Embed Size (px)
Citation preview
Aurora Health AccessProgram Report for CFPHEDecember 2014
During this time period, Aurora Health Access (AHA) had two sources of funding managed by the Colorado Foundation for Public Health and Environment (CFPHE):
1. Phase One Health Equity Advocacy grant from The Colorado Trust o Grant Period: 4/1/2014 to 9/31/2014 Award: $40,000
2. A Project Support Grant funded by the Colorado Health Foundation o Grant Period: 3/1/2013 to 2/23/2017 Award: $107,120/year for 3 years
1. The Colorado Trust - Phase One Health Equity Advocacy Planning GrantThe Health Equity Advocacy grant was awarded as a “general operating” grant with only two requirements. 1) Someone from AHA was to attend each of six monthly meetings hosted by The Colorado Trust. AHA’s Executive Director and/or Chair or Vice Chair attended each meeting as required. 2) AHA must submit an Implementation Plan by September 30, 2014. The Colorado Trust selected up to 19 organizations for funding from among the 38 organizations awarded Phase One Funding. AHA assembled a Work Group to create the Implementation Plan. The grant application template and timeline were shared with CFPHE to make sure they were aware of the deadline and the budgetary attachments required.
December UpdateWe submitted our Implementation Plan Phase II funding on September 29, 2014. Unfortunately, AHA was not one of the 18 applicants selected for further funding. Below, I have included a section of the application, which describes AHA’s involvement in health equity advocacy efforts.
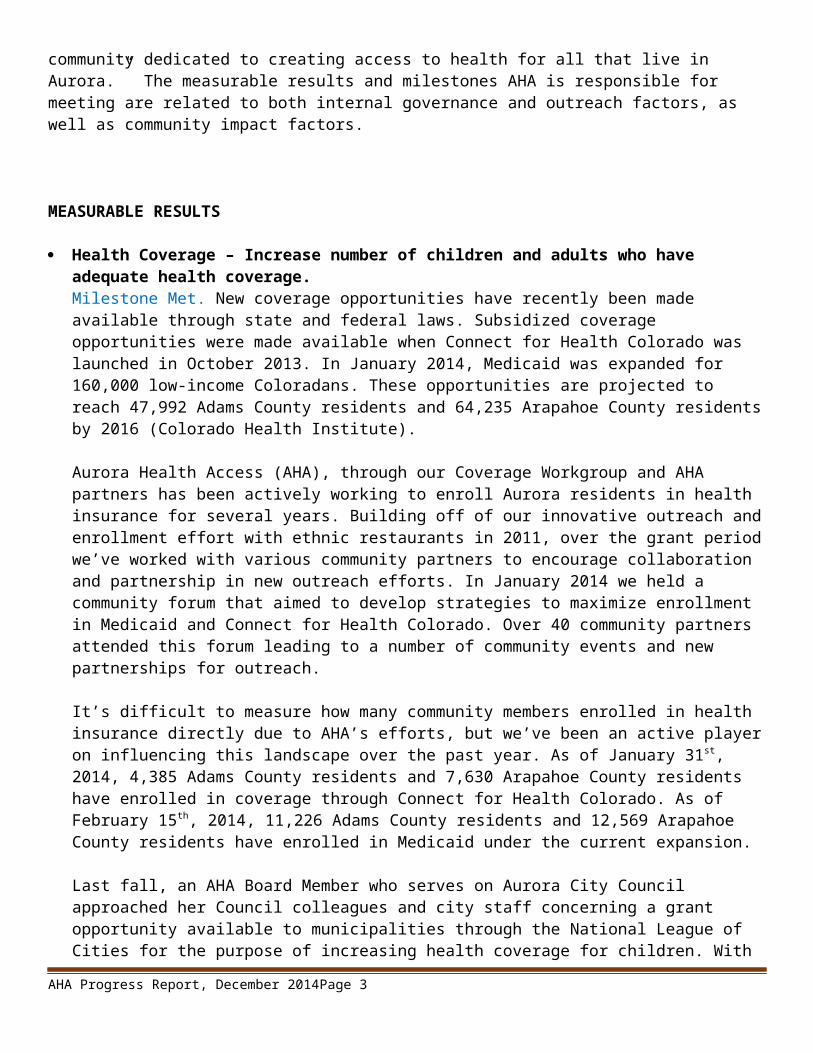
Health Equity Focus Section 1 describes how AHA will advance health equity policy solutions through advocacy. Health equity is a complex issue that needs to be addressed at multiple levels by multiple entities working toward the same goal. AHA’s assessments revealed that our unique contribution to the field of health equity advocacy is the capacity to connect representatives from the full spectrum of health service providers into one place at one time; to serve as an effective “neutral convener.” Additionally, our members believe AHA has earned the reputation of being able to work collaboratively with key stakeholders to identify Aurora’s health disparities, and to help create innovative shared solutions to address them. Here’s what our members say:
“By attending just one of AHA’s quarterly meetings, I can reach out to and hear from so many of Aurora’s health provider agencies. I can’t get that exposure or opportunity anywhere else.“ - AHA Member from Aurora Community Assistance Network
“Our participation in AHA is critical. While we can do grass roots organizing around health care very well, without AHA, we’d have to then work hard to reach all the various hospitals, clinics, decision-makers and bureaucrats’ one at a time. AHA gives us a platform to reach our intended audience more efficiently.” - AHA Member from Together Colorado
AHA Progress Report, December 2014 Page 1
“We value our AHA membership because we know that through AHA we are better connected to Aurora’s health care infrastructure and its communities.” - AHA Member from Kaiser Permanente
AHA will build on this existing capacity to serve as a catalyst and neutral convener to identify and address health disparities in Aurora.
2.The Colorado Health Foundation - Project Support GrantNote: For the CFPHE report,
I am using the annual Progress Report submitted to The Colorado Health Foundation in February 2014 as the template. You will see the updates I added in August, and the new updates for activities in September, October, and November added in green.
The purpose of this grant is to “support AHA, a community health alliance. Funds will enable the hiring of staff and formalize as an entity in the community dedicated to creating access to health for all that live in Aurora.” The measurable results and milestones AHA is responsible for meeting are related to both internal governance and outreach factors, as well as community impact factors.
MEASURABLE RESULTS
Health Coverage – Increase number of children and adults who have adequate health coverage.Milestone Met. New coverage opportunities have recently been made available through state and federal laws. Subsidized coverage opportunities were made available when Connect for Health Colorado was launched in October 2013. In January 2014, Medicaid was expanded for 160,000 low-income Coloradans. These opportunities are projected to reach 47,992 Adams County residents and 64,235 Arapahoe County residents by 2016 (Colorado Health Institute).
Aurora Health Access (AHA), through our Coverage Workgroup and AHA partners has been actively working to enroll Aurora residents in health insurance for several years. Building off of our innovative outreach and enrollment effort with ethnic restaurants in 2011, over the grant period we’ve worked with various community partners to encourage collaboration and partnership in new outreach efforts. In January 2014 we held a community forum that aimed to develop strategies to
AHA Progress Report, December 2014 Page 2
maximize enrollment in Medicaid and Connect for Health Colorado. Over 40 community partners attended this forum leading to a number of community events and new partnerships for outreach.
It’s difficult to measure how many community members enrolled in health insurance directly due to AHA’s efforts, but we’ve been an active player on influencing this landscape over the past year. As of January 31st, 2014, 4,385 Adams County residents and 7,630 Arapahoe County residents have enrolled in coverage through Connect for Health Colorado. As of February 15 th, 2014, 11,226 Adams County residents and 12,569 Arapahoe County residents have enrolled in Medicaid under the current expansion.
Last fall, an AHA Board Member who serves on Aurora City Council approached her Council colleagues and city staff concerning a grant opportunity available to municipalities through the National League of Cities for the purpose of increasing health coverage for children. With the City’s approval, AHA took the lead in researching and writing an application for grant funding. In November, Aurora was one of twelve cities in the country selected for a grant to develop a business plan for an outreach campaign to ensure coverage for young children and emancipated youth. This is the only “KidsWell” grant in the state funded and coordinated by the National League of Cities to use the credibility of the city to increase enrollment of the estimated 7,400 eligible but not enrolled Aurora children by 50%. The City issued an RFP and selected a project facilitator who hosted the first of three stakeholder meetings on February 26 th. Six of the twelve cities that received planning grants will be selected by the NLC to receive two-year implementation grants for innovative messaging and outreach communications.
August Update: AHA continues to coordinate closely with Aurora Coverage Assistance Network (ACAN) to expand coverage throughout Aurora. ACAN, housed within Aurora Mental Health Center, brings five local agencies together, which were funded to provide coverage guides for the city – Aurora NAACP, Metro Provider Community Network, Asian Pacific Development Center, the Colorado African Organization, and Aurora Mental Health Center. During the last meeting, we approved a calendar of events for the 2014-15 open enrollment season, which includes health and enrollment fairs at the Aurora Mall, enrollment desks at King Soopers grocery stores, a health fair at Aurora Community College, phone banks, and door-to-door canvasing in targeted communities.
In order to reach small businesses, AHA has convened a partnership with the Small Business Majority and Aurora Chamber of Commerce to explore the feasibility of offering “lunch and learn” events.
AHA is partnering with South Metro Health Alliance and Tri-County Health to explore ways to increase access to oral health services and coverage throughout Arapahoe County. We have scheduled a planning group of oral health stakeholders, who will meet on September 24 th to develop a work plan. The participants include representatives from Oral Health Colorado, Health Care Policy and Financing, ClinicNET, the UC School of Dental Health, and others.
In August, AHA met with Arapahoe County Cooperative Extension to learn more about their “Smart Choice Health Insurance” training program. This program offers an intensive 2-hour training and case study to teach participants how to assess and shop for health insurance plans. AHA will coordinate with ACAN navigators to test the effectiveness of the training module before offering it in the community.
December Update
AHA Progress Report, December 2014 Page 3
The Oral Health Convening was held on September 24th. Participants from fifteen organizations attended including the Metro Denver Dental Society, Kids in Need of Dentistry, the UC School of Dental Medicine, and the Division of Health Care Policy and Financing. The participants discussed access and coverage issues, and identified current and ongoing oral health access and expansion efforts. All participants agreed to serve as an informal Oral Health Interest Group of AHA. AHA compiled and distributed the meeting notes, and will use the information to populate our website with additional oral health access and coverage information. Attachment: Oral Health Convening Participant List One of the gaps noted by the Aurora Community Assistance Network (ACAN) – with whom we collaborate in our coverage expansion efforts, is information and support for small businesses regarding the health insurance market. On October 22, AHA hosted a “lunch and learn” workshop titled: “Your Bottom Line: What the Affordable Care Act Means for Your Small Business.” The event was organized in collaboration with the Aurora Chamber of Commerce, the Aurora Community Assistance Network, and the Small Business Majority. The workshop was a success based on filling every seat available in the community room, and results of the evaluation. Attachment: Workshop Evaluation Summary
Health Care – Increase number of underserved Coloradans who receive integrated care.Milestone Met. Through both our Adult and Pediatric Access to Care Workgroups, Aurora Health Access has been an integral community partner in several community initiatives working to improve access to integrated care in Aurora.
MCPN and Together Colorado’s Bridges to Care program, which AHA was essential in creating, has enrolled nearly 300 high-utilizers of Aurora’s hospital systems. This program provides comprehensive case management and integrated primary care services to these high needs Aurora patients.
Aurora Health Access was also a key driver in the creation of the Triage Project, a project between Aurora Mental Health Center and Arapahoe House targeting high-utilizers of the EMS system in Aurora. This project enrolled 120 individuals in 2013 providing them with an integrated medical home and robust medical and behavioral health interventions. The project saved thousands of dollars of system expenditures.
August Update: MCPN and Together Colorado recently held a “graduation celebration” for Bridges to Care participants. Preliminary data shows that the program resulted in a 43% reduction in total hospital utilization and 41% reduction in ER visits for UC Hospital. Results also indicate per person savings cost to the hospital of $22,930 per enrollee, for a total savings of over $2.2 million. AHA will continue to support MCPN in finalizing the findings and seeking future funds to continue the program.
The Pediatric Access Workgroup is seeking a grant from the Piton Foundation to develop Spanish “novellas,” which will promote preventive care, the medical home model, and explain coverage options. AHA will assist in distribution of the novella throughout the community. The Pediatric Workgroup is also finalizing a current, detailed resource list of medical home sites available to Aurora residents. AHA will host the list in a new section of our website, “Data Resources, Resource Lists, and Reports.”
Unfortunately, the City of Aurora was not selected for funding for the KidsWell project. AHA provided administrative support to facilitate the development of the application.
AHA Progress Report, December 2014 Page 4
December UpdateWhile the KidsWell application was not funded by the National League of Cities, AHA is supporting the City’s efforts to share the application with an appropriate organization to implement the proposed activities. The City is meeting with the Early Childhood Council to explore collaboration.
One of the tactics proposed by the AHA Pediatric Access Workgroup to increase access to integrated care was to find a medical home for each of Aurora’s children. In November, the Workgroup finalized a resource list of medical homes serving children in and around north Aurora – Aurora’s most underserved area. This list will be used by patient navigators, case managers, and discharge planners at Children’s hospital to help families find an appropriate practice. AHA will post the list on our website, and help distribute it to health and social service agencies throughout the community. It will be updated and redistributed every six months by Children’s Hospital staff.
The Pediatric Workgroup has also agreed to host a second “Healthy Kids Aurora” convening in May 2015, in partnership with Children’s Hospital.
The Adult Access Workgroup has added a focus on access to specialty care services, which has been become even more challenging as many new patients enter the system due to the Affordable Care Act. AHA participated in a meeting on October 30th between the leadership of the University of Colorado Hospital and University Physicians, Inc. and primary care providers and community representatives. Several short-term strategies were identified for addressing the problems. AHA will serve as a neutral convener and catalyst for exploring and implementing these strategies.
AHA has played an integral role in supporting the creation of an Interdisciplinary Student Run Free Clinic, which is scheduled to start seeing patients in January 2015. The following Executive Summary describes the clinic operations:
The Colorado chapter of Primary Care Progress, representing the interests of 740 Anschutz health professional trainees, will oversee and manage this interdisciplinary student-run free clinic (SRFC). It will operate in partnership with the Dayton Opportunity Center, a new community hub at 1445 Dayton Street managed jointly by the Fields Foundation and Mosaic Church of Aurora. This partnership allows for not only traditional primary care delivery, but comprehensive management of patients’ health maintenance and social needs. Close community-campus partnership enables provision of sustainable, desperately needed primary care for uninsured adults in Aurora.
The SRFC will initially be open to see adult patients from 5:30-9:00pm on Wednesday evenings, with the potential for expanded hours as the venture becomes established. Thursday evenings will be devoted to patient care coordination, with clinic leaders and Fields Foundation navigators working together to ensure that we follow through on our patients’ holistic care plans. We may add additional clinic activity times for clinical psychology and physical therapy, which may be limited by privacy and space on Wednesday evenings.
The target population is primarily low income, uninsured, young working adults with children. However, we do expect to see an influx of older patients with more chronic disease over time as the clinic becomes established. We will not provide any medical care to children. Rather, children without primary care will be enrolled in appropriate insurance programs on-site and referred to Children’s Health Clinics at Children’s Hospital and other area pediatric providers through the Colorado Children’s Health Access Program (CCHAP).
AHA Progress Report, December 2014 Page 5
These children will be offered enrollment in the Fields Foundation’s central Pediatric Care Coordination (PCC) program, whereby the Colorado Health Foundation has provided a 2-year $360,000 grant to hire a nurse care coordinator and 3 community health workers. This team provides care navigation to families with vulnerable children in Original Aurora and will go live this autumn. Given that we expect many parents of our pediatric patients to lack access to primary care, the SRFC will take adult referrals from the Fields Foundation PCC team.
Patients will be seen at the clinic in a variety of settings, depending on their needs. The space includes 3 sound-proof, 3 private, and 3 semi-private exam rooms, plus 1 group visit room and a large waiting room and café area. This will allow us to see approximately 25-30 patients per week, or 1500 patients per year. All students will practice according to their future scope of practice, with faculty from each interprofessional field closely supervising. Examples of work include:
1. Medical students to see traditional patient consults in-person and by telephone and staff with faculty preceptors.
2. Pharmacy students to titrate medications and provide health education for existing chronic conditions such as diabetes, hypertension, and obstructive lung disease, staffing with faculty preceptors.
3. Nursing students to check-in and initially assess patients, provide education, answer questions, arrange follow-up, and coordinate care, with close supervision from faculty preceptors.
4. Clinical health psychology students to assist with mental health evaluation and basic psychotherapy with supervision from faculty preceptors.
5. Dental students to provide dental hygiene education and screening initially, with the goal to provide basic dental treatment as the venture becomes established.
6. Physical Therapy students to provide rehabilitation regimens and patient education with faculty preceptors, with the goal of performing home safety evaluations once the venture becomes established.
MILESTONES - INTERNAL
Hire a full-time director and part-time associate to manage the day-to-day operations and community engagement work of Aurora Health Access.Milestone Not Met. Aurora Health Access just concluded its third round of recruiting and interviewing applicants for the Executive Director position. The first two were not fruitful, with only a limited pool of applicants and on two occasions the applicant we wished to hire accepted other offers. We are extremely hopeful that the third time will be the charm. We attracted a large pool of applicants which was narrowed to three stellar candidates selected for interviews on February 19, 2014. All three candidates were as impressive in person as they were on paper. Members of the Board’s Governance Committee, which conducted interviews, were especially impressed with one candidate because of her many years of experience as an executive director of a health-care related organization in Colorado. The committee unanimously agreed to introduce her to the Board of Directors at its February 27th meeting with a recommendation that she be offered the position.
As for a part-time associate, the Board felt that the Executive Director should select the individual for this position. In the interim, the Colorado Foundation for Public Health and the Environment, on behalf of Aurora Health Access, entered into an hourly contract with an independent contractor to provide organizational and communication services. The contractor continues to provide services for Aurora Health Access.
AHA Progress Report, December 2014 Page 6
August Update: Milestone Met. Denise Denton was hired as AHA’s first Executive Director on March 1, 2014. She comes to AHA with 25 years of experience with not-for-profit start up and sustainability and working with medically underserved populations. Her bio is attached at the end of this report.
We are partnering with 2040 Partners for Health in creating a job share arrangement for our administrative and communications support position Final candidates were interviewed on August 19th, and we hope to have someone in place early in September. By partnering with 2040, who had need for a part-time administrative position, we will be able to offer a full-time position and office setting to this staff person.
December UpdateAHA finalized a contract with 2040 Partners for Health, and hired Sharon Cairns as their Coordinator of Administration and Communications in September. She will work for AHA 12/hours week from her office at 2040, which is conveniently located in Northwest Aurora near Colfax and Elmira.
Finalize a governance structure that includes a board of directors and approved articles of incorporation.Milestone Met. At a January 23, 2013 quarterly meeting attended by the many community-based organizations that provide health care and other services to underserved residents of Aurora, nineteen individuals were elected by their peers to the first Board of Directors of Aurora Health Access. Rich McLean was elected to serve as the Board chair, along with other Executive Committee Members: Mariana Ledezma (Vice Chair), Joe Sammen (Treasurer) and Mitzi Schindler (Secretary). At the same meeting, formal articles of incorporation were approved, and by-laws were adopted on March 28, 2013. The Board may have up to twenty members. Currently, the Board numbers fourteen, as three members resigned for different reasons in the past year. The Board Governance Committee is drafting a policy for filing vacancies that reflects community values. Current vacancies will be filled at an Annual Meeting on April 24, 2014.
In addition to an Executive Committee, the Board established the following committees: Governance; Events and Communication; and, Fund Development. Five Work Groups that focus on AHA’s areas of interest are also a part of the organizational structure:
- Adult Access and Care Coordination - Pediatric Access and Care Coordination- Community Health Integration (Community Health Workers)- Coverage- Community Education and Mobilization
Another milestone occurred on April 1, 2013, when Aurora Health Access signed a formal two year agreement with Colorado Foundation for Public Health and the Environment to serve as its fiscal agent. Over the past year, we have formed a close working relationship and are very appreciative of the assistance and guidance provided by CFPHE.
August Update: Even though several individuals have indicated an interest in serving on the AHA board, with 16 members currently, none of whom wished to leave the AHA Board, we decided NOT to hold new elections in 2014. The bylaws do not clearly outline the specifics of the board or officer election process, so the Governance Committee and Executive Committee
AHA Progress Report, December 2014 Page 7

have been charged to develop portions of the board recruitment and election procedures. The current officers have agreed to continue serving until new officers are elected.
Our new Executive Director, Denise Denton, was charged with reviewing and revising AHA’s workgroup structure and process. Not all workgroups have proven to be productive or timely. Guidelines were developed to more effectively create and support future workgroups. These guidelines include factors to be considered prior to forming a new workgroup such as mission match, staffing capacity, board leadership, opportunity, and timeliness. The Adult Access, Coverage, and Pediatric Workgroups will be continued. Community Health Integration and Community Education were dissolved. Based on member input and board leadership, an Oral Health Interest Group has been formed, that might evolve in to a workgroup.
December UpdateFinalizing a governance structure has proven to be more challenging than any of us expected it to be. The luxury of operating as an informal community alliance has meant that AHA has become different things to different people. Moving forward, to create a more formal structure, requires tough decisions and prioritizations to be made, and less flexibility in how AHA operates. We have been relying on Tuckman’s “Stages of Group Dynamics” to understand some of the issues we are facing. His stages of group process are forming, storming, norming, and performing. There is general agreement that our dynamic board is somewhere between the “storming” and “norming” phase. Our participation in the Colorado Network of Health Alliances has proven invaluable as we look to colleagues for best practices, organizational models, and sometimes – commiseration.
In order to improve the productivity of our board meetings, and more specifically define the expectations of board members, the Governance Committee was charged with creating Meeting Guidelines. These were approved by the Board and implemented in October, 2014.
The Governance Committee also developed a new Board Member Agreement, which outlines the expectations AHA has of its board members. With a more formal organizational structure, the expectations the AHA organization places on its governing board need to shift pretty dramatically. AHA’s current board members can use this Agreement to assess whether they are able and willing to fill this new role. The Agreement will also serve as a “job description” for recruiting future board members in a thoughtful, planned process. Attachment: AHA Board Agreement
Maintain and strengthen the communications of Aurora Health Access including the monthly newsletter, website, social media and other communications.Milestone Met. The organization’s monthly electronic newsletter is sent to over four hundred individuals. In addition to reporting on AHA activities, the newsletter incorporates announcements of health fairs and other health care events/activities that may be of interest to this constituency. A goal is to update the AHA website (www.aurorahealthaccess.org) and we anticipate this may be accomplished by summer 2014.
August Update: We have improved the content and look of the newsletter and added a section to the website where past editions are uploaded. We added a section to the newsletter called, “Partner Spotlight” where we highlight the activities and accomplishments of various community partners.
December Update
AHA Progress Report, December 2014 Page 8
Our recent monthly newsletters have included Partner Spotlights on the Asian Pacific Development Center, Innovage PACE, and Aurora Community Partners. We have also created a newsletter archive on the website.
Thanks to having brought Sharon Cairns on board as AHA’s Administrative and Communications Coordinator, our plan is to make our Facebook presence much more dynamic. We will increase postings that direct members to our website and those of our community partners.
We have decided not to try and expand the use of Twitter, and instead focus on our website and Facebook for outreach and promotion. Several inquiries of our membership revealed that Twitter is simply not often used for this purpose.
Hold an annual community meeting with the goal to stay connected to and lead by the needs of the residents of Aurora. Milestone Not Met. In 2013, an annual community meeting was held in January. Absent an Executive Director and the expectation that this position would be filled early in 2014, a conscious decision was made to schedule the annual meeting for April 16, 2014 in conjunction with a quarterly meeting. In addition to promoting the event in the AHA newsletter, media releases will be sent to outlets that reach our community, including Spanish language media.
August Update: Milestone Met. AHA held its annual community meeting on April 16, 2014. The meeting was attended by forty-seven members. We assessed the number of individuals who live in Aurora – only 10, and the number who work in health and human services – 42. AHA will continue to track these characteristics to assess membership and outreach. The members we asked to identify health issues which should be considered by the AHA board for effort and involvement, then to vote for priority issues. The priority issues identified included: Health Equity Mental/Behavioral Health Wellness and Preventative Care Immigrant Health GLBTQ Community Health Advocacy Senior Care Education and Outreach Oral HealthThe board will consider this member input, along with AHA capacity, in determining future areas of growth.
December UpdateThe next Annual Community Meeting is scheduled for April 2015.
Convene the Board no less than 10 times per year and all members of Aurora Health Access quarterly.Milestone Met. The AHA Board has had ten meetings since the grant agreement of March 1, 2013. Meetings were held on the fourth Wednesday of each month, except in November because of the Thanksgiving holiday, and December when the Board met on the 19 th. Quarterly meetings were held on May 29, 2013, July 17, 2013, October 16, 2013 and January 15, 2014. The primary presentation at these meetings covered Bridges to Care (May), an Assessment Overview and Connect for Health (July), an Overview of the Aurora Assistance
AHA Progress Report, December 2014 Page 9
Network and CHW Project (October) and a facilitated Connect for Health Brainstorming Session (January).
August Update: The AHA Board continues to meet monthly, and with the energy and capacity brought by the new Executive Director, the Executive Committee has also been meeting monthly to provide guidance and direction.Quarterly meetings were held April 16, and July 16.
December UpdateBoard meetings were held each month and minutes provided for all meetings. Board materials are available upon request.
The Quarterly Community Meeting was held on October 15, hosted by the Asian Pacific Development Center. It was attended by 54 members. During the meeting, AHA board members facilitated a small group activity to ask members to answer three questions: 1) What word describes AHA? 2) What does AHA do well? 3) What could AHA do better? The responses were compiled, and will be used to continue to strengthen our structure and capacity. Attachment: Quarterly Community Meeting Agenda.
MILESTONES - EXTERNAL
Maintain and strengthen the partner relationships and community connections of Aurora Health Access, as demonstrated by the number of people connected to the work of Aurora Health Access and through new or strengthened strategic community relations.Milestone Met. The primary way AHA tracks its community outreach and connections, is through the number of contacts in the database. As of this March 2014 Aurora Health Access has 441 individual contacts. These individuals represent health providers, insurers, interested residents and at least forty community-based organizations serving residents of Aurora.
August Update: AHA is systematically cleaning up its Constant Contact database. We consider a “member” to be anyone who participates in AHA activities and asks to be placed on our membership roster. We recently removed 58 “inactive” members from our database, but through outreach efforts, we still have 488 members. We are using the database in a more robust way, tracking how members participate and when their contact information was last updated. We are also tracking the source of new members. We want to assess various recruitment efforts and the assistance of board members in community outreach.
AHA has also started tracking the number of participants attending the Quarterly Community Meetings as a gauge of partner relationships and community connections. There were 41 participants at the April meeting, and 47 at the July meeting.
December UpdateIn November, AHA’s membership was up to 526; a 9% increase in 3 months. This is a reasonable increase given that we limit ourselves to adding individuals only with their agreement. We are hoping to see similar increases each month moving into the next year. The Board Member agreement includes the expectation that board members recruit at least ten new members each year. The number of participant in the October Quarterly meeting was 54, which shows a steady increase in participation this year.
AHA Progress Report, December 2014 Page 10
In order strengthen community connections – and promote health stakeholders in Aurora – we have decided to move our Quarterly Community Meetings to various locations. Health agencies are asked to host each meeting. We provide the hosts with time on the agenda to talk about their program, and the option of offering a tour of their facilities to the meeting participants. The October meeting was hosted by the Asian Pacific Development Corporation. The January meeting will be hosted by The Medical Center of Aurora.
Identify gaps and opportunities for new efforts to improve access to health in Aurora, create opportunities for networking and provider leadership and momentum to efforts in the community when needed. Milestones Met. As mentioned above, Aurora Health Access has developed five workgroups that correspond with these key health initiatives. Each of the groups meets periodically to organize themselves and plan ongoing work. As a group, our Board of Directors works constantly to identify gaps and opportunities for new efforts in the community. Some highlights of this work include:
- Grant to Coordinate and Deploy Community Health Workers in North Aurora.In 2013, AHA received a grant from the Office of Health Equity (formerly known as Office of Health Disparities) that allowed AHA to coordinate and deploy Community Health Workers to patients at-risk for cardiovascular disease and their families in North Aurora. Community-based CHWs were paired with clinic-based Patient Navigators (PNs). This model enhanced the transitions across health care settings and community settings. PNs and CHWs have demonstrated improved outcomes for the medically underserved populations by bridging health care systems with communities, providing culturally appropriate and accessible health education, and providing informal counseling.
- Bridges to Care.Background relationship building and ongoing participation in the Center for Medicare and Medicaid Innovation "Hot Spotters" grant to Rutgers University which includes a local project led by Metro Community Provider Network and Together Colorado called Bridges to Care (B2C). Bridges to Care is not just a clinical intervention, but also community collaboration. The model takes place in the patient's home and involves key partners: Aurora Mental Health, University Hospital, Together Colorado, and Aurora Health Access. B2C’s primary goals are decreased hospital utilization, demonstrated cost savings, and linking patients into an MCPN medical home for ongoing care, support, and resources. B2C is working to improve health with a sustainable model so the patient receives the right care, at the right place, at the right time.
- Triage Project.We were able to build new momentum and support for the Triage Project, which wraps case management and behavioral health services around the highest utilizers of the EMS and ambulatory system in Aurora.
- KidsWell Project.As discussed earlier, the City of Aurora has partnered with AHA to develop a business plan to develop the KidsWell project for outreach to families with children eligible but not enrolled in Medicaid or CHP+. . This is the first time that the City of Aurora has been involved in developing and implementing strategies for reaching targeted populations in new and creative ways and helping them overcome barriers to enrollment.
AHA Progress Report, December 2014 Page 11
- Campus-Community Partnership.AHA is a part of an active collaboration with all five of the health professional schools on the Anschutz Medical Campus as part of the new Campus-Community Partnership effort funded by the Chancellor.
- Other initiatives to expand health access in Aurora that AHA will continue to support include:
MCPN clinic expansion and walk-in hours in north Aurora. The School of Medicine student-run free clinic initiative. University Hospital’s Community Health Needs Assessment Implementation Plan
that identified access to care as a major health need in the community. Two members of AHA serve on the Implementation team.
One of the ways AHA provides leadership and momentum is through sharing of health data.
- Community Health Assessments in Northwest Aurora. In the spring of 2013, AHA was able to arrange for public health students enrolled in a Community Health Assessment course at the Colorado School of Public Health to conduct a health assessment that focused on the Northwest Aurora community. This assessment was created for Aurora Health Access (AHA) and featured three components: Understanding Existing Data, Adult Healthcare Access, and Forces of Change
The first component, Understanding Existing Data, involved synthesizing, comparing, and congregating data from numerous existing assessments to provide AHA with a consolidation of evidence-based research to aid in identifying priority health concerns in this community.
The second component, Adult Healthcare Access, identified factors and barriers experienced by adults in this community that are associated with access to healthcare and a comprehensive resource directory of healthcare services available in Northwest Aurora was created. The discovery that improved access must take into consideration the locations and timing of services, organization of care, and linguistically and culturally sensitive staff and services informed development of the directory.
The third component, Forces of Change, investigated themes and strengths in assuring a healthy Northwest Aurora through primary and secondary data collection, and the analysis and synthesis of resulting data. This work has been helpful to AHA as we move forward in our work.
The three components were woven together by a Master’s of Public Health Capstone project in the summer of 2013 that synthesized the assessments and suggested strategies for impacting Aurora health care in the future.
With continued AHA sponsorship, the new Community Health Assessment class will study two more topics during the first semester of 2014:
Strategies for expanding specialty care access in Aurora Assessment of the initial Affordable Care Act impact on Aurora in 2014
In addition, our monthly Board meetings, Quarterly Community meetings, and our monthly e-newsletter all serve as avenues for networking and leadership development in our key work areas.
AHA Progress Report, December 2014 Page 12
August Update: All the activities described above are active and ongoing within the organizations that assumed the lead in carrying them out after AHA served as a convener and encourager to get them started. During Workgroup meetings, representatives from the lead organizations continue to provide updates and to request support or advice as needed. Additionally, AHA has identified new opportunities to encourage networking and leadership.
It is challenging to acquire data specific to Aurora. AHA has developed a new page on its website titled, “Data Sources, Resource Lists, and Reports, which will help address this challenge. This resource page will include information about and links to health-related data specific to the city of Aurora. We are working with the State Demographer’s Office and the Colorado Health Institute to populate this section. The Resource List section will include compendiums of health and human service resources available to residents of Aurora. AHA will negotiate MOA’s with the developers of the list to assure timeliness and updates. The reports section will include uploads or links to reports generated on AHA’s behalf by the Colorado School of Public Health and other needs assessment reports specific to Aurora.
AHA is convening a gathering called Community Health Engagement Group (CHNG). This group includes organizations involved in providing community-based service and research opportunities for healthcare students. It will also involve programs that explore undergraduate students to health career opportunities. The participants of CHNG include 2040 Partners for Health, Fields Foundation, Primary Care Progress, Community Campus Partnership, Metro Community Providers Network, Student-Run Free Clinic, Denver Health – Health Care Interest Program, School of Nursing, School of Med, etc.
The two new assessments by CSPH students were completed, presented to AHA membership during the April Quarterly meeting, and posted to the AHA website. AHA staff is working with the current class to design a new project which will examine health disparities in all 17 of Aurora’s zip codes.
December UpdateThe next Community Assessment Class project is titled, “Understanding Health Equity in Aurora.” The goal of the project is “to identify the health issues and priorities related to the City of Aurora as a whole, in order to guide the directions of AHA.” The students will conduct a modified community health assessment for the City of Aurora, define the community sociodemographics, and list the top ten causes of morbidity and mortality. The project includes two deliverables:
1. Presentation summarizing a modified community health assessment of the City of Aurora and results of a comparison to Original Aurora assessments delivered to the AHA steering committee and interested community members. This was completed on November 12 th.
2. Executive summary and final report discussing the findings and recommendations of the modified health assessment and group methods- December 12.
AHA is an active participant in the University of Colorado Hospital’s (UCH) Health Care Needs Assessment Implementation Steering Committee. The Committee recommended that UCH fund stronger Emergency Department case management and collaboration with community primary care. Simultaneous with this recommendation, Dr. Roberta Capp (also a member of the CHNA Implementation Steering Committee) initiated a research project (Hotspotters) to analyze how the social determinants of health and barriers to accessing care in the community can lead to emergency department utilization. The results underscore the need for programs to strengthen
AHA Progress Report, December 2014 Page 13
community primary care such as recommended by the UCH CHNA Steering Committee and to enhance education for future health care providers. AHA has posted a presentation of this study on its website.
Provide evidence of the impact of Aurora Health Access’ work on the Aurora community through documentation of ANY of the following: 1. Behavioral changes in the community (individuals or partner agencies).2. Increased engagement in health issues by targeted audiences.3. Any specific organizational, local, regional, state policy or practice changes to which
Aurora Health Access contributed.Milestone Not Met. As organized currently, we are an all-volunteer Board of Directors doing the work to meet our goals as an “add-on” to our professional lives. Over the past six months, we’ve work diligently to develop governance structures for the organization and have attempted to find an Executive Director. We haven’t had the capacity to develop sophisticated evaluation tools to measure our influence in complex ways. It is our intention that our new Executive Director, once identified, will help lead the organization in these efforts.
August Update: Denise Denton is meeting with AHA’s Project Officer on September 4th to explore possible evaluation techniques. The Colorado Network of Health Alliances, of which AHA is a founding member, is exploring tools that can help track and assess the impact of community-based networks. These tools should prove useful to AHA.
December UpdateMilestone Met. While AHA can’t claim to be responsible for behavioral changes in the community, we can track increased engagement in health issues by targeted audiences and specific policy or practice changes to which we have contributed.
One of the AHA’s target audiences was the oral health community. Through the Oral Health Convening, we created an Oral Health Interest Group, added twelve key stakeholder agencies to our membership base, and are enhancing our webpage to include information on oral health advocacy, services, and coverage resources.
AHA targeted increase participation of students – tomorrow’s health care providers. We targeted students not only to diversify of our membership with young people, but to encourage students to work with and within the Aurora community during their training. This experience not only offers invaluable health care resources to the community, but hopefully instills in tomorrow’s providers a better understanding of Aurora’s different cultures, ethnicities, and needs. While AHA has been working with students at the Colorado School of Public for the past two years, by hosting the new Community Health Engagement Group (CHeNG) and supporting the new Student Run Free Clinic, we have engaged new students from many disciplines in AHA efforts.
AHA is reaching out to Aurora’s small business community through the Lunch and Learn workshop held in October, membership the Aurora Chamber of Commerce, and our Executive Director’s participation in Leadership Aurora. This has resulted in several new members particularly in the insurance and banking industries.
We have identified seniors as one our next target audiences. We are convening representatives from organizations serving seniors into an Interest Group, and plan to host an Educational Forum in April 2015, which will focus on Aurora’s senior population – their health needs and the resources available to meet them.
AHA Progress Report, December 2014 Page 14

A small, but important policy change that AHA contributed to is on the application form for the purchase of health insurance. Previously, when shopping for health insurance through the Exchange, an applicant could acknowledge the insurance broker/agent OR health guide who helped them through the process. This documentation is necessary for brokers and agents to earn their commission; health guides and their agencies used this tracking to verify their efforts and justify their grant funding. Because there was room on the form for only one tracking number, this competition resulted in “turfism” and resentment among some health guides and the private sector. AHA, through our Coverage Workgroup and our collaboration with Aurora Community Assistance Network used multiple avenues to work with the Exchange and change the intake form. This has resulted in increased collaboration among Aurora’s health guides and the private insurance carriers.
AHA has been a strong advocate for strengthening the City of Aurora’s healthy community efforts. The City Council recently embraced the “Let’s Move” program, which will enhance Aurora’s parks, trails, and recreation programs and activities.
AHA, primarily through the efforts of our Chair, Rich McLean, has been helping lay the groundwork for the creation of a new Mental Health Wellness Court, which will develop programs to help address the mental health issues that put the same Aurora residents frequently before the judicial system. Rich has been tireless in building collaboration between the judicial system and the health and human service organizations throughout Aurora.
C. Describe the method used to track and calculate these results.Aurora Health Access continually keeps track of the direct outcomes that occur as a result of programs that have been lead or catalyzed by the organization. We also pay close attention to key health indicators pertaining to Aurora from various data sources, including the Colorado Health Access Survey, the American Community Survey, and Kids Count.
August Update: While AHA will continue to rely on these data sources, we are working with several entities to identify methodologies for tracking and documenting AHA’s contribution to “moving the needle.” These entities include the evaluation staff at the Colorado Health Foundation, the Colorado School of Public Health, and the Colorado Network of Health Alliances. AHA needs to be able to demonstrate value in order to assure our sustainability.
December Update: AHA continues to refine our membership data base in order to better track community engagement. We measure increased community engagement by tracking the number of active members and participation at AHA-hosted events.
The Colorado School of Public Health students continue to provide valuable information about health status and demographics in Aurora, although since this has only been happening for a little over two years, it is difficult to gauge dramatic changes.
To track health insurance coverage, AHA relies on our partner organization, Aurora Community Assistance Network. The results for the last enrollment period showed that a total of 4,380 individuals were “engaged” or served by health guides in Aurora, 733 individuals were signed up for Medicaid, and 226 purchased insurance through the Exchange.
AHA Progress Report, December 2014 Page 15
ATTACHMENTS
A. Communications Tracking
B. Oral Health Convening Participant List
C. Attachment: Workshop Evaluation Summary
D. Attachment: AHA Board Agreement
E. Attachment: Quarterly Community Meeting Agenda
AHA Progress Report, December 2014 Page 16
COMMUNICATION TRACKING 2014
Month
SourceApri
lMay
June
July
August
September
October
November
December
NEWSLETTER
Sent 418 45146
4 488 497 504 526
Opened 128 13714
5 151 130 166 162 Open Rate % 31 31 33 35 25 35.4 33.1
Bounces 11 15 27 29 32 35 36 FACEBOOK
New Page Likes 9 1 1 1 0 22 Total Page Likes 94 95 96 97 97 119 Pages We Like 62 64 64 68 68 68
Total Posts 9 4 10 10 13 18 TWITTER
New Followers 3 16 9 10
Total Followers 459 46247
8 487 497
Following 167 10810
8 108 109
Attachment B. Oral Health Convening Participant List
Oral Health Access in Arapahoe County Planning Group
September 24, 2014 Meeting | 1:00 to 3:00 p.m.
INVITED PARTICIPANTSUpdated 10/23/14
First Name Last Name Organization Attendee E-‐mail
Sharon Adams ClinicNet [email protected]
Rita Beam Tri-‐County Health Department [email protected]
Marcy Bonnett CDPHE - ‐ Cavity Free at Three [email protected]
Patty Boyd Tri-‐County Health Department [email protected]
Diane Brunson CU School of Dental Medicine [email protected]
Deidre Callanan Colorado Association for School-‐Based Health Care [email protected]
Julie Collett Kids in Need of Dentistry (KIND) [email protected]
Denise Denton Aurora Health Access (AHA) [email protected]
Lynn Doan Colorado Consumer Health Initiative (CCHI) [email protected]
Joan Eskens Tri-‐County Health Department [email protected]
Deb Foote Oral Health Colorado [email protected]
Anne Gibbs CDPHE - ‐ Cavity Free at Three [email protected]
Gretchen Hammer Colorado Coalition for the Medically Underserved (CCMU) [email protected]
Jan Jenkins Refugee Wellness Center [email protected]
Bebe Kleinman Doctors Care [email protected]
Michelle Kohler Community College of Denver -‐ Dental Hygiene Program [email protected]
Alison Lawrence CDPHE - ‐ Cavity Free at Three [email protected]
Jason Mauterer Denver Metro Dental Society [email protected]
Francoise Mbabzi Oral Health Colorado [email protected]
Rich McLean St. Therese FAMILY / Together Colorado [email protected]
Laura Poole Asian Pacific Development Center [email protected]
Callie Preheim Aurora Health Access (AHA) [email protected]
Valerie Purser South Metro Health Alliance [email protected]
Gail Reeder Health Care Policy and Financing [email protected]
Joe Sammen Colorado Coalition for the Medically Underserved (CCMU) [email protected]
Sally Walker Kids in Need of Dentistry (KIND) [email protected]
Maya Wheeler Aurora Health Access (AHA) [email protected]
Dennis Wilken Metro Community Provider Network [email protected]
Beth Wyatt CDPHE - ‐ Cavity Free at Three [email protected]
AHA Progress Report, December 2014 Page 17
Attachment C. Workshop Evaluation Summary
ACA Lunch and Learn Workshop – October 22, 2014
Evaluation Summary
Background: On October 22, 2014, Aurora Health Access (AHA) organized a “lunch and learn” workshop entitled, “Your Bottom Line: What the Affordable Care Act Means for Your Colorado Small Business.” Our host was the Aurora Chamber of Commerce; our co-sponsor was the Aurora Community Assistance Network (ACAN); and l our presenter was Tim Gaudette, from the Small Business Majority. We were limited to 40 participants; 42 were there. The workshop was held from 11:30 to 1:00 in the Chamber’s community meeting room. AHA provided box lunches for the participants. There was no fee to attend, but we did ask that participants pre-register.
While we had over 40 participants, we got back evaluations from only 24 of them.
Q1. BEFORE the event, how would you describe your feelings about the Affordable Care Act?Strongly Support – 6 Support – 6 Neutral – 5 Against – 2 Strongly Against - 1
Q2. AFTER the event, how would you describe your feelings about the Affordable Care Act?Strongly Support – 8 Support – 11 Neutral – 3 Against – 1 Strongly Against - 0
Q3. How well was the information presented today to address your questions and concerns about federal health care reforms?
Extremely Well - 19 Somewhat well - 5 Not at all - 0
Q4. If you're not currently offering health insurance to your employees, how did the information presented today affect your thinking on the topic? Less likely to offer – 1 No change – 6 More likely to offer - 6
Q5. What do you think are the most important issues facing the small business community? (Select all that apply)15 - Rising cost of healthcare 5 - Rising material and supply cost 1 - Lack of demand 3 - Government regulation 6 - Competition from big corporations 5 - I am not a small business owner
Q6. As a small business owner, where do you get most of your information? (Select most applicable) 2 - Friends and family 6 - Accountant/financial advisor/CPA 8 - Industry peers/trade organization 1 - Television 4 - Internet 2 - Other – Brokers, CO Nonprofit Association 8 - I am not a small business owner
AHA Progress Report, December 2014 Page 18
Q7. For healthcare issues, where do you get most of your information? (Select most applicable) 5 - Friends and family 3 - Accountant/financial advisor/CPA 0 - Industry peers/trade organization 7 - Television 2 - Internet 5 - Insurance companies 7 - Insurance brokers 2 - Other – Kaiser, nurse practitioner, CO Nonprofit Assoc. 7 - I am not a small business owner
Q8. Would you like to get more involved with Small Business Majority? 5 - I'd like to speak to media regarding important small business issues 5 - I'd like to sign up for your newsletter/be made aware of future events 2 - I'd like to write letter to the editor or op-eds 3 - I'd like to join SBM's Network Council nationally or in my state 17 - I'm not interested at this time
AHA Progress Report, December 2014 Page 19
Attachment D. AHA Board Agreement
AHA Board Member Agreement
I ____________ ________________ understand that as a member of the Board of Directors of Aurora Health Access (AHA), I have an ethical responsibility to ensure that the organization does the best work possible in pursuit of its mission and goals. I believe in the mission of the organization, and I will act responsibly and prudently on its behalf.
As a Board Member of Aurora Health Access (AHA), I agree that:
Before agreeing to serve on the AHA Board, I have reviewed the expectations of AHA Board Members, assessed my availability and my commitment to the AHA mission and goals, and agree to devote the time, effort, and energy expected from its Board Members to help AHA achieve its mission.
Mission: Collaboratively improve access to care and create a healthier Aurora.
Active Participation While AHA hasn’t set a specific number of meetings I am expected to attend, I understand that I am
expected to be an active participant in AHA Board, Committee, and Workgroup meetings to which I am assigned.
When I cannot attend a meeting, I will notify the Executive Director or Chair, in advance if possible.
Participation on AHA’s Board is estimated to involve approximately 6-8 hours/month including board meetings, committee/work group service, meeting preparation, participation in community meetings, and serving as an ambassador for the organization.
When feasible, staff will arrange for meeting participation via conference call, however, I understand that in-person participation is preferred.
I understand that a majority of AHA meetings are scheduled during the day on weekdays.
I will serve actively on at least one AHA Workgroup and/or one Board Committee.
I will stay informed about what is going on in AHA and enhance AHA’s knowledge base by sharing relevant information with Board and staff.
I will be mindful that my behavior and participation in AHA meetings contributes to their effectiveness and productivity.
I will act and vote in the best interests of AHA in Board and Committee decision-making.
I will honor AHA Meeting Guidelines and other principles of practice developed to assure an effective board and successful organization.
Community Engagement and Representation
AHA Progress Report, December 2014 Page 20
I will actively promote AHA to the public to increase community and organizational awareness and engagement.
I will refer at least 10 individuals each year to AHA staff for follow-up.
When asked to represent AHA, I will be conscientious about the separation between my personal views, and those discussed and agreed upon by the AHA Board.
Fiduciary and Governance Responsibilities I will strictly adhere to AHA’s Conflict of Interest Policies, and excuse myself from any discussions or
activities where I have a real or perceived conflict of interest.
I will review, be familiar with, and abide by AHA’s bylaws and governance policies and guidelines, and I will raise the issue if I see we are not following these agreements.
When and if asked, I will make an annual personal financial contribution to AHA that is meaningful to me.
Commitment to Board Member Agreement I understand that if I do not adhere to this Agreement, a member of the Executive Committee will
contact me to discuss my ongoing participation on the AHA Board, and that my inability or unwillingness to meet the expectations outlined in this Agreement can be cause for removal from the AHA Board.
Approved by the AHA Board of Directors September 25, 2014
______________________________________________________________________________SIGNATURE DATE
PRINTED NAME AND TITLE
AHA Progress Report, December 2014 Page 21
E. Attachment: Quarterly Community Meeting Agenda
AHA Quarterly Community MeetingWednesday October 15, 2014
2:00 TO 4:30Asian Pacific Development Center
AGENDA
Settling In, Networking, Welcome: Rich McLean, Chair AHA Welcome from Rich; AHA board members and staff introductions.
Student Run Free Clinic: Joseph Johnson and Tom Clagget Primary Care Progress has been working diligently many partners to open a student-run
free clinic to help serve Aurora’s uninsured at the Dayton Opportunity Center. Well, it’s going to happen. You’ll hear the details!
Introductions: Denise Denton, Exec. Director AHA A chance for each participant to introduce themselves.
Announcements, Inquiries, and Information Sharing Your opportunity to make a brief announcement, ask for assistance or input, or share
information. Take advantage of our resource table to display your materials.
Host: Asian Pacific Development Center: Laura Poole, APDC An overview of APDC – what they do and for whom.
AHA Activities Update and Member Input: Denise An update about what AHA has been up to including the new vision, mission, and goals
just adopted by the Board, and a chance for AHA members to provide input on AHA strategies and direction.
Bridges to Care Project: Eliana Mastrangelo, Together CO and Heather Logan, MCPN The Bridges to Care program is a CMMI funded community intervention taking place in
Aurora that focuses on high hospital utilizers. The goal of the program is to link patients to appropriate care, decrease hospital utilization, and lower costs.
Triage Project: Heather Dolan Jackson, AuMHC The Aurora Triage Project is a joint project between Aurora Mental Health Center and
Arapahoe House to reduce the on-site interventions by EMS, Fire and Aurora Police Department for frequent utilizers of making 911 calls for non-emergency related causes (as identified by the project team which includes EMS, AFD, APD, AuMHC and AH).
Meeting Adjourns: Rich Next Quarterly Membership meeting – January 21, 2014 2:00 to 4:30 Suggestions for a meeting place?
Networking/ Tour of APDC
AHA Progress Report, December 2014 Page 22