Embed Size (px)
Citation preview

6/2/2016
1
Michigan Osteopathic AssociationDavid D. Wartinger, D.O., J.D.
Michigan State UniversityCollege of Osteopathic Medicine
May 13, 2016 1400 -1830
Integrated Treatment of the Adult Geriatric Male Patient
BPHProstate CancerLow TestosteroneErectile DysfunctionIncontinenceHematuria

6/2/2016
2
The Urological “Magic Bullet”
5 – alpha Reductase InhibitorProscar/Avodart
Alpha Adrenergic BlockerMinipress / Hytrin / Cardura / Flowmax / Uroxatrol/ Rapiflo
Testosterone ReplacementAndroderm / Androgel / Testim/ Axiron/ Fortesta/ Natesto / Striant / injection or implant / not Oral
Erectile DysfunctionViagra/ Levitra / Cialis
1st choice for symptomatic BPH, low T and ED
Avodart 0.5 mg PO q daily
Uroxatrol 10 mg PO q daily
AndroGel 2 pumps q AM applied to skin
Cialis 5 mg PO q bedtime
6/2/2016
3
Transitional Zone develops BPH
Peripheral Zone develops CaP
5
Obstructive Voiding Symptoms
Decreased force of streamHesitancyStrainingIncomplete bladder emptyingNocturia
6

6/2/2016
4
Irritative Voiding Symptoms
FrequencyUrgencyOccasionally dysuria
7
Voiding Dysfunction Factors
Changes in bladder, prostate and /or urethra Bladder instability Decreased bladder compliance Urethral stricture; bladder neck contracture
8
6/2/2016
5
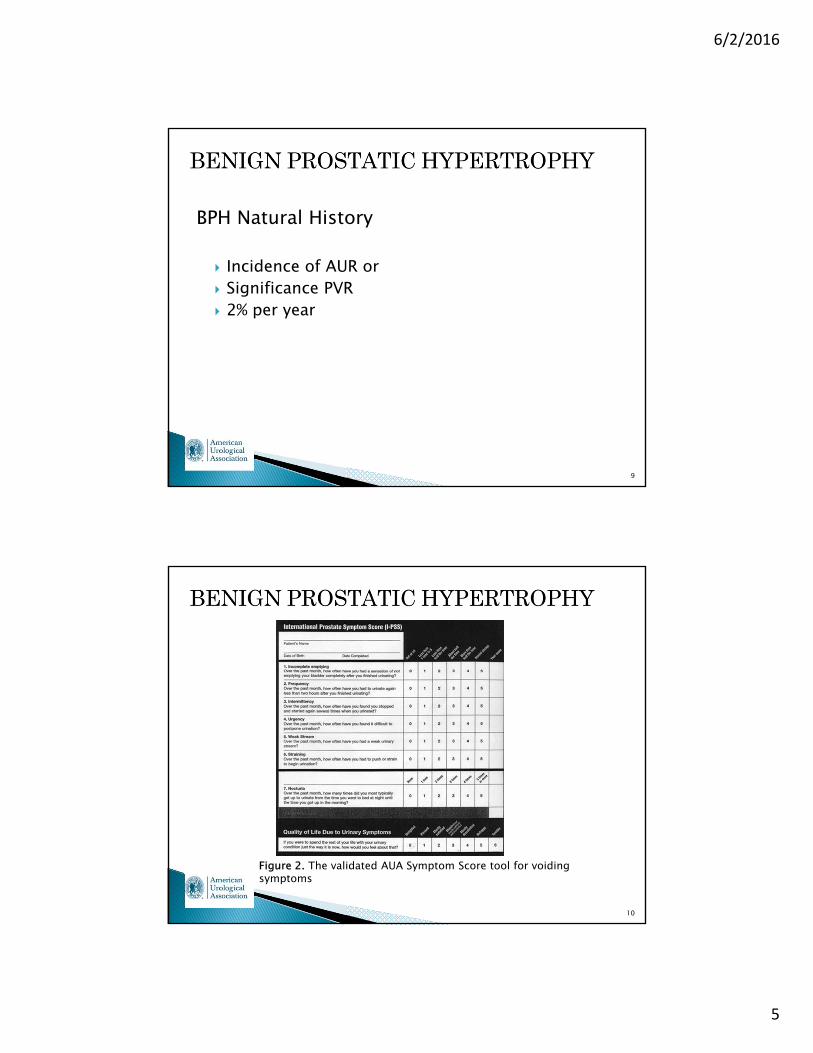
BPH Natural History
Incidence of AUR or Significance PVR 2% per year
9
Figure 2. The validated AUA Symptom Score tool for voiding symptoms
10

6/2/2016
6
Medical Therapy for BPH
Shrink or stop growth of prostate Open urethral channel within prostate
11
Inhibit Production of DHT
finasteride (Proscar) 1992 dutasteride (Avodart) 2001
Prevent or reduce acinar gland growth
12

6/2/2016
7
Relax Smooth Muscle of Prostate and Bladder Neck
Alpha Blockers◦Antihypertensives terazosin (Hytrin)doxazosin (Cardura)
◦Prostate Specific tamsulosin (Flomax)alfuzosin (Uroxatrol)
13
Minimally Invasive Procedures for BPH
Transurethral microwave procedures (TUMT)Transurethral needle ablation (TUNA)Water-induced thermotherapyHigh intensity focused ultrasound (HIFU)
14

6/2/2016
8
Conventional Surgical Therapy
Transurethral Resection of the Prostate◦“Gold Standard” treatment◦Resectoscope◦60 – 90 minute operation◦Wire loop◦General or spinal anesthesia
15
Laser Surgery Variations for BPH
Photo selective Vaporization of the Prostate (PVP)Interstitial Laser Coagulation (ILC)
16
6/2/2016
9
17
Prostate Cancer: Screening and Management
Prostate Cancer (CaP)
Treatment Stratagem
• Early detection while tumor confined to prostate or surrounding tissues and can be cured by either removal or treatments aimed at the primary
18
Prostate Cancer: Screening and Management
PSA and Overdiagnosis
Identification of patients with CaP that don’t benefit from diagnosis or treatment of their disease

6/2/2016
10
19
Prostate Cancer: Screening and Management
United States Preventative Services Task Force (USPSTF)
“Fair evidence that [PSA Screening] is ineffective or that harms outweigh the benefits.”
• PSA screening and DRE in asymptomatic patients
20
Prostate Cancer: Screening and Management
AUA DISAGREES with USPSTF
• PSA used since 1986, total CaP deaths decreased ≈ 30%
• Decreased “dire consequences “ of advanced CaP
• American Cancer Society (ACS) and the American Society of Clinical Oncologists (ASCO) agree with AUA

6/2/2016
11
21
Prostate Cancer: Screening and Management
Localized Prostate Cancer Treatment
• Radiation• Surgery• Cryosurgery• High intensity focused ultrasound• Expectant management (watchful waiting)
22
Prostate Cancer: Screening and Management
Hormone Therapy for CaP
• Most commonly used after metastasis
• Only palliative, not curative
• Hormone refractory or androgen independent
6/2/2016
12
23
Prostate Cancer: Screening and Management
Summary of CaP Treatment
• No free lunch
• Surgery with 30 year life expectancy, localized CaP
• Radiation or expectant management for patients, over 70 years of age and localized CaP
• Metastatic CaP, palliative with hormone manipulation
Testosterone Replacement
1. Only men with symptoms of low testosterone
2. Blood levels confirm low testosterone as cause of symptoms

6/2/2016
13
Symptoms of Low Testosterone
Low sex drive (libido) Erectile dysfunction Fatigue and poor energy level Decreased muscle mass Hair loss Difficulty concentrating Depression Irritability Low sense of well-being
Forms of TestosteroneSkin patch (transdermal): Androderm – worn on arm or upper body, applied once a
dayGels: AndroGel and Testim – absorbed through skin, applied once
a day, comes in packets AndroGel, Axiron and Fortesta – comes in pump Natesto – gel applied inside the noseMouth Patch: Striant – tablet sticks to upper gums, applied twice a dayInjections and implants: Injection directly into the muscles Implanted pellets into the soft tissueOral ? Negative effects on liver Bypass the liver with other delivery methods
6/2/2016
14
Risks of Testosterone Therapy Rash, itching or irritation at application site Evidence for increased risk of:
Heart attack Stroke Acne Fluid Retention Breast Enlargement Decreased Testes Size Increased Aggression Mood Swings Decreased Sperm Count Infertility PSA Increase Cholesterol/Lipids
Benefits and Risks of long-term testosterone therapy are
UNKNOWN.

6/2/2016
15
Conditions that may worsen with testosterone therapy Benign Prostatic Hypertrophy (BPH):◦ Prostate grows naturally under the stimulation of testosterone
Prostate Cancer (CaP):◦ Can stimulate prostate cancer to grow◦ Screen for CaP before starting testosterone◦ CaP or elevated PSA should probably not receive testosterone
treatment Sleep Apnea Blood Clots:
Risk of deep vein thrombosis and pulmonary embolism Congestive Heart Failure
Testosterone Replacement vs. Performance – Enhancing Steroids
Testosterone replacement only achieves physiologic levels of hormone
Doping uses much higher doses of testosterone and often combined (“stacked”) with other substances

6/2/2016
16
31
Definition
• The inability to achieve and maintain an erection sufficient for satisfactory sexual intercourse
32
Erectile Dysfunction
• Estimated to affect 20-30 million men in the US
• One or more factors• Psychological• Neurologic• Hormonal • Arterial• Venous

6/2/2016
17
33
Erectile Dysfunction
• “Silent Marker” for later development of cardiovascular disease
34
Figure 1. Anatomy of the Penis. The penile erection occurs as a result of 3 processes: a) smooth muscle relaxation among arteries and trabecular tissue increases blood flow, which b) lengthens and enlarges penis through sinusoidal filling, and c) expanded sinusoids compress the subtunical venous plexus, reducing venous outflow.

6/2/2016
18
35
Block Phosphodiesterase Enzyme Activity
• Sildenafil
• Vardenafil
• Tadalafil
36
Hormonal ED• Androgen deficiency
• Decrease in nocturnal erections decreases libido
• Erections with visual sexual stimulation preserved
• Androgen may not be essential for erection
6/2/2016
19
37
Sexual Function over time• Progressively declines in “healthy” aging men
• Latent period between sexual stimulation and erections increases
• Erections are less turgid
• Ejaculation less forceful
• Ejaculatory volume decreases
• Refractory period between erections lengthens
• Decrease in serum testosterone
38
Recommended Laboratory Tests
• Urinalysis
• Complete Blood Count
• Fasting blood glucose
• Creatinine
• Cholesterol
• Triglycerides
• Testosterone

6/2/2016
20
39
If Testosterone low
• Serum free (or bioavailable) testosterone
• Prolactin
• Lutenizing hormone
40
Erectile dysfunction is not just a sexual health issue,
it may be a serious harbinger of life-threatening cardiovascular conditions

6/2/2016
21
41
ED is as important a CV disease risk factor as Smoking, or
Family history of Heart Disease
42
Erectile Dysfunction – Treatment
Drug Therapy
• Administration: oral, injected directly into penis, inserted into distal urethra
• March 1998 sildenafil, first pill
• Vardenafil and tadalafil
• Phosphodiesterse (PDE) inhibitors
6/2/2016
22
43
Erectile Dysfunction – Treatment
Intracavernosal Injections
• Inject drugs into penis to engorge with blood
• Papaverine hydrochloride, phentolamine, and alprostadil (a prostaglandin E2)
• Widen blood vessels, induce and maintain erections
• Side effects: persistent erection (priapism) and scarring
44
Erectile Dysfunction – TreatmentIntraurethral Injections
• Insert pellet of alprostadil into urethra, prefilled applicator
• MUSE, inch into urethra
• Onset 8 to 10 minutes, may last 30 to 60 minutes
• Side effect: penile pain, warmth or burning sensation in urethra, redness of penis, minor urethra bleeding or spotting
6/2/2016
23
45
Erectile Dysfunction – Treatment
Vacuum Erection Devices
• Creates partial mechanical vacuum
• Draws blood into penis, engorging and expanding it
• 3 components: plastic cylinder, pump and elastic band
46
Erectile Dysfunction – Treatment
Penile Surgery
• Procedures to improve erections1. Implant a device, make rigid2. Reconstruct arteries, improve
flow3. Occlude veins, prevent leak

6/2/2016
24
Urinary Incontinence• Often treatable
• Identify patients who might benefit from treatment
• Treatment depends on etiology
• Identify the etiology
Urge Incontinence
• Sudden sensation to void
• Unable to suppress sensation fully
• Severe case, may not be aware sensation until actually leaking
6/2/2016
25
Overactive Bladder (OAB)
Newer term
Frequency and Urgency
With or without
Urge Incontinence
Overflow Incontinence• Occurs at extreme bladder volumes, or
• Bladder volume reaches the limit of viscoelastic properties
• Elevation in detrusor pressure
• Incomplete bladder emptying• Obstruction• Poor bladder contractility

6/2/2016
26
Overflow Incontinence
Symptoms
• Constant dribbling
• Extreme frequency
Evaluation of the Incontinent Patient• History
• Physical examination
• Laboratory tests
• Possibly urodynamic testing

6/2/2016
27
Evaluation of the Incontinent Patient
Urinalysis
• Hematuria
• Pyuria
• Glucosuria
• Proteinura
• Cytology, if hematuria or irritative voiding symptoms
Evaluation of the Incontinent Patient
Urine Culture and Sensitivity if
• Pyuria
• Bacteriuria
• Treat infection prior to further W/U
• > 3 RBC/HPF, further investigation
6/2/2016
28
Evaluation of the Incontinent Patient
Post Void Residual (PVR)
• Measure with ultrasound or catheter
• Normal <50ml / >200 ml abnormal
• Increased PVR,• Bladder outlet obstruction• Poor bladder contractility• Differentiate with urodynamic testing
Treatment of Urinary Incontinence
Urge Incontinence
• Bladder contracts with or without warning
• Timed voiding
• Remind patients to void every 1-2 hours during the day
• Void before urge to void

6/2/2016
29
Urge IncontinenceAnticholinergic – Antimuscarinics
• Mainstay of medical therapy
• Side Effects• Urinary retention• Dry mouth• Constipation• Nausea• Blurred vision• Tachycardia• Drowsiness• Confusion
Urinary IncontinenceUrge Incontinence
Poor Bladder Compliance
• Primary Goal: treat high bladder pressure
• Complete bladder emptying• ICC and anticholinergics
• May add to anticholinergic –antimuscarinics and alpha-agonists
• Bladder augmentation when medical management fails

6/2/2016
30
Urinary IncontinenceTreatment of Urinary Incontinence
Overflow Incontinence
• Treated by emptying the bladder
• Relieve Obstruction
• Males
• Urethral stricture• Prostatic obstruction
Urinary IncontinenceTreatment of Urinary Incontinence
Urethral Stricture Disease
• Urethral dilation
• Internal urethrotomy
• Urethroplasty

6/2/2016
31
Urinary IncontinenceTreatment of Urinary Incontinence
Prostatic Obstruction
• “Gold Standard” TURP
• Transurethral Resection of the Prostate
Urinary IncontinenceTreatment of Urinary Incontinence
Overflow Incontinence
• Poor detrusor contractility
• ICC (intermittent clean catheterization)
6/2/2016
32
Urinary IncontinenceTreatment of Urinary Incontinence
Indwelling Catheters
• Not optimum long term treatment
• Eventually infected urine
• Predisposes to bladder calculi
• Possible ultimate squamous cell carcinoma
Urinary IncontinenceTreatment of Urinary Incontinence
Males with Stress Incontinence
• Artificial urinary sphincter• Cuff compresses bulbar urethra “Gold
Standard”
• Male slings• Compress under urethra
• Elevate the urethra to more retro pubic position
• Lesser degrees of incontinence, pad weight test
6/2/2016
33
Urinary IncontinenceSummary – Key Diagnostic Points
Urge Incontinence
• Symptoms
• Urgency
• Frequency
• Nocturia
• Unable to reach the toilet with urge
Urinary IncontinenceSummary – Key Diagnostic Points
Stress Incontinence
• Symptoms
• Leakage with physical activity
• Signs
• Bladder neck mobility
• Positive stress test

6/2/2016
34
Urinary IncontinenceSummary – Key Diagnostic Points
Mixed Incontinence
• Symptoms• Urgency• Frequency• Nocturia• Unable to reach the toilet with urge• Leakage with physical activity
• Signs• Bladder neck mobility• Positive stress test
Urinary IncontinenceSummary – Key Diagnostic Points
Overflow Incontinence
• Symptoms• Frequency• Nocturia• Urgency• Leakage with physical activity
• Signs• High post void residual

6/2/2016
35
Urinary IncontinenceSummary – Key Treatment
Urge Incontinence
• Avoidance of bladder irritants
• Timed voiding
• Pelvic muscle exercises
• Weight loss
Urinary IncontinenceSummary – Key Treatment
Urge Incontinence• Anticholinergics – Antimuscarinics -
Nonselective for M3 Receptor• Propantheline (Pro-Banthine)
• 7.5 to 30 mg orally, three to five times daily
• Tolterodine (Detrol LA)• 4 mg orally daily
• Trospium (Sanctura)• 20 mg orally two times daily
• Solifenacin (Vesicare)• 5 – 10 mg orally, daily

6/2/2016
36
Urinary IncontinenceSummary – Key Treatment
Urge Incontinence
• Anticholinergics – Antimuscarinics –Selective for M3 Receptor
• Darifenacin (Enablex)• 7.5 to 15 mg orally, daily
Urinary IncontinenceSummary – Key Treatment
Urge Incontinence
• Anticholinergic – Antimuscarinics/Smooth Muscle Relaxant
• Oxybutynin• Regular (Ditropan)
• 2.5 to 5.0 mg orally, one to three times daily
• Extended Release (Ditropan XL)• 5 – 30 mg orally, daily
• Transdermal (Oxytrol)• 4.9 mg patch twice per week
• Hyoscyamine (Lesin)• 0.125 to 0.375 mg orally, two to four
times daily

6/2/2016
37
Urinary IncontinenceSummary – Key Treatment
Urge Incontinence
• Anticholinergic/Alpha-Agonist• For urge or mixed
• Imipramine (Tofranil)• Not FDA approved for this indication• 10 to 25 mg, once to three times daily
Urinary IncontinenceSummary – Key Treatment
Stress Incontinence
• Behavioral Changes• Weight loss• Quitting smoking• Pelvic muscle exercises

6/2/2016
38
Urinary IncontinenceSummary – Key Treatment
Stress Incontinence
• Alpha Agonists• Pseudoephedrine (Sudafed)
• Not FDA approved for this indication
• 30 to 60 mg, up to four times per day
Urinary IncontinenceSummary – Key Treatment
Stress Incontinence
• Anitcholinergics / Alpha – Agonist• Imipramine (Tofranil)
• Not FDA approved for this indication
• 10 to 25 mg, once to three times daily

6/2/2016
39
0.000ml
0.008ml
0.017ml
0.034ml
0.068ml
0.125ml
0.250ml
0.500ml
1.000ml
2.000ml
4.000ml
8.000ml
1.000SG – U
Row A
1.010SG – U
Row B
1.020SG – U
Row C
HEMATURIA REFERENCE CHARTMICHIGAN STATE UNIVERSITY
Column = Added ML Blood Per Cup Rows = Specific Gravity of Urine SG – U Specimen Cup 50 ML
1 2 3 4 5 6 7 8 9 10 11 12
OBJECTIVE:
This study was approved by the Michigan State University IRB: IRB#: 11-808SI
Very small amounts of blood can be visually detected in the urine and may be the only warning sign of a life threatening problem. A systematic documentation of the visual appearance of gross hematuria specimens was not previously performed. The clinical advantage of possessing a library of photographs documenting exact volumes of blood in known urine specimen volumes was not appreciated. To simulate hematuria, known quantities of anti-coagulated blood were added to 50 ml urine specimens of various specific gravities/concentrations and then photographed on white graph paper. The gross hematuria specimen photographs were arranged sequentially to create a Hematuria Reference Chart. An unknown hematuria specimen can now be visually matched to the Hematuria Reference Chart to determine blood loss per ml of voided urine. The Hematuria Reference Chart is available on-line to health care professionals and patients for documentation, education and diagnosis.
Cancer Trauma Inflammation Infection Foreign Bodies Vascular Glomerular Disease Hematologic Activity Menstruation Loin Pain –Hematuria Syndrome
Hematuria is not normal and its cause must be determined. Most episodes of gross hematuria are not due to life threatening conditions or diseases; but, some episodes are the only warning sign of a life threatening problem. Very small amounts of blood can be visually detected in urine and the amount of blood does not reliably predict the seriousness of the underlying cause of the hematuria. The presence of visible blood in the urine can cause fear and anxiety in patients and healthcare providers alike. Accurately estimating the volume of blood mixed in the urine can help direct treatment and eliminate unwarranted concerns of serious blood loss. Without a reference standard, estimating blood loss from hematuria is imprecise and without scientific basis.
A photographic library of simulated gross hematuria specimens was created and arraigned to produce a hematuria reference chart. Voided urine was collected from a solitary volunteer during various hydration states to obtain urine of different specific gravities / concentration. Increasing amounts of whole anti-coagulated blood were added to volumes of collected urine to create 50 ml simulated gross hematuria specimens. The simulated gross hematuria specimens were photographed (in clear urine specimen cups) on white graph paper background with blue lines. All of the simulated gross hematuria specimen photographs and the Hematuria Reference Chart were uploaded to YouTube and Google Images.
ABSTRACT
INTRODUCTION
CAUSES OF HEMATURIA
METHODS AND MATERIALS
PROCEDURE FOR USING HRC
Example:
Step 1:Verify a total of 50 ml of gross hematuria sample in a clear standard 120 ml urine specimen cup viewed on a background of white graph paper.
Step 2:Select the most appropriate row based on urine specific gravity and match the unknown specimen to the column of added blood on the HRC.
Step 3:Calculate blood loss from hematuria (Voided volume/50 X added blood volume from HRC/cup) = total whole blood loss in ml/void.
If patient voids 500 ml:
500ml/50=10; 10 x 0.034ml= 0.34 total whole blood loss ml/void
DISCUSSION
The online availability of the Michigan State University College of Osteopathic Medicine Hematuria Reference Chart enables patients and health care providers to quantify and document hematuria. Even when patients don’t have online access to the Hematuria Reference Chart, they can photograph their hematuria specimen using a smartphone and send the pictures to their caregiver for comment. Urinary blood loss can now be tracked over the duration of the disease. The Hematuria Reference Chart is both an educational and diagnostic tool with documentation capabilities.
VISUAL ESTIMATION OF BLOOD IN GROSS HEMATURIA
David D. Wartinger, D.O., J.D. Osteopathic Surgical Specialties College of Osteopathic Medicine Michigan State University Shannon Grochulski-Fries
IRB #02-970/APP #i008313