Embed Size (px)
Citation preview

VN057 Gerontology 10Ch 17 cont’d; 18


Dental Caries
Tooth decay, loose teeth, and lost teeth-ongoing problem
Poor nutrition & decreased appetite-often caused by dental problems
Decay [caries/cavites]-caused by bacteria penetrates through enamel that protects tooth
Destruction of inner structures of tooth
infection
3



caries


Periodontal Disease
less obvious than caries
potentially more serious complication of poor oral care
Food debris & plaque build up in mouth & on teeth
Bacteria multiply-lots of “food “ for them
Disrupts “seal” between gum and tooth
Infection; bone loss
bacteria cause bad breath, or halitosis. disturbing to the older person and anyone in close contact
8



Periodontal Disease (cont.)
Gingivitis-the beginning of periodontal disease
gum swelling, tenderness, and bleeding
eventually recession of gum tissue away from the tooth
11

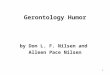
Healthy gums

Gingivitis

Gingivitis with some recession



Pain
caries & periodontal disease most common reason for oral pain
Sometimes oral lesions, stomatitis
may be limited to mouth or may affect the face and jaw
can cause loss of appetite, decreased food/fluid intake
negative effect on the overall quality of life
17

Dentures
Partial plates-tend to catch particles of food-can weaken healthy teeth
Complete dentures-difficult to fit
Dentures may not fit properly if a significant amount of weight is gained or lost
Dentures can cause irritation, inflammation, and ulceration of gums and oral mucous membranes
18




Dry Mouth
Xerostomia, or dry mouth is common normal age-related reduction in saliva
medication side effects
inadequate hydration
diseases such as diabetes
Makes chewing and swallowing more difficult, promotes tooth decay, and alters the sense of taste
22

Leukoplakia
White patches in the mouth
Often are precancerous and require prompt medical attention
Can also be med s/e or thrush
Lesions on the posterior third or sides of the tongue often are abnormal and should be brought to the attention of the physician
23

Leukoplakia (cont.)
24

A disease that is suspected to play a role in thromboembolic disorders, bacterial endocarditis, and myocardial infarction is:
A. dental caries.
B. halitosis.
C. gingivitis.
D. periodontal disease.
25

Cancer
Oral or pharyngeal cancer have poor prognosis
Early recognition and treatment before mets to other tissues offer the best hope
Symptoms- include leukoplakia or erythroleukoplakia, sores in the mouth that do not heal, oral bleeding, pain or difficulty swallowing, difficulty wearing dentures, swollen lymph nodes in the neck, earache
26

Disorders Caused by Vitamin Deficiencies
deficiencies of riboflavin, niacin, and vitamin C can affect oral mucous membranes
A smooth purplish sore tongue may be related to riboflavin deficiency
Complaint of a burning sensation or soreness of the mouth may indicate niacin deficiency
27

Superinfections
relatively common
Caused by broad-spectrum antibiotic therapy for some other infection Antibiotics destroy the normal mouth flora
allow opportunist bacteria or yeast colonies to become established and grow
28

Superinfections (cont.)
A hairy tongue result of enlargement of the papillae on the tongue
often follows antibiotic therapy
Black or brown discoloration on the tongue may be caused by tobacco use or by a chromogenic (color-producing) bacterium
29



Alcohol- and Tobacco-Related Problems
Alcohol and tobacco, even in small amounts, can harm the mucous membranes
Alcohol- chemically irritating and drying to the mucous membranes
Tobacco- smoked, chewed, or snuff, increases risk for oral cancer
32

Problems Caused by Neurologic Conditions
Neuro conditions such as stroke, multiple sclerosis, or Parkinson’s disease decrease coordination and strength difficult to manipulate toothbrush & floss
Can be difficult to open mouth
Difficult to raise arm[s]
33

Problems Caused by Neurologic Conditions (cont.)
severe arthritis-equipment difficult to manipulate difficult to open the mouth
Can’t hold toothbrush or floss
Raise arms to be able to get to mouth
medication for seizure or other neuro disorders need to use special precautions medications often cause gum problems
34

Nursing Interventions for Impaired Oral Mucous Membranes
Complete a thorough assessment of the oral mucous membranes
Initiate referral to a dentist or dental hygienist
Provide oral hygiene
35

Nursing Interventions for Impaired Oral Mucous Membranes (cont.)
Promote adequate intake of nutrients and fluids
lozenges or topical analgesics as prescribed
Report suspected side effects of medication therapy to the physician and dentist
36

Dental care
Access to dental care is often an issue for people with impaired mobility Getting to the office
Ability to tolerate time in wheel chair/use walker
Getting on to the chair
Ability to cooperate with personnel
Ability to open their mouth

Chapter 18Elimination
38

Objectives
Describe normal elimination processes.
Identify people who are most at risk for problems with elimination.
Describe age-related changes in bladder and bowel elimination.
39

Normal Elimination Patterns
40

Bowel Elimination
typical adult:
moderate amount formed brown stool passed without difficulty
every 1- 2 days
urge usually occurs 30 to 45 minutes p meal gastrocolic and defecation reflexes stimulate peristalsis
41

Urinary Elimination
Usual adult:
urge when bladder has about 300 mL of urine This varies greatly
Voluntary control of external sphincter allows healthy adults to hold larger amounts until it’s
convenient
Most adults void between 6 and 10 times per day
42


Elimination and Aging
44


Constipation
Hard, dry stools- difficult to passIncreased risk associated with aging
decreased abdominal muscle toneInactivity &/or immobilityinadequate fluid intake
Especially combined with bulk forming agents [metamucil]
46

Constipation
inadequate dietary bulk
disease conditions [parkinsons, gastroparisis + more]
Medications
dependence on laxatives or enemas
various environmental conditions
Inability to get to toilet
holding too long, lack of privacy
47

Constipation (cont.)
Dietary fiber-important role in promoting normal elimination
indigestible substance traps moisture & provids bulk
Repeatedly ignoring the urge to defecate
can lead to problems with defecation reflex
48


Fecal Impaction
mass of hardened feces trapped in the rectum & can’t be passed result of unrelieved constipation
Symptoms longer-than-usual delay in defecation
Passage of small amounts of liquid stool without any formed fecal material
Digital examination of the rectum may reveal presence of a hardened mass of feces
50



Objectives
Discuss methods for assessing elimination practices.
Identify selected nursing diagnoses related to elimination problems.
Describe interventions used to prevent or reduce problems related to elimination.
53

Nursing Interventions for Constipation
Assess bowel elimination patterns and contributing factors
Increase physical activity
Increase intake of dietary fiber and fluids
Schedule or encourage toileting at times when the person’s defecation urge is strongest r/t meals
Cup of warm liquid in am
Position to facilitate ease of elimination
Provide privacy for elimination
54

Nursing Process for Diarrhea
55


Diarrhea
Frequent passage of liquid, unformed stools Stools are liquid because they pass through the large intestine too
rapidly and are expelled before sufficient water can be absorbed in the large intestine
Symptom of another problem many causes
malabsorption syndromes
Obstruction- tumors of the GI tract or stool
lactose intolerance
Diverticulosis
pathogenic organisms
medications
57


Nursing Interventions for Diarrhea
Assess the elimination pattern and suspected causative factors
Maintain adequate fluid intake
Institute measures to maintain skin integrity
Promptly report observations to the physician, and follow up on physician’s orders regarding medications that decrease intestinal motility
Stool testing as ordered
59

Bowel Incontinence
common for those who are unable to recognize &/or respond to normal sensation mental impairment
Mobility
Delayed assistance
Less frequently disorders of color or rectum Cancer
inflammatory bowel disease
Diverticulitis
weak rectal muscles
diarrhea
60

Nursing Goals/Outcomes
Exhibit regular patterns of bowel elimination
Identify behaviors that promote normal bowel functioning
Modify behaviors to enhance regular bowel elimination
61

Nursing Interventions
Assess patterns of elimination and causative factors
Establish a toileting schedule Bowel training program
Take measures to prevent or reduce episodes of constipation
Use appropriate aids or garments
Clean the person promptly after each episode of incontinence
62

Nursing Process for Impaired Urinary Elimination
63


Urinary Retention
Abnormal accumulation of urine in the bladder; bladder unable to empty completely Normally, no more than 50 mL of urine remains in the bladder after voiding
decreased muscle tone in the bladder wall
medications
prostate gland enlargement/uterine prolapse
trauma to the muscles of the perineum
neurologic problems
anxiety
Decreased fluid intake
65

Urinary Retention (cont.)
Symptoms feeling of fullness, discomfort, or tenderness
Small frequent voids
Frequent bladder infections
Restlessness
diaphoresis
66





Urinary Retention Treatment
If caused by perineal trauma or anxiety noninvasive tx such as medications, peppermint oil [inhaled scent] or a
sitz bath may be enough to stimulate effective voiding
If severe retention is caused by an obstruction such as an enlarged prostate, catheterization or surgery may be necessary prevent serious bladder damage that could result from persistent or
excessive bladder distention
Pessarys were once commonly used with uterine prolapse, now usual tx is surgery
71

Urinary Incontinence
The involuntary loss of urine social or hygiene problem
In some cases, incontinence is curable using surgery ,medications, or other treatments
Kegel exercises
In others- better managed, thus allowing the older person a more normal lifestyle
72

Types of Urinary Incontinence
Stress incontinence Leakage of urine
conditions that increase intra-abdominal pressure
exercise, lifting heavy objects, laughing, coughing, or sneezing
Urge incontinence Caused by involuntary contraction of the detrusor muscle of
the bladder
Overflow incontinence Leakage of small amounts of urine from an overly full
bladder
Common with retention problems
73

Types of Urinary Incontinence (cont.)
Functional incontinence normal urethral and bladder function
cognitive or physical in nature
Total incontinence A condition in which older adults experience continuous and
unpredictable loss of urine
74

Nursing Goals/Outcomes
Exhibit a reduction in episodes of urinary incontinence or retention
Urinate at acceptable times in acceptable places
Identify measures that reduce episodes of urinary incontinence or retention Ie-toilet every 2 hours
Bladder training program
Establish a routine to reduce or prevent the occurrence of bladder elimination problems
75

Nursing Interventions
Assess elimination and fluid intake patterns
Explain measures that help improve tone of the sphincter muscles Kegel exercises
Modify clothing to make toileting easier
Reduce environmental barriers grab bars in the bathroom, installing toilet risers, keeping
the urinal or bedpan readily available, and providing a call signal for assistance
76

Nursing Interventions (cont.)
Answer call signals promptly
Develop a toileting schedule
Familiarize older adults with the locations of bathrooms throughout the facility
Provide support and encouragement
Initiate actions to maintain skin integrity
Provide incontinence pads or garments when appropriate
77

Disposable and Reusable Incontinence Garments
78