Embed Size (px)
Citation preview
WCLA MCLE 9-8-11
• AMA Guides (Part 2): How Impairment Is Rated & More Case Studies
• Thursday September 8, 2011 from 12:00 noon to 1:00 pm
• WCLA member Robert T. Bernat, JD, MD• James R. Thompson Center Auditorium,
Chicago, IL• 1.0 Hour General MCLE Credit
New Section 8.1b 820 ILCS 305/8.1b
• Sec. 8.1b. Determination of permanent partial disability. For accidental injuries that occur on or after September 1, 2011, permanent partial disability shall be established using the following criteria: (a) A physician licensed to practice medicine in all of its branches preparing a permanent partial disability impairment report shall report the level of impairment in writing. The report shall include an evaluation of medically defined and professionally appropriate measurements of impairment that include, but are not limited to: loss of range of motion; loss of strength; measured atrophy of tissue mass consistent with the injury; and any other measurements that establish the nature and extent of the impairment. The most current edition of the American Medical Association's "Guides to the Evaluation of Permanent Impairment" shall be used by the physician in determining the level of impairment. (b) In determining the level of permanent partial disability, the Commission shall base its determination on the following factors: (i) the reported level of impairment pursuant to subsection (a); (ii) the occupation of the injured employee; (iii) the age of the employee at the time of the injury; (iv) the employee's future earning capacity; and (v) evidence of disability corroborated by the treating medical records. No single enumerated factor shall be the sole determinant of disability. In determining the level of disability, the relevance and weight of any factors used in addition to the level of impairment as reported by the physician must be explained in a written order.

3
KEY POINT• Physicians rate impairment– Medical determination– Medical training required (Anatomy, Physiology)
• Judges rate disability– Judge “factors in” NON-medical factors
• Doctor: “DoDoctor: “Do NOTNOT think aboutthink about the ability to do his/her job, availability of similar jobs in the local economy, etc., as that is the judge’s task, NOT your task.”

4
Impairment DOES NOT equal Disability• Example: both a lawyer and a pianist sustain
an amputation of the non-dominant little finger.– Both have the same impairment• 100% of the digit, 10% of the hand, 9% of
the upper extremity, 5% whole person– The lawyer has no disability– The pianist is unable to perform his occupation• Totally disabled for his occupation• Fully capable of many jobs
• Physician’s role: Determine IMPAIRMENT

5
Impairment is NOT Disability
• “In disability evaluation, the impairment rating is ONE of several determinants of disablement. Impairment rating is the determinant most amenable to physician assessment; it must be further integrated with contextual information typically provided by nonphysician sources regarding psychological, social, vocational, and avocational issues.” – page 6
Unless otherwise specified page numbers refer to the Guides, 6th Edition

Basic AMA Guides Analysis• Maximum Medical Improvement• Determine Diagnosis (DBI) & Class (CDX) (0-4)• Default Impairment is middle # in array of 5 in CDX• Adjust Default by Net Adjustment for Grade Modifiers (GM):
– Functional History (FH) (0-4)– Physical Examination (PE) (0-4)– Clinical Studies (CS) (0-4)
• Net Adjustment for each GM is GM minus CDX • Move Default Impairment to left or right based on Net Adjustment
Formula (e.g. -2 net adjustment moves 2 spaces to left)• Never leave the CDX (e.g. +4 does not go into next CDX)• Combine Impairments if necessary

Maximum Medical Improvement
• “Individual’s ability to work” is “beyond the scope of the Guides.” pg. 24.
• “as good as they are going to be from the medical and surgical treatment available” pg. 26
• “Date from which further recovery or deterioration is not anticipated, although over time (beyond 12 months) there may be some expected change.” pg.26.
• Compare to IWCC Rule 7030.20 ( 6 months)

Diagnosis (DBI) & Class (CDX)
• DBI: Diagnosis; going down more severe • CDX: 5 Classes 0-4; left to right more severe• Regional Grids – Upper Extremities (Chapter 15): Digit; Wrist;
Elbow; Shoulder (CTS is UE)– Lower Extremities (Chapter 16): Foot & Ankle;
Knee; Hip (Foot is UE)– Spine & Pelvis (Chapter 17): Cervical; Thoracic;
Lumbar; Pelvis

Cervical Spine Regional GridCervical Spine Regional Grid

Methodology for Grade Determination Within-Methodology for Grade Determination Within-Class:Class:

Grade ModifierFunctional History (FH or GMFH)
• Functional impact of the condition– Subjective reports– Self-report tool (administered, scored, consistent)• UE: QuickDash (Disabilities Arm, Shoulder & Hand)• LE: AAOS Lower Limb Questionnaire • Spine: PDQ (Pain Disability Questionnaire)
• Determine GMFH (0-4)• Subtract CDX from GMFH(GMFH-CDX)=net
GMFH

Adjustment Grid SummaryAdjustment Grid Summary
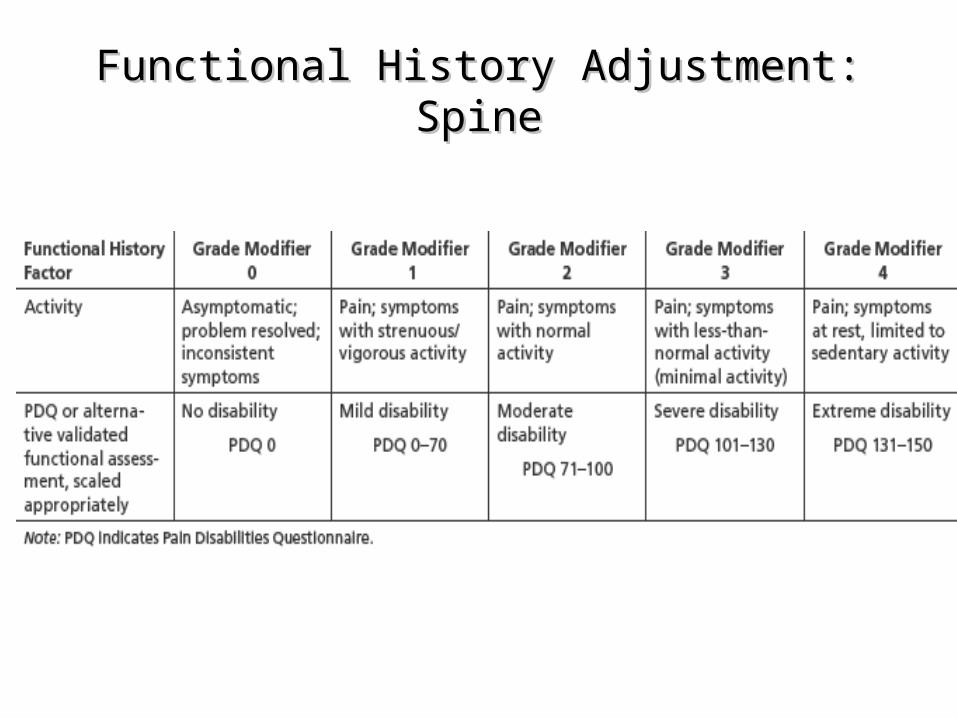
Functional History Adjustment: SpineFunctional History Adjustment: Spine

Grade ModifierPhysical Examination (PE or GMPE)• “Facilitate communication by easing anxiety” pg. 28• “Patient should be encouraged to give full” effort”• “Extremities should be documented bilaterally”• “Specific measurements should be reproducible”• Determine GMPE (0-4)• Subtract CDX from GMPE(GMPE-CDX)= net GMPE

Physical Examination Adjustment: SpinePhysical Examination Adjustment: Spine
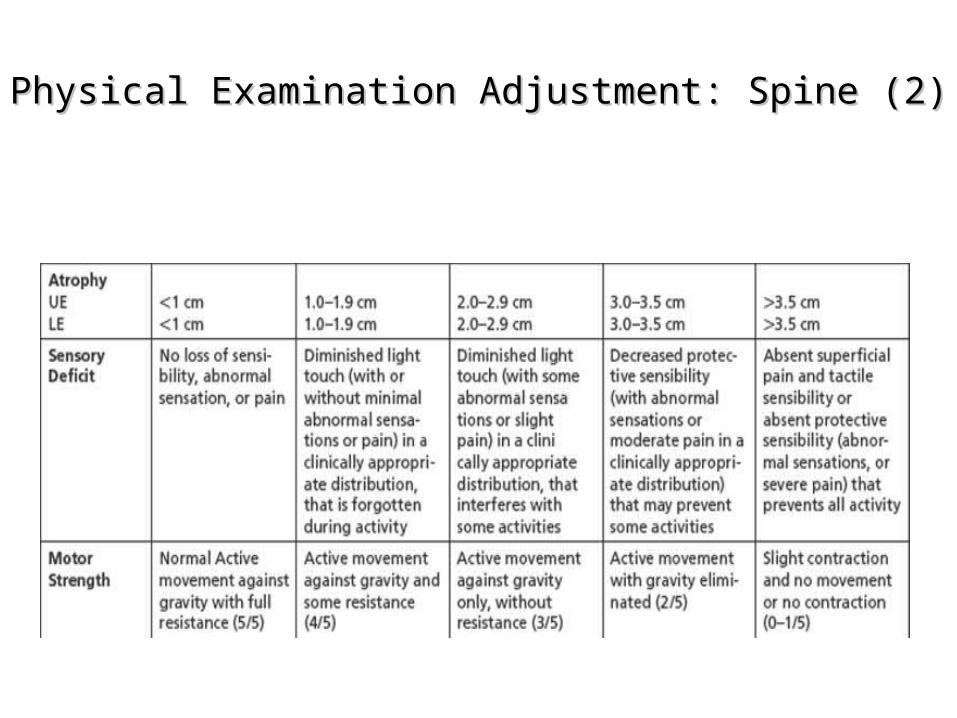
Physical Examination Adjustment: Spine (2)Physical Examination Adjustment: Spine (2)

Grade ModifierClinical Studies (CS or GMCS)
• Imaging & Electrodiagnostic: X-ray; MRI; EMG; NCV
• Operative reports• Current?• Determine GMCS (0-4)• Subtract CDX from GMCS(GMCS-CDX)=net
GMCS

Clinical Studies Adjustment: SpineClinical Studies Adjustment: Spine

Net Adjustment Formula
• CDX = Class of Diagnosis (Regional Grid) • GMFH = Grade Modifier Functional History• GMPE = Grade Modifier Physical Exam• GMCS = Grade Modifier Clinical Studies• Net Adjustment = (GMFH-CDX) + (GMPE-CDX) + (GMCS-CDX)• CDX will always be same in Net Adjustment• Each subtotal can be positive or negative• Total Net Adjustment can be positive or negative• Move grade within CDX to right or left of Default based on
Net Adjustment (+ right; - left)

Net Adjustment Formula
• CDX = Class of Diagnosis = 2• Default = 11 ( 9 10 11 12 13) • GMFH = Grade Modifier Functional History = 2• GMPE = Grade Modifier Physical Exam = 3• GMCS = Grade Modifier Clinical Studies = 2 • Net Adjustment = (GMFH-CDX) + (GMPE-CDX) + (GMCS-CDX)• Net adjustment = (2-2) + (3-2) + (2-2)= 0 + 1 + 0 = +1• Move grade within CDX to right or left of Default based on
Net Adjustment (+ right; - left)• Default is 11, move +1 to right = 12% WPI
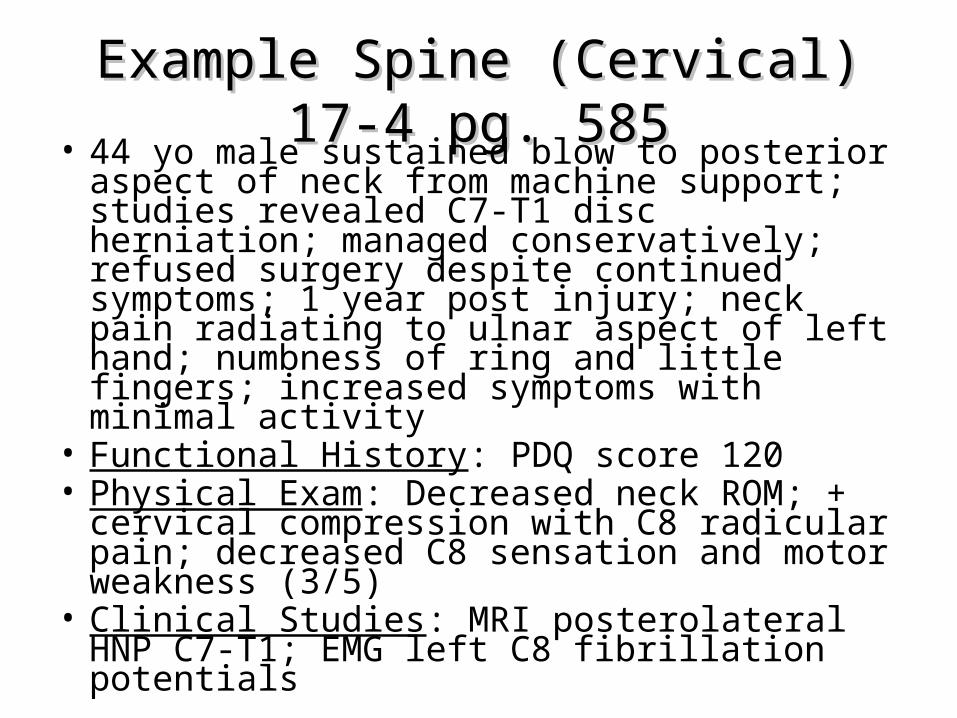
Example Spine (Cervical) 17-4 pg. 585Example Spine (Cervical) 17-4 pg. 585• 44 yo male sustained blow to posterior aspect of
neck from machine support; studies revealed C7-T1 disc herniation; managed conservatively; refused surgery despite continued symptoms; 1 year post injury; neck pain radiating to ulnar aspect of left hand; numbness of ring and little fingers; increased symptoms with minimal activity
• Functional History: PDQ score 120 • Physical Exam: Decreased neck ROM; + cervical
compression with C8 radicular pain; decreased C8 sensation and motor weakness (3/5)
• Clinical Studies: MRI posterolateral HNP C7-T1; EMG left C8 fibrillation potentials

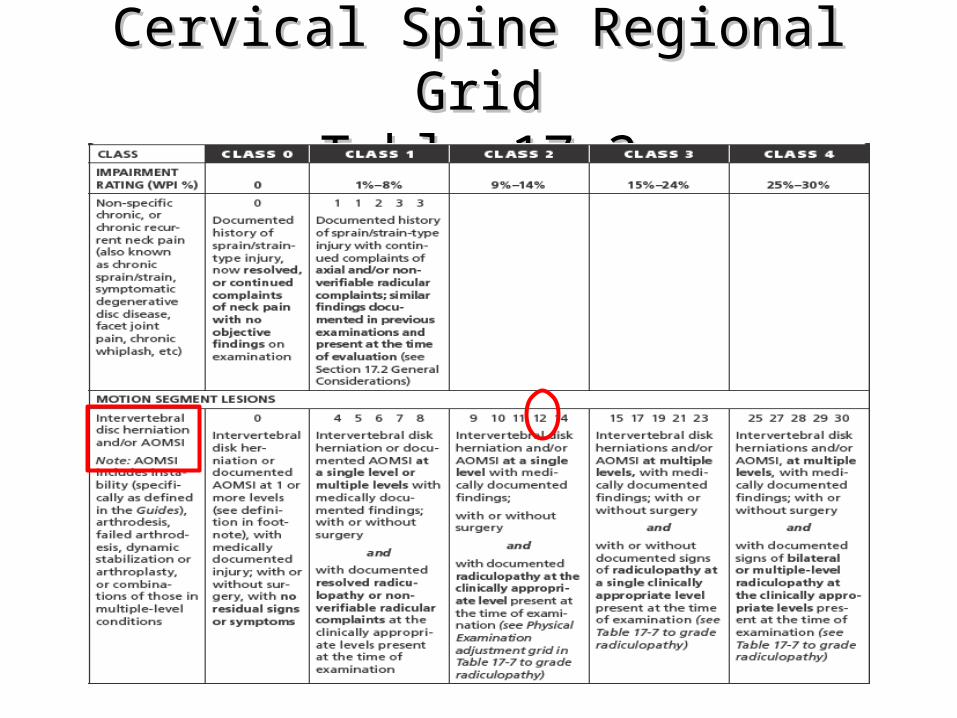
Example Spine (Cervical) 17-4 pg. 585Example Spine (Cervical) 17-4 pg. 585• Diagnosis: (Table 17-2) Regional Impairment Diagnosis
for Cervical Spine is consistent with “Intervertebral disc herniation and/or AOMSI at a single level with medically documented findings; with or without surgery and with documented radiculopathy at the clinically appropriate level present at the time of the examination”; assigned to Class 2, default Grade C value is 11% (CDX=2)
• Functional History: (Table 17-6) Grade 3 modifier based on symptoms with minimal activity (3) and PDQ score 120 (3) (FH=3)
• Physical Exam: (Table 17-7) Grade 2 modifier based on sensory and motor findings; decreased neck ROM; + cervical compression with C8 radicular pain; decreased C8 sensation and motor weakness (3/5) (PE=2)
• Clinical Studies: (Table 17-9) Grade 2 modifier based on positive EMG left C8 fibrillation potentials (CS=2)

Example Spine (Cervical) 17-4 pg.585Example Spine (Cervical) 17-4 pg.585
• CDX = 2 (diagnosis disc herniation w/radiculopathy)• FH = 3 (PDQ =120)• PE = 2 (3/5 motor weakness)• CS = 2 (EMG single nerve root) • Net adjustment: (GMFH-CDX) + (GMPE-CDX) + (GMCS-CDX)• Net Adjustment: FH(3-2) + PE(2-2) + CS(2-2) = +1• Net Adjustment = +1, move one position to right
from default• Default is 11%; +1 move to the right is 12% • Final Answer: 12% WPI

Cervical Spine Regional Grid Table 17-2Cervical Spine Regional Grid Table 17-2

Cervical Spine Regional Grid Table 17-2

Cervical FHTable 17-6
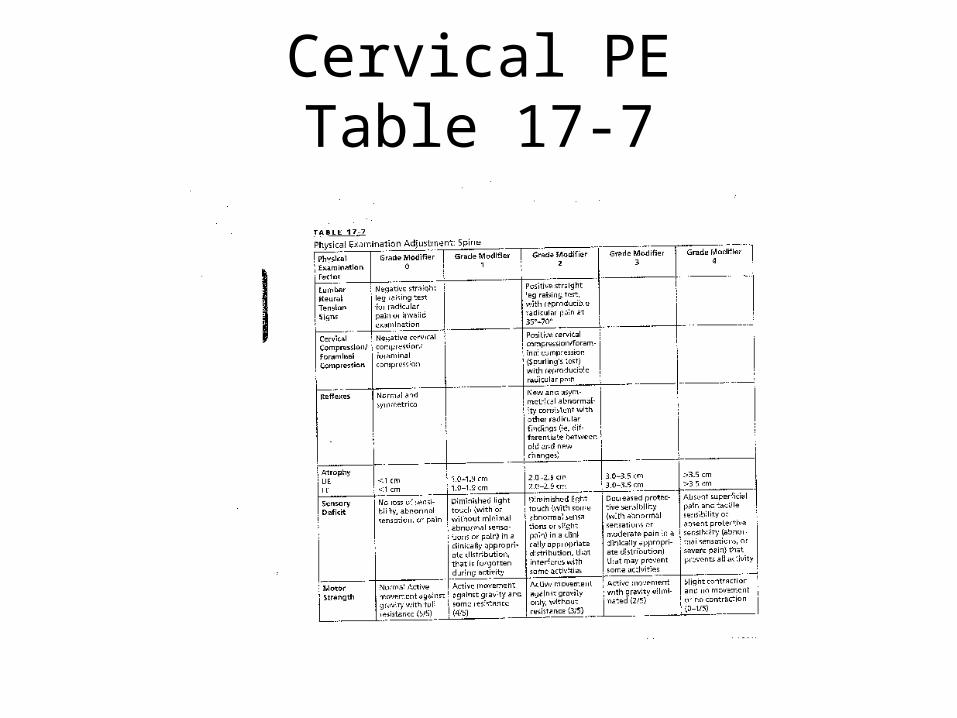
Cervical PETable 17-7

Cervical CSTable 17-9
Cervical Spine Regional GridCervical Spine Regional GridTable 17-2Table 17-2
30
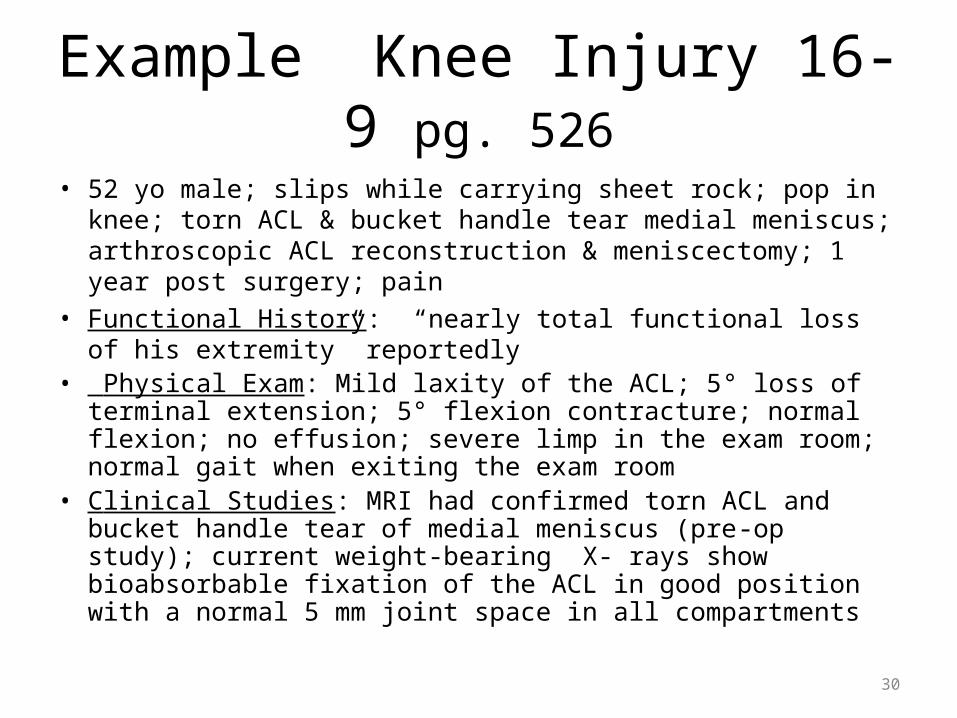
Example Knee Injury 16-9 pg. 526
• 52 yo male; slips while carrying sheet rock; pop in knee; torn ACL & bucket handle tear medial meniscus; arthroscopic ACL reconstruction & meniscectomy; 1 year post surgery; pain
• Functional History: “nearly total functional loss of his extremity” reportedly
• Physical Exam: Mild laxity of the ACL; 5° loss of terminal extension; 5° flexion contracture; normal flexion; no effusion; severe limp in the exam room; normal gait when exiting the exam room
• Clinical Studies: MRI had confirmed torn ACL and bucket handle tear of medial meniscus (pre-op study); current weight-bearing X- rays show bioabsorbable fixation of the ACL in good position with a normal 5 mm joint space in all compartments

31
Example Knee Injury 16-9 pg. 526• Requires the examiner to pick one diagnosis for the region; the anterior instability
diagnosis was chosen; meniscal tear reflected in adjustments• Diagnosis: (Table 16-3) Regional Impairment Diagnosis for LE Knee
consistent with “Cruciate or collateral ligament injury with mild laxity “assigned to Class 1; default Grade C value is 10% LEI (CDX=1)
• Functional History: (Table 16-6) Not used because judged unreliable in the presence of only mild instability and no atrophy; could have been 4 (FH=NA)
• Physical Exam: Grade 1 modifier; instability not used as grade modifier since stability was used in class assignment (could have been 2/3 based on instability); no atrophy would be grade 0; 5° flexion contracture would be rated at 10% LEI (Table 16-23); 10% LEI rating is “mild” (Table 16-25) which is Grade 1 PE modifier for ROM (Table 16-7) (PE=1)
• Clinical Studies: (Table 16-8) Grade 2 modifier; ACL reconstruction in good position without joint space narrowing on current weight bearing x-rays by itself would be a grade 1 or mild pathology adjustment; meniscal tear and subsequent repair (documented in the operation report) would justify moving up grade 2 for the final clinical studies adjustment (CS=2)

32
Example Knee Injury 16-9 p 526• CDX = 1 (diagnosis ACL w/mild laxity ; meniscal injury
not used)• FH = 4 (but not utilized as INVALID)=NA• PE = 1 (flexion contracture)• CS = 2 (meniscal repair in operative report)• Net Adjustment: (GMFH-CDX)+(GMPE-CDX)+(GMCS-CDX )• Net Adjustment: FH(NA)+PE(1-1)+CS(2-1)= +1 • Net Adjustment = + 1, move one position to right
from default • Default is 10%; + 1 move to the right is 12%• Final Answer: 12% LEI

Example Knee Injury Regional GridTable 16-3

Knee Injury Functional HistoryTable 16-6

Knee Injury Physical ExamTable 16-7

Knee Injury Range of MotionTables 16-23 & 16-25
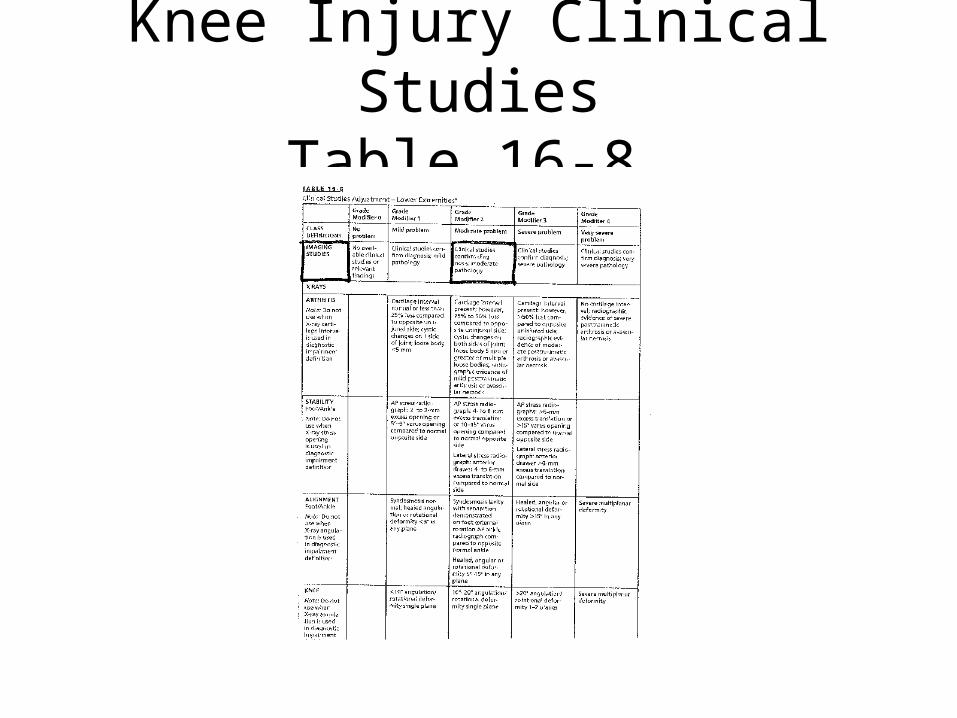
Knee Injury Clinical StudiesTable 16-8

Knee Injury AdjustedTable 16-3

Example Arm Injury 15-9 pg. 417
• 55 year old man sustains injury lifting tire; popping sensation and acute onset of pain; ruptured biceps tendon; surgery refused; at MMI, complaints of decreased strength and pain
• Functional History: pain w/activity; QuickDASH score 30• Physical Exam: tenderness noted in the antecubital fossa
(elbow); stregth in flexion and supination diminished to 4/5; 1 cm. atrophy compared to opposite; ROM elbow normal
• Clinical Studies: MRI elbow confirmed tear of the distal biceps tendon
Example Arm Injury 15-9 pg. 417
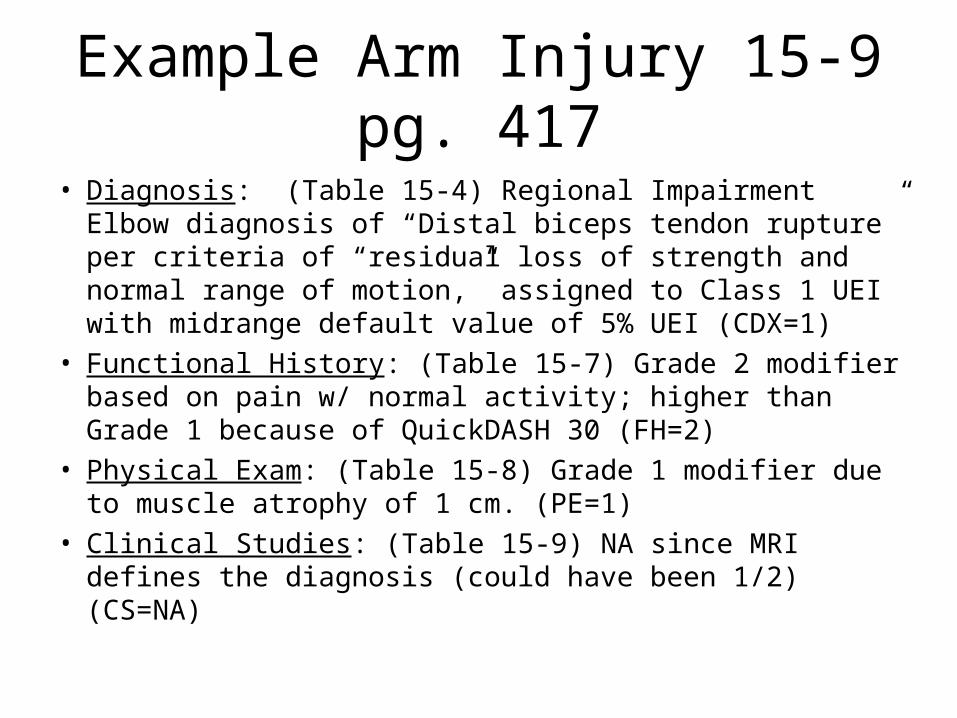
• Diagnosis: (Table 15-4) Regional Impairment Elbow diagnosis of “Distal biceps tendon rupture” per criteria of “residual loss of strength and normal range of motion,” assigned to Class 1 UEI with midrange default value of 5% UEI (CDX=1)
• Functional History: (Table 15-7) Grade 2 modifier based on pain w/ normal activity; higher than Grade 1 because of QuickDASH 30 (FH=2)
• Physical Exam: (Table 15-8) Grade 1 modifier due to muscle atrophy of 1 cm. (PE=1)
• Clinical Studies: (Table 15-9) NA since MRI defines the diagnosis (could have been 1/2) (CS=NA)

Example Arm Injury 15-9 pg. 417Impairment Rating Analysis
• CDX = 1 (diagnosis distal biceps tendon rupture w/loss of strength)
• FH = 2 (pain with normal activity)• PE = 1 (1 cm. atrophy)• CS = NA (MRI defines the diagnosis criteria)• Net Adjustment: (GMFH-CDX)+(GMPE-CDX)+(GMCS-CDX ) • Net Adjustment: FH(2-1)+PE(1-1)+CS(NA)= +1• Net Adjustment = +1, move one position to right from default• Default is 5% UEI; +1 move to the right is 6%UEI • FINAL ANSWER: 6% UEI

Arm Injury Regional GridTable 15-4
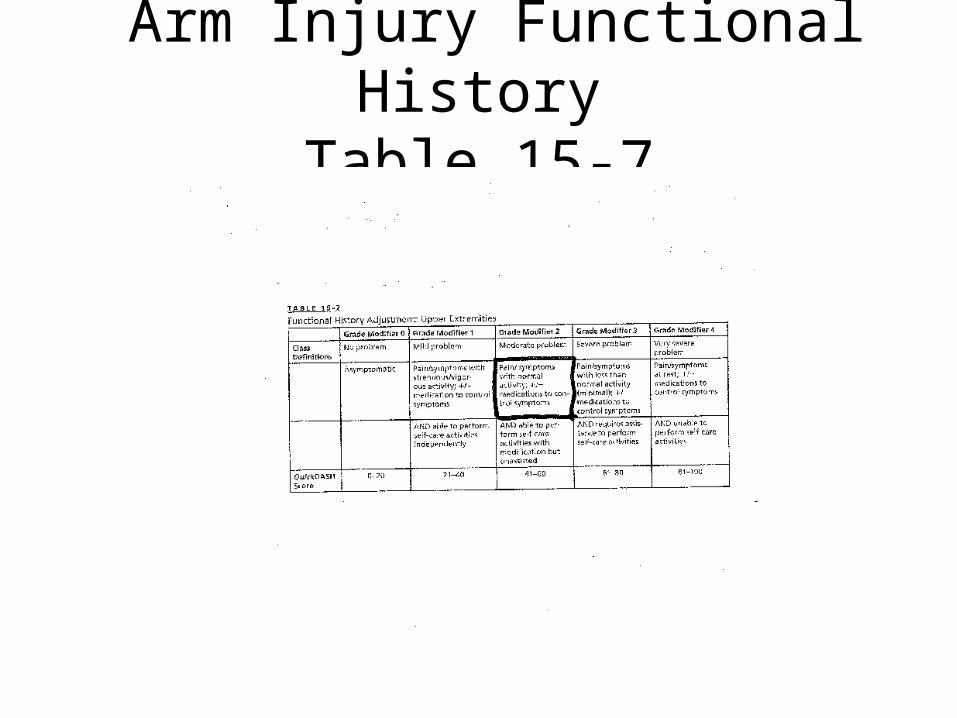
Arm Injury Functional HistoryTable 15-7

Arm Injury Physical ExamTable 15-8
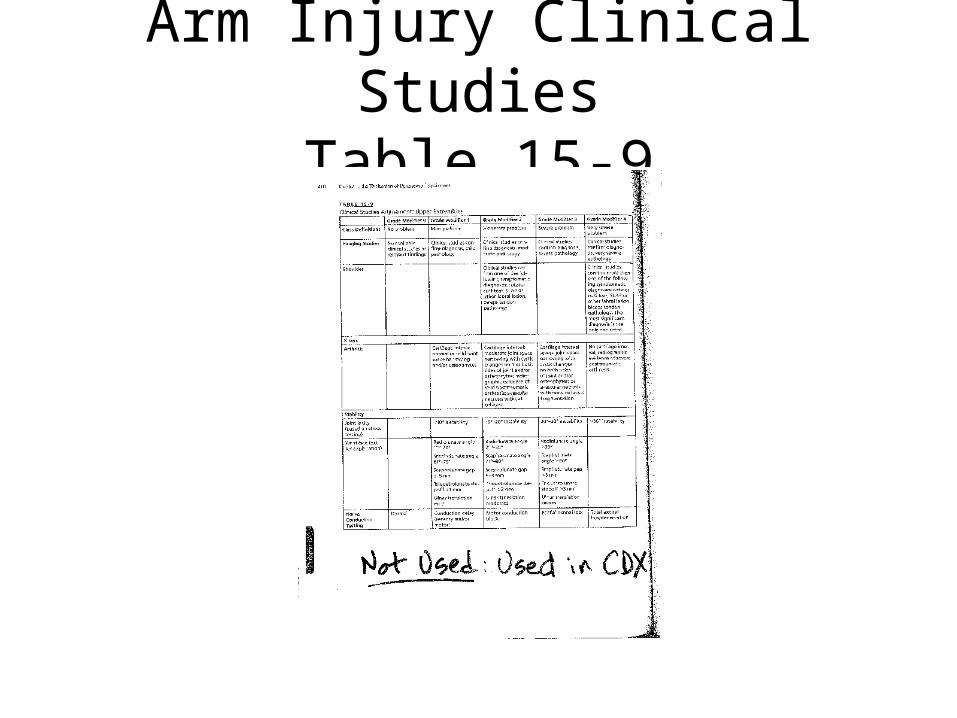
Arm Injury Clinical StudiesTable 15-9

Arm Injury AdjustedTable 15-4











![MCLE Lecture Series 69 · Limited to 80 PARTICIPANTS pursuant to MCLE Governing Board Resolution No. 005-2014 (first to register & pay basis) MCLE Lecture Series 69 Venue W^ ']o Dl](https://img.pdfslide.net/doc/110x75/5e9ecbf5b214b4300d208ca1/mcle-lecture-series-69-limited-to-80-participants-pursuant-to-mcle-governing-board.jpg)

![WCLA 3-27-14.pptx [Read-Only] CLE/WCLA_3... · 2016-12-02 · WCLA 3-27-14 • The Five Factors of Section 8.1b • Thursday March 27, 2014 • 12:00 pm to 1:00 pm • James R. Thompson](https://img.pdfslide.net/doc/110x75/5f397c7167df047dfe28db98/wcla-3-27-14pptx-read-only-clewcla3-2016-12-02-wcla-3-27-14-a-the.jpg)














