Embed Size (px)
Citation preview

Cochlear Implantationin Early-deafened AdultsEVALUATION OF OUTCOMES
Lisa Mallinckrodts1490575
Supervisors:Rolien Free, M.D., Ph.D.
Rutger Hofman, M.D., Ph.D.
October 5, 2011

`
Abstract
Objectives: This retrospective study was conducted to evaluate benefits of cochlear implantation (CI) in early-deafened adults in the UMCG: to assess which patient characteristics are associated with successful cochlear implantation and to investigate the clinical importance and age span of pre- peri- and postlingual hearing loss in CI-users.
Material and method: 41 CI-users, with onset of hearing loss before the age of 12 years and implanted after the age of 16 years were evaluated. Outcome was measured in terms of audio-metric results (speech perception scores and PTA thresholds), quality of life (Nijmegen Cochlear Implant Questionnaire), functioning with the cochlear implant (Cochlear Implant Function In-dex), tinnitus complaints and daily usage in hours. Quality of life was compared with 22 non-im-planted early-deafened patients. To asses associations the following factors were examined: speech- and language related factors, education, age related factors, pre-implantation scores, anatomical anomalies, etiology and vestibular function, surgery related factors, and type of device and processor.
Results: Positive correlations were found between implantation outcomes and intelligibility, language development, lip-reading skills, aural/oral school attendance and educational level. Progression of hearing loss and age of onset of hearing loss were related to better results, with the best results in patients with onset of hearing loss before the age of 2 years. Patients with cochlear ossification scored significantly lower on post-implantation speech perception and quality of life. No relation was found between implantation outcomes and age at discovery of deafness, age at first hearing aid fitting, or age at implantation.
Conclusion: In deciding which prelingual or early-deafened adult can benefit from cochlear im-plantation, it is better to rely on speech and language related factors and school history as op-posed to historically obtained age related factors. In cochlear implantation, clinical relevance of the terms pre- peri- or postlingual deafness seems to be limited. It is therefore more appropriate to speak of early-deafened patients.

3
Table of contentsAbstract.............................................................................................................................................................. 2List of abbreviations...................................................................................................................................... 41. Introduction................................................................................................................................................. 5
1.1 History of the cochlear implant.........................................................................................................................51.2 Basic principles of the cochlear implant........................................................................................................51.3 Results of cochlear implantation.......................................................................................................................61.4 Objectives and hypotheses...................................................................................................................................7
2 Methods......................................................................................................................................................... 72.1 Patients........................................................................................................................................................................ 82.2 Data and outcomes.................................................................................................................................................8
2.2.1 General questionnaire..................................................................................................................................82.2.2 Functioning: Cochlear Implant Function Index.............................................................................82.2.3 Quality of life: Nijmegen Cochlear Implant Questionnaire......................................................82.2.4 Audiometry........................................................................................................................................................ 9
2.3 Statistical analysis....................................................................................................................................................93 Results............................................................................................................................................................. 9
3.1 Patient characteristics.........................................................................................................................................103.2 General results........................................................................................................................................................11
3.2.1 Audiometric performance.........................................................................................................................113.2.2 Quality of life and daily functioning......................................................................................................123.2.3 Daily usage of the cochlear implant......................................................................................................13
3.3 Correspondence of audiometric results, QoL, functioning and daily usage................................133.3.1 Audiometric results and questionnaire outcomes.........................................................................133.3.2 Quality of life and daily functioning......................................................................................................13
3.4 Factors influencing outcome............................................................................................................................143.4.1 Language and speech related factors...................................................................................................143.4.2 Educational factors......................................................................................................................................153.4.3 Time course related factors......................................................................................................................163.4.4 Anatomical anomalies, etiology and vestibular function............................................................163.4.5 Pre-implantation audiometric measurements................................................................................173.4.6 Surgery related factors...............................................................................................................................173.4.7 Device and processor..................................................................................................................................173.4.8 Confounding factors....................................................................................................................................17
3.5 Non-users..................................................................................................................................................................183.6 Tinnitus...................................................................................................................................................................... 19
4 Discussion.................................................................................................................................................... 194.1 Conclusion................................................................................................................................................................ 194.2 Prelingual deafness and brain plasticity.....................................................................................................204.3 Comparison with other studies.......................................................................................................................204.4 Limitations of this study.....................................................................................................................................224.5 Recommendations for future research........................................................................................................22
References...................................................................................................................................................... 24Appendices..................................................................................................................................................... 28
Appendix A: General questionnaire implanted patients..............................................................................28Appendix B: General questionnaire non-implanted patients....................................................................29Appendix C : Cochlear Implant Function Index...............................................................................................30Appendix D: Nijmegen Cochlear Implant Questionnaire.............................................................................31Appendix E : Patient characteristics.....................................................................................................................32Abstract in Dutch.......................................................................................................................................................... 33

4
List of abbreviations
ALD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Assisted Listening Device BPPV . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Benign Paroxysmal Positional Vertigo CI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Cochlear implantation / Cochlear implant CIFI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Cochlear Implant Functioning Index HA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Hearing aid HI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Hearing impaired HL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Hearing loss LVAS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Large vestibular aqueduct syndromeNCIQ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Nijmegen Cochlear Implant QuestionnairePTA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Pure tone audiogramQoL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Quality of lifeSIR . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Speech intelligibility rate SNHL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Sensorineural hearing loss UMCG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . University Medical Center Groningen

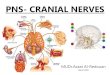
Figure 1.1: Graphical representation of a cochlear implant.
5
1. Introduction
1.1 History of the cochlear implantAs early as 1800, Alessandro Volta reported that electrical stimulation could cause sound per-ception in hearing subjects, as he had experienced noise after inserting electric current into his own ears.1 More than a century and a half later, on February 25, 1957, the first step in cochlear implantation was made, when André Djourno and Charles Eyriès, two French-Algerian surgeons from Paris, for the first time in history successfully excited the cochlear nerve of a deaf person with an electrode.2 Development of cochlear implants continued, and the first device with multi-ple electrodes was implanted in 1964 by Blair Simmons, professor of otology at Stanford Univer-sity Medical School, U.S.A.3 Some years later the first industrially made cochlear implants were developed, through the work of these men and other pioneers such as William House (House/3M), Robin Michelson (Clarion), Graham Clark (Nucleus) and Claude-Henri Chouard (Chorimac).4
1.2 Basic principles of the cochlear implantMost Sensorineural hearing loss (SNHL) is caused by malfunctioning of the auditory hair cells. Without inner hair cells, sound waves cannot be transformed into electrical signals to excite the auditory nerve. A cochlear implant (CI) mimics this function by delivering electrical signals directly to the auditory nerve.
The first industrially made cochlear implant, called Chorimac, weighed a massive 2.3 kg.5
Nowadays all cochlear implants are significantly lighter – a modern cochlear implant (Cochlear Nucleus 5) weighs 28 gram – and contain multiple electrodes, enabling the recipient to perceive different frequencies of sound and often acquire open-set speech understanding. The basic components are however much like the earlier models.

6
A graphical representation of a cochlear implant is shown in figure 1.1. The microphone can pick up sounds, which are converted to digital streams by the external sound processor (1). The processor, microphone and battery are housed in a "behind the ear unit" or in a body-worn unit on children. The sound processor consists of a digital signal processing unit (the computer of the cochlear implant system) which can be programmed and modified, a power amplifier and a radio frequency transmitter. After conversion, processing, and encoding into a radio frequency the signal is sent to the transmitter inside a headpiece (2). The headpiece is transcutaneously connected with a strong magnet to the subcutaneous internal receiver/stimulator (3), which is placed in a surgically created niche in the mastoid bone. The internal receiver has no battery and derives its energy from the sound processor by means of induction. The stimulator is a micro-processor that receives the radio frequency signal, decodes it and converts it into electric cur-rents which are sent along the intra-cochlear array (4). The electrodes (5) at the end of the array stimulate the spiral ganglion cells, which innervate the auditory nerve (6), taking advantage of the tonotopic encoding of frequency in the cochlea. In the central nervous system these signals produce a hearing sensation. This sensation is not the same as normal hearing, since only 6-8 distinct bands of frequency can be perceived, in contrast to about 60 bands in the normal audi-tory system. Finally, all modern systems contain a feedback system that monitors electric and neural activities and transmits the information back to the external unit from which it can be downloaded by the audiologist using a PC program.6,7
1.3 Results of cochlear implantationMany CI-recipients develop open speech understanding and sometimes even the ability to use the telephone,8 while some others experience no benefit at all and stop using their cochlear implants.9,10 To evaluate outcomes of cochlear implantation, CI-recipients are usally divided into three groups: postlingually deafened adults, prelingually deafened children, and – a relatively young group in terms of indication – prelingually deafened adolescents and adults.
Usually, prelingual deafness is defined as hearing loss (HL) acquired before language devel-opment. Although the term “prelingual” is in use since at least 1966,11 the age limit has never been well defined: the upper age boundary for prelingual hearing loss ranges from the age of 30 months12 to the age of 6.13 Some authors have used “perilingual” deafness to identify hearing loss with onset during the years in which development of speech is taking place. Definition of this term is also inconclusive: some authors define “perilingual” hearing loss as hearing loss with onset between the age of 2 and 3,14 while others use the same term to define onset of hearing loss between 2 and 4 years.15
The primary goal of cochlear implantation in postlingually deaf adults is to re-enable a patient with severe to profound hearing loss to communicate effectively through spoken lan-guage. In children, the main goal is to ensure auditory input, in order to create the best environ-ment for development of speech and language. For children with cognitive disabilities, enhance-ment of safety, e.g. in traffic, can also be a good reason to opt for cochlear implantation (i.e. signal function). In prelingually deafened adults the goal of implantation depends on the patient’s characteristics, possibilities and expectations. In this group three levels of goals are used: to hear and distinguish basic sounds, to improve lip-reading abilities or understanding spoken language in quiet situations.
The results of cochlear implantation in postlingually deafened adults are excellent; the majority of these patients can recognize over 80% of the words in a high context sentences. 16
Likewise, many prelingually deaf children demonstrate strong improvements in word recogni-tion with and without lip-reading.17-23 Multiple studies have shown speech and language outcome to be negatively correlated with age at implantation.24-32 Moreover, since children implanted between the ages of 12 to 36 months have a speech-language development delay of approxi-mately one year compared to children who are implanted in the first year of life, early implanta -tion is becoming the trend.33 Usually, cochlear implantation is performed around the age of 8–10 months, but implantation in children at the age of 6 months has been reported.34, 35 However,

Indications:• bilateral SNHL• aided free field speech perception <50%• in children: PTA loss >60dBTable 2.1: Indications for cochlear implantation in the University Medical Center Groningen
7
anesthetic risks are slightly bigger in younger patients and repeated audiological testing is nec-essary to obtain more definite knowledge on the depth of hearing loss.36 Additionally, a three month trial period with hearing aids is needed to find out the depth of hearing loss, and thus the indication for cochlear implantation. Only in some cases of meningitis, with the pending risk of partial or total cochlear ossification, very early implantation is strictly necessary to prevent losing the opportunity of implantation.37-39
Results in prelingually deafened adults are in general less successful compared to postlin-gually deafened adults and prelingually deafened children. In the first decennia of cochlear implantation prelingually deafened adults were considered poor candidates because of limited advantage in speech perception.40-46 Recent studies have reported moderate improvements in open-set speech perception after implantation and rejected age as a contraindication for cochlear implantation as a result.32,47-56 A major part of the improvement of results over time can be credited to better speech processing strategies.32 Detailed explanation of these sound process-ing strategies goes beyond the scope of this paper. Just like in other CI-recipient groups, multiple studies have noted a wide variability in outcomes.44,47,51
In prelingually deafened children and adults, several studies have proven oral communica-tion to be positively correlated with good outcome, as opposed to total communication (oral and sign language) or sign language.20,57-59 Other factors improving speech and language outcome are better pre- implant residual hearing, measured by pure-tone thresholds or conventional speech perception scores.31,58 Better residual hearing positively affects speech and language develop-ment and intelligibility, factors that correlate positively with outcome as well.60-62
Not many studies have been conducted yet on cochlear implantation in prelingually deaf-ened adults. In agreement with studies regarding children, oral communication and intelligibility are proven to be positively related to the success of cochlear implantation in prelingually deaf-ened adults as well.52,63,64 Teoh et al. (2004)16 reviewed all published literature on cochlear im-plantation in prelingual deafness and concluded patient characteristics to be the main responsi-ble factor influencing outcome, as opposed to device properties. According to another study by Teoh et al. (2004)65 limited post-implant performance of adults with prelingual deafness cannot be accounted to pathological degenerative changes of the auditory nerve, cochlear nucleus, or auditory midbrain, but to colonization of the auditory cortex by other sensory modalities. In some studies, post-implant speech and language skills have been noted to correlate with IQ,66
contrary to other studies which showed no association between outcomes and cognitive skills.67
1.4 Objectives and hypothesesThe wide variability between cochlear implant users makes predicting patient outcome difficult. Gaining knowledge about factors predicting prognosis would help clinicians in deciding whether CI surgery could be beneficial for a specific patient. The objectives of this study were (I) to evalu -ate the results of cochlear implantation in early-deafened adults in the UMCG, (II) to investigate which patient characteristics are associated with successful implantation in this specific group and (III) to assess the age span of prelingual and perilingual deafness and the clinical relevance of these terms.
2 MethodsThe first cochlear implantation in the University Medical Center Groningen was performed in December 2000. From that date to June 2011, 362 patients received a cochlear implant in the UMCG. Indications for implantation in the UMCG are listed in table 2.1.

8
A multidisciplinary team assesses whether the patient is suitable for cochlear implanta-tion. A preoperative CT scan is made as an operative map, and to exclude possible cochlear ossification or malformations. After clinical examination by the ENT surgeon, pure tone audiom-etry (PTA) and speech audiometry, both without hearing aids and after optimal fitting of hearing aids, and vestibular tests are performed in the University Audiological Center Groningen (UACG). A psychologist and a social worker are consulted to assess the patient’s expectations, coping skills and social support system, and a speech therapist evaluates speech and language skills. Children are seen by a remedial educationalist to assess development. After extensive testing the results are discussed in the CI team, which provides an advice regarding implantation.
2.1 PatientsAll patients who received their first hearing aid before the age of 12 years and who were im-planted at the age of 16 years or over, and at least before June 2010 were asked to participate in the survey. The age limit of 12 years was chosen to see if not only a prelingual and a postlingual, but also a “perilingual” timescale could be defined. Patients with cognitive disabilities and pa-tients whose first language was not Dutch were excluded. Pre- implant patient characteristics were obtained from reports made prior to cochlear implantation by the multidisciplinary team.
To assess quality of life and day-to-day functioning with the CI, we sent the Nijmegen Cochlear Implantation Questionnaire (NCIQ) and the Cochlear Implant Function Index (CIFI) to the CI-recipients. A general questionnaire was added to obtain additional data and to assess tinnitus complaints. To compare quality of life between implanted and non-implanted patients, shorter versions of the general questionnaire and the NCIQ were sent to non-implanted patients. These patients were deafened before the age of 12, had speech perception scores of less than 50% and did not receive a cochlear implant due to a negative advice by the CI team or by their own choice. After 4 weeks, we sent out reminding letters and questionnaires to non-respon-dents.
2.2 Data and outcomes2.2.1 General questionnaireA general questionnaire with questions on course and etiology of hearing loss, stimulation of language-speech development in early childhood, highest level of education, primary mode of communication and tinnitus was developed for this study. Examples of the general question-naires for CI-users and non-implanted patients (in Dutch) can be found as Appendix A and Ap-pendix B.
2.2.2 Functioning: Cochlear Implant Function IndexThe Cochlear Implant Function Index is a short, easy to use instrument to assess hearing func-tion in different circumstances, developed by Coelho et al.68 Each of the six major questions includes 3 or 4 Guttman scaled sub-questions that are scored using a five-point Likert scale. Based on the total score, participants are categorized into “lowest”, “low”, “high” or “highest” level of functioning. The CIFI was translated into Dutch by the Language Center of the University of Groningen and revised by several professionals working with CI-users. Some phrases were changed to fit the Dutch population. For example, mosque was added to the list of options in the last question: “With my cochlear implant, I can understand at the theater, lecture, church or synagogue. . . ”. Sign language interpreters are uncommon in the Netherlands and therefore this was left out of the questionnaire, to avoid confusion. The original CIFI can be found in the article of Coelho et al.,68 the Dutch translation of the CIFI is added as Appendix C.
2.2.3 Quality of life: Nijmegen Cochlear Implant QuestionnaireThe Nijmegen Cochlear Implant Questionnaire was developed by Hinderink et al.,69 because “generic” Health Related Quality of Life (QoL)-instruments were not sensitive and comprehen-sive enough to evaluate subjective outcomes and QoL changes induced by cochlear implanta-tion.69,70 The NCIQ is a reliable self-assessment to measure functioning on three domains and six

9
sub-domains: i. physical functioning is measured with Basic sound perception, Advanced sound perception and Speech production, ii. psychological functioning is measured with Self-esteem, and iii. social functioning is measured with Activity and Social functioning. Extra questions are added to the NCIQ, to measure limitations of CI use and to compare current functioning with pre- implantation functioning. The NCIQ can be found as Appendix D.
2.2.4 AudiometryAfter cochlear implantation and extensive rehabilitation, follow up is provided every 6 months or earlier when necessary. The audiologist measures PTA thresholds and speech perception scores to optimize implantation fitting. We collected the audiometric data and reviewed postop-erative PTA thresholds and speech perception scores after 6 months, 1 year and 2 years and the most recent score. For PTA measurement we used the mean of the pure tone thresholds at 0.5 kHz, 1 kHz, 2 kHz and 4 kHz, measured with ’warbles’. Speech perception scores were obtained using the Dutch Society of Audiology standard CVC (monosyllabic) word lists. Additional to word lists, speech perception scores were obtained with number lists. Rather than volume levels, maximum obtained scores were used in the analysis. Post-implantation PTA thresholds and speech perception scores were compared with pre-implantation scores for objective evaluation of audiometric functioning in CI-recipients.
2.3 Statistical analysisData were analyzed using SPSS Statistics 18.0 (SPSS Inc, Chicago, IL). Because of small sample sizes and many non-normal distributions (Wilk-Shapiro p <.05), we used non-parametric tests only. Wilcoxon Score Rank test was used to test differences in paired samples. To compare more than two samples we used the Independent-Samples Kruskal-Wallis test. To assess correlation we performed Spearman’s rank correlation coefficient (Spearman’s rho). A rho value of >0.7 was considered as strong correlation and 0.3-0.7 as moderate correlation. Fisher’s exact test was used to investigate differences in categorical data in non-paired groups. The p value to reject the null hypotheses was .05. Because of small sample size, daily CI usage (in hours) was categorized to enable valid interpretation. 2-tailed tests were used unless mentioned explicitly.
3 Results

10
In the implanted group (n=71) 58 patients (82%) returned the questionnaires. 17 patients were
excluded because they received their first hearing aid after the age of 16, which suggests hearing loss was not profound in childhood. In the non-implanted group (n=62) 23 patients (37%) re-turned the questionnaires. One patient was excluded because she received her first hearing aid at the age of 16, and thus cannot be considered early-deafened. 3 patients were previously re-jected, but accepted for cochlear implantation during this study. Characteristics of non-im-planted and implanted patients are added as appendix E.
3.1 Patient characteristicsPatient characteristics are summarized in table 3.1. A graphical representation of etiology in implanted and non-implanted patients is given in figure 3.1. Distribution in etiology between implanted and non-implanted patients did not differ significantly (Kruskal-Wallis Test).
Not implanted n=22
Implanted n=41
pa
Gender % male 40.9 46.3 .792 female 59.1 53.7 Age (years) mean (sd) Current age 45.4 (17.36) 48.1 (14.68) .118 hearing loss discovered 2.5 (1.74) 3.5 (2.55) .341 first hearing aid (HA) fitting 4.3 (3.03) 5.2 (2.89) .192 likely onset of HLb 0.3 (0.66) 1.2 (1.95) .048* Interval (years) mean (sd) duration onset HL to discoveryb 2.3 (1.95) 2.3 (2.74) .642 duration HL noted to first HA 1.8 (2.24) 1.6 (1.62) .977 duration onset HL to first HAb 4.1 (3.15) 4.0 (2.89) .999 Educational level % elementary school 9.1 14.6 .251 secondary school 59.1 36.6 vocational education 27.3 26.8
*Not implanted: Pendred’s syndrome (n=2), Mastiocytosis X (n=1). Implanted: parotitis (n=2), measles (n=1), LEOPARD syndrome (n=1), neonatal encephalopathy (n=1), hemolytic disease of the newborn (n=1), scarlet fever (n=1)
3.1: Graphical representation of etiology in implanted and non-implanted patients

11
university of applied sciences 4.5 12.2 research university .0 9.8 school for the deafc 75.0 36.6 .033* school for hearing impaired 18.8 43.9 aural/oral school 6.3 19.5 Communication % in childhood <001** sign language .0 4.9

12
oral + sign language 72.7 24.2 oral language 27.3 70.7 before implantation .024* sign language 9.1 2.4 oral + sign language 54.5 26.8 oral language 36.4 70.7 after implantation N/A 001**d sign language .0 oral + sign language 19.5 oral language 80.5
* P <.05 ** P <.01a Using Fisher’s exact test (2-tailed) for nominal data and Independent Samples Mann Whitney U test (2-tailed) for ordinal and continuous data.b Not included are patients with hearing loss of unknown etiology (implanted n=14, non-implanted n=3).c Missing values of non-implanted n=6.d Comparison with distribution not implanted, before implantation.

13
** p<.01, pre-implantation vs. post-implantation scores
Figure 3.2: Graphical summary of PTA thresholds and speech perception scores of implanted patients.
Table 3.1: Overview of patient characteristics.
3.2 General results3.2.1 Audiometric performanceThe mean most recent scores were 51.5% (±30.74) for speech perception with word lists, 76.8% (±29.76) for speech perception with number lists and 38.2dB (±16.90) for PTA thresholds. After exclusion of non-users, scores of 56.6% (±27.78), 84.0% (±22.65) and 35.4dB (±8.10) are found. A graphical summary of pre- and post-implantation PTA thresholds and speech perception scores measured at different times is presented in figure 3.2.

14
PTA thresholds were significantly lower and speech perception scores were significantly higher after implantation. In patients who were implanted before 2008, speech perception scores measured with word lists >24 months after implantation were significantly higher than those measured 12 months and 24 months after implantation. This might be due to the general trend in audiometric outcomes; as a result of improved technologies, speech perception scores are increasing and PTA thresholds are decreasing through the years. This trend can be seen in figure 3.3
3.2.2 Quality of life and daily functioningImplanted patients had significant higher QoL scores, with higher scores on NCIQ sub-domains Sound perception basic, Sound perception advanced, Speech production, Activity and Social interactions compared to non-implanted patients. No significant difference was seen in sub-do-main Self-esteem. Two CI-recipients (non-users) did not complete the NCIQ. A graphical over-view of the scores and additional details can be seen in figure 3.4.
On the CIFI, of the CI-recipients 11 respondents (26.8%) were scored “lowest” functioning, 14 respondents (34.1%) were “low” functioning, 11 respondents (26.8%) were “high” functioning and 5 respondents (12.2%) were scored “highest” functioning. Mean scores per sub-scale (level of hearing function) are shown in figure 3.5. Partici-pants reported the highest level of functioning in the area of work and reliance on assisted listen-ing devices. 46.3% (19 CI-users) were able to use the telephone for short (19.5%) or short and long (26.8%) conversations. 16 subjects (39%) were unemployed, and thus unable to score points on the questions concerning communication at work.ALD’s: Assisted Listening Devices
Figure 3.5: Mean CIFI scores in different settings
* p<.05, ** p<.01, non-implanted vs. implanted patients, Mann-Whitney U test, 1-tailed.Clustered box plot showing medians and quartiles
Figure 3.4: Scores on NCIQ sub-domains
** Linear trend p<.01. Speech perception scores measured with number lists showed no significant trend over the years, and therefore not shown.
Figure 3.3: Trend of mean PTA threshold and speech perception scores

15

16
Quality of Life: NCIQ sub-domainSound
perception basic
Sound perception advanced
Speech produc-
tionSelf-
esteemActiv-
ity
Social interac-
tionsTotal score Comparison
Fu
nct
ion
ing:
CIF
I le
vel
Noise + + + + + + +Reliance on ALD's + +
Phone + + + +Group Work + ++ + + + + +Public events + + +Overall CIFI level + + ++ + + +
Spearman’s rank correlation coefficient, 2-tailed. + indicates moderate correlation (rho=0.3–0.5), ++ indicates strong correlation (rho >0.7). ALD’s: Assisted listening devices
Table 3.2: Correlations between Quality of Life and Functioning.
3.2.3 Daily usage of the cochlear implantOn average, CI recipients wear their CI all waking day ( =12.4h, median=15h). 30 subjectsσ (73.2%) reported using their device at least 12 hours per day, 4 patients (9.8%) use the CI for 8–11 hours daily and 3 patients (7.3%)reported to wear the CI 4–7 hours daily. 4 patients (9.8%) were non-users. In non-users, reasons for not using their device were pain (n=3), “irritation in the brain” (n=2), dizziness and nausea (n=2) and unpleasant sounds (n=1).
In patients who did use the CI, reasons to turn their device off were sleeping and taking a shower (90.2%), fatigue (17.1%), being in noisy environments (12.2%) and headaches (4.9%). One patient mentioned device weight as a reason to turn of the CI, and one patient noted he sometimes felt too ashamed to wear the CI in public.
3.3 Correspondence of audiometric results, QoL, functioning and daily usage3.3.1 Audiometric results and questionnaire outcomesQuality of life: A negative, moderate correlation was seen between pure tone measurements and NCIQ sub-domains Sound perception basic, Sound perception advanced and Social interac-tions. Moderate positive correlations were found between speech perception scores and multi-ple NCIQ sub-domains. Correlations were strongest with sub-domains Sound perception ad-vanced, Speech production and Self-esteem (rho >0.5), followed by sub-domain Social interac-tions. Patients with higher speech perception scores also reported higher on the additional NCIQ questions concerning pre- and post-implant comparison.
CI functioning: Overall functioning and Functioning in noise (CIFI) were better in patients with lower PTA thresholds. Higher speech perception scores were strongly correlated with better overall functioning and higher scores on all CIFI functioning levels, especially for the ability to use the telephone.
Daily usage: No correlations were found between daily CI usage in hours and PTA thresholds. However, a moderate positive correlation with speech perception scores was noted.
3.3.2 Quality of life and daily functioningAn overview of correlations between NCIQ sub-domains and CIFI functioning levels is presented in table 3.3 Additional NCIQ questions regarding limitations did not correlate with any of the CIFI functioning levels, nor with any of the NCIQ sub-domains. Functioning in groups was not correlated with quality of life, whereas functioning at work was positively correlated with all NCIQ sub-domains, especially with sound perception advanced.
Audiometric scores Quality of life Functioning Daily usage

17
Language and speech:– intelligibility– SIR score– language development– communication (childhood)
Education:– school for the deaf attendance– education level
Time:– progression– age of onset
Anatomical anomalies:– cochlear ossification
Language and speech:– intelligibility– lip-reading skills– language development
Education:– school for the deaf attendance– educational level
Time:– progression
Etiology:– LVAS
Language and speech:– intelligibility– aided lip-reading score– lip-reading skills– language development– communication (before CI)
Education:– school for the deaf attendance– educational level
Time:– progression– age of onset
Etiology:– LVAS
Pre- implantation functioning:– speech perception before CI
Device and type:– speech processor
Education:– education level
Time:– progression– age of onset
Anatomical anomalies:– any anatomical anomaly
Table 3.3: Summary of factors influencing outcome
Daily usage: No correlations were found between Quality of Life scores and daily CI usage in hours, or between functioning and daily CI usage in hours. Patients use the CI regardless of their functioning or possibilities.
3.4 Factors influencing outcomeA summary of factors influencing implantation outcome is given in table 3.3. We will now discuss these factors in the following sections.
3.4.1 Language and speech related factorsThe most important factors influencing CI outcome are related to language and speech. We used several speech and language factors in the analysis.
First, we used pre- implantation scores measured by speech therapist: intelligibility and SIR score (speech intelligibility rate, measured from 1: unintelligible, to 5:intelligible to all listeners), lip-reading skills, speech tracking (the patient repeats words spoken by the speech therapist, scored in correct words per minute), aided and unaided lip-reading scores (% words correct), and lan-guage development level. Second were communication method in childhood and before implantation.
Audiometric outcomes: Moderate positive associations were found between post-implantation speech perception scores and intelligibility, SIR score and language development level. Despite very small samples, patients who were scored a SIR 5 showed significantly better audiometric outcomes (higher speech perception scores and lower PTA thresholds) than patients score SIR 4. This is especially striking in post-implantation speech perception scores measured with word lists (78.0% vs. 12.2%). Patients with low developed language had significantly lower speech perception scores after implantation.
Patients who communicated primarily through speech in childhood, had significant higher speech perception scores than patients who used both speech and sign language in childhood (word list scores 58.6% vs. 32.8%).
Intelligibility low (n=5)moderate (n=9)high (n=27)
SIR score 2 (n=1)3 (n=2)4 (n=5)5 (n=5)
Lip-reading skills moderate (n=5)high (n=31)
Speech tracking = 45 ±σ 17.9(n=13) Aided lip-reading score = 84 ± 11.7σ (n=16) Unaided lip-reading score = 67 ± 19.8σ (n=16) Language development low (n=9)
moderate (n=5)high(n=27)

18
Quality of life: No correlations were found between speech and language related factors and NCIQ sub-domains Sound perception basic, Self-esteem, Activity or Social interactions. Also, speech and language related factors were not associated with comparison scores. High intelligi -bility scores were associated with higher scores on sub-domains Sound perception advanced and Speech production, but also with lower scores concerning CI limitations. Lip-reading skills showed moderate positive correlation with sub-domains Sound perception advanced, Speech production and total NCIQ scores. Language development was positively correlated with higher scores on sub-domains Speech production, but also with higher limitation scores. Communica-tion method in childhood and before implantation showed no association with Quality of life.
Functioning: Factors positively associated with overall CI functioning were intelligibility, aided lip-reading scores, lip-reading skill and language level. Furthermore, intelligibility was positively associated with functioning levels Phone, Work and Public events, lip-reading skills were moder-ately positively associated with functioning levels Noise, Phone and Work and language level showed a moderate positive association with Public events. In addition, Patients who communi-cated primarily through speech before implantation and patients with higher SIR scores are more able to use the telephone.
Daily usage: None of the language and speech related factors were associated with CI usage in hours per day.
3.4.2 Educational factorsTo analyze associations between education factors and implantation outcomes, we used educa-tion level (primary school, secondary school, vocational education, university of applied sciences or research university) and school for the deaf attendance and duration.
Audiometric outcomes: Patients who attended school for the deaf had significantly lower speech perception scores than patients who attended school for the hearing impaired (HI) and those who received aural/oral education (60.4% vs. 35.1%), and longer school for the deaf attendance was strongly associated with lower speech perception scores. No significant differ-ences were found between subjects who received aural/oral education and subjects who at-tended school for the hearing impaired. Patients who attended school for the deaf but also at-tended school for the hearing impaired had higher speech perception scores than those who went to school for the deaf only. Duration of HI school attendance was strongly positively corre-lated to speech perception (number lists and word lists).
Educational level was moderately positively associated with number list scored speech perception scores, but no association with word list speech perception scores or PTA thresholds was found.
Quality of life and functioning: Patients who attended aural/oral school or school for the hearing impaired scored higher on Speech production than those who went to school for the deaf. Subjects who attended school for the hearing impaired also showed significantly higher scores on Sound perception advanced and on extra questions regarding pre- and post-implant comparison. These differences were not found between former school for the deaf students and aural/oral school students, possibly due to a smaller sample size of the latter (n=8). Patients who attended aural/oral school reported more limitations as a result of the CI than patients who attended school for the deaf or school for the HI. In patients who attended school for the hearing impaired, duration of HI school attendance was positively correlated with limitations of the CI.
Regarding functioning, former school for the deaf students had significantly lower overall scores than those who went to aural/oral school or school for the hearing impaired. No differ-ences were found in QoL and functioning between CI users who went to aural/oral school and those who went to a school for the hearing impaired.
Education level was moderately positively associated with Speech production and Self- esteem. There were also moderate positive associations found between educational level and overall functioning with CI, and for functioning levels Group, Work and Public events.

19
Anatomical anomalies LVAS (n=2)ossification (n=3)incomplete cochlear partition (n=1)
Vestibular function hyper-excitable (n=1)ipsi-lateral normal (n=15)
hypo-excitable (n=1)not excitable (n=5)
Vestibular function normal (n=15) contra-lateral hypo-excitable (n=2)
not excitable (n=5)
Daily usage: No difference was found in daily CI usage (hours per day) between former school for the deaf students, subjects who went to a school for the hearing impaired and subjects who received aural/oral education.
Education level was moderately positively associated with daily CI usage. Patients who received primary education only wear the CI shorter than patients with a higher education level.
3.4.3 Time course related factorsTime course related factors used in the analysis were as following: Progression of hearing loss (slowly progressive or sudden/rapidly progressive), age at onset of hearing loss, age when hearing loss was first noticed, age at first hearing aid fitting, age at implantation and current age. The intervals between these ages were used in the analysis as well.
Audiometric outcomes: patients whose hearing loss progressed slowly showed significantly higher audiometric outcomes scores than those with rapidly progressive hearing loss (speech perception scores with word lists 58.9% vs. 22.0%). The only age factor associated with post-im-plantation audiometric scores was age of onset of hearing loss. Patients with onset of hearing loss between the age of 2 and 4 scored (n=3) significantly lower than patients before the age of 2 (n=20) or after the age of 4 (n=4) (word list score 0.0% vs. 52.3% and % 36.3 respectively), regardless of HL progression.
Quality of life and functioning: Patients with slowly progressive hearing loss scored higher on Speech production. When we look at age related factors, patients with onset of HL before the age of 2 years had significantly higher total NCIQ scores and higher scores on NCIQ sub-domains Activity. On the other hand, patients with onset of HL after the age of 4 had significantly lower scores on NCIQ sub-domain Sound perception advanced. Although patients with onset of HL between the age of 2 and 4 years had significantly lower speech perception scores, scores on NCIQ sub-domains Sound perception basic, Sound perception advanced and Speech production were higher than average, but not not significanly. On extra questions regarding comparison a moderate positive association was found with age at discovery of hearing loss and the interval between age of onset and age at first hearing aid fitting.
In subjects with slowly progressive HL, overall functioning was also higher, with significant higher scores in functioning levels Phone, Group and Public events. Regarding age related fac-tors, only patients with onset of hearing loss before the age of 2 years were able to use the tele-phone. Furthermore, this group scored significantly higher on functioning level Work.
Daily usage: Patients with slowly progressive HL wear the CI more prolonged compared to patients with rapidly progressive HL. Regarding age factors, subjects with age of onset below 2 years wear their CI during longer periods than subjects in which HL has started after the age of 2.
3.4.4 Anatomical anomalies, etiology and vestibular functionWe used the following factors in the analysis: etiology, inner ear anatomical anomalies and vestibular function (ipsi- and contra-lateral).Patients with cochlear ossification scored lower on speech perception tests measured with word lists. Etiology and vestibular func-tion were not associated with audiometric outcomes.

20
Patients who are implanted in the better ear experience fewer limitations than patients who received the CI in the worse ear. Patients with LVAS scored significantly higher on overall functioning and on NCIQ sub-domain Speech perception advanced, and patients with rubella scored significantly lower on functioning level reliance on ALD’s. Furthermore, patients with anatomical anomalies wear the CI less hours daily. Vestibular function and etiology were not related to QoL, functioning or CI usage.
3.4.5 Pre-implantation audiometric measurementsFor the analysis of pre-implantation audiometric measurements we used pre-implantation PTA thresholds of the implanted and the contra-lateral ear and pre-implantation speech perception scores (word lists and number lists).
No associations were found between pre- and post implant audiometric measurements, nor between pre-implant audiometric measurements and quality of life or daily usage. However, pre- implantation speech perception scores (word lists) were positively associated with better overall functioning and with functioning level Group.
3.4.6 Surgery related factors Surgery related factors used in the analysis were surgery related complications (n=6), implanta-tion year, surgeon who performed the CI, and side of the implanted ear (worse side [n=27]), better side [n=11] or symmetrical HL [n=3]).Surgery related factors were not related to audiological outcome, quality of life, functioning or daily usage.
3.4.7 Device and processorPatients were implanted with cochlear implants manufac-tured by Advanced Bionics or Cochlear Corporation and used speech processors by the same manufacturer. No differences were found between type of CI device for post-implantation audiometric measurements, quality of life and functioning. Patients with the newest CP810 processor scored significantly lower on functioning level.In CI-users with a processor different than the CP810, 30% answered “Always” or “Frequently” to the question “Can you use the voice telephone [...] with anybody, for any length of conversation”, compared to 0% of the CP810-processor users
3.4.8 Confounding factorsSince sample size was too small to perform parametric tests and data were mostly non-normally distributed, we could not perform regression analysis to distinguish independent influencing factors from dependent influencing factors. To get some information about factor dependency we did look for correlations and associations between factors. Between the 40 used patient characteristics over 200 possible combinations were significantly correlated. To mention them all would make this paper too extended, so we will only discuss correlations between factors influencing outcome and remarkable correlations.
Associations between factors influencing outcome: In speech- and language related factors, a moderately positive correlation was found between lip-reading and intelligibility. Lip-reading skills were not significantly related to other speech- and language related factors. All other outcome-related speech- and language factors correlated positively with each other.
Education level and school for the deaf attendance were not related. Outcome-related Speechand language factors significantly lower in patients who attended school for the deaf attendants were intelligibility and language level. Furthermore, former school of the deaf atten-dants used more sign language in childhood and before implantation. Educational level was
Device type AB HiRes (n=11) CI24RE-CA (n=10) CI24R-CA (n=9) CI24R-CS (n=8) CI24R-ST (n=2) CI512 (n=1)
Processor Auria Harmony (n=11) Freedom (n=14)ESPrit 3G (n=8) CP810 (n=8)

21
moderately positively correlated with language level, but not with other speech- and language factors.
Age of onset of HL was not related to progression. Age of onset was moderately negatively correlated with intelligibility and lip-reading skills. Language development level was signifi-cantly lower in patients with rapidly progressive hearing loss. School for the deaf attendance was strongly associated with rapidly progressive hearing loss, but not with age of onset.
No significant correlations were found between anatomical anomalies or etiology and other outcome-related factors. Pre- implantation speech perception score (word lists) was sig-nificantly moderately positively related with aided lip-reading scores, both were related to functioning. CI-users who used the Cochlear CP810 processor had significantly lower SIR scores before implantation. Both were related to functioning with CI.
Remarkable correlations: Complications were more prevalent in patients with anatomical anomalies (66.7% vs. 5.7%). In both patients with LVAS CI was complicated by postsurgical infection. Other complications were low impedance during surgery in a patient with cochlear ossification, gusher and post-surgery hemorrhage in a patient with incomplete cochlear parti-tion, and a perilymph fistula in a patient with normal anatomy. One patient with no anatomical anomalies was admitted 3 months after implantation because of BPPD.
3.5 Non-users4 patients (9.8%) reported to not use their CI. Characteristics of these patients can be seen
in table 3.5. Reasons for not using the CI were pain (patients 2, 3 and 4), “irritation in the brain” (patients 1 and 2), dizziness and nausea (patients 2 and 4) and unpleasant sounds (patient 2). Significant differences in patient related factors between non-users and other CI-users were anatomical anomalies (cochlear ossification) and employment status. Functioning scores were significantly lower in non-users. Non-users 1 and 3 did not fill in the NCIQ. Non-user 2 scored below average on all sub-domains except for Social interactions. On the contrary, non-user 4 scored above average on all sub-domains except for Speech production. This patient was func-tionally deafened in the implanted ear since several years and accustomed to use the non- im-planted ear only. Speech perception scores were 15% on word lists and 80% on number lists. It is likely that the CI did not give any advantage to this patient because of sufficient functioning of the non-implanted ear.
ID Sex Intelligibility SIR score
Lip-read-ing
Language develop-ment
Communication (before/child-hood) Schooling
1. M good 4 good low speech deaf school
2. F good 4 moderate moderate speech + sign deaf school
3. M moderate N/A good low speech + sign HI school
4. M good N/A good high speech HI school
ID Education Job* Progression Etiology Anatomy* Side of CI
Vestibular function (ipsi-, contralateral)
1. secondary no rapidly rubella normal worse hypo-excitable, normal
2. secondary no rapidly rubella normal worse normal, normal
3. secondary no slowly meningitis ossification worse N/A, N/A
4. primary no slowly meningitis ossification worse not excitable, not excitable
Table 3.5: Non-users’ characteristics
* Significant difference with other CI-users. P <.05

22
3.6 Tinnitus20 CI-users (48.8%) reported tinnitus complaints. Of these patients, 40% (n=8) noticed a beneficial effect of the CI on tinnitus, 25% (n=5) reported more tinnitus when the CI was turned on and 35% (n=7) did not notice any effects of the CI on tinni-tus.
Patients who reported tinnitus complaints showed higher scores on NCIQ questions regard-ing Limitations and had a lower mean age of first hearing aid fitting. There was no association be-tween tinnitus and CI usage in hours per day.
Patients with tinnitus received their first hearing aid at a higher age, and patients whose hearing loss was noted after the age of 2 are more likely to experience tinnitus than those who were very young when hearing loss was discovered. The effect of the CI on tinnitus complaints was related to the difference between the implanted ear and the contra-lateral ear. Surprisingly, this was the case regardless of implantation side. A graphical representation is shown in figure 3.6. Patients who experience increase of tinnitus complaints when using the CI are more often unemployed.
4 Discussion
4.1 ConclusionObjectives of this study were (I) to evaluate the results of cochlear implantation in early-deaf-ened adults in the UMCG, (II) to assess which patient characteristics are associated with better outcomes, and (III) to investigate the age span and clinical relevance of prelingual and perilin-gual deafness.
With these objectives in mind, the following conclusions can be made: (I) Results show that early-deafened patients can benefit from cochlear implantation. Mean speech perception score >% and more than 20% of the CI-recipients reaches speech perception scores of >80%. CI-users experience a higher quality of life than non-implanted patients, but a wide variability in implantation outcomes was observed. Furthermore, the majority of the CI-recipients use the CI all waking day. (II) Success of cochlear implantation is correlated with speech- and language related factors, aural/oral school attendance and educational level. Also related to better implan-tation outcome is slow progression of hearing loss. Patients with anatomical anomalies wear the CI less, and those with cochlear ossification score lower on speech perception tests. (III) The only age factor related to outcome is age of onset of hearing loss. Significantly higher scores on QoL and several functioning levels were seen in patients with onset of HL before the age of 2 years.
With the CI turned on, some patients experience alleviation, whereas others experience aggravation of tinnitus complaints. This was related to difference between both ears and em-ployment status. Patients who experience a beneficial effect of the CI on tinnitus have more symmetrical hearing loss than those whose tinnitus worsens with the CI turned on. However, because no question regarding the perceived side of the tinnitus was asked, it is difficult to find an explanation for this finding.
Bars show mean difference between the implanted and contra-lateral ear with 95% CI bars.
Figure 3.6: Effect of CI on tinnitus

23
Patients with LVAS scored higher in overall functioning and QoL sub-domain Sound per-ception advanced. This can be explained by the fact that hearing loss was slowly progressive in both patients. Furthermore, they were both employed, and both scored high on intelligibility, lip-reading skills and language development. All these factors are related to better functioning scores.
CI-users who use the newest CP810-processor scored lower on functioning level Noise. This does not necessarily mean that these speech processors are less effective; another explana-tion for this finding could be that these patients received a newer speech processor because they were unhappy with the older processor and were functioning equally or even lower with the older processor.
Another interesting finding in this study is that daily usage is not related to functioning or quality of life. In other words, some patients are low functioning but still wear the CI all waking day, whereas other relatively good functioning patients wear the CI for shorter periods. This could be explained by the fact that patients have different expectations. It is important to talk about expectations prior to implantation in order to avoid disappointment, especially in the highly variable group of early-deafened adults and adolescents.
4.2 Prelingual deafness and brain plasticityAuditory input is necessary for normal development of auditory processing in the central neural system.71 After a sensitive period, the auditory system becomes less plastic, which limits further cortical reorganization.72 When auditory deprivation is corrected before the age of 3.5 years, cortical auditory evoked potentials can be recovered, but when auditory deprivation lasts be-yond the age of 7 years, developmentally normal neural organization will be irreversibly lost.73
Animal studies have shown decoupling between the primary auditory cortex and higher cortical areas in congenital deafness.74 Presence of bilateral SNHL at the onset of hearing results in a significant reduction in synaptic density the inferior colliculus, as opposed to unilateral SNHL.75
Not only auditory processing, but also linguistic development depends on auditory input in early childhood.73 Exposure to sign language in the first three years of life prevents possible future acquisition of aural/oral language, as a result of cortical reformation.76
In this study we did not find direct associations between age at different stages and inter-vals in between, and subjective outcome scores, apart from post-implant speech perception scores and age of onset. This could be explained by the variability in hearing loss progression: patients with the same age at notion of deafness can have totally different residual hearing some years later.
In adult patients, audiological test results of early childhood are rarely available, due to lack of appropriate testing methods (e.g. BERA) in earlier times. Furthermore, the newborn hearing screening programme was introduced between 2002 and 2006. In early-deafened adults and adolescents, age at discovery therefore rarely corresponds with age of onset of profound hearing loss, and it is difficult to estimate residual hearing during the period of language devel-opment. Since language development halts at a certain age, we can however estimate the amount of auditory deprivation in childhood in terms of language development delay. This could explain the correlations between speechand language related factors and implantation outcome.
4.3 Comparison with other studies In this study 41 early-deafened patients were evaluated to assess results of cochlear implanta-tion. This study differs from previous studies in several ways. First, we did not only measure quality of life, but also functioning, audiometric outcomes and daily usage. These aspects of cochlear implantation are all important in determining success. Second, since most studies include prelingual patients only, 12 years as the age limit for onset of hearing loss is unusual. Finally, as a result of this extended inclusion criterion, a relatively large group could be evalu-ated.

24
In a prospective study by van Dijkhuizen et al.,64 intelligibility of 9 prelingual patients (moderate to profound bilateral hearing loss before the age of 4 year) was tested prior to CI. Speech perception scores and quality of life (NCIQ) were tested before and after implantation. Intelligibility and post-implantation speech perception scores were found to be positively re-lated to NCIQ sub domain Sound perception advanced only. In our study, intelligibility was cor-related with NCIQ sub domains Sound perception advanced and Speech production. Further-more, speech perception scores were correlated with Sound perception advanced, Speech pro-duction and Self-esteem and Social interactions. Additional correlations in our study are likely to be a result of a much larger sample size. It should be noted that our patient group was not only larger, but also more heterogenic with regard to age of onset of hearing loss. However, only 4 patients were certainly deafened after the age of 4. These patients scored lower on sub-domain Speech perception advanced, but inclusion of these patients made correlation between intelligi-bility and sub-domains Speech perception and Sound perception advanced only stronger. We agree with the suggestion of the authors to discard early age of onset of deafness as an exclusion criterion for cochlear implantation.
Klop et al.53 evaluated sound and speech perception and quality of life in 8 prelingually deafened CI-recipients (deaf school attendance since the age of 4). Significant improvement in speech perception and several quality of life measures were found after implantation. No signifi-cant correlations were found between post-implantation speech perception and patient factors, probably as a result of a small sample size. In this study, mean post-implantation speech percep-tion score was 43%. This is significantly lower than the speech perception found in the CI-users our study. This difference is likely to be a result of different selection criteria, as deaf school attendance has been found to correlate with lower speech perception scores. In our study, many patient factors were found to be related with implantation outcome. This is likely to be a result of a much larger sample size. Similar to our experience, the authors mention that the moment of being profoundly deaf (HL >80-90 dB) is very difficult to establish. Since also individual varia-tion in onset, duration and progression of speech and language development play a role, the authors propose the term “early deafened adult” instead of classifying the patient as pre-, peri-, or postlingually deafened. This is also a term that we gladly use.
In a study by Manrique et al. (2006)15 65 prelingual (onset of hearing loss before the age of two) and perilingual patients (onset between the age of two and four) implanted after 14 years of age were evaluated. The authors found that no subject showed enough improvement in speech recognition to participate in a conversation without the visual support of lip-reading. The results of the our study show the contrary; 46.3% of the CI-recipients are able to use the tele-phone and are therefore not dependent on visual input when talking. All of the patients included in our study had onset of hearing loss before the age of two. It’s possible that the difference between our results and their results can be contributed to different selection criteria for im-plantation. However, since the study of Manrique et al. provides very few details on implantation and inclusion criteria, this explanation is hardly more than a guess.
In accordance with a study by Chee et al.77 on 30 early-deafened patients, the majority of the early deafened CI-recipients in the UMCG wear the CI throughout all their waking hours, and over 90% of the CI-recipients in our study only turn off the CI before going to bed or taking a shower. Santarelli et al.54 suggest high educational level to be a positive predictor for implanta-tion outcome. The present study shows that educational level is indeed positively correlated with functioning and quality of life after implantation, but no correlation with speech perception (word lists) was found. However, it is possible that higher education is actually a result of better developed language. In that case, educational level should not be interpreted as an independent factor.
4.4 Limitations of this study
Strengths of this study are the high response rate (82%) in the CI recipient group and the fact that not only audiometrical outcomes, but also quality of life and functioning are used to assess

25
whether cochlear implantation is successful.
Limitation of this study is the low response rate in non-implanted subjects (37%). As a result, only non-parametric analysis of the data was possible. Results of non-implanted subjects are biased by low response rate: it is likely that non-responders are more often declined by the CI team instead of by their own choice. In that case, QoL scores of the physical sub domain in non-implanted patients are expected to be lower than presented in this study.
Furthermore, to assess stimulation of speech-language development in childhood an open ended question was added to the general questionnaire. It was impossible to quantify the an-swers due to variability. It would have been more useful to use a scale from 0 to 10 to assess stimulation. To assess tinnitus and the influence of hearing loss asymmetry on tinnitus it would have been useful to ask if tinnitus was experienced in the implanted or in the non-implanted ear.
Although easy to use, the CIFI had its limitations. First, the original scoring system is based on a 0 to 24 scale, whereas the maximum score is 22 points. Second, 4 points are based on func -tioning at work. Since (39%) of our study group was unemployed, the maximum score for those patients was only 18 points, making it impossible to score “highest” functioning. Finally, our Dutch translation of the CIFI is not tested on validity and results should therefore be interpreted with caution. The CIFI does correspond with the NCIQ sub-domains regarding physical function-ing (Sound perception basic, Sound perception advanced and Speech production). Since these sub-domains match with the aimed goals of implantation, the CIFI can provide a decent repre-sentation of CI outcome.
Lastly, we compared quality of life scores of different groups. Since quality of life is a highly subjective score, it is better to compare individual pre- implantation with post-implanta-tion scores. Furthermore, both groups are not composed randomly, but as a result of implanta-tion criteria, the advice of the CI-team and in some patients the personal choice not to be im -planted.
4.5 Recommendations for future research
To assess whether the factors mentioned in this study are predictors for successful cochlear implantation, a prospective study with pre- and post-implantation quality of life scores is recom-mended. A more objective reflection of speech- and language development could be obtained by using a standardized test instrument to assess both spoken language and written language, with special attention to language syntax. It is also interesting to see if stimulation of language- and speech development during childhood is predictive for better outcomes. To evaluate this, a quantitative test should be developed, e.g. a questionnaire with Likert-scale questions regarding verbal conversations, singing, being read to by parents, reading aloud etc. during childhood.
In deciding whether a patient is suited for cochlear implantation, it could be helpful to have a scoring list with items related to successful implantation. Points could be assigned to each beneficial item depending on the influence of this particular item on implantation outcome. The total of these points can estimate the chance of a successful cochlear implantation in an individ-ual patient. The possibilities to develop such a scoring system are currently being evaluated.
AcknowledgementsFirst and foremost, I am very grateful to my supervisors Rolien Free and Rutger Hofman, who guided and supported me throughout this study. I would also like to express my thanks to Pro-fessor Paul E. Hammerschlag for permitting me to use and translate the CIFI, to Gerda Boven for her patience and perseverance in collecting patient charts for me, and to Bert Maat for providing answers to audiological questions and for helping me with data collection. Finally, this study was not possible without the help of the CI-team.

26
References [1] Shah SB, Chung JH, Jackler RK. Lodestones, quackery, and science: electrical stimulation of the ear before cochlear implants. Am J Otol. 1997;18(5):665–670.
[2] Djourno A, Eyriès C. [Audi-tory prosthesis by means of a distant electrical stimulation of the sensory nerve with the use of an indwelt coiling]. Presse Med. 1957;65(63):1417.
[3] Simmons FB, Epley JM, Lummis RC, Guttman N, Fr-ishkopf LS, Harmon LD, et al. Auditory Nerve: Electrical Stimu-lation in Man. Science. 1965;148:104–106.
[4] Eisen MD. The History of Cochlear Implants. In: Niparko JK, Kirk KI, Mellon NK, Robbins AM, Tucci DL, Wilson BS, editors. Cochlear implants: principles & practices. 2nd ed. Philadelphia (PA): Lippincott Williams & Wilkins; 2009. p. 89–94.
[5] Blume SS. The Making of the Cochlear Implant. In: The artifi-cial ear: cochlear implants and the culture of deafness. 1st ed. New Brunswick, NJ: Rutgers University Press; 2010. p. 30–57.
[6] Zeng FG, Rebscher S, Harri-son WV, Sun X, Feng H. Cochlear Implants: System Design, Inte-gration and Evaluation. IEEE Rev Biomed Eng. 2008;1:115–142.
[7] Bond M, Mealing S, Anderson R, Elston J, andR S Taylor GW, Hoyle M, et al. The effectiveness and cost-effectiveness of cochlear implants for severe to profound deafness in children and adults: a systematic review and economic model. Health Technology Assessment. 2009;13(44):1–330.
[8] Adams JS, Hasenstab MS, Pippin GW, Sismanis A. Tele-phone use and understanding in patients with cochlear implants. Ear Nose Throat J. 2004;83(2):96, 99–100, 102–3.
[9] West RE, Stucky J. Cochlear implantation outcomes: experi-ence with the Nucleus 22 im-plant. Ann Otol Rhinol Laryngol Suppl. 1995;166:447–449.
[10] Summerfield AQ, Marshall DH. Non-use of cochlear im-plants by post-lingually deafened adults. Cochlear Implants Int. 2000;1(1):18–38.
[11] Huizing HC. Recent Devel-opments in Modern Language Teaching for the Deaf Child. International Journal of Audiol-ogy. 1966;5(3):344–348.
[12] Gibson W. The current status of cochlear implants. Indian Journal of Otolaryngology and Head & Neck Surgery. 1995;47:83–90. 10.1007/BF03047933.
[13] Bassim MK, Buss E, Clark MS, Kolln KA, Pillsbury CH, Pillsbury HC, et al. MED-EL Combi40+ cochlear implantation in adults. The Laryngoscope. 2005;115(9):1568–1573.
[14] Kiefer J, Gall V, Desloovere C, Knecht R, Mikowski A, von Ilberg C. A follow-up study of long-term results after cochlear implantation in children and adolescents. Eur Arch Otorhino-laryngol. 1996;253(3):158–166.
[15] Manrique M, Ramos A, Morera C, Cenjor C, Lavilla MJ, Boleas MS, et al. [Analysis of the cochlear implant as a treatment technique for profound hearing loss in pre and postlocutive
patients]. Acta Otorrinolaringol Esp. 2006 Jan;57(1):2–23.
[16] Teoh SW, Pisoni DB, Miyamoto RT. Cochlear implan-tation in adults with prelingual deafness. Part I. Clinical results. The Laryngoscope. 2004;114(9):1536–1540.
[17] Eisenberg LS, Johnson KC, Martinez AS, DesJardin JL, Stika CJ, Dzubak D, et al. Comprehen-sive evaluation of a child with an auditory brainstem implant. Otol Neurotol. 2008;29(2):251–257.
[18] Lachs L, Pisoni DB, Kirk KI. Use of audiovisual information in speech perception by prelin-gually deaf children with cochlear implants: a first report. Ear Hear. 2001;22(3):236–251.
[19] Franz DC. Pediatric perfor-mance with the Med-El Combi 40+ cochlear implant system. Ann Otol Rhinol Laryngol Suppl. 2002;189:66–68.
[20] Kirk KI, Miyamoto RT, Lento CL, Ying E, O’Neil T, Fears B. Effects of Age at Implantation in Young Children. Annals of Otol-ogy, Rhinology & Lanyngology. 2002;111(5):69–73.
[21] Uziel AS, Sillon M, Vieu A, Artieres F, Piron JP, Daures JP, et al. Ten-year follow-up of a con-secutive series of children with multichannel cochlear implants. Otol Neurotol. 2007;28(5):615–628.
[22] Zwolan TA, Ashbaugh CM, Alarfaj A, Kileny PR, Arts HA, El-Kashlan HK, et al. Pediatric cochlear implant patient perfor-mance as a function of age at implantation. Otol Neurotol. 2004;25(2):112–120.
[23] Kirk KI, Hay-McCutcheon MJ, Holt RF, Gao S, Qi R, Gehrlein

27
BL. Audiovisual Spoken Word Recognition by Children with Cochlear Implants. Audiol Med. 2007;5(4):250–261.
[24] Fryauf-Bertschy H, Tyler RS, Kelsay DM, Gantz BJ, Woodworth GG. Cochlear implant use by prelingually deafened children: the influences of age at implant and length of device use. Journal of Speech, Language, and Hear-ing Research: JSLHR. 1997;40(1):183–199.
[25] Connor CM, Hieber S, Arts HA, Zwolan TA. Speech, vocabu-lary, and the education of chil-dren using cochlear implants: oral or total communication? J Speech Lang Hear Res. 2000;43(5):1185–1204.
[26] Hehar SS, Nikolopoulos TP, Gibbin KP, O’Donoghue GM. Surgery and functional outcomes in deaf children receiving cochlear implants before age 2 years. Arch Otolaryngol Head Neck Surg. 2002;128(1):11–14.
[27] Houston DM, Pisoni DB, Kirk KI, Ying EA, Miyamoto RT. Speech perception skills of deaf infants following cochlear im-plantation: a first report. Int J Pediatr Otorhinolaryngol. 2003;67(5):479–495.
[28] Kirk KI, Miyamoto RT, Ying EA, Perdew AE, Zuganelis H. Cochlear Implantation in Young Children: Effects of Age at Im-plantation and Communication Mode. Volta Review. 2000;102(4):127–144.
[29] Nikolopoulos TP, O’Donoghue GM, Archbold S. Age at implantation: its importance in pediatric cochlear implanta-tion. Laryngoscope. 1999;109(4):595–599.
[30] Yoshinaga-Itano C, Sedey AL, Coulter DK, Mehl AL. Lan-
guage of earlyand later-identi-fied children with hearing loss. Pediatrics. 1998;102(5):1161–1171.
[31] Holt RF, Svirsky MA. An exploratory look at pediatric cochlear implantation: is earliest always best? Ear Hear. 2008;29(4):492–511.
[32] Waltzman SB, Roland JT, Cohen NL. Delayed implantation in congenitally deaf children and adults. Otology & Neurotology: Official Publication of the Ameri-can Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2002;23(3):333–340.
[33] Miyamoto RT, Houston DM, Kirk KI, Perdew AE, Svirsky MA. Language development in deaf infants following cochlear im-plantation. Acta Otolaryngol. 2003;123(2):241–244.
[34] Luxford WM, Eisenberg LS, Johnson KC, Mahnke EM. Cochlear implantation in infants younger than 12 months. Inter-national Congress Series. 2004;1273:376–379. Cochlear Implants. Proceedings of the VIII International Cochlear Implant Conference.
[35] Colletti V, Carner M, Miorelli V, Guida M, Colletti L, Fiorino FG. Cochlear implantation at under 12 months: report on 10 patients. Laryngoscope. 2005;115(3):445–449.
[36] Tyler RS, Fryauf-Bertschy H, Kelsay DM, Gantz BJ, Woodworth GP, Parkinson A. Speech perception by prelingually deaf children using cochlear implants. Otolaryngology–Head and Neck Surgery: Official Journal of American Academy of Otolaryn-
gology-Head and Neck Surgery. 1997;117(3 Pt 1):180–187.
[37] Merkus P, van Furth AM, Goverts ST, Suèr M, Smits CF, Smit C. [Postmeningitis deafness in young children: action war-ranted before obliteration of the cochlea]. Ned Tijdschr Geneeskd. 2007 Jun;151(22):1209–1213.
[38] Philippon D, Bergeron F, Ferron P, Bussières R. Cochlear implantation in postmeningitic deafness. Otol Neurotol. 2010 Jan;31(1):83–87.
[39] Durisin M, Bartling S, Arnoldner C, Ende M, Prokein J, Lesinski-Schiedat A, et al. Cochlear osteoneogenesis after meningitis in cochlear implant patients: a retrospective analy-sis. Otol Neurotol. 2010 Sep;31(7):1072–1078.
[40] Clark GM, Busby PA, Roberts SA, Dowell RC, Tong YC, Blamey PJ, et al. Preliminary results for the cochlear corporation multi-electrode intracochlear implant in six prelingually deaf patients. The American Journal of Otology. 1987;8(3):234–239.
[41] Tong YC, Busby PA, Clark GM. Perceptual studies on cochlear implant patients with early onset of profound hearing impairment prior to normal development of auditory, speech, and language skills. The Journal of the Acoustical Society of America. 1988;84(3):951–962.
[42] Working Group on Commu-nication Aids for the Hearing-Im-paired. Speech-perception aids for hearing-impaired people: current status and needed research. Working Group on Communication Aids for the Hearing-Impaired. The Journal of the Acoustical Society of Amer-ica. 1991;90(2 Pt 1):637–683.

28
[43] Skinner MW, Binzer SM, Fears BT, Holden TA, Jenison VW, Nettles EJ. Study of the performance of four prelinguisti-cally or perilinguistically deaf patients with a multi-electrode, intracochlear implant. The Laryngoscope. 1992;102(7):797–806.
[44] Waltzman SB, Cohen NL, Shapiro WH. Use of a multichan-nel cochlear implant in the congenitally and prelingually deaf population. The Laryngo-scope. 1992;102(4):395–399.
[45] Zwolan TA, Kileny PR, Telian SA.Self-report of cochlear implant use and satisfaction by prelingually deafened adults. Ear and Hearing. 1996;17(3):198–210.
[46] Snik AF, Makhdoum MJ, Vermeulen AM, Brokx JP, van den Broek P. The relation be-tween age at the time of cochlear implantation and long-term speech perception abilities in congenitally deaf subjects. International Journal of Pediatric Otorhinolaryngology. 1997;41(2):121–131.
[47] Sarant JZ, Cowan RS, Blamey PJ, Galvin KL, Clark GM. Cochlear implants for congenitally deaf adolescents: is open-set speech perception a realistic expecta-tion? Ear and Hearing. 1994;15(5):400–403.
[48] Manrique N, Huarte A, Molina M, Perez N, Espinosa JM, Cervera-Paz FJ, et al. Are cochlear implants indicated in prelingually deaf adults? The Annals of Otology, Rhinology & Laryngology Supplement. 1995;166:192–194.
[49] Hinderink JB, Mens LH, Brokx JP, van den Broek P. Performance of prelingually and
postlingually deaf patients using single-channel or multichannel cochlear implants. The Laryngo-scope. 1995;105(6):618–622.
[50] Waltzman SB, Cohen NL. Implantation of patients with prelingual long-term deafness. The Annals of Otology, Rhinology & Laryngology Supplement. 1999;177:84–87.
[51] Schramm D, Fitzpatrick E, Séguin C. Cochlear implantation for adolescents and adults with prelinguistic deafness. Otology & Neurotology: Official Publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2002;23(5):698–703.
[52] Kaplan DM, Shipp DB, Chen JM, Ng AHC, Nedzelski JM. Early-deafened adult cochlear implant users: assessment of outcomes. The Journal of Otolaryngology. 2003;32(4):245–249.
[53] Klop WMC, Briaire JJ, Stiggelbout AM, Frijns JHM. Cochlear implant outcomes and quality of life in adults with prelingual deafness. The Laryn-goscope. 2007;117(11):1982–1987.
[54] Santarelli R, Filippi RD, Genovese E, Arslan E. Cochlear implantation outcome in prelin-gually deafened young adults. A speech perception study. Audiol-ogy & Neuro-Otology. 2008;13(4):257–265.
[55] Yoshida H, Kanda Y, Miyamoto I, Fukuda T, Takahashi H. Cochlear implantation on prelingually deafened adults. Auris, Nasus, Larynx. 2008;35(3):349–352.
[56] Kos M, Deriaz M, Guyot J, Pelizzone M. What can be ex-pected from a late cochlear
implantation? International Journal of Pediatric Otorhino-laryngology. 2009;73(2):189–193.
[57] Geers A, Brenner C. Back-ground and educational charac-teristics of prelingually deaf children implanted by five years of age. Ear and Hearing. 2003;24(1 Suppl):2S–14S.
[58] Osberger MJ, Fisher L. Preoperative predictors of postoperative implant perfor-mance in children. Ann Otol Rhinol Laryngol Suppl. 2000;185:44–46.
[59] Loundon N, Busquet D, Roger G, Moatti L, Garabedian EN. Audiophonological results after cochlear implantation in 40 congenitally deaf patients: preliminary results. Interna-tional Journal of Pediatric Otorhinolaryngology. 2000;56(1):9–21.
[60] Hiraumi H, Yamamoto N, Sakamoto T, Ito J. Cochlear implantation in patients with prelingual hearing loss. Acta Oto-Laryngologica Supplementum. 2010;130(S563):4–10.
[61] Wiley S, Meinzen-Derr J, Choo D. Auditory skills develop-ment among children with developmental delays and cochlear implants. Ann Otol Rhinol Laryngol. 2008;117(10):711–718.
[62] Edwards LC, Frost R, Witham F. Developmental delay and outcomes in paediatric cochlear implantation: implica-tions for candidacy. Int J Pediatr Otorhinolaryngol. 2006;70(9):1593–1600.
[63] Watson SD, Balko KA, Comer LK, Bishop RD, Reilley D, Backous DD. Benefits of cochlear implantation in pre- lingual adult

29
users: oral and manual commu-nicators. Cochlear Implants International. 2003;4 Suppl 1:75–76.
[64] van Dijkhui zen JN, Beers M, Boermans PPBM, Briaire JJ, Frijns JHM. Speech intelligibility as a predictor of cochlear im-plant outcome in prelingually deafened adults. Ear Hear. 2011;32(4):445–458.
[65] Teoh SW, Pisoni DB, Miyamoto RT. Cochlear implan-tation in adults with prelingual deafness. Part II. Underlying constraints that affect audiologi-cal outcomes. The Laryngoscope. 2004;114(10):1714–1719.
[66] Cohen NL, Waltzman SB, Fisher SG. A prospective, ran-domized study of cochlear implants. The Department of Veterans Affairs Cochlear Im-plant Study Group. N Engl J Med. 1993;328(4):233–237.
[67] Gantz BJ, Tyler RS, Knutson JF, Woodworth G, Abbas P, McCabe BF, et al. Evaluation of five different cochlear implant designs: audiologic assessment and predictors of performance. Laryngoscope. 1988;98(10):1100–1106.
[68] Coelho DH, Hammerschlag PE, Bat-Chava Y, Kohan D. Psy-chometric validity of the Cochlear Implant Function Index (CIFI): a quality of life assess-ment tool for adult cochlear implant users. Cochlear Implants Int. 2009;10(2):70–83.
[69] Hinderink JB, Krabbe PF, Broek PVD. Development and application of a health-related quality-of-life instrument for adults with cochlear implants: the Nijmegen cochlear implant questionnaire. Otolaryngol Head Neck Surg. 2000;123(6):756–765.
[70] Krabbe PF, Hinderink JB, van den Broek P. The effect of cochlear implant use in postlin-gually deaf adults. Int J Technol Assess Health Care. 2000;16(3):864–873.
[71] Syka J. Plastic changes in the central auditory system after hearing loss, restoration of function, and during learning. Physiol Rev. 2002 Jul;82(3):601–636.
[72] Kral A, Hartmann R, Tillein J, Heid S, Klinke R. Hearing after congenital deafness: central auditory plasticity and sensory
deprivation. Cereb Cortex. 2002 Aug;12(8):797–807.
[73] Sharma A, Dorman M, Spahr A, Todd NW. Early cochlear implantation in children allows normal development of central auditory pathways. Ann Otol Rhinal Laryngol SuppL 2002 May;189:38-41.
[74] Kral A, Tillein J, Heid S, Hartmann R, Klinke R. Postnatal cortical development in congeni-tal auditory deprivation. Cere-bral Cortex (New York, NY 1991). 2005;15(5) 552-562.
[75] Nishiyama N, Paolini AG, Shepherd RK Intracellular recording from the primary auditory cortex. Adv Otorhino-laryngoL 2000;57:18--21.
[76] Nishimura H, Hashikawa K, Doi K, lwaki T, Watanabe Y, Kusuoka H, et al. Sign language 'heard' in the auditory cortex. Nature. 1999;397(6715) 116.
[77] Chee GH, Goldring JE, Shipp DB, Ng AHC, Chen JM, Nedzelski JM. Benefits of cochlear implan-tation in early-deafened adults: the Toronto experience. J Otola-ryngoL 2004 Feb;33(1) 26-31.

30
Appendices
Appendix A: General questionnaire implanted patients

31
Appendix B: General questionnaire non-implanted patients

32
Appendix C : Cochlear Implant Function Index

33
Appendix D: Nijmegen Cochlear Implant Questionnaire

34
Appendix E : Patient characteristics

35
*Implanted during this study, ** non-users

36
Abstract in DutchDoel: In dit retrospectieve onderzoek werden uitkomsten van cochleaire implantatie implantatie bij vroeg-dove volwassenen in het UMCG geëvalueerd: er werd gekeken welke patiëntgebonden factoren gerelateerd zijn aan succesvolle uitkomst en naar het klinische belang en de leeftijdsgrenzen van pre- peri- en postlinguale doofheid bij CI-gebruikers.
Materiaal en methode: Bij 41 CI-gebruikers, die vóór de leeftijd van 12 jaar slechthorend zijn geworden en na de leeftijd van 16 jaar geïmplanteerd zijn, werd gekeken naar audiologische uitkomsten (foneemscores en PTA-drempels), kwaliteit van leven (Nijmegen Cochlear Implant Questionnaire), functioneren (Cochlear Implant Function Index) en tinnitusklachten na cochleaire implantatie, en naar het aantal draaguren per dag. Kwaliteit van leven werd vergeleken met 22 niet-geïmplanteerde vroeg-dove patiënten. Er werd gezocht naar verbanden met spraak- en taalgebonden factoren, opleiding, leeftijdsgebonden factoren, pre-implantatie scores, anatomische afwijkingen, vestibulaire functie en etiologie, operatiegerelateerde factoren, en implantaat type en spraakprocessor.
Resultaten: Positieve correlaties werden gevonden tussen implantatie-uitkomsten en spraakverstaanbaarheid, taalniveau, lipleesvaardigheden, oraal-auraal onderwijs en opleidingsniveau. Ook progressie en leeftijd waarop de slechthorendheid is ontstaan zijn van invloed, waarbij aanvang van slechthorendheid voor de leeftijd van 2 jaar gunstig is. Patiënten met cochleaire ossificatie scoorden significant slechter. Er werd geen verband gevonden tussen implantatie-uitkomsten en leeftijd van eerste hoortoestel, leeftijd waarop slechthorendheid werd opgemerkt of leeftijd bij implantatie.
Conclusie: Bij het selecteren van prelinguaal- of vroeg-dove volwassenen voor cochleaire implantatie is het van groter belang te kijken naar logopedische factoren en genoten onderwijs dan naar leeftijdsgebonden factoren. De klinische relevantie van pre- peri- of postlinguale periode lijkt bepert te zijn en het is daarom passender om te spreken over vroeg-dove patiënten.