Embed Size (px)
Citation preview

Vision through cataractsR. Hess and G. Woo*
Contrast thresholds for a range of different spatial frequencies were compared with "acuity"tests for 10 subjects with uniocular senile cataract. The results indicate that the magnitude andextent of the intra -^resolution limit abnormality vary dramatically in cataract subjects and that,for some subjects, vision is abnormal for objects of all sizes. This finding indicates that thepresent acuity evaluation of vision with cataracts is inadequate because, in some cases, itgrossly overestimates the nature of the visual world of the cataract patient.
Key words: contrast sensitivity, spatial frequency, senile cataract, visual acuity,optical filtering, intraocular scattering
I n the clinical environment visual functionhas been traditionally assessed by estimatingthe smallest-sized, high-contrast object cap-able of being resolved. This procedure mea-sures only the limit of vision, and one has tomake an assumption about the relationshipbetween relative visibility and object sizewithin the resolution limit. Such an assump-tion is valid, for example, when the visualabnormality is due to or can be equated withdioptric defocus because, in this case, the ex-tent and magnitude of the intra-resolutionlimit abnormality are intuitively appreciatedand can be quantitatively predicted.
Recently it has been suggested1 that theintra-resolution limit abnormality resultingfrom conditions in which substantial intraocu-lar scattering occurs cannot be modeled bydioptric defocus loss because, in the formercase, vision for large objects (e.g., low-spatial-frequency gratings) is affected morethan would be predicted from the abnormal-ity measured for small objects (e.g., high-spatial-frequency gratings). Furthermore, it
From the Department of Optometry, University of Mel-bourne, Parkville, Victoria, Australia.
Submitted for publication Aug. 25, 1977.Reprint requests: R. Hess, Physiological Laboratory,
Cambridge CB2 3EG England, U.K.*On leave from the Department of Optometry, Univer-
sity of Waterloo, Waterloo, Ont., Canada.
was found that when low spatial frequenciesare disproportionately affected more thanhigh frequencies, vision is much more dra-matically restricted. This result led to thesuggestion1' 2 that visual assessment of casesin which intraocular scattering occurs shouldinvolve not only measurement of the limit ofresolution (acuity assessment) but also thequality of vision for object sizes within theresolution limit (intra-resolution limit as-sessment).
The general notion of the need for sup-plementing the present "acuity" assessmentof vision in which scattering occurs has beenrecognized by Miller et al.,3 who suggestedmeasuring glare recovery. The contrast-threshold function is an ideal candidate forevaluating relative visibility for object sizeswithin the resolution limit because it allowsmeasurement of contrast thresholds for awide range of object sizes (spatial frequen-cies) while maintaining a fixed level of lightadaptation. With the use of this test, as-sumptions are not necessary concerning thenature of the intra-resolution limit abnor-mality, since this can be directly measured. Ifthe visual loss has a purely optical basis, thenthis test measures the contrast transfercharacteristics of the eye's optics.
In the present investigation, the predictionthat cases involving substantial intraocular
428 0146-0404/78/0517-0428$00.80/0 © 1978 Assoc. for Res. in Vis. and Ophthal., Inc.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933310/ on 02/12/2018

Volume 17Number 5 Vision through cataracts 429
500
> 100
t~ 10<
L.K.
001i i i 11 mi i i i i i mi l
Z <o enu
01
Io—a—o—
\
500i i i 11 in
\\
Xl I I I I III
10
KS.
i i 11 iiin
SPATIAL FREQUENCY (c/deg)100 /T \ 001
SPATIAL FRE&UENCY (eydeg.)
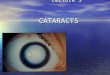
Figs. 1 and 2. Contrast sensitivity functions for two representative subjects with uniocularsenile nuclear (N) cataracts. In the lower frame, the response of the normal eye (o) is comparedto that of the fellow cataractous eye (•). In the upper frame, the ratio of these two responses (o)is plotted and compared with that expected from defocus aberration (dashed sloping line). Fig.1. Low-frequency contrast sensitivity is normal. Fig. 2. Contrast sensitivity is depressed for allfrequencies (p < 0.001).
scattering have a disproportionate low-fre-quency visibility abnormality and thereforevisual function is being grossly overestimatedby present acuity tests was evaluated.Contrast-threshold measurements for a widerange of spatial frequencies were comparedwith acuity measurements (letter and gratingacuity) for a sample of subjects with senilecataracts. In order to eliminate the consider-able intersubject variability of absolute con-trast threshold4 from the description of thevisual abnormality due to cataract, only sub-jects with uniocular cataract were selected fortesting. In this way each subject acted as hisown control, the normal eye's response rep-resenting a baseline from which the responseof the fellow cataractous eye could be accu-rately compared.
Apparatus, method, and subjects
Contrast thresholds. Vertical sinewave gratingsof variable frequency and contrast were generated
on the screen of a specially contructed 40 by 30 cmvideo monitor (P4 phosphor) by the method ofRobson.5 The screen's mean luminance was set to80 cd/m2, and contrast was modulated about thisluminance and adjusted by the subject with an80-position switched logarithmic attentuator con-nected to a digital voltmeter. The oscilloscopesurround-area was illuminated by indirect lightingto approximately that of the screen's mean lumi-nance. The video monitor's frequency responseand contrast linearity were measured with a PINphotodiode, and contrast testing was confined towithin the linear contrast region and the flatfrequency-response region of these respectivecurves. The viewing distance was varied from 57cm, for spatial frequencies up to 2 c/degree, to 456cm for higher spatial frequencies. The grating fieldsize therefore varied from 40 by 30 degrees to 5 by3.7 degrees. Subjects were carefully refracted forametropia and viewing distance, and naturalpupils were used. For the subjects tested, thepupil diameters ranged from 2 to 3.5 mm, and foreach subject pupil diameters were equal betweeneyes. The method of adjustment (staircase tech-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933310/ on 02/12/2018

430 Hess and Woo Invest. Ophthal. Visual Sci.May 1978
01 1 10SPATIAL FRE8UENCY (c/deg)
01 1 10 100SPATIAL FREQUENCY (c /deg)
Figs. 3 and 4. Contrast sensitivity functions for two representative subjects with uniocularsenile cortical (C) cataracts. In the lower frame, the response of the normal eye (o) is comparedto that of the fellow cataractous eye (•). In the upper frame, the ratio of these two responses (a)is plotted and compared with that predicted from defocus aberration (dashed sloping line). Fig.3. Low-frequency, contrast sensitivity is normal. Fig, 4. Contrast sensitivity is depressed for allspatial frequencies (p < 0.001).
nique) was used by the subject to set thresholds,each data point representing the average of threereadings. To establish valid comparisons that wereuncontaminated by time-dependent threshold var-iation, the procedure was such that each eye wasalternately compared for each spatial frequency(point-to-point comparison). An eye patch wasused to occlude the eye not being tested.
Letter acuity. Letter acuity was measured withsingle Landolt C's (approximately 100% contrast),and frequency-of-seeing data were probit-ana-lyzed6 to obtain a more accurate 50% threshold.Each letter size was presented eight times. Themean luminance and testing conditions wereidentical to those already described for the con-trast-threshold measurements.
Subjects. Subjects were selected from the filesof the departmental clinic according to very strictguidelines, so that only subjects who had a purelyoptical (cataract) basis for their visual loss (i.e.,with no neural component) were selected. Theselection guidelines were as follows: (1) uniocularcataract, (2) good observer, (3) no history of gen-
eral medical illness, (4) full normal ocular historyprior to cataract formation combined with no signof any degenerative or other neural abnormality inthe good eye after cataract formation, and (5) noother optical or oculomotor abnormality. Thecriteria for a normal eye (i.e., uniocular cataract)were as follows: no ophthahnoscopically visiblecataract formation within the pupillary region, noassociated ocular abnormality, and normal visualacuity. The cataracts were classified as cortical ornuclear depending upon the site of the majoropacity.
Results
The sinewave contrast threshold functionwhich represents the contrast necessary forthreshold detection over a 2V£ log unit rangeof spatial frequency was measured for thenormal and fellow cataractous eye of 10 sub-jects with uniocular cataract. The resultscould not be described by a single family ofvisual loss functions. Recent results concern-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933310/ on 02/12/2018

Volume 17Number 5 Vision through cataracts 431
i
0-5
0-2
z11
< 02
o
o
ct
t-in
cci—zo
1
05
0-2
1
0-5
0-2
0-1
005
L.K.L.H.
ff H
01 1 10 100SPATIAL FREQUENCY (c/deg )
M.F?
— O O Q
M.S_ _ - — _ _ _ _ .
-o—o—a
tO 1 01
FREQUENCY ( c / d e g )
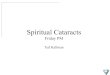
Fig. 5. Summary of the contrast attenuation results for the 10 uniocular senile cataract subjectstested. These results, which were derived from contrast sensitivity functions, have beenseparated into two groups depending upon the extent of the intra-resolution limit abnormal-ity. The low-frequency attenuation (right) is statistically significant and repeatable (p < 0.001).The senile cataracts have been divided into cortical (C) and nuclear (N).
ing optical1 and neural4 abnormalities suggestthat an obvious and most useful classificationcan be based upon the presence or absence oflow-frequency involvement. According tothis criterion the results from this limitedsample were found to fall generally into oneor other of two discrete response categories;an example of each of these is seen in Figs. 1
and 2 for nuclear cataracts and Figs. 3 and 4for cortical cataracts.
In the lower portion of each of these figuresthe normal eye's response (unfilled symbols)is compared with the response of the fellowcataractous eye (filled symbols). The ratio ofthese responses, which represents the con-trast attenuation due to the cataract, is plot-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933310/ on 02/12/2018

432 Hess and WooInvest. Ophthal. Visual Set.
May 1978
02
0-4
0-6
0-8
1
-
-
- •
i
II ii
• 0
J Ii
°>1c)
8O
i mr>
• 0
i i
o
. r1 0-8 0-6 <K 0-2
ACUITY RATIO (cataract /normal eye)
Fig. 6. The acuity ratio (cataract/normal acuity) forsingle Landolt C's (o) and gratings (•) is plottedagainst the magnitude of the low-spatial-frequency(average for 0.12 and 0.24 c/degree) abnormality(ratio of cataract/normal eye). An insignificant cor-relation exists between these two parameters forthe 10 subjects tested, and the results exhibit adichotomous behaviour (see text).
ted in the upper portion. The standard errorof the mean in these and subsequent figuresis always less than the symbol size. Fig. 1typifies a response in which there is afrequency-dependent loss of contrast withnormal low-frequency vision remaining. Thisresult, which represents the largest acuityloss for the subjects tested, can be consideredin general terms to be similar to dioptric de-focus in that there is a range of low frequen-cies (large bars) for which vision is normaland the contrast loss at high frequencies canbe approximately modeled, in this case, bythat predicted from dioptric defocus. Thedashed line in Figs. 1 to 4 denotes the pre-dicted contrast loss (approximated slope ofhigh-frequency region) from dioptric de-focus, which was computed (autocorrelationcomputations of the pupil function) for aschematic eye (2 mm pupil) exhibiting 0.16wavelengths of primary spherical aberration.Because defocus degradation can be easilysimulated, this represents a convenient ref-erence plane for appreciating the type ofhigh-frequency contrast degradation due tocataract. Fig. 2 illustrates a response in which
there is a frequency-dependent loss of con-trast for high spatial frequencies combinedwith a constant low-frequency depression.This low-frequency depression is statisticallysignificant (p < 0.1%). Figs. 3 and 4 showsimilar results for two subjects with pre-dominantly cortical opacities. For one sub-ject (Fig. 3) the intra-resolution limit ab-normality is restricted to only high spatialfrequencies, whereas for the other subject(Fig. 4) contrast detection is abnormal at allspatial frequencies. In both cases the high-frequency contrast loss is much more gradualthan would occur from defocus.
The contrast-loss functions due to cataractfor the ten subjects tested are displayed inFig. 5. These results have been separatedinto two categories depending upon whetherthe intra-resolution limit abnormality is re-stricted to high-medium frequencies or af-fects all spatial frequencies. The results showthat two distinctly different types of intra-resolution limit abnormalities occur, eitherthe visual abnormality is restricted to highfrequencies or it involves all spatial frequen-cies. Close inspection of the results showsthat these two abnormalities have no correla-tion with the question of whether the cataractis cortical or nuclear and that for a completepicture of the type of intra-resolution limitabnormality one has to know the followingvalues: the cut-off acuity, slope of the high-frequency fall-off, and the magnitude of thelow-frequency abnormality. It would seemthat all these factors can vary independently,and so more extensive results are requiredbefore their interrelationships are known.One interpretation of the present results isthat as a cataract develops, optical aberra-tions and narrow-angle scattering are themajor contributors to visual loss. When scat-tering becomes isotropic, vision for all fre-quencies will be affected equally, and so thecontrast-loss function undergoes a predomi-nantly vertical shift. A longitudinal studyusing the present technique to monitor thevisual loss during the course of cataract for-mation should be able to test this suggestion.The interrelationship of these three factorsmay vary from one cataract to another, and to
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933310/ on 02/12/2018

Volume 17Number 5 Vision through cataracts 433
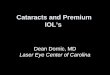
Fig. 7. Photographs of an image formed by an artificial eye (3 mm diameter pupil) for threeconditions of viewing. In-focus (A), defocus (B), and diffuse imagery (C) are compared. Thedefocus and diffusing filters had identical acuity (high-frequency) responses, and all conditionswere equated for the same total diffuse transmission. The diffuser, which affects low frequen-cies as well as high frequencies, produces a more visually debilitating result than the equiva-lent defocus (see text).
this extent each cataract will be unique andrequire individual assessment.
What is certain from the present results isthat the type and extent of the intra-resolution limit abnormality (whether all orjust a limited band of frequencies are af-fected) cannot be detected by measurementof acuity. The presence of the two responsegroups in Fig. 5 would not have been ap-preciated from conventional acuity tests. Thispoint is more clearly seen in the results ofFig. 6 in which the acuity abnormality (ratioof cataract eye's acuity to normal eye's acuity)for letters and for gratings is plotted againstthe magnitude of the low-frequency abnor-mality. The letter acuity results were ob-tained after probit analysis6 of frequency-of-seeing data for single Landolt C detection.The grating acuity results were obtained by
extrapolation to the abscissa of the individualhigh-frequency contrast-threshold results.These results were replotted on semi-logcoordinates and fitted by linear regression.7
The results show that there is no significantcorrelation (r = 0.1; p > 0.1) between themagnitude of the low-frequency abnormalityand either the letter or grating acuity abnor-mality. There is however a good correlation(r = 0.7) between acuity (grating or letter)and magnitude of the low-frequency abnor-mality within the low-frequency-abnormalitygroup, although for the sample size this cor-relation coefficient is not significant (0.1 >p > 0.05).
Discussion
The main finding of this investigation isthat visual loss for subjects with senile cata-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933310/ on 02/12/2018

434 Hess and WooInvest. Ophthal. Visual Sci.
May 1978
ract cannot be described by a single visual-loss function because, for some subjects,vision for low frequencies (large bars) is dis-proportionately depressed. It is in the findingof this significant low-spatial-frequency ab-normality that the present results differ fromthose of a previous study1 on simulatedcataract. In this respect visual loss from allcataracts cannot be thought of or assessed interms of contrast loss from dioptric defocus.Because the presence or absence of a low-frequency contrast abnormality is not corre-lated with the degree of high-frequency de-gradation (Fig. 6), present acuity tests willnot be able to detect this extra intra-resolution limit abnormality.
The fact that contrast threshold are ele-vated for low spatial frequencies has impor-tant visual significance. Because the cause ofthis threshold elevation has a purely opticalbasis, it can be predicted that contrast per-ception in the suprathreshold region will bedepressed by the same ratio. This luxury ofbeing able to go from threshold results tosuprathreshold predictions may not be validif the visual loss has a neural basis. In the caseof neural loss, threshold may be affectedwithout any significant suprathreshold con-sequence if the abnormality occurs after thecontrast gain-setting mechanism. It is onlywhen the abnormality has a purely opticalbasis that suprathreshold prediction musthold, since the abnormality must occur be-fore the neural contrast gain-setting mecha-nism. It is for this reason that the results inFig. 5 have been expressed as a contrastratio. These results therefore represent thesuprathreshold contrast matching functionsfor cataracts and allow estimation of the per-ceptual world of the cataract subject at anycontrast level.
The previous finding1 that optical depres-sion of contrast perception at low spatial fre-quencies has a very debilitating visual effectis further supported by the results of opticalfiltering (Fig. 7). In this figure a complex vi-sual scene has been optically filtered by adiffuser (consisting of 5 /x diameter sphericalparticles in liquid media) in Fig. 7, C, and adefocus lens in Fig. 7, B, giving identical
high-frequency degradation (equal acuity for3 bar military test target). The optical set-upfor this filtering consisted in photographingthe image formed by an artificial eye (3 mmdiameter pupil). Each optical filter wasplaced as close as possible to the anterior lenssurface of the artificial eye, and each filterwas luminance-matched for total forward dif-fuse transmittance. The diffuser, unlike thedefocus lens, affects low spatial frequencies1
and can be seen to produce more severe vi-sual degradation than the "equivalent de-focus." Similarly, cataract subjects whoexhibit low-frequency visual abnormalitiesmay have much greater visual loss undereveryday conditions than would be indicatedby our acuity assessment.
These results add to our present apprecia-tion of the type of vision that a cataract pa-tient experiences and may have an importantbearing upon the question of when to referthe patient for removal of the cataract. It issuggested that the assessment of the visibilityof large objects (e.g., low-spatial-frequencygratings) be used in the clinical environmentto supplement the present acuity evaluationof vision for cataract subjects. These cataractfindings raise the more general question as tohow any residual visual function should beassessed for occupational or legal needs. Isthe present acuity evaluation and visual fieldrequirement adequate to define "blindness"or partial sightedness? Assessment andspecification of the intra-resolution abnor-mality, combined* with an understanding ofits suprathreshold consequences, shouldallow a much more adequate definition oflegal blindness. When the visual loss has apurely optical basis as, for example, incataract, visual assessment should involvemeasurement of the visibility of large objectsas well as the limit of resolution. When this isdone, the suprathreshold contrast-matchingfunction is automatically known, and contrastperception at any suprathreshold level can becalculated.
We gratefully acknowledge the assistance of LeoCarney, George Smith, Ed Howell, and Stephen Jen-kins.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933310/ on 02/12/2018

Volume 17Number 5 Vision through cataracts 435
REFERENCES1. Hess, R., and Garner, L.: The effect of comeal edema
on visual function, INVEST. OPHTHALMOL. VISUAL SCI.
16:5, 1977.2. Zuckerman, J. E., Miller, D., Dyes, W., and Keller,
M.: Degradation of vision through a simulatedcataract, INVEST. OPHTHALMOL. 12:213, 1973.
3. Miller, D., Jernigan, M. E., Molnar, S., Wolf, E.,and Newman, J.: Laboratory evaluation of a clinicalglare tester, Arch. Ophthalmol. 87:324, 1972.
4. Hess, R., and Howell, E.: The threshold contrast
sensitivity function in strabismic amblyopia; evidencefor a two type classification, Vision Res. 17:1049,1977.
5. Campbell, F. W., and Green, D. G.: Optical andretinal factors affecting visual resolution, J. Physiol.181:576, 1965.
6. Finney, D. J.: Probit Analysis, Cambridge, England,1947, Cambridge University Press.
7. Campbell, F. W., Kulikowski, J. J., andLevinson, J.:The effect of orientation on the visual resolution ofgratings, J. Physiol. 187:427, 1966.
Information for authorsMost of the provisions of the Copyright Act of 1976 became eflPective on January 1, 1978.
Therefore all manuscripts must be accompanied by the following statement, signed by eachauthor: "The undersigned author(s) transfers all copyright ownership of the manuscriptentitled (title of article) to The Association for Research in Vision and Ophthalmology, Inc.,in the event the work is published. The author(s) warrant that the article is original, is notunder consideration by another journal, and has not been previously published." Authorswill be consulted, when possible, regarding republication of their material.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933310/ on 02/12/2018