Embed Size (px)
Citation preview

VITRECTOMY FOR DIABETIC VITREOUS HEMORRHAGE
RONALD G. M I C H E L S , M.D. , THOMAS A. R I C E , M.D. , AND E L L E N F. R I C E , B.A. Baltimore, Maryland
The surgical results for 248 eyes that underwent vitrectomy for diabetic vitreous hemorrhage showed that at the final examinations, 194 (78%) had improved visual acuities, 43 (17%) had worse visual acuities, and 11 (4%) were unchanged. Of the 248 eyes, 60 (24%) had final visual acuities of 20/40 or better, 128 eyes (52%) had final visual acuities of 20/50 to 20/800, and 60 (24%) had final visual acuities worse than 20/800. Eyes with preoperative iris neovascularization had a substantially worse visual result than eyes without this complication. Eyes in which the lenses were removed during vitrectomy also had worse visual results, primarily because they had a higher cumulative incidence of postoperative iris neovascularization and neovascular glaucoma.
Vitreous surgery is frequently used to treat the complications of proliferative diabetic retinopathy that cause severe visual loss. With these surgical methods, vitreous hemorrhage can be cleared and traction on the retina can be reduced by excising the posterior vitreous surface and portions of extraretinal fibrovascular tissue. Vitreous surgery is often recommended in diabetic eyes with (1) non-clearing vitreous hemorrhage, (2) traction retinal detachment involving the macula, and (3) rhegmatogenous retinal detachment in which release of vitreoretinal traction facilitates treatment of any posterior retinal break causing the rhegmatogenous component. We analyzed our results and the complications that occurred during treatment of dense vitreous hemorrhages in 248 diabetic eyes in which no retinal break was present preoperatively and the macula was not involved by traction retinal detachment.
Accepted for publication Sept. 17, 1982. From the Department of Ophthalmology, Johns
Hopkins University School of Medicine, Baltimore, Maryland.
Reprint requests to Ronald G. Michels, M.D., Wilmer Institute 116, Johns Hopkins Hospital, Baltimore, MD 21205.
SUBJECTS AND M E T H O D S
We reviewed the charts of 259 consecutive diabetic eyes in which we had performed pars plana vitrectomy to treat dense vitreous hemorrhage of more than six months' duration, in which no retinal breaks were present preoperatively, and in which the macula was not involved by traction retinal detachment. Data were recorded for factors regarding (1) the patient's medical history, (2) preoperative vision and anatomic findings in the eye undergoing surgery, including the status of the cornea, iris, and lens, the intraocular pressure, and the vitreoretinal relationships, (3) details of the operation, including whether the surgical objectives were achieved and whether complications occurred, and (4) visual acuity, anatomic features, and complications postop-eratively.
We asked the patients to return for further examination if they had not been examined at least six months after the operation. If the patient could not return, the referring ophthalmologist provided current findings.
Detailed follow-up information for at least six months after the operation was available for 248 of the 259 eyes. We
12 ©AMERICAN JOURNAL OF OPHTHALMOLOGY 95:12-21, 1983

VOL. 95, NO. 1 VITRECTOMY FOR VITREOUS HEMORRHAGE 13
excluded the other 11 eyes that had less than six months of follow-up. Therefore, our study group included 248 eyes.
These 248 cases occurred in 119 men and 105 women ranging in age from 20 to 80 years (median age, 53 years). Twenty-four patients had both eyes operated on at different times. The series included 124 right eyes and 124 left eyes. The follow-up intervals ranged from \six months to 75 months (median follow-up, 16 months).
RESULTS
Of the 248 eyes, 188 eyes (76%) attained final visual acuities of 20/800 or better, which is considered to be in the useful functional range (Table 1). Sixty eyes (24%) had final visual acuities worse than 20/800. Only ten eyes (4%) achieved final visual acuities of 20/20, but 60 eyes (24%) attained visual acuities of 20/40 or better. Most eyes (128 eyes; 52%) had impaired but functional vision, with visual acuities ranging from 20/50 to 20/800. Of the 248 eyes, however, 135 (54%) remained legally blind with visual acuities of 20/200 or worse and 16 eyes (6%) had no light perception postoperatively.
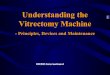
Figure 1 shows a comparison of the final visual acuities to the preoperative visual acuities. A total of 194 eyes (78%) had better postoperative than preopera-
TABLE 1 FINAL VISUAL ACUITY IN 248 DIABETIC EYES OPERATED ON FOR VITREOUS HEMORRHAGE
Final Visual Acuity
20/15 to 20/20 20/25 to 20/40 20/50 to 20/180 20/200 20/300 to 20/800 4/200 to 1/200 Hand motions Light perception No light perception
Eyes No.
10 50 53 42 33 6
12 26 16
%
4 20 21 17 13 2 5
10 6
tive visual acuities, 43 eyes (17%) were worse postoperatively, and 11 eyes were unchanged. If a clinically significant change from the preoperative to the final visual acuity is assumed to be at least a doubling or halving of the subtended visual angle (of the smallest test letter), visual acuities improved in 190 eyes (77%), worsened in 42 eyes (17%), and remained the same in 16 eyes (6%).
We analyzed various preoperative and surgical factors to determine whether they influenced the visual results of surgery (Table 2).
Of 225 eyes without preoperative iris neovascularization, 177 (79%) achieved final visual acuities of 20/800 or better, whereas only 11 (48%) of 23 eyes with preoperative iris neovascularization achieved this level. The difference was statistically significant (P < .01 by chi-square test). Abnormal blood vessels visible on the iris, including vascular tufts along the pupillary margin or vessels in the anterior-chamber angle, or both, were recorded as iris neovascularization. Transient dilated vessels in the stroma, judged to be the result of inflammation, were not recorded as iris neovascularization. We did not use iris fluorescein angi-ography to determine whether iris neovascularization was present.
The poorer visual outcome in the group of eyes with preoperative iris neovascularization was associated with several postoperative complications, including neovascular glaucoma, vitreous hemorrhage, and retinal detachment. Seventeen (74%) of the 23 eyes had persistent iris neovascularization after vitrectomy, and four eyes (17%) developed neovascular glaucoma; the rate of these complications was much lower in eyes without preoperative iris neovascularization.
We found that other preoperative factors were not associated to a statistically significant degree with postoperative visual acuities worse than 20/800. These factors included the severity of preopera-

14 AMERICAN JOURNAL OF OPHTHALMOLOGY JANUARY, 1983
O < _l < ù > _é <
6/4.5 6 / 6
6/7.5
6/15
6/30
6/60
6/80
6/120
6/240
6/1200
HM
LP
NLP
· · — · · ·
- · · • • • - ·
· · · - · · · · · ·
· · · · · · — · • · · - · • •
V
£Λ
/ 1 1
· · · · θ · · 1 5 i • · · ·
· · · : : •
· · · · · • · ·
• · β · ·
X 1
•
• · · · · ·
· · · · · · · · · ·Λ · · Τ· .
• •
2*2··· · ·
•
• /
• /
/ ·
• · ·
· · · · · ·
• · · 1 1 1
· · •
· ·
•
1
· ·
• · · ·* > • · /
•
•
•
1 1 1 1 1 1 NLP LP HM 6 6
1200 240 120 80 60 30 15 7.5 ' 4 . 5
INITIAL VISUAL ACUITY Fig. 1 (Michels, Rice, and Rice). Scattergram shows the initial (preoperative) visual acuity vs the final
postoperative visual acuity for each of the 248 diabetic eyes. Each dot represents one eye. Dots above the diagonal line had improved final visual acuities, dots below the diagonal line had worse final visual acuities, and dots on the diagonal line had unchanged visual acuities.
tive retinal neovascularization, the presence or absence of preoperative scatter retinal photocoagulation, and the presence or absence of preoperative extra-macular traction retinal detachment. Eyes with traction detachments of the macula were excluded from this study.
As a group, eyes that underwent lens removal during vitrectomy had poorer final visual results than those in which the lenses were not removed. In the early
part of this study, many clear lenses were removed. Table 2 shows that 61 of 71 eyes (86%) in which the lenses were retained achieved visual acuities of 20/800 or better, but only 112 of the 156 eyes (72%) in which the lenses were removed achieved this level (P < .001 by chi-square test). Many of the aphakic eyes with poor postoperative vision also had iris neovascularization and resultant complications. These complications accounted for some

VOL. 95, NO. 1 VITRECTOMY FOR VITREOUS HEMORRHAGE 15
TABLE 2 EFFECT OF VARIOUS PHEOPERATIVE AND SURGICAL FACTORS ON FINAL VISUAL RESULTS
Eyes With Final Visual Acuities of 20/800 or Better
Factors No.
Preoperative Factors Iris neovascularization
Absent Present
Retinal neovascularization None or atrophie Severe
Retinal scatter photocoagulation None 75% of retina to complete
Extramacular traction retinal detachment Absent Present
177 of 225 11 of 23
17 of 23 64 of 81
92 of 129 18 of 21
132 of 176 56 of 72
Surgical Factors Status of lens
Not removed during vitrectomy Removed during vitrectomy Aphakic before vitrectomy
Prophylactic 360-degree peripheral retinal cryotherapy No Yes
Prophylactic encircling band No Yes
Iatrogenic retinal break No Yes
62 of 71 112 of 156 15 of 21
56 of 76 92 of 117
80 of 103 79 of 104
159 of 207 26 of 35
79 48 74 79 71 86 75 78
86 72 71
74 79 78 76 77 74
of the visual differences, although aphakic eyes also had retinal detachment after vitrectomy more frequently.
Peripheral retinal cryotherapy (for 360 degrees) and an encircling silicone band to create a scierai buckle beneath the vitreous base were used in many eyes in the first part of this series, even when no retinal break was found during the operation, to reduce the chance of later retinal detachment caused by anterior retinal breaks. We later discontinued these techniques as a prophylactic measure. These additional steps were not associated with a significantly different visual outcome. Ninety-two of 117 eyes (79%) that underwent peripheral retinal cryotherapy achieved final visual acuities of 20/800 or
better, and 56 of 76 eyes (74%) that did not undergo retinal cryotherapy attained that level. Of the 76 eyes that did not undergo prophylactic peripheral cryo-pexy, four (5%) developed postoperative rhegmatogenous retinal detachments compared to 15 of 117 eyes (13%) that did undergo prophylactic peripheral cryo-pexy, but this difference was not statistically significant.
Of the 104 eyes in which prophylactic encircling scierai bands were placed, 79 (76%) achieved final visual acuities of 20/800 or better, and 80 of 103 eyes (78%) in which scierai buckles were not placed attained this level. Of the 103 eyes in which prophylactic encircling bands were not placed, six (6%) developed postopera-

16 AMERICAN JOURNAL OF OPHTHALMOLOGY JANUARY, 1983
tive rhegmatogenous retinal detachment, compared to 14 eyes of the 104 eyes (13%) with prophylactic encircling bands, but this difference was not statistically significant. Intraocular gas was used in most instances to treat retinal breaks, and therefore no meaningful comparisons of visual outcome in eyes in which gas was used to visual outcome in eyes in which it was not used can be made.
Retinal breaks were the most common serious surgical complication. Retinal breaks occurred in 35 eyes (14%) and were usually treated with a combination of cryotherapy, intraocular gas, and a scierai buckle. Of the 35 eyes with iatro-genic retinal breaks, 26 (74%) had final visual acuities of 20/800 or better. This was not significantly different from the results in 207 eyes without retinal breaks; 159 of the 207 (77%) attained this level.
Other surgical and postoperative complications also affected the visual outcome and, in some cases, required additional surgery or laser treatment. Fifty-seven eyes (23%) had further surgery, and 15 eyes (6%) had two or more reoperations. The two main reasons for reoperation were repairing rhegmatogenous retinal detachment and removing persistent postoperative vitreous hemorrhage. Repeat surgery for retinal detachment, with or without lavage of vitreous hemorrhage, was performed in 28 eyes (11%); 12 (43%) of these eyes had final visual acuities of 20/800 or better. Therapeutic lavage of the vitreous cavity without retinal reat-tachment surgery was done in 14 eyes (6%); seven (50%) of these eyes had final visual acuities of 20/800 or better.
Laser retinal photocoagulation was used on one or more occasions postopera-tively in 42 of 248 eyes (17%). Sixty percent of these laser treatments (38 of 63 treatments) consisted of scatter retinal photocoagulation to treat postoperative iris neovascularization in 28 eyes. Of these 28 eyes, 20 (71%) achieved regression or stabilization of the iris neovascu
larization. Laser treatment was also used for other reasons, such as to treat retinal breaks.
Some of the postoperative complications resolved or were treated successfully, but others were present at the final examinations. In the immediate postoperative period, transient corneal epithelial defects or increased intraocular pressure, or both, were present in some eyes; these abnormalities usually resolved. Other persistent and severe complications included corneal stromal opacities, iris neovascularization, neovascular glaucoma and other types of glaucoma, cataract, persistent vitreous hemorrhage, retinal detachment, and phthisis bulbi (Table 3).
Visually significant corneal opacities were present at the final postoperative examinations in 30 eyes (12%), 14 of which had glaucoma or phthisis bulbi.
Iris neovascularization occurred in 88 of 248 eyes (35%) after vitrectomy, including 17 of 23 eyes (74%) that had had
TABLE 3 POSTOPERATIVE COMPLICATIONS AFTER VITRECTOMY FOR DIABETIC VITREOUS
HEMORRHAGE
Complication
Corneal opacity at final examination Unassociated with glaucoma Associated with glaucoma or
phthisis bulbi Iris neovascularization Neovascular glaucoma Other glaucoma Cataract at final examination
Mild to moderate Severe Secondary lens removal for cataract
Persistent vitreous hemorrhage at final examination Mild Moderate Severe
Retinal detachment at final examination Traction, macular involvement Rhegmatogenous, macular involvement
Phthisis bulbi at final examination
Eyes No.
29 15
14 88 36 26 31 31 0 4
33
3 13 17 37 22 15 9
%
12 6
6 35 15 10 13 13 0 2
13
1 5 7
15 9 6 4

VOL. 95, NO. 1 VITRECTOMY FOR VITREOUS HEMORRHAGE 17
preoperative iris neovascularization. Excluding eyes that had had preoperative iris neovascularization, 71 of 225 eyes (32%) developed iris neovascularization after vitrectomy. As a group, the eyes with postoperative iris neovascularization had worse final visual results than eyes without this complication. Of 160 eyes that did not have postoperative iris neovascularization, 142 (89%) had final visual acuities of 20/800 or better, but only 46 of 88 eyes (52%) that had iris neovascularization after vitrectomy attained this level.
Postoperative iris neovascularization regressed in some cases, but 62 of 88 eyes (70%) had iris neovascularization at the final examinations. Of these 62 eyes, 27 (44%) had retinal detachments involving the macula at the final examinations. The macular detachment caused these eyes to be visual failures whether or not iris neovascularization was present. Of the 35 eyes (14% of the 248 eyes in the series) with iris neovascularization but without retinal detachment involving the macula at the final examinations, 18 (51%) had final visual acuities of 20/800 or better. The other 17 eyes (7% of the 248 eyes) had final visual acuities worse than 20/800.
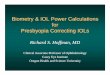
Figure 2 shows a survival curve for the cumulative incidence of iris neovascularization in two groups of eyes—those in which the lenses were removed and those in which they were retained. The curve includes eyes with less than six months of follow-up (not in our series of 248 eyes) but excludes eyes with preoperative iris neovascularization and eyes that were aphakic before vitrectomy. Eyes with moderate or severe lens opacities preop-eratively were also excluded from the analysis because the lens was removed in most of these eyes at vitrectomy and including them would have made the two groups dissimilar. The group that underwent lerjs removal had a statistically significant higher cumulative incidence of
is HI * υ io
IA> �
9 0 -
eo-7 0 -
6 0 -
5 0 -
4 0 -
3 0 -
2 0 -
10-
Lens removal, no cataract No lens removal, no cataract
^ - ^ (
r — i —Vs- i T- r T 1 1 r
,
1 1 8 9 10 II 12
MONTHS AFTER VITRECTOMY
Fig. 2 (Michels, Rice, and Rice). Survival curves show the cumulative incidence of iris neovascularization after vitrectomy for eyes that underwent lensec-tomy and eyes that did not.
postoperative iris neovascularization than did the group that did not undergo lens removal (P < .005 by a log-rank test). Subgroup analysis showed no other factors that invalidated these results. A more extensive analysis of this subject appears elsewhere in this issue.1
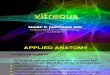
Thirty-four of the 36 eyes (94%) that developed neovascular glaucoma after vitrectomy were aphakic. The survival curve in Figure 3 shows the cumulative incidence of neovascular glaucoma for the same two groups of eyes. This difference
<t 2
Id O ά. 0-o a LI j
H m z
0- I I-3
éõõ-é 9 0 -
8 0 -
7 0 -
6 0 -
5 0 -
4 0 -
30-
20-
éï-0-
Lens removal, no cataract
No lens removal, no cataract
, I __J __
2 3 4 5 6 7 8 9 IO II
MONTHS AFTER VITRECTOMY
Fig. 3 (Michels, Rice, and Rice). Survival curves show the cumulative incidence of neovascular glaucoma after vitrectomy for eyes that underwent lensec-tomy and eyes that did not.

18 AMERICAN JOURNAL OF OPHTHALMOLOGY JANUARY, 1983
was statistically significant (P < .01 by a log-rank test).
Twenty-six eyes (10%) had other types of glaucoma after vitrectomy, excluding those eyes with transient increases in intraocular pressure in the immediate postoperative period. Most of the hypertensive eyes without neovascular glaucoma were successfully treated with medical therapy.
At the final examinations, 186 eyes (75%) were aphakic. These aphakic eyes included 156 in which the lenses were removed during vitrectomy, nine in which they were removed later, and 21 that were aphakic before vitrectomy. Of the 62 eyes (25%) in which the lenses were retained, 31 (50%) had no lens opacities at the final examinations and 31 (50%) had mild to moderate cataractous changes. No patient had severe lens opacities at the final examination. Later lens removal was performed in four of the nine eyes to remove cataracts. In the other five eyes a noncataractous lens was removed as part of an operation to remove persistent postoperative vitreous hemorrhage; two of these five eyes also underwent retinal reattachment surgery.
Vitreous hemorrhage was present in 33 eyes (13%) at the final examinations. This usually was blood remaining after intraoperative bleeding or from bleeding during the immediate postoperative period, but occasionally it resulted from later postoperative bleeding. Seventeen of these 33 eyes were judged to have severe vitreous hemorrhage at the final examinations, and 16 had mild to moderate amounts of blood in the vitreous cavity. Twenty-three of 186 aphakic eyes (12%) and ten of 62 eyes (16%) with lenses had vitreous hemorrhage at the final examinations. Moderate or severe vitreous hemorrhage was present in 21 of the aphakic eyes (11%) and in nine of the eyes with lenses (14%). Of the 33 eyes with vitreous hemorrhage at the final examinations, only eight (24%) had this as the
sole complication. Twenty-one eyes (64%) had iris neovascularization, seven (21%) had neovascular glaucoma, five (15%) had phthisis bulbi, and 16 (48%) had retinal detachments involving the macula. When opacities of the media obscured the fun-dus, the retina (for the purposes of this study) was judged to be detached at the final examination if it had been irreversibly detached previously or if ultrasono-graphy showed a detachment.
At the final examinations, 56 eyes (23%) had retinal detachments. These were traction detachments in 40 eyes and rhegmatogenous detachments in 16 eyes. The macula was detached in 37 of these 56 eyes (66%). Of the 186 aphakic eyes 34 (18%) had traction retinal detachments at the final examinations. In 21 of these eyes the maculas were detached. Fourteen of these 186 aphakic eyes (8%) had rhegmatogenous retinal detachments, and the maculas were detached in 13 of the 14. Of the 62 eyes with lenses at the final examinations, six (10%) had traction retinal detachments; in one of these the macula was detached. Two (3%) had rhegmatogenous retinal detachments, and the macula was detached in both.
Many eyes with complications at the final examinations had more than one complication. Of the 62 eyes with iris neovascularization, 27 (44%) had severe retinal detachments with macular involvement, and 13 (22%) had retinal detachment with macular involvement and vitreous hemorrhage. Of 33 eyes with vitreous hemorrhage, 16 (48%) had severe retinal detachments with macular involvement. Also, of these 33 eyes, 21 (64%) had iris neovascularization.
Many eyes, however, had no severe complications at the final examinations. Of the 248 eyes in the series, 165 (67%) had no neovascular glaucoma, vitreous hemorrhage, retinal detachment of the macula, or phthisis bulbi and 157 of these 165 eyes (95%) had final visual acuities of 20/800 or better.

VOL. 95, NO. 1 VITRECTOMY FOR VITREOUS HEMORRHAGE 19
DISCUSSION
The 248 diabetic eyes in this series all had preoperative dense, nonclearing vitreous hemorrhages without retinal breaks or traction retinal detachments involving the macula. However, in other ways the group was heterogeneous. There were various degrees of complexity of the vit-reoretinal relationships and differing amounts and features of fibrovascular tissue in the posterior segment. Visually significant cataracts, extramacular traction detachments, or both, were present in some eyes but not in others. The combination of vitrectomy with lens removal or scierai buckling, or both, also varied from case to case depending on preoperative and surgical findings and on the occurrence of complications.
The basic mechanical objectives of the operation, however, were constant throughout this series.24 In each case the objectives were to excise the opaque vitreous gel and as much of the posterior vitreous surface as possible in order to limit traction on the retina and to remove the scaffold of the posterior vitreous surface on which extraretinal fibrovascular tissue grows. This often included separating the epiretinal (flat) fibrovascular tissue from the retina or segmenting the tissue into separate islands.
In this study we required a minimum of six months of follow-up but the durations of follow-up varied from case to case. Comparisons within our series and comparisons of our series to others were not
controlled with regard to the differences in duration of follow-up. Other studies have shown, however, that the long-term visual and anatomic results are stable in 83% to 92% of diabetic eyes if a successful result is achieved for the first six months after vitrectomy.5,6 Because of this stabilization, disparities in the length of follow-up after the first six months are probably not important in comparing different groups of eyes.
The results obtained in this series were similar to those obtained by others7'9
(Table 4). Of the 248 eyes in our series, 194 (78%) had better visual acuities at the final examinations than they did preoper-atively. The only preoperative factor that was associated with a statistically significant poorer visual outcome was preoperative iris neovascularization, a finding supported by the results of another series.10
Of the eyes with preoperative iris neovascularization in our series, 74% had postoperative iris neovascularization, similar to the 66% reported by Blankenship.10
The poor visual outcomes in eyes with preoperative iris neovascularization was attributable in part to postoperative neo-vascular glaucoma, which occurred in 17% of these eyes, but also to a high frequency of coexisting retinal detachment.
We found that other preoperative factors did not significantly affect the postoperative success rate. The visual outcome was no worse in eyes with severe preoperative retinal neovascularization than in eyes with mild or atrophie neovas-
TABLE 4 RESULTS OF VITRECTOMY FOR SIMPLE DIABETIC VITREOUS HEMORRHAGE
Study
Peyman and associates7
Blankenship8
Machemer and Blankenship9
Present study
No. of Eyes
109 299 414 248
Improved No. %
72 182 242 194
66 61 59 78
Visual Results Unchangi
No.
29 66 84 11
ed %
27 22 21 4
Worse No.
8 50 87 43
%
7 17 20 17

20 AMERICAN JOURNAL OF OPHTHALMOLOGY JANUARY, 1983
cularization. This finding differed from that of Machemer and Blankenship,9 who reported that eyes with severe preoperative retinal neovascularization had an especially poor outcome. The reason for this difference is not clear, although differences in the grading of "severe" retinal neovascularization may have been partially responsible.
The only surgical factor associated with a significantly poorer visual outcome was lens removal. Of the 71 eyes in which the lenses were retained, 61 (86%) achieved final visual acuities of 20/800 or better, whereas only 112 of 156 eyes (72%) in which the lenses were removed during vitrectomy achieved this level. This difference was primarily the result of the significantly higher cumulative incidence of postoperative iris neovascularization and neovascular glaucoma in the eyes undergoing lens removal and the complications associated with these conditions. Also, eyes that were aphakic at the final examinations had retinal detachment more frequently.
Blankenship, Cortez, and Machemer11
did not find a poorer visual outcome in aphakic eyes. In their study, however, iris neovascularization, neovascular glaucoma, and associated complications were also more common in aphakic eyes. They believed that the increased occurrence of nonclearing postoperative vitreous hemorrhage in eyes with retained lenses counterbalanced the adverse effect on vision from anterior segment complications in aphakic eyes. In our series, moderate or severe vitreous hemorrhages at the final examinations were also more common in the eyes with retained lenses (nine of 62 eyes; 14%) than in aphakic eyes (21 of 186 eyes; 11%). However, this difference was slight and the effect was insufficient to counteract the adverse effects of iris neovascularization, neovascular glaucoma, and retinal detachment in the aphakic eyes.
Iatrogenic retinal breaks occurred in 35 of the 248 eyes (14%) in this series, comparable to the 17% to 18% rate reported in other series.8,9 In our series, creation of a retinal break did not adversely affect the final visual outcome, because in most such eyes this complication was successfully treated during surgery. Using prophylactic peripheral retinal cryotherapy or an encircling scierai buckle, or both, did not change the success rate. We did not use these methods in the latter part of the series unless definite retinal breaks or rhegmatoge-nous detachments were found.
Postoperative complications occurred in a clinically significant number of cases. Some complications, such as corneal epithelial defects and increases in intraocular pressure soon after vitrectomy, were transient and easily treated. Other complications required additional surgery or laser treatment. Some complications eventually resulted in loss of functional vision.
Iris neovascularization and neovascular glaucoma were frequent postoperative complications. These occurred significantly more frequently in aphakic eyes. The eyes that developed postoperative iris neovascularization had significantly worse final visual acuities than those that did not. The higher percentage with final visual acuities worse than 20/800 was partly the result of a higher frequency of retinal detachments involving the macula in eyes with iris neovascularization at the final examinations (27 of 62 eyes; 44%), but failures from complications of iris neovascularization without coexisting retinal detachment occurred in 17 eyes (7%). Because iris neovascularization and neovascular glaucoma had a higher cumulative incidence in aphakic eyes, it is reasonable to continue the current practice of not performing lensectomy along with diabetic vitrectomy in eyes without cataracts.

VOL. 95, NO. 1 VITRECTOMY FOR VITREOUS HEMORRHAGE 21
Reoperations were performed in 57 eyes (23%), a rate higher than the 17% reported in another series.8 In our series, 28 eyes (11%) had later retinal reattach-ment surgery, and 14 eyes (6%) underwent lavage of persistent vitreous hemorrhage. Retinal reattachment operations were performed more frequently in our series than in some others, in which there was a 3% to 4% rate of retinal surgery during the first six postoperative months.8·9
Corneal opacities were present in 30 eyes (12%), 14 of which had glaucoma or phthisis bulbi. This was similar to the 7% rate of postoperative corneal opacities found by Peyman and associates.7
Only 62 eyes (25%) still had lenses at the final examinations, although the percentage increased in the latter part of the series. No eye had a severe cataract, although four eyes (2%) underwent secondary lens removal for cataract. Thirty-one eyes had mild to moderate catarac-tous changes at the final examinations and 33 (13%) had some residual vitreous hemorrhage. The vitreous hemorrhage was mild to moderate in 16 eyes and severe in 17 eyes.
The best time for vitreous surgery in diabetic eyes with vitreous hemorrhage is unknown.12 Acute vitreous hemorrhage often clears up during the first six to 12 months, but thereafter the likelihood of resolution is less than 10%.12 Prompt surgery is recommended if there is ultrason-ographic evidence of retinal detachment involving the macula. If the vitreous hemorrhage does not clear up within six months, vitrectomy can be considered, especially if vision is poor in the other eye. The risks of vitreous surgery are substantial, however, and severe surgical and postoperative complications can cause the operation to fail or require additional surgery or laser treatment.
Therefore, vitrectomy is usually reserved for eyes in which dense vitreous hemorrhage remains for more than six months or in which there is ultrasonographic evidence of retinal detachment involving the macula. The effect of earlier vitrectomy on eyes with vitreous hemorrhage is being examined in a prospective randomized clinical trial.12
REFERENCES 1. Rice, T. A., Michels, R. G., Maguire, M. G.,
and Rice, E. F.: The effect of lensectomy on the incidence of iris neovascularization and neovascular glaucoma after vitrectomy for diabetic retinopathy. Am. J. Ophthalmol. 95:1, 1983.
2. Michels, R. G.: Vitrectomy for complications of diabetic retinopathy. Arch. Ophthalmol. 96:237, 1978.
3. : Vitreous Surgery. St. Louis, C. V. Mosby Co., 1981, pp. 215-227.
4. : Proliferative diabetic retinopathy. Pathophysiology of extraretinal complications and principles of vitreous surgery. Retina 1:1, 1981.
5. Blankenship, G. W.: Stability of pars plana vitrectomy results for diabetic retinopathy complications. A comparison of five-year and six-month post-vitrectomy findings. Arch. Ophthalmol. 99:1009, 1981.
6. Rice, T. A., and Michels, R. G.: Long-term anatomic and functional results of vitrectomy for diabetic retinopathy. Am. J. Ophthalmol. 90:297, 1980.
7. Peyman, G. A., Huamonte, F. U., Goldberg, M. F., Sanders, D. R., Nagpal, K. L.; and Raichand, M. : Four hundred consecutive pars plana vitrectomies with the vitrophage. Arch. Ophthalmol. 96:45, 1978.
8. Blankenship, G. : Pars plana vitrectomy for diabetic retinopathy. A report of eight years' experience. Mod. Probi. Ophthalmol. 20:376, 1979.
9. Machemer, R., and Blankenship, G.: Vitrectomy for proliferative diabetic retinopathy associated with vitreous hemorrhage. Ophthalmology 88:643, 1981.
10. Blankenship, G.: Preoperative iris rubeosis and diabetic vitrectomy results. Ophthalmology 87:176, 1980.
11. Blankenship, G., Cortez, R., and Machemer, R. : The lens and pars plana vitrectomy for diabetic retinopathy complications. Arch. Ophthalmol. 97:1263, 1979.
12. Kupfer, C : The Diabetic Retinopathy Vitrectomy Study, editorial. Am. J. Ophthalmol. 81:687, 1976.