Embed Size (px)
DESCRIPTION
journal of pedaitric
Citation preview

CORRESPONDENCE* All letters must be typed with double spacing and signed by all authors.
* No letter should be more than 400 words.
* For letters on scientific subjects we normally reserve our correspondence columnsfor those relating to issues discussed recently (within six weeks) in the BMJ.
* We do not routinely acknowledge letters. Please send a stamped addressedenvelope ifyou would like an acknowledgment.
* Because we receive many more letters than we can publish we may shorten thosewe do print, particularly when we receive several on the same subject.
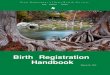
Abortion rates still risingSIR,-A recent report from the Office ofPopulationCensuses and Surveys' has been widely quoted inthe press,2 3and was reported by Ms Luisa Dillner,4as indicating that the abortion rate has tripled inthe past 20 years in England and Wales. Detailedanalysis of these figures, however, shows thatrequests for abortion have remained remarkablyconstant since 1972 (figure).The initial rapid rise from 3-5/1000 women aged
15-44 in 1968 (the first year when abortions werenotified) to a level rate of 11 0/1000 in the 1970sprobably reflects the increasing availability of legaltermination of pregnancy and corresponds to adecrease in illegal abortion. Much of the modestincrease since then (35%) can be explained bydemographic changes rather than a profoundchange in women's requests for abortion. Womenborn during the "baby boom" of 1960-5 reachedsexual maturity during the 1980s, and hence alarger proportion of the female population is at riskof unwanted pregnancy. The Office of PopulationCensuses and Surveys calculated that becausethere has been an increase in the proportion ofwomen aged between 16 and 29 (a group that has ahigher termination rate than older women) withoutany change in the age specific termination rates thenumber of terminations would have been expectedto increase by 14% between 1972 and 1989.The remaining increase is likely to be due mainly
to a gradual change in the attitudes of doctors,and particularly gynaecologists, to therapeuticabortion in certain parts of the country. In Scotlandthere were appreciable regional differences in theabortion rate in 1972, with the rate in the westbeing half that in the north and east. Though therates in the east and north have remained fairlyconstant over the past 20 years (for example, thatin Grampian), the rate in Greater Glasgow hasdoubled to reach the national average. Thesedifferences probably reflect the influence of two
X1 16 pEngland and14 / Wales(o)
12 A ,c~~~~ cE >rGlasgow (e)
10 Grampiana(*)88d;/;96 so -°'> W < Scotand (o)
S6 *i
Z 21970 1974 1976 1980 1984 1988
Abortion rate among women aged 1544 in Grampianregion, Greater Glasgow, Scotland, and England andWales, 1970-88*Figures for North East Scotland Regional Hospital Board. tFiguresfor West ofScotland Regional Hospital Board.
eminent senior gynaecologists. My father, SirDugald Baird, who worked in Aberdeen, played animportant part in supporting the change in theAbortion Law in 1967; Professor Ian Donald inGlasgow was vehemently opposed to therapeuticabortion. Though religious and social factors mayhave had some role, it seems unlikely that the risein abortion rate in Glasgow is totally unrelated tothe retiral of Professor Donald in 1976. Similarregional differences in attitudes existed throughoutEngland and Wales, and hence the increase in theabortion rate nationally probably reflects thegradual levelling out of provision of abortionservices rather than an increased resort to abortionas a means of controlling fertility.A major factor determining the demand for
abortion is the provision of contraceptive services.The abortion rate in Scotland (9-8/1000 womenin 1989) is lower than that in most Europeancountries and less than one third that in the UnitedStates' partly because contraception is widelyavailable to all sections of the community from theNHS. Recent attempts by many health authoritiesto limit the provision of "social" sterilisations andto reduce budgets for family planning services maylead to a rise in the incidence of unplanned andunwanted pregnancies. The consequent increasein the demand for therapeutic abortion would bevery undesirable at a personal level and would putincreasing strain on medical services.
DAVID T BAIRDCentre for Reproductive Biology,Department ot Obstetrics and Gynaccology,University of Edinburgh,Edinburgh EH3 9EW
I Office of lopulation Censuses and Surveys. 'I'rends in abortion.In: Population trends 64. London: Government StatisticalService, 1991:19-29.
2 Fletcher D. Abortion rate has trebled in 20 years. Daily Telegraph1991 June 19:4(col 1).
3 Hunit L. Abortions on the increase. Independent 1991 June19:4(col ).
4 Dillner L. Abortion rates still rising. BMJ 1991;302:1559-60.(29 June.)
5 Henshaw SK. Induced abortion: a world review. FamilyPlanning Perspecti'ves 1990;22:76-89.
Vital statistics of birthsSIR,-The measurement of maternal mortalityis important enough that a minor point in DrGeoffrey Chamberlain's excellent paper' deservesmention. The denominator for maternal mortalityin a given year is either the total number of birthsor the number of live births during that year, notthe number of maternities-the term maternities isambiguous. The World Health Organisation'sdefinition states that "A 'maternal death' is definedas the death of a woman while pregnant or within42 days of termination of pregnancy, irrespectiveof the duration and the site of the pregnancy,
from any cause related to or aggravated by thepregnancy or its management, but not fromaccidental or incidental causes" and goes on tosay that "the denominator used for calculatingmaternal mortality should be specified as eitherthe number of live births or the total number ofbirths (live births plus fetal deaths). Where bothdenominators are available, a calculation should bepublished for each."2To allow for an extension of the period during
which deaths can be related to pregnancy or itsoutcome, the 1989 international conference for thetenth revision of the International Classification ofDiseases introduced the concept of late maternaldeath: "A 'late maternal death' is defined as thedeath of a woman from direct or indirect obstetriccauses more than 42 days but less than one yearafter the termination of pregnancy."2
Similarly, the conference has introduced theconcept of "pregnancy related death" to permitclassification of deaths of women while pregnantor when recently delivered, even though localfacilities may not allow the cause of death to beidentified as "related to or aggravated by thepregnancy or its management." A pregnancyrelated death is thus defined as "the death of awoman while pregnant or within 42 days oftermination of pregnancy, irrespective of the causeof death." It. is likely, for instance, that somehomicides and suicides of pregnant or recentlypregnant women fall into this category, andaccidents may also be considered in this light,in so far as fatigue or reduced mobility in advancedpregnancy affects ability to avoid or surviveaccidents.'
A C P' L'HOURSM C THURIAUX
Division ot Epidemiological Surveillance andHealth Situation and Trend AssessmentStrengthening of Epidemiological andStatistical Services,
World Health Organisation,1211 Geneva,Switzcrland
I Chamberlain G. Vital statistics of births. BMJ 1991;303:178-81.(20 July.)
2 International conference for the tenth revision of the InternationalClassification of I)iseases, Geneva, 26 September-2 October1989. Wttrld Health Statistics Quarterly 1990;43:204-45.
3 Fortney JA. Implications of the ICD-I( definitions related todeath in pregnancy, childbirth or the puerpwrium. WorldHealth Statistics Quarterly 1990;43:246-8.
Nursing: an intellectual activitySIR,-For doctors to comment on matters con-cerning nursing risks touching a raw nerve-the"doctor's handmaiden" nerve-but the forthrightviews of June Clark, a professor of nursing,deserve discussion.' Doctors and nurses need each
BMJ VOLUME 303 7 SEPTEMBER 1991 579