Embed Size (px)
Citation preview
Vitreous Hemorrhage after Closed Vitrectomy for Proliferative Diabetic Retinopathy FELIPE I. TOLENTINO, MD,t,2,3 VICfORIO N. CAJITA, MD,t,2 THEODORE GANCA YCO, MD,l STEVEN SKATES, PhD4
Abstract: The authors reviewed the medical records of 191 patients (232 eyes) who underwent closed vitrectomy for complications of diabetic retinopathy to evaluate the clinical picture of postvitrectomy hemorrhage (PVH). One hundred thirty-nine eyes (59.9%) had at least one episode of PVH (average, 1.5 per eye) that was variable in onset, not associated with a known cause in four fifths, with no noted source in two thirds, and severe in three fourths of the cases. Using logistic regression statistical analyses, the factors significantly associated with decreased incidence of PVH include older age of patient (P = 0.0004), long duration of surgery (P = 0.0002), and poor preoperative vision (P = 0.05). Of the 139 eyes with PVH, 65 (47%) had spontaneous clearing in an average of 11.3 weeks, 53 (38%) required repeat surgery, and 21 (15%) were inoperable, lost to follow-up, or refused reoperation. Postvitrectomy hemorrhage did not significantly influence the final visual outcome. Ophthalmology 96: 1495-1500, 1989
Vitreous hemorrhage after vitrectomy for diabetic retinopathy remains a significant postoperative problem and occurs in 63 to 75% of reported series. 1
,2 Although the hemorrhage resorbs spontaneously in most cases, some patients require intervention for hemorrhages that did not resolve and other complications.2
-5 In this article, we re-
port a retrospective study of the factors that may be responsible for vitreous hemorrhage after vitrectomy for complications of proliferative diabetic retinopathy, evaluate the clinical course of the hemorrhage, and assess the conditions influencing final visual acuity.
Originally received: September 9, 1988. Revision accepted: April 27, 1989.
1 Eye Research Institute of Retina Foundation, Boston. 2 Department of Ophthalmology, Harvard Medical School, Boston. 3 Retina Associates, Boston. 4 Department of Medicine, Harvard Medical School, Boston.
Presented at the American Academy of Ophthalmology Annual Meeting, Las Vegas, October 1988.
Supported by the Emily Bashara·Hatem Ophthalmic Research Fund and the Ophthalmic Microsurgery Laboratory Fund (Dr. Tolentino).
Reprint requests to Felipe I. Tolentino, MD, Library, Eye Research Institute, 20 Staniford St, Boston, MA 02114.
PATIENTS AND METHODS
We reviewed the medical records of 207 diabetic patients who underwent closed vitrectomy by one of us (FIT) from January 1980 through December 1986. Eight cases each were excluded either because of follow-up of less than 6 months or because the patient had no retinopathy but was operated because of rhegmatogenous retinal detachment (RD) complicated with proliferative vitreoretinopathy (PVR). Table 1 summarizes the database of the study population from which the results of this article were derived. Table 2 lists the follow-up periods for the 232 eyes.
1495

OPHTHALMOLOGY • OCTOBER 1989 • VOLUME 96 • NUMBER 10
Table 1. Database of Study Population
Factor
Patients (n = 191) M F
Eyes (n = 232) 00 OS
Indication for surgery Nonresolving hemorrhage TRD/RRD
No. (%)
104 (54.4) 87 (45.6)
122 (52.6) 110 (47.4)
61 (26.3) 171 (73.7)
00 = right eye; OS = left eye; TRD/RRD = tractional retinal detachment with or without a rhegmatogenous component.
Table 2. Follow-up Periods after Closed Vitrectomy in 232 Eyes
No. of No. of Bleeders Nonbleeders
Mos (n = 139) (n = 93)
~6-<12 66 49 >12-<18 15 13 > 18-<24 14 5 ~24-<30 6 5 ~30-<36 7 2 ~36-<42 6 3 ~42-<48 4 2 ~48 21 14
SURGICAL PROCEDURE
Standard pars plana vitrectomy techniques6-
tO were used for nonresolving vitreous hemorrhage. They were combined with multiple ancillary procedures including elevation, segmentation, and delamination ofvitreoretinal membranes; hemostasis of bleeding membranes; intraoperative panretinal photocoagulation of fundus areas with inadequate laser treatment; laser or cryoretinopexy for all retinal breaks; scleral buckling for rhegmatogenous RD; and lensectomy for cataracts that obstructed adequate posterior segment visualization. Surgery lasted from 45 minutes to 6 hours (average, 2.6 hours).
The patients had routine postoperative fundus examinations daily for 2 to 5 days in the hospital. Postoperative check-ups were performed at 10 to 14 days, 4 weeks, 3 months, and then every 6 months after hospital discharge.
REVIEW OF EVALUATED DATA
The pre-, intra-, and postoperative factors likely to influence rebleeding and final vision were collected from the medical records for evaluation.
Preoperative data included age at the time of surgery; sex; laterality of the eye; age at onset, duration, and treatment of diabetes mellitus; cardiovascular, renal, and other systemic medical problems; diabetic retinopathy; concomitant ocular problems (e.g., rubeosis iridis, neovas-
1496
cular glaucoma, and cataract); previous ocular surgery (lens extraction and vitreoretinal surgery); lens status (phakia, aphakia, or pseudophakia); best-corrected visual acuity, indication for vitreoretinal surgery (nonresolving vitreous hemorrhage alone and tractional RD with or without rhegmatogenous component [TRD/RRD]); and age of vitreous hemorrhage, if present.
Intraoperative factors reviewed for analysis were endophotocoagulation, endodiathermy, elevation, dissection and segmentation or circumcision of vitreoretinal membranes, scleral buckling, lensectomy, vitreous injection, retinopexy with either diathermy or cryoprobe, complications, duration of surgery, and fundus appearance at completion of surgery.
Postoperative factors evaluated included excessive fibrin formation, occurrence of vitreous hemorrhage, postoperative complications (recurrent RD, rubeosis iridis, neovascular glaucoma, cataract, corneal decompensation, maculopathy, retinal and optic nerve atrophy, endophthalmitis), reoperation for operative and postoperative complications, aphakia, and final visual acuity.
In the eyes with postvitrectomy hemorrhage (PVH), the following data were recorded: number of episodes, possible cause, onset, source, severity, whether spontaneous clearing occurred or repeat surgery was done, types of surgical procedures, and outcome of surgery. Postoperative vitreous bleeding is defined as new bleeding as diagnosed by the surgeon (FIT) from the first postoperative day up to the last follow-up visit. When opacities were present in the anterior segment or inflammatory reaction in the media obscured the vitreous, diagnosis of rebleeding was based on ultrasonographic findings of increased echoes in the vitreous cavity on serial examination or on the appearance of bright red reflex in the vitreous on indirect ophthalmoscopy. The possible sources of bleeding (e.g., sclerotomy sites and retinal or disc neovascularization) were examined during the follow-up visits as long as the clarity of the media allowed.
In the eyes that required reoperation, inspection of the whole fundus was performed intraoperatively. A certain area of the fundus was considered the source of PVH when it contained clotted blood and oozed actively after intraoperative removal of the clot by aspiration with the vitrectomy probe or the flute needle. An area also was considered suspicious when residual traction membranes pulled on congested, actively proliferating, neovascular membranes on the retinal surface or the optic disc. The bleeding was considered mild if it was localized or if most retinal features were visible by ophthalmoscopy, moderate if the retinal vessels and optic disc were barely visible, and severe if no retinal details were seen.
STATISTICAL ANALYSES
All data were computerized. For the response variable, eyes were categorized into two groups (with and without PVH) and further classified as having poor or good final visual acuity. Poor final visual acuity was defined as counting fingers or worse at the last follow-up visit. Good final visual acuity was better than counting fingers. The
TOLENTINO et al • DIABETIC POSTVITRECTOMY HEMORRHAGE
Table 3. List of Explanatory Variables and Their Coding Used in the Logistic Regression Analysis
Explanatory Variables
Age First Second
OM onset First Second
OM duration First Second
Previous laser therapy History of cardiac disease Preoperative vision Rubeosis irides Neovascular glaucoma Air-gas injection Endolaser Lens extraction Membrane peeling Cryotherapy Penetrating diathermy Scleral buckling Surgical duration
Coding
Linear and quadratic Categorical (::;;30, ::;;40, ::;;50, ::;;65, >65)
Linear and quadratic Categorical (::;;10, ::;;20, ::;;40, >40)
Linear and quadratic Categorical (::;;15, ::;;20, ::;;25, >25) Present versus absent Present versus absent ::;;CF versus >CF Present versus absent Present versus absent Present versus absent Present versus absent Present versus absent Present versus absent Present versus absent Present versus absent Present versus absent Linear and quadratic
OM = diabetes mellitus; CF = counting fingers.
data initially were examined in a univariate manner. We used the chi-square test for analysis of discrete data and the unpaired t test for continuous data.
Since some explanatory factors are varying together, we performed a multivariate analysis to find the simplest model that explains the variability in PVH occurrence with the least number of variables. We used a stepwise logistic regression method. Table 3 shows all variables and their respective codings considered for analysis including variables found significant in the univariate analysis and those that the investigators thought may influence the outcome. At every step of the analysis, a logistic regression model was fitted, and the least significant variable was eliminated until the simplest model was derived.
RESULTS
The prevalence ofPVH was 139 (59.9%) of232 eyes. One hundred (71.9%) of 139 eyes had one episode of bleeding and 39 (28.1 %) had two or more episodes (range, 2-8 episodes per eye). There were 209 episodes of PVH in 139 eyes (average, 1.5 episodes per eye).
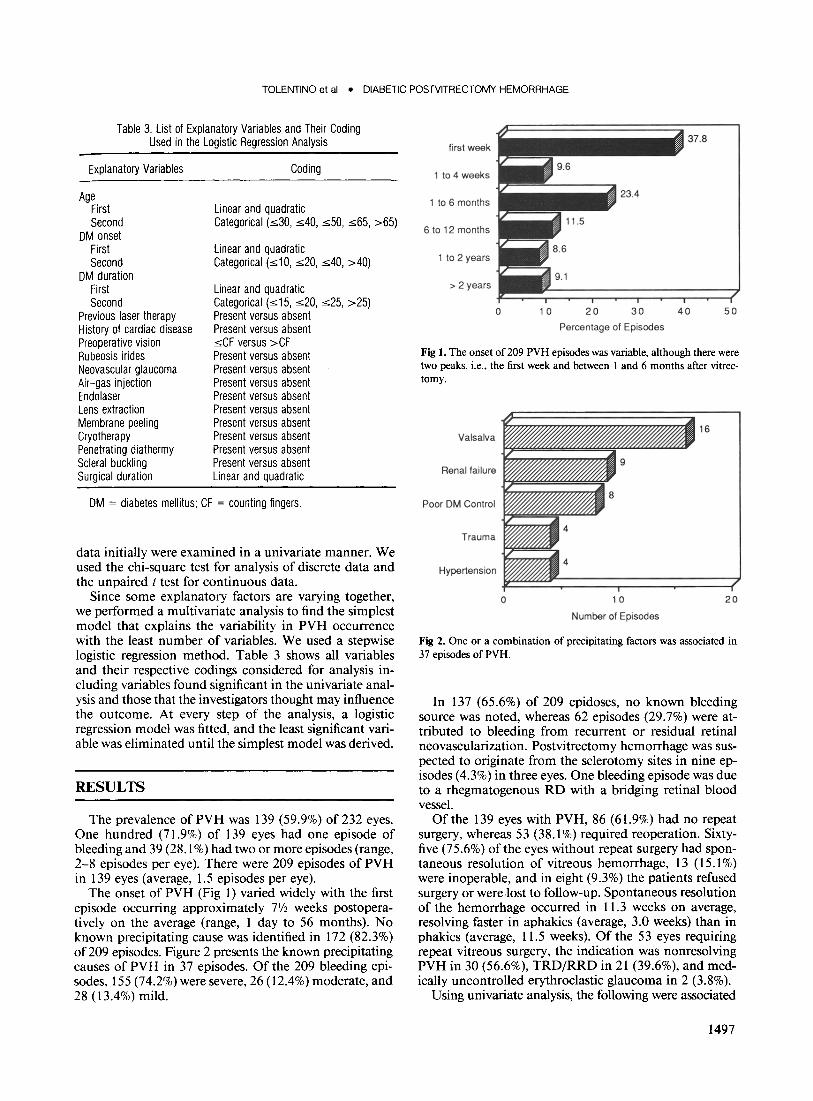
The onset of PVH (Fig 1) varied widely with the first episode occurring approximately 71f2 weeks postoperatively on the average (range, 1 day to 56 months). No known precipitating cause was identified in 172 (82.3%) of 209 episodes. Figure 2 presents the known precipitating causes of PVH in 37 episodes. Of the 209 bleeding episodes, 155 (74.2%) were severe, 26 (12.4%) moderate, and 28 (13.4%) mild.
37.8 first week
1 to 4 weeks
1 to 6 months
6 to 12 months
1 to 2 years
> 2 years
0 10 20 30 40 50
Percentage of Episodes
Fig 1. The onset of 209 PVH episodes was variable, although there were two peaks, i.e., the first week and between I and 6 months after vitrectomy.
16 Valsalva
Renal failure
Poor DM Control
Trauma
Hypertension ~~~~;:::===;:::==:::::;===~) o 10
Number of Episodes
20
Fig 2. One or a combination of precipitating factors was associated in 37 episodes of PVH.
In 137 (65.6%) of 209 epidoses, no known bleeding source was noted, whereas 62 episodes (29.7%) were attributed to bleeding from recurrent or residual retinal neovascularization. Postvitrectomy hemorrhage was suspected to originate from the sclerotomy sites in nine episodes (4.3%) in three eyes. One bleeding episode was due to a rhegmatogenous RD with a bridging retinal blood vessel.
Of the 139 eyes with PVH, 86 (61.9%) had no repeat surgery, whereas 53 (38.1 %) required reoperation. Sixtyfive (75.6%) of the eyes without repeat surgery had spontaneous resolution of vitreous hemorrhage, 13 (15.1%) were inoperable, and in eight (9.3%) the patients refused surgery or were lost to follow-up. Spontaneous resolution of the hemorrhage occurred in 11.3 weeks on average, resolving faster in aphakics (average, 3.0 weeks) than in phakics (average, 11.5 weeks). Of the 53 eyes requiring repeat vitreous surgery, the indication was nonresolving PVH in 30 (56.6%), TRD/RRD in 21 (39.6%), and medically uncontrolled erythroclastic glaucoma in 2 (3.8%).
Using univariate analysis, the following were associated
1497

OPHTHALMOLOGY • OCTOBER 1989 • VOLUME 96 • NUMBER 10
~ c----------------------------------------,
o ci L-____ -L ______ L-____ _L ______ L-____ ~ ____ ~
20 30 40 50 60 70 80
Age
Fig 3. Estimated probabilities of PVH as a function of age in patients with preoperative visual acuity of counting fingers or worse and a surgical duration of 2112 hours.
o ,----------------------------------------,
OJ ci
~ o L-____ _L ______ L-____ ~ ____ _J ______ ~ ____ ~
20 30 40 50
Age
60 70 80
Fig 4. Estimated probabilities of PVH as a function of age in patients with preoperative vision of better than counting fingers and a surgical duration of 2112 hours.
~ c----------------------------------------,
o ci ~ ______ ~ ______ ~ ______ _L ______ _L ______ ~
Surgical Duration
Fig 5. Estimated probabilities of PVH as a function of surgical duration in a 45-year-old patient with preoperative visual acuity of counting fingers or worse.
1498
~ c----------------------------------------,
., ci
'" .~ ci
i 0. ...
ci
o ci L-______ ~ ______ ~ ______ _L ______ _L ______ ~
Surgical Duration
Fig 6. Estimated probabilities of PVH as a function of surgical duration in a 45-year-old patient with preoperative visual acuity of better than counting fingers.
with increased prevalence of PVH: insulin therapy (P < 0.02) and previous laser photocoagulation (P < 0.05). The factors associated with decreased prevalence ofPVH were air-gas injection (P = 0.0001), longer duration of surgery (P < 0.0003), older age (P < 0.0004), scleral buckling (P = 0.001), later onset of diabetes mellitus (P < 0.002), history of cardiac disease (P = 0.006), and poor preoperative vision (P < 0.02).
Using multivariate analysis, the final logistic regression model found that three variables significantly correlated with decreased prevalence of PVH: longer duration of surgery (P = 0.0002), older age (P = 0.0004), and poor preoperative vision (P = 0.05). We interpret the coefficients of the effects estimated by the model as follows. Instead of directly estimating the effect on the probability of PVH occurring, the model examines the effect on the odds of PVH occurring, where odds = PI( 1 - P). For a baseline group with the following characteristics--age, 45 years; surgical duration, 21/2 hours; and preoperative vision, counting fingers or worse--the model estimates th~ odds of PVH occurring to be 3:2, or the probability to be 60%. Table 4 displays the multiplicative change in the odds of PVH occurring, corresponding to changes in any significant factors. For example, for a 55-year-old patient with a preoperative vision of counting fingers or worse and a surgical duration of 21f2 hours, the estimated odds of PVH occurring decreases by two thirds from the estimated odds of 3:2 in a 45-year-old patient with the other characteristics the same. This translates to estimated odds of 1: 1, or a probability of 50%. Similarly, for a 45-yearold patient with a surgical duration of 21/2 hours and preoperative vision of better than counting fingers, the odds ofPVH occurring are 2.3 times greater than for a similar patient with preoperative vision of counting fingers or worse.
Finally, Figures 3 to 6 give the estimated probabilities of PVH as both a function of age and surgical duration in the two groups: poor and good preoperative vision. The estimates are enclosed in 95% confidence bands. For
TOLENTINO et al • DIABETIC POSTVITRECTOMY HEMORRHAGE
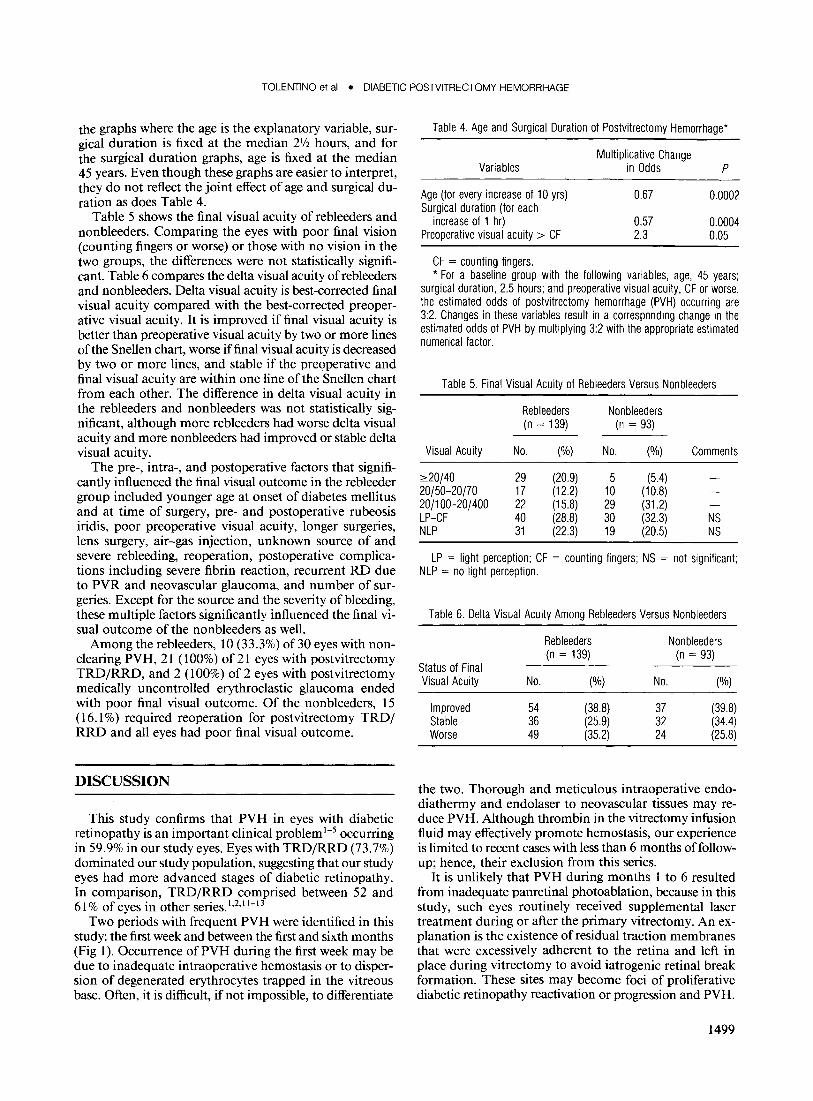
the graphs where the age is the explanatory variable, surgical duration is fixed at the median 21f2 hours, and for the surgical duration graphs, age is fixed at the median 45 years. Even though these graphs are easier to interpret, they do not reflect the joint effect of age and surgical duration as does Table 4.
Table 5 shows the final visual acuity of rebleeders and nonbleeders. Comparing the eyes with poor final vision (counting fingers or worse) or those with no vision in the two groups, the differences were not statistically significant. Table 6 compares the delta visual acuity of rebleeders and nonbleeders. Delta visual acuity is best-corrected final visual acuity compared with the best-corrected preoperative visual acuity. It is improved if final visual acuity is better than preoperative visual acuity by two or more lines of the Snellen chart, worse if final visual acuity is decreased by two or more lines, and stable if the preoperative and final visual acuity are within one line of the Snellen chart from each other. The difference in delta visual acuity in the rebleeders and nonbleeders was not statistically significant, although more rebleeders had worse delta visual acuity and more nonbleeders had improved or stable delta visual acuity.
The pre-, intra-, and postoperative factors that significantly influenced the final visual outcome in the rebleeder group included younger age at onset of diabetes mellitus and at time of surgery, pre- and postoperative rubeosis iridis, poor preoperative visual acuity, longer surgeries, lens surgery, air-gas injection, unknown source of and severe rebleeding, reoperation, postoperative complications including severe fibrin reaction, recurrent RD due to PVR and neovascular glaucoma, and number of surgeries. Except for the source and the severity of bleeding, these multiple factors significantly influenced the final visual outcome of the nonbleeders as well.
Among the rebleeders, 10 (33.3%) of30 eyes with nonclearing PVH, 21 (100%) of 21 eyes with postvitrectomy TRD/RRD, and 2 (100%) of 2 eyes with postvitrectomy medically uncontrolled erythroclastic glaucoma ended with poor final visual outcome. Of the nonbleeders, 15 (16.1 %) required reoperation for postvitrectomy TRD/ RRD and all eyes had poor final visual outcome.
DISCUSSION
This study confirms that PVH in eyes with diabetic retinopathy is an important clinical problem 1-5 occurring in 59.9% in our study eyes. Eyes with TRD/RRD (73.7%) dominated our study population, suggesting that our study eyes had more advanced stages of diabetic retinopathy. In comparison, TRD/RRD comprised between 52 and 61 % of eyes in other series. 1,2,1 1-13
Two periods with frequent PVH were identified in this study: the first week and between the first and sixth months (Fig 1). Occurrence of PVH during the first week may be due to inadequate intraoperative hemostasis or to dispersion of degenerated erythrocytes trapped in the vitreous base. Often, it is difficult, if not impossible, to differentiate
Table 4. Age and Surgical Duration of Postvitrectomy Hemorrhage*
Variables
Age (for every increase of 10 yrs) Surgical duration (for each
increase of 1 hr) Preoperative visual acuity> CF
CF = counting fingers.
Multiplicative Change in Odds P
0.67 0.0002
0.57 0.0004 2.3 0.05
* For a baseline group with the following variables, age, 45 years; surgical duration, 2.5 hours; and preoperative visual acuity, CF or worse, the estimated odds of postvitrectomy hemorrhage (PVH) occurring are 3:2. Changes in these variables result in a corresponding change in the estimated odds of PVH by multiplying 3:2 with the appropriate estimated numerical factor.
Table 5. Final Visual Acuity of Rebleeders Versus Nonbleeders
Rebleeders (n = 139)
Visual Acuity No. (%)
~20/40 29 (20.9) 20/50-20/70 17 (12.2) 20/100-20/400 22 (15.8) LP-CF 40 (28.8) NLP 31 (22.3)
Nonbleeders (n = 93)
No. (%)
5 (5.4) 10 (10.8) 29 (31.2) 30 (32.3) 19 (20.5)
Comments
NS NS
LP = light perception; CF = counting fingers; NS = not Significant; NLP = no light perception.
Table 6. Delta Visual Acuity Among Rebleeders Versus Nonbleeders
Rebleeders Nonbleeders (n = 139) (n = 93)
Status of Final Visual Acuity No. (%) No. (%)
Improved 54 (38.8) 37 (39.8) Stable 36 (25.9) 32 (34.4) Worse 49 (35.2) 24 (25.8)
the two. Thorough and meticulous intraoperative endodiathermy and endolaser to neovascular tissues may reduce PVH. Although thrombin in the vitrectomy infusion fluid may effectively promote hemostasis, our experience is limited to recent cases with less than 6 months offollowup; hence, their exclusion from this series.
It is unlikely that PVH during months 1 to 6 resulted from inadequate panretinal photoablation, because in this study, such eyes routinely received supplemental laser treatment during or after the primary vitrectomy. An explanation is the existence of residual traction membranes that were excessively adherent to the retina and left in place during vitrectomy to avoid iatrogenic retinal break formation. These sites may become foci of proliferative diabetic retinopathy reactivation or progression and PVH.
1499

OPHTHALMOLOGY • OCTOBER 1989 • VOLUME 96 • NUMBER 10
The logistic regression model estimated the effects of three important predictors ofPVH. To quantify these effects, the model estimates the change in odds over a baseline group for changes in the explanatory variables. These effects are estimated jointly. This is an important improvement over univariate analysis, because we can conclude that if two variables change, their corresponding effects jointly multiply the odds of hemorrhaging. With univariate analysis, we do not know if the changes in the explanatory variables should jointly affect the odds or whether the two variables are highly correlated, change together, and hence, only singly contribute to the change in odds.
The fact that the three explanatory variables (i.e., age, surgical duration, and preoperative vision) were declared significant by this model means that they were the strongest joint predictors of outcome, and that after accounting for these factors, there was little explanatory power left in the other predictors. It is important to realize, however, that other variables, such as diabetes mellitus onset, are highly correlated with age. The logistic regression analysis also will provide almost as good a prediction model if any of these alternative variables could be chosen. Because they are highly correlated, they measure the same underlying quantity.
The beneficial effect of long surgical duration on PVH is puzzling. It may reflect thorough surgery including meticulous membrane dissection, better hemostasis, scleral buckling that relieves traction on the peripheral retina, supplemental panretinal photoablation, and gas injection. Increasing risk ofPVH with decreasing age and early onset of diabetes mellitus are usually associated with the active phase of diabetic retinopathy. Increased risk of PVH with insulin therapy and history of previous laser treatment appears contradictory. However, these factors may be consistent with increased risk because they are inherent in patients with severe diabetic retinal disease who are unresponsive to treatment and in whom progressive proliferative diabetic retinopathy developed. Decreased risk of PVH in eyes with poor preoperative vision indicates "burned-out" or atrophic retinas, which are less likely to bleed.
In this study, PVH did not significantly affect the final and delta visual acuities, confirming the findings of other investigators l3
-17 that visual failure in diabetic eyes that
underwent vitrectomy is caused by multiple factors associated with severe diabetic ocular disease. Because PVH usually resolves spontaneously and reoperation may be associated with increased morbidity, we recommend watchful waiting unless the following are present: (1) recurrent vitreous hemorrhage persisting for 4 months, (2) florid rubeosis iridis, (3) ultrasonographic evidence of new RD, (4) erythroclastic glaucoma unresponsive to medical
1500
management, and (5) PVH in the only seeing eye. Recurrent PVH suggests active proliferative diabetic retinopathy that may require supplemental panretinal photoablation or endodiathermy. Eyes with florid rubeosis may require additional peripheral retinal laser ablation. Rhegmatogenous RD increases the risk of neovascular glaucoma and requires reattachment surgery. Finally, to shorten visual disability, we believe that reoperation is justified in an only seeing eye with dense PVH with no sings of spontaneous resolution after 2 months of observation.
REFERENCES
1. Novak MA, Rice TA. Michels RG. Auer C. Vitreous hemorrhage after vitrectomy for diabetic retinopathy. Ophthalmology 1984; 91: 1485-9.
2. Schachat AP. Oyakawa RT. Michels RG. Rice TA. Complications of vitreous surgery for diabetic retinopathy II. Postoperative complications. Ophthalmology 1983; 90:522-30.
3. Rice TA. Michels RG. Rice EF. Vitrectomy for diabetic rhegmatogenous retinal detachment. Am J Ophthalmol 1983; 95:34-44.
4. Blankenship GW. Management of vitreous cavity hemorrhage following pars plana vitrectomy for diabetic retinopathy. Ophthalmology 1986; 93:39-44.
5. Tolentino Fl. Freeman HM. Tolentino FL. Closed vitrectomy in the management of diabetic traction retinal detachment. Ophthalmology 1980; 87:1078-89.
6. Machemer R. Aaberg TM. Vitrectomy. 2nd ed. New York: Grune & Stratton. 1979; 41-144.
7. Michels RG. Vitreous Surgery. 2nd ed. St. Louis: CV Mosby. 1981; 135-200.
8. Peyman GA. Schulman JA. Intravitreal Surgery: Principles and Practice. East Norwalk: Appleton & Lange. 1986; 163-84.
9. Charles S. Vitreous Microsurgery. 2nd ed. Baltimore: Williams & Wilkins. 1987; 55-133.
10. Freeman HM. Tolentino FI. Atlas of Vitreoretinal Surgery. Vol. III. New York: Thieme Medical Publishers (in press).
11. Oyakawa RT. Schachat AP. Michels RG. Rice TA. Complications of vitreous surgery for diabetic retinopathy. I. Intraoperative Complications. Ophthalmology 1983; 90:517-21.
12. Thompson JT. de Bustros S. Michels RG. et al. Resultes of vitrectomy for proliferative diabetic retinopathy. Ophthalmology 1986; 93: 1571-4.
13. Thompson JT. Auer CL. de Bustros S. et al. Prognostic indicators of success and failure in vitrectomy for diabetic retinopathy. Ophthalmology 1986; 93:290-5.
14. Michels RG. Rice TA. Rice EF. Vitrectomy for diabetic vitreous hemorrhage. Am J Ophthalmol 1983; 95: 12-21.
15. Rice TA. Michels RG. Rice EF. Vitrectomy for diabetic traction retinal detachment involving the macula. Am J Ophthalmol1983; 95:22-33.
16. Blankenship G. Preoperative iris rubeosis and diabetic vitrectomy results. Ophthalmology 1980; 87:176-82.
17. Aaberg TM. Abrams Gw. Changing indications and techniques for vitrectomy in management of complications of diabetic retinopathy. Ophthalmology 1987; 94:775-9.