Embed Size (px)
Citation preview
NDPHS Evaluation Team 2013Third MeetingStockholm, Sweden5 September 2013
Title Minutes from the 3rd ET 2013 meeting
Submitted by Secretariat
Summary / Note This document recalls the main discussion points and decisions made during the 3rd ET 2013 meeting
List of Annexes Annex 1 - Evaluation Team’s views regarding the Evaluation Consultant’s recommendations and other issuesAnnex 2 - Development of the NDPHS Strategy beyond 2013Annex 3 – List of documents submitted to the meetingAnnex 4 – List of participants
1. Welcome and opening of the meeting
The meeting was opened and chaired by Mr. Thomas Ifland, the Evaluation Team Chair.
Ms. Karin Berlin, Head of Section, Division for EU and International Affairs, the Ministry of Health and Social Affairs of Sweden, welcomed the participants on behalf of Sweden.
2. Adoption of the agenda
The Meeting adopted the Provisional agenda (submitted as document ET2013 3/2/1).
3. Draft evaluation report – presentation by the ET Consultant
With reference to document ET2013 3/3/1, the Evaluation Consultant addressed to the attention of the Evaluation Team the key conclusions from the evaluation.
The Meeting thanked the Evaluation Consultant for his work and agreed to discuss the report in detail in the next agenda item.
4. Draft evaluation report – discussion and ET’s recommendations to the CSR
The Meeting discussed the Evaluation Consultant’s report, including the key conclusions and recommendations, as well as other issues raised by ET members beyond the scope of the Evaluation Consultant’s report, and agreed to submit to the CSR 22 a document “Evaluation Team’s views regarding the Evaluation Consultant’s recommendations and other issues” (cf. Annex 1).
Further, with reference to document ET2013 3/4/1, the Evaluation Team discussed issues related to the development of the NDPHS Strategy beyond 2013 and agreed as follows:
To introduce some amendments to the procedure proposed in the document ET2013 3/4/1 (cf. Annex 2);
The ET Chair will send a letter to the CSR members informing them about the following:
document.docx 1

a) during the CSR 22 meeting the CSR members will be invited to adopt the Terms of Reference of the Strategy Working Group (SWG) and establish the SWG as well as to hold a first, preliminary discussion on priorities (headlines) for the NDPHS Strategy 2014-2020;
b) the CSR members will be invited to nominate their representatives for the SWG and submit their final input to the paper specifying suggested priorities (headlines) of the NDPHS Strategy 2014-2020 until 1 November 2013. The Secretariat will compile them into one paper, which can serve as a background paper for discussions during the ministerial-level PAC on 22 November 2013;
The Evaluation Consultant is invited to make corrections in his report taking into account the Evaluation Team’s discussions and submit it to the NDPHS Secretariat no later than 24 September 2013.
5. Presentation of the evaluation results to the CSR
Having discussed the issue of presenting the evaluation results to the CSR, the Meeting agreed as follows:
The Evaluation Team’s views regarding the Evaluation Consultant’s recommendations and other issues will be submitted as a CSR 22 meeting document (cf. Annex 1);
After a few introductory words by the ET Chair, the Evaluation Consultant will make a 30-minutes long presentation, to be followed by a presentation by the ET Chair.
6. Any other business
No issues were discussed under this agenda item.
7. Adoption of the ET 3 meeting minutes
The Meeting agreed that the Secretariat would send out draft ET 3 meeting minutes, accompanied with the documents discussed and revised during the meeting, to the participants on 16 September 2013.
8. Closing of the meeting
The Chair thanked the participants for the very good meeting and Sweden for hosting it.
The Meeting closed on 5 September 2013 at 16:30 hours.
document.docx 2

Reference Annex 1
Title Evaluation Team’s views regarding the Evaluation Consultant’s recommendations and other issues
document.docx 3

Committee of Senior Representatives (CSR)Twenty Second MeetingReykjavik, Iceland16-17 October 2013
Reference CSR 22/6/1
Title Evaluation Team’s views regarding the Evaluation Consultant’s recommendations and other issues
Submitted by Evaluation Team
Summary / Note This document lists the Evaluation Team’s views regarding the Evaluation Consultant’s recommendations. The members’ views and recommendations extending beyond the Evaluation Consultant’s recommendations are also included in the separate table at the end of the document.
Requested action For discussion and decision
document.docx 4

No. Evaluation Consultant’s recommendations/placement (page #) in the reportEvaluation Team’s views
Comments Main responsibility1
Development of a new strategy1 If activities planned are dependent on external actors – like funding agencies – no targets and
indicators should be formulated without explicit knowledge of the conditions laid down by these external actors and without pointing out the challenge that the target is depending on external funding and that this involves a risk (e.g. insert a clause “subject to available funding” (pp 18, 30)
The Evaluation Team supports the recommendation
Strategy Working Group
2 In the new strategy, indicators chosen should be time-bound within the mandate of the strategy (like up until 2020) and should not go beyond that time-frame (pp 15, 30)
The Evaluation Team supports the recommendation
Strategy Working Group
3 In setting up the new strategy, first the political leadership of the partnership has to define needed health areas, set priorities and general goals based on a variety of inputs; afterwards the Expert Groups deal with the development of an operational plan (pp 29-30, 33)
The Evaluation Team supports the recommendation
Partnership Annual ConferenceCommittee of Senior RepresentativesStrategy Working Group
4 Every target and indicator has to be strictly connected to resources. Targets without a resource analysis attached to it should not be formulated. Resources include time, expertise and money. Resource-demands by external obligations – especially the role of NDPHS within the EUSBSR – have to be defined beforehand (pp 15, 32-33)
The Evaluation Team supports the recommendation and proposes an additional recommendation When discussing the new strategy, and more specifically the project-based activities, it is necessary to properly address the issue of the NDPHS’ own co-financing. The Evaluation Consultant
Strategy Working Group
1NDPHS structure(s) to bear the main/direct responsibility for the implementation of a given recommendation. Involvement/contribution(s) of other structure(s) may be necessary.
document.docx 5

touched upon this to some extent in recommendation 4, but did not raise the issue of own-co-financing for projects when NDPHS structures apply for, e.g., EU funds.
5 Every target should have one specific and responsible Expert Group in the lead, with other Expert Groups as secondary contributors (p 15, 32-33)
The Evaluation Team supports the recommendation
Strategy Working Group
6 In order to have sufficient time for the development of the new strategy, the mandate of the current strategy should be extended into 2014 (p 29)
The Evaluation Team supports the recommendation in principle. It suggests the following approach: To focus on the development of the Expert and Task Groups’ Work Plans for 2014 and the extension of their mandates, rather than on the extension of the mandate of the current NDPHS Strategy that includes some Operational Targets, which are either not anymore prioritized or a given group will not be able to implement during 2014.
Committee of Senior Representatives
7 A strategy working-group should be formed, consisting of CSR-members, the leadership of Expert Groups and, if needed, external expertise in planning methods (p 29, 31/32)
The Evaluation Team supports the recommendation
Committee of Senior RepresentativesPartner Countries
8 The proposed process is as follows: 1. EGs are asked to provide input into the development of goals. 2. The strategic working group compares input with the ideas from the CSR and with relevant strategies (EUSBSR, WHO, relevant Russian strategies), 3. Strategy working group provides first documents with vision and goals and prioritization of health-areas, 4. Relevant EGs develop operational plan including indicators, 5. Operational plan is reviewed by strategy
The Evaluation Team supports the recommendation The proposed process and timeline is provided in doc.
Committee of Senior RepresentativesStrategy Working Group
document.docx 6

working group, changes are asked for or made as needed, 6. Resulting comprehensive document is put to the PAC for final decision (p 30)
CSR 22/7.1/1
9 The second strategy should, alongside with the EU Vision 2020, last up until the year 2020 (p 30)
The Evaluation Team supports the recommendation
Committee of Senior RepresentativesStrategy Working Group
10 Important international organizations associated with the NDPHS should explicitly be invited into the strategy-development process (p 39)
The Evaluation Team supports the recommendationThe Evaluation Team will invite the CSR to explicitly invite the respective international organisations.
Committee of Senior Representatives
11 The new strategy should only include goals, targets, indicators and, as an annex, operational plans. It should not include anything in regard to statutes (terms of reference, procedures, administrative issues) (p 29)
The Evaluation Team supports the recommendation
Strategy Working Group
12 Targets should be formulated clearly, short and without description of activities, they should not include many targets in one sentence and shouldn’t mix targets and connected sub-targets (p 31)
The Evaluation Team supports the recommendation
Strategy Working Group
13 Indicators should clearly reflect the target and should have a target-value (p 31) The Evaluation Team supports the recommendation
Strategy Working Group
14 In order to implement their part of the strategy-development, Expert Groups need to have the capacity and competence to implement a logframe-planning-process according to the professional standards, to develop indicators which are SMART and to have the necessary resources in time (pp 31-33)
The Evaluation Team supports the recommendation
Expert/Task Group ChairsLead Countries
15 The secretariat should have its own operational plan in regard to targets and goals of the partnership (p 15)
The Evaluation Team supports the recommendation
Strategy Working Group
16 Do not add new health areas to the strategy. Review if the current ones are all needed (p 33) The Evaluation Team does not support the recommendationPartner Countries react to changing health threats;
document.docx 7

this is an evolving process.17 Aspects of social-wellbeing in projects should be encouraged, if e. g. funding opportunities
allow. Aside from that, if the partnership doesn’t want to put additional resources in this topic, the significance of this area should be presented more diligently in the reporting, but additional and specific activities should not be planned (p 34)
The Evaluation Team supports the recommendation Aspects of social-wellbeing shall be encouraged in the Partnership’s work in all aspects and on all levels, not only projects.
Strategy Working Group
18 Projects and networking/policy advise should continue to be balanced in the new strategy. The definition of project should include the development of reports or documents, not only direct implementation of methods with the target-group. The minimum requirement should be one flagship project per Expert Group, any additional amount should correspond closely with funding opportunities (pp 35-36)
The Evaluation Team supports the recommendation with an additional recommendation:It is suggested that the CSR would adopt a clear-cut definition of a “NDPHS project” (NB. The CSR has already adopted a NDPHS-labelled project” label that can be given to any organization to demonstrate a project’s quality).
Strategy Working Group
19 Decide upon the future of Expert Groups based on a common strategy, not based on individual interests of individual member-states (pp 36-37)
The Evaluation Team supports the recommendation The Evaluation Team supports the recommendation in general, but prefers a positive wording in line with the already existing process, therefore “Not based on individual interests” shall be replaced with “based on shared
Committee of Senior Representatives
document.docx 8

interests”.20 In regard to the AMR group, the growing importance and public anxiety about the topic calls
for a continuation of the group’s activities (pp 36, 47) The Evaluation Team will not provide a view on this recommendation, as this is an issue to be decided upon exclusively by the CSR/PAC
Committee of Senior Representatives
21 In regard to the IMHAP group, the consultant recommends to formally end the operation (pp 37, 47)
The Evaluation Team will not provide a view on this recommendation, as this is an issue to be decided upon exclusively by the CSR/PAC
Committee of Senior Representatives
22 In regard to the PPHS group, the CSR should carefully discuss whether the continuation of the Prison Health topic is worthwhile vis-à-vis existing resources (pp 33/34, 36)
The Evaluation Team will not provide a view on this recommendation, as this is an issue to be decided upon exclusively by the CSR/PAC
Committee of Senior Representatives
Organizational issues in general23 In order to avoid apprehension about information regarded as too unnecessary, presentations
held during EG meetings by representatives of the secretariat should be prediscussed with the chairpersons (p 40)
The Evaluation Team supports the recommendation The recommendation shall be addressed bilaterally between the Expert Groups’ Chairs and the Secretariat
SecretariatExpert Groups’ Chairs
24 Internal information should be better structured, more targeted towards the potential recipient and, if many documents are attached, provided with a short summary (p 40)
The Evaluation Team supports the recommendation
All actors involved in the Partnership
25 If documents for CSR- or other meetings are expected to be late and therefore attending participants will most likely not be able to digest them in time, adjustments in the agenda
The Evaluation Team supports the
Committee of Senior Representatives
document.docx 9

should be made to reflect this issue, as far as possible (p 40) recommendation and proposes additional recommendation: It is proposed that the Committee of Senior Representatives would agree on deadlines for submission of documents to the meetings (can be different deadlines for decision papers and information papers), as well as on the applicable procedures if the deadlines are not respected
26 Efforts should be intensified to reduce the permanent workload of the secretariat in order to increase sustainability of the secretariat’s work. The CSR should furthermore, as the employer of the secretariat, through the chair of the partnership take its responsibility of oversight in this matter seriously (pp 41-42)
The Evaluation Team supports the recommendation
Strategy Working Group (in the context of developing the operational plan of the Secretariat)
27 If Expert Groups are involved in projects, they should concentrate on initiating a project, to a lesser degree in planning and finally in evaluation. Planning is only important as far as in a given area a suitable implementing organization which is also competent in developing a good proposal is missing (p 45)
The Evaluation Team supports the recommendation
Expert Group ChairsLead Countries
28 ITAs should be well trained and experienced in current project-planning methods and the demands of the quality of project-funding organizations. If ITAs do not meet these criteria, they have to be either retrained or replaced (pp 45-46)
The Evaluation Team supports the recommendation The Evaluation Team has agreed on the recommended general scope of ITA’s responsibilities and qualifications required of an ITA (cf. Annex 1)
Expert Group ChairsLead Countries
29 Designate new groups only as task groups, if the task is very specific – like monitoring of a given regulation, the completion of a given project – and doesn’t have any wider implications which can’t be taken up by other Expert Groups. Once the scope of the group widens, these should rightly be described as Expert Groups (p 47)
The Evaluation Team supports the recommendation with
Committee of Senior Representatives
document.docx 10

one addition: Designate and establish new groups as task groups, only if a given task is very specific – like monitoring of a regulation, implementation of a project – and it doesn’t have any wider implications, which can’t be taken up by an Expert Group(s). Once the scope of a group widens, it should rightly be transformed to an Expert Group
30 It is recommended, at least in the long term, to provide NDPHS with a centralized and consolidated budget run by the secretariat covering all income and all expenses (p 49)
The Evaluation Team does not support the recommendation although it recognizes its merit
31 All current targets and indicators should be regularly included in all reports made by the partnership where ongoing activities are discussed, including the minutes of the respective Expert Groups (p 49)
The Evaluation Team supports the recommendation
All actors involved in the reporting
32 Aspects of social wellbeing in the activities and projects of the partnership should be continuously highlighted specifically (pp 34, 50)
The Evaluation Team supports the recommendation
All actors involved in the Partnership
33 The annual report needs a more stringent structure, closely following the new strategy, and needs to be less convoluted and repetitive (p 50)
The Evaluation Team supports the recommendation
Secretariat
34 Annual reports should only be published in a completely edited state, ready for public scrutiny. Draft versions are only for internal consumption (p 50)
The Evaluation Team supports the recommendation with an additional recommendation as spelled out in item 41.
Secretariat
document.docx 11
document.docx 12
Evaluation Team’s recommendations extending beyond the Evaluation Consultant’s recommendations
No. Recommendation Responsibility
35
The concept of side events should be revised. A side-event-programme should be targeted at a wider audience and should also serve as a public-relations-event and inclusion of media-representatives should be considered.
Committee of Senior Representatives
36Partner Countries should try to promote the Health in All Policies approach within their governments also concerning the NDPHS’ work
Partner Countries
37 Further strengthen the NDPHS’ relations with other relevant actors in the region
Chair CountryCommittee of Senior Representatives
38
Develop new approaches for future collaboration within the NDPHS, in order to maximize the benefits and added value of the cooperation within the network
Strategy Working Group
39 Renew the NDPHS mid-term vision Strategy Working Group
40
Develop new approaches to ensure that the relevant results and recommendations from the Expert Groups’ work are conveyed to the policy level, both within the NDPHS and nationally, and taken into account in policy development processes.
Strategy Working Group
41
Decide on the establishment of password-protected area on the NDPHS website to, e.g., publish/discuss/work on draft documents. Decide which sections on the NDPHS website shall be available for the general public and which only for the members of the network. The latter should be used for posting of, e.g., draft/incomplete documents. Upgrade the website accordingly.
Committee of Senior Representatives (decision)Secretariat (implementation)
document.docx 13

ANNEX 1
Proposed general scope of ITA’s responsibilities (the list to be completed with specific issues of relevance to a given EG):
Providing analytical and secretarial support to the EG in collaboration with the EG Chairperson;
Drafting of EG’s documents, including, but not limited to: (i) documents for EG meetings (e.g. discussion papers, work plans and progress reports, policy documents), (ii) meeting minutes; (iii) briefing notes;
Assisting in monitoring the overall progress of activities relevant to his/her EG, stipulated in the operational plan of the NDPHS;
Facilitating the periodic assessments of the EG performance and its functions; Leading and/or providing assistance for development and implementation of log-frame-
planning processes; Assisting in (i) either initiating and evaluating projects or planning and developing
projects, (ii) facilitating applications for project financing and, finally, (iii) implementing projects, if needed;
Networking with other individuals and organizations to ensure wide participation in issues that the Partnership addresses;
Promoting and encouraging the involvement of external actors in the regional health and social well-being activities in collaboration with the EG Chair and members;
Liaising with other relevant regional actors operating in the area covered by the EG to help avoid duplication of efforts between the EG and those actors, as well as to help make proper use of data and material generated by them, where appropriate;
Assisting the EG Chair in arranging EG meetings; Keeping in contact with EG members in-between the meetings; Maintaining continuous dialogue with the NDPHS Secretariat and other NDPHS
expert-level structures to ensure coordination of activities within the Partnership; Participation in other relevant meetings and conferences related to the substance
areas of the EG.
Proposed qualifications required of an ITA (the list to be completed with specific issues of relevance to a given EG):
Advanced university degree (a degree in the area of relevance to the EG will be considered an advantage);
Sufficient and relevant professional experience of which some at the international level and/or a national level with links to the international processes on public health or social issues in the Northern Dimension area (preferably in the areas relating to the EG);
Knowledge and good understanding of the EG’s mandate and activities; Knowledge and good understanding of the work of the EG and the NDPHS in the
context of regional and international health initiatives and processes; Very good co-ordination, networking and organisational skills and experience; Reliable and able to work in an environment with challenging workload and deadlines; Highly-motivated and determined to achieve tangible results; Capacity to work independently and as part of a team; Strong communications skills; Proficiency in project development, facilitation/implementation as well as in fund-
raising; Knowledge of and experience in using logical framework or similar planning tools,
including for identification of problem areas and development of goals, targets, outputs and correct formulation of SMART indicators;
document.docx 14

Excellent command of oral and written English with several years of practical experience. Excellent drafting skills in English;
Computer literacy – very good user skills in Internet as well as word processing software and hardware.
document.docx 15

Reference Annex 2
Title Development of the NDPHS Strategy beyond 2013
document.docx 16

Committee of Senior Representatives (CSR)Twenty Second MeetingReykjavik, Iceland16-17 October 2013
Reference CSR 22/7.1/1
Title Development of the NDPHS Strategy beyond 2013
Submitted by Secretariat
Summary / Note The current NDPHS Strategy expires in 2013. To that end, the CSR 21 Meeting requested the Secretariat to prepare, with input from the Evaluation Team, a discussion document regarding the process and aspects to take into consideration while developing the NDPHS Strategy beyond 2013 (NDPHS Strategy 2014-2020).
The present discussion document takes into account respective recommendations included in the Evaluation Report prepared by the Evaluation Team Consultant. As requested by the CSR, it has been discussed by the Evaluation Team (ET) and the ET’s comments have been included in it. The main focus of this discussion document is on the process of the development of the NDPHS Strategy 2014-2020, rather than its content.
Requested Action For decision
It is proposed that the Committee of Senior Representatives consider and decide upon the following issues relating to the development of a new NDPHS Strategy:
1. Prolongation, where relevant, of the mandates of the Expert and Task Groups
Background
The Goals, operational targets and indicators of the current NDPHS Strategy are valid until the end of 2013. Linked to them are the Terms of Reference of the eight NDPHS Expert and Task Groups, which are also valid until 2013.
Excerpts from the Evaluation Report 2013
Recommendation No. 6: In order to have sufficient time for the development of the new strategy, the mandate of the current strategy should be extended into 2014;
Recommendation No. 20: In regard to the AMR group, the growing importance and public anxiety about the topic calls for a continuation of the group’s activities;
Recommendation No. 21: In regard to the IMHAP group, the consultant recommends to formally end the operation;
Recommendation No. 22: In regard to the PPHS group, the CSR should carefully discuss whether the continuation of the Prison Health topic is worthwhile vis-à-vis existing resources.
Issues for discussion and decision
document.docx 17

Extension, where relevant, of the mandates of the current NDPHS Expert and Task Groups until the new mid-term Strategy is adopted and enters into force. In this regard, recommendations No. 20-22, quoted above, are relevant.
Adoption of EG/TG Work Plans for 2014 (included/to be included in a NDPHS Work Plan for 2014). To that end the following excerpt from the NDPHS Work Plan for 2013 should be recalled:
o “(2.5) Plan the implementation process beyond 2013.
NDPHS Expert Groups and Task Groups to be in operation beyond 2013: develop annual work plans for 2014. These plans will be elaborated consistent with the Elements for the development of NDPHS EG/TG Annual Work Plans and shall specify the methods, milestones and resources with which the respective objectives will be pursued and achieved during 2014.”
2. Establishment of the Strategy Working Group
Background
In 2009 the Strategy Working Group led by Sweden and consisting of the representatives of Canada, Finland, Germany, Lithuania, Norway, Poland, Russia and the NDPHS Secretariat, developed the current NDPHS Strategy.
Excerpt from the Evaluation Report 2013
Recommendation No. 7: A strategy working-group should be formed, consisting of CSR-members, the leadership of Expert Groups and, if needed, external expertise in planning methods.
Issues for discussion and decision
Establishment of a Strategy Working Group (SWG) (including its composition); Adoption, of the SWG Terms of Reference (ToR). First draft of the ToR is enclosed (cf.
Annex 1).
3. Political priorities in the new Strategy
Background
The current Strategy covers four thematic areas: (1) Containing the spread of HIV/AIDS and tuberculosis; (2) Accessibility and quality of primary health care; (3) Prison health care policy and services; (4) Lifestyle-related non-communicable diseases and good social and work environments, and lists 12 goals:
Goal 1: The role and working methods of the NDPHS are strengthened; Goal 2: Prevention of HIV/AIDS and associated infections in the ND-area has
improved; Goal 3: Social and health care for HIV infected individuals in the ND area is integrated;Goal 4: Resistance to antibiotics is mitigated in the ND area;Goal 5: Inequality in access to qualified primary health care in the ND area is reduced;Goal 6: Health and other related needs of people kept in places of detention are readily
met, access to the health services is improved, and gender specific needs are addressed;
Goal 7: The impact in the ND countries on society and individuals of hazardous and harmful use of alcohol and illicit drugs is reduced;
document.docx 18

Goal 8: Pricing, access to and advertising of alcoholic beverages is changed to direction, which supports the reduction of hazardous and harmful use of alcohol;
Goal 9: Tobacco use and exposure to tobacco smoke is prevented and reduced in the ND area;
Goal 10: The NDPHS Strategy on Health at Work is implemented in the ND area;Goal 11: Public health and social well-being among indigenous peoples in the ND area
is improved;Goal 12: The impact of all main causes / risk-factors of lifestyle related NCDs in the ND
countries are addressed (in addition to alcohol and tobacco targeted through Goals 7-9): overweight, low fruit and vegetable intake, trans fat avoidance, high salt-intake, insufficient vitamin-D intake, high blood pressure, high blood cholesterol, low physical activity (sedentary lifestyle), and factors related to mental health problems.
Excerpts from the Evaluation Report 2013
Recommendation No. 3: In setting up the new strategy, first the political leadership of the Partnership has to define needed health areas, set priorities and general goals based on a variety of inputs; afterwards the Expert Groups will deal with the development of an operational plan.
Recommendation No. 4: Every target and indicator has to be strictly connected to resources. Targets without a resource-analysis attached to it should not be formulated. Resources include time, expertise and money. Resource-demands by external obligations – especially the role of NDPHS within the EUSBSR – have to be defined beforehand.
Recommendation No. 16: Do not add new health areas to the strategy. Review of the current ones are all needed.
Issues for discussion and decision
“Setting priorities in the new NDPHS Strategy” has been included as an item on the draft agenda of the forthcoming ministerial-level PAC (cf. agenda item 4.3). Political guidance provided by the ministers during the PAC will serve as the point of departure when developing the NDPHS Strategy 2014-2020. To prepare the ministerial discussion, the following procedure is proposed:
16-17 October 2013 CSR holds first, preliminary discussion on priorities (headlines) for the NDPHS Strategy 2014-2020
Until 1 Nov. 2013 Submission, by NDPHS Partners, of inputs to a background paper specifying suggested headlines for the NDPHS Strategy 2014-2020
Until 5 Nov. 2013 The Secretariat compiles the received contributions into a PAC document and disseminates it
4. Ownership and quality issues
Excerpts from the Evaluation Report 2013
The development process of the (current) mid-term strategy has not been perfectly designed to fulfil both the needs for a certain standard of quality management as well as the inclusion of all Expert Groups in order to achieve ownership (page 6);
The consultant is doubtful at this time if all Expert Groups are in a position to meet the relevant quality standards. In order to develop an operational plan according to these standards, it is necessary that
document.docx 19

- Expert Groups have the competence and capacity to understand, develop and implement a logframe-planning-process according to the professional standards of using this method;
- Expert Groups have the competence and capacity to understand and develop indicators, which fully live up to the criteria of being SMART (specific, measurable, achievable, relevant and timebound).
- Expert Groups have the necessary resources to present their operational plans within a given time-frame and are available for revision and comments after their proposals have been scrutinized by a strategy working-group.
If these three preconditions are not fully met, the process of development is in serious danger. If any Expert Group finds itself in doubt in regard to these competences, it will either be necessary to retrain at least the ITA so that he/she will be capable of conducting the planning process properly or to find external expertise that will be able to fulfil that task. If the Expert Group will not be capable of providing the necessary input according to quality standards and in time, the consequence will be that- the strategy working group will be forced to take over planning of the operational
targets and indicators by itself in order to be able to finalize the document in time and consequently
- the Expert Groups affected might suffer the same lack of ownership in regard to the targets like during the last five years.
Expert Groups should take this exercise as a good chance to remedy perceived shortcomings of the development of the first mid-term strategy. For this, considerable effort from their side is to be expected.
In addition, the strategy working-group needs to include the relevant competence as outlined above as well in order to be able to scrutinize the quality of the proposals submitted by the Expert Groups and, if they are lacking, to be able to fill the gaps by itself, if necessary. The composition of the strategy working-group should reflect this (pages 31-32).
Issues for discussion
How to assess (and who should do it) the capability of the Expert Groups and the Strategy Working Group members to develop the new Strategy and how to identify gaps in capacity and training needs (e.g., through a self-assessment), if necessary;
How to address the identified gaps (e.g., by training, involving external expertise) and how to finance the proposed solutions.
5. Timeline for the development of the new Strategy1
Excerpt from the Evaluation Report 2013
The setup of the second mid-term strategy embodies all the chances and possible pitfalls of the future development of NDPHS and needs careful management. Rushing it in order to meet unrealistic deadlines will not be helpful. It will be better to do things thoroughly and in an inclusive way, as this will enhance the quality of the new strategy as well as its effectiveness (page 51).
Proposed timeline (for adoption)This is a very challenging timeframe. But in order to proceed in time it seems to be the best way forward.
1 Latvia does not support the proposed timeline
document.docx 20

16-17 October 2013 Decision on the establishment of a Strategy Working Group (SWG) and adoption of the Terms of Reference (ToR) for itCSR nominates the SWG members and holds first, preliminary discussion on priorities (headlines) for the NDPHS Strategy 2014-2020
Until 1 Nov. 2013 Nomination of the SWG members Submission, by NDPHS Partners, of inputs to a background paper specifying suggested headlines for the NDPHS Strategy 2014-2020
Until 5 Nov. 2013 The Secretariat compiles the received contributions into a PAC document and disseminates it
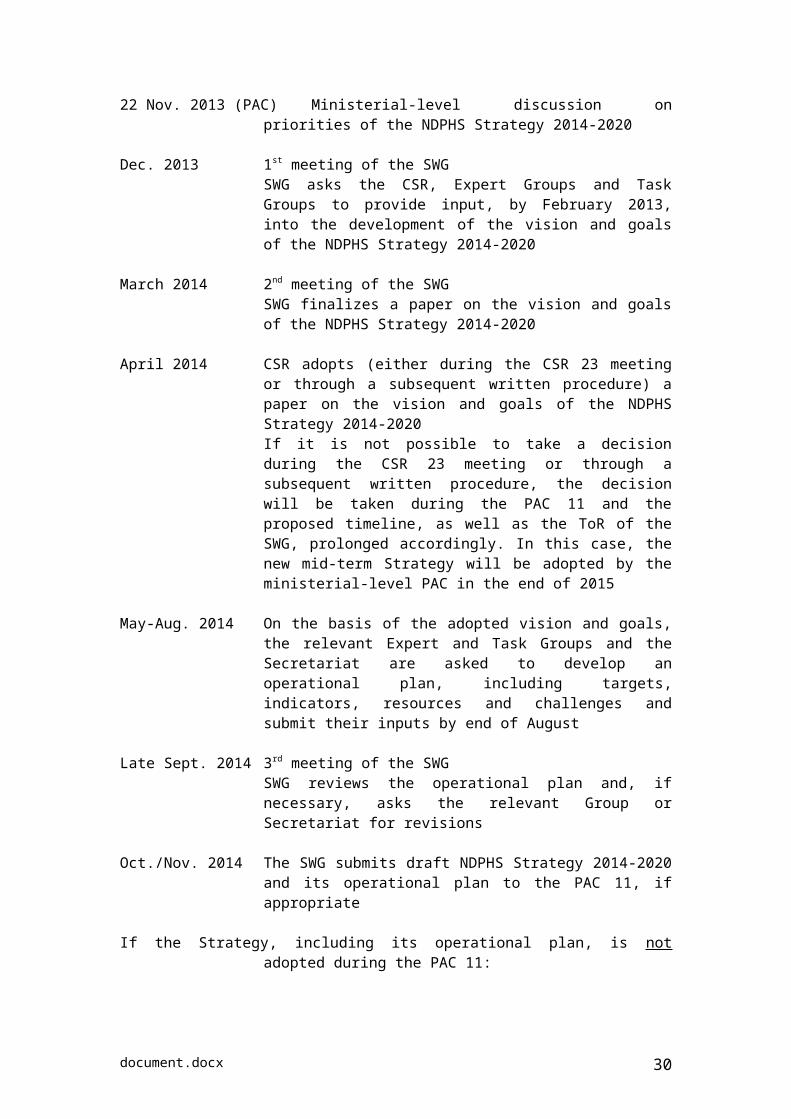
22 Nov. 2013 (PAC) Ministerial-level discussion on priorities of the NDPHS Strategy 2014-2020.
Dec. 2013 1st meeting of the SWGSWG asks the CSR, Expert Groups and Task Groups to provide input, by February 2013, into the development of the vision and goals of the NDPHS Strategy 2014-2020
March 2014 2nd meeting of the SWGSWG finalizes a paper on the vision and goals of the NDPHS Strategy 2014-2020
April 2014 CSR adopts (either during the CSR 23 meeting or through a subsequent written procedure) a paper on the vision and goals of the NDPHS Strategy 2014-2020If it is not possible to take a decision during the CSR 23 meeting or through a subsequent written procedure, the decision will be taken during the PAC 11 and the proposed timeline, as well as the ToR of the SWG, prolonged accordingly. In this case, the new mid-term Strategy will be adopted by the ministerial-level PAC in the end of 2015
May-Aug. 2014 On the basis of the adopted vision and goals, the relevant Expert and Task Groups and the Secretariat are asked to develop an operational plan, including targets, indicators, resources and challenges and submit their inputs by end of August
Late Sept. 2014 3rd meeting of the SWGSWG reviews the operational plan and, if necessary, asks the relevant Group or Secretariat for revisions
Oct./Nov. 2014 The SWG submits draft NDPHS Strategy 2014-2020 and its operational plan to the PAC 11 for adoption, if appropriate
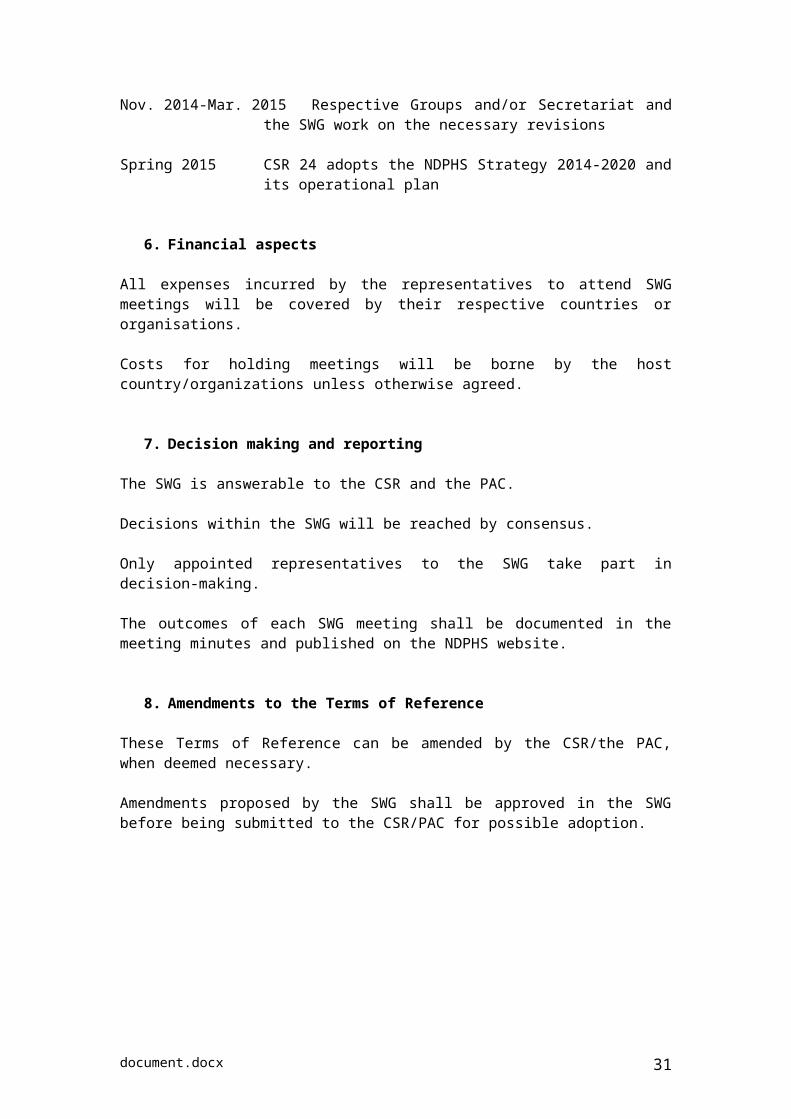
If the Strategy, including its operational plan, is not adopted during the PAC 11:
Nov. 2014-Mar. 2015 Respective Groups and/or Secretariat and the SWG work on the necessary revisions
Spring 2015 CSR 24 adopts the NDPHS Strategy 2014-2020 and its operational plan
6. Resources for the development of the NDPHS Strategy 2014-2020
document.docx 21
The following resources need to be made available for the development of the new mid-term Strategy:
1) Working time of the Expert Group and Strategy Working Group (SWG) members;2) Travel costs of the SWG members to attend the SWG meetings;3) Training and/or involvement of external expertise to ensure that inputs from the Expert
Groups meet quality standards, if deemed necessary, and to provide advice on the methodology to the SWG.
Issues for discussion
Whether Partners are ready to allocate the necessary resources, including for training and involvement of external expertise.
document.docx 22

ANNEX 1
Proposed Terms of Reference and Timelinefor the NDPHS ad hoc Working Group for the Development of a NDPHS
Strategy 2014-2020 (Strategy Working Group, SWG)
Adopted by the CSR on 16-17 October 2013
1. Background
Consistent with the NDPHS Strategy stipulating the need to carry out an “evaluation approximately every five years, which would be aided by an external consultant”, the NDPHS had established an Evaluation Team. The Team conducted the evaluation with the inputs of the NDPHS Partners and the inputs and support of an independent consultant appointed by the CSR. The results of the Evaluation Team and the Evaluation Team’s Consultant work were presented to the CSR 22 meeting on 16-17 October 2013 in Reykjavik, Iceland.
Having considered the presented recommendations and proposals, the CSR decided to establish an ad hoc Strategy Working Group to help develop the NDPHS mid-term Strategy 2014-2020 (hereinafter the NDPHS Strategy 2014-2020).
2. Scope
The main task of the SWG is to facilitate the development of the NDPHS Strategy for the period 2014-2020 and act as the focal point for inputs from the NDPHS Partner Countries and Organisations, the Participant and the Expert and Task Groups. In this capacity, the SWG has the overall objective to produce a draft NDPHS Strategy 2014-2020, including its operational plan, and present it to the PAC 11 in 2014.
The SWG will address Recommendations No. 1-5; 8-13; 15; 17-18; 26 of the consultant’s report, as well as additional recommendations agreed upon during the CSR 22 meeting (Appendix 1).
The SWG will not address issues that have already be decided by the CSR 22 or shall be decided exclusively by the CSR or the PAC, such as:
- Extension of the mandate of the current Strategy (Recommendation No. 6)- Establishment of the Strategy Working Group (Recommendation No. 7)- Ensuring capacity and competence of the Expert Groups to implement a
logframe-planning-process according to the professional standards (Recommendation No. 14)
- Deciding upon the establishment or dissolution of Expert and Task Groups (Recommendations No. 19-22).
document.docx 23
3. Composition [preferably to be decided before PAC 10]
The SWG will be composed of:
CSR members representing the Chair and Co-Chair country; Representatives from other NDPHS Partner and Participant countries; At least one representative from the European Commission and the WHO; Representatives of other Partner Organisations that wish to join in At least one representative of the leadership (Chair, co-Chair or ITA) of a
NDPHS Expert Group; The NDPHS Secretariat.
The SWG members will elect a SWG Chairperson from among themselves. The NDPHS Secretariat will provide a technical support to the SWG Chairperson.
3.a Support from an external consultant
In performing its tasks the SWG shall be/may be supported by an external consultant providing methodical advice in planning processes. Engagement of the consultant shall be without financial consequence for the NDPHS annual budget.
4. Outputs
The following outputs will be delivered by the SWG:
Paper on the vision and goals of the NDPHS Strategy 2014-2020 to be submitted to the CSR 23 Meeting in spring 2014;
Draft NDPHS Strategy 2014-2020, including its operational plan, to be submitted to the PAC 11 meeting in autumn 2014, either for adoption or comments. In the latter case, final draft strategy, including its operational plan, to be submitted to the CSR 24 Meeting in spring 2015.
5. Timeframe1
The mandate of the SWG is valid from 17 October 2013 until the adoption of the NDPHS Strategy 2014-2020.
22 Nov. 2013 (PAC) Ministerial-level discussion on priorities of the NDPHS Strategy 2014-2020
Dec. 2013 1st meeting of the SWGSWG asks the CSR, Expert Groups and Task Groups to provide input, by February 2013, into the development of the vision and goals of the NDPHS Strategy 2014-2020
March 2014 2nd meeting of the SWGSWG finalizes a paper on the vision and goals of the NDPHS Strategy 2014-2020
1 Latvia does not support the proposed timeframe
document.docx 24

April 2014 CSR adopts (either during the CSR 23 meeting or through a subsequent written procedure) a paper on the vision and goals of the NDPHS Strategy 2014-2020If it is not possible to take a decision during the CSR 23 meeting or through a subsequent written procedure, the decision will be taken during the PAC 11 and the proposed timeline, as well as the ToR of the SWG, prolonged accordingly. In this case, the new mid-term Strategy will be adopted by the ministerial-level PAC in the end of 2015
May-Aug. 2014 On the basis of the adopted vision and goals, the relevant Expert and Task Groups and the Secretariat are asked to develop an operational plan, including targets, indicators, resources and challenges and submit their inputs by end of August
Late Sept. 2014 3rd meeting of the SWGSWG reviews the operational plan and, if necessary, asks the relevant Group or Secretariat for revisions
Oct./Nov. 2014 The SWG submits draft NDPHS Strategy 2014-2020 and its operational plan to the PAC 11, if appropriate
If the Strategy, including its operational plan, is not adopted during the PAC 11:
Nov. 2014-Mar. 2015 Respective Groups and/or Secretariat and the SWG work on the necessary revisions
Spring 2015 CSR 24 adopts the NDPHS Strategy 2014-2020 and its operational plan
6. Financial aspects
All expenses incurred by the representatives to attend SWG meetings will be covered by their respective countries or organisations.
Costs for holding meetings will be borne by the host country/organizations unless otherwise agreed.
7. Decision making and reporting
The SWG is answerable to the CSR and the PAC.
Decisions within the SWG will be reached by consensus.
Only appointed representatives to the SWG take part in decision-making.
The outcomes of each SWG meeting shall be documented in the meeting minutes and published on the NDPHS website.
8. Amendments to the Terms of Reference
document.docx 25
These Terms of Reference can be amended by the CSR/the PAC, when deemed necessary.
Amendments proposed by the SWG shall be approved in the SWG before being submitted to the CSR/PAC for possible adoption.
document.docx 26

APPENDIX 1
List of all recommendations to be addressed bythe NDPHS ad hoc Strategy Working Group (SWG)
(NB. This list will need to be updated taking into account the CSR conclusions)
I. Recommendations from the consultant’s report
R1. If activities planned are dependent on external actors – like funding agencies – no targets and indicators should be formulated without explicit knowledge of the conditions laid down by theseexternal actors and without pointing out the challenge that the target is depending on external funding and that this involves a risk (e.g. insert a clause “subject to available funding”).
R2. In the new strategy, indicators chosen should be time-bound within the mandate of the strategy (like up until 2020) and should not go beyond that time-frame.
R3. In setting up the new strategy, first the political leadership of the partnership has to define needed health areas, set priorities and general goals based on a variety of inputs; afterwards the Expert Groups deal with the development of an operational plan.
R4. Every target and indicator has to be strictly connected to resources. Targetswithout a resource analysis attachedto it should not be formulated. Resources include time, expertise and money. Resource-demands by external obligations – especially the role of NDPHSwithin the EUSBSR – have to be defined beforehand.
R5. Every target should have onespecific and responsible Expert Group in the lead, with other Expert Groups as secondary contributors.
R8. The proposed process is as follows: 1. EGs are asked to provide input into the development of goals. 2. The strategic working group compares input with the ideas from the CSR and with relevant strategies (EUSBSR, WHO, relevant Russian strategies), 3. Strategy working group provides first documents with vision and goals and prioritization of health-areas, 4. Relevant EGs develop operational plan including indicators, 5.Operational plan is reviewed by strategy working group, changes are asked for or made as needed, 6. Resulting comprehensive document is put to the PAC for final decision.
R9. The second strategy should, alongside with the EU Vision 2020, last up until the year 2020.
R10. Important international organizations associated with the NDPHS should explicitly be invited into the strategy-development process.
R11. The new strategy should only include goals, targets, indicators and, as an annex, operational plans. It should not include anything in regard to statutes (terms of reference, procedures, administrative issues).
R12. Targets should be formulatedclearly,short and without description of activities, they should not include many targets in one sentence and shouldn’t mix targets and connected sub-targets.
R13. Indicators should clearly reflect the target and should have a target-value.
document.docx 27

R15. The secretariat should have its own operational plan in regard to targets and goals of the partnership.
R17. Aspects of social-wellbeing in projects should be encouraged, if e.g. funding opportunities allow. Aside from that, if the partnership doesn’t want to put additional resources in this topic, the significance of this area should be presented more diligently in the reporting, but additional and specific activities should not be planned.
R18. Projects and networking/policy advise should continue to be balanced in the new strategy. The definition of project should include the development of reports or documents, not only direct implementation of methods with the target-group. The minimum requirement should be one flagship project per Expert Group, any additional amount should correspond closely with funding opportunities.
R26. Efforts should be intensified to reduce the permanent workload of the secretariat in order to increase sustainability of the secretariat’s work. The CSR should furthermore, as the employer of the secretariat, through the chair of the partnership take its responsibility of oversight in this matter seriously.
II. Additional recommendations (including from the Evaluation Team)
a) Develop new approaches for future collaboration within the NDPHS, in order to maximize the benefits and added value of cooperation within the network.
b) Renew the NDPHS mid term vision.
c) Develop new approaches to ensure that the relevant results and recommendations from the Expert Groups’ work are conveyed to the policy level, both within the NDPHS and nationally, and taken into account in policy development process.
d) Define what a “NDPHS project” is.
document.docx 28
Reference Annex 3
Title List of documents submitted to the meeting
Summary / Note This list includes all documents submitted to the meeting
Main documents
Code Title Submitted by Date
ET2013 3/2/1 Provisional agenda with timetable Secretariat 30/07/13
ET2013 3/2/2 Provisional annotated agenda Secretariat 05/08/13
ET2013 3/3/1 Independent Evaluation of the NDPHS 2013
Evaluation Consultant 05/08/13
ET2013 3/4/1 Development of the NDPHS Strategy beyond 2013 Secretariat 29/08/13
ET2013 3/4/2Proposed general scope of ITA’s responsibilities and qualifications required of an ITA
Secretariat 29/08/13
ET2013 3/4/Info 1
Evaluation Team’s members’ preliminary views regarding the Evaluation Consultant’s recommendations and other issues proposed for discussion during the meeting
Secretariat 29/08/13
Auxiliary documents
Code Title Submitted by Date
ET2013 3/Info 1 Practical information for participants Secretariat 07/05/13
ET2013 3/Info 2 Preliminary timetable Secretariat 17/07/13
ET2013 3/Info 3 List of documents Secretariat 05/08/13
ET2013 3/Info 3/Rev 1 Revised list of documents Secretariat 29/08/13
ET 2013 3/Info 4 Preliminary list of participants Secretariat 28/08/13
document.docx 29
Reference Annex 3
Title List of participants
Summary / Note This list includes all persons who attended the meeting
Germany (Chair)
Mr. Thomas IflandSenior AdvisorGerman Ministry of HealthRochusstrasse 153123 BonnGermanyPhone: +49 228 9413311E-mail: [email protected]
Finland (co-Chair)
Dr. Marja AnttilaSenior ExpertNational Institute for Health and WelfareP.O.BOX 3000271 HelsinkiFinlandPhone: +358 295 247045Fax: +358 97732922E-mail: [email protected]
Latvia
Ms. Agnese RabovičaDirector of European Affairs and International Cooperation DepartmentCivil ServantBrivibas street 72LV-1010 RigaLatviaPhone: +371 67876060Fax: +371 67876002E-mail: [email protected]
Norway
Dr. Andreas SkulbergMinistry of Justice and Public Security Deputy Director GeneralMember of the PPHS EGGullhaug torg 4a0030 OsloNorwayPhone: +47 97 65 34 05Fax: +47 22245580E-mail: [email protected]
Russia
Dr. Eduard SalakhovHead of Unit for International Cooperation in Public HealthMinistry of HealthRakhmanovsky per., 3127994 MoscowRussian FederationPhone: +7 495 627 26 24Fax: +7 495 621 86 03E-mail: [email protected]
Sweden
Ms. Karin BerlinHead of SectionDivision of EU and International AffairsFredsgatan 810333 StockholmSwedenPhone: +46 8 405 15 61Fax: +46 8 21 78 76E-mail: [email protected]
Expert Group on HIV/AIDS and Associated Infections
Dr. Ali ArsaloHIV/AIDS&AI EG Chair Kuusijärventie 11699510 RaudanjokiFinlandPhone: +358 50 5376265Fax: +358 16 633303E-mail: [email protected]
CEval
Prof. Dr. Dirk van den BoomConsultantCEvalLehmkaulweg 1566119 SaarbrueckenGermanyPhone: +49 681 6853887E-mail: [email protected]
document.docx 30
NDPHS Secretariat
Mr. Marek MaciejowskiDirector of SecretariatSlussplan 9SE-111 30 StockholmSwedenPhone: +46 735 405900E-mail: [email protected]
Ms. Silvija Juscenko Senior AdviserSlussplan 9SE-111 30 StockholmSwedenPhone: +46 760 219544E-mail: [email protected]
document.docx 31