Embed Size (px)
Citation preview

Walking Velocity in Aged Persons: Its AssociationWith Lower Extremity Joint Range of MotionAGUSTIN ESCALANTE,1 MICHAEL J. LICHTENSTEIN,2 AND HELEN P. HAZUDA3
Objective. To measure the association between walking velocity and hip and knee flexion range, ethnic background,anthropometrics, comorbid pathologies, and coimpairments, in a sample of community-dwelling aged persons.Methods. To reach our objective, we used data from the San Antonio Longitudinal Study of Aging (SALSA), a population-based cohort of Mexican American and European American persons aged 64 to 79. By fitting hierarchical regressionmodels, we measured the variance in the walking velocity over 50 feet explained by hip and knee flexion range, adjustingfor the combined influence of demographic and anthropometric variables, coexistent pathologic conditions, impairments,and the examiners who conducted the assessments.Results. The average walking velocity among the 702 subjects for whom data were available was 73.6 meters per minute(range 20 to 121). Bivariate analyses revealed significant associations between walking velocity and age, sex, ethnicbackground, height, weight, presence of arthritis, diabetes mellitus, stroke, upper leg pain, peripheral vascular disease,left ventricular hypertrophy, and forced expiratory volume at 1 second. The correlation (r) between walking velocity andflexion range of the hip and knee were 0.40 and 0.35, respectively (P < 0.001 for each). Multivariate hierarchical modelsadjusting for demographic and anthropometric characteristics of the subjects, and examiner variation, revealed that hipand knee flexion range explained 6% of the variance in walking velocity. Adjusting for the presence of comorbidconditions and coimpairments reduced the variance attributable to hip and knee flexion range only slightly, to 5%.Conclusion. Hip and knee flexion range contribute significantly to walking velocity in the SALSA cohort of community-dwelling aged persons.
KEY WORDS. Hip; Knee; Joint range of motion; Walking velocity; Diabetes mellitus; Mexican Americans.
INTRODUCTION
Joint range of motion (ROM) is important to normal phys-iology because it enables displacement of the body and its
parts in space. Owing to joints in the upper extremities,hands can be placed in the required location for graspingand manipulating objects. Lower extremity joints permitthe individual to cover distances required to be in prox-imity with the environment. Impairments in the ability tomove joints through their normal ROM can result in sig-nificant physical functional limitations and disability.
Because the statements above appear self-evident, fewinvestigators have measured the functional consequencesof impaired articular ROM in population-based studies.Most published studies about joint ROM come from clin-ical populations affected by articular pathology (1,2) or bynonarticular conditions that can impair ROM, such asdiabetes mellitus (3,4). The few studies of articular func-tion among persons unselected for any pathology have notevaluated the contribution of ROM to other measures ofphysical function (1,2,5,6). We present data that build onour previous report describing the hip and knee flexionrange among subjects participating in the San AntonioLongitudinal Study of Aging (SALSA) (7), a population-based study of Mexican American and European Americanaged persons. The purpose of the present report is toexamine the association between the velocity of ambula-
Supported by NIA grant 1-RO1-AG10444 and by NIHgrant M01-RR-01346 for the Frederick C. Bartter GeneralClinical Research Center. Dr. Escalante’s work was sup-ported in part by an award from the Robert Wood JohnsonMinority Medical Faculty Development Program.
1Agustı́n Escalante, MD, Division of Clinical Immunologyand Rheumatology, Department of Medicine, The Univer-sity of Texas Health Science Center at San Antonio; 2Mi-chael J. Lichtenstein, MD, Division of Geriatrics and Geron-tology, Department of Medicine, The University of TexasHealth Science Center at San Antonio, and Geriatric Re-search and Education Center (GRECC) (182), South TexasVeterans Health System–Audie Murphy Division; 3Helen P.Hazuda, PhD, Division of Clinical Epidemiology, Depart-ment of Medicine, The University of Texas Health ScienceCenter at San Antonio.
Address correspondence and reprint requests to Helen P.Hazuda, PhD, 7703 Floyd Curl Drive, San Antonio, TX78284.
Submitted for publication November 8, 1999, accepted inrevised form February 15, 2001.
ARTHRITIS CARE & RESEARCH 45:287–294, 2001
ORIGINAL ARTICLE
© 2001, American College of RheumatologyPublished by Wiley-Liss, Inc. 287

tion over 50 feet, an important measure of physical func-tion (8), and the flexion range of hips and knees amongSALSA participants. We took into account the concurrentinfluence of sex and ethnic background, anthropometrics,coexistent pathologic conditions and impairments in otherorgans, and examiner variation on velocity of ambulation.We demonstrate the influence of these variables on theodds of being among the slowest walkers in our studysample, and we show the associations between the differ-ent variables measured in this analysis.
SUBJECTS AND METHODS
Details of the design and procedures employed in SALSAhave been described previously (7,9). Briefly, SALSA is afollowup of the San Antonio Heart Study (SAHS) (10,11),for which households were randomly sampled from low-,middle-, and high-income San Antonio neighborhoods be-tween October 1979 and November 1982, and later be-tween October 1984 and October 1988. The strategy wasaimed at providing a cohort with comparable numbers ofMexican Americans (MA) and European Americans (EA),while maximizing sociocultural variation among MA inthe study. All men and nonpregnant women between 25and 64 years of age in the sampled households were eligi-ble for the study. The overall response rate for the SAHSwas 65.3% for a total of 5,158 community-dwelling sub-jects enrolled.
In 1991, the oldest SAHS subjects, aged 65 to 78, wererecruited for SALSA to participate in a comprehensive2-part evaluation. The first part was a home-based assess-ment (HBA), conducted in subjects’ homes. The secondpart, a performance-based assessment (PBA), was con-ducted in a clinical research center. Of 1,247 eligibleSAHS subjects, 166 (13.3%) had died prior to the start ofSALSA. Of the 1,081 survivors, 888 were recruited suc-cessfully, and 833 (77.1% of survivors) completed thehome-based assessment. The performance-based assess-ment was conducted with 749 subjects, 709 of whom wereable to come to the Frederick C. Bartter General ClinicalResearch Center, located at the Audie L. Murphy VeteransAdministration Hospital.
Home-based assessment. The HBA consisted of a com-prehensive, 3-hour interview that assessed chronic dis-eases, impairments, functional limitations, disability, andvarious modifiers of the disablement process. It was con-ducted by trained personnel using a standardized proto-col. Variables measured during the HBA that were em-ployed in the current analysis are listed below:
1. Demographic characteristics. Age, sex, and ethnicbackground were noted. Ethnic background was classifiedas MA or EA according to the definitions of the SAHS (12).
2. Pain. The presence or absence of pain was assessedusing the second question of the McGill Pain Question-naire (MPQ), “During the past week, how much of the timehave you been troubled by pain?” (13). Subjects respond-ing “rarely” to “most of the time” were administered thefull MPQ, including the pain map. The pain map consistsof anterior and posterior projections of the human body,
where subjects’ painful areas are marked. The map isscored by overlaying a plastic template of the map, dividedinto 36 anatomic areas, over the figure with the subjects’painful areas marked. Marks in the groin, buttocks, orthighs were considered indicative of hip pain, and marksin the knee were considered indicative of knee pain. Wehave demonstrated the validity and reliability of the painmap in our populations (14,15).
A cross-culturally adapted and validated Spanish-lan-guage version of the questionnaire was used for Spanish-speaking subjects (16). We previously developed a factorstructure for pain location and demonstrated associationsbetween pain and self-reported physical functional limi-tations (17). Using this structure, pain in the upper legincludes hip and knee pain. Pain in the lower leg includespain distal to the knee (17).
3. Arthritis. Arthritis was ascertained by self-report, us-ing the question “Have you ever been told by a doctor thatyou have arthritis?” Subjects answering in the affirmativewere considered to have arthritis. This approach is similarto the one employed in large epidemiologic studies ofaging such as the Longitudinal Study of Aging (18) and theEstablished Populations for Epidemiologic Studies of theElderly (19).
4. Diabetes. Diabetes was established using the WorldHealth Organization criteria based on a fasting plasmaglucose of $ 140 mg/dl, a 2-hour post–glucose loadplasma glucose $ 200 mg/dl, or the current use of antidia-betes medications (20). Diabetes severity was measured onan ordinal scale, where the value of 0 was assigned tosubjects who were not diabetic, 1 to subjects with diabeteswho were not receiving insulin, and 2 to subjects whowere receiving insulin.
5. Stroke. The existence of a stroke was ascertainedbased on participants’ response to 2 questions: “Have youever been told by a doctor that you had a small stroke ormini-stroke?” and “Have you ever been told by a doctorthat you had a major stroke?” Stroke was consideredpresent if participants answered “yes” to either question,and absent if they answered “no” to both.
Performance-based assessment. The full assessmenttook approximately 3 hours for each subject, during whichanthropometric features, physical measures of cardiovas-cular disease, cardiopulmonary, neurosensory, and mus-culoskeletal impairments, and performance-based mea-sures of upper and lower extremity functional limitationswere assessed. These assessments were conducted by oneof 2 trained research nurses or 2 physicians following astandardized protocol. The following variables employedin the current analysis were measured during the PBA:
1. Height and weight. Weight was measured in kilo-grams using a clinical scale, height in centimeters using astandard tape. Body mass index (BMI) was calculated asthe weight divided by the squared height. Subjects wereclassified as overweight for BMI $ 27.8 kg/m2 for menand $ 27.3 kg/m2 for women. Severely overweight wasdefined as $ 31.1 kg/m2 for men and $ 32.3 kg/m2 forwomen (21).
288 Escalante et al Vol. 45, No. 3, June 2001

2. Waist:hip ratio. The waist circumference at the levelof the umbilicus was divided by the hip circumference atthe level of the greater trochanters and expressed as acontinuous variable.
3. Joint range of motion. Passive flexion of the kneeswas measured in the clinical research center with subjectssupine, using a standard goniometer, as described (22).Passive hip flexion was measured with a Cybex EDI Incli-nometer (Ronkonkoma, NY) (22). Agreement between the4 examiners who measured hip and knee flexion was eval-uated in a sample of 24 ambulatory adults between theages of 65 and 80 years. The mean hip flexion (6 SD)among the 4 examiners was 125° 6 16°. The maximumdifference between examiners averaged 25° 6 10° in themeasurement of hip flexion, and 14° 6 6° in the measure-ment of knee flexion. The intraclass correlation coefficientamong the 4 examiners was 0.61 for hip flexion and 0.46for knee flexion. Extrapolating guidelines for the interpre-tation of weighted kappa (23,24), which is equivalent tothe intraclass correlation in measuring agreement (25), weconsidered that our measurements of hip and knee flexionrange were sufficiently reliable for the analyses at hand.Nevertheless, because of the observed differences betweenobservers in measuring hip and knee ROM, we adjusted forthe effect of the examiners in all multivariate models.
4. 50-foot walking velocity. Subjects were timed with astopwatch as they walked 50 feet, starting from a standingposition, at their usual pace in a tiled, straight, flat hall-way, with the examiner walking alongside the subject. Noeffort was made to conceal the stopwatch from partici-pants. Results are expressed in meters per minute. Theaverage of 2 measurements is employed in this analysis.
5. Electrocardiogram. A 12-lead electrocardiogram(EKG) was obtained with the subject lying flat on an ex-amining table. The EKG was interpreted to determinewhether left ventricular hypertrophy was present usingstandardized criteria (26).
6. Spirometry. Spirometry was performed with the sub-ject seated, using a hand-held spirometer (Welch-AllynPneumocheck, Skaneateles, NY). Three measurements offorced expiratory volume at 1 second (FEV1) were ob-tained and averaged. In our hands, this system compareswell with clinically employed spirometry (r 5 0.98) (27).
7. Peripheral vascular disease. Peripheral vascular dis-ease (PVD) was assessed using the ankle–brachial index.Doppler measurements of supine ankle and arm systolicblood pressures were taken. The ankle:arm systolic bloodpressure ratio was calculated for the posterior tibial anddorsalis pedis arteries on both legs relative to the mean ofthe right and left brachial systolic blood pressure. PVD isconsidered present if at least one of the 4 ankle:arm ratiosfrom the right or left posterior tibial or dorsalis pedisarteries is , 0.95 (28).
Analyses. Descriptive comparisons of dichotomousvariables in the entire sample were performed using oddsratios (OR) and 95% confidence intervals (CI). For descrip-tive purposes, the slowest 10% of the population werelabeled as “slow walkers,” and hip and knee ROM weredivided into quartiles (29). Pearson product-moment cor-
relation coefficients were calculated to measure bivariateassociations between walking velocity and other measureswith an interval distribution (30).
To quantify the influence of hip and knee flexion rangeon walking velocity, hierarchical regression models wereconstructed using walking velocity as the dependent vari-able (31). Groups of variables were entered sequentially in5 stages. The first stage contained demographics, the sec-ond anthropometrics. In the third stage, hip and kneeflexion range were entered. To isolate the influence ofcoexistent pathologic conditions and impairments, we in-cluded these variables in the fourth stage, excluding hipand knee flexion range. The fifth model included allgroups of variables. The explanatory contribution of eachgroup of variables within the overall model was estimatedfrom the value of R2 in each stage. To adjust for the pos-sibility of examiner bias, we included indicator variablesfor each rater as covariates in all regression models. Allparts of the analysis were performed on a personal com-puter using the Intercooled Stata statistical software, ver-sion 6.0 (Stata Corporation, College Station, Texas).
RESULTS
Descriptive analyses. Walking velocity was measuredon 702 SALSA participants who attended the GeneralClinical Research Center. These represented 65% of survi-vors of the SAHS who were eligible for SALSA, 84% ofsubjects who participated in the home-based assessment,and 99% of those who attended the clinical research cen-ter. Overall response rates and demographic, anthropomet-ric, and clinical characteristics of the SALSA cohort havebeen described previously (7,9). Nonresponders had sig-nificantly fewer years of education than responders andwere more likely to be MA. There were no differences inage, sex, or prevalence of diabetes mellitus or arthritisbetween responders and nonresponders.
Participants in our study were examined by one of 4examiners: 2 registered nurses who were women and 2physicians who were men. All were trained in the properperformance of the performance-based assessments. Walk-ing velocity differed significantly between subjects as-sessed by the different examiners, from a mean (6 SD) of58.3 meters per minute (6 17 meters per minute), amongthe 47 persons assessed by examiner 2, to 77.3 meters perminute (6 16 meters per minute) among the 187 assessedby examiner 4 (P # 0.001). Examiner 1 assessed 107 sub-jects and examiner 3 assessed 361.
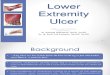
Walking velocity in the 702 subjects assessed averaged73.6 meters per minute (standard deviation 15.9, median74.7, range 20.6 to 121.8) (Figure 1). Bivariate comparisonsin walking velocity according to demographic characteris-tics and the pathologies and impairments considered inthis analysis are shown in Table 1.
We considered the 71 subjects in the slowest decile to be“slow walkers,” among whom the walking velocity aver-aged 41.8 meters per minute (standard deviation 12.1,range 6.4 to 55.1). Mexican Americans were more likelythan European Americans to be slow walkers (OR 3.25;95% CI 1.85, 5.69; P # 0.001), as were persons with dia-
Arthritis Care & Research Walking Velocity and Joint Range of Motion 289

betes mellitus (OR 3.11; 95% CI 1.90, 5.12; P # 0.001), paststroke (OR 2.83; 95% CI 1.43, 5.63; P 5 0.002), peripheralvascular disease (OR 3.26; 95% CI 1.85, 5.73; P # 0.001),electrocardiographic signs of left ventricular hypertrophy(OR 2.01; 95% CI 1.07, 4.08; P 5 0.03), or obesity (OR 2.05;95% CI 1.22, 3.45; P 5 0.006). Persons with pain weremore likely to be slow walkers only if the pain was locatedin the upper leg region, which included the hip and knee(OR 2.03; 95% CI 1.23, 3.37; P 5 0.006). Among partici-pants with self-reported, physician-diagnosed arthritis,there was a trend toward being a slow walker, which didnot reach the traditional definition of statistical signifi-cance (OR 1.52; 95% C.I. 0.93, 2.51; P 5 0.09). Sex was notassociated with an increased likelihood of being a slowwalker.
The probability of being a slow walker was significantlyhigher among participants whose hip and knee ROM werein the lowest quartiles (Table 2). However, we observed a
reverse J–shaped association between the hip and kneeROM quartiles and slow walking, with the probability ofbeing slow rising slightly in the highest ROM quartiles(Figure 2).
Associations among variables. Bivariate correlation co-efficients among age, height, weight, hip and knee flexionrange, and FEV1 are shown in Table 3. As expected, walk-ing velocity was significantly correlated in a positive di-rection with height, hip and knee flexion range, and FEV1.The magnitude of the coefficients was modest to moderate.We previously showed that hip and knee flexion rangecorrelate negatively with BMI (7). Table 3 demonstratesthat weight has a negative influence on the flexion range ofthese 2 joints, while the influence of height is variable andmodest.
Hierarchical models. The multistage regression modelsof walking velocity are shown in Table 4. Model 1 exam-ines the combined influence of the demographic charac-teristics alone (age, sex, and ethnic background), whichexplained 18% of the variance in walking velocity (R2 50.18). In model 2, height and weight were included in themodel, with a corresponding increase in explanatorypower to 25%, and a loss in the significant influence of sexon walking velocity (model 2, Table 4). In model 3, hip andknee flexion range were added, with a resulting increase inexplained variance to 31%, or an incremental varianceattributable to hip and knee flexion range of 6%. Of note,inclusion of hip and knee flexion range resulted in a loss ofsignificance for the influence of weight on walking veloc-ity.
In the following stage, we added the 3 pathologic con-ditions and 5 impairments that we ascertained, leaving outhip and knee flexion range (model 4, Table 4). This modelexplained 33% of variance in walking velocity. Of note inmodel 4 is that diabetes mellitus and stroke were associ-ated with reduced walking velocity, but self-reported phy-sician-diagnosed arthritis was not. However, upper legpain, an impairment often related to hip or knee arthritis,
Figure 1. Distribution of walking velocity among 702 members ofthe San Antonio Longitudinal Study of Aging cohort. Subjectswere timed walking 50 feet over a flat indoor surface. Meanwalking velocity was 73.6 meters per minute (median 74.7, range20.6 to 121.8).
Table 1. Bivariate comparison in walking velocity in the San Antonio LongitudinalStudy of Aging cohort (n 5 702)
Walking velocity*(meters per minute)
Characteristic Present Absent P value
Male sex (n 5 299) 76.9 6 15.1 71.1 6 16.0 # 0.001Mexican American ethnic background (n 5 366) 70.1 6 16.6 77.3 6 14.2 # 0.001Arthritis† (n 5 326) 71.5 6 16.3 75.4 6 15.2 0.001Diabetes mellitus (n 5 200) 68.3 6 17.5 75.6 6 14.7 # 0.001Stroke (n 5 54) 64.3 6 19.7 74.3 6 15.3 # 0.001Pain‡ (n 5 321) 71.8 6 16.7 75.0 6 15.0 0.008Peripheral vascular disease (n 5 96) 67.1 6 18.3 74.9 6 15.0 # 0.001Left ventricular hypertrophy (n 5 68) 67.1 6 14.3 74.2 6 15.9 # 0.001
* Measured over a distance of 50 feet, starting from a standing position. Mean 6 SD.† A positive response to the question “Has a doctor ever told you that you have arthritis?”‡ In response to the question “During the past week, how much of the time have you been troubled bypain?” Persons responding “Rarely,” “Some of the time,” “Occasionally,” or “Most of time” wereconsidered to have pain.
290 Escalante et al Vol. 45, No. 3, June 2001

was associated with a loss of walking velocity rangingfrom 1.43 to 6.57 meters per minute (model 4, Table 4).This effect remained even after including hip and kneeflexion range in the next model (model 5, Table 4). Thisfinal model explained 38% of the variance in walkingvelocity. The incremental variance associated with hipand knee flexion range, adjusting for 3 comorbid condi-tions and 5 coimpairments, was 5%.
We included indicator variables for the 4 examiners ascovariates in each of the multivariate models. All modelsdemonstrated a significant influence of the examiners onwalking velocity, contributing 5% of variance in model 1and 3% in model 5.
DISCUSSION
Disability develops as a sequence of linked events thatbegins with a pathologic condition. This condition causesimpairments, which then lead to functional limitations,and finally to disability (32). Our intent in this analysiswas to evaluate the link between a measure of impairment,hip and knee flexion range, and a measure of functionallimitation, walking velocity, within the framework of thedisablement process (32). Using hierarchical regression,we assembled a series of models, each representing a stagein the disablement process. Models 1 and 2 representcontextual and anthropometric background characteris-tics, and model 3 measures the influence of hip and kneeflexion range on walking velocity without considering the
competing influence of pathologies or other impairments.Model 4 measures the influence of pathologies and otherimpairments, and model 5 shows the full model. Becausewe were only interested in measuring the link betweenimpairment and functional limitation, we did not includea measure of disability in these models. It can be antici-pated that impaired hip and knee flexion range, actingthrough impaired walking velocity, would lead to disabil-ity in activities that require the lower extremities, such asgrocery shopping, getting in a car to go visit friends, orgoing to church.
The normal function of joints is to move within a certainrange, to allow displacement of the body in space. Impair-ments in joint range of motion should result in reductionsin an individual’s capacity to move within his environ-ment, which in turn should be measurable as reducedmobility. Following this line of reasoning, we have dem-onstrated the contribution of hip and knee flexion range towalking velocity. In fact, we found that an aged person’sodds of being in the slowest decile of walking velocitywere between 2.56 and 5.59 times higher if he or she wasin the lowest hip or knee ROM quartile. Moreover, wefound that the flexion range of these 2 major lower extrem-ity joints explains 5% to 6% of the variance in the 50-footwalking velocity of community-dwelling aged persons.Based on the size of the regression coefficients in ourmodels, for every additional degree of hip flexion range,there was a corresponding increment in velocity rangingfrom 0.13 to 0.28 meters per minute (Table 4, model 3).This increment remained nearly unchanged after account-ing for comorbid conditions and coimpairments.
The hierarchical modeling approach we used allowed usto isolate the influence of hip and knee flexion range fromthat of other factors that contribute to the speed of ambu-lation, such as age, sex, ethnic group, height, comorbidconditions and coimpairments, and inter-examiner varia-tion. The finding that the incremental R2 associated withhip and knee flexion range was very similar before andafter accounting for the influence of comorbid conditionsand coimpairments supports the notion that the influenceof the 2 joints is independent of other important determi-nants of walking velocity.
The probability of being in the slowest decile of walkingvelocity increased slightly among the persons in the high-est ROM quartiles compared with those in the secondhighest quartiles (Figure 2). Thus, the association is likely
Figure 2. Associations between quartiles of hip and knee range ofmotion (ROM) (see Table 2 for quartile cutoff points) and theprobability of being in the slowest decile of walking velocity(# 55.1 meters/minute).
Table 2. Odds of San Antonio Longitudinal Study of Aging participants being in the slowest decile of walking velocity,according to quartiles of hip or knee range of motion (ROM).
Right hip Left hip Right knee Left knee
ROMquartile ROM
Odds ratio(95% CI)* ROM
Odds ratio(95% CI)* ROM
Odds ratio(95% CI)* ROM
Odds ratio(95% CI)*
1 137° to 164° 1.00 (referent) 136° to 167° 1.00 (referent) 146° to 166° 1.00 (referent) 147° to 174° 1.00 (referent)2 126° to 136° 0.68 (0.21, 2.19) 125° to 135° 0.40 (0.12, 1.30) 139° to 145° 0.65 (0.26, 1.67) 141° to 146° 0.50 (0.20, 1.25)3 114° to 125° 2.17 (0.86, 5.45) 112° to 124° 1.16 (0.49, 2.76) 134° to 138° 1.54 (0.68, 3.49) 135° to 140° 0.73 (0.32, 1.68)4 29° to 113° 5.69 (2.39, 13.56) 24° to 111° 5.05 (2.37, 10.75) 33° to 133° 2.88 (1.39, 5.98) 42° to 134° 2.56 (1.30, 5.07)
* CI 5 Confidence interval.
Arthritis Care & Research Walking Velocity and Joint Range of Motion 291

to be nonlinear. This reverse J–shaped association is likelydue to frailty, because the persons in the highest ROMquartile also had the lowest BMI (data not shown). In thesepersons, factors other than joint ROM, such as weakness,decreased endurance, or other impairments that we didnot account for in this analysis, are the likely cause ofreduced walking speed.
In addition to our results concerning the influence of hipand knee flexion range on walking velocity, several aspectsof our study warrant discussion. The first is that the sig-nificant positive association between male sex and walk-ing velocity is lost when anthropometrics (i.e., height) areentered into the model (Table 4, model 2). This suggeststhat the reason men in our study walked faster is that theyare taller and thus have a larger stride. Also of interest isthat the influence of sex was reversed in the full model(Table 4, model 5). In other words, when height, hip andknee flexion range, comorbidity, and coimpairment areheld constant, women walk faster than men in the SALSAcohort (7).
Mexican Americans were slower than the EuropeanAmericans in our cohort and were more than 3-fold morelikely than EA to be slow walkers. This finding persistedeven through model 5, which accounted for all variablesstudied. In the SALSA cohort, MA are more likely to havediabetes mellitus, obesity, peripheral vascular disease, andimpaired hip ROM, all of which are associated with slowerwalking velocity. The persistence of an ethnic differenceafter adjustment for a number of disease and impairmentfactors may be due to cultural differences (33). MA mayinterpret the specific task of walking 50 feet at their usualpace differently from EA. The difference in walking veloc-ities between the 2 ethnic groups does not necessarilyimply that MA may have more functional limitations thanEA. Rather, this difference points out the importance ofcross-cultural adaptation of performance-based measures,as is done with self-report instruments, in multiculturalresearch (34). Alternatively, ethnic group–specific cutoffpoints may be necessary to compare functional limitationsand disability between ethnic groups.
The influence of hip and knee flexion range was inde-pendent of cardiovascular and peripheral vascular impair-ments. This is noteworthy in that walking velocity wasmeasured over a distance of 50 feet, rather than the more
often used 8- or 10-foot measure. The distance we em-ployed may be more likely to require that subjects mobi-lize their cardiovascular reserves. Indeed, peripheral vas-cular impairment was associated with reduced walkingvelocity (Table 4, model 4), but this association was lostwhen hip and knee flexion range were accounted for (Ta-ble 4, model 5). This is additional evidence of the impor-tance of joint ROM.
We cannot prove a causal link between impaired hipand knee flexion range and reduced walking velocity witha cross-sectional study such as this one. However, a plau-sible chain of events would link impaired hip and kneeflexion range to restricted stride length. This would causewalking speed to drop when the person is not able tocompensate by increasing stride frequency.
Clinicians and researchers should recognize impairedROM in hips and knees in their elderly subjects, in order toimplement corrective measures. This would likely im-prove their physical function and ultimately reduce dis-ability. Although there have not been any studies directlyevaluating the effect of interventions to increase ROM onthe level of disability or quality of life, there is an ampleliterature demonstrating a beneficial effect on these 2 out-comes for 2 interventions that enhance joint ROM: totalhip replacement and total knee replacement (35). These 2procedures reduce arthritis pain as well, but it is likelythat their salutary effects are mediated, at least in part, bycorrecting impaired ROM (36).
We did not have any information on the anatomic site ofarthritis in any of the subjects in our study. This probablyexplains the lack of effect of self-reported, physician-diag-nosed arthritis on walking velocity, as a subject reportingarthritis in our study could have osteoarthritis of the handsbut normal hips and knees, and therefore normal ambula-tion. A clue to the potential influence of arthritis is pro-vided by the association of upper leg pain with reducedwalking velocity, as arthritis is often associated with painin SALSA members.
Strengths of our study include the population-basedsource of our subjects and the comprehensive nature ofdata collected. Our multivariate analytic approach is also astrength because it allowed us to quantify the contributionof hip and knee flexion range, measured as continuousvariables, to walking velocity, while at the same time
Table 3. Bivariate comparisons in variables measured in the San Antonio Longitudinal Study of Aging cohort*
Walkingvelocity Age Height Weight
Waist:hipratio
Hipflexionrange
Kneeflexionrange
Age 20.17† – – – – – –Height 0.36† 20.03 – – – – –Weight 20.00 20.11‡ 0.45† – – – –Waist:hip ratio 20.13† 0.04 0.06 0.35† – – –Hip flexion range 0.40† 0.05 0.26† 20.23† 20.14† – –Knee flexion range 0.35† 0.01 20.16† 20.32† 20.11‡ 0.61† –FEV1 0.38† 0.17† 0.58† 0.25† 0.07 0.23† 0.25†
* Values shown are Pearson correlation coefficients. FEV1 5 forced expiratory volume at 1 second.† P # 0.001.‡ P # 0.01.
292 Escalante et al Vol. 45, No. 3, June 2001

accounting for the influence of potential confounders. Ourstudy also has some limitations. In addition to the unavail-ability of information about arthritis location, the cross-sectional design prevents us from making strong causal
inferences. We have been cautious to frame our results asassociations and influences rather than effects, so as not toimply causation.
There was inter-examiner variation in our measurement
Table 4. Hierarchical regression model of the influence of hip and knee flexion range on walking velocity in the SALSAcohort, adjusting for demographic and anthropometric characteristics, pathologic conditions, and coexistent impairments*
Model 1Demographics 1
examiners
Model 2Demographics 1anthropometrics
1 examiners
Model 3Demographics 1anthropometrics1 hip and kneeflexion range 1
examiners
Model 4Demographics 1anthropometrics1 pathologies 1impairments 1
examiners
Model 5Demographics 1anthropometrics1 hip and kneeflexion range 1pathologies 1
impairments 1examiners
Age, years (60 to 74) 21.01†(21.34, 20.68)
20.98†(21.30, 20.66)
20.78†(21.09, 20.47)
20.68†(21.00, 20.36)
20.58†(20.89, 20.27)
Sex (men 5 1, women 5 0) 5.13†(2.89, 7.36)
21.32(24.61, 1.97)
21.04(24.21, 2.12)
22.72(26.04, 0.60)
22.66(25.88, 0.56)
Ethnic background (MexicanAmerican 5 1, EuropeanAmerican 5 0)
27.37†(29.55, 25.19)
22.31‡(25.06, 20.17)
23.06‡(25.42, 20.69)
22.31(24.71, 0.85)
22.45‡(24.77, 20.12)
Height, cm (136 to 190) – 0.65†(0.47, 0.83)
0.36†(0.18, 0.55)
0.47†(0.29, 0.66)
0.27§(0.08, 0.45)
Weight, kg (36.8 to 157.4) – 20.18†(20.26, 20.10)
20.02(20.07, 0.11)
20.19†(20.27, 20.11)
20.01(20.10, 0.08)
Waist:hip ratio – 217.6‡(232.83, 22.45)
215.16‡(229.89, 20.43)
26.99(222.00, 8.02)
24.99(219.69, 9.70)
Hip flexion range, degrees (33 to163)
– – 0.24†(0.16, 0.32)
– 0.24†(0.16, 0.32)
Knee flexion range, degrees (74 to162)
– – 0.16§(0.05, 0.26)
– 0.10‡(0.002, 0.21)
Diabetes, WHO criteria (yes 5 1,no 5 0)
– – – 22.75‡(25.11, 20.39)
22.72‡(25.01, 20.44)
Arthritis, self-reported, physician-diagnosed (yes 5 1, no 5 0)
– – – 21.03(23.11, 1.05)
20.73(22.76, 1.31)
Stroke, self-reported (yes 5 1, no5 0)
– – – 28.13†(212.07, 24.20)
27.33†(211.15, 23.52)
Impaired peripheral vascularcirculation (Doppler) (yes 5 1,no 5 0)
– – – 24.39§(27.46, 21.33)
24.00§(26.94, 21.06)
Electrocardiographic leftventricular hypertrophy (yes 51, no 5 0)
– – – 22.47(25.90, 0.95)
22.21(25.56, 1.13)
Upper leg pain (yes 5 1, no 5 0) – – – 23.75§(26.29, 21.21)
23.12‡(25.65, 20.71)
Lower leg pain (yes 5 1, no 5 0) – – – 20.03(23.08, 3.02)
20.10(23.06, 2.88)
FEV1, liters (0.14 to 4.04) – – – 4.74†(2.68, 6.80)
4.20†(2.21, 6.19)
Examiner 2 (vs. Examiner 1) 20.62(23.75, 2.51)
22.05(25.06, 0.96)
22.11(25.10, 0.88)
22.09(25.03, 0.85)
22.21(25.11, 0.70)
Examiner 3 (vs. Examiner 1) 213.15†(217.57, 28.72)
210.85†(215.14, 26.56)
211.30†(215.49, 27.13)
210.74†(214.99, 26.90)
211.03†(215.18, 26.88)
Examiner 4 (vs. Examiner 1) 3.00‡(0.32, 5.68)
3.42§(0.87, 5.98)
23.31‡(26.24, 20.38)
1.92(20.56, 4.41)
23.95§(26.81, 21.09)
Adjusted R2 of model 0.18 0.25 0.31 0.33 0.38Hip and knee flexion range
incremental R2– – 0.06 – 0.05
* Values shown are regression coefficients (95% confidence intervals), expressed in meters per minute. SALSA 5 San Antonio Longitudinal Study ofAging; WHO 5 World Health Organization; FEV1 5 forced expiratory volume at 1 second.† P # 0.001.‡ P # 0.05.§ P # 0.01.
Arthritis Care & Research Walking Velocity and Joint Range of Motion 293

of hip and knee ROM, which should act to attenuate anyobserved influence of hip and knee ROM on walking ve-locity. That we could still measure a significant associa-tion between these 2 variables, in spite of inter-examinervariance, speaks for the robustness of the link between hipand knee ROM and walking velocity. Muscle strength is anadditional and important determinant of walking velocityin the elderly, even more important than joint pain (37).We did not include muscle strength as a covariate in thepresent analysis, as our intent was to focus on the contri-bution of hip and knee flexion range to walking velocity.
We timed subjects’ walking 50 feet starting from a stand-ing position, rather than ask the subject to accelerate andget “up to speed” before measuring the 50-foot distance.Thus, the walking velocity results that we show here maymarginally underestimate true walking velocity because ofthe slower pace in the first few feet of the 50-foot distance.
In summary, we have provided previously unavailabledata on the functional significance of the flexion range of 2major weight-bearing joints in the lower extremities. Thisinformation adds to our understanding of the chain ofevents in the disablement process.
REFERENCES
1. Walker JM, Sue D, Miles-Elkousky N, Ford G, Trevelyan H.Active mobility of the extremities in older subjects. Phys Ther1984;64:919–23.
2. James B, Parker AW. Active and passive mobility of lowerlimb joints in elderly men and women. Am J Phys Med Re-habil 1989;68:162–7.
3. Kapoor A, Sibbitt WL Jr. Contractures in diabetes mellitus: thesyndrome of limited joint mobility. Semin Arthritis Rheum1989;18:168–80.
4. Schulte L, Roberts MS, Zimmerman C, Ketler J, Simon LS. Aquantitative assessment of limited joint mobility in patientswith diabetes: goniometric analysis of upper extremity pas-sive range of motion. Arthritis Rheum 1993;36:1429–43.
5. Boone DC, Azen SP. Normal range of motion of joints in malesubjects. J Bone Joint Surg Am 1979;61:756–9.
6. Roach KE, Miles TP. Normal hip and knee active range ofmotion: the relationship to age. Phys Ther 1991;71:656–65.
7. Escalante A, Lichtenstein MJ, Dhanda R, Cornell JE, HazudaHP. Determinants of hip and knee flexion range: results fromthe San Antonio Longitudinal Study of Aging. Arthritis CareRes 1999;12:8–18.
8. Pincus T, Callahan LF, Vaughn WK. Questionnaire, walkingtime and button test measures of functional capacity as pre-dictive markers of mortality in rheumatoid arthritis. J Rheu-matol 1987;14:240–51.
9. Escalante A, Lichtenstein MJ, Hazuda HP. Determinants ofshoulder and elbow flexion range: results from the San Anto-nio Longitudinal Study of Aging. Arthritis Care Res 1999;12:277–86.
10. Stern MP, Pugh JA, Gaskill SP, Hazuda HP. Knowledge, atti-tudes, and behavior related to obesity and dieting in MexicanAmericans and Anglos: the San Antonio Heart Study. Am JEpidemiol 1982;115:917–28.
11. Gardner LI, Stern MP, Haffner SM, Gaskill SP, Hazuda HP,Relethford JH, et al. Prevalence of diabetes in MexicanAmericans: relationship to percent of gene pool derived fromnative American sources. Diabetes 1984;33:86–92.
12. Hazuda HP, Comeaux PJ, Stern MP, Haffner SM, Eifler CW,Rosenthal M. A comparison of three indicators for identifyingMexican Americans in epidemiologic research: methodologic
findings in the San Antonio Heart Study. Am J Epidemiol1986;123:96–112.
13. Melzac R, Torgerson WS. On the language of pain. Anesthe-siology 1971;34:50–9.
14. Escalante A, Lichtenstein MJ, White K, Rios N, Hazuda HP. Amethod of scoring the pain map of the McGill Pain Question-naire for use in epidemiologic studies. Aging 1995;7:358–66.
15. Escalante A, Lichtenstein MJ, Lawrence VA, Roberson M,Hazuda HP. Where does it hurt? Stability of recordings of painlocation using the McGill pain map. J Rheumatol 1996;23:1788–93.
16. Escalante A, Lichtenstein MJ, Rios N, Hazuda HP. Measuringchronic rheumatic pain in Mexican Americans: cross-culturaladaptation of the McGill Pain Questionnaire. J Clin Epidemiol1996;12:1389–99.
17. Lichtenstein MJ, Dhanda R, Cornell JE, Escalante A, HazudaHP. Disaggregating pain and its effect on physical functionallimitations. J Gerontol A Biol Sci Med Sci 1998;53:M361–71.
18. Kovar MG, Fitti JE, Chyba MM. The Longitudinal Study ofAging: 1984-1990. Vital Health Stat 1 1992:1–248.
19. Cornoni-Huntley J, Brock DW, Ostfeld AM, Taylor JO, Wal-lace RB. Established populations for epidemiologic studies ofthe elderly. Vol. 2. Resource data book. Bethesda (MD): Na-tional Institutes of Health; 1986.
20. World Health Organization Expert Committee. Second reporton diabetes mellitus. Geneva: World Health Organization;1980. Technical Report Series, No.: 646.
21. Van Itallie TB. Health implications of overweight and obesityin the United States. Ann Intern Med 1985;103:983–8.
22. Gerety MB, Mulrow CD, Tuley MR, Hazuda HP, LichtensteinMJ, Bohannon R, et al. Development and validation of aphysical performance instrument for the functionally im-paired elderly: the Physical Disability Index (PDI). J Gerontol1993;48:M33–8.
23. Fleiss JL. Statistical methods for rates and proportions. NewYork: John Wiley and Sons; 1981.
24. Landis JR, Koch GG. The measurement of observer agreementfor categorical data. Biometrics 1977;33:159–74.
25. Fleiss JL, Cohen J. The equivalence of weighted kappa and theintraclass correlation coefficient as measures of reliability.Educ Psychol Meas 1973;33:613–9.
26. Rose GA, Blackburn H. Cardiovascular survey methods.Geneva: World Health Organization; 1968.
27. Barkley B, Lichtenstein MJ, Garza C, Hazuda HP. Clinicalvalidation of the Welch-Allyn Pneumocheck hand-held spi-rometer. Am J Med Sci 1994;308:357–9.
28. Haffner SM. Macrovascular complications of diabetes in Mex-ican Americans. Diabetes Care 1991;14:665–71.
29. Knapp RG, Miller MC III. Clinical epidemiology and biosta-tistics. Baltimore: Williams & Wilkins; 1992.
30. Pearson K. Mathematical contributions to the theory of evo-lution. III. Regression, heredity and panmixia. Philos Trans RSoc Lond A Math Phys Sci 1896;187:253–318.
31. Cohen J, Cohen P. Applied multiple regression/correlationanalysis for the behavioral sciences. 2nd ed. Hillsdale (NJ):Lawrence Erlbaum Associates; 1983.
32. Verbrugge LM, Jette AM. The disablement process. Soc SciMed 1994;38:1–14.
33. Lichtenstein MJ, Escalante A, Hazuda HP. Ethnic differencesin walking time [abstract]. Gerontologist 1998;38 Spec No: 258.
34. Hazuda HP. Inclusion of ethnic minorities in sarcopenia re-search. Muscle Nerve Suppl 1997;5:S27–31.
35. Hawker G, Wright J, Coyte P, Paul J, Dittus R, Croxford R, et al.Health-related quality of life after knee replacement. J BoneJoint Surg Am 1998;80:163–73.
36. Harris WH, Sledge CB. Total hip and total knee replacement.N Engl J Med 1990;323:725–31,801–7.
37. Chang RW, Dunlop D, Gibbs J, Hughes S. The determinants ofwalking velocity in the elderly: an evaluation using regressiontrees. Arthritis Rheum 1995;38:343–50.
294 Escalante et al Vol. 45, No. 3, June 2001