Embed Size (px)
Citation preview
Appendix 1
The Insertion of a Peripherally Inserted Central Catheter under the guidance of ultrasound.
Written by: Meinir Hughes
Reviewed by:
Approved by: Medicines Management Committee (MMC)
Any other committees?
Approved date:
Review date: Sept 2020
This information is issued by the Medicines Management Committee on the understanding that it is the best available from the resources at our disposal at the time of preparation. These guidelines are intended to support clinical judgment. The clinician must use his discretion when following them.
Guideline Version
Date re-written Summary of amendments Date approved
3 Sept 2017
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
1
Appendix 1
Contents
PagePolicy Statement 3
Scope of Policy 3
Aims and Objectives 3
Clinical Information
Education and Training
Pre-placement assessment
Ultrasound guidance
Infection prevention
The procedure
4
4
5
8
10
10
References 17
Appendices 19
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
2
Appendix 1
Statement
This document will provide information describing the procedure required to place a Peripherally Inserted Central Catheter (PICC) using ultrasound guidance.
The document is based on current empirical evidence and best practice consultation resulting from a working collaboration with other expert practitioners in the UK and internationally (RCN 2016, Loveday et al 2014)
The document is mapped to the local National Safety Standards for Invasive procedures (NatSSIPs 2016)
Scope
The document provides a guide for all clinical practitioners placing PICCs in Velindre Cancer Centre and outreach placement clinic in the Macmillan Unit in Prince Charles Hospital, Merthyr.
Aims and Objectives
The aim of this guideline is to describe the safe and effective process of placing a PICC using ultrasound guidance. This will ensure that the standard of practice will be consistent throughout Velindre NHS Trust and that the delivery of care concerning the insertion of PICCs will be of a high standard in order to maximize safety and quality.
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
3
Appendix 1
I. Education and Training
Only practitioners selected by the Intravenous Access Nurse Specialist in consultation with the Chemotherapy Services Manager can undergo PICC placement training. Pre-requisites are: Registered General Nurse; Band 7 clinician with over 3 years experience of peripheral venous cannulation; availability within their role to perform regular PICC placement; fully conversant with the management of PICC-related complications; educated to degree level.
TrainingPractitioners must undergo a period of supervised training which will include the following:
Revision of the anatomy of the upper arm, inclusive of veins, arteries and nerves. Ultrasound training Study Day Overview of ultrasound guided placement presentation by the IV Access Nurse
Specialist or ANP Review of specific documents:
o PICC Insertion guidelineso Patient Group Direction for the administration of Lidocaine prior to PICC
placemento MRSA guidelines
Certified IR(me)R training (3 yearly). This will allow PICC placers to request a chest X-ray post PICC placement therefore becoming a referrer. Strict regulations are required to be followed when requesting an X-ray as a referrer (IR(me)R 200/6).
Interpretation of PICC X-rays
CompetencyAll practitioners will be required to perform PICC placement under supervision for a minimum of 10 placements. The decision to proceed to a formal assessment will be made by the supervising practitioner namely the Intravenous Access Nurse Specialist or an Advanced Nurse Practitioner/PICC placer.
Formal assessment of competency will be performed in order to determine the suitability of the practitioner to practice independently. A specific PICC placement competency assessment document will be used (appendix 1). Once deemed competent by the Intravenous Access Nurse Specialist or ANP, the practitioner can practice independently and require re-assessment of competency every 2 years.
II. Referral
Patients under the care of a Velindre Oncology Consultant from the age of 16 can be eligible for PICC placement in Velindre Cancer Centre or in the Outreach setting in the Macmillan Unit.
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
4
Appendix 1
Any request for PICC placement from Cwm Taff Health Board should be directed to the PICC placement team in the Royal Glamorgan Radiology department. Requests from other Health Boards should be carefully considered with consultation with the Intravenous Access Nurse Specialist, Chemotherapy Services manager or Senior Nurse/ANP. All patients who are deemed suitable for placement in Velindre Cancer Centre or the Macmillan Unit in Prince Charles Hospital will require registration under the care of a Velindre Oncologist.
III. Pre-placement assessment
Clinical criteria for PICC placement Ambulatory chemotherapy Poor Venous Access Patient choice Infusate:
o Intravenous medication or infusion toxic to the endothelial cells of the vein. PH < 5 (acidic) > 9 (alkaline). Osmolality >500mOsm/L
o Infusional DNA binding vesicanto Infusions causing venous pain
Patient assessmentAll patients requiring PICC placement will need an assessment to determine if they are fit to undergo the procedure. Any concerns outside the PICC placers experience must be discussed with a more senior practitioner or the Oncology team. Assessment will be documented on a PICC placement Procedural Safety Checklist in line with the National Standards for Invasive Procedures, Welsh Government (2016) (appendix 2).Patient assessment factors should include:
General wellbeing of the patient Take observations. Escalate high NEWS score to on call Doctor or Nurse. Recent history of thrombocytopaenia – take full blood count. Platelet count
should ideally be 50 or above. Sepsis – if a patient is exhibiting signs of sepsis and is febrile, PICC placement is
not recommended History of mediastinal disease – if present, review recent CT with Radiologist to
determine if Superior Vena Cava obstruction is evident. If there is evidence of SVC obstruction do not proceed with PICC placement and seek advice from the Oncology team.
Skin integrity Assess anticoagulation therapy. If patient is currently on antcoagulation, seek
advice from the Oncology team, Registrar on call or the specialist coagulation Doctor.
Appropriateness of the placement.It is the responsibility of the PICC placer to ensure that the PICC placement is appropriate and justified by following the assessment criteria below:
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
5
Appendix 1
Does the therapy prescribed or intended necessitate the need for a PICC? Does the therapy prescribed or intended necessitate the need for a single or dual
lumen PICC? If poor venous access if the reason for PICC referral, are the peripheral veins
suitable for peripheral cannulation?
Lymph node removal – breast patientsIn cases where there is history of axillary lymph node sampling (sentinel node biopsy) the arm can be used for PICC placement if the other arm is not suitable. Is it not advised to place a PICC in the arm post axillary node clearance – place the PICC in the non-surgical side and if unsuccessful, refer for a tunneled cuffed catheter after consultation with the Oncology team. Refer to the Consensus Document: Proposal for Consensus of Intravenous management of breast cancer patients (July 2017).
Pre-procedural checksWhere possible, the procedure assistant will be present when the Pre Procedural Check List is completed (NatSSIPs 2016)
Patient identification: check name, address and date of birth of patient and cross reference with the patient electronic notes.
Confirm MRSA screen result. If positive, the procedure must not go ahead unless consultation with the oncology team concludes that the urgency for the PICC outweighs the risk of MRSA systemic infection. It is not recommended to place a PICC when a patient has a confirmed MRSA screen unless patient is at risk of death or extreme morbidity if PICC placement is whitheld. When MRSA screen is positive, steps must be taken to decolonise as soon as possible following the MRSA guidelines.
Identify allergies, specifically allergy to nickel or dressings. Where allergy to nickel is confirmed or suspected, the securacath device must not be placed.
Past medical history, specifically injuries to shoulders, arms which have resulted in restriction of movement; CVA, thromboembolic events, cardiac conditions, respiratory conditions, renal disease.
Medication history, specifically anticoagulants – seek advice from the relevant doctor.
Previous PICC placement: identify if patient developed infection, dressing allergy or thrombosis. If a PICC-related thrombosis was diagnosed with a previous PICC, Low Molecular Weight Heparin prophylaxis should be initiated, preferable prior to placement. Identify any previous placement related complications in the patient notes.
Assess infection risk – refer to criteria below.
Infection risk assessment
The following criteria should be followed to determine any additional infection risk. If any of the following is applicable, a biopatch should be placed on the exit site post placement and for the duration of the dwell time with the exception of the patient being an in-patient with no other criteria (Moureau et al 2016):Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines.
|6
Appendix 1
Diabetic (only diet or insulin controled) Recent thrombosis – less than 3 weeks History of skin conditions such as eczema or psoriasis Previous positive MRSA screen BMI < 18 or > 30 IN patient Dual lumen PICC Previous line infection Placement close to the axilla
Contra indicationsPositive MRSA screen – follow the MRSA policyPlatelet count below 50Pyrexial due to infectionSVC obstructionINR above 2.5Lymphoedema or ANC clearanceSensory or motor deficiency of the arm - PICC placement where there is significant sensory impairment might delay recognition of complications.
Prophylaxis prior to PICC placement
Antibiotics: Prophylactic antibiotics should not be used routinely prior to insertion. The exception is in the case of a patient with positive MRSA infection (Kearon et al 2016).
Anticoagulants: Anticoagulant prophylaxis should not be used routinely. Where there is confirmed history of a previous PICC-related thrombosis, therapeutic LMWH needs to be considered by the Oncology team prior to placement (Loveday et al 2014).
Consent
A written consent is required where possible for PICC placement. The patient must have decision-making capability to give consent and must be given voluntarily and freely without duress or coercion. In the event that a patient does not have the capacity to consent discuss with the oncology team and/or the Mental Capacity lead for Velindre Cancer Centre.
The patient must have knowledge and understanding of the proposed procedure, complications and after-care both verbally and written in the form of a patient information leaflet. The patient and family must be given the opportunity to askquestions regarding the procedure or aftercare (Sugarman et al 1998)
An alert card is given to the patient as a prompt – what symptoms to identify and who to contact.
VisitorsAny practitioners or family and friends must be supervised throughout the procedure.Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines.
|7
Appendix 1
Clinic listIt is the responsibility of the PICC placer to review the PICC list for the day and take into consideration any additional cases which may need to be fitted into the list. All list changes to be authorized by the PICC placer (NatSSIPs 2016) .
IV. Ultrasound guidanceThe use of ultrasound guidance is recommended with every PICC placement. NICE guidance (2002). Benefits of using ultrasound include:
Allows the identification of a vein and an artery and distinguishes between the two (Sofocleous 1998)
Increases the success rate of first attempt placement by locating the precise location of the vein (Parkinson 1998)
Decreases the incidence of complications such as mechanical phlebitis and thrombosis (Stokowski 2009).
Reduction in the trauma for the patient caused by failed attempts Provides assessment of the integrity of the vein – detects thrombosis within
the vessel Improves the infusion rates of ambulatory chemotherapy pumps – PICCs may
be placed away from the antecubital fossa.
Ultrasound is a series of high frequency sound waves that are sent into the body and then reflected back to create an image. On ultrasound, fluid filled structures appear black and surrounding tissues appear as various shades of grey. Vessels such as veins and arteries appear well defined. Ultrasound cannot penetrate air or bone; necessitating the use of ultrasound gel between the probe and the skin to conduct the ultrasound beam.
The ultrasound screen will vary in its magnification of the image and can be adjusted. Depth markings will be clearly identified on the screen. It is recommended that scanning should start with the 4cm setting, and then if the vessel is superficial, increase the magnification to 2cm. This setting will magnify the vessel to two times its normal size.
Exposure time to the ultrasound during the procedure to place a PICC should be as low as reasonably achievable (IR(me)R 2000/6).
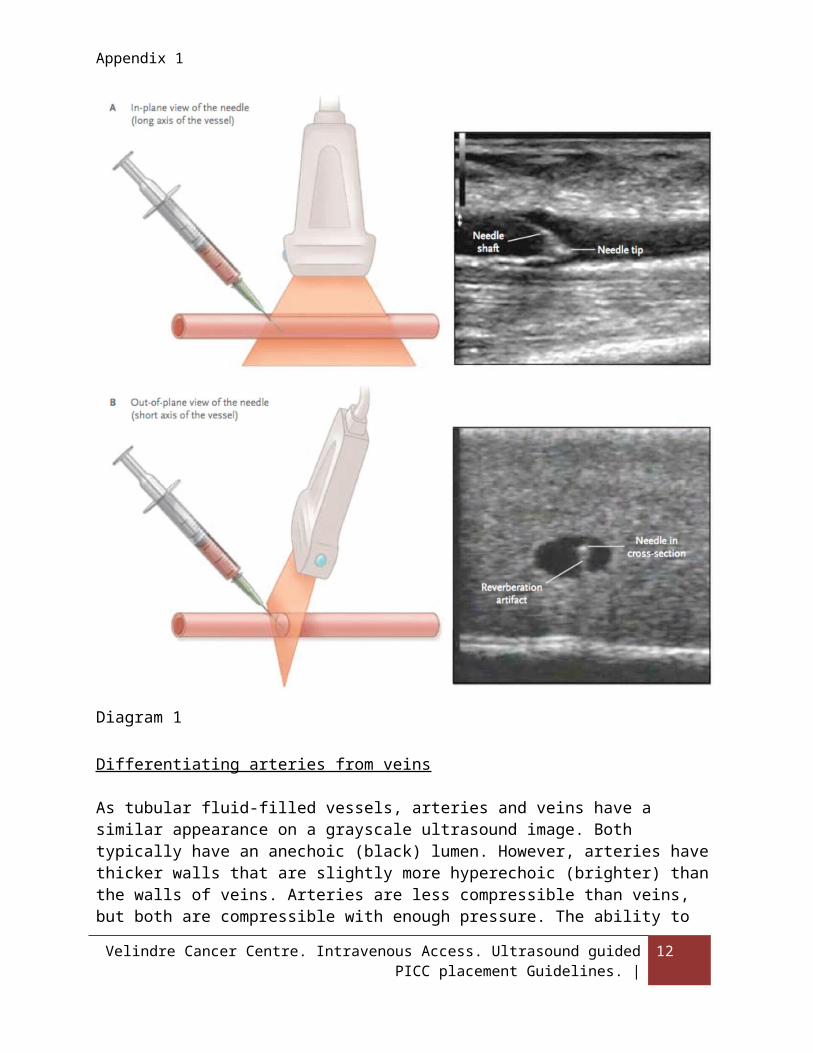
The probe should be held at a 90 degree angle on contact with the skin, and perpendicular (transverse) to the vessel. This can also be described as ‘out of plane’ or ‘short axiis’ – see diagram 1. This is the recommended position of the probe during venous cannulation. A light and steady touch should be maintained in order to view the
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
8
Appendix 1
images. A longitudinal position of the probe can be used where the probe is placed along the length of the vein. This can aslo be described as ‘in plane’ or ‘long axis’. It is more difficult to keep the needle and structure of interest using this approach but the benefits are that it can be advantageous because it shows the entire needle.
Diagram 1
Differentiating arteries from veins
As tubular fluid-filled vessels, arteries and veins have a similar appearance on a grayscale ultrasound image. Both typically have an anechoic (black) lumen. However, arteries have thicker walls that are slightly more hyperechoic (brighter) than the walls of veins. Arteries are less compressible than veins, but both are compressible with enough
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
9
Appendix 1
pressure. The ability to compress the venous walls with relatively minimal pressure is a useful way to distinguish a vein from an artery. Minimising risk: If there is any doubt that a vessel may be arterial, the vessel should be imaged in the short axis and enough pressure applied to slightly deform the vessel, and it should be observed for several seconds to determine whether arterial pulsation is present or absent. A non-compressible venous lumen indicates a thrombus. Doppler imaging may also be used to identify blood flow and to help differentiate arterial from venous flow.
Site Selection
Before placement begins, ultrasound should be used to choose the optimalsite for access. The choice of site should include factors such as vessel size, depth, course, surrounding structures, proximity to the axilla and antecubital fossa and adjacent pathology (such as overlying cellulitis). The vessel should be assessed for patency and other anatomic issues such as vein valves. It is extremely important to choose a vein away from arteries and nerves where possible. In the event that the only access into a vein is close to an artery, an angle of needle approach that will avoid the artery if the needle penetrates the posterior wall should be used (AIUM 2012).
V. Infection Prevention
The PICC must be inserted using maximal sterile barrier precautions utilising surgical Aseptic Non Touch Technique (ANTT) principles (Rowley et al 2010). The nurse will wear a hat, mask and gown. During the procedure the ultrasound probe must be covered with a sterile probe cover. The assistant must wear a hat during preparation and placement (Loveday et al 2014, O’Grady 2011).
The inserter will protect the critical aseptic field at all times wearing sterile gloves and gown. During the procedure s/he must not touch anything that has not been recently opened from a sterile package or parts of the patient’s skin which have been cleaned with 2% chlorhexidine gluconate / 70% isopropyl alcohol. S/he must not touch the underside of any drape (Loveday et al 20`4, O’Grady 2011).
In addition s/he should wherever possible follow non-touch principles even within the surgical field in accordance with Surgical ANTT. This will involve avoiding touching the PICC itself where possible (Public Health Wales 2016).
Surgical handscrub should be performed by the inserter for a minimum of 2 minutes using a sponge impregnated with chlorhexidine gluconate or betadine, paying attention to the 6 step handwashing technique.
VI. The procedure
Personnel
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
10
Appendix 1
PICC placement should be a two person procedure. Only a certified PICC placer can place a PICC. The assisting practitioner can be any practitioner deemed appropriate by the PICC placer which is not a relative or friend of the patient. The responsibility for the staffing and placement procedure lies with the practitioner placing the PICC. If a PICC placer needs to address other urgent clinical issues during PICC placement, another PICC placer can continue as long as a complete handover has taken place (NatSSIPs 2016).
Preparation
Where possible, the patient should lie supine with the arm extended to 40-45degrees and rotated. A full assessment of the anatomy of the vein should take place prior to placement.
Vein selection
The basilic vein is preferred as it offers the largest diameter of upper extremity vessels and affords a non-tortuous entry into the subclavian vein away from arteries and nerves. If the basilic vein is not suitable in one arm, the next vessel of choice is the basilic vein the other arm (unless contraindications apply). If neither basilic veins are accessible, assess the cephalic and brachial veins. The cephalic vein should not be the first vein of choice as it angles sharply to enter the terminal portion of the axillary vein making catheter advancement difficult. The route from the cephalic vein to the SVC is more arduous and longer than from the basilic vein. Care must be taken cannulating the brachial veins due to their proximity to the brachial artery and the median nerve. In some circumstances, nerve clusters can be identified on ultrasound, avoid cannulating a vein in the pathway of an identified nerve cluster. The decision to cannulate the cephalic or the brachial vein should involve the following criteria:
Do not use a small cephalic vein Do not use a brachial vein which is precariously close to the brachial artery Do not use a brachial vein where there is an identifiable cluster of nerves visable
on ultrasound in the cannulation path.
Venous assessment should also include an assessment of vessel health along the whole peripheral length of the vein targeted for use. A non-thrombosed vein should compress effortlessly. If a vessel does not compress easily, regard this as a sign of a thrombosed or phlebitis vein. If the area of difficult compression is fairly significant, refer for a Doppler ultrasound (AIUM 2012).
Pre-placement measurement
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
11
Appendix 1
Post vein selection, measurement of the PICC pathway on the external surface of the patient is required in order to estimate the length of the PICC. Measurement for PICC placement can be performed following the instructions overleaf (measure in centimeters):
Patient to lie supine Place the arm at a 45 degree angle.
Using an indelible ink skin marker pen, mark the skin with an arrow directing towards the site approx 3cms across from the chosen location for vein insertion shortly prior to the procedure. This provides you with an insertion guide when placing the line (NatSSIPs 2016).
Measure from insertion site to the mid clavicle. Measure 3 intercostal spaces down Observe depth of vein on ultrasound and add to measurement.
o Compare this measurement with the Lum measurement (Lum 2004) according to height. Nb: Add 4cm to the Lum measurement when placing in the left side.
o To compare with the Lum measurement : Measure the distance from the venepunture site to the AC fossa and add to the measurement and compare.
Add 6cm to the measurement (for the external portion of the PICC).
Anesthesia
Only local anesthesia will be appropriate for PICC placement. The drug of choice is Lidocaine 1% (lignocaine 1g in 100mls solution). The lidocaine solution is infiltrated at the site prior to placement in small amounts usually less than 1ml per site. The maximum dose of lidocaine, alone as a single agent is 3mg per kg, i.e 21mls of 1% solution for an adult of 70kgs. (BNF 2015) This dose must not be exceeded. The administration of lidocaine must be preceded by a withdrawal technique to verify that a vessel had not been inadvertently punctured. Inject the lidocaine superficially to avoid venous constriction.
Minimising risk:
Care must be taken not to inadvertently inject lidocaine into a vein. Take extreme care when the vein is superficial – inject into the superficial layer of the skin – rising a bleb.
When preparing the equipment on the sterile field, the lidocaine injection must be drawn into a smaller syringe than the saline in order to clearly distinguish between the two. This will minimise the risk of inadvertent use of the lidocaine injection to flush the PICC.
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
12
Appendix 1
Adverse symptoms relating to the use of lidocaine may be delayed post administration, therefore each patient must be observed for 20 minutes post injection.
The lidocaine will be issued as part of a Patient Group Directive signed by each PICC placer.
Equipment requiredPICC insertion pack inclusive of micro-introducer setPICC – proximal valved open endedSterile glovesSafety needlesSecuracathSafety bladeLidocaine 1% Tourniquet
SchedulingAccording to clinic but if infection …
The procedure
Clearly document the measurement guide and at what length to cut the PICC. Placer to wear hat and mask and perform a surgical scrub. Assistant to open the PICC insertion pack onto a clean and dry trolley and open
the required sterile equipment onto the sterile field using a non-touch technique. Dry hands with the sterile towels from within the opened PICC pack working
methodically from the hands down to the arms. Put on gown and sterile gloves. Draw up the idocaine and saline. Minimising risk: Draw the lidocaine into a 5mls
syringe (only) and normal saline 0.9% for intravenous injection into a 20ml syringe (only). This will clearly identify the difference between the syringe size to prevent inadvertent administration of the lidocaine into the vein. Saline must not be drawn into a 10ml syringe.
Using surgical ANTT principles, ensure that any unprotected key parts are covered.
Prime the sheath and dilator with saline. Place a sterile drape beneath the patients arm. Decontaminate the skin at the insertion site (within an aprox 8cm square area
surrounding the insertion site) with a single-use application with 2% chlorhexidine gluconate / 70% isopropyl alcohol (or povidone iodine in alcohol for patients with sensitivity to chlorhexidine) for 60 seconds followed by a continuation of the cleansing outwards approximately another 3-4cm square. Allow to dry. The skin should be cleaned using an up and down, to and fro friction rub.
Drape the patient with a fenestrated full body drape. Cover the probe with a sterile cover – place acoustic gel within the cover.
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
13
Appendix 1
Tighten the tourniquet. Use the ultrasound probe to re-locate the vein. Minimising risk: Care must be taken to ensure that the vessel is not an artery.
Compress and hold with the probe to ensure there is no pulsation. Close observation must always take place to identify any small abhorrent arteries.
Administer intradermal lidocaine at the proposed venepuncture site. Cannulate the vein. When cannulating the vein with a needle, the probe is held
perpendicular to the vein. The needle should be placed slowly into the skin with the bevel facing up. When the needle approaches the vessel target, the anterior wall will indent. A swift insertion into the vein at this time will prevent excessive collapse of the vein wall. Always observe for a blood return from the needle or cannula.
Slowly and carefully introduce the wire into the needle. Minimising risk: The wire must glide into the needle and vein without resistance, if any resistance is encountered, STOP – never force a wire.
Assistant to loosen the tourniquet. Remove the needle leaving the wire in situ. Thread the sheath and dilator over the wire and advance into the vein. If difficulty
is encountered, observe the tip of the sheath to ensure no damage has been caused – if damaged, replace the sheath and dilator. Perform a small dermatotomy if necessary but not routinely.
Minimising risk: To reduce the risk of inadvertent wire migration, never turn your back on a free wire and make a knot in the wire at this point to prevent migration. When placing a wire into a vein, always direct the wire with the ‘floppy tip’ entering the vein.
Minimising risk: To reduce the risk of needle-stick injury, safety devices must be used where possible (HSE 2013). Carefully place any sharps on the sharps pad or within a separate tray on the sterile field and dispose of carefully in the sharps bin.
Prepare the PICC. Ensure that the site of placement corresponds with the mark on the skin – adjust the measurement accordingly. Cut the PICC at the pre-determined measurement using a safety blade – deploy the safety device; place the extension tubing onto the proximal end of the PICC; advance the stylet (wire) through the extension tubing into the PICC until it can be seen exiting the distal tip; withdraw the wire to aprox 1cm and close the roll clamp on the extension tube firmly to prevent movement; flush the PICC - examining the PICC to ensure that there is no damage. Where possible, do not touch the PICC with your gloves.
Hold onto the sheath and dilator and carefully remove the wire; remove the dilator and immediately place your thumb onto the opening of the sheath to prevent blood loss and air entry; place the PICC into the vein using sterile forceps ensuring that there is no contact between the PICC and any other surface or skin.
Once the PICC has been placed to the pre-determined length and whilst the sheath remains in situ, examine the internal jugular vein using ultrasound guidance to identify jugular malposition. If identified, re-position the PICC. Moving
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
14
Appendix 1
the position of the arm may aid successful re-positioning away from the jugular vein.
Remove the sheath using the peel-away technique. Hold the PICC carefully in situ to prevent migration.
Ensure haemostasis is achieved. Medical glue can be used to achieve haemostasis. Place the securacath unless allergic to nickel. Dress the PICC with gauze and semi-occlusive dressing. Chest X-ray to verify tip placement. Each PICC placer has a responsibility to evaluate every PICC X-ray post
placement and to discuss and discrepancies with the Radiologist or Radiographer.
Adjustments post X-ray. The ideal tip location is the caval atrial junction. Placement in the mid or low SVC or just tipping into the atrium are acceptable tip positions if re-positioning is not deemed possible. Re-positioning can only be performed within one hour of placement.
Re-dress the PICC with the biopatch at this point if the patient meets the criteria.Post procedure, the PICC placer and the assistant must observe the counting and disposal of all wires and sharps used (NatSSIPs 2016).
MalpositionWhen catheter malposition is evident on the post PICC placement X-ray, re-positioning of the PICC can take place following the guidance below:
Calculate the number of centimetres to be removed by identifying the distance from the first point of malposition to the catheter tip – add 1-2cm to this measurement.
You will need: Large dressing towel; sterile plastic forceps; semi-occlusive clear dressing; sterile gauze; nitinol floppy tip wire; sterile gloves.
Remove the dressing and gauze with non-sterile gloves. Open the wheel clamp of the adaptor extension until fully open. Put on sterile gloves. Place the large dressing towel under the arm. Open the securacath with sterile gauze to maintain the sterility of your dominant
hand. Remove the PICC using the pre-determined measurement – ensure no contact
between the PICC and the patients’ skin. Whilst maintaining sterility,place the wire into the PICC via the wheel clamp
ensuring that a portion of the wire remains external to the wheel-clamp. Close the wheel-clamp firmly to prevent wire migration. Using the plastic forceps, re-advance the catheter into the vein. Remove the wire. Replace the securacath and the dressing. Re X-ray
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
15
Appendix 1
When the above procedure fails to correct the malposition after two attempts, fluoroscopy can be used to re-position the catheter under the direction of a Radiographer.
Documentation
A standard documentation in the electronic notes should include the following:The name of the PICC placer and the assistantMRSA screen resultSingle or Dual lumen catheter usedSide and vein usedAny complications experienced/procedural difficultiesStrength and dose of lidocaine usedPICC measurementsWhether securacath placed. Location of the tip of the catheter on X-ray and consequently any adjustmentsFinal external measurement If biopatch used Any patient complications
HandoverAll out-patients must be referred to the community nurse or Velindre Day Case clinics or Outreach for follow up care. The referral will be made verbally over the phone supported by documentary guidance outlining the procedure, catheter length and after care instructions. For in-patients, handover will be verbal, over the phone or in person and must include relevant information concerning the procedure, patient-related incidents and any anticipated problems (NatSSIPs 2016.)
Management of intraoperative complicationsA Datix will be completed following any of the following:Stuck wireArterial punctureEmbolisation of guidewireAllergic reaction
Audit
A spreadsheet will record procedural data for audit purposes of all insertion dataAudit will be ongoing, highlighting issues such as:
time frame for placement, number of patients who receive placement using ultrasound device
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
16
Appendix 1
complications during the procedure success of the procedure
VIII. References
AIUM Practice Parameter for the Use of Ultrasound to Guide Vascular Access Procedures American Institute of Ultrasound in Medicine (2012)
BNF (British National Formulary) 2015 ed 69 London. BMJ Group and Pharmaceutical Press.
Consensus Document: Proposal for Consensus of Intravenous management of breast cancer patients (July 2017).http://nww.velindrecc.wales.nhs.uk/opendoc/453532
Kearon et al (2016). Antithrombotic therapy for VTE disease – CHEST guidelines and expert panel report. CHEST. 149 # 2 p315-352.
HSE (Health and Safety Executive) (2013). Health and Safety (Sharp Instruments in Healthcare) Regulations. Guidance for employers and employees http://www.hse.gov.uk/pubns/hsis7.pdf
Loveday HP et al (2014) “epic3: National Evidence-based Guidelines for Preventing Healthcare-Associated Infections in NHS Hospitals in England”. Journal of Hospital Infection 2014; 86S1 (2014) S1–S70
Lum P (2004) A new formula based measurement guide for optimal positioning of CVC’s. Journal of the Association for Vascular Access. Vol 9 Issue 2 p 80-85.
Moureau, Nancy; Chopra, Vineet (2016) Indications for peripheral, midline and central catheters: summary of the MAGIC recommendations. British Journal of Nursing . Vol. 25 Issue 8, pS15-S24. 7p.
National Safety Standards for Invasive Procedures (NatSSIPs) 2016. Welsh Assembly Government.http://www.1000livesplus.wales.nhs.uk/sitesplus/documents/1011/NatSSIPs%20WALES%20%28FINAL%29%20September%202016.pdf
National Institute for Clinical Excellence (September 2002) “Guidance on the Use of Ultrasound Locating Devices for Placing Central Venous Catheters.” NICE Technology Appraisal No 49. London: National Institute for Clinical Excellence.
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
17
Appendix 1
O'Grady NP, Alexander M, Dellinger EP, Gerberding JL, Heard SO, Maki DG, Masur H, McCormick RD, Mermel LA, Pearson ML, Raad II, Randolph A, Weinstein RA (2011) CDC - Guidelines for the Prevention of Intravascular Catheter-Related Infections. Morbidity and Mortality Weekly Report 51: 1-26
Parkinson M et al (1998) Establishing an Ultrasound Guided PICC Insertion Service. The Clinical Radiology. 53 33-36
PublicHealthWalesANTThttp://www2.nphs.wales.nhs.uk:8080/WHAIPDocs.nsf/1f8687d8da97650980256fa30051b0be/e4528983f2eddd3a80257f10003dd2f3/$FILE/ANTT%20Framework%20v4.0.pdf
Rowley S, Clare S, Macqueen S, Molyneux, R (2010) ANTT v2: An updated practice framework for aseptic technique.British Journal of Nursing 2010: 19(5); S5-S11.
Sofocleus C, et al (1998) Sonographically guided placement of PICCs: Review of 355 procedures. American Journal of Roentgen. Vol 170 Part 6 p1613-6.
Stokowski G, Steele D, Wilson D. (2009) The Use of Ultrasound to Improve Practice and Reduce Complication Rates in PICC Insertions. The Art of Science of Infusion Nursing. V32 N3 p145-155.
Sugarman J, Douglas C, Robert C. Hubal (1998) Getting Meaningful Informed Consent from Older Adults: A Structured Literature Review of Empirical ResearchJornal of the American Geriatric Society. Volume 46, Issue 4 Pages 517–524.
The Ionising Radiation (Medical Exposure) Regulations 2000/6. Published on Society of Radiographers (https://www.sor.org)
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
18
Appendix 1
Appendix 1
PICC Insertion using Ultrasound guided imaging technique.
PRACTICAL TRAINING COMPETENCY
DOCUMENT FOR ASSESSMENT
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
19
Appendix 1
Name of placer: ………………………………………………………………
Name of Assessor: …………………………………………………………….
Date: ……………………………………………………………
Statement:
All practitioners new to PICC placement must successfully complete a formal assessment prior to practicing independently. Practicing PICC placers must be re-assessed for competency 2 yearly. Each PICC placer must have placed regularly throughout the year with the minimum standard being to place 2 PICCs monthly using Ultrasound guidance. If a period of time over 3 months has lapsed since placement of a PICC, the placer will need to complete a formal competency assessment prior to being able to practice independently. A formal assessment can only be performed by the Intravenous Access Specialist Nurse in Velindre Cancer Centre.
A theoretical and practical assessment will need to be completed as part of the overall assessment of competency.
Practitioners will pass or be referred.
A certificate of competency will be given to the practitioner once the placer has been deemed competent.
1. Theoretical preparation
To be familiar with the following documentation:
Document Signature
Ultrasound placement PICC guidelines
Patient Group Direction – Lidocaine
Guidelines for exchanging a PICC over a wire
IR(me)R guidelines
CDC guidelines
PPIC2 guidelines
PICC care and management guidelines
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
20
Appendix 1
2. Practical assessment
The placer will demonstrate competency in the following:
a. Patient Assessment and preparation
Achieved Not achieved
Patient Identification
Review of the medical notes. Should include:
What therapy is planned – single or dual lumen to be placed appropriately
Co-morbid conditions Past medical History Contra-indications for PICC placement Anticoagulation therapy and its management pre-PICC Any history of previous PICCs – investigate previous
complications Demonstrate ability to assess lymph node removal history
where applicable and to plan appropriately.
Clinical assessment of the general condition of the patient.
Patient education
Obtaining consent
b. Procedural preparation
Achieved Not achieved
Positioning the patient for placement
Assessment of the structures in the upper arm
Attention to Health and safety and sharps safety
Appropriate measuring technique
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
21
Appendix 1
c. The placer will demonstrate competency in the following:
Achieved Not achieved
The location of the veins and arteries in the upper arm using ultrasound guidance
Demonstrate procedure to alter gain and depth on US device
Clear distinction between artery and vein during ultrasound assessment
How to identify a nerve cluster on ultrasound
d. PICC placement
Achieved Not achieved
Site preparation – cleansing
Observing strict principles of asepsis throughout – surgical ANTT
Appropriate use of the tourniquet
Appropriate steps taken to minimise blood loss and air entry
The appropriate use of lidocaine injection.
Needle insertion technique
PICC insertion technique
Safe insertion practice of the wire
Placing the appropriate length of PICC
Observation of the PICC in the jugular vein with US device
Application of the securacath device
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
22
Appendix 1
Safe disposal of all sharps and equipment
Awareness of patient safety post procedure
e. X-ray confirmation of placement
Achieved Not achieved
Completing a chest X-ray request form
Interpretation of the X-ray
3. Theoretical Assessment:
Question Correct answer
Q: Describe the pre-assessment procedure when a patient has had a previous PICC?
A: Assess for previous infection, thrombosis, dressing allergies. If thrombosis present review Doppler results. Review infection results and time from infection.
Q: Describe the pre-assessment procedure for a Lymphoma patient?
A: Assess position of nodes. If mediastinal disease, review scans with Radiologist
Q: How do you identify a healthy vein on ultrasound?
A: compresses easily. Poor compression could indicate thrombosed vein.
Q: How do you identify an artery on ultrasound?
A: Pulsation – always compress and wait.
Q: Describe the terminology used for the probe being across the vein and along the length of the vein?
A: Across: Transverse. Along: Longitudinal
Q: What is another term for the ‘probe’?
A: Transducer
Q: Describe the venous and arterial anatomy of the upper arm?
A: Cluster of brachial artery surrounded by two brachial veins; cephalic vein laterally
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
23
Appendix 1
and basilic vein medially
Q: What is the maximum dose of lidocaine you can give an average 70kg person?
A: 20mls
Q: Describe 3 adverse events related to the administration of lidocaine?
A: Sleepiness; Dizziness; Vertigo; Confusion; Blurred vision; Dysphagia; Tinnitus;Trembling/restlessness/irritability
Q: What steps must you take to minimise arterial puncture?
A: Careful assessment of the vessels in the upper arm to determine location of the main veins and arteries; Careful assessment of any other small tributary arteries; always compress and wait with all vessels.
Q: What steps must you take to minimise the incidence of nerve injury?
A: Assess the presence of nerves on ultrasound in relation to the brachial veins. Where nerve pathways are close avoid the brachial veins; if the basilic vein in not suitable in the first arm to assess the basilic vein on the other arm, when neither of the basilic veins are suitable assess the cephalic veins on both sides, if large cephalics present use prior to brachials.
Q: What steps must be taken when symptoms of nerve injury are presented during placement?
A: Stop the procedure and remove any instruments.
Q: Describe the safety requirement of using guide wires?
A: To ensure that a guide wire does not migrate into the vein; to always loop and tie a wire to prevent migration; to never lose sight of a wire within the catheter when performing an exchange over a wire.
Q: What is meant by the term ‘referrer’ according to the IR(me)R guidelines and what are the main responsibilities?
A: Health professional who is entitled to request a specific examination involving ionising radiation but must supply accurate and comprehensive information.
Q: Describe and demonstrate on an X-ray the 3 main methods of identifying the location of the catheter tip post X-ray.
A: Curve of RA; Anterior ribs; 5cm down from carina
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
24
Appendix 1
4. Exchanging a PICC over a wire
Question Correct answer
Q: Describe the assessment process prior to exchange over a wire.
A: Assess for diagnosis or symptoms of thrombosis and infection; must relay that in the event of an infection or thrombosis the procedure will not be performed; flush the catheter prior to exchange; prophylactic heat pad along the arm prior to exchange.
Q: Describe the procedure for an exchange over a wire
A: Careful consideration of the wire; lidocaine to be administered after the wire is placed; when exchanging single for dual or vice versa change the securacath
Q:What are the main safety features to observe during an exchange over a wire?
A: Migration of the wire or PICC.
Discussions:
...............................................................................................................................................................
...............................................................................................................................................................
...............................................................................................................................................................
...............................................................................................................................................................
Competency achieved: Pass Fail Referred
Date: ………………………………………………
Name of Assessor: ………………………………………………………………
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
25
Appendix 1
Signature of assessor: ………………………………………………………….
Signature of placer: ..............................................................................
Appendix 2
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
26
Appendix 1 Placement Date: PICC placement VCC: Additional Consent / Procedural Safety check list:
Sign inMRSA screen result: Date of screen:
Check for any previous positive MRSA:
Introduction to all staff present: Yes:Check name and address with pt:Observations performed: Yes
Previous PICC: Yes No Check for DVT/Inf
Anticoagulation therapy: Yes: No:
If patient on warfarin? INR result: ………………
Allergies: Yes: No: ……………………………..Nb: Allergy to nickel: NO securacath.
Relevant past medical history:
Assessment .
Rationale for PICC placement:
Planned treatment: ……………………………………
Reason for PICC: ……………………………………………Breast pt: Yes: No:Surgical history (node removal): …………………….Lymphoma pt: Yes: No:If yes, review scan for obstruction of SVC.
Assessment cont…Infection risk assessment: Criteria for biopatch:
In patient TPN Thrombosis (current)
Diabetic (not diet cont) Prev +ve MRSA
Skin condition such as exzema/psoriasis
Previous line infection Site close to axilla
BMI > 30 < 18.5 Co-morbid condition/sBiopatch decision: Yes: No:
Patient education:
Reason for PICC: Infection control:
Securacath placement and settling in period:
X-ray post placement:
Keeping PICC dry with waterproof sleeve:
Referral to DN, PICC care required weekly:
Complications to discussInfection: Symptoms: exit site and rigorsThrombosis: Discuss possible LMWH 3 mths - do move arm but not to carry heavy objects.Allergies to dressing: Bleeding at site:Alert card discussed and given:
Time OutIs consent form signed:
Patient fit for placement:
Correct PICC prepared: Dual or Single:Bioflow PICC:Assessment of the placement site
Assess appropriate vein:
Identify arteries and nerves in location of the placement:
PICC placer or assistant to review any critical or unexplained restraints:PICC measurement:Count/dispose of all sharps and wires:
Identification of PICC tip on X-ray:
Sign out:
Procedure recorded on Canisc:
Patient referred to DN: In pt:
Name: ………………………….
Signature: ………………………..
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. | 27
YY
Appendix 1
Velindre Cancer Centre. Intravenous Access. Ultrasound guided PICC placement Guidelines. |
28



























