Embed Size (px)
DESCRIPTION
Vitamin D: a growing problem. Dr James Bunn Alder Hey Children’s Hospital NHS FT No commercial interests No conflicts of interest. Vitamin D. Deficiency causes problems in: Bone growth Rickets and musculoskeletal pain craniotabes Muscle functioning Myopathy / cardiomyopathy - PowerPoint PPT Presentation
Citation preview
Vitamin D: a growing problem
Dr James BunnAlder Hey Children’s Hospital NHS FT
No commercial interestsNo conflicts of interest

Vitamin D
Deficiency causes problems in:Bone growth
Rickets and musculoskeletal paincraniotabes
Muscle functioningMyopathy/ cardiomyopathy
Calcium and phosphate regulationHypocalcaemic convulsions in infants
Susceptibility to InfectionIncreased risk of TB, and response to Rx

Metabolism of vitamin D
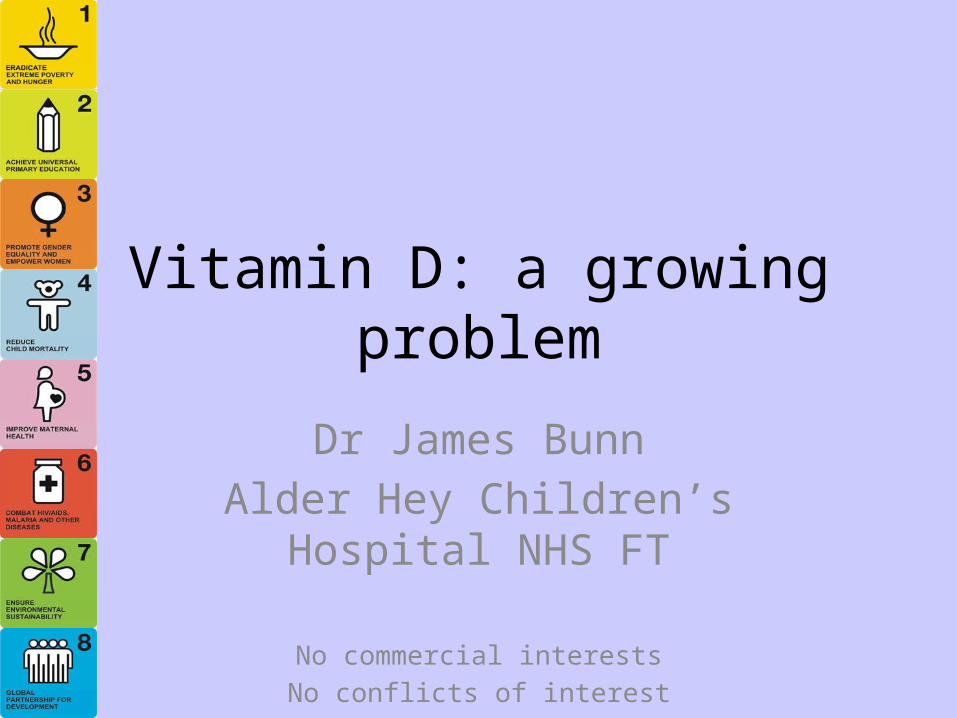
Potential Immunologic effects

8 interesting facts
90% of vit D comes from sunshineSeasonal pattern for deficiencyPigmented skin needs up to 6x more sunFactor 15+ sunscreen blocks >99% of sunBreast milk has limited vit D (25 IU/litre)Maternal vitamin D a good source for babyFortification is only in some foodsBME diets may not utilise fortified foods
A growing problem
Increase in the level set for sufficiencySurveys suggest highly prevalent
In Somali community 82% deficient
Associated conditions increasingChronic diseases and Obesity
Increasingly recognisedHigh profile casesAdvocacyIncreased testing

Clinical cases
3 month old, 5th childAfro-Carribean parentsBreastfed5 minute convulsion,
calcium 1.8mmol/l, PTH 48.1Reduced bone density
Family historyhypocalcaemic convulsion in 12 y old siblingMother vitamin D deficient, no pregnancy vit D

Cardiomyopathy
16 cases at Great Ormond StreetPresenting with heart failureInfants, first year of life12 were exclusively breastfed

Case study
4 year old with aches and painsSome splaying of wrists
X ray changes of ricketsVitamin D deficient 15nmol/lRx cholecalciferol 200,000 units total dose
Choice of 6,000 units daily for 1 monthOr 20,000 units for 10 doses
Check symptomatic response, and bottleRepeat blood biochemistryConsider family members vit D risk
Case study
10 year old Caucasian child referred by GPInsufficient vit D3 (37pmol/l), vit D2 <4 Blood tested as abdominal painAsymptomatic
Vit D probably not cause of symptoms
Supplement 400 IU/ day for winter months
Co- morbidity
Renal diseaseGut malabsorptionCystic fibrosisNeuromuscular diseaseDrug interaction e.g. Anticonvulsants(Obesity)
Pathways now suggesting yearly testing

At risk groups
BMECultural
covered skin (in mother or child)Reduced use of fortified foods
Sunblocks and conflicting messagesBreastfeeding

Guidance on prevention
COMA 2003NICE (in low income households) 2008CMO 2012RCPCH 2012
All indicate children <4-5 years should be supplemented when not on formula milk, and all mothers supplemented in pregnancyBut only NICE is a required provision for CCGs and TrustsHealthy Start vitamins are the available intervention
Uptake Nationally is low, and process complex

Choices in Management
Adequate fortification for populationAdvise high vitamin D containing foodsSupplement allSupplement those on low incomesSupplement high risk groupsTest high risk groups and treatTest only when symptomatic, and treatAwait morbidity (and occasional mortality)
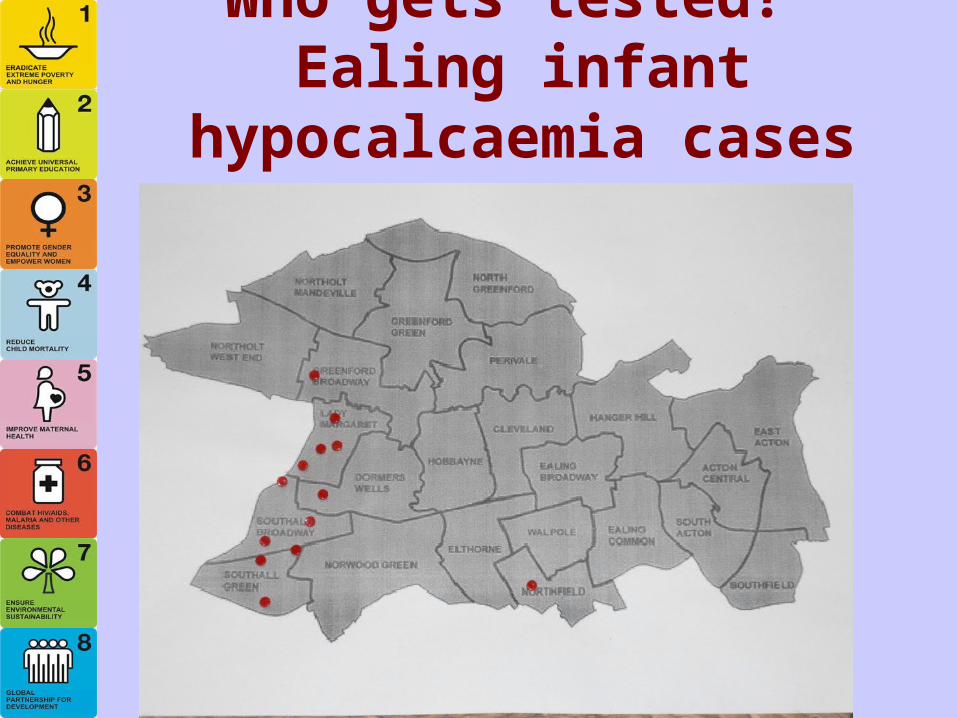
Who gets tested? Ealing infant hypocalcaemia cases

GP vit D tests (yellow) and top 10 vit D prescribing practices (green) in Ealing
Credit to Colin MitchieEaling Hospital for maps

Experience at Alder Hey
2007-8 2008-9 2009-10 2010-11 2011-120
200
400
600
800
1000
1200
1400
Total Tests done

Seasonality of deficiency
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
AdequateDeficientInsufficientSeverely Deficient

Proportion deficient unchanged
Toxic Adequate Insufficient Deficient Severely Deficient0%
10%
20%
30%
40%
50%
60%
70%
80%
2007-82008-92009-102010-112011-12

Increase in deficiency in those first tested
Toxic Adequate Insufficient Deficient Severely Deficient0%
10%
20%
30%
40%
50%
60%
70%
80%
2008-92009-102010-112011-12

Deficiency in older children:? related to testing protocols
<1 year 1-4 Years 5-12 Years >12 YEARS0%
10%
20%
30%
40%
50%
60%
70%
80%
Toxic Adequate
Insufficient Deficient
Severely Deficient

Which specialty is testing?
AE
Cardi
oEn
do
Gastro
Gen P
aeds
GP/Com
mun
ity
Haem
/Onc
HDU/ICU
ID/Im
mun
olog
y
Nephr
o
Neuro
Ortho
Other
Resp
Rheum
Surg
ery
Unkno
wn
0
50
100
150
200
250
2007-82008-92009-102010-112011-12

General practice is more awareand testing kids more

Challenges
What products are available
Multivitamins recommended as supplementVitamin D products +/- calciumCholecalciferol (vit D3) recommended as RxErgocalciferol (Vit D2) alfacalcidol (one alpha) only in renal disease

Drug or food supplement?Quality assurance of vit D
Does not require same level of QA as drugs
QA testing of possible Rx17% active ingredient in one liquidVariable in capsules (~25%)
Specials very expensiveUp to £500 from community pharmaciesModerately cheaper from hospitals
? QA for Healthy Start

Challenges
NICE only for low incomeHealthy Start very low uptake
Targeted v.s. Cost recovery vs Universal
Conflict with Breastfeeding messagesConflict with skin cancer avoidance message
Potential for Commercial interest Vit D supplemented ‘more healthy’ products

Some practical points
If not symptomatic - supplement, don’t testSupplement family members of cases
Under 5, growth spurt, pre pregnant, pregnant
Ensure supplementation in all pregnanciesCheck if iron deficient as wellTop up vitamin D each winter in deficiencyPublic health approaches cheaper than test and treat approaches
Cautions on measuring vitamin D supplementation programme success
Increased recognition of symptomsIncrease in testing, so may identify moreIncreasing numbers on treatment.Case reporting not helpful (eg BPSU)
Poor definition of common morbidityHypocalcaemic convulsions rare
A need for true population surveysMeasure coverage of intervention

Vitamin D: a growing problem
Better recognition of symptomsRisk groups and obesity increasingRecognition of non bony morbidityIncreased testing
? Appropriately directed
Increasing scientific publicationIncreasing public interestCommercial opportunism