Embed Size (px)
Citation preview


• Water is the major component of internal Water is the major component of internal environment in the organism and it is environment in the organism and it is approximately approximately 60 % of body weight varying from varying from 45 % (in the fat elderly people) up to (in the fat elderly people) up to 70 % (in young (in young men). Women have more fat, less muscles, and men). Women have more fat, less muscles, and total quantity of water is total quantity of water is 50 %. The normal The normal deviations are observed approximately within the deviations are observed approximately within the limits of limits of 15 %. In children the content of water is In children the content of water is higher, than in the adult. With age the content of higher, than in the adult. With age the content of water gradually decreases. water gradually decreases.
• The large part of water The large part of water (35-45 % of body weight) is is inside the cells inside the cells (intracellular fluid). Extracellular fluid is is 15-25 % of body weight and is divided on to of body weight and is divided on to
• intravascular (5 %) (5 %)• interstitid (12-15 %) (12-15 %) • transcellular (1-3 %) (1-3 %)






During 24 hours in organism of the person there arrives
about 1,2 l of water with drinking with food - about 1 l about 300 ml of water is formed in oxidation of food
substances In normal water balance as much the same quantity
of water (about 2,5 l) is excreted from the organism:
by kidneys (1-1,5 l) by perspiration (0,5-1 l) and lungs (about 400 ml) with feces (50-200 ml)

• The fluids are The fluids are in constant movementin constant movement: the liquid, which : the liquid, which washes the cells, brings nutritives substances and oxygen washes the cells, brings nutritives substances and oxygen and removes the products of metabolism and and removes the products of metabolism and carbondioxyde. carbondioxyde.
• Cell membranes are freely permeable for water, but are not Cell membranes are freely permeable for water, but are not permeable for many dissolved substances, that’s why permeable for many dissolved substances, that’s why movement of liquid between intracellular and extracellular movement of liquid between intracellular and extracellular takes place takes place by osmotic gradientby osmotic gradient, which is created by , which is created by osmotically active substances. By the law of isoosmolarity osmotically active substances. By the law of isoosmolarity the water moves through the biologic membranes to the the water moves through the biologic membranes to the side of higher concentration of dissolved substances. side of higher concentration of dissolved substances. Dissolved substances, which are freely permeable for Dissolved substances, which are freely permeable for membrane, do not influence the movement of water. membrane, do not influence the movement of water.
• The exchange of water between vessels and tissues is The exchange of water between vessels and tissues is carried out by carried out by Starling’s mechanism:Starling’s mechanism: water, electrolytes, water, electrolytes, some organic substances easily move through the capillary some organic substances easily move through the capillary walls, but more difficult proteins are transported. In healthy walls, but more difficult proteins are transported. In healthy person for one day from blood to tissue 20 l of a fluid is person for one day from blood to tissue 20 l of a fluid is filtered, 17 l is absorbed back to capillaries and about 3 l filtered, 17 l is absorbed back to capillaries and about 3 l flows from tissue by lymphatic capillaries and through the flows from tissue by lymphatic capillaries and through the lymphatic system comes back to the vessels. lymphatic system comes back to the vessels.



• Sodium is main cation of extracellular fluid. Chloride and bicarbonate represent anionic electrolyte group of extracellular space.
• In cell space the main cation is potassium and anionic group is represented by phosphates, sulfates, proteins residual anions and bicarbonate.
• Electrolytes provide 94-96 % of plasma osmolarity and sodium as a main ion of extracellular fluid – 50 % of osmotic pressure.
• As the capillary membrane is not permeable for proteins, colloid-osmotic pressure is the main force which moves free water and electrolytes through the capillary membrane by osmatic laws. Generally the organism is irresistable to osmotic gradients. The sudden change of fluid osmolarity in intracellular space leads to moving of fluid through cell membrane, therefore osmotic gradients are balanced.


• Water-electrolyte exchange is characterized by persistance, which is supported by nervous, endocrine mechanisms, and also by osmotic and electric forces. Its main parameter is water balance.
• The most important condition of persistance of water cell environments is their isotonic state. The value of cationic charges should be equal to the value of anionic charges both inside the cell and outside it. However, in biologic objects the intracellular potential prevails. In this condition the difference of potentials as between the cell and environment equal to 80 mV, as between separate elements of the cell (nucleus, protoplasm and shell or membrane) also is kept.
• Just the preservation of difference of potentials is one of main qualities of a cell ensuring possibility of realization of metabolic processes and its specific function.

• The persistance of volume and osmolarity of intracellular fluid The persistance of volume and osmolarity of intracellular fluid is supported by is supported by regulatory mechanisms, main effectory organ main effectory organ of which are of which are kidneys.
• The increase of blood plasma osmolarity by loss of pure water The increase of blood plasma osmolarity by loss of pure water is specific irritant of is specific irritant of osmoreceptors situated in anterior hypothalamus. In result there is In result there is feeling of thirst. The thirst is The thirst is one of main and the most sensitive signs of water deficiency. one of main and the most sensitive signs of water deficiency. The presence of thirst shows that water volume in The presence of thirst shows that water volume in extracellular space is reduced concerning the content of salts extracellular space is reduced concerning the content of salts in it. in it.
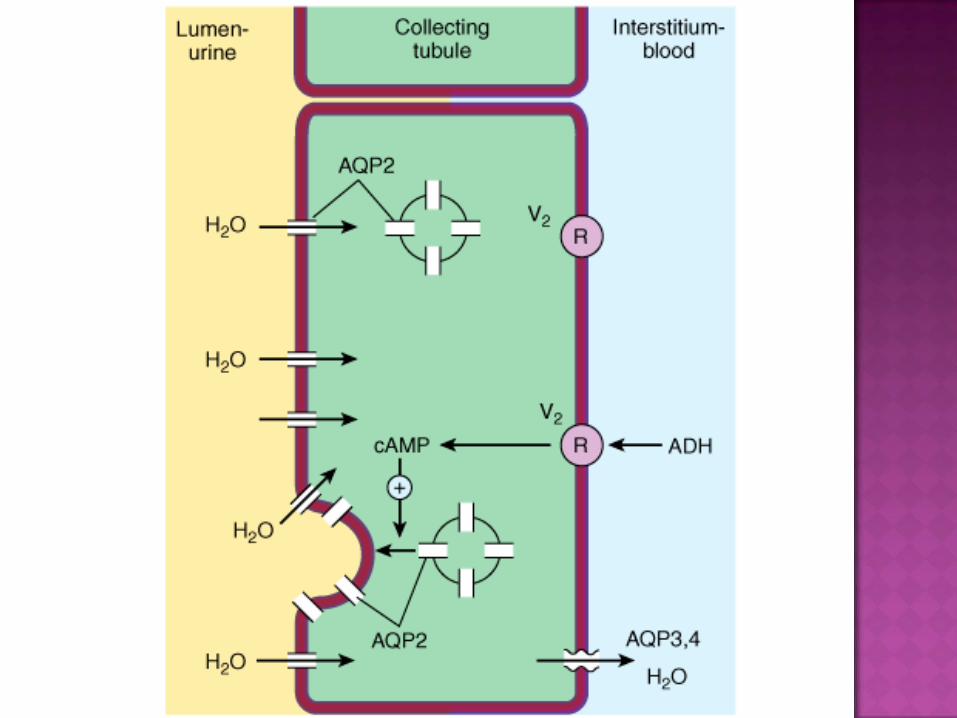
• The irritation of osmoreceptors of hypothalamic area (in The irritation of osmoreceptors of hypothalamic area (in increase of blood osmolarity), and also volume receptors in increase of blood osmolarity), and also volume receptors in left atrium (in decrease of blood volume) stimulates the left atrium (in decrease of blood volume) stimulates the secretion of secretion of vasopressin (ADH) by supraoptical and by supraoptical and paraventricular nuclea of hypothalamus. Vasopressin paraventricular nuclea of hypothalamus. Vasopressin strengthens water reabsorption in distal canaliculi of nephron strengthens water reabsorption in distal canaliculi of nephron through activation of V2 receptors of epithelium and through activation of V2 receptors of epithelium and derivation of cAMP, which increases their permeability for derivation of cAMP, which increases their permeability for water. The stimulating effect of ADH is determined by water. The stimulating effect of ADH is determined by permissive action of ACTH from adenohypophysis. It leads to permissive action of ACTH from adenohypophysis. It leads to decrease of diuresis, increase of volume of circulatting blood. decrease of diuresis, increase of volume of circulatting blood. Besides ADH contracts the arteriolas and increases the Besides ADH contracts the arteriolas and increases the arterial pressure.arterial pressure.



The irritation of receptors in afferent artery of kidneys (decrease of renal circulation, blood loss) and sodium receptors of dense spot in juxtaglomerular apparatus (sodium deficiency) strengthens synthesis and clearing release of renine.
Under influence of renine the angiotensinogen of blood plasma will transforn to angiotensin I. This substance doesn’t have biological activity yet. In passing through lung capillaries angiotensin І under action of converting enzyme of endothelial cells will transform to angiotensin II. Further under influence of angiotensinases there is formation of angiotensin III.
Angiotensin II has two effects: causes contraction of smooth muscles in arteriolas,
therefore there is their narrowing and arterial pressure is increased
acting on glomerular zone of adrenal cortex, it activates the secretion of aldosteron.
Angiotensin III has only one action – it increases the secretion of aldosteron.



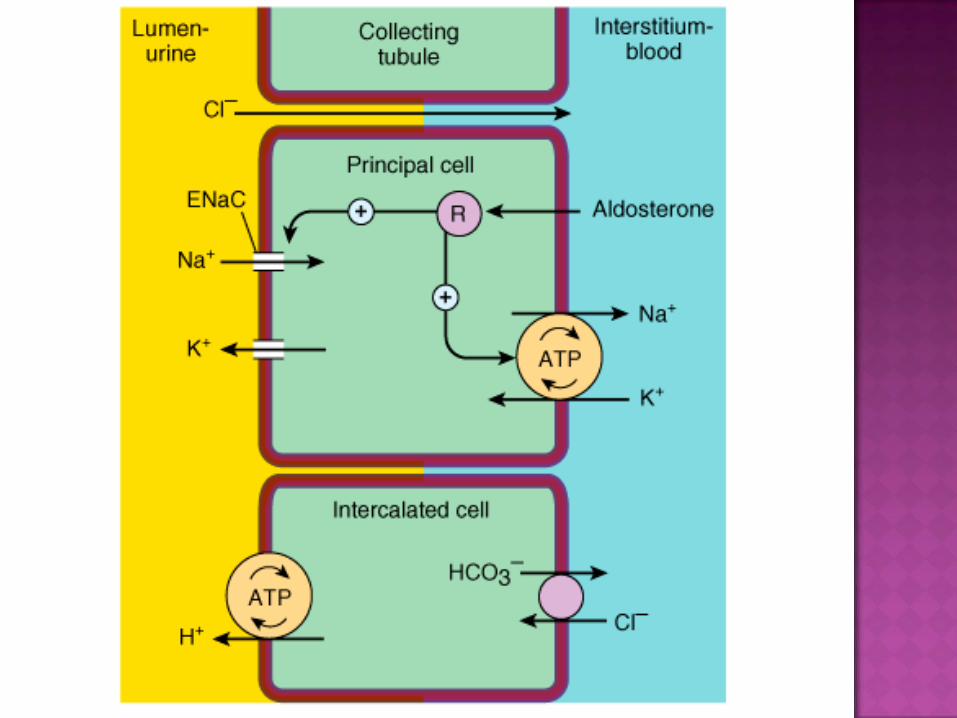
• The main functional effects of aldosteron are connected with its influence on kidneys. Acting on distal curre canaliculi of nephrons, aldosteron causes:
• increases reabsorption of Na • increases secretion of K • increases secretion of Н (strengthens
acidogenesis)


Antidiuretic and antisodiumuretic mechanisms are opposite to diuretic and sodium-uretic.
Their primary factors are renomodular prostaglandins and atrial sodium-uretic. It is synthesized in the cells of atrium left atrium. It increases diuresis and Na-uresis, weakens smooth muscle fibres of vessels and decreases arterial pressure. The content of atrial sodium-uretic factor in left atrium and its secretion to blood is increased after redundant consumption of water and salts, owing to atrial dilation, increase of arterial pressure, and also stimulation of -adrenoreceptors and receptors of vasopressin.
These mechanisms function constantly and provide restoring of water-electrolyte balance after blood loss, dehydration, in case of water excess in the organism, and also change of osmotic concentration of extracellular fluid.


The disturbances of water-salt metabolism are divided on dehydration and hyperhydration
Depending on change of osmotic concentration (the ratio of water and electrolytes) dehydration and hyperhydration are subdivided on
isoosmolaric hypoosmolaric hyperosmolaric.

Isoosmolaric dehydration develops in equivalent loss of water and electrolytes. It is observed in polyuria, intestinal toxicosis, acute bleeding, vomiting, diarrhea. The decrease of amount of tissue fluid goes mainly for the account of extracellular.
Hypoosmolaric dehydration is characterized by decrease of osmotic pressure of extracellular fluid and is observed in case of salt’s loss mainly. It develops in loss of stomach and intestinal secreation (diarrhea, vomiting), increased sweating, if the water loss is compensed by drinking without salt. In such case the decrease of osmotic pressure in extracellular environment results in transition of water in cells, owing to this the condensation of blood and disturbance of blood circulation, hypovolemia occur; the filtrating ability of kidneys is decreased, dehydration of cells develops (in particularly nervous) and violation of their function. Dehydration and loss of electrolytes results in violation of acid-base balance. So, dehydration with loss of chlorides and H ions of gastric juice results in alcalosis. Decrease of pancreatic and intestinal juices, which contain more sodium and hydrocarbonates, leads to acidosis.

Hyperosmolaric dehydration develops at loss of water, therefore osmotic pressure of intracellular liquid is increased. It is observed when the loss of water exceeds loss of electrolytes (first of all, sodium), for example, for want of hyperventilation, proffuse sweating, loss of saliva, and also at diarrhea, vomiting, polyuria, when reimbursement of water loss is not enough. In this case the decrease of volume of extracellular fluid and increase of its osmoticity occurs.

The increased leadingout of water from an organism is observed for want of diabetes insipidus.
The major factor of pathogenesis of diabetes insipidus is the decrease of production of vasopressin.
The reason of diabetes insipidus can be tumours, inflammatory process, sarcoidosis or trauma injuring neurohypophysis.
The second form of illness – primary polydypsia of psychogenic origin, which is accompanied with secondary polyuria.
The third form of illness is nephrogenic diabetes insipidus, in which basis the reduction of sensitivity of kidneys to vasopressin lays. In this case the decrease of production in epithelium of canaliculi of cAMP and decrease of permeability of distal part of nephron canaliculus for water is marked.

Extracellular hyperhydration is an increase of volume of fluid in extracellular sector of an organism. It is a result of positive water balance
The reasons of extracellular hyperhydration can be:
1. Redundant receipt of water in an organism: а) drinkingo of salty water, not compensating
thirst; b) intravenosus introduction of big quantity of
liquid to the patient 2. Delay of water in an organism owing to violation
of its excretion by kidneys: а) renal insufficiency b) violation of regulation of kidneys (primary and
secondary hyperaldosteronism, hyperproduction of antidiuretic hormone)
At isoosmolaric hyperhydration osmotic pressure of extracellular fluid is not changed. This kind of violations can be observed for a while after introduction of redundant amount of isotonic solution.
Hypoosmolaric hyperhydration (the water poisoning) is characterized by decrease of osmotic pressure of extracellular fluid. This kind of hyperhydration in experiment on animals is simulated by repeated introductions of water into stomach on a background of introduction of vasopressin, aldosterone or removal of adrenal glands. In clinic the water poisoning is possible in reflectory anuria, and also in the second stage of acute renal insufficiency.
Hyperosmolaric hyperhydration is characterized by increase of osmotic pressure of extracellular fluid and can develop in use for drinking of salty marine water.


Edemas is a redundant accumulation of fluid in tissues of an organism and serous cavities.
There are general and local edemas. General edemas are manifestation of extracellular hyperhydration, local are connected with the dislocation of fluid balance in the limited site of a tissue or organ.
Depending on mechanisms of development edemas can be:
1) hydrostatic 2) oncotic 3) membranogenic4) lymphogenic5) as a result of violation of neuro-endocrine
regulation

Hydrostatic edemas can be stipulated by the following mechanisms:
increase of blood volume (hypervolemic edemas) increase of venosus pressure (congestive
edemas) primary violation of microcirculation – dilation of
arteriolas and spasm of venules (microcirculatory edemas)

Oncotic edemas naturally develop in decrease of the contents in blood plasma of proteins (albumins) and decrease of gradient of osmotic pressure between blood and intercellular fluid. It arises first of all in hypoproteinemia (proteinuria, starvation, liver cirrhosis) owing to decrease of oncotic pressure of blood, and also in accumulation of osmotically active substances (Na, proteins, products of metabolism) in intercellular space. Edema is increased in increase of oncotic pressure in interstitial fluid, which in turn strengthens filtering. Oncotic pressure of an interstitial fluid is increased also in blockade of lymph circulation. Hydrofilness of tissue colloids depends also on concentration of Н. In shift of рН in the acidic side edema of parenchymatous elements and dehydration of connective tissue occurs. In shift of рН in the alkaline side connective tissue is hydrated.

• Membranogenic edemas arises owing to increase of permeability of vessel wall. In an organism hydrostatic, oncotic and osmotic pressure can show the action only in certain state of vessel permeability. The increase of permeability is accompanied by an exit of proteins from blood into interstitial environment, decrease of oncotic pressure of blood plasma and its increase in interstitial space. Therefore increase of permeability of capillaries is the premise of edema development. This mechanism is leading in development of allergic, inflammatory, toxic edemas.

Lymphogenic edemas arises owing to violations of lymph formation and lymph circulation. In this case the leadingout of proteins with lymph, in norm filtered in tissue is infringed, and tissue oncotic pressure is increased. Among the reasons of development of lymphogenic edemas it is necessary to define the compression of lymphatic vessels by scar tissue; increase of central venous pressure (insufficiency of heart), prohibitive to inflow of lymph in the system of blood circulation. It is found out, that venous congestion, which is accompained by increase of pressure in upper vena cava (as well as local venous congestion, for example, in thrombophlebitis), causes reflectory spasm of lymphatic vessels. Besides collected in edemas interstitial fluid compresses lymphatic vessels.

The delay of water connected with disorder of regulation of water-electrolyte metabolism, is observed in hypofunction of thyroid gland (myxedema), increase of production of vasopressin, insulin, raising hydrofilness of tissue colloids, in primary, and also secondary hyperaldosteronism (for example, in cardiac insufficiency, nephritic syndrome, liver cyrrhosis etc.).
Hormonal factors in regulation of disorder of water-electrolyte metabolism act in close connection with neurogenic.
This interrelation distinctly is visible in pituitary-adrenal mechanism playing the important role in development of cardiac and other kinds of edemas.

In pathogenesis of edemas there are two stages.The first stage – is accumulation of the connected
water. Edematic liquid contacts with tissue colloids and is stored mainly in gel-like structures (collagenic fibres, main substance of connective tissue). In such case the clinical signs of edema insignificant – turgor of tissue is increased a little.
The second stage is accumulation of free water. When weight of the connected water is increased approximately on 30%, and the hydrostatic pressure in tissue achieves atmospheric, free untied water is increased. Then there are expressed signs of edema: free water moves according to force of gravitation, there is a symptom of “fossa” in pressing on tissue.

The main reason of intracellular hyperhydria is decrease of osmotic pressure of extracellular fluid, that is connected to development of hyponatriemia. In these conditions water under the laws of osmos goes from interstitial space in cells – there are signs of generalized cell edema.
Among mechanisms of cell edema major importance belongs to:
Disintegration of intracellular structures, proteins, owing to what connected with them cations (are in main ions K) and intracellular osmotic and oncotic pressure is increased
Disturbances of permeability of cell membrane, therefore the ions of sodium and chlorine arrive into a cell and increase osmotic pressure of cytoplasm
Disorders of functioning of sodium-potassium pumps causing accumulation of sodium ions in a cell

Edema of a cell aggravates processes of its damage. It is connected with that:
the permeability of cell membranes as a result of their osmotic expansion is increased
the phenomenon of electrical “damage” of plasmatic membrane of excitable cells is possible
there is a mechanical break of membranes in their expansion

Depending on the reasons and mechanisms of occurrence there are
cardiac renal liver cachectic inflammatory toxic allergic lymphogenic neurogenic ndocrine etc

arises mainly in case of venous congestion and increase of venous pressure, that is accompanied by increase of filtering of blood plasma in capillary vessels. Developing in blood congestion hypoxia results in disturbance of permeability of a vessel wall. The large significance in occurrence of cardiac edemas in insufficiency of circulation belongs also to reflectory-renin-adrenal mechanism of water delay.

• In pathogenesis of edema at glomerulonephritis primary significance is decrease of glomerular filtering, that leads to delay of water in an organism. In such case sodium reabsorption in nephron canaliculi is also increased, in what the known role belongs to secondary aldosteronism, and also increase of permeability of vessels. In presence of nephrotic syndrome on the foreground the factor of hypoproteinemia (owing to proteinuria) acts which is combined with hypovolemia and stimulation of production of aldosteron.

In development of liver edema in liver injury the important role hypoproteinemia plays, owing to violation of synthesis of proteins in liver. Some value in this case has increase of production or violation of inactivation of aldosterone. In development of ascites in cirrhosis the main role belongs to difficulty of liver blood circulation and increase of hydrostatic pressure in the system of portal vein.

Cachectic edema develops in alimentary dystrophia (starvation), hypotrophia at children, malignant tumours and other exhaustive diseases. The major factor in its pathogenesis is hypoproteinemia, stipulated by violation of protein synthesis, increase of permeability of wall of capillaries and accumulation of products of disintegration in tissues
In pathogenesis of inflamantory and toxic edemas (in action of chemical substances, bites of bees and other poisonous insects) the primary role is played by disorders of microcirculation in the center of injury and increase of permeability of capillary vessels wall. In development of these violations the important role belongs to released vasoactive mediators: biogenic amines (histamine, serotonin), prostaglandins, leukotriens, kinins

Allergic edemas arises in connection with development of allergic respons (urticaria, injury of joints etc.). The mechanism of development of allergic edemas in many things is similar to pathogenesis of inflammatory and neurogenic edema. The disorder of microcirculation and permeability of capillary vessels wall is caused by biologically active substances and immune complexes.
Neurogenic edema develops as a result of damage of nervous regulation of water metabolism, tissue and vessels trophics. Here edema of limbs in hemiplegia and syringomyelia, edema of face in neuralgia of trigeminal nerve and Quincke’s edema are concerned. In origin of neurogenic edema the important role belongs to increase of permeability of vessel wall and disorder of metabolism in damaged tissues.

Myxedematous edemas is special variant of edemas, in which basis the increase of hydrophilic tissue colloids lays. In this case in tissues the amount of connected water increases. Myxedematous (“mucous”) edemas are characteristic for hypofunction of thyroid gland.

• The consequences of edema depend on its degree. The significant accumulation of fluid causes compression of tissues, violation of their functions. The congestion of fluid in body cavities infringes the function of neighboring organs. So, ascites in pleural cavity aggravates the breath, and the accumulation of transsudate in pericardium infringes activity of heart.