Embed Size (px)
Citation preview

Waldenström’s Macroglobulinemia:
Genomic Based Treatment Advances
Steve Treon MD, PhD, FACP, FRCP
Professor of Medicine
Bing Center for Waldenstrom’s Macroglobulinemia
Dana Farber Cancer Institute
Harvard Medical School

Discovery of the MYD88 Mutationin 2011 in WM -2012-
93-97% of WM patientsTreon et al, ASH 2011; NEJM 2012

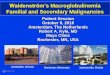
Pro-Survival Signaling Driven by Mutated MYD88
in Waldenström's Macroglobulinemia
Yang et al, Blood 2013
Yang et al, Blood 2016
Degradation
TLRs IL-6
IL-6
IL-6
IL-6R
gp-130
growth survival
IL-6
mTOR
ERK1/2
HCK
NFKB
MYD88
BTKIRAK1/4
AKT
ibrutinib

1 CopyNumber20.9
0.8 20%0.7
0.6 40%0.5
0.4 60%0.3
0.2 80%0.1
0 CopyNumber1
34
56
78
910
Chromosome 6
Num
ber
of
Affe
cte
d P
atie
nts
p25
.3
p25
.2
p25
.1
p24
.3
p24
.1
p2
3
p22
.3
p22
.1
p21
.31
p21
.2
p21
.1
p12
.3
p12
.1
p11
.2
q1
2
q1
3
q14
.1
q14
.3
q1
5
q16
.1
q16
.3
q2
1
q22
.1
q22
.31
q22
.33
q23
.2
q23
.3
q24
.1
q24
.2
q24
.3
q25
.1
q25
.2
q25
.3
q2
6
q2
7
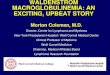
Detection Threshold
HIVEP2
BCLAF1HLA-DQA/B ARID1B
FOXO3
TNFAIP3PRDM1
IBTK
BACH2
CD83 EEF1A1
PLEKHG1
CCR6MAN1A1
COL19A1
Chr. 6q clonal loss is common in WM and impacts
BTK, BCL2, and NFKB regulatory genes
Guerrera et al,
Haematologica
2018
IBTK FOXO3 BCLAF1 TNFAIP3 HIVEP2WM1 0.5 0.52 0.4 1 0.46 0.5 5
WM2 0.56 0.49 0.4 2 0.55 0.4 9
WM3 0.49 0.94 0.4 4 0.51 0.5 5
WM4 0.51 0.53 0.4 8 0.56 0.5
WM5 0.56 0.49 0.5 3 0.47 0.4 3
WM6 0.43 0.54 0.5 4 0.58 0.4 9
WM7 0.58 0.55 0.5 8 0.62 0.5 6
WM8 0.53 0.57 0.6 4 0.66 0.6
WM9 0.69 0.89 0.6 4 0.9 0.8 1
WM10 0.83 0.77 0.7 0.64 0.8 3
WM11 0.82 0.74 0.7 7 0.8 0.8 1
WM12 0.92 0.93 0.7 8 0.97 0.9 8
WM13 0.9 0.93 0.8 1 0.97 0.9
WM14 0.9 1 0.8 4 0.75 0.8 1
WM15 0.83 0.89 0.8 4 0.86 0.8 5
WM16 1.08 0.99 0.8 5 1.06 1.0 1
WM17 0.97 0.82 0.8 7 0.84 0.9 1
WM18 1.01 0.85 0.8 9 0.87 1.0 1
WM19 0.85 0.89 0.8 9 0.9 0.9 1
WM20 1 0.97 0.9 0.9 0.9 9
WM21 0.97 1.1 0.9 0.96 0.9 7
WM22 0.93 0.98 0.9 3 0.89 1.0 6
WM23 1.02 1.04 0.9 4 0.87 1.0 8
WM24 0.93 1.05 0.9 7 1.05 1.0 5
WM25 0.93 0.95 1.0 7 1.15 0.9 7
IBTKFOXO3BCLAF1TNFAIP3HIVEP2
Hunter,
et al.
Blood
2014

Discovery of CXCR4 mutations in WM -2013-
30-40% of WM patients

Mutations impact the “tail” of the CXCR4 receptor
Adapted from Kahler et al, AIMS Biophysics, 2016S338X
352
Most common
mutation is S338X

MYD88 and CXCR4 Mutation Status Impacts
Clinical Presentation of WM Patients
MYD88WT
MYD88 WT L265P L265P L265P
CXCR4 WT WT FS NS
MYD88 WT L265P L265P L265P
CXCR4 WT WT FS NS
BM (%) sIGM (mg/dL
Treon et al, Blood 2014; 123(18):2791-6.

Drug resistance
Bone Marrow StromaCXCR4
WM Cell
Mutated CXCR4 receptor fails to downregulate after
binding its ligand CXCL12 and remains active
CXCL12
Cao et al; Leukemia 2014; Roccaro et al, Blood 2014

Study O
Opened May 2012 R. Advani L. Palomba
420 mg po qD
Ibrutinib
Progressive Disease (PD) or
Unacceptable Toxicity Stable Disease or Response
Continue
Stop Ibrutinib
Event Monitoring
Event Monitoring
Screening
Registration
www.clinicaltrials.gov
NCT01614821
Multicenter study of Ibrutinib in
Relapsed/Refractory WM (>1 prior therapy)
✔ MYD88, CXCR4
Mutation StatusNCT01614821
R Advani L PalombaS Treon PI

FDA MEETING JUNE 2014
First Drug Approval for Waldenstrom’s Macroglobulinemia

Update of Pivotal Study
• The median time on treatment was19.1 months at time of original studyreporting (NEJM, 2015).
• The median time on treatment forupdated study: 47 months (EHA, 2018)
• Last patient follow-up: October, 2018.

Baseline Characteristics for Study Participants (n=63)
Median Range
Age (yrs) 63 44-86
Prior therapies 2 1-9
Refractory to prior therapy 25 (40%) N/A
Hemoglobin (mg/dL) 10.5 8.2-13.8
Serum IgM (mg/dL) 3,520 724-8,390
B2M (mg/dL) 3.9 1.3-14.2
BM Involvement (%) 60 3-95
Adenopathy >1.5 cm 37 (59%) N/A
Splenomegaly >15 cm 7 (11%) N/A
Treon et al, NEJM 372: 1430, 2015

0
1000
2000
3000
4000
5000
6000
7000
8000
9000
Basel
ine
Cyc
le 2
Cyc
le 3
Cyc
le 6
Cyc
le 9
Cyc
le 1
2
Cyc
le 1
5
Cyc
le 1
8
Cyc
le 2
1
Seru
m I
gM
(m
g/d
L)
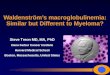
BestIgMResponse:3,520to880mg/dL;p<0.001
N=63
Serum IgM and Hb Levels Following Ibrutinib
BestHemoglobinResponse:10.5to13.8;p<0.001
8
9
10
11
12
13
14
15
16
Bas
eline
Cyc
le 2
Cyc
le 3
Cyc
le 6
Cyc
le 9
Cyc
le 1
2
Cyc
le 1
5
Cyc
le 1
8
Cyc
le 2
1
N=63
He
mo
glo
bin
(g
/dL
)
Serum IgM Hb
Best Hemoglobin Response:10.5 to 13.8; p<0.001
Best IgM Response: 3,520 to 880 mg/dL; p<0.001
Treon et al, N Engl J Med. 2015; EHA 2018
Updated:
Best Hemoglobin Response:10.5 to 14.2; p<0.001
Best IgM Response: 3,520 to 821 mg/dL; p<0.001

ALL MYD88Mut
CXCR4WT
MYD88Mut
CXCR4Mut
MYD88WT
CXCR4WT
P-value
N= 63 36 21 5*
ORR 91% 100% 85.7% 60% 0.005
Major (>PR) 78% 97% 67% 0% <0.001
VGPR 29% 44% 10% 0% 0.007
Time to Minor Response (mos.)
1.0 1.0 1.0 1.0 0.10
Time to Major response (mos.)
2.0 2.0 6.0 N/A 0.05
Responses to ibrutinib are impacted by MYD88 (L265P and non-L265P) and CXCR4 mutations.
*2 patients at initial reporting with major responses were discovered subsequently
to have MYD88 mutated disease (S243N, L265P). One patient at initial reporting
was subsequently found to CXCR4 mutated disease upon genotyping of CD19-
selected WM cells.
Treon et al, EHA 2018

OIbrutinib in Previously Treated WM:
Updated PFS
5 year PFS: 60% (95% CI 46-71%).
All patients MYD88 and CXCR4 Status
MYD88 MUTATED ONLY
BOTH MYD88 AND CXCR4 MUTATED
NO MYD88 OR CXCR4 MUTATIONS
Treon et al, EHA 2018

R
Study O
Opened May 2012 R. Advani L. Palomba
420 mg po qD
Ibrutinib
Progressive Disease (PD) or
Unacceptable Toxicity Stable Disease or Response
Continue
Stop Ibrutinib
Event Monitoring
Event Monitoring
Screening
Registration
www.clinicaltrials.gov
NCT01614821
Ibrutinib Monotherapy in
Symptomatic Treatment Naive WM
✔ MYD88, CXCR4
Mutation Status
Treon et al, JCO 2018NCT02604511

Time to and depth of response to ibrutinib
are impacted by CXCR4 mutations.
All Patients MYD88MUT
CXCR4WT
MYD88MUT
CXCR4MUT P-value
N= 30 16 14 N/A
Overall Response Rate-no. (%)
30 (100%) 16 (100%) 14 (100%) 1.00
Major Response Rate-no. (%)
25 (83%) 15 (94%) 10 (71%) 0.16
Categorical responsesMinor responses-no. (%)
5 (17%) 1 (6%) 4 (29%) 0.16
Partial responses-no. (%)
19 (63%) 10 (63%) 9 (64%) 1.00
Very good partial responses-no. (%)
6 (20%) 5 (31%) 1 (7%) 0.18
Median time to response (months)Minor response (≥Minor response)
1.0 0.9 1.7 0.07
Major response (≥Partial response)
1.9 1.8 7.3 0.01
Median f/u: 14.6 (range 1.8-21.6 months) Data cutoff: Jan. 22, 2018

OIbrutinib Monotherapy in Frontline WM: PFS
18 mo: PFS 92%;
All patients alive.
PD patients were both
CXCR4 mutated.
Median f/u: 14.6 (range 1.8-21.6 months) Data cutoff: Jan. 22, 2018

Ibrutinib (560 mg/day) induced response in a WM patient with Bing Neel Syndrome
Mason et al, BJH 2016

Phase IIII Study of Zanubrutinib vs. Ibrutinib in WM

Strategies to Enhance BTK Inhibitors in WM

ARM B: Placebo
+ Rituximab 375mg/m2 x 8 infusions (weeks 1,2,3,4,17,18,19, and 20)
ARM A: ibrutinib 420mg
+ Rituximab 375mg/m2 x 8 infusions (weeks 1,2,3,4,17,18,19, and 20)
1:1
Randomization
N = 150
ARM C: ibrutinib 420mgSubjects considered
refractory to prior rituximab
N=31
iNNOVATE Study in WMTreatment Naïve + Previously Treated
45 centers in 9 countries
ABC patients genotyped for MYD88 and CXCR4

16 156
17 239
27 22
53
2956
23
58
44
3633
25
3
38
6
15
27
14
0102030405060708090
100
Ibrutinib-RTX
Placebo-RTX
Ibrutinib-RTX
Placebo-RTX
Ibrutinib-RTX
Placebo-RTX
Ibrutinib-RTX
Placebo-RTX
Responses in Innovate AB Study: UpdateB
est
Resp
on
se (
%)
ORR 95%
ORR 48%
aFollowing modified 6th IWWM Response Criteria (NCCN 2014); required two consecutive assessments.
MYD88L265P/CXCR4WT MYD88L265P/CXCR4WHIM MYD88WT/CXCR4WT
ORR 100%
ORR 46%
ORR 96%
ORR 57%
ORR 91%
ORR 56%
CRVGPR
PR
MR
Median time to ≥PR,
months (range)2
(1–28)
6
(2–26)
2
(1–28)
5
(2–17)
3
(1–19)
11
(4–18)
6
(1–17)
6
(5–26)
Median time to ≥MR,
months (range)1
(1–18)
3
(1–24)
1
(1–18)
3
(1–24)
1
(1–11)
3
(1–8)
2
(1-17)
3
(2–17)
Overall
Major
33%
Major
79%
Major
29%
Major
94%
Major
48%
Major
73%
Major
33%
Major
64%
??
Buske et al, ASH 2018

Progression-Free Survival Benefit: Impact of MYD88/CXCR4 Genotype
• Improved PFS
with ibrutinib
• 36-month PFS
rates
▪ MYD88L265P/CXCR4WT:
84% vs 29%
▪ MYD88L265P/CXCR4WHIM:
64% vs 26%
▪ MYD88WT/CXCR4WT:
82% vs 44%
MYD88L265P/CXCR4WT
Pro
gres
sio
n-F
ree
Surv
ival
(%
)
Months
MYD88WT/CXCR4WT
MYD88L265P/CXCR4WHIM
MYD88L265P/CXCR4WHIM
MYD88WT/CXCR4WT
MYD88L265P/CXCR4WT
Ibrutinib-RTX
RTX
Innovate AB Data: Buske et al, ASH 2018.

Phase I/II Trial of Ulocuplumab and Ibrutinib in
CXCR4 mutated patients with symptomatic WM
Ibrutinib Until PD or
Intolerance
Weekly Ulo
4 weeks
Biweekly Ulo
20 weeks
ClinicalTrials.gov Identifier: NCT03225716
STOP
Dose Level Ibrutinib Ulocuplumab Cycle 1 Ulocuplumab Cycles 2-6
Level 1 –Starting dose 420mg PO DQ 400 mg weekly 800 mg every other week
Level 2 420mg PO DQ 800 mg weekly 1200 mg every other week
Level 3 420mg PO DQ 800 mg weekly 1600 mg every other week
Schema

Serial IgM Levels for Evaluable PatientsDose Level 1 (ongoing)
WM Pt

Venetoclax (ABT-199) augments
ibrutinib induced apoptosis
Cao et al, BJH 2015
BCWM.1
MWCL-1
CleavedPARP
CleavedCaspase3
CleavedPARP
CleavedCaspase3
GAPDH
DM
SO
IB
A
BT
A
BT
/IB
A
BT
/IB
/CX
CL1
2
AB
T/IB
/CX
CL1
2/A
MD
D
MS
O
IB
AB
T
AB
T/IB
A
BT
/IB
/CX
CL1
2
AB
T/IB
/CX
CL1
2/A
MD
GAPDH
CXCR4WT CXCR4S338X
Higher BCL2 levels in
MYD88 mutated WM

Screening
Informed Consent and Registration
Venetoclax
200 mg PO QD
800 mg PO QDProgressive Disease or
Unacceptable Toxicity
SD or Response →
Continue for 2 years
Stop ABT-199 Event Monitoring
www.clinicaltrials.gov: NCT02677324
Phase II Study of Venetoclax in Previously Treated WM
Selected inclusion
criteria:
• Clinicopathological
diagnosis of WM
• Serum IgM >2 x
ULN
• Previously treated
• Age ≥18 years
• Good performance
• Normal organ and
marrow function
Selected exclusion
criteria:
• Serious medical
condition
• Concurrent anti-
cancer agent
• Known CNS
lymphoma
• Active HIV, HBV,
HCV infection
• Lactating or
pregnant women
Castillo et al. EHA 2018

Phase II Study of Venetoclax in Previously Treated WM
ResponseNo prior ibrutinib
(n=15)
Prior ibrutinib
(n=15)
Overall 14 (93%) 12 (80%)
Major 13 (87%) 9 (60%)
Very good 4 (27%) 1 (7%)
Partial 9 (60%) 8 (53%)
Minor 1 (7%) 3 (20%)
Stable 1 (7%) 3 (20%)
CXCR4 WT
(n=14)
CXCR4 MUT
(n=16)
12 (86%) 14 (87%)
9 (86%) 13 (63%)
4 (29%) 1 (7%)
8 (57%) 9 (56%)
0 (0%) 4 (25%)
2 (14%) 2 (13%)
1 patient had progressive disease at 9 months (MYD88, CXCR4, TP53)
Castillo et al. EHA 2018
Median follow-up: 11 months

Ibrutinib and Venetoclax in Treatment Naïve WM
Ibrutinib
420 mg/day
x 4 weeks
Ibrutinib
420 mg/day
Add Venetoclax100 mg/day week 5
200 mg/day week 6
400 mg/day weeks 7,8
Ibrutinib
420 mg/day
And
Venetoclax
400 mg/day
Observation
4 weeks 4 weeks 22 months Follow to PD
or off study
24 months
Jorge Castillo, PI (DFCI)

BTK Cys481 Mutations accompany CXCR4 in WM Patients on Ibrutinib.
Patient*
L265P positive cells
with BTK C481RT>C
L265P positive cells
with BTK C481ST>A
L265P positive cells
with BTK C481SG>C
L265P positive cells
with BTK C481YG>A
L265P positive cells with PLCG2
Y495HT>C
L265P positive cells
with CARD11 L878FC>T
P1 None None None None None None
P2 32.4% 6.6% 5.8% 1.0% None None
P3 0.3% 34.4% 6.5% 0.3% None 0.2%
P4 None None None None None None
P5 None None None None None None
P6 None None 10.3% None 11.9% None
Targeted next-generation sequencing for MYD88, CXCR4, BTK, PLCG2, CARD11, LYN.
All patients are MYD88 Mutated.
P2, P3, P6 are CXCR4 WHIM Mutated. Xu et al, BLOOD 2017

BTK C481S cells show uniform ERK 1/2 activation
in the presence of ibrutinib.
Chen et al,
Blood 2018

Ulixertinib blocks ERK-downstream signaling and overcomes
mutated BTK Cys 481 resistance to ibrutinib.
Chen et al, BLOOD 2018


BTK mutated cells release inflammatory cytokines in the presence of
ibrutinib that can be blocked by ERK-inhibitor.
Chen et al, BLOOD 2018

Y
Y
Y Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
YYY
Y
YY
Y
Y
Y
Y
YY
Y
BTKWT
BTKWT
BTKCys481Ser
BTKWT
BTKCys481Ser
BTKWT
+anti-IL6 and -IL10 Abs
BTKCys481Ser mutated clones release cytokines that protect
BTKWT clones from ibrutinib triggered cytotoxicity
Chen et al, Blood 2018
+ibrutinib
IL6
IL10IL6
IL10
+ibrutinib +ibrutinib

BTK mutated clones.. Bad apples that spoil the bunch?

Ibrutinib
+ ERK-inhibitor
DFCI/ELI LILLY COLLABORATION
Phase I/II Clinical Trial of the oral ERK inhibitor LY3214996 in
BTK Cys 481 and PLCG2 mutated CLL, WM, MZL, MCL
S. Treon, PI

Bing Center for WM

www.IMW2019boston.org
REGULAR AND YIA
ABSTRACT DEADLINE
June 19, 2019
LATE BREAKING
July 24, 2019