Embed Size (px)
Citation preview

1
Vision and DrivingSeeing Your Way to Better Client Outcomes
Beth Rolland, OTR, CDRS
What is Vision
The primary sense that we use to acquire information about our environment.
IncludesEye movementAcuityPerception
Vision Facts
90% of the information we gather comes from the visual system.
Vision allows us to be anticipatoryThe visual system is the fastest and
most complicated of all sensory systems.
50% of all neurologic insults cause visual deficits.
Vision Facts
Eye is the only organ in the body innervated by both the central and autonomic nervous systemsCentral – voluntary movements
(pursuits, saccades, lid opening/closing)Autonomic – involuntary control (pupil
constriction and dilation)
Vision Facts
The visual system provides the highest level of sensory information processing in the human body and is the most highly integrated of all systems.
It is estimated that 65% of all nerve fiber interactions with the brain have something to do with the visual information processing system.
Anatomy of the EyeAn Overview

2
Anatomy of the EyeEye Structure & Function
Eye parts resemble a camera Sclera - white outer protective coat; the
"white of the eye". Cornea - transparent, curved structure in
front Iris - colored part seen through the cornea. Pupil - black part in the middle of the iris.
Constricts or dilates according to the amount of light passing through.
Lens - transparent disc (with both sides being convex) immediately behind the iris and pupil.
Eye Structure & Function
Aqueous humour - transparent fluid (water consistency) circulates behind cornea and in front of the lens.
Vitreous humour – fills the eyeball between lens and retina (like transparent jelly).
Retina - light-sensitive layer of millions of nerve cells lining back of the eyeball. Rod cells – tall, thinCone cells - rounder
Eye Structure & Function
Rods - more numerous, mostly at outer edgerespond to low levels of light, peripheral
movement. Cones - far fewer, concentrated in center
respond to color and details. Macula - small center of the retina
responsible for central vision—ie: reading. Retinal pigment epithelium – dark layer of cells at
back of retina Provide oxygen & nutrients to rods/cones.
Eye Structure & Function
Choroid - large network of blood vessels (behind the retina) transport oxygen & nutrients to retinal pigment
cells. Optic disc - small yellow oval structure in retina
nerve cell connections travel from all the rods and cones.
Optic nerve and beyond - "cord" of nerve cell connections that passes from eyeball to destinations throughout brain.
Eye Structure & Function
Retina –located at the back of the eye and connected
to the brain. made up of many millions of light-sensitive cells
known as photoreceptor cells which transmit electrical impulses to the brain to enable sight.

3
Cranial Nerves
Cranial Nerve II (Optic Nerve)Originates at the RetinaConnected to the specialized receptors
in the retina—the rods and cones.Exits the back of the eye in the orbitWhere the optic nerve tract begins.
Cranial Nerve II (cont.)
The optic nerve has only a special sensory component
Visual information enters the eye in the form of photons of light
Light is converted to electrical signals in the photoreceptors (rods and cones) located in the retina
Signals travel optic nerves, chiasm, and tract lateral geniculate nucleus (thalamus) occipital lobe (visual centers)
Cranial Nerves
Cranial Nerve III (Oculamotor Nerve)Raises eyelid and controls pupils
Drooping eyelid = ptosis
Controls several key eye muscles. These muscles include the following: Superior Rectus: the ocular muscle whose contraction turns
the eyeball upward and medially Inferior Rectus: the ocular muscle whose contraction turns
the eyeball down and medially
Cranial Nerve III (cont.)
Medial Rectus: the ocular muscle whose contraction turns the eyeball medially
These muscles are an integral part of how well and how smoothly your eyes move.
Cranial Nerves
Cranial Nerve IV (Trochlear Nerve) Purely motor nerve supplying one muscle: Superior oblique: Intorsion-
inward rotation of upper part of eye about an axis or a fixed point. Secondary movement-moves
eye out and down.Damage results in eye slightly
elevated in primary gaze position (straight ahead gaze)
Cranial Nerves
Cranial Nerve VI (Abducens Nerve)Lateral Rectus:
Pulls the eye away from the nose
Damage to this nerve will result in the affected eye turning inward (cross eye)Intermittent double vision in lateral gazeEffect of esotropia is greater at distanceReading ok, driving a problem

4
Cranial Nerve Summary
Nerve Nerve supplies Function Clinical observations
CNIII- oculomotor Upper eyelidSR, IR, MR, IOCiliary MuscleSphincter of Iris
Eyelid movementEyeball movement-up,down, and mediallyPupil constriction
PtosisExotropia (down&out)Diplopia at nearNo pupil accomodation
CNIV-trochlear Superior obique Eyeball movement- downand out
Hypertropia/phoriaVertical diplopiaLateral tilt of head
CNVI- abducens Lateral rectus Eyeball movementoutwards
Esotropia/phoriaDiplopia at distance
Eye Anatomy Videos
Dr. Tim Roothttps://timroot.com/anatomy-of-the-eye-
video/Anatomy videoNeuro-anatomy Functional Vision
Hierarchy of Visual Adaptation
Oculamotor Control (pursuits, saccades)
Visual AttentionVisual ScanningPattern RecognitionVisual MemoryVisuo-Cognition (perception)Adaptation (thought, reasoning)
Oculamotor Control
Visual Fixation - ability to find target and hold eyes on it
Pursuits – ability to follow a moving target (without head movement)
Saccades – rapid eye movements in any direction (without head movement)
Implication for driving: if you can’t see it, you can’t respond to it!; objects are moving in driving environment – pedestrians, bicycles, cars

5
Visual AttentionCognitive componentAbility to pick out relevant information in an
environment and suppress irrelevant informationSustained attention – maintain over timeShifting attention – change focus from one thing to
another rapidlyDivided attention – attend to multiple factors at
once (ie: hazards on both right and left side)
Implication for driving: if you are not paying attention, you will miss things
Visual Scanning
Visual Scanning – ability to find things in the environment
Peripheral Vision – what can be seen on the side without head or eye movementNot clear, but brain fills in and seems clear Alerts to movement – prompts saccade or head
turn to use central vision for more information
Implication for driving: hazards come from all fields; inadequate scan will miss things
Visual Fields – Peripheral Vision
Norms: 65 degrees upward
70 degrees downward
60 degrees nasally
90-110 degrees temporally
Pattern Recognition
Cognitive process that matches information from a stimulus with information retrieved from memory Allows anticipatory awareness
Implication for driving: if you don’t anticipate, you will respond late
Visual Memory
Recollected information about what one has seen. Mental storage of informationAbility to retrieve stored information
Implication for driving: deficit may lead to difficulty finding your way, finding your car in a lot, remembering what was on the left when you scan right
Visuo-Cognition (perception)
Ability to process and interpret meaning from visual information gained through eye sight visual discrimination visual figure ground – distinguishing object from background visual closure – “seeing” the whole from a part visual memory – recalling what you saw visual form constancy – recognizing objects when they are
turned around visual spatial relationships – where one thing is in relation to
another visual-motor integration – eye/hand coordination

6
Visual Perception
Implication for driving: Poor lane position
Unsure where they are relative to parked cars, lanes Unable to coordinate steering movements quickly enough
to maintain straight path Improperly placed turns
Unsure where to start turn – especially lefts Unsure where curve starts for rights
Poor sign recognition (ie: branch over stop sign) Difficulty driving at night (poor contrast)
Other Crucial Vision Skills
Visual Acuity
Ability to focus either near or farExpressed as a fraction
Numerator: testing distance at which stimulus is recognized
Denominator: distance at which letter being viewed could be recognized by a person with normal visual acuity (20/20)
Implication for driving: state laws for minimum; inability to read signs or see road details
Visual Acuity
Includes Contrast Sensitivity Ability to see objects of decreasing contrast rather than size
High contrast: black on white, etc. Low Contrast: grey on white; white on white, etc.
Contrast Sensitivity has been linked to crash risk
Implication for driving: difficulty driving at night, dusk or dawn; difficulty seeing items against same color background (green car with green bushes)
Contrast Sensitivity Binocular Vision
Combining images from each eye into single image. Images must fall precisely on corresponding positions on
each retina or double vision will occur. Muscles work together to position eyes properly to focus
light on center of each eye, providing clear vision.

7
Binocular and Stereoscopic Vision
Binocular Vision
Focusing near - eyes move closer together (convergence)
Focusing far - the eyes move further apart (divergence)
Misalignment of eyes – double vision Double vision usually either near OR farMuscle weakness pulls eye opposite
May be in one gaze (ie: far left gaze) May be constant
Implication for driving: blurry vision, motion sickness, inability to accurately judge space
Stereoscopic Vision
Depth Perception Slight difference in angles of images received in each eye gives
images depth Loss or suppression of one eye affects depth
Do use other cuesLight, shade, shadows, color and relative
sizes of objects contribute to depth Cognitive component - learn the signs
that enable them to perceive depth.
Implication for driving: difficulty judging space and speed
Binocular and Stereoscopic Vision
People think and learn best in three dimensions. When scanning text quickly, we can absorb 100
letters per second - the computer equivalent of 100 bits per second.
When glancing at a three-dimensional object, we can see the equivalent of 1 billion bits per second.
Implication for driving: good binocular vision lets you see faster and react faster on the road
Vision Screen
Visual History
Patient complaints (diplopia, blurred vision, dizziness, headaches, eye fatigue, balance difficulties)
Optical History (cataracts, glaucoma, diabetes, macular degeneration, surgery)

8
Evaluating Far Acuity
*Must pass state standard for vision in state they hold license
Options:Optec Vision Tester – quick and easy; also
tests contrast sensitivity, alignment, depth, color, road sign recognition
Snellen or Lea Chart – cheap and easy
Evaluating Far Acuity
Test each eye separately and then together (Optec tests separately with both eyes working)Many states have requirements that
both eyes pass the standardTesting separately lets you know which
eye has an issue
Visual Acuity
Equipment Select appropriate assessment tool (Optec,
Snellen chart/ Lea symbols)
Evaluating Far Acuity
Optec ProcedureClient wears corrective lenses for distanceBegin at 20/40 line
Left eye sees left column; right eye sees right column; both eyes see middle column
If client does not start with left column, turn off right eye and have them try again
If client does not read right column, turn off left eye
Evaluating Far Acuity
OptecInstruct client to read down to last line
they can make outFar acuity is last line where 3 out of 4
letters in the column are identified correctly
If the client has aphasia, try giving them a piece of paper and pencil to write the letters
Evaluating Far Acuity
Snellen Chart (or Lea Chart) ProcedureStand 10 or 20 feet away (based on chart)Client wears corrective lenses for distanceTest monocularly then binocularlyBegin at 20/40 line (or line required by state of
license)If patient has difficulty, isolate lines

9
Evaluating Far Acuity
Snellen ChartUse Lea symbols if client has aphasiaFar acuity is last line where 75% or
more of letters are identified correctly
Evaluating Far Acuity
A large discrepancy between eyes can lead to suppression and will affect depth Two line discrepancy – refer to a vision specialist
Older patients often have cataracts, which affect acuity May not meet state standard for vision
Evaluating Far Acuity
Some folks have trouble with Optec If not meeting standard in Optec, try Snellen
**In most cases, it is not legal to take a client on the road if vision does not meet state minimum If below state standard, refer to eye doctor May have to wait for cataract surgery prior to BTW
Evaluating Contrast Sensitivity
Optec 5000 – contrast slidesDay and night testingCan also test glare
Contrast Sensitivity Chart
Contrast Sensitivity-Optec Contrast Sensitivity Charts
Pelli Robson Chart
Hamilton-Veale Chart

10
Evaluating Pursuits
Equipment – colored target, eye patchProcedure:
Patch one eyeTest without glassesHave client hold head still and follow target as
you move it. Hold target 16” from patient and move in the
form of “H”, “X” and “O”
Evaluating Pursuits
Look for: choppy movement, inability to move the eye through entire range of motion, nystagmus (slow beating motion), excessive head movement
Refer to eye doctor if deficits are significant Nystagmus – often in extreme side gaze; can be in
primary gazeWill blur image on that side Can appear like double vision Client will have to be taught to turn head to that side
rather than relying only on saccades
Evaluating Saccades
Equipment: two different colored targets; eye patch
Procedure:Patch one eyeTest without glassesHave patient hold head still and look back and
forth between the targets on your commandHold targets 16” from patient, 12” apartTest in upward, horizontal and downward gaze
Evaluating Saccades
Look for: choppy movement, overshooting, undershooting, nystagmus, searching for target, inability to disassociate head and eye movementsSearching for target may mean field cut or
inattention on that sideMay benefit from visual exercise programRefer to eye doctor with overshooting,
undershooting, significant deficit, searching for target on return (suspect neglect)
Evaluating Visual Fields
Optec has visual field test Will only test horizontal field
Will not test superior or inferior field cutsIf you suspect a field cut, don’t rely only on Optec
Easy for client to cheat!They will move eyes to search for targets
Clients don’t always understand directionsMix up right, left and both
Evaluating Visual Fields
Double simultaneous stimuli Will detect field cuts in planes other
than horizontalObvious when cheating!Use with known or suspected field cutUse with clients who have difficulty
with Optec

11
Evaluating Visual Fields
Optec procedure:Test without glasses (ear piece often obscures
target)Instruct client to look straight ahead
Emphasize that targets will not be in the picture, but will be well to the side
Randomly choose targets right, left or both Check each target several times
Look for targets missed repeatedly, targets seen when singular but missed when double (suspect inattention/neglect), delay in responding
Evaluating Visual Fields
Double simultaneous stimuli procedure:Patch one eye, sit opposite client and instruct
them to look at your nose at all timesStart with arms in horizontal plane and
determine end ranges of fieldsInstruct client to identify right left or both
fingers moving Start with single stimulus then move to
simultaneous stimulus Repeat procedure for vertical and diagonal
planesRepeat binocular (inattention more obvious)
Evaluating Visual Fields
Norms: 60-65 degrees upward
70-75 degrees downward
60 degrees nasally
90-100 degrees temporally
Clinical Correlations1.Macula
2.Optic Nerve
3.Optic Chiasm
4.Optic Tract
5. Lateral Geniculate
6.Optic Radiation
7. Visual Association
8. Primary Visual Area
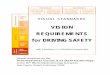
Visual Field Loss
Homonymous field loss – both eyesHemianopsia – half of field; severe loss
Many states will not allow driving with HHQuadranopsia – one quarter of field
Temporal lobe – usually upper fieldParietal love – usually lower fieldEasier to compensate for upper field loss
Location of infarct will dictate field loss Infarcts further back will cause greater loss and be more
permanent More likely to be in one eye if further forward
Visual Field Loss
• Right Homonomous Hemianopsia

12
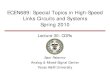
Visual Field Loss
• Binasal Hemianopsia
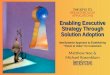
Visual Field Loss
• Bitemporal Hemianopsia
Visual Field Loss
• Quadrantopsia
Visual Field Inattention/Neglect
Can be with field loss or withoutThree types (may have one or all)
Personal space – dressing, shaving, washing facePeripersonal space – arm’s reach, desk activities
Will show up with cancellation tests, field testing, clock drawing, Rey Osterreith figure copy
Extrapersonal space – beyond arm’s reachDifficult to test in officeMore dangerous for drivingMay veer to one side when walking; miss doorway to
office,
Evaluating Inattention/Neglect
Look for patterns: Poor saccade to one side (searching on return) Difficulty with field testing (maybe just unpredictable)Odd clock drawing Leaving out details on one side of Rey Osterreith copy Taking longer to find targets on one side of Trails A or B Ignoring small peripheral shapes on Visual Form
Discrimination Test
Evaluating Inattention/Neglect
Clock drawing Ask client to draw a clock with all the numbers on it, and
the time reading “10 minutes past 11” Look for:
spacing – even, or more on one side? (inattention)
Hand placement (abstract skills)
Rey Osterreith copy Have client copy the picture Look for missing details on one side

13
Clock Drawing Test Rey Osterreith Figure Copy
Rey Osterrieth Errors Evaluating Convergence
ProcedureClient wears reading glasses if applicableHold a pencil 16” in front of client’s noseSlowly move pencil toward client’s noseClient tells you when pencil doublesOR – note when one eye stops coming in toward
the noseNormal is 2”-4” from nose
Evaluating Alignment
Optec – simple, quick Use slide with musical notes and arrow Ask client if they see both notes and an arrow
pointing down from the top of the slide Have them identify to which number note the
arrow is pointing Normal range – between 4 and 12
Evaluating Alignment
Corneal Reflex ProcedureHold pen light 16” from bridge of noseClient looks at lightObserve reflection in both pupilsLook for symmetry of reflection
Medial reflection indicates exophoria
Lateral reflection indicates esophoria
**Do not perform if seizure precautions!**

14
Evaluating Alignment
Maddox Rod Procedure Test each eye separatelyHold rod so lines on rod are oriented horizontallyStand 10 feet from clientHold penlight behind card and direct light through
the hole in the center Client indicates which number the vertical line
passes through. This represents horizontal alignment
Repeat with lines on rod oriented vertically for vertical alignment
**Inability to see line may be a suppression**
Evaluating Visual Scanning
Paper & Pencil Scan sheets C & E Cancellation Sheet Trails A Mesclun Scans Star Cancellations Disadvantage: small space – mostly focal vision
Evaluating Visual Scanning
Dynavision or Wayne Sacadic Fixator Advantage: bigger space; uses periphery Disadvantage: cost, size If your clinic has one, great test to add
Norms Grossly looking for one target per second (60
targets/minute)
Dynavision
What do I do if I find a vision deficit??
Neuro-optometrists
Specialize in functional visionEvaluate more than acuity and eye healthUse interventions such as prism lensesRefer clients for therapy (or treat in their
offices)
Find one and get to know them!Source of referrals as well as help for
your clients

15
Neuro-optometrists
NORANeuro-optometric Rehab Assoc.https://nora.cc
Search feature to find a provider
Courses in evaluation and treating vision dysfunction
Neuro-optometrists
Put off Behind the Wheel evaluation if deficits are significant and have not been addressed Both neurological and congenital diagnoses
may make it to you before a good functional evaluation
If training in the car and noticing poor tracking, trouble with curves/turns, take a step back and send for vision therapy
Vision Therapy
OT clinic with a vision rehab programNeurological Outpatient Rehab siteOften covered by insurance
Neuro-optometrist with in-office programOften out of pocket expense
Vision Exercise Program
Deficits in Pursuits/Saccades Thumb Rotations - pursuitsHart Charts - saccadesEyecanlearn.com
Tracking – Pursuits/SaccadesProgram for kids, but good for adults also
Brock String – eye pointing, accomodation
Vision Deficits Common in Older Drivers
Skills that Decline as we AgeAcuityContrast sensitivitySpatial skillsPeripheral fieldsAwareness – particularly of the periphery,
and of multiple targetsVisual processing speed Anticipatory decision makingVisual/Physical reaction – “reflexes”

16
Vision Deficits
Visual Acuity Static – ability to focus on a target
State standards differ
Road signs designed for 20/40
NJ does not retest after initial licensing (!)
Dynamic – distinguishing details of objects in motion
Useful field of viewVisual area over which information can be
extracted at a brief glance without eye or head movements.
Correlated to crash risk in older drivers UFOV decreases with age
decreases in visual processing speedreduced attentional resources less ability to ignore distracting information.
40% of 90 year olds have a UFOV of less than 20 degrees (tunnel vision)
Visual Diseases/Disorders
Macular DegenerationLoss of central vision; periphery intactVery dangerous for driving as it worsens
ScotomaLoss of a spot of vision (macular degeneration, optic
neuritis, surgery, etc.)Can sometimes learn to move head and adjust spot
to a place it does not interfereGlaucoma
Increased fluid pressure-damages optic nerveLoss of peripheral visionPoor night vision
Visual Diseases/Disorders (cont.)
CataractsClouding of the lens--loss of acuity/hazy visionPoor night vision
Diabetic RetinopathyLeakage and other damage to blood vessels of
the retinaRetinal scars; blind spots from laser treatments
Visual Diseases/Disorders (cont.)
Low Vision Significantly decreased acuity
Bioptic Lenses—some states allow Require significant training
Outside the car
Inside the car
Macular Degeneration

17
Scotoma 20/200 Acuity
Glaucoma
Vision Deficits Common after Stroke/TBI
Ocular-motor deficits
Pursuits, saccadesCranial nerve damage
III drooping eyelid; may impair peripheral vision Eye postures down and out
IV – Difficulty with downgaze Head tilt to opposite side
VI eye won’t move out (“cross eye”) **big effect on driving
Decreased ability to scan for hazardsNystagmus—abnormal oscillations of eye(s)
Cranial Nerve III Damage

18
Cranial Nerve VI Damage Poor Alignment
Strabismus (tropia) – unable to voluntarily align eyes to look at an object; constant “Cross Eyed” – one eye deviates medially “Wall Eyed” – one eye deviates laterally Corrected surgically
Phoria – misalignment that fluctuates; more apparent with fatigue May be alternating – either eye different times
Alignment Deficits
SuppressionBrain ignores image from one eyeCommon when there is double visionLoss of depth perception
New? Or longstanding?
Fusion deficitsNot using both eyes together as a team
Loss of depth perceptionNew? Or longstanding?
Visual Field Loss
Homonymous field loss – both eyesHemianopsia – half of field; severe loss
Many states will not allow driving with HHQuadranopsia – one quarter of field
Temporal lobe – usually upper fieldParietal love – usually lower fieldEasier to compensate for upper field loss
Location of infarct will dictate field loss Infarcts further back will cause greater loss and be more
permanent More likely to be in one eye if further forward
Visual Field Loss
• Right Homonomous Hemianopsia

19
Visual Field Loss
• Binasal Hemianopsia
Visual Field Loss
• Bitemporal Hemianopsia
Visual Field Loss
• Quadrantopsia
Vision Deficits (cont.) Peripheral Deficits
Visual Field Cuts One eye only – easier to compensateHomonymous – most states won’t allow driving (NJ & NY
do, PA does not)Normal binocular field=180 deg. side to side
Effect of vehicle speed on Visual Field200 deg field at 20 mph=104 degrees200 deg field at 40 mph=70 degreesNormal VF at 60 mph=40 degreesField deficit will worsen as speed increases
Peripheral vision is not clear—alerts to motion
Visual Attention Deficits
Inattention/Neglect (neurological dx) Field is either normal or decreased
Unfit for driving if extrapersonal—needs to resolve first
Unable to compensate
Decreased divided attention Field can be either normal or decreased
Work in clinic first
Common in neurological dx, but also prevalent in the well elderly
Impaired Visual Processing
Combines visual and cognitive systemsSlow Processing common in:
Neurological dx – CVA, PD, MS, TBIGeneral aging population
Compounded by: Low illuminationStressIllnessFatigueSensory overload

20
Spatial Skills Deficits
Figure Ground Differentiating foreground from background
Form Constancy Attending to subtle variations in form
Perceiving the whole object when you only see a piece of it
Position in Space Up/down, front/behind, left/right
Spatial Skills Deficits (cont.)
Topographical Disorientation Relationships of places to one another
Finding your way in space
Spatial Relations Position of objects in relation to each other
Interpreting speeds of movement
Spatial Skills Deficits (cont.)
Implications for DrivingTime and space management (stopping too late
or too soon at intersections)Parking difficulties (esp. backing)Not seeing signs, confusing arrowsInterpretation of the unexpected
(construction, car breakdowns)Maneuvering difficulties—position on roadGetting lost in familiar surroundingsLane selection
Vision Deficits Common with Congenital Diagnoses
Vision Deficits
Congenital Diagnoses that often present with vision deficitsCerebral PalsySpina BifidaLearning DisabilitiesADHD/Asperger’sRetinitis PigmentosaAlbinism
Cerebral Palsy
Common DeficitsStrabismus or Phoria Poor Binocular visionAbsent depth perceptionPoor visual/spatial skillsSlow scanningDifficulty multi-tasking
Often have difficulty with lane position, turns and curves
Often see detail at expense of big picture

21
Spina Bifida
Common deficitsWeak eye muscles – strabismusPoor scanning skills
ADHD/Asperger’s
Common deficitsDifficulty with visual multi-taskingDifficulty disassociating head & eye movementsInefficient visual scanning – or looking for the
wrong things Often see detail at expense of big picture
Watch Rey Osterreith drawing
Retinitis Pigmentosa
Common deficitsUnable to see the color redVery poor contrast sensitivity (see brake lights
better in the dark)Low vision – often referred with bioptic lensesDecreased peripheral visionPoor night vision
Ocular Albinism
Common deficitsReduced pigment in eye – crucial for visionLow visionPoor depth perceptionNystagmusStrabismusPhotophobiaAbnormalities in optic nerve – affects
connection to the brain
Driving with Low Vision
Bioptic Lenses
For drivers whose acuity cannot be corrected to the state minimumCarrier lens plus telescopic lensDriver uses carrier lens 95% of timeUses telescopic lens to read signsLegal in 37 states, including NY, NJ, PA
Requires significant training OUTSIDE the car prior to any driving
Requires a driving specialist with special training

22
Driving with Vision Deficits
Driving with Homonymous Hemianopia (HH)
Homonymous hemianopias (HH) Approx. 40% of post-chiasmal lesions
22 states and many countries do not allow driving (2009) Disqualified by arc of vision requirement
Some allow after special evaluation
Monocular Sector Prisms Can increase arc of vision enough to qualify
No research yet to determine if they increase safety (Elgin) Recommend training prior to evaluation on-road
Driving with HH
HH ResearchNo study has looked at actual crash rates Prognosis may be better with macular sparing Lower accuracy in seeing pedestrians in simulator and
traffic/pedestrians in on-road study (Bowers I)Widely differing abilities to compensate (miss rates
from 0-100% ) Greater incidence of positioning errors (over lane line
Bowers II) Age is the best predictor of blind-side miss rates
Driving with HH
HH research (cont.) Most detection errors occurred at intersections (Bowers pilot)
Scan magnitude was not large enough (especially to right side Bowers IV)
No peripheral vision cue how far to scan
Missing pedestrians, etc. on sidewalk
Judgment on fitness to drive cannot be based solely on visual field size (Gera)
Longer time not driving adversely affects outcome (Gera)
Better prognosis with good contrast sensitivity and faster processing speed (Elgin) Research shows that many people with HH are driving AMA
Evaluation – Field Cuts
Tips for Evaluators Know the law in your state for peripheral fields
Clients with significant field loss may be able to drive safely
Question client about navigation in crowded places – malls, supermarkets, etc. Do they run into things?
Send to an OT vision specialist to learn scanning strategies and improve speed and accuracy outside the car first less expensive (often covered by insurance)
safer

23
Evaluation – Field Cuts
Tips for Evaluators Look closely at the following maneuvers during BTW:
lane position – middle line, shoulder line, lane choice
intersection hazard detection – are they scanning far enough to see the sidewalk on both sides?
steering stability – do they hold a straight line?
One drive is not enough to make decision Routes should include a variety of traffic scenarios
Choose routes that challenge client from the blind side
Choose areas with pedestrians
Insist on 8-10 drives with different traffic and times of day
Familiar roads will be safer – but there can be changes, detours, surprises
Training Techniques-Field Cuts
Teach compensation techniques Look as far down the road as possible Turn head when approaching targets identified
Children playing, cars at intersections, people getting into cars in driveways, bicycles, pedestrians
Keep eyes moving constantly Turn head and be especially vigilant at
intersectionsBe sure to scan far enough – all the way to sidewalk
to look for pedestrians
Training Techniques-Field Cuts
Teach compensation techniquesUse mirrors more frequently
Scan for aggressive drivers coming from behind, tailgaters, traffic in lane on vision loss side
Vigilently check the side mirror on side of lossBeware of parking lots!!
Uncontrolled air space – look for backup lights, pedestrians, doors opening, cars cutting across spaces, cars at ends of rows
Training Techniques-Field Cuts
Teach compensation techniquesChoose lane wisely
Driving in lane corresponding with field cut will eliminate cars cutting you off from that lane
Staying in the right lane will avoid difficulty of lane change to the left and vise versa – but eventually left lane drivers may have to lane change right to exit
Plan lane changes far in advance – don’t try to cut over at the last second
Training Techniques-Field Cuts
Teach compensation techniquesWith right side loss, beware of parking
lot entrances/exits, driveways, kids playing in yards
With left side loss, be wary of car in left lane directly next to you
Training Techniques-Field Cuts
Suggest technology If client can purchase a new vehicle, suggest the
following options: Blindspot detection Lane position detection Back-up camera – looking over shoulder will be harder
with field cut Intelligent cruise control
Address position of side mirrors to reduce blindspot
Suggest spot mirrors on both sides Suggest panel rearview mirror

24
Training Techniques-Turns/curves/lane position
Teach client to look ahead, as far around the curve/turn as possibleLook for yellow line aheadTry to keep same distance from yellow line
Use landmarksThere is almost always a manhole where you
need to start a left turn
Use a magnet on the hood of the car to line up with the yellow line
Training Techniques-Field Cuts
Teach compensation techniquesWith right side loss, beware of parking
lot entrances/exits, driveways, kids playing in yards
With left side loss, be wary of car in left lane directly next to you
Training Techniques-New Drivers
Teach hierarchy of scanningMost important to least important (ie:
brake lights ahead vs. car in its lane approaching from ahead
Teach first as passenger – parent/you.Identify one thing, then two, etc.
Commentary driving
Training Techniques-New Drivers
Teach eyes up and outLook far down the roadUse saccadic eye movements
constantlyEmphasize hazardsBicycles, motorcycles, pedestrians,
runners, car approaching over center line
Techniques-Driving at Night
More difficult with: glaucoma, cataracts, photosensivity, poor contrast sensitivity
TechniquesDon’t look at headlights – look to
side of roadDrive new routes first in daylightUse yellow lenses to cut glare
Techniques-Driving in Bad Weather
More difficult with: glaucoma, cataracts, poor contrast sensitivity
TechniquesKeep windshield cleanWindshield wipers fully functioningSlow speedLeave greater following distance

25
Techniques-Lane Position Difficulty
Teach client to use center (yellow line) as guideRight side of road expands and
contractsUse a magnet to line up with center
lineMay need vision therapyVisual midline off
Techniques-Vision/Vestibular Dysfunction
Common after ConcussionDizziness with head turnsUncomfortable with motion in the
peripheryMay feel movement that is not
thereDifficulty judging spaceConvergence and Accomodation
deficits
Techniques-Vision/Vestibular Dysfunction
StrategiesMove eyes first, then head to scanMove more slowlyExpanded rearview mirrors, spot
mirrorsVision therapy
Very effective for convergenceSlower roads, familiar routes at first
Vision Resources
NORA – www.nora.ccNeuro-optometric Rehab
Association – locate a neuro-optometrist
Bernell – www.bernell.comSource for vision testing and
training products
Questions References
Alberti CF, Peli E, Bowers AR. Driving with hemianopia: II. Detection of stationary and approaching pedestrians in a simulator. Invest Ophthalmol Vis Sci. 2013;55:369-374
Bowers AR, Ananyev E, Mandel AJ, Goldstein RB, Peli E. Driving with hemianopia: IV. Head Scanning and Detection at Intersections in a simulator. Invest Ophthalmol Vis Sci. 2014;55:1540-1548
Bowers AR, Mandel AJ, Goldstein RB, Peli E. Driving with hemianopia: III. Detection performance in a simulator. Invest Ophthalmol Vis Sci. 2009;50:5137-5147
Bowers AR, Mandel AJ, Goldstein RB, Peli E. Driving with hemianopia: I. Detection performance in a simulator. Invest Ophthalmol Vis Sci. 2009;50:5137-5147
Bowers AR, Tant M, Peli E. A pilot evaluation of on-road detection performance by drivers with hemianopia using oblique peripheral prisms. Stroke Res Treat. 2012; 2012:176806
de Haan GA, Melis-Dankers BJM, Brouwer WH, Bredwoud RA, Tucha O, Heutink, J. Car driving performance in hemianopia: in On-Road Driving Study. Assoc. for Research in Vision and Ophth. 2014:14-14042

26
References
Dickerson, AE. Screening and Assessment Tools for Determining Fitness to Drive: A Review of the Literature for the Pathways Project. Occupational Therapy in Healthcare. 2014; 28(2):82-121
Dickerson, AD, Bedard, M. Decision Tool for Clients with Medical Issues: A Framework for Identifying Driving Risk and Potential to Return to Driving. Occupational Therapy in Healthcare. 2014; 28(2):194-202
Elgin J, McGwin G, Wood J, Vaphiades MS, Braswell R, DeCarlo D, Kline L, Owsley C. Evaluation of on-road driving in people with hemianopia and quadrantanopia. Amer Journ of OT 2010; 64:268-278
Fisk GD, Owsley C, Mennemeier M. Vision, attention and self-reported driving behaviors in community-dwelling stroke survivors. Arch Phys Med Rehabil. 2002; 83(4):469-477
Fist GD, Owsley C, Pulley LV. Driving after stroke: driving exposure, advice and evaluations. Arch Phys Med Rehabil. 1997;78(12):1338-1345
Glass TA, de Leon CM, Marottoli RA, Berkman LF. Population based study of social and productive activities as predictors of survival among elderly Americans. BMJ 1999;319:478-83
References Glass TA, de Leon CM, Marottoli RA, Berkman LF. Population based study of
social and productive activities as predictors of survival among elderly Americans. BMJ 1999;319:478-83
Korner-Bitensky NA, Mazer BL, Sofer S, Gelina I, Meyer MB, Morrison C, et al. Visual testing for readiness to drive after stroke: A multicenter study. Amer Jour of Physical Med & Rehab 2000;79:254-259
Legh-Smith J, Wade DR, Hewer RL. Driving after a stroke. J R Soc Med 1986; 79:200-3
Liddle J, McKenna K. Older drivers and driving cessation. Br J Occup Ther 2003; 66:125-32
Lundquist A, Gerdle B, Ronnberg J. Neuropsychological aspects of driving after a stroke – the simulator and on the road. Applied Cog Psych, 2000;14, 135-150
Marrottoli RA, de Leon CF, Glass TA, Williams CS, Cooney LM, Berkman LF. Consequences of driving cessation: decreased out-of-home activity levels. J Gerontol B Psychol Sci Soc Sci 2000; 55:S334-40
Mazer Bl, Korner-Bitensky NA, & Sofer S. Predicting ability to drive after stroke. Archives of Phys. Med and Rehab. 1998;79:743-750
References
Michon, J.A. Explanatory pitfalls and rule-based driver models. Accident Analysis and Prevention 21. 1989, 341-353.
Michon, JA. A critical view of driver behavior models: What do we know, what should we do? L Evans & RC Schwing (Eds.) Human behavior and traffic safety, (pp. 485-520). New York: Plenum Press
Moss AM, Harrison AR, Lee MS. Patients with homonymous hemianopia become visually qualified to drive using novel monocular sector prisms. J Neuro-Ophthalmol 2014; 34:53-56 Owsley C, Ball K, McGwin G, et al. Visual processing impairment and risk of motor vehicle crash among older adults. JAMA 1998;279:1083-8
Pierce S, Blackburn, C. Building Blocks for Developing a Driving Program. 1999; p. 50
Schanke AK, Sundet K. Comprehensive driving assessment: Neuropsychological testing and on-road evaluation of brain injured patients. Scandinavian Jour of Psych. 2000;41:113-121
Soderstrom, Staffan T, Petterson, Richard P., Leppert, Jerzy. Prediction of driving ability after stroke and the effect of behind-the-wheel training. Scandinavian Journal of Psychology, 2006;47:419-429
References
Szlyk JP, Brigell M, Seiple W. Effects of age and hemianopic visual field loss on driving. Optom Vis Sci. 1993;70:1031-1037
Tamietto, Marco, Torrini, Gaia, Mauro, Adenzato, Pietrapiana, Paolo, Rago, Roberto, Perino, Claudio. To Drive or not to drive (after TBI)? A review of the literature and its implications for rehabilitation and future research. NeuroRehabilitation 21 (2006) 81-92
Traffic Safety References Traffic Safety Facts 2002: Older Population. US Department of
Transportation, National Highway Traffic Safety Administration. Available at: http://www-fars.nhtsa.dot.gov/pubs/7.pdf. Accessed January 17, 2003.
10 Leading Causes of Injury Deaths, United States, 1999, All Races, Both Sexes. Office of Statistics and Programming, National Center for Injury Prevention and Control, Center for Disease Control. Data source: National Center for Health Statistics Vital Statistics System.
Eberhard J. Safe mobility for senior citizens. International Association for Traffic and Safety Services Research. 1996;20(1):29-37.
Li G, Braver ER, Chen LH. Fragility versus excessive crash involvement as determinants of high death rates per vehicle-mile of travel among older drivers. Accident Analysis and Prevention. 2003;35(2): 227-235.
Preusser DF, Williams AF, Ferguson SA, Ullmer RG, Weinstein HB. Fatal crash risk for older drivers at intersections. Accident Analysis and Prevention. 1998;30(2):151-159.
Traffic Safety References (cont.)
Traffic Safety Facts 2000: A Compilation of Motor Vehicle Crash Data from the Fatality Analysis Reporting System and the General Estimates System. Washington, DC: US Department of Transportation, National Highway Traffic Safety Administration; 2001.
Calculated from reference 7.
Eberhard J. Older Drivers Up Close: They Aren’t Dangerous. Insurance Institute for Highway Safety Status Report (Special Issue: Older Drivers). 2001;36(8):1-2.
Eberhard J. Safe mobility for senior citizens. International Association for Traffic and Safety Services Research.1996;20(1):29-37.