Embed Size (px)
Citation preview

American Journal of Pathology, Vol. 127, No. 3, June 1987Copyright i American Association of Pathologists
Enhancement of Chronic Trypanosoma cruziMyocarditis in Dogs Treated With LowDoses of Cyclophosphamide
ZILTON A. ANDRADE, MD,SONIA G. ANDRADE, MD,
and MOYSES SADIGURSKY, MD
An enhancement ofchronic myocarditis was obtainedin dogs chronically infected with Trypanosoma cruziprotozoa soon after they were submitted to treatmentwith low doses of cyclophosphamide (50 mg/sq m bsthree times a week for 3 weeks). Such treatment did notcause immunodepression. Myocarditis varied in inten-sity, but was quite severe and diffuse in some animals,with focal fibrinoid, coagulative, and lytic necrosis andinvasion of disintegrating myocardial fibers by the
MOST SUBJECTS infected with Trypanosomacruzi, the protozoon causing Chagas' disease, areasymptomatic. They may remain so for prolongedperiods, usually from 5 to 30 years. In about 30% ofthem will eventually develop the picture of progres-sive cardiac failure due to a chronic diffuse myocar-ditis that is thought to develop from a delayed hyper-sensitivity reaction to parasite-related antigens" 2 or toautoimmunity.3'4 The reason for the prolonged pe-riod of latent infection is unknown.The experimental approach to study of this prob-
lem depends on the identification ofa suitable model.So far only in the dog has it been possible to observethe spontaneous development of congestive cardiacfailure, with cardiomegaly, arrhythmias, and diffusemyocarditis after a prolonged period of chronicasymptomatic T cruzi infection.5-7 However, the rar-ity and unexpectedness with which diffuse progressivemyocarditis spontaneously develops in chronically Tcruzi-infected dogs represents a limitation to the utili-zation of such a model.8
In this present study we observed the regular devel-opment of severe myocarditis in dogs with chronic,apparently latent, T cruzi infection after they weretreated with low doses of cyclophosphamide.
From Centro de Pesquisas Gon(alo Moniz, Bahia, Brazil
mononuclear inflammatory cells. Untreated infectedcontrols exhibited mild focal myocarditis, usually rep-resented by accumulation oflymphocytes in the inter-stitial connective tissue. It is suggested that the admin-istration oflow doses of cyclophosphamide interferedwith the immunologic suppressor network that isthought to maintain the chronic indeterminate (or la-tent) phase of T cruzi infection. (Am J Pathol 1987,127:467-473)
It has been claimed that low doses of cyclophos-phamide may exacerbate cell-mediated lesions, prob-ably by selectively destroying suppressor T lympho-cytes, their precursor cells, or other elements in thehost-immune suppressor network.9-'2
Materials and Methods
Twenty-one young (2-3 months old) mongrel dogsof both sexes were used in the experiments. Infectionwas accomplished by means ofblood forms of Tcruzitaken from infected mice. These were outbred Swissmice, infected intraperitoneally with 1 X 105 trypo-mastigotes of the 12SF and Colombian strains of Tcruzi, which have been maintained by serial passagein mice (see Andrade et al'3 for details on strain char-acterization). Mice were bled at the height ofparasite-
Supported by the Brazilian Scientific Council (CNPq)PIDE VI (Grant 40.0631/85).Accepted for publication January 22, 1987.Address reprint requests to Zilton A. Andrade, MD, Cen-
tro de Pesquisas Gonqalo Moniz, Rua Valdemar Falcao,121 (Brotas), 41 930 Salvador, Bahia, Brazil.
467

468 ANDRADE ET AL
mia, and the citrated blood was collected from theaxillary plexus. Trypomastigotes were counted bymeans of Brener's method.'4 Inocula were adjustedaccording to the weight of the animals, and the infec-tion ofthe dogs was done by the intraperitoneal route.The different sets of experiments are listed below.The ten dogs from the first two experiments had
been infected and/or vaccinated with T cruzi andwere under observation for more or less prolongedperiods, showing no apparent external signs of dis-ease, with normal electrocardiograms and negativeparasitemia, when it was decided to subject them totreatment with cyclophosphamide.
1. In 6 of those dogs infected with T cruzi trypo-mastigotes, acute infection (posite parasitemia) devel-oped 16 to 30 days after inoculation, but the dogsrecovered after 2-4 weeks, when the electrocardio-graphic changes returned to normal and trypomasti-gotes could not be found by direct examination ofperipheral blood (Table 1). One ofthe dogs developedsevere disease during the acute phase of the infectionand had to be treated with nitroimidazole and corti-coids as previously described.'5
2. Four dogs were vaccinated with a living non-replicating vaccine'6 given three times subcutane-ously, in 10-day intervals. Each dose, administered in1 ml, contained 1 X 108 epimastigotes. Two of thesevaccinated animals were challenged 1 week after thelast immunizing dose with 60,000 and 82,000 bloodtrypomastigotes, respectively, given intraperitone-ally. The two other dogs were not infected and re-mained as vaccine controls (Table 2), although theywere also treated with cyclophosphamide later on.
3. Five dogs were used in another similar experi-ment. They were likewise infected as the previous 6dogs were, developed acute infection, and were ob-served until they reached the chronic stage of the in-fection. Then 3 dogs were treated with low-dose cy-clophosphamide under the same schedule as theothers, and 2 were left as untreated controls. To evalu-ate the type and degree of myocarditis in these ani-mals, we coded the microscopical slides and the three
pathologists who examined them separately did notknow to which group the slides belonged (Table 3).
4. From the files of the Department the slides con-taining heart tissue from 5 dogs which had been in-fected but not treated with cyclophosphamide wereexamined for illustration of the type of myocarditiswhich is usually found in dogs cronically infected withT cruzi (Table 4). These cases were selected becausethe duration of infection was comparable to that ofthe other experiments; the T cruzi strains used werealso the same.
Sera were obtained prior to inoculation and at dif-ferent time intervals thereafter. The presence of anti-T cruzi antibodies were detected by immunofluores-cence, according to Camargo's methods. 17
Classic 12-lead electrocardiograms (ECGs) weretaken with the dogs under light anesthesia with Nem-butal. The ECGs were taken before inoculation,weekly during the acute phase, and at various inter-vals (at least monthly) during the chronic phase oftheinfection. A single-channel electrocardiograph wasused, with small metal needles for subcutaneousplacement instead of the usual electrodes.Cyclophosphamide (Enduxan, Pravaz-Abbott
Laboratories, Brazil, Ltd.) was administered intra-peritoneally in the dose of 50 mg/sq m of body sur-face, three times a week, for 3 weeks. The dose wascalculated to be comparable with that utilized by Col-ley et al '0 for the mouse. Four days after the last injec-tion ofcyclophosphamide, all the animals were killedand submitted to autopsy. All the organs were exam-ined except for the central nervous system. Fragmentsofthe organs were fixed in 10% buffered formalin andembedded in paraffin, and the sections stained withhematoxylin and eosin (H&E). The entire heart wasfixed for the proper examination of the sinus node byHudson's technique'8 and the atrioventricular con-ducting system by Lev's method.'9
In addition to the routine H&E, the heart sectionswere stained by the Masson's trichrome, periodicacid-Schiff (PAS), and Picro-Syrius red methods forcollagen.20
Table 1 -Data on Young Dogs Infected With T cruzi and Treated During the Chronic Stage of the InfectionWith Low-Dose Cyclophosphamide (Cy)
Dog
23456
T cruzistrain
ColombianColombianColombianColombian
12 SF12 SF
Number ofparasites
in inoculum
5 X 1045 X 1045 X 1045X 1045 X 104
82 X 103
Duration ofinfection(days)
338338338186122122
Antibody titerafter Cy
1:12801:12801:12801:25601:61201:2560
Myocarditis
Focal Diffuse
+
+++
++++
AJP * June 1987

CYCLOPHOSPHAMIDE AND CHAGAS' MYOCARDITIS 469
Table 2 Data on Dogs Vaccinated Against T cruzi, Challenged or Not, and Treated With Low-Dose Cyclophosphamide (Cy)
Dog
8
910
Status
Vaccinated andchallenged
Vaccinated andchallenged
Vaccinated onlyVaccinated only
Strain
12 SF
12 SF
Inoculum
6 x 104
82 X 103
Duration ofinfection orvaccination
(days)
122
122122122
Antibodytiter
after Cy
Myocarditis
Focal Diffuse
1:5120
1:25601:12801:640
00
00
Results
General Data
General clinical, immunologic, and parasitologicdata appear in Tables 1, 2, 3, and 4.
Electrocardiographic Findings
During the acute phase ofthe infection, the electro-cardiograms disclosed some alterations in most oftheanimals. These ranged from sinus bradycardia, inver-sion of T waves, and irregularities in the S-T seg-ments, to premature beats and right bundle branchblock. After resolution of the parasitemia, the ECGabnormalities gradually disappeared, and during thestabilized chronic stage repeated ECGs were withinnormal limits. Four days after the last injection ofcyclophosphamide the treated animals were foundagain to have some mild ECG changes, such as alter-ations in the S-T segments, increased P-R intervals,sinus arrhythmias, and one instance of intraventricu-lar conduction defect.
Pathologic Findings
Gross findings at autopsy were not remarkable, ex-cept for moderate dilatation of the right chambers ofthe heart in a few animals.
Table 3 -Data on 5 Dogs All Infected at the Same Time With12 SF Strain of T cruzi*
T cruzi antibody titers Myocarditis
Dog Cy treatment before Cy After Cy Focal Diffuse
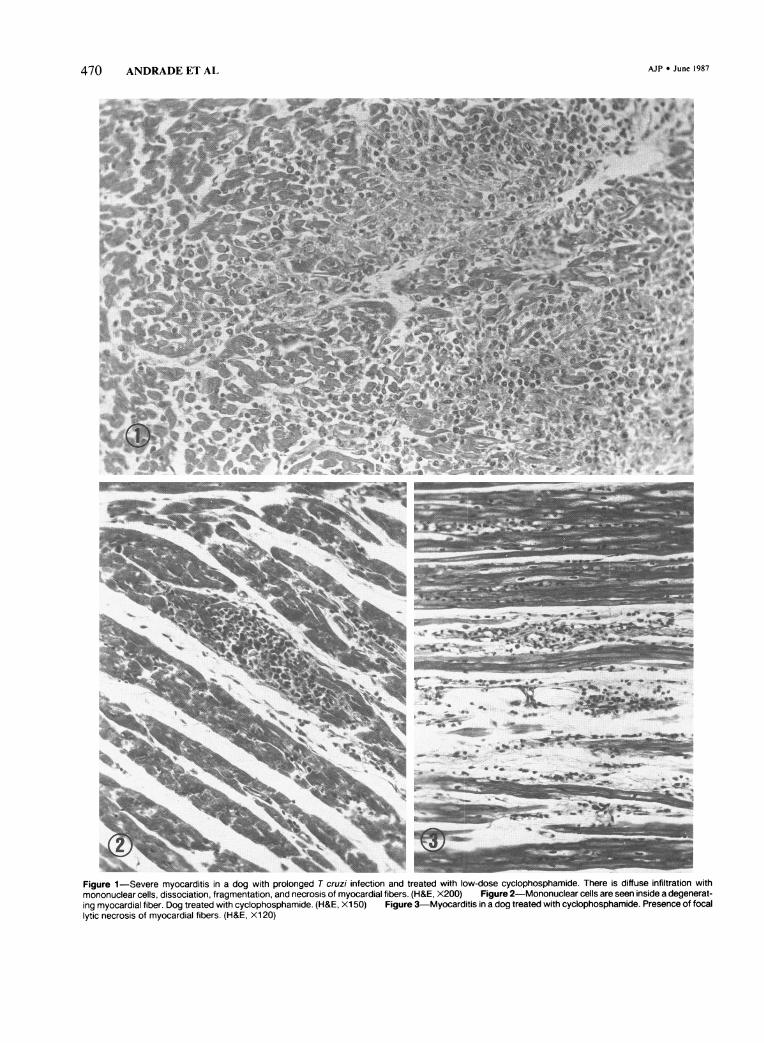
Microscopically, the main changes were limited tothe heart. All the infected animals exhibited variabledegrees of chronic myocarditis. In the first experi-ment, those animals treated with cyclophosphamideshowed marked myocardial inflammation, with focalnecrosis of myocardial fibers (Figure 1). A focal anddiffuse infiltration of macrophages, lymphocytes, andplasmocytes dissociated the myocardial fibers and ex-tended to the endocardium and to the epicardial fi-broadipose tissue. Sometimes the mononuclear in-flammatory cells seemed to be invading, destroying,and replacing the myocardial fibers (Figure 2). Withinareas where the inflammation became more accen-tuated, it was not uncommon to observe fibrinoid,coagulative, and/or lytic necrosis of the myocardialfibers, usually followed by collapse of the connectivetissue framework (Figure 3). Throughout the myocar-dium there were patchy areas of interstitial edema andfibrosis, especially around the vessels. No overt vascu-lar involvement was detected. The sinus node and theatrioventricular conducting tissues were likewise in-volved (Figure 4). The inflammation was more severeat the right atrial walls and reached the autonomicnervous ganglia and other nervous structures in theproximity ofthe sinus-atrial node. The His main bun-dle and its right and left branches were infiltrated bymononuclear inflammatory cells, but its continuitywas maintained.No parasites could be detected within the cardiac
fibers, even after a thorough search. Extracardiacchanges were not remarkable.
Table 4-Data on 5 Young Dogs Infected With T cruzi andKilled During the Chronic Stage of the Infection
1112131415
YesYesYesNoNo
1:3201:1601:1601:3201:640
1:3201: 801:3201:1601:320
++ ++±++ ±++++ 0
+
*At the chronic stage of the infection 3 dogs were treated with low doses ofcyclophosphamide (Cy), and 2 were left untreated. The animals were sacri-ficed 4 days after the last Cy infection.
Inoculum: 1 X 105 parasites per kilogram body weight. Duration of infec-tion: 213 days.
T cruziDog strain
161718192021
12 SF12 SF12 SF
ColombianColombianColombian
Duration ofinfection
Inoculum (days)
5 X 1045 X 1046 X 1 041 X 1061 X 1061 X 106
42542594
274274274
Myocarditis
Focal Diffuse
±+±+±+
000000
Vol. 127 * No. 3
470 ANDRADE ET AL
_~~~~~~~~~~~~~~~~~~~~~VC
Siab'_S5~t2 * _I4- %? Jmt.w
_XNt-M' '
Figure 1-Severe myocarditis in a dog with prolonged T cruzi infection and treated with low-dose cyclophosphamide. There is diffuse infiltration withmononuclear cells, dissociation, fragmentation, and necrosis of myocardial fibers. (H&E, X200) Figure 2-Mononuclear cells are seen inside a degenerat-ing myocardial fiber. Dog treated with cyclophosphamide. (H&E, Xl 50) Figure 3-Myocarditis in a dog treated with cyclophosphamide. Presence of focallytic necrosis of myocardial fibers. (H&E, Xl 20)
AJP * June 1987

CYCLOPHOSPHAMIDE AND CHAGAS' MYOCARDITIS 471
Figure 4-Severe myocarditis involving the His main bundle in a T cruzi-infected dog treated with cyclophosphamide. There are inflammatory mononuclearcells, edema, and "dropping-out" of isolated conducting fibers. (Masson's trichrome, X200) Figure 5-Representative section from the heart of a dogtreated with cyclophosphamide and showing only a moderate degree of myocarditis. The diffuse inflammatory infiltrate and the lytic necrosis of isolatedmyocardial fibers were taken as signs of activity of the myocarditis. (H&E, Xl 50) Figure 6-Control T cruzi-infected and untreated dog. There is anaccumulation of lymphocytes in the interstitium of the myocardium, which otherwise appears normal. (H&E, Xl 50)
Vol. 127 * No. 3
iI

472 ANDRADE ET AL
In the second experiment, the two vaccinated andchallenged animals exhibited severe myocarditis,which did not differ from that described above. Thetwo vaccinated but not challenged dogs did notpresent any heart changes.
In the third experiment, the myocarditis observedin the three treated dogs was less intense than thatdescribed above. It was, however, more marked anddiffuse than the mild focal myocarditis found in thetwo untreated dogs. In addition, the mononuclear in-filtration in the treated animals exhibited signs of ac-tivity not found in those untreated. These consisted ofthe presence offocal necrosis ofmyocardial fibers andinvasion of the fibers by inflammatory cells (Figure5). By looking at the heart sections, three observerswere independently able to separate the slides fromcyclophosphamide-treated dogs from those un-treated.The sections from the hearts of dogs killed during
the chronic stage of the infection and which weretaken from the files and examined, showed a uni-form microscopic picture of mild focal myocarditis.The focal infiltrates tended to be predominantly lym-phocytic and to accumulate in the interstitial tissuerather than to involve the myocardial fibers (Fig-ure 6).
In none ofthe animals included in the present studydid congestive cardiac failure develop at any timeduring the experiments.
DiscussionThe administration of repeated low doses of cyclo-
phosphamide was seen to cause an exacerbation ofthe usually mild myocarditis found in dogs chroni-cally infected with T cruzi. The extraordinary find-ings of the first two experiments here described couldnot be entirely duplicated in the third one. However,the independent assessment by three different exam-iners did agree that the treated animals disclosed amore intense myocarditis, which showed unequivo-cal signs of activity.
In the recent past we have examined several dogswith chronic T cruzi infection,8"2 and only once7 wasit possible to see the spontaneous development of achronic active myocarditis, such as has been de-scribed by others.5'6 Generally our animals have re-mained in the chronic latent (indeterminate) form ofthe disease, with only a mild residual myocarditis, asdescribed by Goble.22We did not determine why cyclophosphamide en-
hanced the Tcruzi myocarditis in dogs. Apparently, itdid not cause T cruzi-specific immunodepression.The antibody titers remained elevated, and no evi-
dence ofexaggerated parasite multiplication could beobserved. At least the extensive and severe myocar-ditis found in cyclophosphamide-treated dogs couldnot be directly correlated with T cruzi multiplicationwhen the tissue sections from the heart were exam-ined. However, when T cruzi chronically infecteddogs are treated with large doses of immunosup-pressive drugs, the acute infection reappears, with nu-merous trypomastigotes directly demonstrated in theperipheral blood.23On the other hand, it has been shown that asympto-
matic T cruzi-infected individuals may develop spe-cific as well as autoimmune antibodies and sensitizedimmunologically competent cells.24 It has beenclaimed that these cells can adhere to and destroycardiac cells in vitro.3'25 Therefore, it is possible that asuppressed immunologically mediated destructive re-action against the cardiac tissue, which is suppressedduring the indeterminate period ofthe infection, maybe triggered during chronic progressive Chagas' myo-carditis.
Experimental data from the literature are contro-versial regarding a specific immunologic suppressionofthe Tcruzi-induced lesions.26'27 It has been demon-strated that a specific suppression of delayed hyper-sensitivity to Tcruzi antigens, but not to an unrelatedantigen, occurs in mice chronically infected with theparasite.28 Further studies on chronic T cruzi mouseinfection have also shown a persistent suppression ofresponses by immunoglobulin G antibody, which ismediated by suppressor T lymphocytes.29
Studies along these lines in the dog are highly desir-able, because the cardiac form of Chagas' disease,with diffuse myocarditis, cardiomegaly, arrhythmias,and progressive heart failure, has so far been experi-mentally obtained only in dogs. Similar to what hasbeen observed in human Chagas' disease," 24 in thedog treated with low-dose cyclophosphamide, activemyocarditis occurs without any indication ofinterfer-ence with the established partial immunity against theparasite, which is present during the chronic latentform.An interesting collateral observation was made
with the vaccinated animals. In the first experimentwe decided to give cyclophosphamide to all the dogswe had at the moment under observation and whichhad presented prolonged T cruzi infection withoutany external signs of disease. Among them there were4 dogs which had been submitted to vaccination. Thevaccine did prove efficient in avoiding the develop-ment of acute disease when the animals were chal-lenged with virulent T cruzi, although it did notprevent the development ofchronic infection. Cyclo-phosphamide treatment indicated that the vaccine
AJP * June 1987
Vol. 127 * No. 3 CYCLOPHOSPHAMIDE AND CHAGAS' MYOCARDITIS 473
did not protect against the development of chronicdisease. On the other hand, although the living vac-cine by itself induced specific antibody response, itdid not cause infection, nor did it seem to sensitize theheart tissue for a hypersensitivity reaction in the non-challenged dogs, despite the fact that they also re-ceived cyclophosphamide treatment. Although theseobservations were made on a rather small number ofanimals and say nothing about the efficacy of thevaccine used, they suggest that future studies may beuseful to clarify whether the administration of lowdoses ofcyclophosphamide may be ofhelp in indicat-ing whether a given experimental vaccine is prone tocause autoimmunity or other delayed type hypersen-sitivity reactions.The results observed in the present study justify
further attempts with the canine model to investigateproblems related to the immunopathology and path-ogenesis of Chagas' disease.
References1. Andrade ZA: Mechanisms of mvocardial damage in
Trvpanosoma cruditz infection, Cytopathology of Para-sitic disease. London, Pitman Books (Ciba FoundationSvmposium 99), 1983. pp 214-233
2. Teixeira ARL, Santos-Buch CA: The immunology ofexperimental Chagas' disease: II. Delayed hypersensi-tivity to Trvpanosoma cruzi antigens. Immunology1975. 28:401-410
3. Santos-Buch CA, Teixeira ARL: The immunology ofexperimental Chagas' disease: III. Rejection ofallogen-eic heart cells in vitro. J Exp Med 1974, 140:38-53
4. Sadigursky M. Acosta AM, Santos-Buch CA: Musclesarcoplasmic reticulum antigen shared by a Tr pano-somna criEzi clone. Am J Trop Med Hyg 1982, 31:934-941
5. Anselmi A, Pifano FC, Suarez JA. Gurdiel 0: Myocar-diopathy in Chagas' disease: Comparative studv ofpathologic findings in chronic human and expenmen-tal Chagas' mvocarditis. Am Heart J 1966. 72:469-481
6. Laranja FS. Pellegrino J. Dias E: Experimental Chagas'disease (Abstr). Am Heart J 1949. 4:646
7. Laranja FS. Andrade ZA: Forma cr6nica cardiaca dadoenVa de Chagas no cao. Arq Bras Cardiol 1980.35:377-380
8. Andrade ZA: The canine model of Chagas' disease.Mem Inst Oswaldo Cruz 1984. 79:77-83
9. Liew FY, Russell SM: Inhibition ofpathogenic effect ofeffector T cells by specific suppressor T cells duringinfluenza virus infection in mice. Nature 1983,304:541-543
10. Colley DG. Lewis FA. Todd CW: Adoptive suppres-sion ofgranuloma formation by T lymphocytes and bylymphoid cells sensitive to cyclophosphamide. Cell Im-munol 1979. 46:192-200
11. Schwartz A. Askenase PW, Gershon, RK: Regulationof delayed-type hypersensitivity reactions by cyclo-phosphamide sensitive T cells. J Immunol 1978.121:1573-1577
12. Turk JL, Parker D, Poulter IW: Functional aspects ofthe selective depletion of lymphoid tissue by cyclo-phosphamide. Immunology 1972, 23:493-501
13. Andrade VG, Brodskyn C, Andrade SG: Correlationbetween isoenzyme patterns and biological behaviourof different strains of Trypanosoma cruzi. Trans R SocTrop Med Hyg 1983, 77:796-799
14. Brener Z: Therapeutic activity criterion ofcure on miceexperimentally infected with Trypanosoma cruzi. RevInst Med Trop Sao Paulo 1962, 4:389
15. Andrade SG, Andrade ZA, Sadigursky M: Combinedtreatment with a nitrofuranic and a corticoid in experi-mental Chagas' disease in the dogs. Am J Trop MedHyg 1980, 29:766-773
16. Enders B, Weinmann E, Nagle CA, Hein B, Zwisler 0:Experimental Chagas' disease in primates Macaca fa-sciciularis and Cebuis apella with special reference topreclinical trials and the evaluation of a living non rep-licating T. cruczi vaccine. Behring Inst Mitt 1982,71:132-156
17. Camargo ME: Fluorescent antibody test for the diag-nosis of American trypanosomiasis: Technical modifi-cation employing preserved culture forms of Trypano-soina crliui in slide test. Rev Inst Med Trop Sao Paulo1966, 8:227-234
18. Hudson REB: The human pacemaker and its pathol-ogy. Br Heart J 1960, 22:153-167
19. Lev M: The normal anatomy ofthe conduction systemin man and its pathology in atrioventricular block. AnnNY Acd Sci 1964, 3:817-829
20. Junqueira LCU, Bignolas G, Brentani R: Picrosiriusstaining plus polarization microscopy, a specificmethod for collagen detection in tissue sections. Histo-chemJ 1979, 11:447-455
21. Andrade ZA, Andrade SG, Sadigursky M: Damage andhealing in the conducting tissue ofthe heart: An experi-mental study in dogs infected with Trvpanosoma crulzi.J Pathol 1984, 143:93-101
22. Goble FC: Observations on experimental Chagas' dis-ease in dogs. Am J Trop Med Hyg 1952, 1:189-204
23. Camargo ME, Kloetzel J, Bachella F: A note on theharvesting of large number of Tripanosoma cruiziblood forms in adult dogs. Rev Inst Med Trop SaoPaulo, 12:217-220
24. Brener Z: Immunity to Trvpanosoma cruizi. Adv Para-sitol 1980. 18:247-292
25. Montufar OMB, Musatti CC, Mendes E, Mendes NF:Cellular immunity in chronic Chagas' disease. J ClinMicrobiol 1977, 5:401-404
26. Hayes MM, Kierszenbaum F: Experimental Chagas'disease: Kinetics of lymphocyte responses and immu-nological control of the transition from acute tochronic Trvpanosoina cruzi infection. Infect Immun1981. 31:1 i 17-1124
27. Ramos CD, Schadtler-Siwon I, Ortiz-Ortiz L: Suppres-sor cells present in the spleen of Trvpanosoma cru--iinfected mice. J Immunol 1979, 122:1243-1247
28. Scott MT: Delayed hypersensitivity to Trypanosomnacriuzi in mice: specific suppressor cells in chronic in-fection. Immunology 1981, 44:409-417
29. Reed SG, Inverso JA, Roters SB: Heterologous anti-body responses in mice with chronic Tcruz-i infection:Depressed T helper function restored with superna-tants containing interleukin. J Immunol 1984,133:1558-1563
AcknowledgmentsThanks are due to Drs. B. Enders, 0. Zwissler, and Mr. K.
Wiegand, of the Behring Institute, Marburg, Germany, fortheir help with the Tcruzi vaccine utilized in this investiga-tion.
























![[Herch Moyses Nussenzveig] Curso de Fisica Basica(BookFi.org)](https://img.pdfslide.net/doc/110x75/55cf9b04550346d033a465d7/herch-moyses-nussenzveig-curso-de-fisica-basicabookfiorg.jpg)




