Embed Size (px)
Citation preview

Journal of Clinical InvestigationVol. 41, No. 1, 1962
STUDIES ON THE FIRST DERIVATIVE OF THE VENTRICULARPRESSUREPULSE IN MAN
By WILLIAM L. GLEASONAND EUGENEBRAUNWALD
(From the Cardiology Branch, National Heart Institute, Bethesda, Md.)
(Submitted for publication August 5, 1961; accepted September 14, 1961)
The rate at which the ventricular pressure riseshas been of interest to investigators for manyyears (1, 2). Wiggers demonstrated that whenventricular end-diastolic filling pressure was ele-vated by increasing the venous return to the heartor the resistance to ventricular ejection, the rateof rise of ventricular pressure also increased (3).When epinephrine (4) or digitalis (5) was ad-ministered the rate of pressure rise increased de-spite a fall in ventricular end-diastolic pressure.Conversely, when myocardial ischemia was induced,the slope of the ventricular pressure rise decreasedin the face of a rising end-diastolic pressure (6).More recently, although further observations havebeen made in the dog on the determinants of theslope of the ventricular pressure pulse (7-11),there have been no systematic studies of the effectsof physiologic stresses, pharmacologic agents, andvarious types of heart disease on the slope of theventricular pressure pulse in man.
Accurate determinations of the instantaneousrate of ventricular pressure change in intact hu-man subjects have been prevented by the technicallimitations imposed by the pressure-recordingsystems that are usually employed in cardiaccatheterization. These systems, which consist ofa fluid-filled catheter and an external manometer,have a very limited range in which the frequencyresponse is uniform (usually to less than 15 cy-cles per second) and they are subject to frequentartifacts related to motion of the catheter withinthe heart. Such artifacts may be manifest as sud-den changes in pressure and will therefore begreatly exaggerated when their first derivative iscomputed. These difficulties have been largelyeliminated by obtaining the ventricular pressuretracings with a catheter that has a high-frequencymicromanometer mounted at its tip, or by directneedle puncture of the ventricle.
METHODS
Percutaneous puncture of the left ventricle was carriedout by the method of Brock, Milstein and Ross (12) as
modified in this laboratory (13). All such tracings wereobtained with a 3.5-inch no. 19 or 20 gage thin-walledneedle attached directly to a Statham P23D pressuretransducer without intervening tubing. All other studiesfrom either the left or right ventricle were carried outwith a Telco intracardiac manometer 1 (14, 15). Thisinstrument consists of a double-lumen catheter, one lu-men of which carries the electrical connection to themicromanometer mounted at the tip, the other serving asa conventional fluid-filled catheter system which is at-tached to a Statham P23D manometer. The sensitivitiesof the micromanometer and the external manometer wereequalized with an air-pressure calibrating system prior tothe introduction of the catheter into the heart. Thecatheter tip was placed in the right or left ventricle andsimultaneous pressure pulses were recorded from thetwo manometers. The baseline for the micromanometerwas made equal to that of the external manometer bysuperimposing the diastolic portions of the two ventricu-lar pressure pulses.
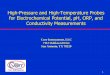
The frequency responses of the micromanometer andof the needle directly attached to the strain gage wereanalyzed in a fluid-filled chamber in which a sinusoidalpressure wave of variable frequency was generated. Thepressure produced was monitored by a Lilly capacitancemanometer built directly into the chamber. Figure 1illustrates a comparison of the pressures recorded simul-taneously from the fluid-filled lumen of the Telco catheter,using a Statham P23D strain gage as the external ma-nometer, the Lilly manometer, and the Telco micro-manometer. It is apparent that, while the response ofthe conventional external manometer system resonates at7 cycles per second (c/sec) and becomes significantly at-tenuated at frequencies above 10 c/sec, the micromanom-eter maintains an almost uniform response, indistinguish-able from the Lilly manometer, to frequencies as high as200 c/sec. With an identical method for comparison itwas observed that the needle attached to the P23D gagemaintained a uniform response to a frequency of 40 c/sec.
The rate of change of the ventricular pressure pulses(dp/dt) was continuously determined with an R-C dif-ferentiating circuit, consisting of a 47 kilo-ohm resistorand a 0.002 microfarad condenser as outlined elsewhere(16). The time constant of this circuit is 9.4 X 10' sec-ond, and it provides differentiation of linear amplitudewithout phase distortion to 50 c/sec. The differentiatingcircuit was calibrated by imposing a signal of constantand known slope from an integrating amplifier and meas-uring the resulting response of the differentiator.
1 Telco, Inc., Gentilly, France. Distributed in theU.S.A. by Dallons Laboratory, Inc., Los Angeles, Calif.
80

FIRST DERIVATIVE OF VENTRICULARPRESSURE
FREQUENCYCYCLES/SEC.
EXTERNAL
MANOMETER
LILLY
MANOMETER
TELCO
MANOMETER
1 4 7 10 14 20 30 100 200
III! i2i~iii. rn*- _-....
11111!!m v v :iAI1 1iiiiybil~l-
FIG. 1. SIMULTANEOUS RECORDINGS OF PRESSURESFROM A FLUID-FILLED CHAMBERTHROUGHTHREETRANSDUCERSAT FREQUENCIES RANGING FROM 1 TO 200 CYCLES PER SECOND. The external manometerresonates at 7 c/sec and its response falls off rapidly thereafter. It is likely that the equal diminution ofthe amplitude responses of both the Lilly and Telco manometers at 100 c/sec reflects a decrease in theamplitude of the generated sine wave.
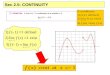
The first derivative of the ventricular pressure pulse mmHg/sec. A B CDwas determined in a total of 40 patients, in some of whom FIRST I\ RVit was recorded in both ventricles. In 13 patients percu- DERIVATIVEtaneous puncture of the left ventricle was carried out OF(13) and in a total of 21 patients, including all 17 pa- VENTRICULAR
tients in whom right ventricular dp/dt was recorded, the PRESSURETelco micromanometer was used. Four patients with _500patent ductus arteriosus and 2 patients with mitral steno- EFsis were studied by direct puncture of the left ventricle 60at the time of thoracotomy. In the patients with patent /ElR/UAductus arteriosus the effects of clamping and of releasing VENTRICULARthe ductus were observed. Congenital or rheumatic heart PRESSUREdisease was present in most of the patients studied in the mm.Hlcatheterization laboratory (Tables I and II). Eight pa- 30 ltients had experienced congestive heart failure prior tostudy and had roentgenographic evidence of ventricularenlargement; in 6 of these the ventricular end-diastolicpressure was distinctly elevated. Thirty-two of the pa-tients studied were in sinus rhythm and 8 had atrial O @5sec.fibrillation. EKG
The cardiac abnormalities present were divided by thetype of hemodynamic burden which they imposed on the FIG. 2. SIMULTANEOUSRECORDINGSOF THE RIGHTventricle. It is fully recognized that considerable varia- TRICULAR PRESSUREPULSE, THE FIRST DERIVATIVE OFtion in the state of ventricular function existed in differ- RIGHT VENTRICULAR PRESSURE, AND THE ELECTROCA]ent patients in the same group and that alterations in ven- GRAMIN A PATIENT WITH MITRAL REGURGITATION, Altricular performance were induced by anethesia and FIBRILLATION AND PULMONARYHYPERTENSION. Thethoracotomy in the patients who were studied under these ous portions of the first derivative arne labeled andconditions. Nonetheless, it was felt that by dividing the cussed in the text.
VEN-THE
RDIO-rRIALvari-
dis-
81

WILLIAM L. GLEASONAND EUGENEBRAUNWALD
patients into three groups the gross effects of chronicelevations of systolic pressure and of stroke volume ondp/dt could be discerned. Group A consists of 15 patientsin whom the ventricle in which dp/dt was determined didnot have an abnormally increased hemodynamic burdenand includes 4 patients with mitral stenosis, 5 with atrialseptal defect, and 1 after complete abolition of an aorticpressure gradient in whom the left ventricle was stud-ied. In addition, in group A there were 3 patients with-out hemodynamic evidence of heart disease and 2 withabnormalities involving the left side of the heart butwithout pulmonary hypertension, in whom dp/dt was de-termined in the right ventricle. Group B consists of 18patients in whom the ventricle which was studied was sub-ject to a chronically augmented flow load. In this groupthere were 5 patients with mitral regurgitation, 5 withaortic regurgitation, and 4 with patent ductus arteriosus
in whom the left ventricular dp/dt was recorded, as wellas 3 patients with atrial septal defect and 1 with ventricu-lar septal defect in whom the right ventricular dp/dt wasdetermined. Group C consists of the 11 patients in whomthe dp/dt was determined in ventricles which developeda distinctly elevated systolic pressure (increased pressureload). This group consists of 3 patients with aortic sten-osis in whom the left ventricle was studied, and 5 pa-tients with pulmonary hypertension and 3 patients withpulmonic stenosis in whom the right ventricle was stud-ied.
During the control observations the patients were askedto relax and to suspend respiration briefly while the elec-trocardiogram, ventricular pressure and dp/dt were re-corded with a multichannel photographic oscilloscopicrecorder. In a number of patients without abnormal he-modynamic burdens the effects of a variety of acute in-
TABLE I
Peak left ventricular dp/dt *
LVPeak Heart pressure
Diagnosis dp/dt rate s/d
Group A, normal LV loadMS; TS; AF 1,032 67 120/8
1,439 96 97/9
1,385 89 118/9
1,300 90 114/15878 86 108/21
1,009 88 99/7
841 71 83/8
1,696 107 103/3
1,611 105 95/8
943 58 87/6
938 86 96/6
Group B, increased LV flow load1,355 108 96/8
PatientMethod
LVPeak Heart pressure
Diagnosis dp/dt rate s/d
Group B, increased LV flow loadJ.E.S.TC
A.R.L.LVP
V.E.R.LVP
W.W.G.tLVP
L.M.L.LVP
E.J.I.tLVP
B.J.McC.tLVP
J.M.B.LVP
W.R.A.tLVP
MI; ASD 1,615 95 110/9
MI; AF
MI; Al; AF
AI severe
Al moderate
Al very severe
Al severe
MI; AF
AL severe.
1,276 73 109/7
1,076 79 120/3
1,252 90 141/9
1,284 87 127/10
1,223 102 160/35
1,308 92 138/10
975 86 98/5
920 74 116/29
Group C, increased LV pressure loadJ.L.W. AS, gradientLVP 41 mmHg 2,150 107 155/9
R.A.Z. AS, gradientLVP 62 mmHg
L.D.S. AS, gradientLVP 50 mmHg
3,239 103 186/15
2,080 94 156/24
PatientMethod
A.T.OR
O.M.H.LVP
G.L.W.OR
N.E.D.t
LVP
J.P.H.TC
J.Y.TC
D.A.T.TC
A.B.C.TC
C.W.C.TC
M.J.S.TC
G.R.P.LVP
MS; AF
MS; AF
MS; AF;dilated LVPreop.Postop.
ASD;normal LV
ASD;normal LV
Postop. AS;no gradient
ASD;normal LV
ASD;normal LV
ASD;normal LV
MI; AF
* Abbreviations: dp/dt = first derivative of pressure pulse; s/d = systolic/diastolic in mmHg; LV = left ventricle;MS= mitral stenosis; TS = tricuspid stenosis; AF = atrial fibrillation; ASD = atrial septal defect; MI = mitral in-sufficiency; AI = aortic insufficiency; AS = aortic stenosis; t = patients with clinical evidence of myocardial failure;LVP = percutaneous left ventricular puncture; OR= study done in operating room at time of thoracotomy;TC = Telco catheter study.
82

FIRST DERIVATIVE OF VENTRICULARPRESSURE
terventions on the ventricular dp/dt were also determined.The pharmacologic agents studied included isoproterenol,norepinephrine, methoxamine, and atropine. Wheneverthe effects of more than one drug were examined, suffi-cient time was allowed between studies for the results ofthe previously injected drug to disappear completely.The effects of exercise in the supine position were stud-ied in 2 patients who were asked to pedal a stationarybicycle ergometer vigorously for 2 minutes.
RESULTS
1. Contour of dpldtThe contour of the first derivative of the ven-
tricular pressure pulse is, in general, similar inboth ventricles. During ventricular diastole, whenthe rate of change of ventricular pressure is slow,dp/dt is flat and at a level of 0 or slightly greater(point A in Figure 2). With the onset of iso-metric ventricular contraction in the left ven-
tricle, dp/dt increases slowly for several milli-seconds and then rises smoothly to reach its peak(PDLV) near the midpoint of the isovolumetriccontraction period. In the right ventricle, dp/dtexhibits either a notch or an inflection on its as-
cending limb (B, Figure 2) and usually reachesits peak (PDRv) at a point higher (C) than themidpoint of the ascending limb of the ventricularpressure pulse; during early ventricular ejectiondp/dt descends to a level either slightly above or
below the baseline and then remains relatively flatduring mid and late ejection (D). It begins to fallabruptly to values far below zero during late sys-
tole, reaching its nadir early during isovolumetricrelaxation (E). Later during isovolumetric re-
laxation the rate of pressure fall diminishes anddp/dt again returns to the baseline (F).
2. Values for PDLV
The peak values of the ascending limb of dp/dtin the left ventricular pressure pulse recorded dur-ing the control period are presented in Table I;these values ranged from 841 to 3,239 mmHg per
second. In the ten patients without an abnormalhemodynamic load on the left ventricle (group A),PDLV varied from 841 to 1,696, with an average
of 1,219 mmHg per second. In the patients inwhom the left ventricular stroke volume was
chronically augmented (group B) the values forPDLVwere in a similar range (920 to 1,615; aver-
age, 1,228.) The PDLV in patients with an eleva-
TABLE II
Peak right ventricular dp/dt *
RVPeak Heart pressure
Patient Diagnosis dp/dt rate s/d
Group A, normal RV loadJ.E.W. AS; AI 263 87 22/6F.W. M. Hyp 229 79 22/3L.C.J. MS; TS 230 77 25/3L.B.H. Funct M 223 111 23/3J.V.G. Postop. ASD 296 83 33/0
Group B, increased RV flow loadJ.E.S. ASD; MI 520 92 42/5:R.F. VSD 309 86 31/0A.B.C. ASD 459 107 34/6J.P.H. ASD 334 85 34/7
Group C, increased RV pressure loadG.S.t Idiopathic PH 382 77 53/7L.D.C. PS 823 64 121/7O.F.C. MS; PH 646 71 58/6S.K.H. PS; VSD 639 87 69/2K.M.M. PS 489 87 51/9T.S.t Hodgkin's dis.; 422 107 53/11
myocard. infilt.;PH
J.M.B. MI; PH 472 81 59/12M.J.S.t ASD; PH 471 85 77/8
* Abbreviations same as in Table I, plus: VSD= ventric-ular septal defect; PS = pulmonary stenosis; PH =pulmonary hypertension; Hyp = systemic hypertension;Funct M = functional murmur.
tion of left ventricular systolic pressure (group C)tended to be much higher (2,080 to 3,239) than ingroups A and B.
3. Valutes for PDRvThe peak values for the first derivative of the
ascending limb of the right ventricular pressurepulse recorded during the control period in pa-tients without an abnormal hemodynamic load onthe right ventricle (Table II, group A) rangedfrom 223 to 296 mmHg per second. In patientswith right ventricular stroke volume greatly aug-mented but only a slight elevation of right ven-tricular systolic pressure (group B), these valuesranged from 309 to 520. In patients with an in-crease in the pressure load on the right ventricle(group C) the PDRVranged from 382 to 823 mmHg per second.
It is thus apparent that the values for the PD ofthe ventricular pressure pulse varied widely amongvarious patients and that the values in the left ven-tricle exceeded those observed in the right ven-tricle. The large variations of PDare attributable,
83

WILLIAM L. GLEASONAND EUGENEBRAUNWALD
LEFTVENTRICLE
NORMAL VENTRICULARO 0 LOAD
INCREASED VENTRICULARo a FLOW LOAD
INCREASED VENTRICULARA A PRESSURE LOAD
.
0
0a *m
* 2 -a0 An
A A
o0
30 60 90 120 150
VENTRICULAR SYSTOLIC PRESSUREmm.Hg
FIG. 3. RELATIONSHIP BETWEENPD AND THE VENTRICULAR SYSTOLIC PRESSURE.
The symbols with the horizontal lines represent the patients who had marked ven-
tricular enlargement and had experienced congestive heart failure, as described inthe text. The correlation coefficient and regression lines were calculated withoutinclusion of the data from these patients; the formula for the regression line is:PD= 15.3 systolic pressure - 254.
at least in part, to the diversity of cardiovascularabnormalities present in the patients who were
studied, as well as the conditions existing at thetime of study. Nonetheless, it was observed inboth ventricles that the PD tended to be higher inpatients with elevation of intraventricular systolicpressure than in those without. When the PD was
related to the peak ventricular pressures, a sig-nificant correlation (r = 0.85) was evident (Fig-ure 3). It was also observed that at any givenventricular systolic pressure, the PD was a func-tion of the heart rate. Accordingly, when PDwas related to the product of the systolic pressure
and heart rate, a somewhat better correlation(r = 0.92) was evident (Figure 4). The dataobtained from the patients with clinical evidence ofmarked myocardial failure tended to fall to theright of the regression lines in Figures 3 and 4;
i.e., their PD's were relatively low for their sys-
tolic pressures and heart rates. When these pa-
tients were excluded from analysis, the coefficientof correlation between systolic ventricular pressure
and PD rose to 0.91 (Figure 3) and between theproduct of systolic pressure and heart rate and PDit rose to 0.97 (Figure 4).
4. Effects of acute intervention
a) Drugs. Isoproterenol (1.5 pg intravenously)resulted in a striking increase in the PD in allfour patients to whom it was administered (TableIII and Figure 5). A clear-cut increase in heartrate was produced in only one of these four pa-
tients. Methoxamine, in doses that raised leftventricular systolic pressure between 25 and 37mmHg, and slowed the heart rate by an average
of 11 beats per minute, had no significant effect on
VENRIGHTTRICLE
3500
3000
2500PEAK
dp/dt
mmHg/sec.2000
1500
1000-
500
A
AA
UU-
,80 210
84

FIRST DERIVATIVE OF VENTRICULARPRESSURE
RIGHTVENTRICLE
0
0
LEFTVENTRICLE
NORMAL VENTRICULARLOAD
INCREASED VENTRICULARFLOW LOAD
INCREASED VENTRICULARA PRESSURE LOAD
A
*
0
On
a
0 *0
* Ae
0 go000
4-
0 30 60 90 120 150IO0
VENTRICULAR SYSTOLIC PRESSURE(mm.Hg) X HEART RATE X 10-2
210
FIG. 4. RELATIONSHIP BETWEENPD AND THE PRODUCTOF VANTRICULARSYSTOLIC
PRESSUREAND HEART RATE. The symbols indicating the patients who had experi-enced heart failure are the same as in Figure 3, and the correlation coefficient andregression line which are shown were calculated without inclusion of the data fromthese patients; the formula for the regression line is: PD= 0.157 (systolic pres-
sure X heart rate) - 149.
I
J.Y,#03-32-68
FIG. 5. SERIAL RECORDINGSOF LEFT VENTRICULAR PRESSUREANDOF DP/DT IN A 12 YEAROLD GIRL WITH
MILD PULMONIC VALVULAR STENOSIS. The first record (control) is in the basal state, the middle recordafter the administration of 1.5 ,ug isoproterenol (Isuprel), and the final record after 0.7 mg atropine.
85
3500
3000
2500PEAK
dp/dt
mm. Hg/sec.2000
1500
1000
500-

WILLIAM L. GLEASONAND EUGENEBRAUNWALD
TABLE III
Acute interventions *
VentriclePatient studied Peak Peak Heart Ventricular
Diagnosis Method of study Intervention dp/dt -dp/dt rate pressure s/d
LV ControlTC Methoxamine, 2.4 mg
ControlIsuprel, 1.5 pgtControlNorepineph., 2.4 pgControlAtropine, 0.7 mg
LV ControlTC Isuprel, 1.5 pg
ControlMethox., 2 mgControlAtropine, 1 mg
LV ControlTC Methox., 2 mg
Isuprel, 1.5 ,gjAtropine, 1 mg
RV ControlTC Atropine, 1 mg
RV ControlTC Isuprel, 1.5 pg
ControlMethox., 1 mgControlAtropine, 1 mg
LV ControlTC 2 min. exercise
RV ControlTC 2 min. exercise
LV ControlTC 2 min. exercise
LV Ductus closedOR
Ductus opened
LXV Ductus closedOR
Ductus opened
LV Ductus closedOR
Ductus opened
LV Ductus closedOR
Ductus opened
841881863
2,425920
1,456845
1,370
9431,228
835737750
1,372
938994
1,1971,008
295318
230453196189239298
1,0091,948
165297
9601,520
2,629
2,950
1,300
1,410
2,030
2,040
968
1,1101,2601,2601,2301,2201,3301,1801,500
661675780960870
1,290
915980
1,0401,060
249267
220254230225228304
1,0701,390
126214
3,850
3,520
1,390
1,520
2,920
2,840
1,510
768 1,210
71 83/845 122/1872 93/6
100 100/674 99/1150 151/1172 93/8
119 109/11
58 87/959 105/858 101/1151 126/954 115/11
112 138/5
86 96/679 111/586 111/3
111 98/1
83 33/0106 29/0
77 25/379 32/368 23/063 25/275 22/-295 23/0
88 99/7111 122/7
99 22/5130 26/3
73 105/9102 120/9
89 191/12
103 178/18
65 145/12
80 120/12
128 111/9
129 105/11
94 90/16
98 78/17
*Abbreviations same as in Tables I and II, plus: PDA = patentaorta; -dp/dt = maximum rate of fall of ventricular pressure.
t Isoproterenol.
ductus arteriosus; Coarc. = coarctation of
J.Y.ASD
C.W.C.ASD
M.J.S.ASD
J.V.G.Postop
ADS
L.C.J.MS; TS
J.P.H.ASD
L.B.H.Funct M
J.G.P.ASD
J.B.PDA;
coarc.
T.B.PDA
C.M.F.PDA
M.Y.J.PDA;
MI
86

FIRST DERIVATIVE OF VENTRICULARPRESSURE
the PD in the four patients to whom it was ad-ministered, in spite of raising the left ventricularend-diastolic pressure (Figure 6). One patientreceived norepinephrine in addition to isoprote-renol and methoxamine; this drug elevated the PDbut to a lesser degree than isoproterenol (PatientJ. Y., Table III, Figures 5 and 6). Atropine, ad-ministered intravenously to five patients in dosesof 0.7 to 1.0 mg, raised the heart rate by an averageof 33 beats per minute and elevated the PD byvalues ranging from 7 to 83 per cent of the controlvalues; the magnitude of the increase in the PDwas related to the increase in heart rate (TableIII).
b) Exercise. In the patients in whomthe effectsof exercise were studied, the PDLV (two patients)and the PDRv (one patient) were greatly aug-mented (Table III).
c) Effects of opening a patent ductus arteriosus.Immediately after the ductus was opened a sig-nificant increase in heart rate occurred in two pa-tients, and in them a modest augmentation of PDLVwas observed. In the other two patients no sig-nificant change in heart rate occurred; PDLV fellslightly in one, and remained unchanged in theother (Table III).
d) Beat-to-beat changes in PD in atrial fibrilla-tion. It was consistently observed that the PDLVvaried with the interval between successive QRS
mmHg /sec.1500.
FIRST 000 CONTROL METHOXAhDERIVATIVE 2.4 mg.
OFVENTRICULAR 0°
PRESSURE -1000C-100
LEFTVENTRICULAR mm
50HgPRESSURE
EKG ZZ
complexes. Furthermore, the peak left ventricu-lar systolic pressure and the aortic pulse pressurewere directly proportional to the PDLV; i.e., whenthe rate of left ventricular pressure rise was rapid,the peak systolic pressure and pulse pressurewhich were developed tended to be greater thanwhen the PDLV was relatively low. The resultsobtained in one patient are plotted in Figure 7 andare representative of those observed in the eightpatients with atrial fibrillation who were studied.
e) Ventricular premiiature contractions. Fourpatients developed an occasional premature ven-tricular contraction in the course of the study.In each instance the PD of the premature con-traction was significantly smaller than that ob-served during normal beats.
5. Negative PD
The maximum rate of decline of the ventricularpressure (negative PD) was usually of an orderof magnitude similar to the PD of the ascendinglimb of the same ventricular pressure pulse. In-terventions that increased nmyocardial contractility(e.g., intravenous isoproterenol, Figure 5) hadlittle effect on the negative PD in spite of theirstriking augmentation of the positive PD. On theother hand, an acutely induced increase in the peakventricular pressure or increase in heart ratetended to augment the negative PD (Table III).
J.Y.# 03-32-68
FIG. 6. SERIAL RECORDINGSOF LEFT VENTRICULARPRESSUREANDOF DP/DT IN THE SAMEPATIENT AS INFIGURE 5. The tracings obtained in the control state are on the left, after methoxamine injection in themiddle, and after norepinephrine injection on the right. These recordings were obtained at a slower pa-per speed than those reproduced in Figure 5.
87

WILLIAM L. GLEASONAND EUGENEBRAUNWALD
L.V. PEAK dp/dt IN ATRIAL FIBRILLATION
LV.PEAK iC
dp/dtmmHg/sec. c
.54 .62 70 78 .86 94 86 90 94 98 102 106 12 18 24 30 36 42
R-R INTERVAL seconds LV SYSTOLIC PRESSUREmm. Hg PULSE PRESSUREmm. Hg
FIG. 7. GRAPHSILLUSTRATING THE RELATIONSHIP BETWEENTHE LEFT VENTRICULARPD AND (A) THEPRECEDINGR-R INTERVAL; (B) THE LV SYSTOLIC PRESSURE; (C) THE BRACHIAL ARTERIAL PULSE PRES-SURE OF THE SAMEBEAT IN A PATIENT WITH RHEUMATICMITRAL VALVE DISEASE ANDATRIAL FIBRILLATION.
DISCUSSION
Sarnoff and Mitchell have recently defined an
increase of myocardial contractility as occurring"when from any given end-diastolic pressure or
fiber length, the ventricle produces more externalstroke work and more stroke work per systolicsecond. Implicit in this definition is an increasedrate of development of tension when contractilityincreases" (17). Rushmer, Smith and Franklinhave demonstrated an increase in the rate of pres-
sure development in the left ventricle when myo-cardial contractility was augmented by the ad-ministration of catecholamines, by muscular ex-
ercise, or by hypothalamic stimulation (18). Theobservations of these and other investigators(1-11) are all compatible with the view that therate at which ventricular pressure is developedreflects a fundamental property of contractingmyocardium. Accordingly, it was thought thatmeasurement of this parameter would provide an
approach to the study of ventricular contractilityin intact, unanesthetized man.
It is well established that certain sympathomi-metic amines. such as isoproterenol and norepi-nephrine, augment myocardial contractile force,
while others, such as methoxamine, fail to do so(19, 20). It could thus be anticipated that ifchanges in the PD reflected changes in myocardialcontractility, the rate of pressure rise should beelevated by administration of the cardioactive sym-pathomimetic amines, but not modified by thedrugs that have no direct cardiac effects; this in-deed was found to be the case (Figure 5). It wasalso demonstrated that muscular exercise and atro-pine-induced tachycardia raised the PD. Theincrease noted with tachycardia may be analogousto the so-called "treppe" phenomenon, describedby Bowditch (21).
Siegel and Sonnenblick, utilizing an isovolu-metrically-beating ventricle, as well as a cat papil-lary muscle preparation, have demonstrated thatrate of development of tension is dependent onthe length of the muscle fiber at the onset of con-traction (8). In patients with mitral valve dis-ease and atrial fibrillation, variations in the dura-tion of diastole result in alterations in the degree ofventricular filling and, therefore, in the ventricularend-diastolic volume and fiber length (22). Inthe present study good correlations between thePD and the duration of the filling period (Figure
88

FIRST DERIVATIVE OF VENTRICULARPRESSURE
7, A), the peak sytolic ventricular pressure (B)and the arterial pulse pressure (C) were ob-served. These observations suggest that in thesepatients with mitral stenosis and atrial fibrillation,the PD correlates closely with the end-diastolicfiber length during a series of consecutive cardiaccycles.
Unlike the effects of acute elevations of ven-tricular end-diastolic volume, hemodynamic ab-normalities which result in a chronic augmentationof ventricular stroke volume did not result in ab-normal values of the PD. In contrast, the PDcor-related well with the peak systolic pressurechronically developed by the ventricle, and in thiscorrelation both ventricles fell on the same regres-sion line (Figure 3). A number of factors may beinvolved in this relationship. Sandler, Dodge andHay have recently presented evidence indicatingthat the thickness of the ventricular wall increasesin proportion to the systolic pressure which ischronically developed by the ventricle (23). Tak-ing the chamber size and wall thickness into con-sideration they have calculated that the tension de-veloped by each unit of myocardium tends to re-main constant, regardless of the level of systolicpressure which the ventricle sustains. In pa-tients with a ventricular "pressure load" and anincreased muscle mass of hypertrophied myo-cardium, the elevated systolic pressure is developedin the same time interval that is required by thenormal myocardium to reach a normal ventricularsystolic pressure. In view of these findings ofSandler and co-workers, it is possible that therates of development of tension of each myocardialunit are similar in the normal and in the hyper-trophied heart. Accordingly, it may be postulatedthat the relatively high PD's observed in ventriclesthat developed elevated pressures reflect the in-creased muscle mass which is present. The differ-ences in the PD's observed between the two ven-tricles in the patients without hemodynamic ab-normalities could also be similarly explained.
The correlation between PD and peak systolicpressure was improved slightly when rate was alsotaken into consideration (Figure 4). It is likelythat the sympathetic stimulation of myocardialcontractility was greater in patients with rapidheart rates than in those with slower rates, andthat this effect, as well as the stimulation of myo-cardial contractility provided by an increase in
heart rate per se-i.e., by the "treppe" phenome-non (21, 24)-was responsible for the improve-ment in this correlation.
The patients who had experienced congestiveheart failure and had roentgenographic evidenceof left ventricular enlargement and elevation of theventricular end-diastolic pressure, tended to havelower PD's than might have been anticipated bytheir systolic ventricular pressure and heart rate(Figures 3 and 4). Two explanations for thisfinding may be advanced. First, when the law ofLaplace (25) is considered, it is apparent that anygiven rate of development of tension by the myo-cardium would result in a slower rate of pres-sure rise and, hence, in a lower PD in a dilatedthan in a normal-sized heart. Second, it is pos-sible that the depression of myocardial contractilitywhich may have been present in these patients isresponsible for their lowered PD's. In sup-port of this view are the demonstrations by Wig-gers in the dog with an intact circulation (6)and by Buckley and Zeig in an isolated heartpreparation (10) that acute left ventricular failureis accompanied by a decrease in the rate of ven-tricular pressure rise. Regardless of the specificmechanism responsible for lowering the PD inpatients with congestive heart failure, it is possiblethat analysis of the first derivative of the ventricu-lar pressure pulse may provide a simple means ofquantifying depressed ventricular function in man.
The findings in this investigation are not con-sonant with the general impression (26) that therate at which ventricular pressure falls usuallyparallels the rate at which it rises (26) (TableIII). However, Zeig, Buckley and Porter haverecently shown that contraction and relaxation canbe altered independently by acutely changing ven-tricular work loads (11).
SUMMARY
Since observations in experimental animals havesuggested that the rate at which ventricular pres-sure rises is a function of myocardial contractility,it was thought that determination of the rate ofchange of ventricular pressure might permit studyof myocardial contractility in intact man. Thefirst derivative of the ventricular pressure pulsewas continuously computed by means of an elec-tronic differentiating circuit in 40 patients. Inorder to avoid the artifacts inherent in pressures
89

WILLIAM L. GLEASONAND EUGENEBRAUNWALD
measured by means of standard catheter-manom-eter systems, these studies were confined to pres-sures obtained from a catheter with a high-fidelitymicromanometer mounted at its tip or by punc-ture of the ventricle with the manometer directlyattached to the needle. The peak first derivative(maximum rate of pressure rise) in patients with-out hemodynamic abnormalities ranged between841 and 1,696 mmHg per second in the left ven-tricle, and between 223 and 296 in the right ven-tricle. Interventions which acutely augmentedmyocardial contractility, such as muscular ex-ercise, isopropyl norepinephrine, norepinephriine,and atropine, resulted in striking increases in thepeak derivative. Beat-to-beat changes in ven-tricular filling in patients with atrial fibrillationproduced changes in the peak derivative whichsuggested that the latter parameter was also de-pendent upon ventricular end-diastolic volume. Inthe control state the peak derivative in both ven-tricles demonstrated a linear correlation with thepeak systolic pressure and a somewhat better cor-relation with the product of systolic pressure andheart rate.
ACKNOWLEDGMENT
The cooperation of Dr. Andrew G. Morrow, who ob-tained the pressure tracings at the operating table, isgratefully acknowledged. Mr. Frank Noble, of theLaboratory of Technical Development, National HeartInstitute, designed the sine-wave generator and the dif-ferentiating circuit and provided helpful technical advicethroughout this study.
REFERENCES
1. Frank, 0. On the dynamics of cardiac muscle (C. B.Chapman, and E. Wasserman, Trans.). Amer.Heart J. 1959, 58, 282.
2. Patterson, S. W., Piper, H., and Starling, E. H.The regulation of the heart beat. J. Physiol.(Lond.) 1914, 48, 465.
3. Wiggers, C. J. Studies on the cardiodynamic ac-tions of drugs. I. The application of the opticalmethods of pressure registration in the study ofcardiac stimulants and depressants. J. Pharmacol.exp. Ther. 1927, 30, 217.
4. Wiggers, C. J. Studies on the cardiodynamic actionsof drugs. II. The mechanism of cardiac stimula-tion by epinephrin. J. Pharmacol. exp. Ther. 1927,30, 233.
5. Wiggers, C. J., and Stimson, B. Studies on thecardiodynamic actions of drugs. III. The mecha-nism of cardiac stimulation by digitalis andg-strophanthin. J. Pharmacol. exp. Ther. 1927, 30,251.
6. Wiggers, C. J. Dynamics of ventricular contractionunder abnormal conditions. Circulation 1952, 5,321.
7. Reeves, T. J., Hefner, L. L., Jones, W. B., Coghlan,C., Prieto, G., and Carroll, J. The hemodynamicdeterminants of the rate of change in pressure inthe left ventricle during isometric contraction.Amer. Heart J. 1960, 60, 745.
8. Siegel, J. H., and Sonnenblick, E. H. A dynamicindex characterizing alterations in the basic stateof cardiac muscle. Circulat. Res. In press.
9. Tolman, R. A., and Young, P. G. Slope changes ofventricular pressure curves compared with ven-tricular function curves. Fed. Proc. 1961, 20, 124.
10. Buckley, N. M., and Zeig, N. J. Acute unilateralventricular failure in the isolated dog heart. Amer.J. Physiol. 1959, 197, 247.
11. Zeig, N. J. Buckley, N. M., and Porter, E. P. Ef-fects of work loads applied at various times inthe cardiac cycle of the isolated dog heart. Circu-lat. Res. 1961, 9, 531.
12. Brock, R., Milstein, B. B., and Ross, D. N. Per-cutaneous left ventricular puncture in the assess-ment of aortic stenosis. Thorax 1956, 11, 163.
13. Brockenbrough, E. C., Morrow, A. G., Talbert, J.,and Braunwald, E. Percutaneous puncture of theleft ventricle. Brit. Heart J. In press.
14. Laurens, P., Bouchard, P., Brial, E., Cornu, C., Bas-culard, P., and Soulie, P. Bruits et pressionscardio-vasculaires enregistres in situ a l'aide d'unmicromanometre. Arch. Bal. Coeur 1959, 52,121.
15. Allard, E. M. Construction et utilisation des cap-teurs de pression in Proc. Second Int. Conf. onMedical Electronics, C. N. Smyth, Ed. London,Ilffe, 1960, p. 263.
16. Noble, F. W. Electrical Methods of Blood-pressureRecordings. Springfield, Ill., Thomas, 1953, p. 40.
17. Sarnoff, S. J., and Mitchell, J. H. The regulation ofthe performance of the heart. Amer. J. Med. 1961,30, 747.
18. Rushmer, R. F., Smith, 0., and Franklin, D. Mecha-nisms of cardiac control in exercise. Circulat.Res. 1959, 7, 602.
19. Goldberg, L. I., Cotten, M. de V., Darby, T. D., andHowell, E. V. Comparative heart contractileforce effects of equipressor doses of several sym-pathomimetic amines. J. Pharmacol. exp. Ther.1953, 108, 177.
20. Goldberg, L. I., Bloodwell, R. D., Braunwald, E., andMorrow, A. G. The direct effects of norepineph-rine, epinephrine, and methoxamine on myocardialcontractile force in man. Circulation 1960, 22,1125.
21. Bowditch, H. P. tber die Eigenthumlichkeiten derReizarbeit, welche die Muskelfasern des Herzenszeigen. Ber. Verh. der kongiglich sachsischen ges.Wissenschaften zu Leipzig 1871, 23, 652.
90

FIRST DERIVATIVE OF VENTRICULARPRESSURE
22. Braunwald, E., Frye, R. L., Aygen, M. M., and Gil-bert, J. W., Jr. Studies on Starling's law of theheart. III. Observations in patients with mitralstenosis and atrial fibrillation on the relationshipsbetween left ventricular end-diastolic segmentlength, filling pressure, and characteristics of ven-
tricular contraction. J. clin. Invest. 1960, 39, 1874.23. Sandler, H., Dodge, H., and Hay, R. Left ventricu-
lar tension and stress in man. Clin. Res. 1961, 9,145.
24. Sarnoff, S. J., Mitchell, J. H., Gilmore, J. P., andRemensnyder, J. P. Homeometric autoregulationin the heart. Circulat. Res. 1960, 8, 1077.
25. Rushmer, R. F. Cardiovascular Dynamics, 2nd ed.Philadelphia, Saunders 1961, p. 69.
26. Wiggers, C. J., and Maltby, A. B. Further observa-tions on experimental aortic insufficiency. IV.Hemodynamic factors determining the character-istic changes in aortic and ventricular pressure
pulses. Amer. J. Physiol. 1931, 97, 689.
91