Embed Size (px)
Citation preview
WASH and Child Growth &
DevelopmentWashington, DC | May 2-3, 2013
Val CurtisLondon School Of Hygiene and Tropical Medicine& Alan Dangour, Oliver Cumming, SHARE, DFID
Clean, Fed & Nurtured: Joining forces to promote child growth and development

WASH basics
• Water – quantity and quality
• Sanitation– Faecal waste
disposal• Hygiene – Hand, Food,
Environment

0.85m deaths a year
2-3.5bn episodes
Source: Liu et al, Lancet 2012

Faeces
Fluids
Fields
Flies
Fingers
FoodsNew Host

Faeces
Fluids
Fields
Flies
Fingers
FoodsNew Host

Faeces
Fluids
Fields
Flies
Fingers
FoodsNew Host

Faeces
Fluids
Fields
Flies
Fingers
FoodsNew Host

Faeces
Fluids
Fields
Flies
Fingers
FoodsNew Host

Faeces
Fluids
Fields
Flies
Fingers
FoodsNew Host

Faeces
Fluids
Fields
Flies
Fingers
FoodsNew Host

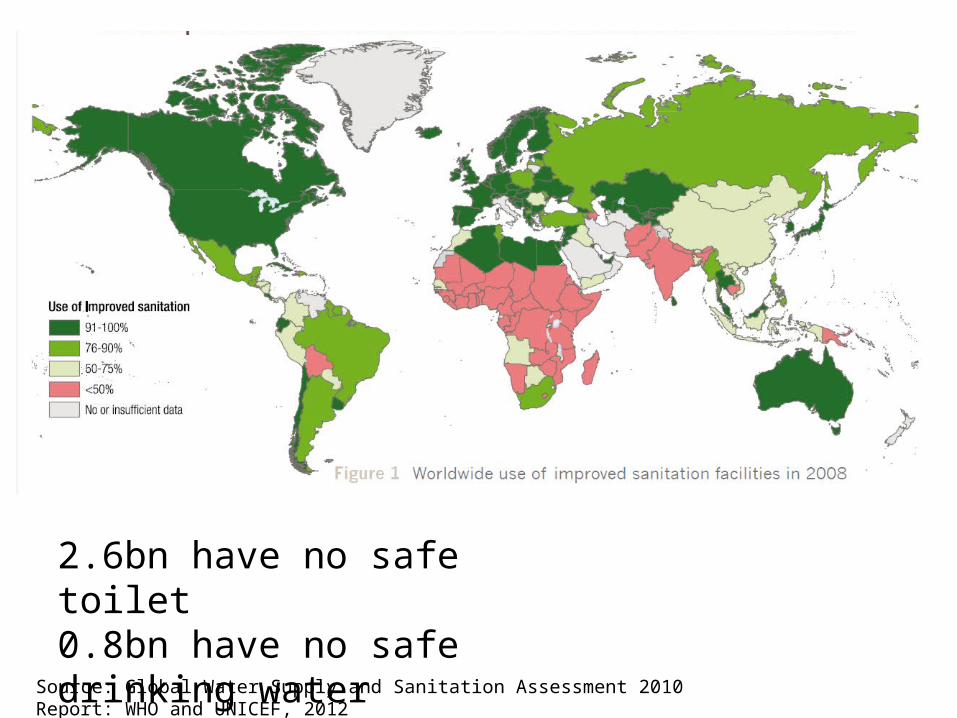
Source: Global Water Supply and Sanitation Assessment 2010 Report: WHO and UNICEF, 2012
2.6bn have no safe toilet0.8bn have no safe drinking water20%?? HWWS

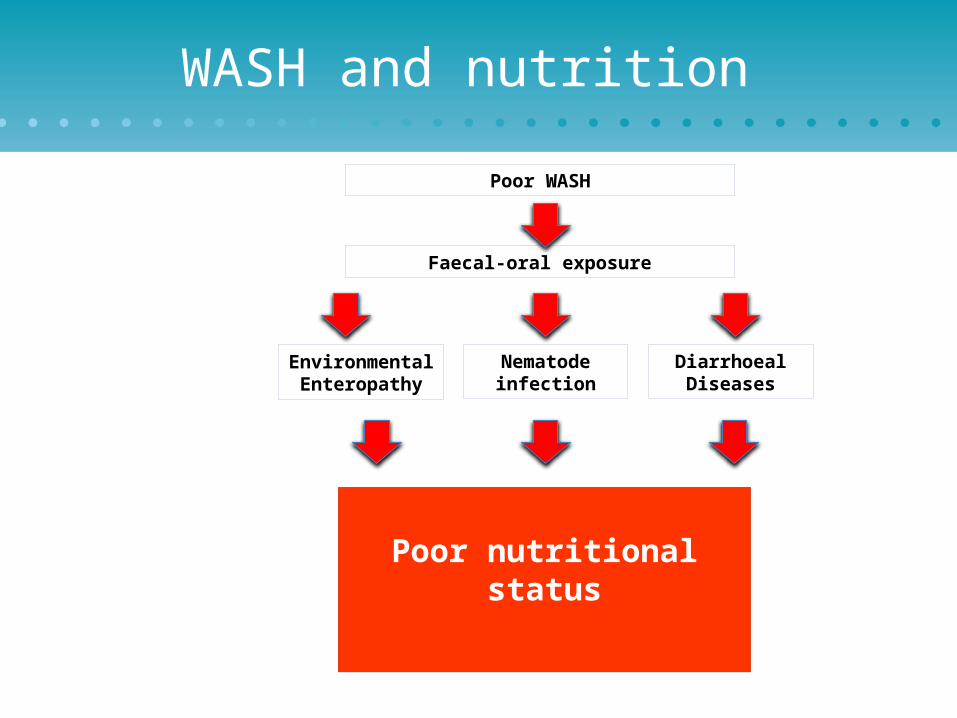
WASH and nutrition
Faecal-oral exposure
Diarrhoeal Diseases
Environmental Enteropathy
Nematode infection
Poor WASH
Poor nutritional status


Cochrane Public Health Group
• Includes– RCTs– non-randomised controlled studies– interrupted time series studies
• WASH included as one intervention

Review protocol
• All included studies to have controlled design
• Participants: children < 18 years old
• Intervention types– Improving access to facilities which ensure the hygienic
separation of human excreta from human contact– Promotion of hand washing with soap– Introducing a new/improved water supply and/or improved
distribution– Improving the microbiological quality of drinking water

Outcomes, search strategy• Primary outcomes (z-scores)– Weight-for-height (wasting)– Weight-for-age (underweight)– Height-for-age (stunting)
• Secondary outcomes– All other child anthropometric measures– Biochemical measures of micronutrient status
• 6 databases searched; keyword and MeSH terms• 3 main Chinese databases searched

Search results

Included studies• 12 studies from 10 countries
– Bangladesh (1989; 1993)– Guatemala (1968; 2009)– Pakistan (2012)– Kenya (2011)– Ethiopia (2012)– Nigeria (1990)– Nepal (2011)– Chile (1983)– South Africa (2010)– Cambodia (2011)
• Duration: 6 mo to 5 years• Sample: n=8,500; all <5 years

Interventions• Studies included from 1 to 4 WASH interventions• Interventions– Provision of flocculent water disinfectant– Provision of a protected water supply– Installation of boreholes and hand pumps– Solar water disinfection (SODIS)– Sanitation education– Construction of sanitary facilities– Provision of soap– Promotion of hand washing with soap

Study designs• Multiple designs
– Randomised controlled trials (3)– Follow-up of cluster randomised controlled trial (1)– Longitudinal study with control group (3)– Repeat cross-sectional with control group (3)– Controlled before-and-after study (1)– Cross-sectional with intervention and historic control group
matched by propensity score matching (1)
• No study considered high quality according to Cochrane criteria

Results table n=8,500Study n Reported effect (HAZ unless stated)
Ahmed 1993 298 Mean WAZ: P< 0.05
Arnold 2009 877 MD: 0.04 (-0.19, 0.27)
Bowen 2012 461 MD: -0.08 (-0.29, 0.13)
Du Preez 2010 329 MD: 0.15 (-0.14, 0.44) (not published)
Du Preez 2011 521 MD: 0.12 (-0.15, 0.39)
Fenn 2012 1899 MD: 0.22 (0.11, 0.33)
Guzman 1968 N.D. Mean height: no stat. test
Hasan 1989 405 No statistically different differences
Huttly 1990 180 – 368 Decline in % children with low W/H: P<0.005
Langford 2011 88 MD: -0.13 (-0.54, 0.28)
McGuigan 2012 753 MD: 0.18 (-0.06, 0.42) (not published)
Schlesinger 1983 199 % low weight: P<0.05 for change in control group

HAZ (all studies)

HAZ meta-analysis n=1,603
I2 = 0%

WAZ meta-analysis n=1,616
I2 = 5%

WHZ meta-analysis n=1,605
I2 = 0%

Interpretation
• Number of children included in studies reasonable
• Quality of studies is limited
• Cochrane meta-analysis suggests that WASH improves HAZ by ~0.15 SD
• Supported by IPD analysis
• “Suggestive evidence of benefit”

Concerns
• Publication bias• Quality of studies• Links in the pathway?

Conclusions of Cochrane review
• First systematic review of WASH and nutrition• 12 studies (of mixed quality) provide data for analysis• Suggestive evidence of benefit of WASH on linear growth• More evidence on the way• And still more needed!
WASH and nutrition
Faecal-oral exposure
Diarrhoeal Diseases
Environmental Enteropathy
Nematode infection
Poor WASH
Poor nutritional status

Diarrhoea and stunting• Diarrhoea associated with poor nutritional status but
causal link hard to demonstrate
• Poor nutritional status associated with greater risk of diarrhoea (Briend, 1990; Checkley et al, 2002)
• Recent analysis of 9 studies with daily diarrhoea morbidity data and longitudinal anthropometry (Checkley et al, 2008):– Odds of stunting at age 24 mo increased with each diarrhoeal episode before 24 mo
(P<0.001)– Odds of stunting at age 24 mo increased by 1.13 (95% C.I. 1.07, 1.19) for every five
episodes– Consistent with hypothesis that higher cumulative burden of diarrhoea increases risk
of stunting

WASH and nutrition
Faecal-oral exposure
Diarrhoeal Diseases
Environmental Enteropathy
Nematode infection
Poor WASH
Poor nutrition
Time, costs, workload
Other Diseases

WASH and ECD
Faecal-oral exposure
Diarrhoeal Diseases
Environmental Enteropathy
Nematode infection
Poor WASH
Poor ECD
Time, costs, workload
Other Diseases

Diarrhoea/Giardia and ECDHigh diarrheal disease burdens before 2 years of age linked with
delayed school entry and poorer performance on intelligence tests– Patrick et al 2005.– Lorntz et al 2006
Multiple infections with Giardia associated with a 4-point (0.27 SD) deficit on a standardized intelligence test at 9 years of age.– Berkman et al 2002

Bowen et al 2012...“At 5 to 7 years of age, children randomized to home-based
handwashing promotion during their first 30 months of life attained global developmental quotients more than 6 points (0.4 SD) greater than control children.
The effect size was similar across all 5 domains (adaptive, personalsocial, communication, cognitive, and motor) ...and is comparable to gains after participation in the US publicly funded Head Start preschool program for poor children (SD, 0.33-0.46 compared with parental care) and early intervention programs for premature infants (SD, 0.46)
Such an effect size is regarded as clinically meaningful and some estimate that a societal shift of this magnitude would yield trillions of dollars in increased productivity.”

Conclusions
• Systematic reviews are blunt instruments but the best we have
• All studies need publishing• Ever more evidence to collect? Should that
hold us back? • Is this about competition?

NUTRITION and Child Growth &
DevelopmentWashington, DC | May 2-3, 2013
Kay DeweyUC-Davis and Alive & Thrive
Clean, Fed & Nurtured: Joining forces to promote child growth and development

Nutrition Basics• IYCF = infant and young child feeding, to 2 years• WHO-recommended feeding practices for:
– Breastfeeding (early initiation; exclusive BF; continued BF)– Complementary feeding (e.g. amount, consistency, frequency,
diversity & types of foods), including:• Safe preparation & storage of complementary foods (relevant to WASH)• Responsive feeding practices (relevant to ECD)
• Established indicators:– Feeding practices (8 core WHO/UNICEF indicators)– Anthropometric measures (e.g., weight for age, height for age,
weight for height, arm circumference)• Reduction in stunting (very short height for age) is a key goal

Key window for nutrition interventions
Preconception through pregnancy
0-6 mo: Exclusive breastfeeding
6-24 mo: Complementary feeding
Guiding principles for complementary feeding (2003; 2005)

Outline
• Impact of nutrition interventions on linear growth (child’s height)
• Impact of nutrition on child development• The need for combined interventions

Impact of nutrition onchild growth

Prenatal nutrition interventions
• Iron & folic acid supplements• Multiple micronutrient
supplements• Balanced protein-energy
supplements• Fortified foods for pregnant
women
• Potential for major impact on stunting, but evidence is mixed

Prenatal nutrition interventions
A. Multiple micronutrient supplements (usually compared with iron & folic acid)
Meta-analysis in 2009 (Fall et al.): • Small but significant increase in birth weight (+22 g) but not birth
length (+0.06 cm)– Measurement issues?
• 11-17% reduction in low birth weight• Impact only evident in mothers with higher BMI
Meta-analysis in 2012 (Ramakrishnan et al.):• Increase in mean birth weight (+53 g); data on birth length not
presented• 14% reduction in low birth weight

Prenatal nutrition interventions
B. Balanced protein-energy supplementation
Meta-analysis in 2003 (Kramer & Kakuma):• Increase in mean birth weight (+38 g) but not birth length (+0.1 cm)• 32% reduction in small-for-gestational-age births• Larger effect on birth weight in hungry season and in
undernourished women
Meta-analysis in 2012 (Imdad & Bhutta):• Increase in mean birth weight (+73 g); did not report birth length• 32% reduction in LBW and 34% reduction in SGA births• Larger effect on birth weight in undernourished women

Prenatal nutrition interventions
C. Fortified foods for pregnant women
Lipid-based nutrient supplement (LNS) (Huybregts et al. Am J Clin Nutr 2009), Burkina Faso
• LNS: 373 kcal/d & similar micronutrients as MMN tablets• LNS group (compared to MMN):
– Birth weight +31 g (p=0.2)– Birth length +0.46 cm (p=0.001)
• effect greater in mothers with BMI < 18.5 (+1.2 cm)
• Same research group previously showed that MMN (vs. control) increased birth length by 0.36 cm; thus predicted impact of LNS vs. control would be 0.46 + 0.36 = 0.82 cm (effect size 0.33)

Exclusive breastfeeding 0-6 mo• Large impact on infant survival • Little evidence of impact on stunting
– Effect may be more likely in populations with high rates of infection during the first 6 mo postpartum, where promotion of exclusive breastfeeding may reduce infection and thus be more likely to promote linear growth than in populations where such infections are less common
– Insufficient evidence to evaluate this question at present
46

Complementary feeding 6-24 mo
• Several strategies:– Educational approaches– Increasing energy density
of complementary foods– Provision of
complementary food– Fortification
• Potential for major impact on stunting but evidence is mixed
47
6-24 mo: Complementary feeding Guiding principles for
complementary feeding (2003; 2005)

Complementary Feeding - 1
• Educational approaches – mixed results– Most showed little or no impact– Peru study illustrated substantial potential to
improve linear growth (Effect size=0.5): emphasized consumption of nutrient-rich animal-source foods & was conducted in a population where animal-source foods were available & affordable
– Two recent studies (Shi et al.; Vazir et al.) show modest impact (Effect size ~0.2): both emphasized key messages including dietary diversity and animal-source foods

Complementary Feeding - 2
• Interventions to increase energy density – mixed results– Of 5 studies, 2 had positive impact but 3 had no
impact on energy intake or growth– May be effective when traditional complementary
food has low energy density & infant unable to compensate by increasing volume of food consumed or feeding frequency
Complementary Feeding - 3
• Provision of complementary food – mixed results– Average effect size ~0.2-0.3, but wide range• May depend on food security of target population• May depend on nutrient quality of food provided
– Two studies directly compared food + education vs. education only (both in S Asia): somewhat greater impact when food included

Complementary Feeding - 4
• Fortification (or improved bioavailability) alone has little effect on linear growth– Exception: fortified vs. unfortified milk powder in India
• Combination of macro- and micro-nutrients in may have a larger impact
• Nutrient quality of fortified products is likely to be important– Amount and bioavailability of nutrients needed for
growth– Inclusion of milk– Essential fatty acids

Summary of impact of nutrition interventions on stunting
• Nutrition interventions (alone) have had a modest impact on linear growth– Need to be realistic about expected impact of
nutrition interventions • However, impact on % with very low height
(stunting) may be larger than effect on mean height

Impact of nutrition onchild development

Potential mechanisms for the effect of nutrient deficiency on children’s
cognitive, motor, and socio-emotional development
From: Prado & Dewey, A&T Technical Brief

Nutrition and Brain Development in Early Life (Prado & Dewey, A&T Technical Brief)
1) Adequate nutrition during pregnancy and the first two years is necessary for normal brain development, laying the foundation for future cognitive and social ability, school success, and productivity.
2) Priority should be given to the prevention of: • Severe acute malnutrition• Intrauterine growth retardation • Stunting• Iron-deficiency anemia• Iodine deficiency

Nutrition and Brain Development in Early Life (Prado & Dewey, A&T Technical Brief)
3) There is growing evidence for beneficial effects on ECD of:• Breastfeeding promotion • Pre- and post-natal multiple micronutrient supplementation• Pre- and post-natal supplementation with essential fatty acids• Fortified food supplements provided during pregnancy and to
the child from 6 to 24 mo
4) An integrated approach is likely to be most effective for promoting optimal child development, i.e., interventions that combine improved nutrition with other strategies such as enhancing the home environment and the quality of caregiver-child interaction.

The need forcombined interventions
Nutrition, infection control & care Prenatal + postnatal (and possibly pre-conception) Macronutrients + micronutrients: Adequate supply of
macronutrients may be needed to ensure growth response to micronutrients

How nutrition can reduce the negative impact of infections on child growth
1. Strengthening the immune system, thereby reducing the severity and duration of infections
2. Providing extra amounts of nutrients to compensate for poor absorption during infection, losses during diarrhoea, reallocation due to immune system activation or reduced appetite during infection
3. Providing nutrients for catch-up growth following infection, particularly those needed to build lean body tissue such as protein, potassium, magnesium, phosphorus, zinc and sodium
4. Preventing poor appetite caused by micronutrient deficiencies, thereby facilitating catch-up growth
5. Favoring the growth of beneficial bacteria in the gut that enhance gut function and immune defenses

Trials with combined nutrition + infection control are underway
• WASH Benefits (water, sanitation and hygiene interventions: singly, combined or in combination with nutrition intervention)
• SHINE (independent and combined effects of improved water, sanitation and hygiene and improved infant feeding)
Both target mainly the postnatal period
Little evidence on impact of combined pre- and postnatal nutrition interventions
• Key trials conducted in 1970s• INCAP trial in Guatemala– Fortified food (atole) with high milk content
• Bogota study in Colombia– Child’s food ration included milk
• Intervention trial with fortified food supplements provided both pre- and postnatally not attempted since

Trials with combined pre- and postnatal nutrition are underway
• iLiNS Project: iLiNS-DYAD trials in Malawi and Ghana– Efficacy of maternal LNS given during pregnancy & first 6 mo
postpartum + child LNS given 6-18 mo• The Early Nutrition and Immune Development (ENID)
Trial in the Gambia– Efficacy of prenatal and infancy nutritional supplementation,
focused on infant immune development• Rang-Din Nutrition Study in Bangladesh
– Program efficacy study with 4 arms – one arm includes maternal LNS given during pregnancy & first 6 mo postpartum + child LNS given 6-24 mo

Next steps?
• Evaluate impact of combined prenatal and postnatal nutrition, ECD enrichment and prevention/control of infection throughout the 1000 days– Efficacy– Effectiveness
• Understand role of pre-conception nutrition (trials underway)
• Understand role of maternal mental health

Early Child Development
Washington, DC | May 2-3, 2013Maureen Black, Ph.D.
University of Maryland School of Medicine
Clean, Fed & Nurtured: Joining forces to promote child growth and development

Objectives
• Define Early Child Development• Threats to Early Child Development– Toxic Stress– Undernutrition
• Development of Disparities & Lifespan Perspective• Early Child Development Interventions– Early Learning Opportunities & Responsive Caregiving
• Integrated Interventions

Early Child Development Basics
• Early Child Development– Orderly progression of skills, based on maturation &
adaptation to specific culture/settings– Direct and Indirect relationships– Confusion: ECD refers to the intervention and the outcome

Social-Ecological Theory of Child Development
Distal threats and opportunities reach the child through
Proximal interactions between child & family
Bidirectional interactions
Bronfenbrenner & Ceci, 1994

Family Support
School and Community
Services
Child Development: Multiple Contributing Factors
Health Nutrition
LearningOpportunities
Sensitive/ResponsiveCaregiving
Social Protection
Protection from Stress/
Harm
Nutrition is necessary for child development, but
not sufficient!

Threats to Early Development
• Poverty and Undernutrition• Toxic stress• Children can handle, even benefit, from mild stress • Toxic stress • Institutionalization, maltreatment, neglect, trauma,
undernutrition• Lack of caregiver responsivity
Shonkoff , Pediatrics, 2012

How Toxic Stress Undermines Child Development
• Non-reversible changes to children’s physiology– Dysregulation of neuroendocrine system
• Hypothalamic Pituitary Adrenal (HPA) Axis• Elevated cortisol production
– Disrupt inflammatory signaling• Increased susceptibility to illness
Johnson et al., Pediatrics, 2013; 131:319-327
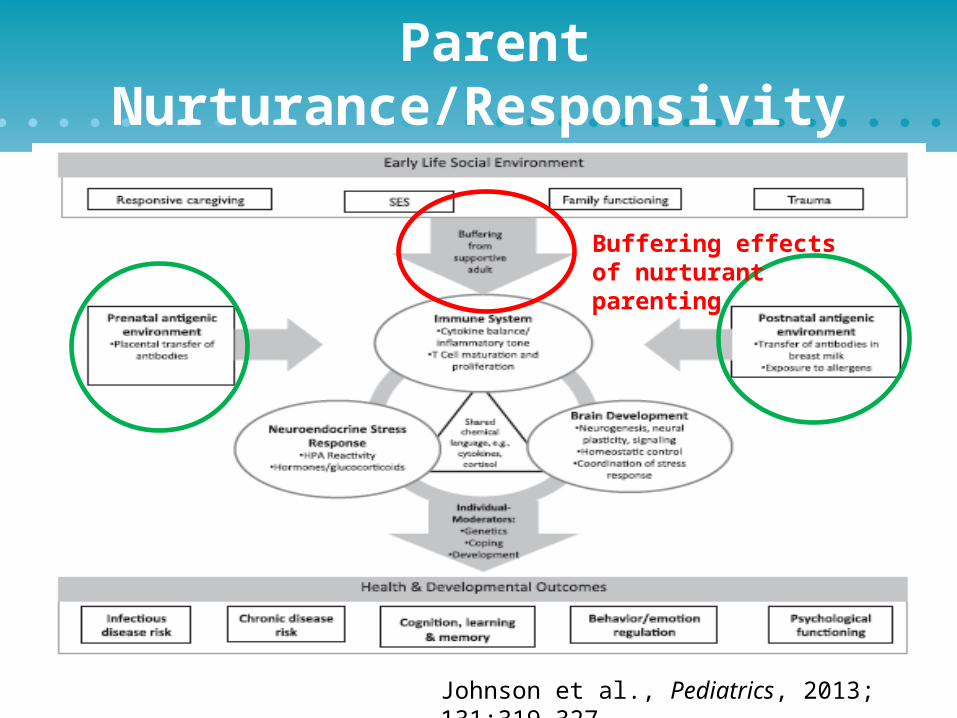
Parent Nurturance/Responsivity
Johnson et al., Pediatrics, 2013; 131:319-327
Buffering effects of nurturant parenting

Hippocampal volume by preschool depression severity & maternal support
Luby, PNAS, 2012;109(8):2854-9
Maternal support in early childhood predicts larger hippocampal volumes at school age.
Positive, responsive relationships can alleviate negative effects of stress (brain structure/function).

Fetus Late Infancy/Toddler Pubertal
Developmental Perspective
Thompson & Nelson, 2000
1000 days

Fetus Late Infancy/Toddler Pubertal
Developmental Perspective
Thompson & Nelson, 2000
Iron: 0.27 mg/day 11 mg/day 7 mg/day 0–6 months 6-12 months 1-3 years
1000 days

Fetus Late Infancy/Toddler Pubertal
Developmental Perspective
Thompson & Nelson, 2000
Iron: 0.27 mg/day 11 mg/day 7 mg/day 0–6 months 6-12 months 1-3 years
1000 days

Development of disparities & lifespan perspective

Development of disparities &lifespan perspective

2007 & 2011 Lancet Series on Child Development
• Over 200 million children < age 5 y in low & middle income countries do not reach developmental potential – Nutrition: Chronic undernutrition, micronutrient deficiencies– Lack of early learning opportunities– Extended to social & environmental risks
• Efficacy of early interventions – Early childhood policies & programs to reduce inequalities
– Cost of not investing in child dev programs
– Need for policies/procedures to scale up
www.globalchilddevelopment.org

Target of Interventions
• Prenatal– Prevent Toxic stress/LBW/Prematurity
• Infancy– Breastfeeding, complementary feeding – Responsive Parenting– Opportunities for early learning– Routines to promote regulation– Family support
Kramer et al., 2008; 2007 & 2011 Lancet series on Child Development

Early Child Development Intervention
• Early learning opportunities– Play– Explore– Interactions: give & take/serve & return
• Responsive Caregiving– Recognize & interpret child’s cues– Prompt– Developmentally appropriate– Enriching– Basis for responsive feeding
Black & Aboud, 2012

Child opens
mouth & accepts
Caregiver offers another
bite
Child looks away,
mouth shut
Caregiver offers a bite
of food
…………………...Time…………
RESPONSIVE FEEDING BEHAVIORS
PROMOTES HEALTHY EATING & GROWTH PATTERNS
Ummm, maybe she is telling me she wants to feed herself.

Child opens
mouth & accepts
Caregiver offers another
bite
Child looks away,
mouth shut
Child picks up food
& eats
Caregiver waits, smiles,
finger food
Caregiver offers a bite
of food
…………………...Time…………
PROMOTES HEALTHY EATING & GROWTH PATTERNS
RESPONSIVE FEEDING BEHAVIORS

Child opens
mouth & accepts
Caregiver offers another
bite
Child looks away,
mouth shut
Caregiver offers a bite
of food
…………………...Time…………
NON-RESPONSIVE FEEDING BEHAVIORS
HINDERS HEALTHY EATING & GROWTH PATTERNS
Oh no, I am late. She has to finish eating.

Child opens
mouth & accepts
Caregiver offers another
bite
Child looks away,
mouth shut
Child Cries & spits
out food
Caregiver holds child &force feeds
Caregiver offers a bite
of food
…………………...Time…………
HINDERS HEALTHY EATING & GROWTH PATTERNS
NON-RESPONSIVE FEEDING BEHAVIORS

Responsive/Unresponsive Feeding
RESPONSIVE• Provides healthy food on a
regular schedule in a setting conducive to eating
• Caregiver reads infant cues of hunger/satiety
• Responds to infant quickly – Direct & Nurturant– Builds regulatory skills
UNRESPONSIVE• Controlling, indulgent, or uninvolved• Ignores/overrides infant cues• Associated with
⁻ Difficult temperament⁻ Maternal mental health
symptoms⁻ Poor growth (under or
overweight)

Parenting interventions (0-3 yrs)
• Home visits, guidance and support from health providers, and group parent training
• Impacts are larger when:– parents and children participate together – interventions involve modeling and practice of
behavior– most disadvantaged children targeted
Lancet series on child development, 2007, 2011

Preschool interventions (3-5 yrs)
• Preschools improve children's cognitive & social-emotional development: school readiness
• Impact is greatest with high quality programs– Teacher-student ratio– Developmental curriculum– Student exploration– Teacher responsivity
Lancet series on child development, 2007, 2011

Characteristics of Successful Programs
• Integrated across sectors• Focus on disadvantaged children• Parents as partners with teachers to support children’s
development• Opportunities for children to initiate learning & play• Blend traditional child care, cultural beliefs &
evidence-based practices (curriculum, materials)• Systematic in-service training, supervision, monitoring,
and evaluation
Lancet series on child development, 2007, 2011

How do Integrated Programs Work?
Child Devel
Intervention Child Development
Direct effect of child development interventionLancet series on child development, 2007, 2011
Social-Emotional
Sensori-Motor
Cognitive/Language

How do Integrated Programs Work?
Nutrition
Intervention Child Development
Social-Emotional
Sensori-Motor
Cognitive/Language
Direct effect of nutrition intervention
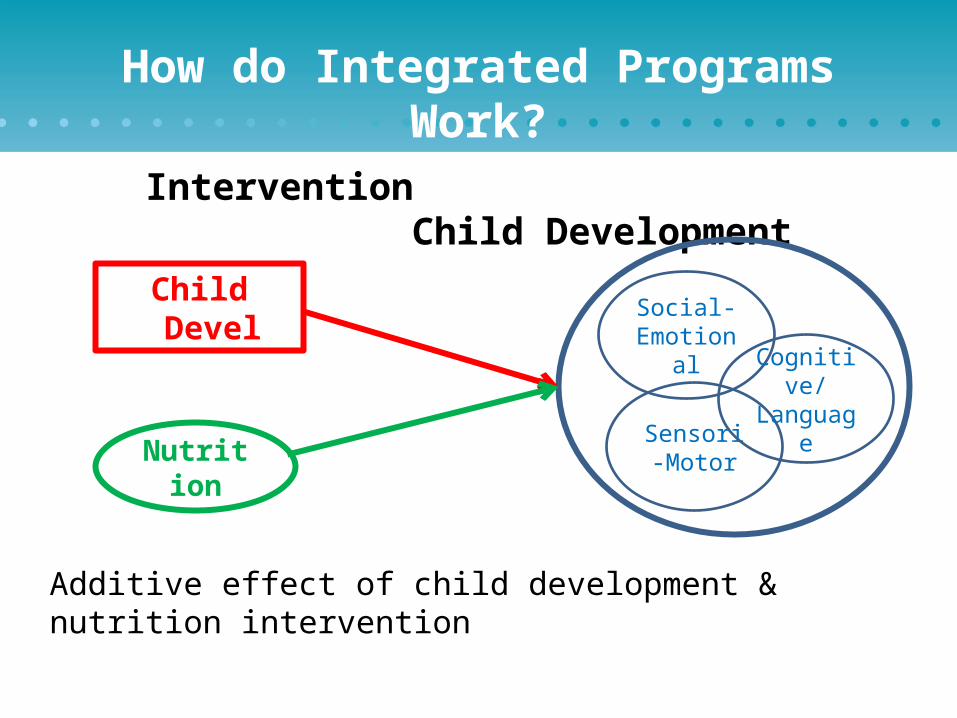
How do Integrated Programs Work?
Nutrition
Child Devel
Intervention Child Development
Social-Emotional
Sensori-Motor
Cognitive/Language
Additive effect of child development & nutrition intervention

Nutritional Supplementation and ECD Intervention in Jamaica
Basel
ine
6 m
os.
12 m
os.
18 m
os.
24 m
os.
80859095
100105110115
Nonstunted Control
Control
ECD Inter-vention
Sup-ple-mentedBoth
Cog
niti
ve t
est
scor
e
Grantham McGregor et al., 1991

DQ/IQ Stunted and Non-stunted Children in Jamaica: Effects of ECD Intervention
Walker et al., 2005
A B C D E
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
Non-stunted
Stunted - ECD
Stunted - ctl
SD
Score
A = 9-24 mos, B = 33-48 mos, C = 7-8 yrs, D = 11-12 yes, E = 17-18 yrs.

How do Integrated Programs Work?
Nutrition
Child Devel
Intervention Child Development
Social-Emotional
Sensori-Motor
Cognitive/Language
Synergistic effect: Impact of 2 interventions greater than their sum. One intervention enhances the impact of the other intervention.
Tested with an interaction term.

Example of Synergistic Intervention
The effect of zinc supplementation onhand-eye coord. enhanced by participation in a stimulation intervention.
Meeks Gardner et al., AJCN, 2005

Integrated Interventions
Considerations• Sectors differ
(education & nutrition)
• Child development beyond 1000 days
• Overwhelm health care/nutrition system
• Overwhelm caregivers• Outcome??
Rationale• Same sites• First 1000 days• Overlapping goals• Economy of scale• Home/clinic visit – integrated messages• Theory-based conceptualization


Integrated InterventionsQuestions
• Timing & severity of deprivations: Both nutrition and child development
• Timing, intensity, & duration of interventions• 1000 days? Beyond?• Training and Supervision: Ensure integration?• Outcomes and analytic models• Policies and integration across sectors• Sustainability and Scale

Lifespan Benefits of Early Child Development Programs
Ensure adequate nutrition, esp. first 1000 days School readiness (parenting & preschool programs)
Academic success Healthy psychological development
Avoid early pregnancyReduce violence & illegal behavior
Positive earning potential Adult health & civic contribution Strong & healthy children – 2nd gen
Break the Cycle of Poverty and DisparitiesPromote Human Capital

I need opportunities to play and learn with a sensitive, responsive caregiver. Remember, I am your future!
One more thing -

Thank You!


Clean, fed and nurtured?
Diarrhoeal Diseases
Environmental Enteropathy
Nematode infection
WASH
Child development
Time, costs, workload,
opportunities
Other Diseases


Dinner: Bistro Bistro
1727 Connecticut Ave NW, Washington, DC 20009





























