Embed Size (px)
Citation preview
Vol. 2/2003 Nr 4(5)
Endokrynologia PediatrycznaPediatric Endocrinology
Vol. 2/2003, Nr 4(5) 9
Intrauterine growth retardation – consequences for individual growing, growth hormone, and IGF-I secretion
Wpływ dystrofi i wewnątrzmacicznej na przebieg wzrastania, wydzielanie hormonu wzrostu i IGF-IJoanna Smyczyńska, Reanta Stawerska, Maciej Hilczer, Michał Karasek, Andrzej Lewiński
Department of Endocrinology and Isotope Therapy, Institute of Endocrinology, Medical University of Łódź at Polish Mother’s Memorial Hospital – Research Institute, Łódź, PolandKlinika Endokrynologii i Terapii Izotopowej Zakładu Endokrynologii Uniwersytetu Medycznego w Łodzi, Instytut Centrum Zdrowia Matki Polki w Łodzi
Adres do korespondencji: Klinika Endokrynologii i Terapii Izotopowej Instytutu Endokrynologii Uniwersytetu Medycznego w Łodzi, Instytut Centrum Zdrowia Matki Polki, ul. Rzgowska 281/289, 93-338 Łódź, e-mail: [email protected]
Key words: intrauterine growth retardation, short stature, growth hormone defi ciency, insulin-like growth factor ISłowa kluczowe: wewnątrzmaciczne zahamowanie wzrastania, niedobór wzrostu, niedobór hormonu wzrostu, insulinopodobny czynnik wzrostowy I
STRESZCZENIE/ABSTRACTSTRESZCZENIE/ABSTRACTSTRESZCZENIE/
Introduction: Intrauterine growth retardation (IUGR) is connected with an increased risk of short stature. The defi nition of IUGR requires the cause-effect relationships between the impact of unfavourable factors and low birth weight. In practice, IUGR is diagnosed in children small for gestational age (SGA). Objective: The aim of the study was to assess the influence of IUGR on individual growing, growth hormone (GH) secretion and insulin-like growth hormone (IGF-I) secretion.Material and methods: The analysis comprised 503 children (348 boys, 155 girls) with short stature (below 3rd
centile for age and sex), diagnosed at age of 11.6 ± 3.2 years (mean ± SD), with known gestational age (GA) and birth weight. Children with birth weight below10th centile for GA were classifi ed as SGA, while the remaining ones were recognised as appropriate for GA (AGA). In case of decreased GH secretion (GH peak below 10.0 ng/mL in two stimulation tests), GH defi ciency was diagnosed. For all the patients IGF-I concentration was assessed, and predicted adult height (PAH) was calculated.Results: In the analysed group, SGA was diagnosed in 131 cases (26%), while – by defi nition – SGA refers to 10% of general population. The incidence of GH defi ciency was insignifi cantly lower in SGA than that in AGA, GH peak was signifi cantly higher in SGA than that in AGA, and IGF-I secretion was also signifi cantly higher in SGA than that in AGA. At the same time patients’ height at diagnosing was signifi cantly lower in SGA than in AGA, and PAH was signifi cantly lower in SGA than in AGA. Prematurity was not associated with higher incidence of either short stature or GH defi ciency.Conclusions: Intrauterine growth retardation is a risk factor of short stature, but its infl uence on growing occurs by mechanisms other than the restriction of GH and IGF-I secretion.
Wstęp: Wewnątrzmaciczne zahamowanie wzrastania (intrauterine growth retardation – IUGR) wiąże się ze zwiększonym ryzykiem niedoboru wzrostu w późniejszych okresach życia. Dla rozpoznania IUGR istotne jest

10
Praca oryginalna Endokrynol. Ped., 2/2003;4(5):9-16
stwierdzenie występowania związku przyczynowo-skutkowego pomiędzy działaniem niekorzystnych czynników a niską urodzeniową masą ciała. W praktyce IUGR rozpoznaje się u wszystkich dzieci, które rodzą się za małe w stosunku do wieku płodowego (small for gestational age – SGA). Cel pracy: Celem pracy była ocena wpływu IUGR na proces wzrastania, wydzielanie hormonu wzrostu (growth hormone – GH) i insulinopodobnego czynnika wzrostowego I (insulin-like growth factor I – IGF-I). Materiał i metody: Analizą objęto 503 dzieci (348 chłopców, 155 dziewcząt) z niedoborem wzrostu (wysokość ciała poniżej 3 centyla dla wieku i płci), w wieku 11,6 ± 3,2 lat (średnia ± SD), dla których znane były wiek ciążowy (gestational age – GA) i masa urodzeniowa. Dzieci urodzone z masą ciała poniżej 10 centyla dla GA zakwalifi kowano jako SGA, pozostałe – jako urodzone z masą ciała odpowiednią dla GA (appropriate for GA – AGA). Niedobór GH rozpoznawano na podstawie obniżonego wydzielania GH (maksymalne wydzielanie w dwóch testach stymulacyjnych poniżej 10 ng/mL). U wszystkich pacjentów oznaczono stężenie IGF-I oraz obliczono przewidywaną ostateczną wysokość ciała (predicted adult height – PAH).Wyniki: W analizowanej grupie pacjentów stwierdzono SGA w 131 przypadkach (26%), podczas gdy – zgodnie z przyjętymi kryteriami progowymi – w populacji generalnej częstość SGA wynosi 10%. Częstość niedoboru GH była nieznamiennie niższa w SGA niż w AGA, maksymalne wydzielanie GH i IGF-I – znamiennie wyższe w SGA niż w AGA, podczas gdy wysokość ciała w momencie diagnostyki była znamiennie niższa, a prognoza wzrostowa – znamiennie gorsza w SGA niż w AGA. Wcześniactwo nie okazało się czynnikiem ryzyka niedoboru wzrostu ani niedoboru GH. Wnioski: Wewnątrzmaciczne zahamowanie wzrastania jest czynnikiem ryzyka niedoboru wzrostu. Wpływ IUGR na proces wzrastania może zachodzić za pośrednictwem mechanizmów niezwiązanych z obniżeniem wydzielania GH i IGF-I.
Introduction
Disturbed intrauterine growing affects individual development. Both genetic defects and the infl uence of harmful environmental factors may disturb foetal growing, causing intrauterine growth retardation (IUGR) and resulting in too small body weight and/or too small body length vs. the gestational age (GA). Because of the variety of factors, which bring about intrauterine dystrophy, the criteria, which qualify a child as the one with IUGR, are based on the scores of birth weight and/or birth body length, referred to GA. For the proper assessment of new-borns, appropriate centile charts of birth weight and birth length for GA should be used [1]. According to WHO criteria, all the children with birth weight below 10 centile for GA are qualifi ed as small for gestational age (SGA). By this defi nition, 10% of all the new-borns are SGA. In fact, only in some of them, intrauterine growth was really disturbed, while the remaining ones are either the smallest of healthy new-borns or they are children with inadequately assessed GA [2]. Thus, the diagno-sis of IUGR on the grounds of low birth weight only does not take into account the signifi cance of foetal growth disturbances in the pathogenesis of intrauterine dystrophy. In practice, however, SGA children are usually identifi ed as those with IUGR [3, 4, 5]. In Poland, the reference values of birth weight for GA have recently been published by Brzozowska [6], Norska-Borówka [7] and Słomko
[4]. It was shown in our previous study [8] that the data of newborns from the Łódź Region are closely related to the normative data of Słomko [4].
It is well known that most of the children with IUGR achieve normal height in the second year of life, however, in 8–20% of them, the catch-up of growth is not observed [9]. In intrauterine dystro-phy, the risk of short stature is 5–7-fold increased in comparison with children with normal birth weight; thus, children born with features of IUGR compose 20% of all the children with short stature [10, 11].
Objective
The aim of the study was the assessment of relationships between birth weight and individual growing, growth hormone (GH) secretion and IGF-I serum concentration in children with short stature, especially with respect to the possible mechanisms responsible for growth defi cit – either connected with decreased GH and IGF-I secretion or not. The infl uence of prematurity (PreM) and pathological delivery on growing has been evaluated.
Material and methods
The analysis comprised 503 children (348 boys, 155 girls) with short stature – height SDS (H SDS) below 3rd centile for age and sex, according to the rd centile for age and sex, according to the rd
national reference values [12], diagnosed at the age of 11.6 ± 3.2 years (mean ± SD). For all the pa-
11
Smyczyńska J. et al. – Intrauterine growth retardation...
tients, both GA and birth weight, as well as the data concerning the course of delivery and Apgar score after birth, were known. According to the national normative data [4], children with birth weight below 10th centile for GA were classifi ed as SGA, while th centile for GA were classifi ed as SGA, while th
the remaining ones were recognised as appropri-ate for GA (AGA). Patients’ height was expressed as height SD score (H SDS) for age and sex, ac-cording to Tanner-Whitehouse normative data [13]. Bone age was assessed, according to Greulich-Pyle standards [14] for all the patients. Growth hormone (GH) defi ciency was diagnosed in case of decreased GH secretion (GH peak below 10.0 ng/mL) in two stimulation tests (with clonidine in a dose of 0.15 mg/m2 p.o. and with glucagon in a dose of 30 μg/kg i.m.). Severe GHD (sGHD) was diagnosed in children with GH peak below 5.0 ng/mL in both tests, while partial GHD (pGHD) – in case of maximal GH peak in two tests, ranging from 5.0 ng/mL to 10.0 ng/mL. The re-maining children, with GH peak above 10.0 ng/mL, were qualifi ed as those with idiopathic short stature (ISS). Insulin-like growth factor-I (IGF-I) and its binding protein-3 (IGFBP-3) secretion was also as-sessed for all the patients and expressed as SD score (IGF-I SDS) for age and sex, according to own data for short children. On the grounds of patient’s height and bone age, the predicted adult height was calcu-lated according to Bayley-Pinneau method for all the children. Thyroid function, assessed on the basis of thyrotropin and free thyroxine serum concentrations, was normal in all the cases.Serum GH concentration was measured with by immunometric assay (IMMULITE, DPC) for the quantitative measurement of human GH (hGH), calibrated to WHO IRP 80/505 standard, with an analytical sensitivity up to 0.01 ng/mL, calibration range up to 40 ng/mL, the intra-assay coeffi cient of variance (CV) 5.3–6.5%, and the inter-assay CV 5.5–6.2%. Serum IGF-I concentration was assessed with radioimmunoassay IGF-I-D-RIA-CT, Bio-Source Europe S.A., with a minimal detectable con-centration of 0.4 ng/mL, intra-assay CV 3.9–9.5%, inter-assay CV 5.0–8.0%. Serum IGFBP-3 concen-tration was assessed with with immunoradiometric (IRMA) assay – IRMA DSL-6600, Diagnostic System Laboratories, Inc., USA, with a minimal detectable concentration of 0.5 ng/mL, intra-assay CV 1.8–3.9%, and inter-assay CV 0.5-1.9%.
Patients’ height, PAH, and IGF-I serum concen-tration were expressed as SDS, in order to allow a comparison among children with different age and sex. Because the distribution of some of the
analysed parameters was different from the nor-mal distribution, the analysis was performed with nonparametric tests for two independent samples (U Mann-Whitney test) and for many independent samples (ANOVA rank Kruskall-Wallis test).
Results
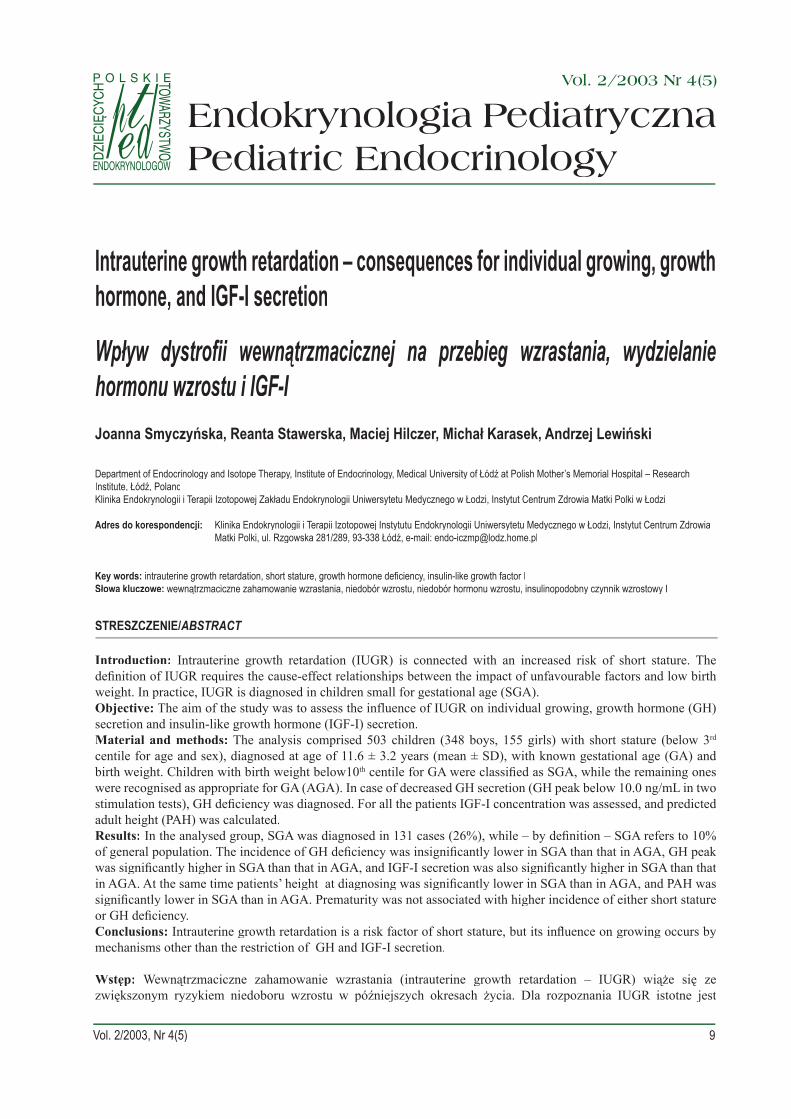
For the whole analysed group, the mean dura-tion of gestation was 39.1 weeks (range: 26.0–42.0 weeks), 445 children (88.5%) were full-term deliv-ered, while 58 children (11.5%) were PreM. For comparison, the occurrence of PreM among chil-dren, born at the Polish Mother’s Memorial Hos-pital in Łódź during one year (1999) was 19.5%, being probably slightly higher than the incidence of PreM in the Łódź Region, this difference resulting from a certain condensation of affected gestation cases treated at our Hospital. Thus, the incidence of PreM does not seem to be higher in short children than the total incidence of PreM in children of the Łódź Region. The distribution of GA is shown in Figure 1.
In 200 out of 445 full-term children (44.9%) and in 24 out of 58 PreM (41.4%), GHD was diagnosed. The incidence of GHD was insignifi cantly lower in PreM than that in the full-term children. So, PreM was not a risk factor of GHD. The incidence of sGHD was also insignifi cantly lower in PreM children (6.9%) than that in the full-term children (9.4%), while the occurrence of pGHD was very similar in both groups (34.5% and 35.5%, respec-tively). Thus, PreM is not a risk factor of GHD. Table I presents detailed data, concerning the inci-
Fig. 1. GA distribution in the analysed group of patientsRyc. 1. Rozkład wieku ciążowego w analizowanej grupie pacjentów
12
Praca oryginalna Endokrynol. Ped., 2/2003;4(5):9-16
dence of GHD with respect to GA in the analysed group of children.
There were no signifi cant differences in the severity of height defi cit and both the target height and the predicted adult height between PreM and full-term neonates. The mean values of GH peak and IGF-I SDS were very similar in both groups. Detailed data, concerning the above parameters, are shown in Table II. Because no differences were found in the analysed parameters between PreM and full-term children, further studies involved all the children together.
All the patients were then divided, according to the normal or low birth weight for GA, with the cut-off value of 10th centile of birth weight for GA, accord-th centile of birth weight for GA, accord-th
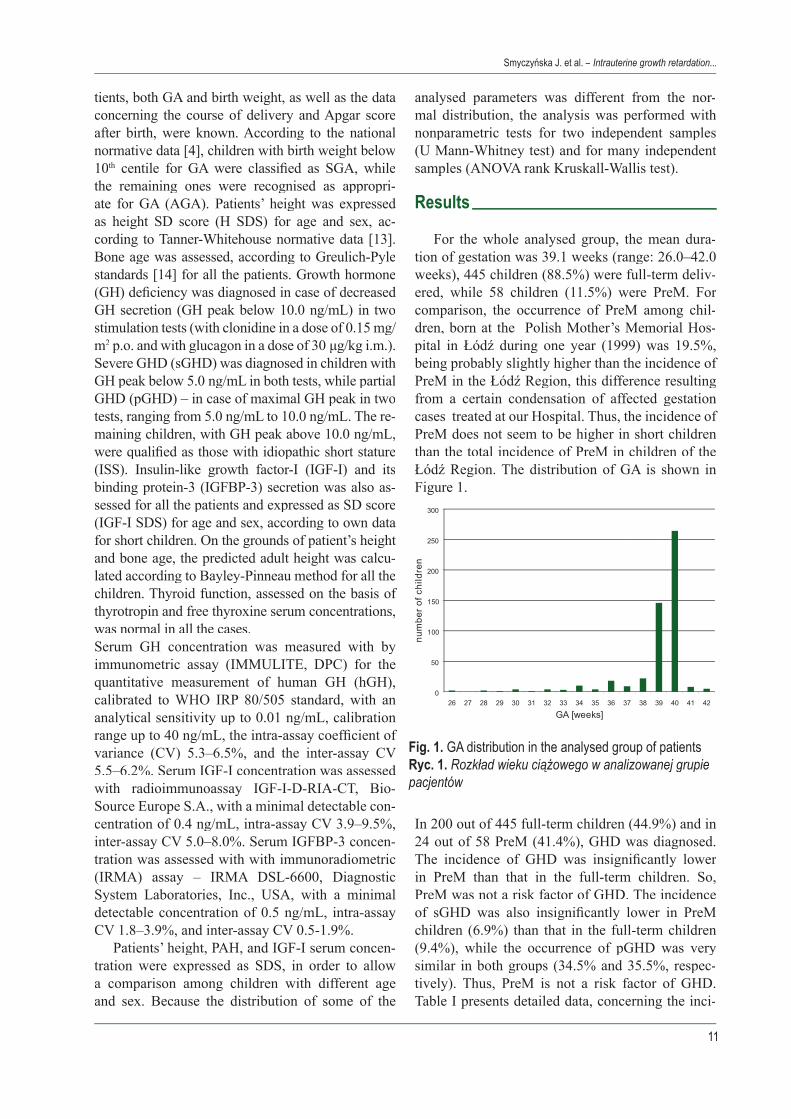
ing to the national reference values [4]. In 131 cases (26.0%), SGA was diagnosed, while the remaining 372 children (74.0%) were classifi ed as AGA. In the examined group of short children, over 1⁄4 was born SGA, while – in accordance with the cut-off criteria – the incidence of SGA is 10% in the general popula-
tion. The occurrence of SGA is over 2.5 times higher in children with short stature than that in the total population of children, appearing to be an important risk factor of short stature (see Fig. 2).
The occurrence of GHD was insignifi cantly low-er in SGA (39.7%) than that in AGA (46.2%). De-tailed data, concerning the incidence of GHD, both severe and partial, are shown in Table III. Thus, in the analysed group of children with short stature, SGA does not seem to be a risk factor of GHD. However, taking into account the higher incidence
PreM On-time
ISS 34 (58.6%) 245 (55.1%)
GHD 24 (41.4%) 200 (44.9%)
sGHD 4 (6.9%) 42 (9.4%)
pGHD 20 (34.5%) 158 (35.5%)
total 58 (100%) 445 (100%)
Table I. The incidence of ISS and GHD with respect to GA in short childrenTabela I. Częstość ISS i GHD u dzieci z niedoborem wzrostu w zależności od GA
PreM Full-term
Age [years] 11.7 ± 3.3 11.6 ± 3.2
H SDS -2.20 ± 0.69 -2.14 ± 0.65
TH SDS -0.68 ± 0.82 -0.70 ± 0.74
PAH SDS -1.27 ± 1.00 -1.19 ± 1.02
GH peak [ng/mL] 14.9 ± 9.8 13.4 ± 8.8
IGF-I SDS 0.26 ± 1.28 0.11 ± 1.34
Table II. Selected auxological parameters, GH and IGF-I secretion vs. GA in short childrenTabela II. Wybrane wskaźniki rozwoju auksologicznego oraz wydzielanie GH i IGF-I w zależności od GA u dzieci z niedoborem wzrostu
Fig. 2. The incidence of IUGR in the examined group of children with short stature and in general populationRyc. 2. Częstość IUGR w badanej grupie pacjentów z niedoborem wzrostu i w populacji generalnej
SGA AGA
ISS 79 (60.3%) 200 (53.8%)
GHD 52 (39.7%) 172 (46.2%)
sGHD 10 (7.6%) 42 (11.3%)
pGHD 42 (32.1%) 130 (34.9%)
total 131 (100%) 372 (100%)
Table III. The incidence of GHD in short children, according to birth weight for GATabela III. Częstość GHD u dzieci z niedoborem wzrostu w zależności od urodzeniowej masy ciała w odniesieniu do GA
13
Smyczyńska J. et al. – Intrauterine growth retardation...
of short stature in SGA than in AGA, it becomes clear that, in fact, the incidence of GHD is higher in SGA than that in AGA. [Table III]
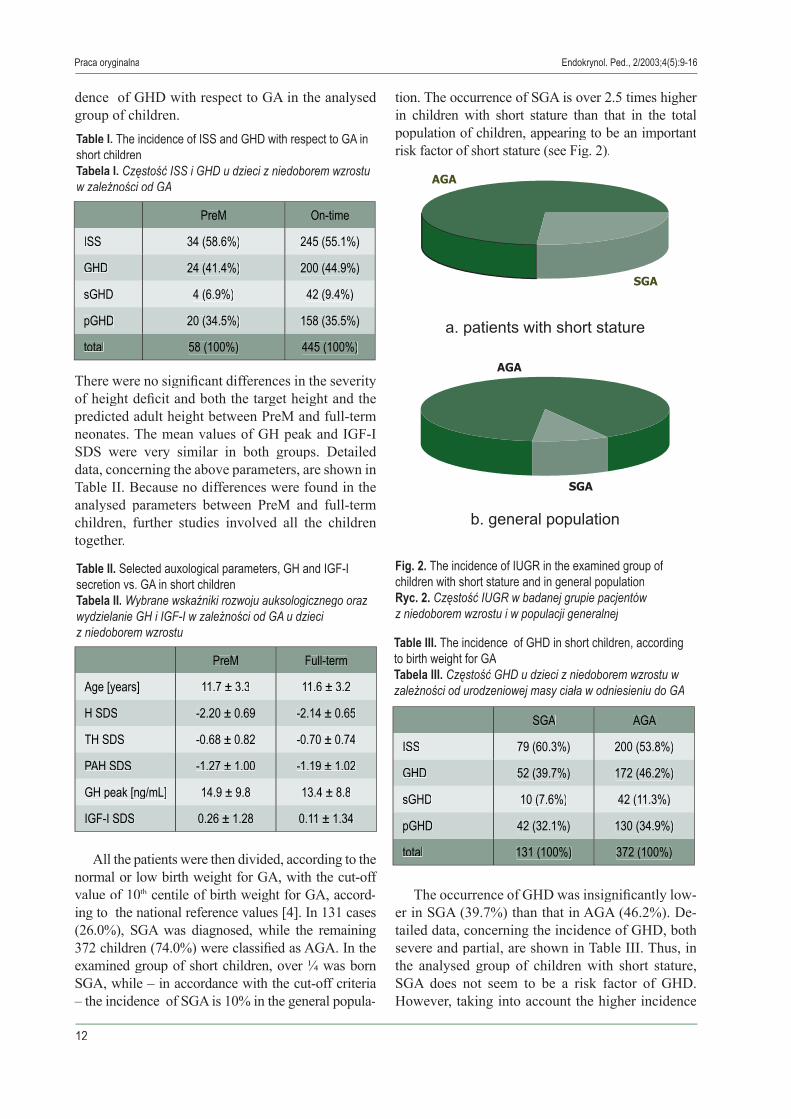
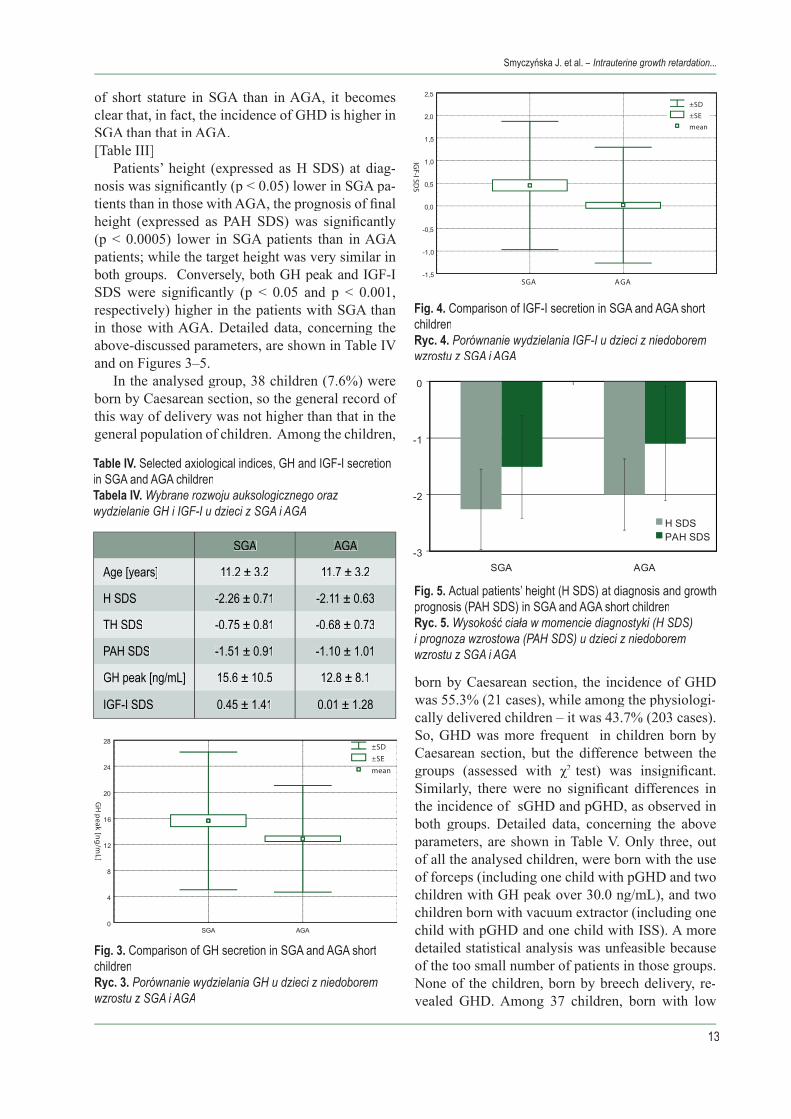
Patients’ height (expressed as H SDS) at diag-nosis was signifi cantly (p < 0.05) lower in SGA pa-tients than in those with AGA, the prognosis of fi nal height (expressed as PAH SDS) was signifi cantly (p < 0.0005) lower in SGA patients than in AGA patients; while the target height was very similar in both groups. Conversely, both GH peak and IGF-I SDS were signifi cantly (p < 0.05 and p < 0.001, respectively) higher in the patients with SGA than in those with AGA. Detailed data, concerning the above-discussed parameters, are shown in Table IV and on Figures 3–5.
In the analysed group, 38 children (7.6%) were born by Caesarean section, so the general record of this way of delivery was not higher than that in the general population of children. Among the children,
born by Caesarean section, the incidence of GHD was 55.3% (21 cases), while among the physiologi-cally delivered children – it was 43.7% (203 cases). So, GHD was more frequent in children born by Caesarean section, but the difference between the groups (assessed with χ2 groups (assessed with χ2 groups (assessed with χ test) was insignifi cant. Similarly, there were no signifi cant differences in the incidence of sGHD and pGHD, as observed in both groups. Detailed data, concerning the above parameters, are shown in Table V. Only three, out of all the analysed children, were born with the use of forceps (including one child with pGHD and two children with GH peak over 30.0 ng/mL), and two children born with vacuum extractor (including one child with pGHD and one child with ISS). A more detailed statistical analysis was unfeasible because of the too small number of patients in those groups. None of the children, born by breech delivery, re-vealed GHD. Among 37 children, born with low
SGA AGA
Age [years] 11.2 ± 3.2 11.7 ± 3.2
H SDS -2.26 ± 0.71 -2.11 ± 0.63
TH SDS -0.75 ± 0.81 -0.68 ± 0.73
PAH SDS -1.51 ± 0.91 -1.10 ± 1.01
GH peak [ng/mL] 15.6 ± 10.5 12.8 ± 8.1
IGF-I SDS 0.45 ± 1.41 0.01 ± 1.28
Table IV. Table IV. T Selected axiological indices, GH and IGF-I secretion in SGA and AGA childrenTabela IV. Wybrane rozwoju auksologicznego oraz wydzielanie GH i IGF-I u dzieci z SGA i AGA
Fig. 3. Comparison of GH secretion in SGA and AGA short childrenRyc. 3. Porównanie wydzielania GH u dzieci z niedoborem wzrostu z SGA i AGA
Fig. 4. Comparison of IGF-I secretion in SGA and AGA short childrenRyc. 4. Porównanie wydzielania IGF-I u dzieci z niedoborem wzrostu z SGA i AGA
Fig. 5. Actual patients’ height (H SDS) at diagnosis and growth prognosis (PAH SDS) in SGA and AGA short childrenRyc. 5. Wysokość ciała w momencie diagnostyki (H SDS) i prognoza wzrostowa (PAH SDS) u dzieci z niedoborem wzrostu z SGA i AGA
14
Endokrynol. Ped., 2/2003;4(5):9-16Praca oryginalna
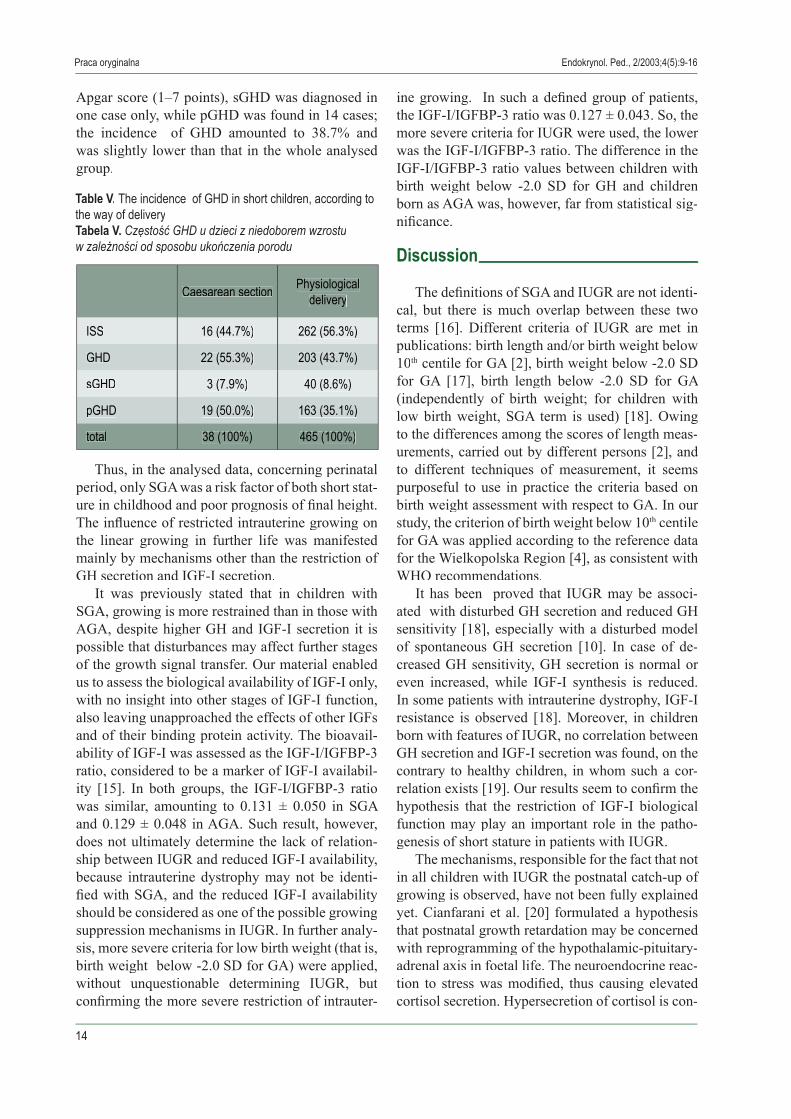
Apgar score (1–7 points), sGHD was diagnosed in one case only, while pGHD was found in 14 cases; the incidence of GHD amounted to 38.7% and was slightly lower than that in the whole analysed group.
Thus, in the analysed data, concerning perinatal period, only SGA was a risk factor of both short stat-ure in childhood and poor prognosis of fi nal height. The infl uence of restricted intrauterine growing on the linear growing in further life was manifested mainly by mechanisms other than the restriction of GH secretion and IGF-I secretion.
It was previously stated that in children with SGA, growing is more restrained than in those with AGA, despite higher GH and IGF-I secretion it is possible that disturbances may affect further stages of the growth signal transfer. Our material enabled us to assess the biological availability of IGF-I only, with no insight into other stages of IGF-I function, also leaving unapproached the effects of other IGFs and of their binding protein activity. The bioavail-ability of IGF-I was assessed as the IGF-I/IGFBP-3 ratio, considered to be a marker of IGF-I availabil-ity [15]. In both groups, the IGF-I/IGFBP-3 ratio was similar, amounting to 0.131 ± 0.050 in SGA and 0.129 ± 0.048 in AGA. Such result, however, does not ultimately determine the lack of relation-ship between IUGR and reduced IGF-I availability, because intrauterine dystrophy may not be identi-fi ed with SGA, and the reduced IGF-I availability should be considered as one of the possible growing suppression mechanisms in IUGR. In further analy-sis, more severe criteria for low birth weight (that is, birth weight below -2.0 SD for GA) were applied, without unquestionable determining IUGR, but confi rming the more severe restriction of intrauter-
ine growing. In such a defi ned group of patients, the IGF-I/IGFBP-3 ratio was 0.127 ± 0.043. So, the more severe criteria for IUGR were used, the lower was the IGF-I/IGFBP-3 ratio. The difference in the IGF-I/IGFBP-3 ratio values between children with birth weight below -2.0 SD for GH and children born as AGA was, however, far from statistical sig-nifi cance.
Discussion
The defi nitions of SGA and IUGR are not identi-cal, but there is much overlap between these two terms [16]. Different criteria of IUGR are met in publications: birth length and/or birth weight below 10th centile for GA [2], birth weight below -2.0 SD for GA [17], birth length below -2.0 SD for GA (independently of birth weight; for children with low birth weight, SGA term is used) [18]. Owing to the differences among the scores of length meas-urements, carried out by different persons [2], and to different techniques of measurement, it seems purposeful to use in practice the criteria based on birth weight assessment with respect to GA. In our study, the criterion of birth weight below 10th centile for GA was applied according to the reference data for the Wielkopolska Region [4], as consistent with WHO recommendations.
It has been proved that IUGR may be associ-ated with disturbed GH secretion and reduced GH sensitivity [18], especially with a disturbed model of spontaneous GH secretion [10]. In case of de-creased GH sensitivity, GH secretion is normal or even increased, while IGF-I synthesis is reduced. In some patients with intrauterine dystrophy, IGF-I resistance is observed [18]. Moreover, in children born with features of IUGR, no correlation between GH secretion and IGF-I secretion was found, on the contrary to healthy children, in whom such a cor-relation exists [19]. Our results seem to confi rm the hypothesis that the restriction of IGF-I biological function may play an important role in the patho-genesis of short stature in patients with IUGR.
The mechanisms, responsible for the fact that not in all children with IUGR the postnatal catch-up of growing is observed, have not been fully explained yet. Cianfarani et al. [20] formulated a hypothesis that postnatal growth retardation may be concerned with reprogramming of the hypothalamic-pituitary-adrenal axis in foetal life. The neuroendocrine reac-tion to stress was modifi ed, thus causing elevated cortisol secretion. Hypersecretion of cortisol is con-
Caesarean section Physiological delivery
ISS 16 (44.7%) 262 (56.3%)
GHD 22 (55.3%) 203 (43.7%)
sGHD 3 (7.9%) 40 (8.6%)
pGHD 19 (50.0%) 163 (35.1%)
total 38 (100%) 465 (100%)
Table V. The incidence of GHD in short children, according to the way of deliveryTabela V. Częstość GHD u dzieci z niedoborem wzrostu w zależności od sposobu ukończenia porodu

15
sidered to be responsible for growing restriction. The postulated mechanism of this phenomenon relies on suppressing IGFBP-3 proteolysis, thus reducing IGF-I bioavailability.
Much attention is paid to the relationships be-tween IUGR and the metabolic syndrome disclo-sure in adult life. Barker et al. [21] showed associa-tions between IUGR and the increased prevalence of metabolic syndrome, including obesity, hyperten-sion, and non-insulin dependent diabetes mellitus in adulthood. It has been proved in experimental stud-ies on mice that IUGR/SGA may be a consequence of altered insulin and IGF-I action in foetal life [22]. In human with IUGR, an association was observed between the postnatal growth catch-up suppression and insulin resistance. It is hypothesised that com-mon mechanism – probably dysfunction of insulin and/or IGF-I receptor – may be responsible for both IUGR and later development of the metabolic syndrome [16]. The observed IGF-I-resistance, connected with insulin-resistance, may result from the homology between IGF-I receptors and insulin receptors [18]. Defects of IGF-I receptor are consid-ered to be another cause of IUGR and short stature, especially in patients with normal GH and IGF-I secretion. It was shown that in transgenic mice with IGF-I receptor knock out (likewise IGF-I knock out), alone or in combination with IGF-II knock out), profound embryonic and postnatal growth de-fi ciency is observed [23, 24]. Interesting data have been published by Hattori et al. [25] from the stud-ies on Pygmies – the population of the smallest peo-ple of the entire world. In this population, a marked reduction in the number of IGF-I receptors on cell surface of T lymphocytes, decreased IGF-I receptor gene transcription, and reduced receptor signalling were observed. The above data confi rm the hy-pothesis that human stature is, in part, genetically controlled by the expression of IGF-I receptor. Our
data, pointing to higher IGF-I secretion, connected with more severe growth defi cit in SGA, seem to be an indirect confi rmation of the possible signifi cance of this mechanism. Recently, point mutations have been detected in IGF-I receptor gene in some IUGR patients with postnatal growth failure and increased IGF-I secretion [26]. The last report provides a di-rect confi rmation of the association between IGF-I receptor defects and linear growing disorders in patients with IUGR.
If it is well documented that IUGR unfavourably infl uences the growing process in further periods of life, less signifi cance will be attributed to prema-turity. In our material, prematurity, as well as the mode of birth, turned out not to be the risk factors of GHD.
Numerous data confi rm the effectiveness of GH therapy in short children, born with IUGR, point-ing to the close relation between the dose of GH and the observed improvement of height velocity, independently from either normal or reduced GH secretion in stimulation tests [17, 18, 27]. Unfor-tunately, in Poland, so far, short stature caused by IUGR has not been an indication to GH therapy reimbursement by the Polish Ministry of Health. It seems to be purposeful to consider the indication to GH therapy for, at least, some of the patients with IUGR, especially when spontaneous growing catch-up in early childhood is not observed and the prognosis of fi nal height is poor.
Conclusions
The infl uence of IUGR on individual growing occurs mainly by mechanisms other than restric-tion of GH secretion and IGF-I secretion. The role of IGF-I receptor defects should be taken into ac-count in the pathogenesis of short stature in IUGR patients.
PIŚMIENNICTWO/REFERENCES
[1] Lubchenco L.O., Hansman C., Boyd E.: Intrauterine growth in length and head circumference as estimated from live birth at gestational ages from 26 to 42 weeks. Pediatrics, 1966:37, 403-408.
[2] Wollmann H.: Intrauterine growth restriction: defi nition and etiology. Horm. Res., 1998:49, suppl. 2, 1-6.[3] Osuch-Jaczewska R.: Wewnątrzmaciczne zahamowanie wzrastania, wcześniactwo, dystrofi a. [in:] Neonatologia. Red.
Łozińska D., Twarowska I., PZWL, Warszawa 1993, 339-361.[4] Słomko Z.: Relacja wieku ciążowego i masy urodzeniowej. [in:] Medycyna perinatalna. Red. Słomko Z., PZWL, Warszawa
1986:2, 356-372.
Smyczyńska J. et al. – Intrauterine growth retardation...

16
Praca oryginalna
Vol. 2/2003 Nr 4(5)[1] Lubchenco L.O., Hansman C., Boyd E.: Intrauterine growth in length and head circumference as estimated from live birth at
gestational ages from 26 to 42 weeks. Pediatrics, 1966:37, 403-408.[2] Wollmann H.: Intrauterine growth restriction: defi nition and etiology. Horm. Res., 1998:49, suppl. 2, 1-6.[3] Osuch-Jaczewska R.: Wewnątrzmaciczne zahamowanie wzrastania, wcześniactwo, dystrofi a. [in:] Neonatologia. Red.
Łozińska D., Twarowska I., PZWL, Warszawa 1993, 339-361.[4] Słomko Z.: Relacja wieku ciążowego i masy urodzeniowej. [in:] Medycyna perinatalna. Red. Słomko Z., PZWL, Warszawa
1986:2, 356-372.[5] Walczak M.: Podstawowe terminy stosowane dla określenia wieku ciążowego i urodzeniowej masy ciała. [in:] Ocena
wybranych wyznaczników procesów wzrastania i dojrzewania u wcześniaków oraz noworodków urodzonych z hipotrofi ą. Red. Szczapa J., Twarowska I., Postępy w neonatologii, Poznań 1997 (supl. III): 11-12.
[6] Brzozowska I.: Kształtowanie się wielkości parametrów rozwoju fi zycznego noworodków w Polsce. Problemy Medycyny Wieku Rozwojowego, 1973:3, 83.
[7] Norska-Borówka I.: Noworodek przedwcześnie urodzony oraz o niskiej masie ciała. [in:] Medycyna perinatalna. Red. Słomko Z., PZWL, Warszawa 1986:2, 373-385.
[8] Smyczyńska J., Stawerska R., Hilczer M.: The incidence of intrauterine growth retardation (IUGR) among newborns delivered at selected reference units (I0 and III0) in Łódź in 1999. Endokrynol. Pol. – Polish J. Endocrinol., 2000:51, suppl. 1/3, 113-118.
[9] Chatelain P.G., Cauderay M.C., de Zegher F. et al.: Growth hormone secretion and sensitivity in children born small for gestational age. Acta Paediatr., 1996:suppl. 417, 15-16.
[10] Albertsson-Wikland K., Boguszewski M., Karlberg J.: Children born small-for-gestational age: postnatal growth and hormonal status. Horm. Res., 1998:49, suppl. 2, 7-13.
[11] Stawerska R., Smyczyńska J., Hilczer M.: Comparison of the incidence of intrauterine growth retardation (IUGR), perinatal data and diagnostic observations in children with short stature of different etiology. Endokrynol. Pol.– Polish J. Endocrinol., 2000: 51, suppl. 1/3, 123-127.
[12] Palczewska I., Niedźwiecka Z.: Wskaźniki rozwoju somatycznego dzieci i młodzieży warszawskiej. Medycyna Wieku Rozwojowego, 2001:5, suppl. I/2, 17-118.
[13] Tanner J.M., Whitehouse R.H., Takaiashi M.: Standards from birth to maturity for height, weight, height velocity and weight velocity: British children, 1965. Arch. Dis. Child., 1966:41, 454-471, 613-635.
[14] Greulich W.W., Pyle S.I.: Radiographic Atlas of Skeletal Development of the Hand and Wrist. Stanford University Press, Stanford, California 1993.
[15] Juul A., Dalgaard P., Blum W.F. et al.: Serum levels of insulin-like growth factor (IGF) binding protein 3 (IGFBP-3) in healthy infants, children and adolescents: the relation to IGF-I, IGF-II, IGFBP-1, IGFBP-2, age, sex, body mass index, and pubertal maturation. J. Clin. Endocrinol. Metab., 1995:80, 2534-2542.
[16] Chatelain P.: Children born with intra-uterine growth retardation (IUGR) or small for gestational age (SGA): long term growth and metabolic consequences. Endocr. Regul., 2000:33, 33-36.
[17] De Zegher F., Jönsson P., Löfström A. et al.:. Growth hormone treatment of short children born small for gestational age: analysis of controlled trial and clinical experience in KIGS. [in]: Growth Hormone Therapy in KIGS – 10 Years’ Experience. Ed. Ranke M.B., Wilton P., Johann Ambrosius Verlag, Heidelberg 1999, 321-326.
[18] Chatelain P.G., Nicolino M., Claris O. et al.: Multiple hormone resistance in short children born with intrauterine growth retardation? Horm. Res., 1998:49, suppl 2, 20-22.
[19] De Wall W.J., Hokken Koelega A., Stijnen T. et al.: Endogenous and stimulated GH secretion, urinary GH excretion, and plasma IGF-I and IGF-II levels in prepubertal children with short stature after intrauterine growth retardation. The Dutch Working Group on Growth Hormone. Clin. Endocrinol., 1994:41, 621-630.
[20] Cianfarani S., Geremia C., Scott C.D. et al.: Growth, IGF system, and cortisol in children with intrauterine growth retardation: is catch-up growth affected by reprogramming of the hypothalamic-pituitary-adrenal axis? Pediatr. Res., 2002:51, 94-99.
[21] Barker D.J.P., Gluckmann P.D., Godfrey K.M. et al.: Fetal nutrition and cardiovascular disease. Lancet, 1993:341, 938-941.[22] Borelli E., Heyman R.A., Arias C. et al.: Transgenic mice with inductible dwarfi sm. Nature, 1988:339, 528-541.[23] Baker J., Liu J.P., Perkins A.S. et al.: Role of insulin-like growth factors in embryonic and postnatal development. Cell, 1993:
75, 73-82.[24] Liu J.P., Baker J., Perkins A.S. et al.: Mice carrying null mutations of the genes encoding insulin-like growth factor I (Igf-1) and
type 1 IGF receptor (Igf1r). Cell, 1993:75, 59-72.[25] Hattori Y., Vera J.C., Rivas C.I. et al.: Decreased insulin-like growth factor receptor expression and function in immortalized
African Pygmy T cells. J. Clin. Endocrinol. Metab., 1996:81, 2257-2263.[26] Abuzzahab M.J., Goddard A., Grigoriescu F. et al.: Human IGF-I receptor mutations associated with intrauterine and postnatal
growth retardation. Proc. of the 82nd Annual Meet. of the Endocrine Soc., 2000:abstr. 1947.[27] Juul A., Bernasconi S., Chatelain P. et al.: Diagnosis of growth hormone (GH) defi ciency and the use of GH in children with
growth disorders. Horm. Res., 1999:51, 284-299.
Endokrynol. Ped., 2/2003;4(5):9-16





























