-
7/27/2019 vit d jpen 2012
1/9
http://pen.sagepub.com/Nutrition
Journal of Parenteral and Enteral
http://pen.sagepub.com/content/36/6/713The online version of
this article can be found at:
DOI: 10.1177/0148607112444449
2012 36: 713 originally published online 20 April 2012JPEN J
Parenter Enteral Nutravid M. Higgins, Paul E. Wischmeyer, Kelly M.
Queensland, Stefan H. Sillau, Alexandra J. Sufit and Daren K.
Hey
Relationship of Vitamin D Deficiency to Clinical Outcomes in
Critically Ill Patients
Published by:
http://www.sagepublications.com
On behalf of:
The American Society for Parenteral & Enteral Nutrition
can be found at:Journal of Parenteral and Enteral
NutritionAdditional services and information for
http://pen.sagepub.com/cgi/alertsEmail Alerts:
http://pen.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Apr 20, 2012OnlineFirst Version of Record
- Oct 17, 2012Version of Record>>
at A.S.P.E.N on August 28, 2013pen.sagepub.comDownloaded
from
http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/content/36/6/713http://pen.sagepub.com/content/36/6/713http://www.sagepublications.com/http://www.sagepublications.com/http://www.nutritioncare.org/http://www.nutritioncare.org/http://pen.sagepub.com/cgi/alertshttp://pen.sagepub.com/cgi/alertshttp://pen.sagepub.com/subscriptionshttp://pen.sagepub.com/subscriptionshttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsPermissions.navhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://pen.sagepub.com/content/early/2012/04/19/0148607112444449.full.pdfhttp://pen.sagepub.com/content/early/2012/04/19/0148607112444449.full.pdfhttp://pen.sagepub.com/content/36/6/713.full.pdfhttp://pen.sagepub.com/content/36/6/713.full.pdfhttp://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/http://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://pen.sagepub.com/content/early/2012/04/19/0148607112444449.full.pdfhttp://pen.sagepub.com/content/36/6/713.full.pdfhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsReprints.navhttp://pen.sagepub.com/subscriptionshttp://pen.sagepub.com/cgi/alertshttp://www.nutritioncare.org/http://www.sagepublications.com/http://pen.sagepub.com/content/36/6/713http://pen.sagepub.com/
-
7/27/2019 vit d jpen 2012
2/9
Journal of Parenteral and Enteral
Nutrition
Volume 36 Number 6
November 2012 713-720
2012 American Society
for Parenteral and Enteral Nutrition
DOI: 10.1177/0148607112444449
http://jpen.sagepub.com
hosted at
http://online.sagepub.com
Original Communication
Clinical Relevancy Statement
Vitamin D deficiency has been associated with a myriad of
disease conditions in the general population. However, the
impact of vitamin D deficiency on outcome in critically ill
patients remains unclear. Although studies have described a
high burden of vitamin D deficiency in this population and
suggested a correlation with adverse outcomes, few studies
have addressed specific outcomes. Furthermore, the useful-
ness of obtaining vitamin D levels in critically ill patients
is
not clear because most studies have evaluated preintensive
care unit (ICU) vitamin D levels, and no large studies to
date
have trended vitamin D levels during the ICU stay. We con-
firm in this study that vitamin D deficiency is common in
this
population and is associated with a longer ICU length of
stay,
may increase the risk of ICU-acquired infections and pneumo-nia,
and may be associated with elevated organ failure scores.
In addition, we describe the trend of vitamin D status
during
the stay of patients in the ICU and demonstrate that there is
a
statistically significant decrease in the levels of vitamin
D.
These results add to the growing fund of knowledge concern-
ing the association of vitamin D deficiency with adverse
out-
comes in the critical care population and indicate that
further
research is warranted in defining whether vitamin D supple-
mentation is beneficial and what is the optimal dose and
tim-
ing of vitamin D in this population.
. / i i
From the 1Department of Anesthesiology, University of
Colorado
School of Medicine, Aurora, Colorado; 2Department of
Biostatistics and
Informatics, Colorado School of Public Health, University of
Colorado,
Aurora, Colorado; and3Clinical Evaluation Research Unit,
Kingston
General Hospital, Kingston, Ontario, Canada;4Department of
Medicine,
Queens University, Kingston, Ontario, Canada.
This work was presented at the following meetings: Society for
Critical
Care Medicine, San Diego, California, January 16, 2011;
American
Society for Parenteral and Enteral Nutrition, Vancouver, Canada,
January
30, 2011; and SHOCK society, Norfolk, Virginia, January 12,
2011.
Financial disclosure: This study was a secondary analysis of an
existing
database.
Received for publication December 7, 2011; accepted for
publication
January 6, 2012.
Corresponding Author: Paul Wischmeyer, MD, University of
ColoradoSchool of Medicine, Department of Anesthesiology, RC-2,
Mail Stop
8602, 12700 E 19th Ave, Aurora, CO 80045; e-mail:
Paul.Wischmeyer@
ucdenver.edu
Relationship of Vitamin D Deficiency to Clinical Outcomes in
Critically Ill Patients
David M. Higgins, MS1; Paul E. Wischmeyer, MD
1; Kelly M. Queensland, BA
1;
Stefan H. Sillau, MS2; Alexandra J. Sufit, BA1; and Daren K.
Heyland, MD3, 4
Abstract
Background: Despite the numerous disease conditions associated
with vitamin D deficiency in the general population, the
relationship
of this deficiency to outcome in critically ill patients remains
unclear. The objective of this study is to determine the burden of
vitamin
D deficiency in intensive care unit (ICU) patients and determine
if it is associated with poor patient outcomes. Methods: The
authors
conducted an analysis of samples collected from a prospective
study of 196 patients admitted to a medical/surgical ICU in a
tertiary
care hospital. They measured serum 25-hydroxyvitamin D at
admission and up to 10 days following admission and followed
patients
prospectively for 28-day outcomes.Results: Of analyzable
patients, 50 (26%) were deficient (30 nmol/L) and 109 (56%) were
insufficient
(>30 and 60 nmol/L). Baseline 25(OH)D levels decreased
significantly in all patients after 3 days in the ICU and remained
significantly
lower through 10 days (P< .001). 25(OH)D status was not
significantly associated with 28-day all-cause mortality (hazard
ratio [HR],
0.89; 95% confidence interval, [CI] 0.372.24). Higher levels of
25(OH)D were associated with a shorter time-to-alive ICU
discharge(HR, 2.11; 95% CI, 1.273.51). 25(OH)D-deficient patients
showed a nonstatistically significant trend toward a higher
infection rate
(odds ratio [OR], 3.20; 95% CI, 0.78413.07;P= .11) compared with
patients with sufficient levels of 25(OH)D. Conclusions: This
study
demonstrates significant decreases in vitamin D status over the
duration of the patients ICU stay. Low levels of vitamin D are
associated
with longer time to ICU discharge alive and a trend toward
increased risk of ICU-acquired infection. (JPEN J Parenter Enteral
Nutr.
2012;36:713-720)
Keywords
immunonutrition; research and diseases; vitamins; nutrition;
critical care; research and diseases
Download a QR code reader on your smart-
phone, scan this image, and listen to the
podcast for this article instantly. Or listen to
this and other JPEN podcasts at http://pen.
sagepub.com/site/misc/Index/Podcasts.
xhtml.
at A.S.P.E.N on August 28, 2013pen.sagepub.comDownloaded
from
http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/
-
7/27/2019 vit d jpen 2012
3/9
714 Journal of Parenteral and Enteral Nutrition36(6)
Introduction
Vitamin D deficiency is a common disorder that is associated
with excess morbidity and mortality in general population
studies.1-4 The role of vitamin D in the regulation of
calcium,
phosphorus, and skeletal growth has been extensively
described.5,6
Evidence is mounting that vitamin D deficiencyalso has an
association with the immune system, affecting
cancer, multiple sclerosis, diabetes, and autoimmune disor-
ders.7-13 The recent discovery that many cells of the immune
system express both the enzyme 25-hydroxyvitamin D-1-
hydroxylase to convert circulating 25(OH)D to hormonally
active 1,25(OH)2D and vitamin D receptors may reveal a new
and significant function of vitamin D on immune system regu-
lation.10,14 Specifically, vitamin D may play a key
physiologic
role in attenuating potentially pathogenic cell-mediated
immune responses and thus has been linked to an increased
incidence of autoimmune disorders.7-13 Vitamin D may also be
important for optimizing host defense against infection as
children with rickets are more susceptible to infection,15
and
vitamin D has been implicated in the pathogenesis of infec-
tions such as tuberculosis.16
Vitamin D deficiency in the critically ill patient was
observed more than 20 years ago, primarily in hypocalcemic
patients.17 Recent studies in normocalcemic critically ill
patients have suggested a very high burden of vitamin D
defi-
ciency in this population and suggested a previously
unrecog-
nized contribution of deficient states to
non-calcium-related
consequences.18-24 However, to our knowledge, no large stud-
ies have specifically addressed vitamin D status trends
through
the duration of stay in the intensive care unit (ICU).
Critically
ill patients are at an especially high risk for many of the
disor-ders that vitamin D deficiency may be associated with.
Yet,
evaluation of 25(OH)D status is rarely performed in the
critical
care setting.25
The hypothesis of this study is that vitamin D status in ICU
patients is significantly decreased at admission and
continues
to decrease throughout their hospital stay. Furthermore, we
hypothesize that vitamin D deficiency is associated with
poor
patient outcomes, particularly longer ICU stay and greater
risk
of infection.
Materials and Methods
The original purpose of the prospective observational study
was
to evaluate a diagnostic marker for sepsis in critical illness.
This
trial was conducted at the Kingston General Hospital, a
tertiary
care, mixed medical-surgical ICU,26 and 2 other hospitals. In
the
original study, 597 patients were enrolled at the 3 sites.
However, additional blood was collected and available for
analysis only from patients at the Kingston General Hospital
site, which included 203 total patients, and this is the
cohort
studied in this report. Here we report a secondary analysis of
the
serum samples collected in this study evaluating the
relationship
between 25(OH)D levels and clinical outcomes. The patients
were enrolled over the period of 1 year from October 2002 to
October 2003. Research ethics boards from Queens University
approved the protocol for the original study; informed
consent
was obtained from next of kin before enrollment. The
inclusion
criteria of the patients included all consecutive patients 18
years
and older who were expected to stay more than 24 hours in
the
ICU and were enrolled within the first 24 hours of ICU
admis-sion. Only patients admitted for overdoses were excluded
from
the study. The study protocol at Kingston General Hospital
included blood sample collection daily for a maximum of 10
days. Serum samples were also collected and stored at 80C
prior to analysis.
Data Collection
Demographics, past medical history, and medications were
obtained from the patients charts and included age, race,
sex,
body mass index (BMI; determined prior to ICU admission or
estimated as pre-ICU dry weight [in kg] divided by height
[in
cm] squared in the ICU on admission), season of admission
(summer admission was defined as admission between June 21
and September 22 of the year of the study), admission
category
(cardiovascular, respiratory, neurological, metabolic,
gastroin-
testinal, hematologic, sepsis, postoperative), and
comorbidities
(coronary artery disease, hypertension, chronic obstructive
pul-
monary disease, diabetes, renal disease, liver disease,
cancer).
Necessary variables were recorded to calculate Acute
Physiology
and Chronic Health Evaluation II (APACHE II)27 and
Sequential
Organ Failure Assessment (SOFA) scores28 at admission.
Clinical outcomes were assessed at 14 and 28 days. No
patients
were lost to follow up for the 14- or 28-day clinical end
points.
Outcomes recorded included mortality, time-to-alive ICU
dis-charge, and infection status. The diagnosis of ICU-acquired
infection was defined as infection present after 48 hours of
ICU
admission. Suspected infection was defined by the presence
of
a new positive culture result or initiation of new antibiotics
after
48 hours of ICU admission. The charts of all patients with
sus-
pected infections were reviewed by 2 independent blinded
physicians using standardized definitions.29 Adjudicators
then
met to determine the presence or absence of infection. In case
of
discrepancy, the physicians would meet and resolve the issue
by
reanalyzing the chart. Given the uncertainty around the
absolute
diagnosis of a new infection, we used standard definitions
of
probable and possible for each type of infection, where
probable reflected a higher degree of probability, in the
opinion
of the adjudicator, that infection was present compared with
pos-
sible infection. This adjudication technique has been
validated
and published in previous large clinical ICU trials.30,31 The
max
SOFA score was calculated as the worse score for each organ
component over the patients ICU stay. The delta SOFA score
was determined by subtracting the maximum SOFA score from
the admission total SOFA score. As vitamin D insufficiency
has
been associated with an increased susceptibility to
pulmonary
infections,32 the subgroup of patients with ICU-acquired
pneu-
monia >48 hours after admission was analyzed separately.
at A.S.P.E.N on August 28, 2013pen.sagepub.comDownloaded
from
http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/
-
7/27/2019 vit d jpen 2012
4/9
Vitamin D Deficiency in Critically Ill Patients/ Higgins et al
715
Serum was collected on the day of ICU admission (within
24 hours of ICU admittance) and daily for 10 days while in
the
ICU. All samples were stored at 80C for future analysis and
did not undergo more than 1 freeze-thaw cycle before running
assays. Serum 25(OH)D levels were assessed using a radioim-
munoassay (RIA) method (DiaSorin, Antony, France) at The
Childrens Hospital Clinical and Translational Research
CenterCore Lab in Denver, Colorado, at baseline and with
samples
from days 3, 5, 7, and 10 (when available). This laboratory
participates biannually in the Vitamin D External Quality
Assessment Scheme to ensure the analytical reliability of
the
25(OH)D assay. The coefficient of variation for the 25(OH)D
RIA assay is 0.046. Samples were run in 4 batches according
to the day after admission. The following 25(OH)D values
were used for deficient, insufficient, and sufficient
patients
according to previously reported subgroups: sufficient,
>60
nmol/L; insufficient, >30 to 60 nmol/L; and deficient, 30
nmol/L,19 which are similar to the recent Institute of
Medicine
report cutoffs.33
Statistics
For baseline SOFA scores, multiple regression was used to
calculate adjusted least squares means using PROC GLM in
SAS Version 9.2 (SAS Institute, Inc, Cary, NC) between
25(OH)D groups. In all multivariate models, we controlled
for
age, gender, BMI, and APACHE II score. Ethnicity was not
included in the analysis because 201 of the 203 patients
were
white. Except for gender, all covariates were continuous.
Logistic and proportional hazards models used Wald tests and
confidence intervals. To assess the change in 25(OH)D status
over the patients stay in the ICU, the PROC MIXED functionwas
used in SAS to run a mixed model regression. 25(OH)D
status was expressed as a categorical variable, and a multi-
variate Cox proportional hazard ratio model was used to
iden-
tify variable association with time to ICU discharge or
mortality. The PROC PHREG function in SAS was used to
calculate the hazard ratios for time-to-alive ICU discharge
and
mortality variables. Patients who died were censored because
their time to recovery was unknown. Because a 1-nmol/L
increase in 25(OH)D is not clinically relevant, we
represented
a 1-unit increase as a 30-nmol/L increase in 25(OH)D levels
for hazard ratio estimates. This unit selection scales the
hazard
ratio estimates but does not have any effect on the
statistical
significance. The P value for this analysis was determined
using a type 3 Wald test. Logistic regression was used to
model probable and possible ICU-acquired infections in the
25(OH)D groups using the PROC LOGISTIC function in SAS
Version 9.2. The Student ttest (unpooled [Satterthwaite])
was
used to compare the means of baseline 25(OH)D between
patients with and without pneumonia. The SAS Version 9.2
statistical package was used for all analyses. Means (SD)
are
reported. All tests were 2-sided, and P< .05 was
considered
significant. A statistical trend was consideredP< .20.
Results
Patients and 25(OH)D Status
In the original study, 203 patients were enrolled at
Kingston
General Hospital. However, baseline serum samples were not
available for analysis in 7 patients. Thus, a total of 196
patients
on admission day were included in this analysis. Of the
196patients analyzed, 66 (33.7%) were admitted as postoperative
patients and 130 (66.3%) were admitted for medical reasons.
The primary admission categories, including cardiovascular,
respiratory, neurological, metabolic, gastrointestinal, and
hematologic disorders, were not statistically different
between
the groups (see Table 1). Comorbid conditions existing prior
to
ICU admission, including coronary artery disease, hyperten-
sion, diabetes, renal disease, liver disease, or cancer, were
not
significantly different between the groups. In addition,
APACHE II scores, presence of sepsis on admission, and base-
line SOFA scores were similar between the 25(OH)D groups
(see Table 1). Furthermore, there were no significant
differ-
ences in mean parenteral nutrition (PN) and enteral
nutrition
(EN) over ICU length of stay between the groups.
Upon admission to the ICU, a low baseline serum 25(OH)
D (60 nmol/L) level was observed in 159 patients (82% of
total cohort), as seen in Figure 1. Of analyzable patients,
50
(26%) were deficient (30 nmol/L), 109 (56%) were insuffi-
cient (>30 and 60 nmol/L), and 37 (18%) were sufficient
(>60 nmol/L) at baseline. At baseline, the mean 25(OH)D
level
was 47.0 nmol/L. The mean dropped significantly by post
admission day 3 to 44.4 nmol/L (n = 138, P < .001) and
remained significantly decreased compared with baseline in
patients who stayed 10 days or longer (45 nmol/L at baseline
to
39 nmol/L on day 10, n = 44,P< .001). The mean 25(OH)Dfor
patients who stayed at least 10 days (n = 44) in the insuffi-
cient or sufficient groups significantly decreased compared
with the baseline on days 3, 7, and 10, as seen in Figure 2.
Of
the 23 patients who were sufficient at ICU admission and
stayed longer than 3 days (14 patients excluded), 9 of 23
suf-
ficient patients (39.1%) developed insufficiency at some
point
during their stay.
Effect of 25(OH)D Level on Mortality and
Time-to-Alive ICU Discharge
All-cause 28-day mortality in the study population was
26.2%.
The mortality rates and average time to death for 25(OH)D
sufficient, insufficient, and deficient groups were 27.0%
and
8.0 7.0 days, 27.5% and 8.8 7.2 days, and 22.0% and 9.0
8.8 days, respectively. Using a multivariate Cox
proportional
hazard ratio (HR) model, 25(OH)D category was not associ-
ated with 28-day all-cause mortality (HR, sufficient vs
defi-
cient groups: 0.89; 95% confidence interval [CI], 0.372.24),
as shown in Table 2.
The mean SD time-to-alive ICU discharge for all patients
in the study population was 7.5 8.5 days. The mean time-to-
at A.S.P.E.N on August 28, 2013pen.sagepub.comDownloaded
from
http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/
-
7/27/2019 vit d jpen 2012
5/9
716 Journal of Parenteral and Enteral Nutrition36(6)
alive ICU discharge for 25(OH)D sufficient, insufficient,
and
deficient groups was 5.9 5.4, 6.8 6.0, and 10.6 8.4,
respectively. Sufficient levels of 25(OH)D were
significantly
associated with a shorter time-to-alive ICU discharge (HR,
1.74 per 30 nmol/L; 95% CI, 1.192.53 at 14 days and HR,
3.49; 95% CI, 1.368.95 at 28 days). Using the multivariate
Cox proportional hazards model with 25(OH)D represented as
a categorical variable, we found that 25(OH)D sufficient or
insufficient patients left the ICU sooner than patients with
defi-
cient levels of 25(OH)D, as shown in Table 2.
Max SOFA scores were calculated and showed nonsignifi-
cantly higher SOFA scores in deficient patients compared
with
the other groups (deficient max SOFA 9.7 4.2, insufficient
max SOFA 8.4 4.2, and sufficient max SOFA 8.4 3.3; P=
.12). Delta SOFA scores were 1.3 1.7, 1.6 2.1, and 2.1 2.3
in sufficient, insufficient, and deficient groups,
respectively
(P= .29).
In addition, the mean duration of ventilation was deter-
mined and found to be 141.5 18.1 hours in vitamin
Ddeficient patients compared with 138 16.9 hours in insuf-
ficient and 120 20.9 hours in sufficient groups (P= .49), as
shown in Table 3.
Infection StatusPatients were followed for infection status, and
the relationship
of baseline 25(OH)D status to new infections diagnosed after
48
hours in the ICU is summarized in Table 3. 25(OH)D-deficient
and insufficient patients had a higher rate of at least 1
probable
infection compared with patients with sufficient levels of
25(OH)D, but this was not statistically significant (odds
ratio
[OR], 3.20; 95% CI, 0.78413.07,P= .11). There was no rela-
tionship between rate of culture-confirmed infections and
pos-
sible infections and 25(OH)D levels (Table 3).
Table 1. Comparison of Demographics Between 25(OH)D Groups
Sufficient
(>60 nmol/L)
Insufficient
(>30 to 60 nmol/L)
Deficient (30
nmol/L) PValue
25(OH)D status, No. (%) 37 (18.5) 109 (55.9) 50 (25.6)
Age, y, mean SD 65.0 13.3 64.3 14.4 62.9 14.1 .41
Male sex, No. (%) 17 (46) 72 (66) 32 (64) .09b
Body mass index, mean SD 26.7 5.0 30.1 6.9 29.8 8.8 .76a
Summer admission, No. (%) 7 (26) 28 (36) 18 (36) .19a
APACHE II, mean SD 20.8 8.4 19.7 7.8 20.8 7.4 .47a
Baseline SOFA, mean SD 7.1 2.9 6.8 3.6 7.6 3.7 .45a
Sepsis, No. (%)c
15 (40) 52 (48) 22 (44) .29b
Parenteral + enteral nutrition, kcal/d,
mean SDd
485.5 82.5 613.3 57.7 573.5 73.4 .49a
Comorbidity, No. (%)
CAD 6 (17) 23 (21) 8 (16) .74b
Hypertension 12 (33) 50 (46) 21 (42) .35b
COPD 7 (19) 18 (17) 12 (24) .44b
Diabetes 8 (22) 29 (27) 14 (28) .93b
Renal disease 4 (11) 9 (8) 10 (20) .15b
Liver disease 3 (8) 1 (1) 3 (6) .15b
Cancer 3 (8) 9 (8) 4 (8) .99b
Admission category, No. (%)
Cardiovascular 5 (14) 14 (13) 8 (16) .77b
Respiratory 13 (36) 24 (22) 20 (40) .66b
Neurological 3 (8) 8 (7) 3 (6) .99b
Metabolic 2 (6) 9 (8) 3 (6) .99b
Gastrointestinal 0 (0) 2 (2) 3 (6)6 .26b
Sepsis 2 (6) 4 (4) 0 (0) .18b
Postoperative 8 (22) 45 (41) 13 (30) .81b
APACHE II, Acute Physiology and Chronic Health Evaluation II;
CAD, coronary artery disease; COPD, chronic obstructive pulmonary
disease; SOFA,
Sequential Organ Failure Assessment. A total of 196 patient
blood specimens were available for analysis.Pvalues are from
univariate analysis.aAnalysis of variance testPvalue.
b2 testPvalue.cPatients were classified as having sepsis if at
any time during their stay they met systemic inflammatory response
syndrome criteria and had a source of
infection.dMean parenteral and enteral nutrition per day.
at A.S.P.E.N on August 28, 2013pen.sagepub.comDownloaded
from
http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/
-
7/27/2019 vit d jpen 2012
6/9
Vitamin D Deficiency in Critically Ill Patients/ Higgins et al
717
Pneumonia rates were 5%, 10%, and 16% in sufficient,
insufficient, and deficient patients, respectively. Although
the
rate of culture-positive and probable pneumonia between the
groups was higher in the 25(OH)D-deficient group, these
results were not significant (culture confirmed: OR, 4.24;
95%
CI, 0.5038.8, P= .21; probable pneumonia: OR, 3.07; 95%
CI, 0.76312.36,P= .11). Patients with a probable pulmonary
infection or pneumonia from documented infection or culture-
confirmed pneumonia diagnosed >48 hours after admission
had significantly lower levels of baseline 25(OH)D compared
with those who did not have pneumonia, as seen in Figure 3.
Discussion
Here we report an observational study evaluating the
relation-
ship between vitamin D deficiency and clinical outcomes in
an
unselected, heterogeneous critically ill patient population.
This study showed that a significant number of ICU patients
had inadequate vitamin D status (82% of patients were insuf-
ficient or deficient) on admission. In addition, this is the
first
study to describe a significant decrease in 25(OH)D levelsfrom
admission 25(OH)D levels as early as 3 days after admis-
sion and as late as 10 days. Our data also demonstrate a
high
incidence (39.1%) of sufficient patients becoming
insufficient
during their stay. We did not observe an association between
baseline 25(OH)D status and 28-day all-cause mortality, but
25(OH)D-deficient patients stayed significantly longer in
the
ICU, tended to develop more organ failure, and tended to
experience a higher number of infections, particularly pneu-
monia, compared with sufficient patients.
The outcomes associated with inadequate 25(OH)D status
seen in this study corroborate the findings of a recent
smaller
study (n = 41) by Lee et al19 that showed that 93% of
patients
had inadequate baseline 25(OH)D levels. However, little is
known about the measurement of 25(OH)D status during a
patients duration of stay. Only 1 smaller study21 (12
patients)
indirectly evaluated 25(OH)D status beyond admission levels
in the ICU, and to our knowledge, no studies have
demonstrated
a significant decrease in 25(OH)D status during the patients
stay. In our study, we show a significant decrease in
25(OH)D
levels over the first 310 days in the ICU in the sufficient
and
insufficient groups but no changes in patients who are
already
deficient. The explanation for this acute decrease in
25(OH)D
0
20
40
60
80
100
120
140
160
180
200
1-002
1-008
1-014
1-020
1-026
1-032
1-038
1-045
1-051
1-057
1-063
1-069
1-075
1-081
1-087
1-093
1-099
1-105
1-111
1-117
1-123
1-129
1-135
1-141
1-147
1-153
1-159
1-165
1-171
1-177
1-183
1-189
1-195
1-201
Admission25(OH
)D(nmol/L)levels
Paents
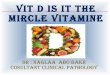
Figure 1. Admission levels of 25(OH)D (nmol/L) in 196
intensive care unit (ICU) patients. The following 25(OH)
D values were used for deficient, insufficient, and
sufficient
patients according to previously reported subgroups:
sufficient,
>60 nmol/L; insufficient, >30 to 60 nmol/L; and deficient,
30
nmol/L.
15
35
55
75
95
1 3 7 10
25(OH)D(nmol/L)
Days aer admission
All paents (n=44)
Deficient (n=15)
Insufficient (n=21)
Sufficient (n=8)
****
**
****
** **
****
Figure 2. Levels of 25(OH)D decreased over intensive care
unit
(ICU) patient stay. Levels of 25(OH)D on days 1, 3, 7, and
10
following admission were assayed from patient serum samples.
A
total of 44 patients (only patients who stayed 10 days or
longer)
are displayed in this figure. The data represent the mean SE
bars. The All patients line represents all patients who stayed
10
days or longer. The Sufficient, Insufficient, and Deficient
lines represent patients in the respective group who stayed
at
least 10 days or longer. **Pvalues
-
7/27/2019 vit d jpen 2012
7/9
718 Journal of Parenteral and Enteral Nutrition36(6)
in the sufficient and insufficient groups is not clear but could
be
due to changes in vitamin D binding protein (VDBP), which
approximately 85% of 25(OH)D is bound to.34 VDBP is
decreased in ICU patients and has been shown to be a
predictor
of ICU mortality.35 Another recent study demonstrated that
ICU
patients with sepsis and worse outcomes had significantly
lower levels of VDBP compared with those without sepsis.20 A
decrease in VDBP may be due to decreased protein synthesis
or
increased clearance of VDBP in ICU patients with liver,
renal,
or intestinal diseases. However, because VDBP concentrations
are much higher than 25(OH)D and VDBP has a high affinity
for vitamin D metabolites, reduced levels of VDBP often
result
in lower total 25(OH)D but do not affect free
concentrations.36
The VDBP relationship should be considered in any future
studies examining the acute changes in 25(OH)D observed in
this study.
In our study, we did not observe an association with 28-day
all-cause mortality and 25(OH)D status. This is in contrast
to
a recent study by Braun et al24 that evaluated preadmission
vitamin D levels and found vitamin D deficiency to be
significantly associated with 30-, 90-, and 365-day
mortality.
However, the prior study was limited by selection bias and
measurement of vitamin D status up to 365 days prior to ICU
admission. The lack of association of vitamin D status with
mortality in our study may be due to our study being
under-powered. We were not able to run a power analysis a
priori
because the relationship of vitamin D to mortality was not
the
initial end point of the trial at conception, but post hoc
power
analysis suggests that this study did not have the power to
detect small differences in mortality or infection rates
between
the groups (data not shown). Therefore, the failure to
demon-
strate statistically significant differences in mortality as
well as
infection rates in this study should not be interpreted as
evi-
dence for lack of a true difference. In fact, the magnitude of
the
association with infection and vitamin D levels is quite
large
(OR, 1.73.2), but we lacked statistical precision because of
our limited sample size.
The data presented here are the largest thus far to report
an
increased time-to-alive ICU discharge associated with admis-
sion vitamin D deficiency. Our study also suggests a
hypothe-
sis for the observed increased time-to-alive ICU discharge.
We
used a very rigorous adjudication process to determine the
presence or absence of infection and a rigorous definition
of
pneumonia. Our observation of increased infection rates and
decreased organ function may be factors associated with
vita-
min D deficiency that could contribute to prolonged time-to-
alive ICU discharge and poorer outcomes in ICU patients.
This
potentially could be due to the role vitamin D has on the
immune system. In line with this, a recent report found
Table 3. Infection Outcomes in 25(OH)D Groups
Sufficient, No. (%)
Insufficient,
No. (%)
Deficient,
No. (%)
Deficient vs
Sufficient OR PValue
Possible ICU infection 5 (13%) 19 (17%) 12 (24%) 1.7 (0.48, 2.7)
.35
Probable ICU infection 4 (11%) 15 (14%) 9 (18%) 3.2 (0.78, 13.0)
.11
Probable pneumonia 2 (5%) 10 (10%) 8 (16%) 4.2 (0.46, 38.8)
.11Culture-positive pneumonia 2 (5%) 8 (7%) 6 (12%) 3.0 (0.76,
12.3) .20
Duration of ventilation, h,
mean SD
120 20.9 138 16.9 141 18.1 .49
Intensive care unit (ICU) infections were defined as infections
diagnosed >48 hours after ICU admission. Possible/probable
infection or probable pneu-
monia status was adjudicated by 2 independent clinicians. OR,
odds ratio.
0
10
20
30
40
50
0
10
20
30
40
50
60
No infecon Infecon
25(OH)D(nmol/L)
25(
OH)D(nmol/L)
A)
B)
* p=0.01
No pneumonia
(n=176)
* p=0.01 *p=0.05
Culture posive
(n=16)
No infecon (n=160) Infecon (n=36)
Pneumonia
(n=20)
Figure 3. (A) Baseline levels of 25(OH)D in patients with a
probable new infection vs no new infection diagnosed >48
hours after admittance to the intensive care unit (ICU). The
data represent the mean SD andPvalues compared with
no infection. (B) Baseline levels of 25(OH)D in patients
with
new culture-positive pneumonia, probable pneumonia, and no
pneumonia diagnosed >48 hours after admission to the ICU.
The
probable pneumonia group included culture-positive pneumonia
patients in addition to 4 patients without culture positivity
butclinical presentation of pneumonia. The data represent the
mean
SD andPvalues compared with patients with no pneumonia.
*P < 0.05.
at A.S.P.E.N on August 28, 2013pen.sagepub.comDownloaded
from
http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/
-
7/27/2019 vit d jpen 2012
8/9
Vitamin D Deficiency in Critically Ill Patients/ Higgins et al
719
significantly lower levels of the endogenous antimicrobial
peptide cathelicidin (LL-37) in critically ill patients who
were
vitamin D deficient, suggesting a role for vitamin D in
main-
taining innate immunity to infection in the ICU.20
Furthermore,
1,25(OH)D has been shown to have a stimulatory effect on the
innate immune system by increasing interleukin-1 (IL-1) pro-
duction and stimulating monocyte proliferation.37
Withoutthese important innate immune system stimulating
effects,
patients may be more susceptible to ICU infections. On the
other hand, sufficient levels of vitamin D have been
associated
with lower rates of autoimmune disorders, and it may be that
adequate levels of vitamin D are necessary to regulate
overac-
tive, pathologic inflammatory immune responses.10,14
Therefore
patients may be more susceptible to pathologic, overactive
immune responses to common ICU infections.
Limitations to this study include a relatively small sample
size and confounding variables that could not be accounted
for
in our multivariate analysis. For instance, the observed
vitamin
D deficiency in this study could be due to a number of con-
founding causes, including the fact that many patients have
limited exposure to UV-B light during chronic disease and
often have significant dietary alterations, and the calcium
parathyroidvitamin D axis may be disrupted in critical
illness,
so a consideration of PTH and Ca levels should be considered
in future studies.25,38 Although our study suggests an
associa-
tion between inadequate vitamin D levels and poor patient
out-
comes, this does not mean vitamin D is the direct cause of
the
poor outcomes. It is possible that the conditions leading to
poor outcomes cause a decrease in vitamin D levels, which
are
reactionary and not causal. More studies are needed to
deter-
mine if there is direct causality between admission vitamin
D
status and patient outcomes. Furthermore, although there wasnot
a statistically significant difference in the rates of
infection
and pneumonia, the significant differences in baseline levels
of
25(OH)D between infected and noninfected patients suggest
an association that this study may not have had the power to
observe in actual infection rates.
A recent report from the Institute of Medicine (IOM) points
out that cutoffs for vitamin D deficiency have not been
system-
atically developed.33 The cutoffs used for this study to
define
sufficient, insufficient, and deficient groups were selected
according to recently published articles on vitamin D in ICU
patients to allow for across-study comparison in ICU
patients.
Our cutoffs, although not exactly matching, are similar to
the
IOM report that suggests 25(OH)D levels
-
7/27/2019 vit d jpen 2012
9/9
720 Journal of Parenteral and Enteral Nutrition36(6)
Acknowledgments
The authors thank the Childrens Hospital Clinical and
Transla-
tional Research Center Core Lab in Denver, Colorado, for
techni-
cal support in analyzing vitamin D levels from serum.
References
1. Holick MF. High prevalence of vitamin D inadequacy and
implications for
health.Mayo Clin Proc. 2006;81(3):353-373.
2. Looker AC, Dawson-Hughes B, Calvo MS, Gunter EW, Sahyoun
NR.
Serum 25-hydroxyvitamin D status of adolescents and adults in
two sea-
sonal subpopulations from NHANES III.Bone. May
2002;30(5):771-777.
3. Rosen CJ. Clinical practice: vitamin D insufficiency. N Engl
J Med.
2011;364(3):248-254.
4. Ross AC, Manson JE, Abrams SA, et al. The 2011 report on
dietary refer-
ence intakes for calcium and vitamin D from the Institute of
Medicine:
what clinicians need to know.J Clin Endocrinol Metab.
2011;96(1):53-58.
5. DeLuca HF. Overview of general physiologic features and
functions of
vitamin D.Am J Clin Nutr. 2004;80(6)(suppl):1689S-1696S.
6. Holick MF. Vitamin D deficiency.N Engl J Med.
2007;357(3):266-281.
7. Munger KL, Levin LI, Hollis BW, Howard NS, Ascherio A.
Serum
25-hydroxyvitamin D levels and risk of multiple sclerosis.
JAMA.
2006;296(23):2832-2838.
8. Holick MF. Sunlight and vitamin D for bone health and
prevention of auto-
immune diseases, cancers, and cardiovascular disease. Am J Clin
Nutr.
2004;80(6)(suppl):1678S-1688S.
9. Holick MF. Vitamin D: importance in the prevention of
cancers, type 1
diabetes, heart disease, and osteoporosis. Am J Clin Nutr.
2004;79(3):
362-371.
10. Moro JR, Iwata M, von Andriano UH. Vitamin effects on the
immune system:
vitamins A and D take centre stage.Nat Rev Immunol.
2008;8(9):685-698.
11. Feskanich D, Ma J, Fuchs CS, et al. Plasma vitamin D
metabolites and
risk of colorectal cancer in women. Cancer Epidemiol Biomarkers
Prev.
2004;13(9):1502-1508.
12. Holick MF. Calcium plus vitamin D and the risk of colorectal
cancer.N
Engl J Med. 2006;354(21):2287-2288; author reply 2287-2288.
13. Merlino LA, Curtis J, Mikuls TR, Cerhan JR, Criswell LA,
Saag KG. Vita-
min D intake is inversely associated with rheumatoid arthritis:
results from
the Iowa Womens Health Study.Arthritis Rheum.
2004;50(1):72-77.
14. DeLuca HF. Evolution of our understanding of vitamin D.Nutr
Rev. Oct
2008;66(10)(suppl 2):S73-S87.
15. van Etten E, Mathieu C. Immunoregulation by
1,25-dihydroxyvitamin D3:
basic concepts.J Steroid Biochem Mol Biol.
2005;97(1-2):93-101.
16. Shapira Y, Agmon-Levin N, Shoenfeld Y. Mycobacterium
tuberculosis,
autoimmunity, and vitamin D. Clin Rev Allergy Immunol.
2010;38(2-
3):169-177.
17. Zaloga GP, Chernow B. The multifactorial basis for
hypocalcemia dur-
ing sepsis: studies of the parathyroid hormonevitamin D axis.Ann
Intern
Med. 1987;107(1):36-41.
18. Lucidarme O, Messai E, Mazzoni T, Arcade M, du Cheyron D.
Incidence and
risk factors of vitamin D deficiency in critically ill patients:
results from a
prospective observational study.Intensive Care Med.
2010;36(9):1609-1611.
19. Lee P, Eisman JA, Center JR. Vitamin D deficiency in
critically ill patients.
N Engl J Med. 2009;360(18):1912-1914.
20. Jeng L, Yamshchikov AV, Judd SE, et al. Alterations in
vitamin D status
and anti-microbial peptide levels in patients in the intensive
care unit with
sepsis.J Transl Med. 2009;7:28.
21. Mata-Granados JM, Vargas-Vasserot J, Ferreiro-Vera C, Luque
de Castro
MD, Pavon RG, Quesada Gomez JM. Evaluation of vitamin D
endocrine
system (VDES) status and response to treatment of patients in
intensive
care units (ICUs) using an on-line SPE-LC-MS/MS method.J Steroid
Bio-
chem Mol Biol. 2010;121(1-2):452-455.
22. McKinney JD, Bailey BA, Garrett LH, Peiris P, Manning T,
Peiris AN.
Relationship between vitamin D status and ICU outcomes in
veterans. J
Am Med Directors Assoc. 2011;12(3):208-211.
23. Cecchi A, Bonizzoli M, Douar S, et al. Vitamin D deficiency
in septic
patients at ICU admission is not a mortality predictor.Minerva
Anestesiol.
2011;77(12):1184-1189.
24. Braun A, Chang D, Mahadevappa K, et al. Association of low
serum
25-hydroxyvitamin D levels and mortality in the critically ill.
Crit Care
Med. 2011;39(4):671-677.
25. Lee P, Nair P, Eisman JA, Center JR. Vitamin D deficiency in
the intensive
care unit: an invisible accomplice to morbidity and mortality?
IntensiveCare Med. 2009;35(12):2028-2032.
26. Heyland DK, Govert, J, Garrard C. Waveform abnormalities of
APPT in
critically ill hospitalized patients: the WATTCH study. Crit
Care Med.
2006;34(12):A100.
27. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a
sever-
ity of disease classification system. Crit Care Med.
1985;13(10):818-829.
28. Moreno R, Vincent JL, Matos R, et al. The use of maximum
SOFA score to
quantify organ dysfunction/failure in intensive care: results of
a prospec-
tive, multicentre study. Working Group on Sepsis related
Problems of the
ESICM.Intensive Care Med. 1999;25(7):686-696.
29. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance
definition of
health careassociated infection and criteria for specific types
of infections
in the acute care setting.Am J Infect Control.
2008;36(5):309-332.
30. Heyland DK, Dodek P, Muscedere J, Day A, Cook D. Randomized
trial of
combination versus monotherapy for the empiric treatment of
suspected
ventilator-associated pneumonia. Crit Care Med.
2008;36(3):737-744.
31. A randomized trial of diagnostic techniques for
ventilator-associated pneu-
monia.N Engl J Med. 2006;355(25):2619-2630.
32. Ginde AA, Mansbach JM, Camargo CA Jr. Vitamin D, respiratory
infec-
tions, and asthma. Curr Allergy Asthma Rep. 2009;9(1):81-87.
33. Ross AC, Institute of Medicine Committee to Review Dietary
Reference
Intakes for Vitamin D and Calcium.Dietary Reference Intakes for
Calcium
and Vitamin D. Washington, DC: National Academies Press;
2011.
34. Jafri L, Khan AH, Siddiqui AA, et al. Comparison of high
performance
liquid chromatography, radio immunoassay and
electrochemilumines-
cence immunoassay for quantification of serum 25 hydroxy vitamin
D.
Clin Biochem. 2011;44(10-11):864-868.
35. Dahl B, Schiodt FV, Nielsen M, Kiaer T, Williams JG, Ott P.
Admis-
sion level of Gc-globulin predicts outcome after multiple
trauma. Injury.
1999;30(4):275-281.
36. Bikle DD, Halloran BP, Gee E, Ryzen E, Haddad JG. Free
25-
hydroxyvitamin D levels are normal in subjects with liver
disease and reduced
total 25-hydroxyvitamin D levels.J Clin Invest.
1986;78(3):748-752.
37. Mora JR, Iwata M, von Andrian UH. Vitamin effects on the
immune system:
vitamins A and D take centre stage.Nat Rev Immunol.
2008;8(9):685-698.
38. Kelly A, Levine MA. Hypocalcemia in the critically ill
patient.J Intensive
Care Med. 2011 Aug 12. [Epub ahead of print]
39. Binkley N, Krueger D, Gemar D, Drezner MK. Correlation
among
25-hydroxy-vitamin D assays. J Clin Endocrinol Metabolism.
2008;93
(5):1804-1808.
40. Leino A, Turpeinen U, Koskinen P. Automated measurement
of
25-OH vitamin D3 on the Roche Modular E170 analyzer. Clin
Chem.
2008;54(12):2059-2062.
41. Ersfeld DL, Rao DS, Body JJ, et al. Analytical and clinical
validation of
the 25 OH vitamin D assay for the LIAISON automated analyzer.
Clin
Biochem. 2004;37(10):867-874.
42. Antoniucci DM, Black DM, Sellmeyer DE. Serum
25-hydroxyvitamin
D is unaffected by multiple freeze-thaw cycles. Clin Chem.
2005;51(1):
258-261.
43. A.S.P.E.N. Board of Directors and the Clinical Guidelines
Task Force.
Guidelines for the use of parenteral and enteral nutrition in
adult and pediat-
ric patients.JPEN J Parenter Enteral Nutr.
2002;26(1)(suppl):1SA-138SA.
44. Van den Berghe G, Van Roosbroeck D, Vanhove P, Wouters PJ,
De Pourcq
L, Bouillon R. Bone turnover in prolonged critical illness:
effect of vitamin
D.J Clin Endocrinol Metab. 2003;88(10):4623-4632.
45. Amrein K, Sourij H, Wagner G, et al. Short-term effects of
high-dose oral
vitamin D3 in critically ill vitamin D deficient patients: a
randomized,
double-blind, placebo-controlled pilot study. Crit Care.
2011;15(2):R104.
at A.S.P.E.N on August 28, 2013pen.sagepub.comDownloaded
from
http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/http://pen.sagepub.com/
















![43 Fitrah - Vit D Status_rev [Indo, 141124]](https://img.pdfslide.net/doc/110x75/55cf8fa9550346703b9e8550/43-fitrah-vit-d-statusrev-indo-141124.jpg)










