Embed Size (px)
Citation preview

Ocular Immunology and Inflammation, 15:19–25, 2007Copyright ©c Informa HealthcareISSN: 0927-3948 print; 1744-5078 onlineDOI: 10.1080/09273940601147737
ORIGINAL ARTICLE
Vitreous Hemorrhage in MultipleSclerosis-Associated Uveitis
Natasa Vidovic Valentincic,Aleksandra Kraut,and Aniki RothovaUniversity Medical Centre,Department of Ophthalmology,Ljubljana, Slovenia
ABSTRACT Purpose: To report on six patients who developed vitreous hemor-rhage (VH) in the course of intermediate uveitis (IU) associated with multiplesclerosis (MS). Methods: Observational case series. Results: Six out of 25 patients(24%) with IU and MS seen at two tertiary centers developed VH. Average ageat onset of MS was 26 years and average age at the onset of IU was 25 years. IUdeveloped before the onset of MS in four of the six patients (67%). All patientshad IU associated with peripheral phlebitis. The average interval between theonset of IU and the occurrence of VH was five years (range: 0–11 years; VHwas the initial sign of uveitis in 2 patients). VH cleared spontaneously in allcases; however, subsequent retinal detachment developed in two eyes. All sixpatients had ischemic retinal areas and four had subretinal neovascularizations.Optimal visual acuity five years after VH varied from no light perception to fullvisual acuity. The causes of diminished acuity included optic neuritis, cystoidmacular edema (CME), and retinal detachment. Conclusion: The possibility ofMS-associated uveitis should be considered in patients with IU and VH.
KEYWORDS Multiple sclerosis; uveitis; vitreous hemorrhage
INTRODUCTIONMultiple sclerosis (MS) is an inflammatory disorder of the central nervous
system white matter and a common cause of neurological disability in youngadults.1 The origin of MS is unknown and probably represents a combination ofyet unknown environmental factors and susceptibility genes. The disease courseis mostly characterized by recurrent attacks followed by recovery; sometimes,however, the attacks leave permanent deficits.
Ocular manifestations of MS are numerous and include typically diverseneuro-ophthalmologic disorders, especially optic neuritis. The latter may re-sult not only in optic atrophy, but also in intermediate uveitis (IU), peripheralretinal phlebitis, and occasional cases of anterior uveitis and panuveitis; reti-nal vasculitis has been noted in 10–35% of the patients with MS.2−4 Uveitis,most commonly IU (including pars planitis and retinal periphlebitis), was found
Accepted 30 November 2006.
Correspondence and reprint requeststo: N. Vidovic Valentincic, UniversityMedical Centre, Department ofOphthalmology, Ljubljana, Slovenia;e-mail: [email protected]
19
Ocu
l Im
mun
ol I
nfla
mm
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
10/3
0/14
For
pers
onal
use
onl
y.

to precede the neurological symptoms of MS in 25–46% of the patients.5,6 The development of vitreoushemorrhage (VH) has rarely been reported.7−11 Herein,we report on six patients with VH occurring during IUassociated with MS.
METHODSPatients were selected from the databases of two ter-
tiary ophthalmologic centers (Ljubljana, Slovenia, andUtrecht, the Netherlands). Twenty-five patients had MSand IU. Six of the 25 also developed VH and were in-cluded in the study. These six had MS proven by dis-seminated plaques of demyelinization on magnetic res-onance imaging (MRI) along with oliogoclonal bandsof proteins in cerebrospinal fluid.1 All patients under-went screening for IU (detailed medical history, erythro-cyte sedimentation rate, complete blood counts, serumangiotensin-converting enzyme levels, syphilis and Bor-relia serology, chest radiography, and Mantoux testing)and the results were within the normal limits.
CASE REPORTSCase 1
A 21-year-old female developed IU, which was symp-tomatically treated. Since she suffered from recurrent
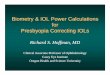
FIGURE 1 Fluorescein angiography: multiple arterial occlusions and neovascularizations.
bilateral VHs, multiple arterial occlusions, and occlu-sive phlebitis, the patient was referred for further analy-sis. She had unexplained neurological complaints thathad been present for the past eight years. The evalua-tion by the neurologist disclosed the diagnosis of MS.Fluorescein angiography documented multiple arterialocclusions and the development of multiple neovascu-larizations (Fig. 1). CME and ischemic macular areaswere also noted. The patient was treated with perioc-ular and systemic corticosteroids and laser coagulationof affected areas. Her visual acuity (VA) remained 20/80due to macular abnormalities.
Case 2A 33-year-old female developed optic neuritis in her
right eye (RE) and was diagnosed with MS. Seven yearslater, VH occurred, which spontaneously cleared. Onfluorescein angiography, phlebitis, ischemic areas, andmultiple neovascularizations were noted in both eyes.The patient was treated with panretinal laser coagula-tion and her VA stabilized at 20/30 (Fig. 2).
Case 3A seven-year-old girl with a history of amblyopia in
her RE was referred with IU in both eyes. Examination
N. V. Valentincic et al. 20
Ocu
l Im
mun
ol I
nfla
mm
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
10/3
0/14
For
pers
onal
use
onl
y.

FIGURE 2 Fluorescein angiography: phlebitis, ischemic areas, and multiple neovascularizations. Treatment with panretinal lasercoagulation.
revealed a best-corrected vision of 20/200 RE and 20/20LE; there were no abnormalities except bilateral vitritis.The patient was treated with periocular steroid injec-tions; later, systemic methotrexate and cyclosporin wereadded. The inflammation persisted and her RE devel-oped phthisis due to tractional retinal detachment. Thelow-grade activity in her left eye persisted over time andVH occurred, which spontaneously cleared. On fluores-cein angiography, focal areas of vasculitis were observedas well as cystoid macular edema. At present, her VA is20/40 with ongoing low-grade vitritis. Eleven years afterthe onset of IU, at the age of 18 years, the patient wasdiagnosed with MS.
Case 4A 28-year-old female was referred for analysis of her
IU. She was treated with periocular steroid injections atthe times of active uveitis and her VA remained 20/20.Four years later, she was diagnosed with MS and threeyears after that diagnosis, she suffered from acute lossof VA in her RE because of VH. Her VA spontaneouslyrecovered; however, a large retinoschisis was noted. Flu-orescein angiography revealed bilateral staining of pe-ripheral vessels and capillary non-perfusion. At the age
of 36, she gave birth to a healthy child; however, newdemyelization plaques developed in the months follow-ing the delivery along with a decline in her neurologicalfunctions.
Case 5A 20-year-old female developed IU. The patient’s
sister was previously diagnosed with MS. The patienthad regular recurrences of IU characterized by vitritisand snowbanking and was treated with periocular in-jections and later with systemic steroids, cyclosporine,and peripheral cryocoagulation. Although she had noneurological complaints at the onset of IU, three yearslater she was diagnosed with MS. Eleven years after theonset of IU, VH developed in her LE, which sponta-neously cleared. Fluorescein angiography showed pe-ripheral phlebitis in both eyes with cystoid macularedema and avascular areas with neovascularization adja-cent to scars of previous cryocoagulation (Fig. 3). Lasercoagulation of ischemic retinal areas was performed.Thirteen years after the onset of IU, optic neuritis de-veloped in both eyes. The patient developed cataracts,which were removed. Twenty years after the onsetof IU, the inflammation subsided and treatment was
21 Vitreous Hemorrhage in MS-Associated Uveitis
Ocu
l Im
mun
ol I
nfla
mm
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
10/3
0/14
For
pers
onal
use
onl
y.

FIGURE 3 Fluorescein angiography: peripheral phlebitis and avascular areas with neovascularization adjacent to scars of previouscryocoagulation.
stopped. VA at that time was 20/25 RE and 20/30 LE,respectively.
Case 6An 18-year-old male patient was diagnosed with MS
and 13 years later with IU, which was initially treatedwith local medications and subsequently with systemicsteroids and cyclosporin. VH occurred in the RE fiveyears after the onset of IU. The patient underwent parsplana vitrectomy; however, VA in the RE remained lim-ited to hand movements. At that time, exacerbation ofIU in the LE was complicated by central retinal vein oc-clusion (CRVO) and, in consequence, the left eye hadoptimal VA limited to 20/100. Five years later, a secondhemorrhage in the RE followed and was complicatedby retinal detachment. Despite surgical treatment, hisVA worsened to no light perception. In the next years,retinal hemorrhages in the LE and vitritis occurred reg-ularly and were treated with steroids. The patient un-derwent cataract surgery and gained a postoperative VAof 20/80 due to macular edema. Twenty-two years afterthe onset of IU, the inflammation decreased. The pa-tient has been free of medications for the past five yearsand has stable VA.
RESULTSAs noted above, six of the 25 patients (24%) with IU
and MS seen at the two tertiary centers developed VH(4/14 [29%] in Utrecht and 2/11 [18%] in Ljubljana).The general characteristics of the patients are given inTable 1.
IU developed before the onset of MS in four of thesix patients (67%). VH was bilateral in two patients andone patient developed CRVO in the fellow eye. All pa-tients had IU associated with peripheral phlebitis andischemic retinal areas and four had subretinal neovas-cularizations, three of them multiple. Two eyes devel-oped retinal detachment. Although VH spontaneouslycleared in all patients, optimal VA thereafter varied fromno light perception to full VA. The causes of dimin-ished acuity included optic neuritis, CME, and retinaldetachment.
DISCUSSIONWe report on six patients with VH occurring in the
course of MS-associated IU. IU and peripheral retinalphlebitis have been repeatedly reported as common oc-ular manifestations of MS.5,6,12 The classification ofperipheral phlebitis in MS, however, has been confus-ing: usually, phlebitis is considered a form of IU, but
N. V. Valentincic et al. 22
Ocu
l Im
mun
ol I
nfla
mm
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
10/3
0/14
For
pers
onal
use
onl
y.

TAB
LE1
Ch
ara
cte
ris
tic
so
fp
ati
en
tsw
ith
mu
ltip
les
cle
ros
isa
nd
as
so
cia
ted
inte
rme
dia
teu
ve
itis
an
dv
itre
ou
sh
em
orr
hag
e
Ag
eat
on
set
of
Ag
eat
on
set
of
Uve
itis
Inte
rval
bet
wee
nIU
Ag
eat
on
set
Eyes
wit
hV
isu
alac
uit
yo
faf
fect
edV
isu
alac
uit
yo
faf
fect
edN
o.
Gen
der
MS
(yea
rs)
IU(y
ears
)fe
atu
res
and
VH
(yea
rs)
of
VH
VH
Neo
vasc
ula
riza
tio
ney
es1
year
afte
rV
Hey
es5
year
saf
ter
VH
1F
3121
Vit
riti
sp
hle
bit
is0
212
Yes
20/2
5;20
/60
20/8
0;20
/80
2F
3340
Vit
riti
sp
hle
bit
is0
402
Yes
20/3
0;20
/30
20/3
0;20
/30
3F
187
Vit
riti
sp
hle
bit
is7
141
No
20/4
020
/40
4F
3228
Vit
riti
sp
hle
bit
is7
351
No
20/2
0N
ot
yet
kno
wn
5F
2320
Vit
riti
sp
hle
bit
is11
311
Yes
20/6
020
/40
6M
1831
Vit
riti
sp
hle
bit
is5
361∗
Yes
Han
dm
ove
men
ts;
No
ligh
tp
erce
pti
on
;20
/100
20/8
0
MS,
mul
tiple
scle
rosi
s;IU
,int
erm
edia
teuv
eitis
;VH
,vitr
eous
hem
orrh
age.
∗ Sec
ond
eye
ofth
epa
tient
deve
lope
dce
ntra
lret
inal
vein
occl
usio
n.
23
Ocu
l Im
mun
ol I
nfla
mm
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
10/3
0/14
For
pers
onal
use
onl
y.

sometimes it is assumed to represent a specific disorderdistinct from IU. According to the new Standardiza-tion of Uveitis Nomenclature,13 IU is a subset of uveitiswhere the vitreous is the major site of the inflammation.One of the associated features in IU might be the pres-ence of peripheral vascular sheathing and, therefore, weconsider peripheral retinal vasculitis a characteristic ofIU. All of our patients had IU with vitritis and associ-ated phlebitis.
VH was observed in 8–14% of the patients withIU14,15 and Malinowski and colleagues noted the de-velopment of retinal neovascularization with or with-out associated VH in 6.5% of patients with IU.4 Personswith VH and IU were significantly younger than IU pa-tients without VH (prevalence of VH in children withIU was 28% compared to 6% in adults with IU).15 Thefrequency of 24% found in the present series is higherthan might be expected in adults with IU. Althoughthe number of patients in our series is very limited, itcannot be excluded that VH is more common in MS-associated IU than in other types of IU.
Few reports on VH in MS-associated IU have beenpublished.9−12 In these previously described cases ofVH in IU with MS, the causes of VH were attributedeither to vitreous traction or to retinal ischemia withsubsequent neovascularization.7−12,16 Hochwarter andcolleagues presented three MS patients with vitreoreti-nal traction syndrome.7 In addition to isolated casereports,9−12 Towler reported on eight eyes with oc-clusive retinal vasculitis, ischemia, and neovasculariza-tion in MS.16 All of our patients had retinal ischemiaand four had neovascularizations on angiography. Inone patient, peripheral retinoschisis was present whichmight have been associated with both ischemia andtraction.
Eales’ disease is an idiopathic condition that man-ifests with recurrent VH due to obliterative reti-nal perivasculitis and is sometimes accompanied byneovascularization.17 An association between Eales’disease and diverse neurological disorders has been re-peatedly noted.18−20 In some cases, the neurologicalsymptoms specifically suggested MS.19 It might be pos-sible that a similar association was present in these pa-tients as in our series. The possibility of MS should beconsidered in patients with Eales’ disease, specificallyin patients with neurological problems.
In general, VH in uveitis develops as a consequenceof occlusive vasculitis in the retina. Therefore, the dif-ferential diagnosis of VH in uveitis includes, in addition
to idiopathic vasculitis, mainly sarcoidosis and Behcet’sdisease because retinal ischemia and/or neovasculariza-tions regularly develop in these patients.21−25 Four per-cent of the patients with posterior segment involvementin sarcoidosis had VH. This percentage increased to16% among the young patients with sarcoidosis andposterior segment involvement.26 A generalized hyper-coagulable state with endothelial cell activation is typ-ical of Behcet’s disease and the occlusive retinal vas-culitis is a feature which can be followed by vitreoushemorrhage or tractional retinal detachment.27 In addi-tion, VH developed in one patient with Lyme diseaseand retinal vasculitis.28
In conclusion, VH may complicate the course ofMS-associated IU. Moreover, the possibility of MS-associated uveitis should be considered in IU patientswith VH.
REFERENCES[1] Compston A, Coles A. Multiple sclerosis. Lancet. 2002;359:1221–
1231.[2] Engell T, Andersen PK. The frequency of periphlebitis in multiple
sclerosis. Acta Neurol Scand. 1982;65:601–608.[3] Graham EM, Francis DA, Sanders MD, et al. Ocular inflammatory
changes in established multiple sclerosis. J Neurol Neurosurg Psy-chiatry. 1989;52:1360–1363.
[4] Malinowski SM, Pulido JS, Folk JC. Long-term visual outcomeand complications associated with pars planitis. Ophthalmology.1993;100:818–825.
[5] Zein G, Berta A, Foster CS. Multiple sclerosis-associated uveitis. OculImmunol Inflamm. 2004;12:137–142.
[6] Biousse V, Trichet C, Bloch-Michel E, et al. Multiple sclerosis as-sociated with uveitis in two large clinic-based series. Neurology.1999;52:179–181.
[7] Hochwarter A, Prainer C, Binder S, et al. Vitreoretinal traction syn-drome in multiple sclerosis. Ophthalmologe. 2004;101:153–157.
[8] Patte M, Rouher FN, Vernay D, et al. Proliferative retinal vasculitis andmultiple sclerosis: a case report. J Fr Ophtalmol. 2003;26:381–385.
[9] Ronzani M, Lang GE, Wagner P, et al. Severe occlusive retinal pe-riphlebitis with vitreous hemorrhage in multiple sclerosis. Ger J Oph-thalmol. 1995;4:328–331.
[10] Guigui A, Brezin A, Gaudric A, et al. Vitreous hemorrhage and neo-vascular proliferation in multiple sclerosis. Bull Soc Ophtalmol Fr.1989;89:501–505.
[11] Katsimpris JM, Petropoulos JK, Pharmakakis NM. Bilateral peripheralretinal neovascularization in a patient with multiple sclerosis. J FrOphtalmol. 2002;25:813–816.
[12] Vine AK. Severe periphlebitis, peripheral retinal ischemia, and pre-retinal neovascularization in patients with multiple sclerosis. Am JOphthalmol. 1992;113:28–32.
[13] Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of UveitisNomenclature SUN) Working Group. Standardization of uveitisnomenclature for reporting clinical data. Results of the First Interna-tional Workshop. Am J Ophthalmol. 2005;140:509–516.
[14] Deane JS, Rosenthal AR. Course and complications of intermediateuveitis. Acta Ophthalmol Scand. 1997;75:82–84.
[15] Lauer AK, Smith JR, Robertson JE, et al. Vitreous hemorrhage isa common complication of pediatric pars planitis. Ophthalmology.2002;109:95–98.
N. V. Valentincic et al. 24
Ocu
l Im
mun
ol I
nfla
mm
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
10/3
0/14
For
pers
onal
use
onl
y.

[16] Towler HM, Lightman S. Symptomatic intraocular inflammation inmultiple sclerosis. Clin Exp Ophthalmol. 2000;28:97–102.
[17] Biswas J, Sharma T, Gopal L, et al. Eales disease—an update. SurvOphthalmol. 2002;47:197–214.
[18] Singhal BS, Dastur DK. Eales’ disease with neurologic involvement.Part I. Clinical features in 9 patients. J Neurol Sci. 1976;27:313–321.
[19] Rodier G, Derouiche F, Bronner P, et al. Eales disease with neurologicmanifestation: differential diagnosis of multiple sclerosis. Report oftwo cases. Presse Med. 1999;28:1692–1694.
[20] Katz B, Wheeler D, Weinreb RN, et al. Eales’ disease with centralnervous system infarction. Ann Ophthalmol. 1991;23:460–463.
[21] Girmens JF, Fajnkuchen F, Badelon I, Chaine G. Peripheral retinalneovascularization and sarcoidosis: two case reports. J Fr Ophtalmol.2002;25:303–307.
[22] Steahly LP. Sarcoidosis and peripheral neovascularization. Ann Oph-thalmol. 1988;20:426–427, 430.
[23] Hirose S, Ohno S. Argon laser treatment of retinal neovasculariza-tion associated with sarcoidosis. Jpn J Ophthalmol. 1984;28:356–361.
[24] Nakamura T, Takahashi K, Kishi S. Optic nerve involvement in neuro-Behcet’s disease. Jpn J Ophthalmol. 2002;46:100–102.
[25] Graham EM, Stanford MR, Shilling JS, Sanders MD. Neovas-cularisation associated with posterior uveitis. Br J Ophthalmol.1987;71:826–833.
[26] Khalatbari D, Stinnett S, McCallum RM, Jaffe GJ. Demographic-related variations in posterior segment ocular sarcoidosis. Ophthal-mology. 2004;111:357–362.
[27] Evereklioglu C. Current concepts in the etiology and treatment ofBehcet disease. Surv Ophthalmol. 2005;50(4):297–350.
[28] Leys AM, Schonherr U, Lang GE, Naumann GO, Goubau P, HonoreA, Valvekens F. Retinal vasculitis in Lyme borreliosis. Bull Soc BelgeOphtalmol. 1995;259:205–214.
25 Vitreous Hemorrhage in MS-Associated Uveitis
Ocu
l Im
mun
ol I
nfla
mm
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
elbo
urne
on
10/3
0/14
For
pers
onal
use
onl
y.
























![Why worry about strabismus? [1,8] Vitreous Hemorrhage (dark reflex) Hypopyon (layering of WBCs in anterior chamber)](https://img.pdfslide.net/doc/110x75/5697bfc21a28abf838ca5133/why-worry-about-strabismus-18-vitreous-hemorrhage-dark-reflex-hypopyon.jpg)



