathic orofacial pain. J Orofacial Pain 1996; 10:297-305.
19. Bonica JJ. Causalgia and other reflex sympathetic dystrophies. In: Bonica JJ, editor. The management of pain. Pennsylvania: Lea and Febiger; 1990. p. 220-43.
20. Walker SM, Cousins MJ. Complex regional pain syndromes, including "reflex sympathetic dystrophy" and "causalgia." Anaesthesia and Intensive Care 1997;25:113-25.
2I. Amer S. Intravenous phentolamine test: diagnostic and prognos- tic use in reflex sympathetic dystrophy. Pain 1991;46:17-22.
22. Raja SN, Treede R, Davis KD, Campbell JN. Systemic alpha- adrenergic blockade with phentolamine: a diagnostic test for sympathetically maintained pain. Anesthesiology 1991 ;74:691- 8.
23. Stanberry LR, Bourne L, Bravo FJ, Bemstein DI. Capsalcin-sen- sitive peptidergic neurons are involved in the zosteriform spread of herpes simplex virus infection. J Med Virol 1992;38:142-6.
24. Crimi N, Polosa R, Maccarrone C, Palermo B, Palermo F, Mistretta A. Effect of topical application of capsaicin on skin responses to bradykinin and histamine in man. Clin Exp Allergy 1992;22:933-9.
25. Gyorfi A, Fazekas A, Rosivall L. Neurogenic inflammation and the oral mucosa. J Clin Periodontol 1992;19:731-6.
26. Bevan S, Szolcs~inyi J. Sensory neuron-specific actions of cap- saicin: mechanisms and applications. Trends in Pharmacological Sciences 1990;11:330-3.
27. Melzack R. The McGill Pain Questionnaire: major properties and scoring methods. Pain 1975;1:277-99.
28. Gerschman JA, Wright JL, Hall WD, Reade PC, Burrows GD, Holwill BJ. Comparisons of psychological and social factors in patients with chronic oro-facial pain and dental phobic disor- ders. Aust Dent J 1987;32:331-5.
29. Vickers ER, Cousins MJ. Management of chronic orofacial pain. Aust Fam Physician 1994;12:2315-21.
30. Marbach JJ, Hulbrock J, Hohn C, Segal AG. Incidence of phan- tom tooth pain: an atypical facial neuralgia. Oral Surg Oral Med Oral Pathol 1982;53:190-3.
31. Sato J, Perl ER. Adrenergic excitation of cutaneous pain recep- tors induced by peripheral nerve injury. Science 1991 ;251:1608- 10.
32. Sanjue H, Jun Z. Sympathetic facilitation of sustained dis- charges of polymodal nociceptors. Pain 1989;38:85-90.
ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY January 1998
33. Dubner R. Topical capsaicin therapy for neuropathic pain. Pain 1991;47:247-8.
34. McLachlan EM, Janig W, Devor M, Michaelis M. Peripheral nerve injury triggers noradrenergic sprouting within dorsal root ganglia. Nature. 1993;363:543-6.
35. Roberts WJ. A hypothesis on the physiological basis for causal- gia and related pains. Pain 1986;24:297-311.
36. Levine JD, Taiwo YO. Hyperalgesic pain: a review. Anesthesia Progress 1990;37:133-5.
37. Tracey D J, Cunningham JE, Romm MA. Peripheral hyperalge- sia in experimental neuropathy: mediation by c~2-adrenorecep- tors on post-ganglionic sympathetic terminals. Pain 1995;60: 317-27.
38. Gregg JM. In discussion: Comparison of sympathetic neurons in orofacial and upper-extremity nerves: implications for causal- gia). J Oral Maxillofac Surg 1990;48:727.
39. Gregg JM. Studies of traumatic neuralgia in the maxillofacial region: surgical pathology and neural mechanisms. J Oral Maxillofac Surg 1990;48:228-37.
40. Hoffman KD, Mathews MA. Comparison of sympathetic neu- rons in orofacial and upper-extremity nerves: implications for cansalgia. J Oral Maxillofac Surg 1990;48:720-6.
41. Dubner R. Neuronal plasticity and pain following peripheral tis- sue inflammation or nerve injury. In: Bond MR, Charlton JE, Woolf CJ, editors. Pain research and clinical management, Vol 4. New York: Elsevier; 1991. p. 263-76.
42. H6kfelt T, Zhang X, Weisenfeld-HaUin Z. Messenger plasticity in primary sensory neurons following axotomy and its function- al implications. Trends in Neuroscience 1994;17:22-9.
43. Harris M. Psychogenic aspects of facial pain. Br Dent J 1974;136:199-202.
44. Mahan PE, Alling CC, editors. Facial pain. Philadelphia: Lea and Febiger; 1991. p. 304-5.
45. Presley RW, Cousins MJ. Current concepts in chronic pain man- agement. Current Therapeutics 1992;18:51-60.
46. Saxen MA, Adams WR, Splonik KS, Campbell RL. Diagnostic lidocaine infusion in patients with chronic orofacial pain. Anesthesia Progress 1994;41:116-26.
Reprint requests: E. Russell Vickers, MDSc, BDS Department of Anaesthesia and Pain Management Royal North Shore Hospital St. Leonards 2065 NSW