Embed Size (px)
Citation preview

1
Video Elicitation and the Study of Doctor-Patient Interactions:
Poor Acting and Mixed Reviews
Candidate: Rachel Evans
Module Tutor: Professor David Clarke
Module: C83 PAD
Degree: BSc Psychology (International Study),
University of Nottingham
2
Contents
1. Introduction
2. Doctor-Patient Interactions
2.1. The Nature of DPI
2.2. Why Study DPI?
2.3. Approaches to the Study of DPI
3. Video Elicitation
3.1. History
3.2. Principles
3.3. Methodology and Recommendations for those Conducting VE Studies
3.4. Further Considerations for those Using VE to study DPI
3.5. Limitations of the Suggested Approach
3.5.1. context is disregarded.
3.5.2. data quality.
3.5.3. practical issues.
3.5.4. ethical issues.
4. Conclusion
5. References
Abbreviations
DPI= doctor-patient interaction
SDM= shared decision making
VE= video-elicitation
Word count= 3 946

3
1. Introduction
Improving patient satisfaction and health outcomes is understandably a priority for
health care organisations. As medical consultations constitute a large proportion of patient
contact with health care providers, improving the effectiveness of doctor-patient
interactions (DPI) can make a valuable contribution to achieving this aim (Ogden et al.,
2004). However, the DPI is the result of complex interpersonal processes, which can be
understood on multiple levels (Saba et al., 2006). As such, a special Issue of Patient and
Education Counselling (Volume 83, Issue 3, 2011) discusses the need to apply integrative
approaches to enable a deeper understanding of interaction in health care settings. In
keeping, the current paper explores the use of video elicitation ([VE] also termed video-
stimulated-recall) as a method to collect behavioural data (i.e. a video of the DPI) to be
analysed by an observer, as well as subjective reports from participants in the DPI (Henry &
Fetters, 2012). Moreover, although data is collected in a qualitative format it may be
analysed by quantitative methods. These possibilities mean that VE has face validity as a
useful approach for investigating what makes an effective DPI. Nevertheless, caveats to the
application of VE to study DPI are also noted.
2. Doctor Patient Interactions
2.1. The Nature of DPI
For the purposes of this paper DPI will be regarded as face-to-face interactions
between a patient and a single health care provider, be this their local GP, a specialist
doctor (e.g. oncologist), or surgeon etc. In these circumstances there is a mutual influence
between individuals (Melbourne et al., 2011). This may be shown between speech turns, for
example, question-and-answer sequences. Although, cross-contingency may also be shown
over the whole consultation, for example, how the patient’s presentation of their symptoms
influences the questions that the doctor asks to try and determine the diagnosis (Connor,
Fletcher, & Salmon, 2009). Interpersonal processes within DPI are clear from anecdotal
experience (Rao et al., 2010). But stronger evidence from statistical sequence analysis and
micro- analysis of doctor-patient verbal communication confirms the reciprocal nature of
DPI (Bensing, Verheul, Jansen, & Langewitz, 2010; Eide, Quera, Graugaard, & Finset, 2004;
Heritage & Maynard, 2006).
4
However, the medical consultation involves more than verbal communication.
Whilst important functions of the DPI can be achieved by verbal means, such as information
exchange and medical decision making, these processes also involve non-verbal cues and
subjective experiences (Pawlikowska, Zhang, Griffiths, van Dalen, & van der Vleuten, 2012;
Zimmerman, Del Piccolo, & Finset, 2007). This can be seen in research which shows that
patients can experience task-focused behaviour, such as bio-medical information provision
by doctors, as caring and relationship building (Young, Ward, Forsey, Gravenhorst, &
Salmon, 2011). This highlights the inter-subjective nature of DPI and development of the
therapeutic interpersonal relationship between doctors and patient (Radley, 1994).
Moreover, it also demonstrates that behaviour can be multidimensional, with the doctor’s
information giving utterance in the example above serving both instrumental and socio-
emotional functions. The complex nature of DPI, therefore, has implications for how DPI
should be studied.
2.2. Why Study DPI?
It is important to investigate DPI because how these individuals interact can impact
upon the course and outcomes of the medical consultation in a positive or negative manner
(Ong, de Haes, Hoos & Lammes, 1995). For example, unvoiced patient concerns can give rise
to misunderstandings, incorrect diagnoses and poor patient satisfaction (Bensing et al.,
2010). As a result researchers are interested in what constitutes an effective DPI and how
this can be promoted in medical practice. In contrast to the ‘authoritarian doctor’
perspective prominent before the 1990’s (Marks, Murray, Evans, & Estacio, 2011), which
assumed that the doctor held power over the consultation, many researchers and policy
makers now emphasise the importance of ‘patient-centred’ care and ‘shared decision
making’ (SDM; Hall, 2003; Kaba & Sooriakumaran, 2007). This means that doctors should
aim to create a therapeutic relationship with the patient based on mutual trust and patient
involvement in treatment decision making (Mead & Bowers, 2000). However, training
programmes to improve doctor communication and shared decision making have produced
observable improvements in patient-centred behaviours that have not been mirrored in the
views of patients towards the interaction (Davis et al., 2003; Rogers, Kenny, Nelson &
Robinson, 2005). Together with evidence that doctors and patients often have different
5
views of the same interactions (Kenny et al., 2010; Young et al., 2011), this suggests that
further research is necessary to uncover what makes a successful DPI.
2.3. Approaches to the Study of DPI
Research surrounding DPI has differed in its epistemological underpinning (Salmon,
Mendick & Young, 2011). Two distinctions have been made, based on the source of
knowledge and the format of data collected (see Table 1). Firstly, researchers often choose
between self-reports from those involved in the interaction (emic) or an observer’s (etic)
classification of the event (Saba et al., 2006). For example, a post-consultation questionnaire
completed by a patient, versus, analysis of a video-recorded DPI by a researcher. Secondly,
data has been collected in a quantitative (i.e. number-based) or qualitative (i.e. language-
based) format (Neumann, Kreps & Visser, 2011). For example, analysis of a video-recorded
interaction by counting the number of utterances in a coding category, versus, identification
of the main themes within the DPI reported as a written description.
Historically these approaches have been applied independently (Bryman, 2006; Zoppi &
Epstein, 2002). However, this limits the conclusions that can be drawn from the study. It has
already been shown (in sections 2.1. and 2.2.) that self-reports of the DPI from the doctor
and patient do not always agree with each other or with etic classifications (e.g. Kenny et
al., 2010; Saba et al., 2006; Young et al., 2011). Researchers approaching the study of DPI
from only one perspective would, therefore, fail to collect important data, which may have
important theoretical and practical implications. This suggests that multiple data sources
and formats should be used within the same study to generate comprehensive data.
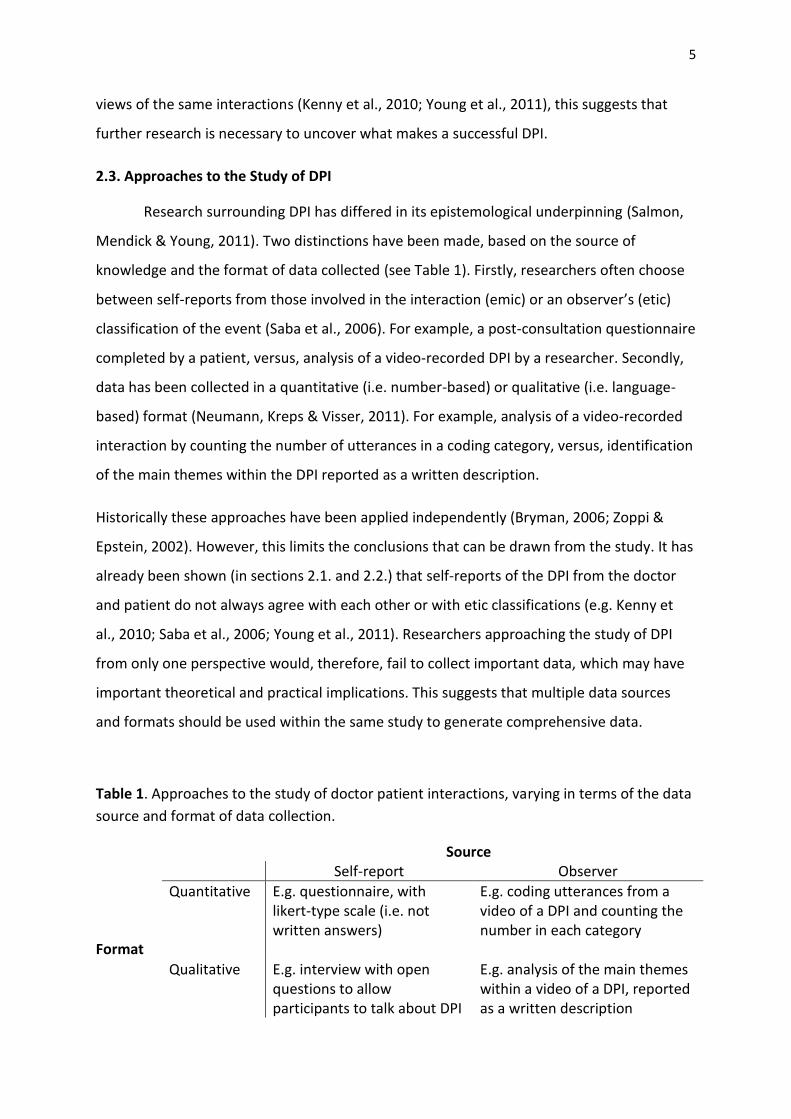
Table 1. Approaches to the study of doctor patient interactions, varying in terms of the data
source and format of data collection.
Source Format
Self-report Observer
Quantitative E.g. questionnaire, with likert-type scale (i.e. not written answers)
E.g. coding utterances from a video of a DPI and counting the number in each category
Qualitative E.g. interview with open questions to allow participants to talk about DPI
E.g. analysis of the main themes within a video of a DPI, reported as a written description
6
3. VIDEO ELICITATION
3.1. History
VE entails the use of a video-recording to stimulate recall, reliving, and reflection on
the recorded interaction by those involved (Henry & Fetters, 2012). The use of VE in
research studies was inspired by the work of Norman Kagan and colleagues on a skill
development programme for therapists, known as the Interpersonal Process Recall Method
(Kagan & Kagan, 1990; Kagan, Schauble, Resnikof, Danish, & Krathwohl, 1969). This
programme makes use of a video-recording of a recent therapy session to aid recall and
stimulate discussion. The therapist, with the help of a supervisor, views the recording and
tries to recall covert thoughts experienced at the time of the interaction. In addition, cues
expressed by the client that indicate they may have unvoiced thoughts are also identified
from the video. This is intended to aid communication and the development of better
therapeutic relationships (Larsen, Flesaker, & Stege, 2008). However, VE procedures have
been adapted by researchers to enable the exploration of participants’ views on the
interaction and other data that is not explicitly captured within the video-recording.
3.2. Principles
Henry and Fetters (2012) highlight that VE studies have traditionally taken a
qualitative approach and adhered to five basic principles (Green and Britten, 1998). Firstly,
data is collected from naturalistic settings (i.e. everyday contexts, such as a doctor’s surgery)
rather than experimental, laboratory based contexts. Secondly, data should be interpreted
with reference to the meaning that participants bring to and take away from the interaction.
Thirdly, studies should focus on the social processes within communication, for example,
how the meaning of symptoms is created by the doctor and patients (Puustinen, 1999).
Fourthly, there is acknowledgement of the reciprocal influence between participants, which
is fundamental in face-to-face interactions. Lastly, researchers take a relativist stance, which
respects the perspectives of all participants involved. Within the context of medical
communication this means that the view of the doctor is not regarded as superior to that of
that patient. The philosophy underlying VE is, therefore, beneficial for the study of DPI as it
is congruent with current formulations of the nature of DPI (see section 2.1).
7
3.3. Methodology and Recommendations for Those Conducting VE Studies
Although aspects of VE methodology are flexible, it necessarily involves video-
recording of participants involved in an interaction, followed by VE-interviews with one or
all of the participants. These interviews are then analysed based on qualitative principles
(explained in section 3.2.). Allowing participants to view the video-recorded interaction
throughout the interview is believed to facilitate recall, producing a more detailed report
than using a standard/ non-stimulated interview (Larsen et al., 2008). However, further
extensions to the basic methodology, including etic analysis of video-recordings, mean that
VE is an appropriate method to explore what makes an effective DPI. These adaptations will
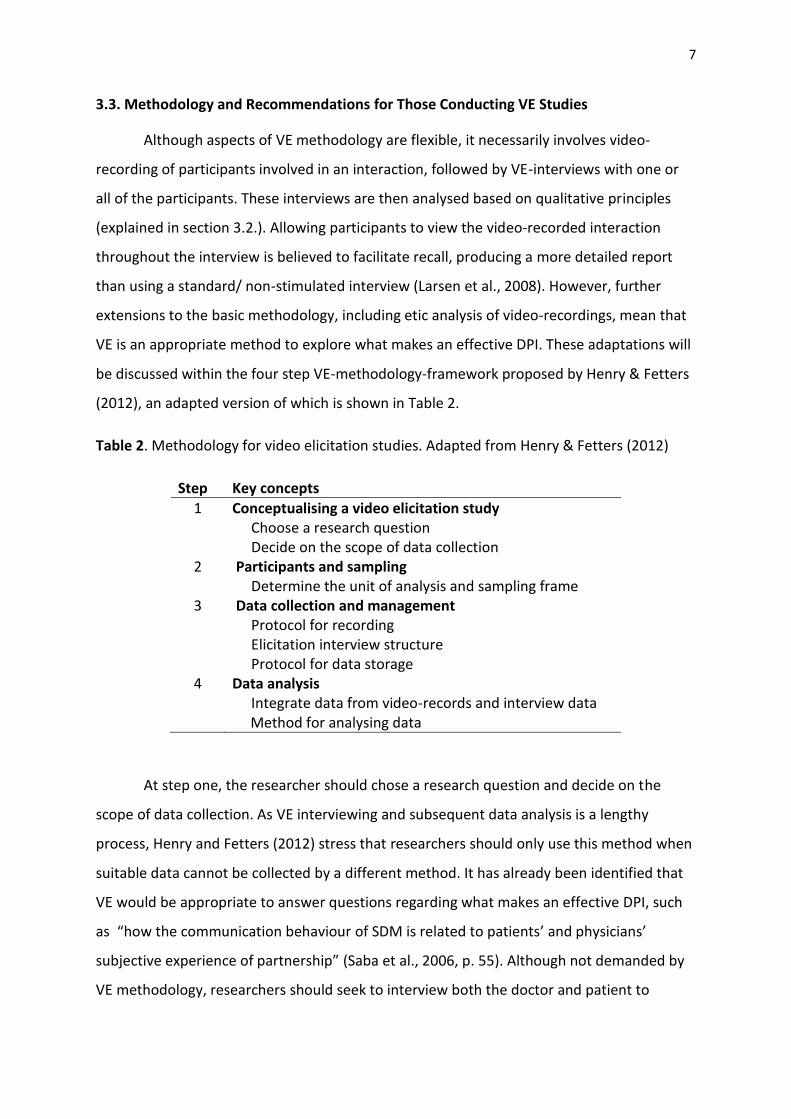
be discussed within the four step VE-methodology-framework proposed by Henry & Fetters
(2012), an adapted version of which is shown in Table 2.
Table 2. Methodology for video elicitation studies. Adapted from Henry & Fetters (2012)
Step Key concepts
1 Conceptualising a video elicitation study Choose a research question Decide on the scope of data collection
2 Participants and sampling Determine the unit of analysis and sampling frame
3 Data collection and management Protocol for recording Elicitation interview structure Protocol for data storage
4 Data analysis Integrate data from video-records and interview data
Method for analysing data
At step one, the researcher should chose a research question and decide on the
scope of data collection. As VE interviewing and subsequent data analysis is a lengthy
process, Henry and Fetters (2012) stress that researchers should only use this method when
suitable data cannot be collected by a different method. It has already been identified that
VE would be appropriate to answer questions regarding what makes an effective DPI, such
as “how the communication behaviour of SDM is related to patients’ and physicians’
subjective experience of partnership” (Saba et al., 2006, p. 55). Although not demanded by
VE methodology, researchers should seek to interview both the doctor and patient to
8
enable subsequent data triangulation. This may be important to highlight instances in which
the doctors’ and patients’ views on the effectiveness of the DPI are discordant.
Step two requires researchers to consider the participants and sampling frame. A
representative sample of participants is desirable to increase external validity (i.e. the
extent to which the results are generalisable beyond the participants in the study).
However, this would require a large sample size, which is often unachievable due to the cost
and time involved in VE studies (Henry & Fetters, 2012). Therefore, selective sampling of
participants based on characteristics of interest (e.g. women in the early stages of breast
cancer [O’Brien et al., 2008]), may be more appropriate. In addition, researchers are
required to specify the unit of analysis in step two. It has already been recommended above
that VE interviews with the doctor and patient should form two units of analysis. A further
unit is the video-recording itself. Etic classification of the video-recording is beneficial as it
enables the comparison of the objective behaviour and subjective feelings of participants
regarding the effectiveness of the interaction (Kasper, Heesen, Köpke, Fulcher & Geiger,
2011; Melbourne et al., 2011). Moreover, since it has been identified that within DPI
individuals show multidimensional behaviour (see section 2.1), the capture of participants’
verbal and non-verbal behaviour within the interaction, as well as their impressions of these
behaviours is particularly important.
The third step involves data collection. This begins with the recording of the DPI in
video format. In order to stimulate recall and discussion within the VE interview the
recording should be of a good quality and capture the behaviour of both the doctor and
patient. As a result researchers should give consideration to the video-recording equipment
used and how this is positioned within the room (Haw & Hadfield, 2011). How the videos
will be used within the VE interview is also worthy of consideration because interview
structure, interviewer skills, and question formats have the ability to shape the resulting
data (Larsen et al., 2008). For example, interviews may be conducted on the whole video-
recording or on pre-selected segments of interest. These interviews may also take a range of
formats. The most popular is semi-structured, in which the researcher is free to select
questions to elicit information on the unexpressed thoughts and beliefs of the participant
(see Figure 1 for example questions). Usually the interviewer and participant can choose to

9
Can you tell me more about how you felt at this point?
Were there any other thoughts going through your mind?
What were your impressions of the physician’s/patient’s actions at this point?
What do you notice about your actions at this point?
How much pressure did you feel under making this decision?
Figure 1. Questions that could be used in a video elicitation-interview. Adapted from Henry
& Fetters 2012
stop the video and comment on important elements (Larsen et al., 2008). However, in some
cases researchers may feel it is necessary to conduct multiple interviews with the same
participant to allow for spontaneous comments and more narrow and focused questioning
(Arborelius & Timpka, 1990; Cromarty, 1996). It is recommended that variation in VE
interview procedure should be tailored to the research question and expertise of the
researchers (Marks et al., 2011). Consequently, the current paper has highlighted multiple
strategies for data collection, but does not a make a judgement about their objective value.
The final step is data analysis. If researchers have followed the recommendations
within this paper they will be required to analyse and integrate three sources of data; video-
recordings, doctor-interviews and patient-interviews. Nowak (2011) recognised that there
is no ‘gold-standard’, or even standardised procedure for the integration of data from
multiple sources. This means that researchers will need to consider a range of strategies.
Within the research literature there are three main approaches to integration of video and
interview data. Approach one involves editing the interview over the video-recording prior
to analysis (e.g. Frankel & Beckman, 1982), which may be beneficial when timing of
comments is regarded as important. However, generation of a single data source in this way
would not be possible when both the doctor and patient have been interviewed. In this case
researchers may choose from the remaining approaches. A second approach uses a single
group of researchers working concurrently with all sources to build a comprehensive picture
of the interaction (e.g. Young et al., 2011). This is an iterative process, which involves
repeated viewing and switching of sources. A caveat of this approach, however, is the
tendency to prioritise data from a single source, which may bias the results. The final
approach is analysis of individual data sources by different sub-groups of researchers
followed by integration of the findings (e.g. Saba et al., 2006). In practice, researchers may
10
adapt these approaches or generate a novel integration strategy (Neumann et al., 2011).
Therefore, comprehensive reporting of methodology is of vital importance.
3.4. Further Considerations for Those Using VE to Study DPI
Two further questions are raised as a result of the extensions to VE studies proposed
in section 3.3 and the application of VE to investigate what makes DPI effective. How should
the DPI video-recording be analysed? And is it necessary to measure clinical outcomes?
The analysis of video-recordings has been approached from both a qualitative and
quantitative perspective. Although VE studies have traditionally taken a qualitative
approach to the analysis of interviews there is no reason that this should restrict the
methods used to analyse the video-recording of the DPI. Qualitative approaches, such as
conversation analysis or thematic analysis (see Howitt & Cramer, 2008) provide a detailed
account of the nature of the DPI, including micro-analytic structure and social construction
of meaning (Peräkylä, 2004). In contrast, quantitative approaches commonly use a coding
scheme to classify units of behaviour into pre-selected categories (e.g. Bales, 1950; Ford,
Hall, Ratcliffe & Fallowfield, 2000; Roter & Larson, 2002). The frequency of each code may
then be extracted. Behaviours of interest can be investigated by combining codes that
measure the construct. For example patient-centeredness has been indexed by features
such as discussion of family medical history, patient question asking and physician enquiry
about the results of ongoing treatment (Bertakis & Azari, 2011). This approach assumes that
meaning is inherent to actions. The relative advantages of these systems and the philosophy
on which they are based have been widely debated, with no method the outright winner
(e.g. Heritage & Maynard, 2006; Peräkylä, 2004; Sandvik et al., 2002). Therefore,
researchers are free to make an informed decision as to which method of video-analysis to
use.
It is also important to consider the inclusion of clinical outcome measures in VE
studies, for example, treatment adherence, improvement in symptoms or quality of life.
This will allow researchers to assess the effectiveness of DPI on improving patients’ health,
which is arguably one of the main objectives of the medical consultation (Hugman, 2009).
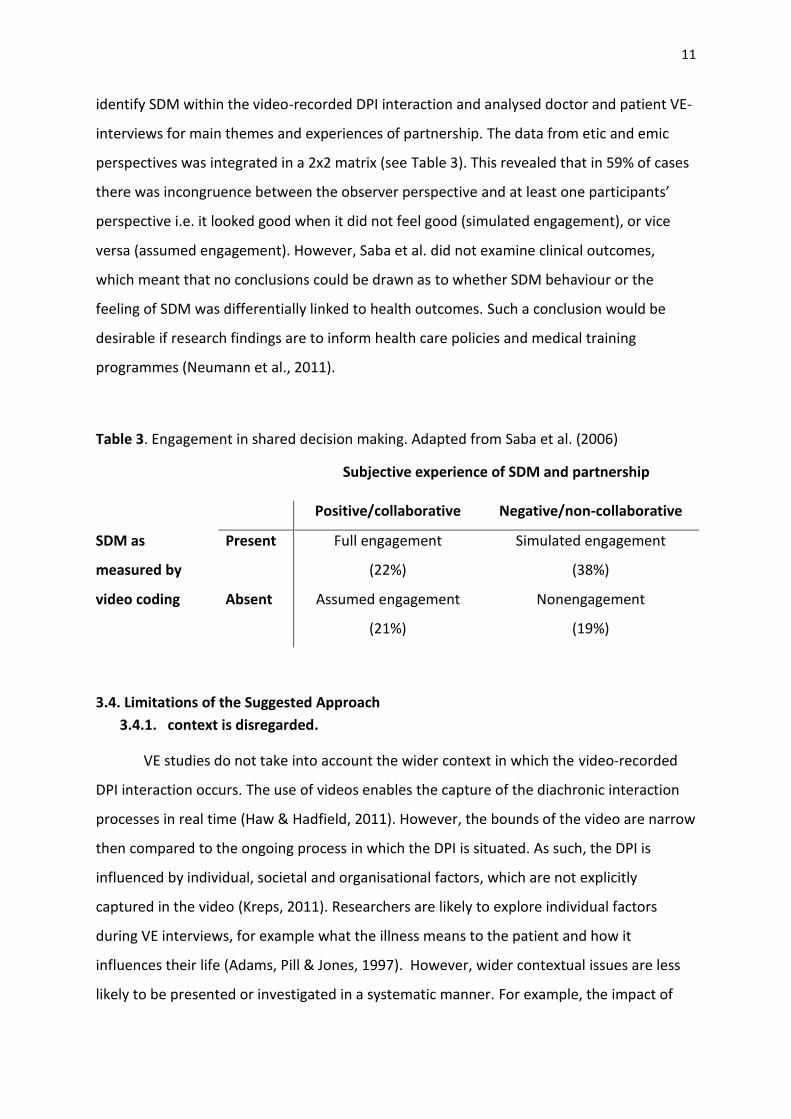
For example, Saba et al. (2006) used VE to explore SDM. In keeping with the
recommendations above, the researchers developed a quantitative coding scheme to
11
identify SDM within the video-recorded DPI interaction and analysed doctor and patient VE-
interviews for main themes and experiences of partnership. The data from etic and emic
perspectives was integrated in a 2x2 matrix (see Table 3). This revealed that in 59% of cases
there was incongruence between the observer perspective and at least one participants’
perspective i.e. it looked good when it did not feel good (simulated engagement), or vice
versa (assumed engagement). However, Saba et al. did not examine clinical outcomes,
which meant that no conclusions could be drawn as to whether SDM behaviour or the
feeling of SDM was differentially linked to health outcomes. Such a conclusion would be
desirable if research findings are to inform health care policies and medical training
programmes (Neumann et al., 2011).
Table 3. Engagement in shared decision making. Adapted from Saba et al. (2006)
Subjective experience of SDM and partnership
Positive/collaborative Negative/non-collaborative
SDM as
measured by
video coding
Present Full engagement
(22%)
Simulated engagement
(38%)
Absent Assumed engagement
(21%)
Nonengagement
(19%)
3.4. Limitations of the Suggested Approach
3.4.1. context is disregarded.
VE studies do not take into account the wider context in which the video-recorded
DPI interaction occurs. The use of videos enables the capture of the diachronic interaction
processes in real time (Haw & Hadfield, 2011). However, the bounds of the video are narrow
then compared to the ongoing process in which the DPI is situated. As such, the DPI is
influenced by individual, societal and organisational factors, which are not explicitly
captured in the video (Kreps, 2011). Researchers are likely to explore individual factors
during VE interviews, for example what the illness means to the patient and how it
influences their life (Adams, Pill & Jones, 1997). However, wider contextual issues are less
likely to be presented or investigated in a systematic manner. For example, the impact of
12
limited consultation length on patient-centred care (Mead & Bowers, 2000; Ogden et al.,
2004) or the influence of gender norms on patients’ presentation of concerns (Kaba &
Sooriakumaran, 2007). Puustein (1999) argues that the variability between DPI cannot be
explained without reference to the context in which it occurs. Therefore, despite the use of
multiple data sources and formats of data analysis, VE studies may still not fully capture the
nature of DPI.
3.4.2. data quality.
The use of a video-recording to stimulate recall of a recent DPI may lead to a more
detailed and accurate description than achieved by a standard interview because cues
displayed in the video can help to trigger memories (Elliot, 1986; Henry & Fetters, 2012).
This is particularly important as individuals may have poor memory and meta-cognitive
skills, meaning they are likely to forget or misremember events under free recall conditions
(Nisbett & Wilson, 1977). However, despite this advantage of VE, researchers should be
cautious that interview reports consist of reconstructed memories and may contain
inaccuracies and deliberate or unconscious biases (Hertwig, Fanselow & Hoffrage, 2003). For
example, patients may not be comfortable expressing negative views about their doctor in
VE interviews (i.e. social desirability bias; Kazdin, 2003) or hindsight bias (Fischoff, 2007)
may mean that the patients’ knowledge of the results of their decision may influence how
they recall their involvement in decision making.
Also worthy of consideration is Henry and Fetters’ (2012) warning that the self-
selected sample of participants may introduce a systematic bias into the results. It has been
suggested that doctors and patients who volunteer to let researchers record their medical
consultation may differ from those who do not. For example, patients with mental health
problems or ‘embarrassing’ conditions may be less likely to consent to video-recording
(Coleman & Manku-Scott, 1998). As informed consent is necessary before video-recording
DPI (see section 3.4.4.) researchers cannot avoid this potential bias. However, they should
acknowledge this and interpret their results accordingly.
In addition, questions have been raised as to whether knowledge that the
interaction is being recorded influences the behaviour of the participants. This is a problem
because it would reduce the internal validity of the data collected (Coleman, 2000). Through
13
analysis of video-taped consultations between 14 oncologists and 45 patients, Penner et al.
(2007) discovered few camera-related behaviours (e.g. looking at the camera or speaking
about the camera). Consistent with previous research (Hargreaves & Peppiatt, 2001; Martin
& Martin, 1984), participants in Penner et al.’s study reported that they forgot they were
being recorded. In further support, evidence shows that the clinical routine of doctors are
not significantly different when the participants are aware that they are being filmed and
when they were unaware; participants spent the same amount of time on 26/27 tasks
(Pringle and Stewart-Evans, 1990). This can be taken as evidence that doctor and patient
behaviour is not greatly affected by video-recording of the medical interaction.
Nevertheless, these studies only measured camera related behaviour and time on task, thus
limiting the conclusions that can be drawn about the influence of video-recording on the
content and social processes within DPI overall.
3.4.3. practical issues.
Despite the rich data generated from VE studies, practical issues relating to time,
data handling, equipment, and cost may prevent such research from being conducted. VE
interviews should be carried out as soon as possible after the DPI has taken place (Lyle,
2003). However, doctors’ busy schedules often prevent this. Moreover, VE interviews are
time consuming to conduct. For example, Larsen et al. (2008) report that it is common for a
50 minute long interaction to result in VE-interviews lasting for two-to-three hours. Analysis
of videos and interview is likely to take at least twice as long. With three data sources to
analyse, the study will require a substantial time commitment from researchers and
participants. Moreover, a single case generates huge amounts of data, which must be
systematically stored and analysed. This problem is exacerbated as there is no standardised
procedure.
Equipment is also important in VE studies. As has been noted in section 3. 3, the
video-recording should be high-quality and capture the behaviour of both participants to
provide participants with many cues to stimulate recall. But this is not always achieved in
practice (Haw & Hadfield, 2011). Researchers should also make provisions for the possibility
of equipment failure, such as noise within the video-recording or digital analysis software
crashing. Overall, these practical issues mean that the VE studies would be financially
14
costly. Nevertheless, the potential of such studies to gain an insight into the nature of an
effective DPI is a good incentive for researchers to overcome these practical limitations.
3.4.4. ethical issues.
Any research study will need to gain ethical approval before it commences.
However, those conducting VE studies may need to pay special attention to three issues
highlighted within the British Psychological Society, Code of Ethics and Conduct (Ethics
Committee of the British Psychological Society, 2009). Firstly, informed consent. This means
that researchers should ensure that individuals understand the purpose and possible
consequences of their participation. All participants must then agree to take part in the
research. It is also desirable for researchers to request permission to use DPI-videos and VE
interviews in secondary analyses, medical training, and conferences (Roberts, 2010). This
will extend the utility of the data and can enable researchers to answer new questions using
existing data sources. Secondly, video-recordings are hard to de-identify, causing the
potential for issues regarding privacy. This may be addressed to some extent by storing
videos in a secure location, separate from the participant’s details (Henry & Fetters, 2012).
Lastly, the content of medical consultations may be upsetting or embarrassing for
participants to discuss in VE interviews, for example, those involving treatment for a
terminal illness. Thus, interviewers should approach these topics sensitively and honour
their responsibility not to cause participants distress.
4. Conclusion
VE studies offer the opportunity to study multiple perspectives on the DPI, which
may be integrated to form a rich data source. Given the complex nature of dyadic, face-to-
face interactions in medical settings, integrative research is often required (Neumann et al.,
2011). Nevertheless, the benefits of VE must be weighed against the practical issues
surrounding such research, resulting from the wealth of data to be collected and analysed.
When interpreting the data researchers should also consider the impact of contextual
factors and the quality of the information obtained from VE interviews.
Furthermore, the ideas presented in this paper raise the question of what is an
effective DPI? It has been explored that this question may be answered from the
15
perspective of an observer, the doctor, the patient, or based on clinical outcomes. In
addition, this paper has proposed a research methodology to be conducted in pursuit of
discovering the ‘perfect’ DPI, which satisfies on all accounts. However, research using VE
methodology suggests that disparity is more common than convergence of these
perspectives (Saba et al., 2006). Moreover, there does not appear to be a systematic link
from objective or subjective features of the DPI to consequences of the interaction
(Silverman, 1987; Young et al., 2011). This may be because contextual factors not identified
through application of the VE methodology can influence how participants approach the DPI
and respond to their partner, and thus the outcomes. As a result, it would be a philosophical
question as to which perspective should be regarded as the most important. However,
adoption of this idea would negate the need for multiple approaches since only one would
be of value.
Irrespective of the difficulties in exploring the nature of DPI, VE can make a valuable
contribution to research, psychological theory and medical practice. VE provides an
opportunity for the development of integrative approaches in research, which has been
recognised as important for the progression of science (Neumann et al., 2011). The findings
of research may also be used to inform existing theoretical approaches to the study of
health care communication and DPI (e.g. Rao et al., 2010). Importantly, it can be used to
support the move from the uni-dimensional, ‘authoritarian doctor’ perspective to one in
which the behaviour of both the patient and doctor are seen as integral to the medical
consultation and its outcomes (Marks et al., 2011). Research findings may also be translated
into recommendations for medical training and policies.
It is doubtful that application of VE methodology will reveal the screenplay for the
‘perfect’ DPI. However, VE studies have highlighted the complex, multi-dimensional and
inter-subjective nature of DPI interactions. This finding is important in itself, but has also
influenced health care research and practice, with changes implemented to increase the
effectiveness of DPI.
16
5. References
Adams, S., Pill, R., & Jones, A. (1997). Medication, chronic illness and identity: The
perspective of people with asthma. Social Science & Medicine, 45(2), 189–201. doi:
10.1016/S0277-9536(96)00333-4
Arborelius, E., & Timpka, T. (1990). In what way may videotapes be used to get significant
information about the patient-physician relationship? Medical Teacher, 12(2), 197-
208.
Bales, R. F. (1950). Interaction process analysis: A method for the study of small groups.
Reading, MA: Addison-Wesley.
Bensing, J. M., Verheul, W., Jansen, J., & Langewitz, W. A. (2010). Looking for trouble: the
added value of sequence analysis in finding evidence for the role of physicians in
patients' disclosure of cues and concerns. Medical Care, 48(7), 583-588. doi:
10.1097/MLR.0b013e3181d567a5
Bertakis, K. D., & Azari, R. (2011). Determinants and outcomes of patient-centered care.
Patient Education and Counseling, 85(1), 46-52. doi: 10.1016/j.pec.2010.08.001
Bryman, A. (2006). Integrating quantitative and qualitative research: How is it done?
Qualitative Research, 6(1), 97-113. doi: 10.1177/1468794106058877
Coleman, T. (2000). Using video-recorded consultations for research in primary care:
Advantages and limitations. Family Practice, 17(5), 422-427. doi:
10.1093/fampra/17.5.422
Coleman, T., & Manku-Scott, T. (1998). Comparison of video-recorded consultations with
those in which patients’ consent is withheld. British Journal of General Practice
48(427), 971-974.
Connor, M., Fletcher, I., & Salmon, P. (2009). The analysis of verbal interaction sequences in
dyadic clinical communication: A review of methods. Patient Education and
Counseling, 75(2), 169–177. doi: 10.1016/j.pec.2008.10.006
Cromarty, I. (1996). What do patients think about during their consultations? A qualitative
study. British Journal of General Practice, 46(410), 525-528.
Davis, R. E., Dolan, G., Thomas, S., Atwell, C., Mead, D., Nehammer, S., ... Elwyn, G. (2003).
Exploring doctor and patient views about risk communication and shared decision-
17
making in the consultation. Health Expectations: An International Journal of Public
Participation in Health Care and Health Policy, 6(3), 198-207.
Eide, H., Quera, V., Graugaard, P., & Finset, A. (2004). Physician-patient dialogue
surrounding patients' expression of concern: Applying sequence analysis to RIAS.
Social Science & Medicine, 59(1), 145-155. doi :10.1016/j.socscimed.2003.10.011
Elliott, R. (1986). Interpersonal process recall as a psychotherapy process research method.
In L. S. Greenberg & W. M. Pinsof (Eds.), The psychotherapeutic process: A research
handbook (pp. 503-527). New York, NY: Guilford.
Ethics Committee of the British Psychological Society (2008). Code of Ethics and Conduct.
Retrieved from http://www.bps.org.uk/sites/default/files/documents/code_of_
ethics_and_conduct.pdf
Fishoff, B. (2007). An early history of hindsight research. Social Cognition, 25(1), 10-13. doi:
10.1521/soco.2007.25.1.10
Ford, S., Hall, A., Ratcliffe, D., & Fallowfield, L. (2000). The Medical Interaction Process
System (MIPS): An instrument for analysing interviews of oncologists and patients
with cancer. Social Science & Medicine, 50(4), 553-566. doi: 10.1016/S0277-
9536(99)00308-1
Frankel, R. M., & Beckman, H. B. (1982). IMPACT: An interaction-based method for
preserving and analysing clinical transactions. In L. S. Pettigrew (Ed.), Straight Talk:
Explorations in Provider and Patient Interactions (pp.71-85). Louisville, KY: Humana,
Inc.
Green, J., & Britten, N. (1998). Qualitative research and evidence based medicine. British
Medical Journal, 316(7139), 1230–1240. doi: 10.1136/bmj.316.7139.1230
Hall, J. A. (2003). Some observations on provider–patient communication research. Patient
Education and Counseling, 50(1), 9-12. doi: 10.1016/S0738-3991(03)00072-7
Hargreaves, P. N., & Peppiatt, R. (2001). Is videotaping of consultations acceptable to
patients attending a hospice day centre? Palliative Medicine, 15(1), 49-54. doi:
10.1191/026921601678110992
18
Haw, K., & Hadfield, M. (2011). Video in social science research: Functions and forms. New
York, NY: Routledge.
Henry, S. G., & Fetters, M. D. (2012). Video elicitation interviews: A qualitative research
method for investigating physician-patient interactions. Annals of Family Medicine,
10(2), 118-125. doi: 10.1370/afm.1339
Heritage, J., & Maynard, D. W. (2006). Introduction: Analyzing interaction between doctors
and patients in primary care encounters. In J. Heritage & D. W. Maynard (Eds.),
Communication in Medical Care: Interaction between primary care physicians and
patients (pp.1-21). Cambridge, UK: Cambridge University Press.
Hertwig, R., Fanselow, C., & Hoffrage, U. (2003). Hindsight bias: How knowledge and
heuristics affect our reconstruction of the past. Memory, 11(4-5), 357-377. doi:
10.1080/09658210244000595
Howitt, D., & Cramer, C. (2008). Introduction to research methods (2nd ed.). Essex, UK:
Prentice-Hall.
Hugman, B. (2009). Healthcare communication. London, UK: Pharmaceutical Press.
Kaba, R., & Sooriakumaran, P. (2007). The evolution of the doctor-patient relationship.
International Journal of Surgery, 5(1), 57-65. doi: 10.1016/j.ijsu.2006.01.005
Kagan, N. I., & Kagan, H. (1990). IPR - A validated model for the 1990s and beyond.
Counseling Psychology, 18(3) 436-440. doi: 10.1177/0011000090183004
Kagan, N., Schauble, P., Resnikof, A., Danish, S. J., & Krathwohl, D. R. (1969). Interpersonal
process recall. Journal of Nervous and Mental Disease, 148(4), 365-374. doi:
10.1097/00005053-196904000-00004
Kasper, J., Heesen, C., Köpke, S., Fulcher, G., & Geiger, F. (2011). Patients' and Observers'
Perceptions of Involvement Differ. Validation Study on Inter-Relating Measures for
Shared Decision Making. PLoS ONE 6(10), e26255. doi:
10.1371/journal.pone.0026255.t001. Retrieved from
http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0026255
Kazdin, A. E. (2003). Research design in clinical psychology (4th ed.). Boston, MA: Allyn &
Bacon.
19
Kenny, D. A., Veldhuijzen, W., van der Weijden, T., LeBlanc, A., Lockyer, J., Légaré, F., &
Campbell, C. (2010). Interpersonal perception in the context of doctor–patient
relationships: A dyadic analysis of doctor–patient communication. Social Science &
Medicine, 70(5), 763–768. doi: 10.1016/j.socscimed.2009.10.065
Kreps, G. L. (2011). Methodological diversity and integration in health communication
inquiry. Patient Education & Counseling, 82(3), 285-291. doi:
10.1016/j.pec.2011.01.020
Larsen, D., Flesaker, K., & Stege, R. (2008). Qualitative interviewing using Interpersonal
Process Recall: Investigating internal experiences during professional-client
conversations. International Journal of Qualitative Methods, 7(1), 18-37.
Lyle, J. (2003) Stimulated recall: A report on its use in naturalistic research. British
Educational Research Journal, 29(6), 861–78. doi: 10.1080/0141192032000137349
Marks, D. F., Murray, M., Evans, B. & Estacio, E. V. (2011). Health psychology: Theory,
research and practice (3rd ed.). London, UK: SAGE.
Martin, E., & Martin, P. M. L. (1984). The reactions of patients to a video camera in the
consulting room. Journal of the Royal College of General Practitioners, 34(268), 607-
610.
Mead, N., & Bower, P. (2000). Patient-centredness: A conceptual framework and review of
the empirical literature. Social Science & Medicine, 51(7), 1087-1110.
Melbourne, E., Roberts, S., Durand, M-A., Newcombe, R., Légaré, F., & Elwyn, G. (2010).
Dyadic OPTION: Measuring perceptions of shared decision-making in practice.
Patient Education & Counseling, 83(1), 55–57. doi: 10.1016/j.pec.2010.04.019
Neumann, M., Kreps, G., & Visser, A. (2011). Methodological pluralism in health
communication research. Patient Education and Counseling, 82(3), 281-284. doi:
10.1016/j.pec.2011.01.018
Nisbett, R. E., & Wilson, T. D. (1977). Telling more than we can know: Verbal reports on
mental processes. Psychological Review, 84(3), 231-259. doi: 10.1037/0033-
295X.84.3.231
Nowak, P. (2011). Synthesis of qualitative linguistic research: A pilot review integrating and
generalizing findings on doctor-patient interaction. Patient Education and
Counseling, 82(3), 429-441. doi: 10.1016/j.pec.2011.01.022
20
O’Brien, M. A., Whelan, T. J., Charles, C., Ellis, P. M., Gafni, A., Lovrics, P., ... Dimitry, S.
(2008). Women's perceptions of their treatment decision-making about breast
cancer treatment. Patient Education and Counseling, 73(3), 413-436. doi:
10.1016/j.pec.2008.07.015
Ogden, J., Bavalia, K., Bull, M., Frankum, S., Goldie, C., Gosslau, M., ... Vasant, K. (2004). “I
want more time with my doctor”: A quantitative study of time and the consultation.
Family Practice, 21(5), 479–483. doi: 10.1093/fampra/cmh502
Ong, L. M. L., de Haes, J.C.J.M., Hoos, A. M., & Lammes, F. B. (1995). Doctor-patient
communication: A review of the literature. Social Science & Medicine, 40(7), 903-
918. doi: 10.1016/0277-9536(94)00155-M
Pawlikowska, T., Zhang, W., Griffiths, F., van Dalen, J., & van der Vleuten, C. (2012). Verbal
and non-verbal behavior of doctors and patients in primary care consultations: How
this relates to patient enablement. Patient Education and Counseling, 86(1), 70-76.
doi: 10.1016/j.pec.2011.04.019
Penner, L. A., Orom, H., Albrecht, T. L., Franks, M. M., Foster, T. S., & Ruckdeschel, J. C.
(2007). Camera-related behaviors during video recorded medical interactions.
Journal of Nonverbal Behavior, 31(2), 99-117. doi: 10.1007/s10919-007-0024-8
Peräkylä, A. (2004). Two traditions of interaction research. British Journal of Social
Psychology, 43(1), 1-20. doi: 10.1348/014466604322915953
Pringle, M., & Stewart-Evans, C. (1990). Does awareness of being video recorded affect
doctors’ consultation behaviour? British Journal of General Practice, 40(340), 455-
458.
Puustinen, R. (1999). Bakhtin's philosophy and medical practice: Toward a semiotic theory
of doctor-patient Interaction. Medicine, Health Care & Philosophy, 2(3), 275-281. doi:
10.1023/A:1009970712856
Radley, A. (1994). Making sense of illness: The social psychology of health and illness.
London, UK: SAGE.
Rao, J. K., Anderson, l. A., Sukumar, B., Beauchesne, D. A., Stein, T., & Frankel, R. M. (2010).
Engaging communication experts in a Delphi process to identify patient behaviors
that could enhance communication in medical encounters. BMC Health Services
21
Research, 10(97). doi: 10.1186/1472-6963-10-97. Retrieved from
http://www.biomedcentral.com/1472-6963/10/97
Roberts, F. (2010). Qualitative approaches to clinician-patient communication. In D. W.
Kissane, B. D. Bultz, P. M. Butow, & I. G. Finlay (Eds.), Handbook of Communication in
Oncology and Palliative Care (pp. 695-705). Oxford, UK: Oxford University Press.
Rogers, A., Kennedy, A., Nelson, E., & Robinson, A. (2005). Uncovering the limits of patient-
centeredness: Implementing a self-management trial for chronic illness. Qualitative
Health Research, 15(2), 224-239. doi: 10.1177/104973230427204
Roter, D., & Larson, S., (2002). The Roter interaction analysis system (RIAS): Utility and
flexibility for analysis of medical interactions. Patient Education and Counseling,
46(4), 243-251. doi: 10.1016/S0738-3991(02)00012-5
Saba, G.W., Wong, S. T., Schillinger, D., Fernandez, A., Somkin, C. P., Wilson, C. C., &
Grumbach, K. (2006). Shared decision making and the experience of partnership in
primary care. Annals of Family Medicine, 4(1), 54-62. doi: 10.1370/afm.393
Salmon, P., Mendick, N., & Young, B. (2011). Integrative qualitative communication analysis
of consultation and patient and practitioner perspectives: Towards a theory of
authentic caring in clinical relationships. Patient Education & Counseling, 82(3), 448-
454. doi: 10.1016/j.pec.2010.10.017
Sandvik, M., Eide, H., Lind, M., Graugaard, P. K., Torper, J., & Finset, A. (2002). Analysing
medical dialogues: Strengths and weaknesses of Roter’s interaction analysis system
(RIAS). Patient Education and Counseling, 46(4), 235–241. doi: 10.1016/S0738-
3991(02)00014-9
Silverman, D. (1987). Communication and medical practice: Social relations in the clinic.
London, UK: SAGE.
Young, B., Ward, J., Forsey, M., Gravenhorst, K., & Salmon, P. (2011). Examining the validity
of the unitary theory of clinical relationships: Comparison of observed and
experienced parent-doctor interaction. Patient Education and Counseling, 85(1), 60-
67. doi: 10.1016/j.pec.2010.08.027
22
Zimmerman, C., Del Piccolo, L., & Finset, A. (2007). Cues and concerns by patients in medical
consultations: A literature review. Psychological Bulletin, 133(3), 438-468. doi:
10.1037/0033-2909.133.3.438
Zoppi, K., & Epstein, R. M. (2002). Is communication a skill? Communication behaviors and
being in relation. Family Medicine, 34(5), 319-324.





![Nicolas Bousquet arXiv:1007.4740v3 [stat.ME] 21 Oct … treated along the paper. Key Words subjective prior elicitation, Weibull distribution, expert opinion, virtual data, posterior](https://img.pdfslide.net/doc/110x75/5aca74f97f8b9aa1298db5bd/nicolas-bousquet-arxiv10074740v3-statme-21-oct-treated-along-the-paper.jpg)