Embed Size (px)
Citation preview

Supplement table 1. Review of the literature of intracranial myeloid sarcoma with treatment and progression.
No. Author Report Time
Patient Age
(Years)Patient Gender
Course of disease and cytogenetic
characteristics
TreatmentsPrognosis
Surgery Chemotherapy Radiotherapy Others
1Katsuya
Yamamoto et.[1]
1999 38 M M2 Craniotomy
1. Five courses of cytarabine(40mgand prednisolone(20mg)were infused through an Ommaya reservoir;2. 6 cycle Cytarabine (600mg X 2 , Day 1-5) and etoposide (200mg, Day 1-5) as prevention
Whole brain with total dose
40Gy- CR for 21 months
2 Georg Widhalm et.[2] 2006 35 F t(8;21)(q22;q22) Craniotomy Cyclophosphamide
Whole-body radiotherapywith 13.2Gy
follow chemotheray
allo-HSCT
No Lesions after 2 years.
CR persists 7 years
3Georgina
Hodges et.[3]
2012 29 F t(15;17) Craniotomy
1. Induction: idarubicin-high dose cytarabine-big ICE;2. Consolidation: cytarabine-idarubicin-little ICE;3. Four doses of intrathecal cytarabine
28.8 Gy of radiation in 16 fractions to the
whole brain and 7.2 Gy
boost in four fractions to the
tumour bed followed
chemotherapy
- 22 months from diagnosis the patient remains in CR
4 Hyeon-Jin Park et.[4] 2003 3 F
Both kidneys,the brain,and multiple bone
-
AML induction chemotherapy (BHAC,300mg/m2/day,Day 0-6;6-thioguanine,100mg/m2,bid,Day 0-6;idarubicin,12mg/m2/day,Day 0-2;cytarabine,70mg,Day 0)
- - CR after 3 cycles of chemotherapy
5 David D. Grier et.[5] 2008 41 F
t(8;21;12)(q22;q22;q21) Craniotomy Four cycles of cytarabine - -
Mental status improved after 4 cycles of chemotherapy.
She was lost to follow-up after 7 months.

6 Ali Akhaddar et.[6] 2011 27 M - - Daunorubicin-aracytin-imatinib - - CR for the 6-month follow-up.
7Shintaro
Fukushima et.[7]
2006 39 F PML/RARα(+) Craniotomy 1. Idarubicin, 10 mg/m2/day d1;2. Cytarabine, 1000 mg/m2/day d1. - -
Died 4 days after surgery because of cerebellar hemorrhage and DIC
8Satoshi
Nishimura et.[8]
2004 30 F
M2, t(8;21) AML1/MTG8 (+)
46, XX, add(3)(q27) ,
relapse 8 months after Allo-PBCST
Craniotomy 2 courses of high-dose cytarabine were given followed by radiotherapy
Whole brain with 16Gy total spinal 24Gy.
- CR in a 2 year follow-up
9 Sharon W.W. Chan [9] 2003 70 M PMF,Hypereosinop
hilic Myelofibrosis Craniotomy - - -Ran a rapid downhill course and died within 1 month after admission
10 Pin Kei et.[10] 2011 49 M - - Further consolidated with systemic che- motherapy preemptively to prevent Radiotherapy -
Follow-up MRI scan performed 4 months later showed complete
resolution of the lesions
11 Karuna Dewan et.[11] 2019 65 F
t(8;21) ,RUNX1-RUNX1T1-balanced translocation;
Relapse with del(20)(q11.2) but t(8;21)
Craniotomy
1.Cytarabine and daunorubicin (7+3 regimen induction)
2. Cycle High-dose cytarabine (consolidative regimen)
3.Salvage chemotherapy with G-CLAM after relapse
Consolidative whole brain radiotherapy
-
After a slow and incomplete recovery, the family take the patient home and she subsequently passed away.
12 No authors listed [12] 2009 56 M PML/RARα(+) Craniotomy
Aggressive chemotherapy followed by consolidation with ATRA+ATO for relapse 3 months later.
Radiotherapy - Achive CR2 4 months later.
13Ali H. Palejwala et.[13]
2019 50 F PML/RARα(+) Craniotomy - - - -
14 Martha Romero et.[14] 2018 83 M CMML Craniotomy - - -
pssed peacefully on
hospital day 8

15 Bao Yang et.[15] 2017
27 M - CraniotomyIA(idarubicin at 45 mg/m2/day for 3 days and cytarabine at 100 mg/m2/day for 5 days) - - Death after 6 days
6 F - Craniotomy - - - sustained at 29 months of follow-up
16Maria Grazia Passarin, et.[16]
2008 29 M
10 yeaes after four courses of PEB
regimen Chemotherapy for Pineal Germinoma
and Testicular Cancer
- - - - Clinical conditions rapidly worsened, and then death
17
Angelo Borsarelli Carvalho Brito et.[17]
2015 21 M - - Methotrexate and cytarabine - - CR(The brain occupying masses disappeared )
18 Jing-Feng Wang et. [18] 2014 38 M - Craniotomy Chemotherapy - - CR in a 17‐month follow‐up
19 Meral Gunaldi et. 19] 2012 22 M - Craniotomy
Methotrexate 3.5 g/m2, cytosine arabinoside 2×2 g/m2, leucovorin 4×100 mg/m2
- - The brain occupying masses disappeared
20Mineko
Murakami et.[20]
2011 52 M t(8;21) Craniotomy Chemotherapy - -
died 12 days postoperatively of brain herniation caused by tumor enlargement and rebleeding in the right temporal lobe
21 Dhandapani E et. [21] 2015 23 F M2a - Chemotherapy and anti-tumor lysis
syndrome prophylaxis. - -responded well to chemotherapy after 7 days,but died of severe pancytopenia
22Philippe Prouet
et.[22] 2015 65 F t(8;21) - - - - PD
23 Jun Qian et.[23] 2015 27 M ETO(+) Craniotomy
2 cycles of 10 mg idarubicin and 1.5 g cytarabine for 3 days with intrathecal injections of 10 mg methotrexate and 5 mg dexamethasone.
Radiotherapy(40Gy) -
ETO (-), immunophenotyping (-). MRI : spinal tumor mass size
significantly decreased, receive a further 4 cycles of
chemotherapy.

24 Qinsheng Xu et.[24] 2009
29 M 10 years after BMT for CML Craniotomy Chemotherapy Radiotherapy - achieved CR during the 6-month
follow-up
34 F 3 years after CR of AML-M2a Craniotomy - Radiotherapy - PD and Death
CR:complete remission; PD:progressive disease;Allo-PBSCT: Allogeneic Peripheral Blood Stem Cell Transplantation;BMT:Bone Marrow Transplantation;CML:Chronic myeloid leukemia;CMML:Chronic Myelomonocytic Leukemia;PMF:Primary MyelofibrosisCraniotomy:Lesions were not completely removed;ATRA+ATO:all-transretinoic acid and arsenic trioxide;PEB regimen :bleomycin 30 mg intravenously on days 2, 8 and 15; etoposide100 mg/m2 and cisplatin 20 mg/m2 intravenously on days 1 through 5.
References:1. Yamamoto, K., et al., Isolated recurrence of granulocytic sarcoma of the brain: successful treatment with surgical resection, intrathecal injection,
irradiation and prophylactic systemic chemotherapy. Jpn J Clin Oncol, 1999. 29(4): p. 214-8.2. Widhalm, G., et al., Myeloid sarcoma with multiple lesions of the central nervous system in a patient without leukemia. Case report. J Neurosurg,
2006. 105(6): p. 916-9.3. Hodges, G., et al., Isolated intracranial myeloid sarcoma. Pathology, 2012. 44(6): p. 571-4.4. Park, H.J., et al., Myeloid sarcoma of both kidneys, the brain, and multiple bones in a nonleukemic child. Yonsei Med J, 2003. 44(4): p. 740-3.5. Grier, D.D., et al., Intracranial myeloid sarcoma. Br J Haematol, 2008. 142(5): p. 681.6. Akhaddar, A., et al., Acute myeloid leukemia with brain involvement (chloroma). Intern Med, 2011. 50(5): p. 535-6.7. Fukushima, S., et al., Granulocytic sarcoma: an unusual complication of acute promyelocytic leukemia causing cerebellar hemorrhage. Case
report. J Neurosurg, 2006. 105(6): p. 912-5.8. Nishimura, S., et al., Isolated recurrence of granulocytic sarcoma manifesting as extra- and intracranial masses--case report. Neurol Med Chir
(Tokyo), 2004. 44(6): p. 311-6.9. Chan, S.W., et al., Intracranial chloroma in hypereosinophilic myelofibrosis. Surg Neurol, 2003. 59(1): p. 55-7.10. Kei, P.L., et al., Butterfly lesion of the corpus callosum: an unusual case of extramedullary myeloid sarcoma (granulocytic sarcoma). Clin Nucl
Med, 2011. 36(5): p. 365-6.11. Dewan, K., J.H. Baird, and C.B. Shires, An Unusual Cause of Epistaxis: Paranasal Sinus Myeloid Sarcoma. Case Rep Hematol, 2019. 2019: p.
1312630.12. Granulocytic sarcoma. Blood, 2009. 114(1): p. 5. ([No authors listed)13. Palejwala, A.H., et al., Chronic myeloid leukemia manifested as myeloid sarcoma: Review of literature and case report. J Clin Neurosci, 2019. 64:
p. 269-276.14. Romero, M., et al., An 83 year-old man with fever and speech difficulties. Brain Pathol, 2018. 28(6): p. 1025-1026.15. Yang, B., et al., Clinicoradiological characteristics, management and prognosis of primary myeloid sarcoma of the central nervous system: A
report of four cases. Oncol Lett, 2017. 14(3): p. 3825-3831.16. Passarin, M.G., et al., Intracranial granulocytic sarcoma after chemotherapy for pineal germinoma and testicular cancer. J Clin Oncol, 2008.
26(27): p. 4507-9.

17. Brito, A.B., et al., Intracerebral Granulocytic Sarcoma in recurrence of Chronic Myeloid Leukemia. Arq Neuropsiquiatr, 2015. 73(1): p. 68.18. Wang, J.F., et al., Intracranial granulocytic sarcomaina in a non-leukemia patient. Neurol India, 2014. 62(6): p. 693-5.19. Gunaldi, M., et al., Primary intracerebral myeloid sarcoma. Onkologie, 2012. 35(11): p. 694-7.20. Murakami, M., et al., Isolated recurrence of intracranial and temporal bone myeloid sarcoma--case report. Neurol Med Chir (Tokyo), 2011. 51(12):
p. 850-4.21. Dhandapani, E., Thirumavalavan, and Sowrirajan, Acute Myeloid Leukemia Presenting as Intracerebral Granulocytic Sarcoma. J Assoc Physicians
India, 2015. 63(10): p. 70-1.22. Prouet, P., Rapid evolution of intracranial myeloid sarcoma in 4 weeks: images in blood. Blood, 2015. 126(10): p. 1256.23. Qian, J., et al., Isolated primary intracranial myeloid sarcoma with neuromeningeal infiltration: A case report. Oncol Lett, 2015. 9(4): p. 1647-
1650.24. Xu, Q., et al., Isolated recurrence of granulocytic sarcoma-two case reports. Neurol Med Chir (Tokyo), 2009. 49(12): p. 61

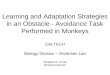
Supplement Figure 1Cranial CT of the patient 1 week after intracranial space occupation surgery.Left occipital bone flap shadow was seen, the contractile was good, and the left occipital lobe showed patchy shadow with slightly lower density and patchy density degree increase shadow, the boundary is not clear.

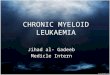
Supplement Figure 2Cranial CT of the patient 2 weeks after intracranial space occupation surgery.Left occipital bone flap shadow was seen, the contractile was good, and the left occipital lobe showed patchy shadow with slightly lower density shadow, the boundary is not clear.