Embed Size (px)
Citation preview
Epidemiology & Molecular
Pathogenesis of Vulvar &
Vaginal cancer
DR. SRAVANTHI
FELLOW IN GYNECOLOGICAL ONCOLOGY
KIDWAI MEMORIAL INSTITUTE OF ONCOLOGY
Incidence
Constitutes
5% of all the malignancies of female genital tract
0.6% of female cancer
Estimated new cases and deaths from vulval cancer in the
United States in 2015
New cases: 5150
Deaths: 1080
Rare malignancy (28th) in the United States and accounts for
0.3% of all new cancers.
Cancer Facts and Figures 2015. Atlanta
American Cancer Society, 2015.
SEER Stat Fact Sheets:
Vulval cancer
Lifetime Risk of Developing Cancer : Approximately
0.3 percent
0.2% of all cancer deaths (Estimated).
5-years survival rate of 71.2%
Based on2010-2012 data
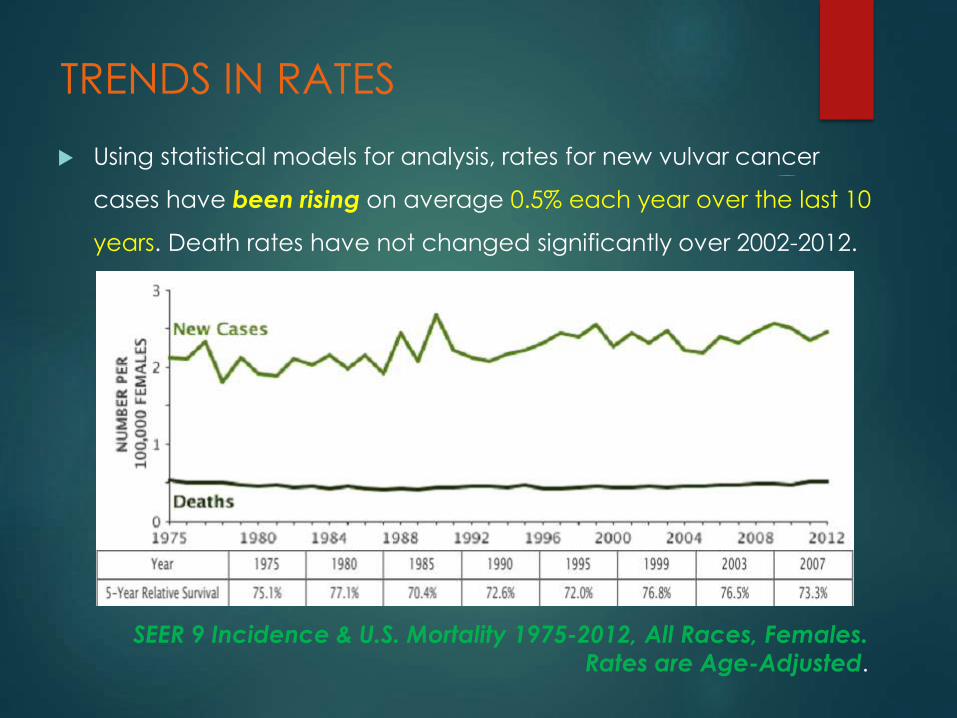
TRENDS IN RATES
Using statistical models for analysis, rates for new vulvar cancer
cases have been rising on average 0.5% each year over the last 10
years. Death rates have not changed significantly over 2002-2012.
SEER 9 Incidence & U.S. Mortality 1975-2012, All Races, Females. Rates are Age-Adjusted.
Age
A disease of older women.
Delayed diagnosis is typical, despite vulva being an external
organ.
Vulvar cancer is most frequently diagnosed among women
aged 75-84.
Median Age at Diagnosis is 68 years.
SEER Stat Fact Sheets: Vulval cancer, 2014
Etiology - HPV Approximately, 40% vulvar cancers are HPV (Human Papilloma
Virus) Positive.
Of these HPV positive invasive vulvar cancers – 85% are attributed
to HPV 16.
Prophylactic HPV vaccines have the potential to decrease the
incidence of invasive vulvar cancer by about one-third overall,
and to be even more effective in younger women.
Smith JS et al.
Human Papillomavirus Type-Distribution in Vulvar and Vaginal Cancers and Their
Associated Precursors
Obstet Gynecol. 2009; 113:917-24
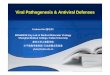
Etiology – Vulval
Intraepithelial Neoplasia (VIN) The International Society for the Study of Vulvovaginal Disease
(ISSVD) in 2004 officially divided VIN into two types:
VIN Usual Type – HPV infection related (warty/ basaloid
/mixed)
VIN Differentiated Type - unrelated to HPV infection
The older classification of VIN 1, 2, and 3 was based on the
degree of histologic abnormality, but there is no evidence that
the VIN 1 to 3 morphologic spectrum reflects a biologic
continuum,
or that VIN 1 is a cancer precursor
Etiology – Vulval
Intraepithelial Neoplasia (VIN)
There has been a significant increase in the incidence of
vulvar intraepithelial Neoplasia (VIN) in recent decades, and
this has been attributed to
changing sexual behavior ,
human papillomavirus (HPV) infection, and
cigarette smoking.
In a study designed to investigate the malignant potential of
the vulvar premalignant conditions, Eva et al. identified 580
women from Birmingham, England, who had vulvar biopsies
showing VIN, lichen sclerosus, or Squamous hyperplasia over a
5-year period. These women were studied for the presence of
a synchronous or metachronous vulvar cancer.
differentiated VIN had a higher risk of malignancy (85.7%) than
usual VIN (25.8%),
lichen sclerosus (27.7%) or
Squamous hyperplasia (31.7%).
Eva et al.
Differentiated type VIN has a high-risk association with vulval
squamous cell carcinoma
Int J Gynecol Cancer 2009;19:741-744
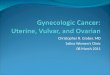
Basloid or warty type
multifocal
In younger
Related to HPV infection
Vulvar Intraepithelial
Neoplasia
Cigarette smoking
Keratinizing type
Unifocal
In older
Not related to HPV
In area adjacent to lichen
sclerosis and Squamous
hyperplasia(80%)
VIN uncommon -
Differentiated type
Types
Etiology The increased risk of a subsequent cancer to be 1.3-fold.
Most of the second cancers were related to
smoking (i.e., cancers of the lung, buccal cavity , pharynx,
nasal cavity , or larynx) or
human papillomavirus infections (e.g., cervix, vagina, or
anus).
Pathology Squamous cell carcinoma = 85–90%
Basal cell, Invasive paget’s disease, bartholin glands Ca,
Sarcoma
SURVIVAL Historically, (in early 20th century) – presentation with
advanced diseases.
5-years survival – 20-25% ONLY
Radical en-bloc dissection by Taussig - US (1940) and Way -
Britain (1960) – Improved survival of 60-70%. (High post-
operative morbidities –
wound breakdown, infection, and
prolonged hospitalization,
pelvic exenteration- for patients with disease involving the anus,
rectum, or proximal urethra)
Since approximately 1980, there has been a
paradigm shift in the approach to vulvar cancer.
1. Individualization of treatment for all patients with invasive
disease
2. Vulvar conservation for patients with unifocal tumors and an
otherwise normal vulva.
3. Omission of the groin dissection for patients with T1 tumors
and no more than 1 mm of stromal invasion
4. Elimination of routine pelvic Lymphadenectomy.
5. The use of separate groin incisions for the groin
dissection to improve wound healing.
6. Omission of the contra lateral groin dissection in
patients with lateral T1 lesions and negative ipsilateral
nodes.
7. The use of preoperative radiation therapy or definitive
radiation therapy to obviate the need for exenteration
in selected patients with advanced disease.
8. The use of postoperative radiation to decrease the
incidence of groin recurrence and improve survival of
patients with multiple positive groin nodes.
9. Resection of bulky positive groin and pelvic nodes
without complete
10. The use of sentinel node biopsy to obviate the need for
complete groin dissection in carefully selected patients
with early vulvar cancer
Survival
Overall 5 years survival rate in USA is 71.2%
Based on data from SEER 18 2005-2011
The earlier vulvar cancer is diagnosed, the better chance a
person has of surviving five years after being diagnosed.
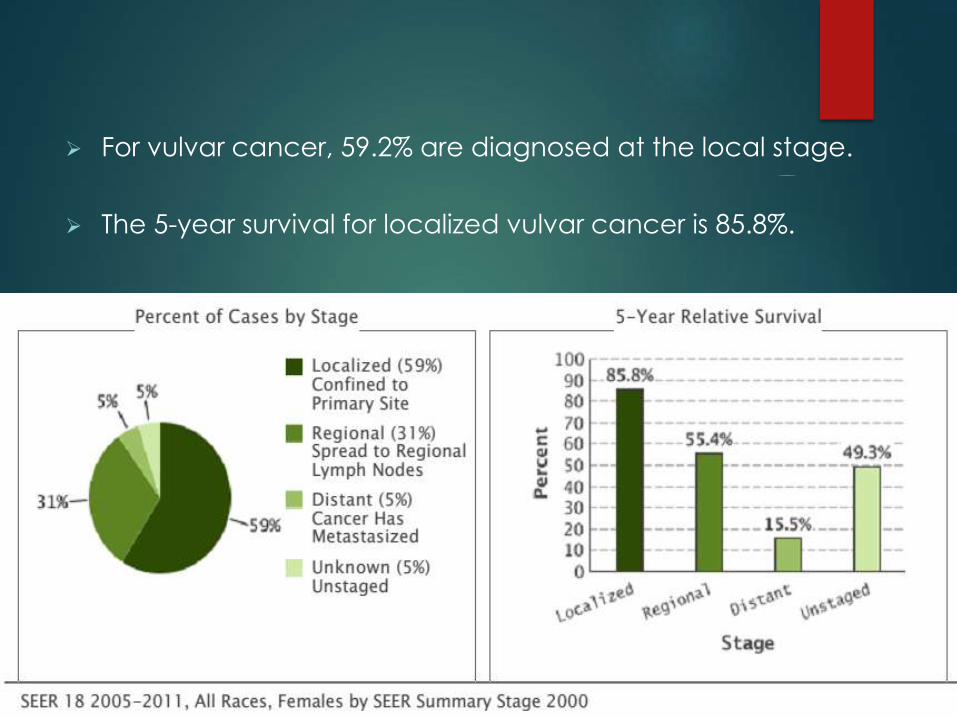
For vulvar cancer, 59.2% are diagnosed at the local stage.
The 5-year survival for localized vulvar cancer is 85.8%.
Vaginal Cancer
Primary carcinomas of the vagina represent 1–2% of
malignant neoplasms of the female genital tract.
In the United States, it is estimated that
there will be 3,170 new cases diagnosed in 2014, and
880 deaths from the disease
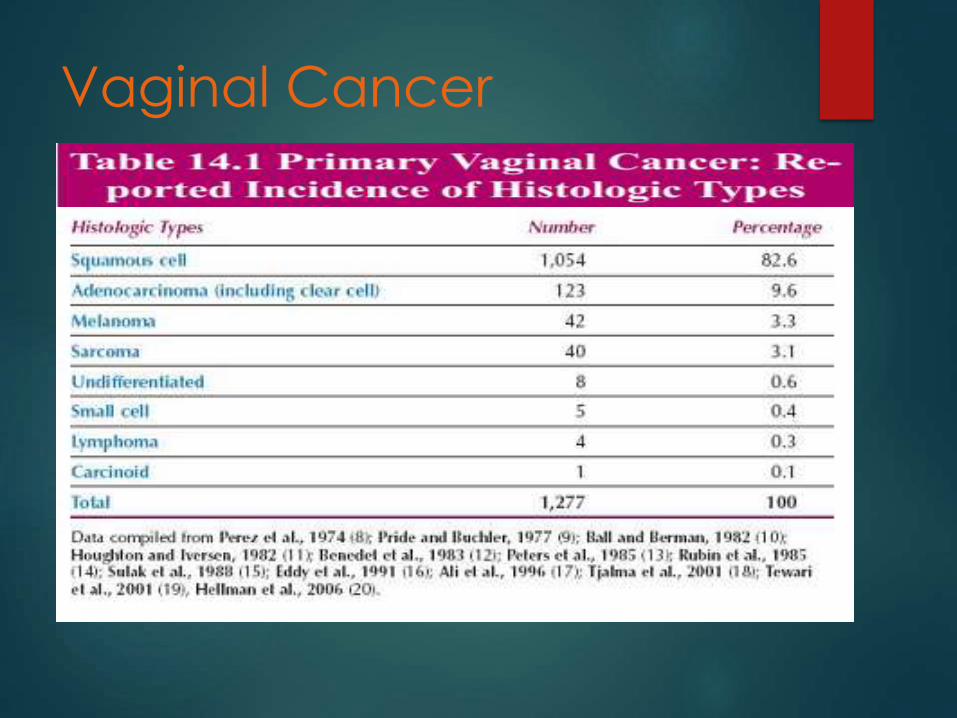
Like cervical cancer, squamous cell histology accounts for
70–80% of cases.
Vaginal Cancer
Fu reported that 84% of carcinomas involving the vagina
were secondary , usually from the
cervix (32%);
endometrium(18%);
colon and rectum (9%);
ovary (6%);
or vulva (6%).
Vaginal Cancer
Unlike cervical cancer, more than 50% of patients are
diagnosed in the seventh, eighth, and ninth decades of life.
Squamous cell carcinoma is the most common vaginal
cancer .
The mean age of the patients is approximately 67 years,
although the disease occasionally is seen in the third and
fourth decades of life.
About 80% of patients are older than 50 years.
Vaginal Cancer
Vaginal Cancer - Etiology
Women who have been treated for a prior anogenital
cancer , particularly of the cervix have a high relative risk
of developing vaginal cancer , although the absolute risk
is low.
A study of 341 cases from the Radiumhemmet reported
that the disease seemed to be etiologically related to
cervical cancer , and thus HPV infection, in young
patients, but in older patients, there was no such
association
Vaginal Cancer - Etiology
The relative rarity of invasive vaginal cancer suggests that
the cervical transformation zone is an important, but not
necessary, factor in malignant transformation .
There are three possible mechanisms for the occurrence of
vaginal cancer after cervical neoplasia
1. Occult residual disease
2. New primary disease arising in an“at-risk” lower genital tract
3. Radiation carcinogenicity
Vaginal Cancer - Etiology
Controversy exists regarding the distinction between a new
primary vaginal cancer and a recurrent cervical cancer .
Some authorities use a 5-year cutoff because 95% of
cervical cancer recurrences will occur within this period but
others prefer a10-year interval.
Vaginal Cancer - Etiology
Over 90% of high-grade VAIN 2–3 lesions and 70% of vaginal
cancers are associated with HPV infections.
HPVs 16 and 18 are associated with over 60% of high-grade
VAIN and 40% of low-grade VAIN
Role of prophylactic HPV vaccines???
Prior pelvic radiation therapy has been considered a
possible cause of some vaginal carcinomas.
The true malignant potential of vaginal intraepithelial
neoplasia (VAIN) is unclear because after diagnosis, the
condition is usually treated.
Chronic local irritation from long-term use of a pessary may
be associated with vaginal cancer.
Diethylstilbestrol Exposure In
Utero - Adenocarcinoma The estimated risk of clear cell adenocarcinoma in an
exposed offspring was 1:1,000 or less, and 70% of cases
were stage I at diagnosis.
Although DES exposure in Utero rarely led to vaginal
adenocarcinoma, vaginal adenosis occurred in about
45% of patients, and 25% of exposed women had
structural changes to the cervix and vagina, such as a
transverse vaginal septum, a cervical collar, a
cockscomb (a raised ridge, usually on the anterior cervix),
or cervical hypoplasia.
Herbst et al. reported a 5-year survival rate for DES-
related patients with clear cell carcinoma of the vagina,
regardless of the mode of therapy of 78%.
The survival rate correlated well with stage of disease:
87% for patients with stage I, 76% for patients with stage II,
and 30% for those with stage III disease.
In contrast, the prognosis of patients with primary non–
DES-related adenocarcinomas appears to be relatively
poor .