Embed Size (px)
Citation preview
VOL 3 NO 1 JANUARY 2016
PAGE 1
DCMC Emergency DepartmentRadiology Case of the Month
These cases have been removed of identifying information and are intended for peerreview and educational purposes only.
Welcome to the DCMC Emergency Department Radiologycase of the month!
In conjunction with our pediatric radiologyspecialists from ARA we hope you enjoy these monthlyradiological highlights from the case files of the EmergencyDepartment at DCMC. These cases are meant to highlightimportant chief complaints, cases, and radiology findings thatwe all encounter every day.
If you enjoy these reviews we invite you check outPediatric Emergency Medicine Fellowship RadiologyRounds, which are currently offered quarterly and are heldwith the outstanding support of the pediatric radiologyspecialists at Austin Radiologic Association.
If you have any questions or feedback regarding the Case of the Month format, feel free to email Robert Vezzetti, MD at [email protected].
PEM Fellow Conference Schedule January 2016
5th - Simulation Faculty Development
6th - 8:00 Sim: Burns, Submersions.........Sim Faculty and Dr Boeck 11:00 Burn Trauma....................................Drs Vezzetti and Yee
13th - 9:15 Calculating Sample Size..........Drs Wilkinson & Gardiner 11:15 Grand Rounds................................................Dr Macias 20th - 9:15 Toxicology (Street Drugs)......................Drs Earp and Hill 10:15 Cardiac Ultrasound..........................................Dr Boeck 12:15 ED Staff Meeting
26th - Journal Club...............................................Drs Fiesen and Hill
27th - 9:15 M&M...........................................Drs Tabarrock and Berg 10:15 Board review:Tox/Environment......................Dr Remick 12:15 Research Update.......................................Dr Wilkinson
Grand Rounds:Spread of Pediatric Best Practice and CollabarativeCharles Macias, MDTexas Children’s Hospital All conferences are held in the DCMC Command Center (Rooms 3&4).Simulations are held at the Clinical Education Center - Brackenridge.
This month: It was inevitable! Coughing season is here and children are in the middle of a full and productive (pardon the pun) upper respiratory infection. Most of these children have a viral cause of their symptoms; some do not. Sorting out who needs chest imaging and who doesn’t can be tricky. Let’s ring in the New Year by looking at some chest films....
“Docendo Discimus”
January is named after Janus, the roman god with two faces, one looking forward and one looking backward. He was in charge of beginnings and transitions.The ancient Greeks had no equivalent of Janus, which the romans claim exclusively for their own!
VOL 3 NO 1 JANUARY 2016
PAGE 2
CASE 3A 17 month old female with a past history of bronchiolitis presents with cough, congestion, and fever to 104 for the past 3 days. She has had nonbilious emesis and decreased po intake; in fact she has had only 1 wet diaper in 24 hours. On exam, she is listless and in respiratory distress. Her mucous membranes are dry; she has moderate intercostal retractions and scattered rhonchi; there is decreased breath sounds to the right and crackles to the right lower lobe. Her respiratory rate is 60 and her oxygen saturation is 97% on 3L nasal cannula. You obtain IV access and give her a fluid bolus. Labs are obtained; her CBC shows a white blood cell count of 23 with 85 segs and 15 bands. Her flu test is negative. Does this child need an imaging study?
The first ball dropping celebration atop One Times Square was held on December 31, 1907. The original New Year's Eve Ball weighed 700 pounds and was five feet in diameter. It was made of iron and wood and was decorated with 100 25-watt light bulbs.
2008 gave the world a new Ball for New Year’s! This one is a geodesic sphere, 12 feet in diameter and weighing 11,875 pounds. It is built to withstand high winds and fluctuating temperatures. Waterford Crystal introduces a different pattern for each New Years celebration.
BIG NEWS!! Match Day was in December and we matched ALL of our positions. Starting July 2016 are new PEM Fellows:Drs. Anna Salinas, Whitney Wroe, Nina Vaidya, Whitney Irwin, Megan McClungWe look forward to working with them in the ED and throughout DCMC!
CASE 1Cough, cough everywhere...Ah Winter and Pediatrics! They do together like mac & cheese, peas & carrots, you get the idea. First up is a 7 year old male who has had cough and fever (up to 103) for the past 2 weeks. He has had some mild congestion. He also has begun to complain about right upper and epigastric abdominal pain for the past 7 days. He was seen several times by his Pediatrician. This last visit, which was 3 days ago, ended with a prescription for Amoxicillin for a throat infection (no strep test done per his mother). They deny travel or sick contacts, but he’s in school.His exam shows an afebrile child who has a respiratory rate of 22 (without retractions) and a room air pulse oximetry of 95%. He is nontoxic and conversing. His ears and throat look completely normal. He is not meningitic. His heart sounds fine (no murmur, rub) and his chest exam is relatively ok too. He does not have wheezing or crackles, but he does have slightly decreased breath sounds on the right. His abdomen is benign. The thought crosses you that this child may have pneumonia. Does he need an imaging test? He is on Amoxicillin and he continues with fever. Is this a reason to get a xray? Mom is demanding answers!
CASE 2A 20 month old female with an extensive past medical history (GERD with Nissen and G button, ASD, Coractation of the aorta, now repaired) presents to the ED with cough and congestion for 4 days. She was seen at an outside ED where an CBC was obtained that revealed a WBC of 13 with 66 segs and 18 lmphs; she had a normal CMP and a negative influenza test; the treating ED physician said an RSV test was negative but he “doesn’t believe it.” A chest xray was obtained and this showed pneumonia for which she was given a dose of Ceftriaxone. Today, she developed fever to 101.5 and increased work of breathing. There has been no vomiting or diarrhea.Her exam demonstrates a well-appearing child with respiratory distress. She has a temperature of 101.5 and a respiratory rate of 75, with moderate intercostal retractions and scattered bilateral rhonchi and wheezing, without crackles, grunting or stridor. Oxygen saturation is 93% on room air.The outside chest films were not sent and the ED from which the patient came is 4 hours away...great. Mom wants to know if her daughter does indeed have pneumonia and if so, what antibiotics should you continue? She also wants to know if admission is necessary. Should you repeat the film?
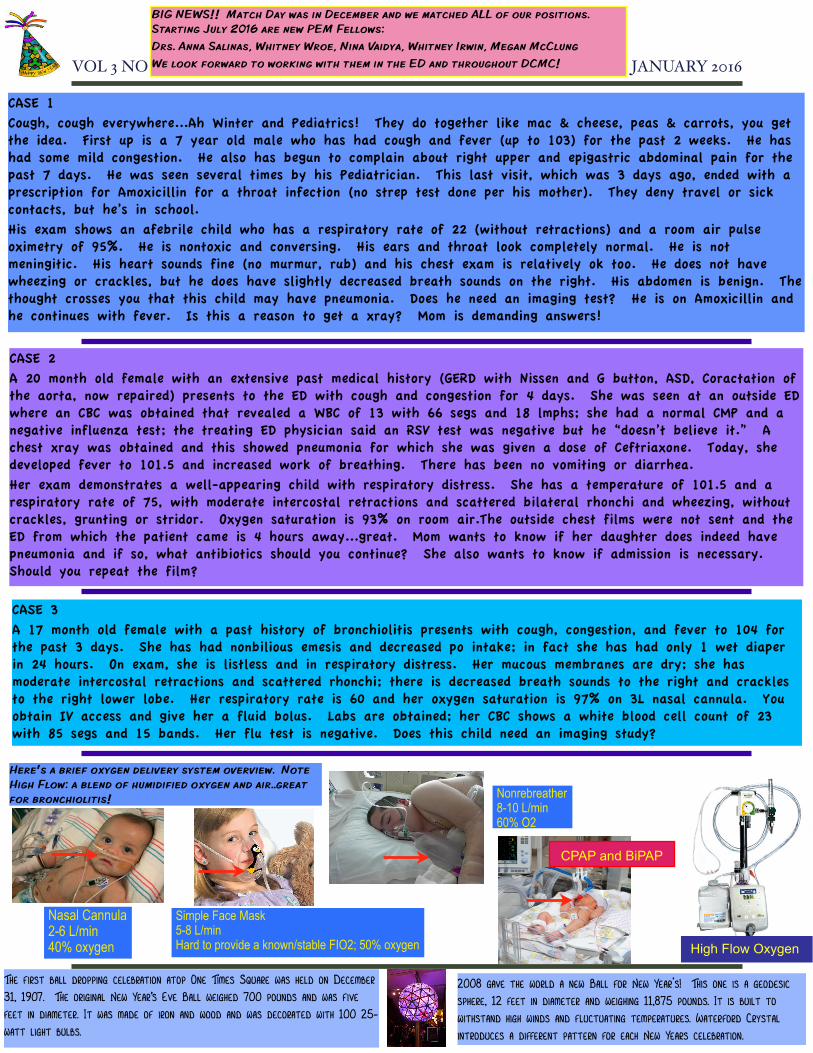
Nasal Cannula 2-6 L/min40% oxygen
Simple Face Mask5-8 L/minHard to provide a known/stable FIO2; 50% oxygen
Nonrebreather8-10 L/min60% O2
High Flow Oxygen
CPAP and BiPAP
Here’s a brief oxygen delivery system overview. Note High Flow: a blend of humidified oxygen and air..great for bronchiolitis!
VOL 3 NO 1 JANUARY 2016
PAGE 3
What’s with that cough? The differential diagnosis of cough in Pediatrics can be enormous, involving intrapulmonary and extrapulmonary disease. For the purposes of this month’s newsletter, we are going to focus on cough due to an infectious etiology. Always keep in mind, though, that cough sometimes is gastroesophageal reflux disease, a foreign body, an anatomic issue (vascular ring or sling), a mass...one could keep going.
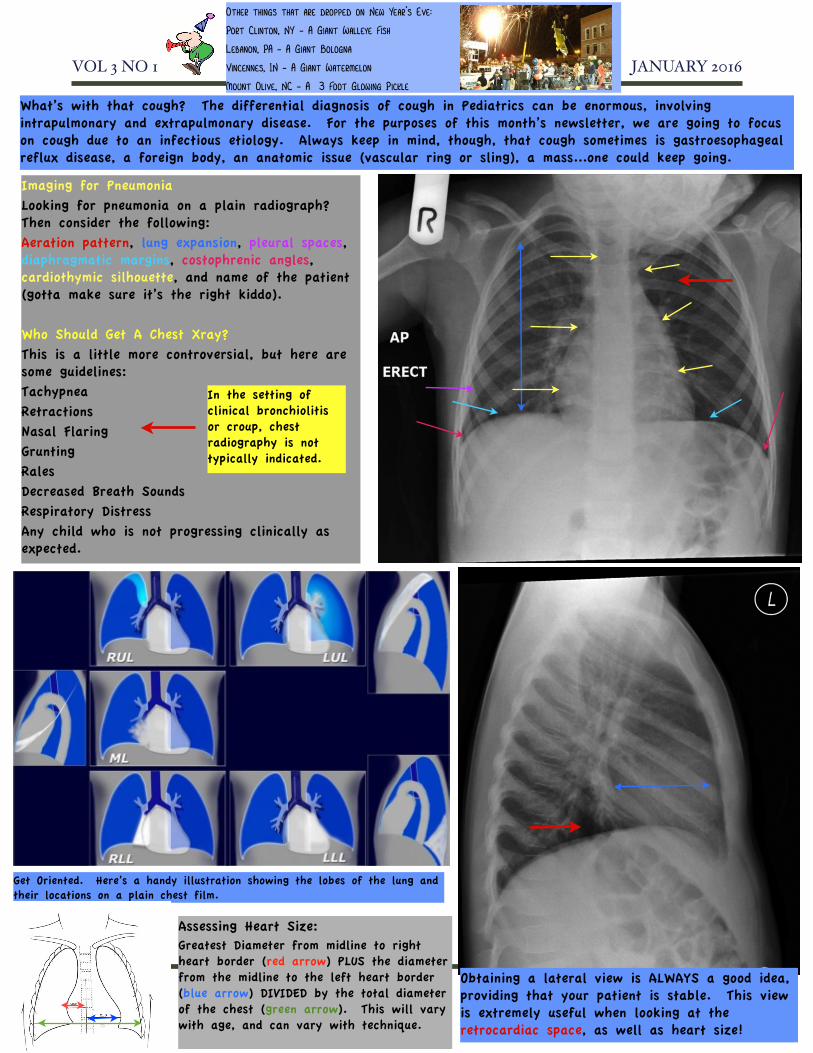
Imaging for PneumoniaLooking for pneumonia on a plain radiograph? Then consider the following:Aeration pattern, lung expansion, pleural spaces, diaphragmatic margins, costophrenic angles, cardiothymic silhouette, and name of the patient (gotta make sure it’s the right kiddo).
Who Should Get A Chest Xray?This is a little more controversial, but here are some guidelines:TachypneaRetractionsNasal FlaringGruntingRalesDecreased Breath SoundsRespiratory DistressAny child who is not progressing clinically as expected.
In the setting of clinical bronchiolitis or croup, chest radiography is not typically indicated.
Obtaining a lateral view is ALWAYS a good idea, providing that your patient is stable. This view is extremely useful when looking at the retrocardiac space, as well as heart size!
Get Oriented. Here’s a handy illustration showing the lobes of the lung and their locations on a plain chest film.
Assessing Heart Size:Greatest Diameter from midline to right heart border (red arrow) PLUS the diameter from the midline to the left heart border (blue arrow) DIVIDED by the total diameter of the chest (green arrow). This will vary with age, and can vary with technique.
Other things that are dropped on New Year’s Eve:
Port Clinton, NY - A Giant Walleye Fish
Lebanon, PA - A Giant Bologna
Vincennes, IN - A Giant Watermelon
Mount Olive, NC - A 3 Foot Glowing Pickle
VOL 3 NO 1 JANUARY 2016
PAGE 4
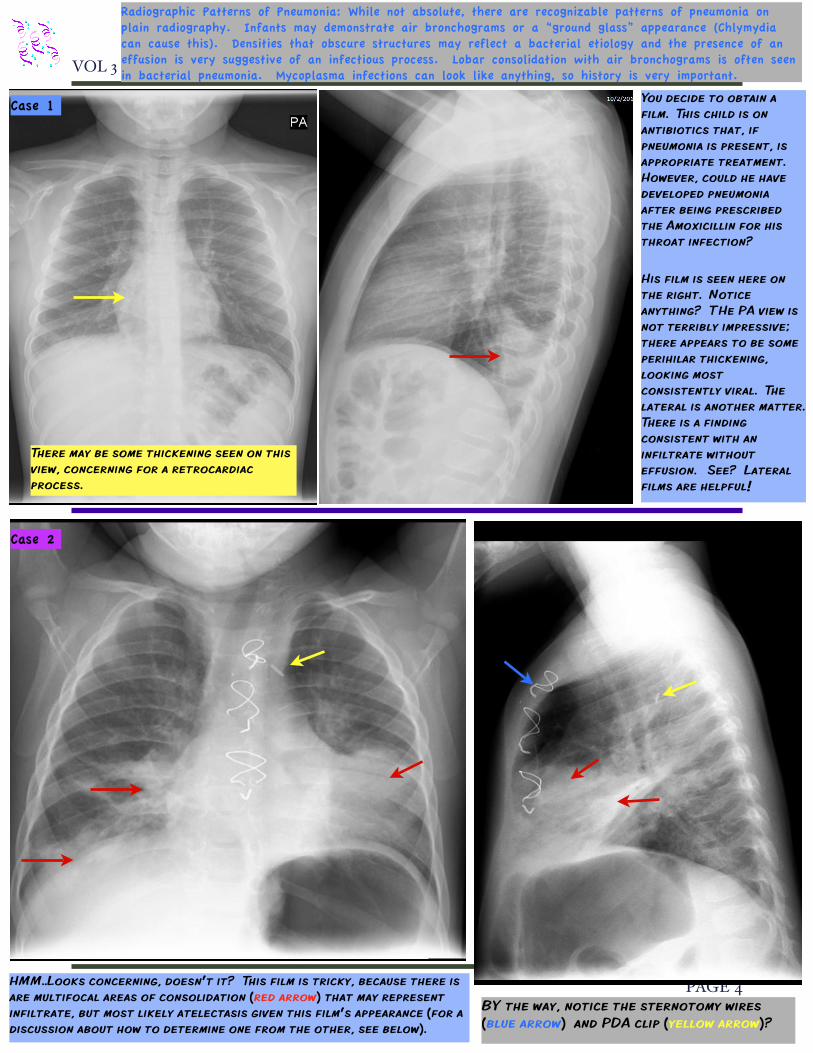
You decide to obtain a film. This child is on antibiotics that, if pneumonia is present, is appropriate treatment. However, could he have developed pneumonia after being prescribed the Amoxicillin for his throat infection?
His film is seen here on the right. Notice anything? THe PA view is not terribly impressive; there appears to be some perihilar thickening, looking most consistently viral. The lateral is another matter. There is a finding consistent with an infiltrate without effusion. See? Lateral films are helpful!
Case 1
There may be some thickening seen on this view, concerning for a retrocardiac process.
Case 2
HMM..Looks concerning, doesn’t it? This film is tricky, because there is are multifocal areas of consolidation (red arrow) that may represent infiltrate, but most likely atelectasis given this film’s appearance (for a discussion about how to determine one from the other, see below).
BY the way, notice the sternotomy wires (blue arrow) and PDA clip (yellow arrow)?
Radiographic Patterns of Pneumonia: While not absolute, there are recognizable patterns of pneumonia on plain radiography. Infants may demonstrate air bronchograms or a “ground glass” appearance (Chlymydia can cause this). Densities that obscure structures may reflect a bacterial etiology and the presence of an effusion is very suggestive of an infectious process. Lobar consolidation with air bronchograms is often seen in bacterial pneumonia. Mycoplasma infections can look like anything, so history is very important.
VOL 3 NO 1 JANUARY 2016
PAGE 5
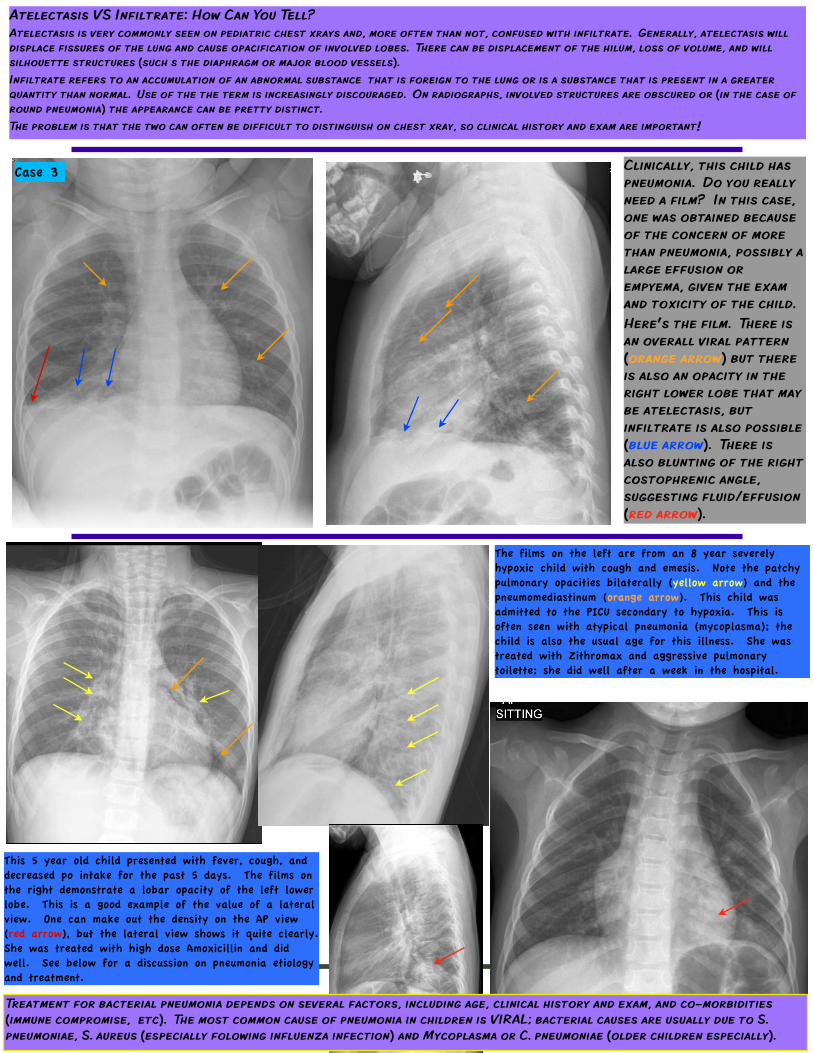
Atelectasis VS Infiltrate: How Can You Tell?Atelectasis is very commonly seen on pediatric chest xrays and, more often than not, confused with infiltrate. Generally, atelectasis will displace fissures of the lung and cause opacification of involved lobes. There can be displacement of the hilum, loss of volume, and will silhouette structures (such s the diaphragm or major blood vessels).Infiltrate refers to an accumulation of an abnormal substance that is foreign to the lung or is a substance that is present in a greater quantity than normal. Use of the the term is increasingly discouraged. On radiographs, involved structures are obscured or (in the case of round pneumonia) the appearance can be pretty distinct.The problem is that the two can often be difficult to distinguish on chest xray, so clinical history and exam are important!
Case 3 Clinically, this child has pneumonia. Do you really need a film? In this case, one was obtained because of the concern of more than pneumonia, possibly a large effusion or empyema, given the exam and toxicity of the child.Here’s the film. There is an overall viral pattern (orange arrow) but there is also an opacity in the right lower lobe that may be atelectasis, but infiltrate is also possible (blue arrow). There is also blunting of the right costophrenic angle, suggesting fluid/effusion (red arrow).
The films on the left are from an 8 year severely hypoxic child with cough and emesis. Note the patchy pulmonary opacities bilaterally (yellow arrow) and the pneumomediastinum (orange arrow). This child was admitted to the PICU secondary to hypoxia. This is often seen with atypical pneumonia (mycoplasma); the child is also the usual age for this illness. She was treated with Zithromax and aggressive pulmonary toilette; she did well after a week in the hospital.
This 5 year old child presented with fever, cough, and decreased po intake for the past 5 days. The films on the right demonstrate a lobar opacity of the left lower lobe. This is a good example of the value of a lateral view. One can make out the density on the AP view (red arrow), but the lateral view shows it quite clearly. She was treated with high dose Amoxicillin and did well. See below for a discussion on pneumonia etiology and treatment.
Treatment for bacterial pneumonia depends on several factors, including age, clinical history and exam, and co-morbidities (immune compromise, etc). The most common cause of pneumonia in children is VIRAL; bacterial causes are usually due to S. pneumoniae, S. aureus (especially folowing influenza infection) and Mycoplasma or C. pneumoniae (older children especially).
VOL 3 NO 1 JANUARY 2016
PAGE 6
Teaching Points1. Pneumonia in most children is a clinical diagnosis, supported by history and physical examination findings. Imaging is not indicated in all patients with
pneumonia.2. Plain radiography is typically sufficient for imaging children with pneumonia. Obtaining two views is ideal, especially to evaluate the retrocardiac space. 3. When suspecting emphyema or abscess, Ultrasound is a good first choice for evaluation, Ct may also be used. (See the JUNE 2015 issue for a more detailed
discussion of this).4. Most pneumonia in children is caused by viral infections. When bacterial infections are suspected, then the most common causes are S. pneumoniae, S. aureus,
and, especially in older children, M. pneumoniae and C. pneumoniae.5. Amoxicillin is the first ine antibiotic choice in children whom bacterial pneumonia is suspected. For complicated pneumonia/empyema, or when MRSA is
suspected, Clindamycin or Vancomycin are typically added. (See the DCMC PNeumonia and Complicated Pneumonia Pathway, available on the DCMC website).
References1. Shah S, Bachur R, Kim D, Neuman MI. Lack of predictive value of tachypnea in the diagnosis of pneumonia in children. Pediatr Infect Dis J. 2010 May. 29(5):406-9.2. Lynch T, Platt R, Gouin S, Larson C, Patenaude Y. Can we predict which children with clinically suspected pneumonia will have the presence of focal infiltrates on chest
radiographs?. Pediatrics. 2004 Mar. 113(3 Pt 1):e186-9.3. Murphy CG, van de Pol AC, Harper MB, Bachur RG. Clinical predictors of occult pneumonia in the febrile child. Acad Emerg Med. 2007 Mar. 14(3):243-9.4. Neuman MI, Kelley M, Harper MB, File TM Jr, Camargo CA Jr. Factors associated with antimicrobial resistance and mortality in pneumococcal bacteremia. J Emerg Med. 2007
May. 32(4):349-57.5. Williams DJ, Hall M, Shah SS, et al. Narrow Vs broad-spectrum antimicrobial therapy for children hospitalized with pneumonia. Pediatrics.
2013 Nov. 132(5):e1141-8.6. Mathews B, Shah S, Cleveland RH, Lee EY, Bachur RG, Neuman MI. Clinical predictors of pneumonia among children with wheezing. Pediatrics. 2009 Jul. 124(1):e29-36.7. Wahlgren H, Mortensson W, Eriksson M, Finkel Y, Forsgren M, Leinonen M. Radiological findings in children with acute pneumonia: age more important than infectious agent.
Acta Radiol. 2005 Jul. 46(4):431-6.
Case ResolutionsCase 1 - This child was treated for community acquired pneumonia. Because he had been on oral antibiotics (Amoxicillin is an appropriate first line choice for community acquired [pneumonia) and was not improving, he was given a dose of Ceftriaxone and oral antibiotics were changed to Omnicef (other considerations would have been Zithromax to cover for atypicals or Clindamycin to cover for Staph). He did well after that.Case 2 - While this films certainly looks concerning and the child was admitted to DCMC for observation, after chest therapy and pulmonary toilette, the child clinically improved. She developed wheezing while in the hospital and had supportive care for clinical bronchiolitis. Antibiotics were not continued and after 2 days, she was discharged home.Case 3 - This child was admitted to the hospital; antibiotics were continued for pneumonia and supportive care (IV fluids) was also continued. She did well after 3 days and was able to be discharged home, completing a course of Amoxicillin.
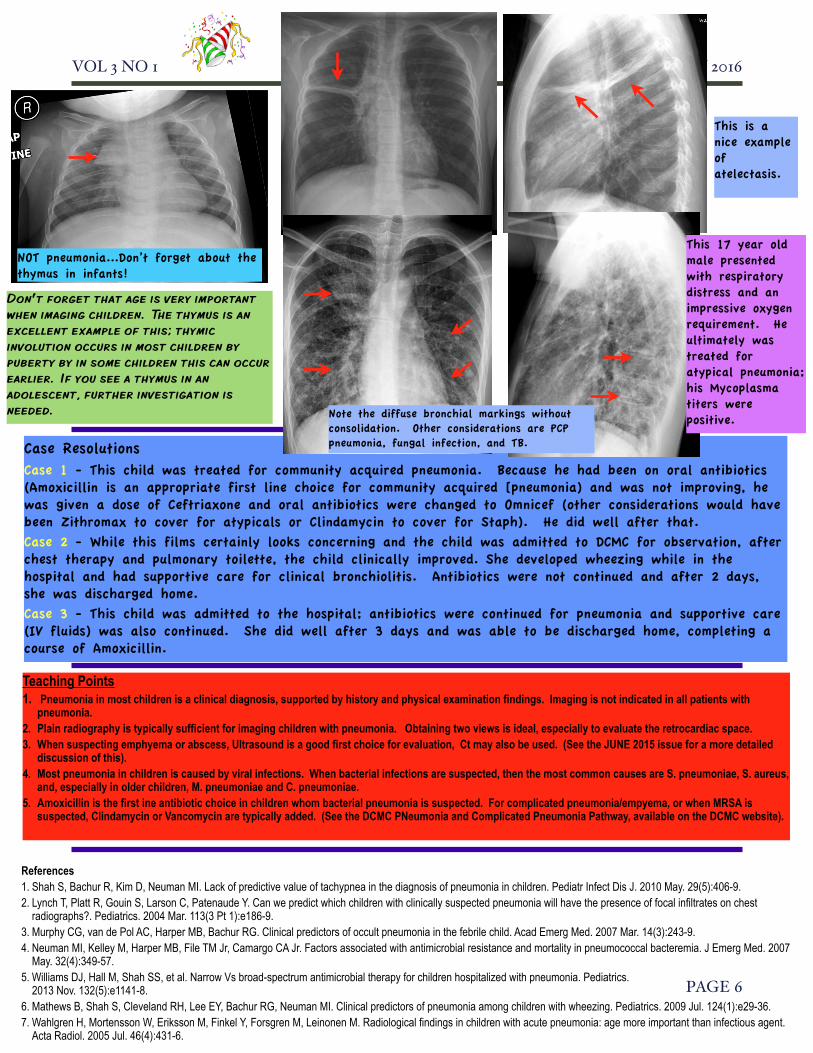
NOT pneumonia...Don’t forget about the thymus in infants!
This is a nice example of atelectasis.
Don’t forget that age is very important when imaging children. The thymus is an excellent example of this; thymic involution occurs in most children by puberty by in some children this can occur earlier. If you see a thymus in an adolescent, further investigation is needed.
This 17 year old male presented with respiratory distress and an impressive oxygen requirement. He ultimately was treated for atypical pneumonia; his Mycoplasma titers were positive.Note the diffuse bronchial markings without
consolidation. Other considerations are PCP pneumonia, fungal infection, and TB.