Embed Size (px)
Citation preview
Appendix A. Occupational Exposures and Pregnancy
Table of ContentsForeword................................................................................................................................................... 2
Physical Agents……………………………………………………………………………………………………………………………………..3
Ionizing Radiation..................................................................................................................................3
Non-Ionizing Radiation..........................................................................................................................5
Temperature..........................................................................................................................................6
Noise and Vibration............................................................................................................................... 7
Chemicals.................................................................................................................................................. 9
Solvents................................................................................................................................................. 9
Plastics, Epoxies, and Resins................................................................................................................11
Formaldehyde......................................................................................................................................13
Chemotherapy drugs........................................................................................................................... 15
Anesthetic Gases................................................................................................................................. 16
Carbon Monoxide and Other Combustion Byproducts........................................................................18
Pesticides............................................................................................................................................. 19
Polychlorinated Biphenyls (PCBs)........................................................................................................20
Metals......................................................................................................................................................21
Lead..................................................................................................................................................... 21
Mercury............................................................................................................................................... 23
Cadmium............................................................................................................................................. 24
Cobalt.................................................................................................................................................. 25
Biological/Infectious Agents....................................................................................................................26
Other workplace factors..........................................................................................................................29
Shift Work and Long Working Hours....................................................................................................29
High physical demands........................................................................................................................30
References Cited………………………………………………………………………………………………………………………………….32
Website urls checked 2/26/2016
1

Appendix A. Occupational Exposures and Pregnancy
Foreword
All workers have the right to safe working conditions.
Regulations and guidance for workers concerned about their reproductive health have not kept pace
with the large number of potential reproductive hazards in workplaces.
Accurate information about occupational reproductive risks and workplace options are important
first steps to good reproductive health for both women and men. Workplace reproductive hazards
are relevant to preconceptional planning, pregnancy, and breastfeeding.
Workplace hazards should be eliminated or reduced to provide a safe working environment for
workers. Where this is not feasible, use of personal protective equipment (PPE), including
respirators, may be an option—but not all PPE can be used effectively during pregnancy. If neither
hazard elimination nor PPE are feasible, a worker may wish to consider avoiding hazardous duties
preconceptionally or during pregnancy or breastfeeding, depending on the hazard.
Appendices A and B provide information to share with patients who are pregnant, breastfeeding,
or planning a pregnancy. Information can also be found on our web pages:
http://www.cdc.gov/niosh/topics/repro/pregnancy.html. For assistance with specific questions
about occupational reproductive hazards, reproductive health, and many other health topics, CDC-
INFO may be able to help (https://wwwn.cdc.gov/dcs/ContactUs/Form; Phone 800-CDC-INFO
(800-232-4636) ).
Workplaces vary greatly. Informed discussion between a working patient and her health provider
can begin to determine the best actions for her situation. Speaking with the patient’s employer about
safer alternatives may also be useful.
2
Appendix A. Occupational Exposures and Pregnancy
Physical Agents
Ionizing Radiation
Potential Fetal/Maternal Complications Jobs where Exposures are Found
Recognized reproductive toxicant1
Effects include fertility problems, miscarriage,
certain birth defects (depending on timing and
dose)2-4
Healthcare/veterinary workers
Flight crew members
Certain industrial/laboratory applications
Tools and Prevention Strategies
Ionizing radiation is radiation with enough energy to remove tightly bound electrons from the orbit
of an atom, causing the atom to become charged or ionized.
Ionizing radiation exposure is well-regulated and guidelines are in place in most US workplaces.
Pregnant workers need to be aware of these guidelines and follow them closely. The best first step is
for employees to talk to their supervisor and their workplace Radiation Safety Officer.
o If a Radiation Safety Officer is not available, consult with your state’s department of radiation
protection.
Certain workplace radiation exposures may incur a higher level of risk during pregnancy, including:
o caring for patients who have been administered nuclear medicine radioactive materials,
especially Iodine-131
o portable x-ray machines
o fluoroscopy procedures.
Flight attendants and pilots are exposed to cosmic ionizing radiation at levels which may be of
concern for crewmembers during pregnancy. More information and suggestions for managing
cosmic radiation exposures are at the NIOSH website
(http://www.cdc.gov/niosh/topics/aircrew/cosmicionizingradiation.html) or CDC-INFO for more
3

Appendix A. Occupational Exposures and Pregnancy
information.
4
Appendix A. Occupational Exposures and Pregnancy
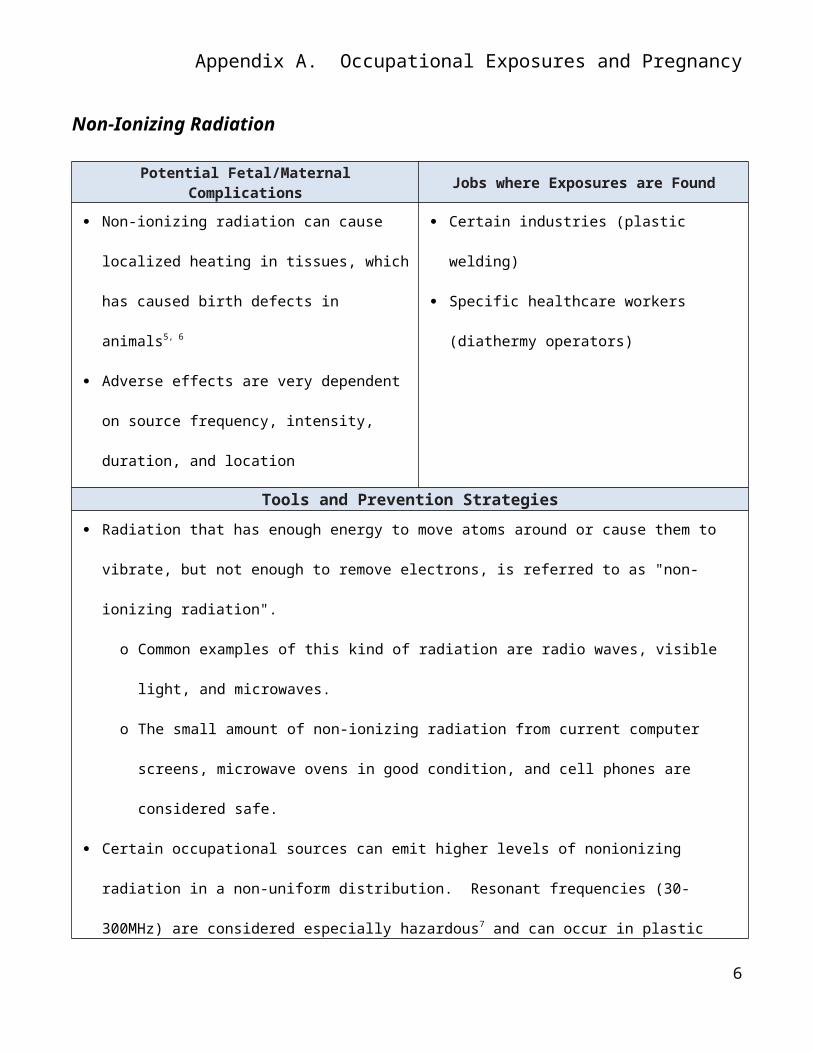
Non-Ionizing Radiation
Potential Fetal/Maternal Complications Jobs where Exposures are Found
Non-ionizing radiation can cause localized
heating in tissues, which has caused birth defects
in animals5, 6
Adverse effects are very dependent on source
frequency, intensity, duration, and location
Certain industries (plastic welding)
Specific healthcare workers (diathermy
operators)
Tools and Prevention Strategies
Radiation that has enough energy to move atoms around or cause them to vibrate, but not enough to
remove electrons, is referred to as "non-ionizing radiation".
o Common examples of this kind of radiation are radio waves, visible light, and microwaves.
o The small amount of non-ionizing radiation from current computer screens, microwave ovens in
good condition, and cell phones are considered safe.
Certain occupational sources can emit higher levels of nonionizing radiation in a non-uniform
distribution. Resonant frequencies (30-300MHz) are considered especially hazardous7 and can occur
in plastic welding, diathermy, and other jobs.
Because information on frequency, intensity, and location are necessary to estimate exposure,
consultation with a Safety Officer is recommended.
5
Appendix A. Occupational Exposures and Pregnancy
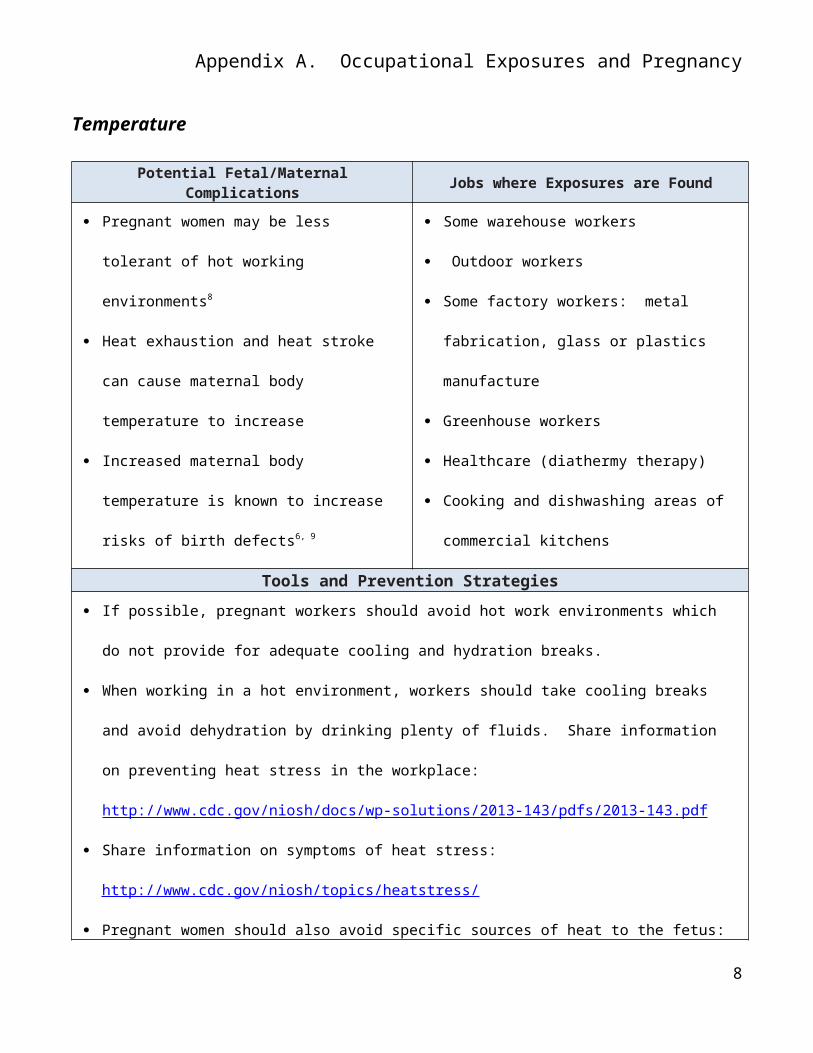
Temperature
Potential Fetal/Maternal Complications Jobs where Exposures are Found
Pregnant women may be less tolerant of hot
working environments8
Heat exhaustion and heat stroke can cause
maternal body temperature to increase
Increased maternal body temperature is known
to increase risks of birth defects6, 9
Some warehouse workers
Outdoor workers
Some factory workers: metal fabrication, glass
or plastics manufacture
Greenhouse workers
Healthcare (diathermy therapy)
Cooking and dishwashing areas of commercial
kitchens
Tools and Prevention Strategies
If possible, pregnant workers should avoid hot work environments which do not provide for adequate
cooling and hydration breaks.
When working in a hot environment, workers should take cooling breaks and avoid dehydration by
drinking plenty of fluids. Share information on preventing heat stress in the workplace:
http://www.cdc.gov/niosh/docs/wp-solutions/2013-143/pdfs/2013-143.pdf
Share information on symptoms of heat stress: http://www.cdc.gov/niosh/topics/heatstress/
Pregnant women should also avoid specific sources of heat to the fetus: very hot/prolonged saunas,
hot tubs,10 and diathermy treatments.6
6

Appendix A. Occupational Exposures and Pregnancy
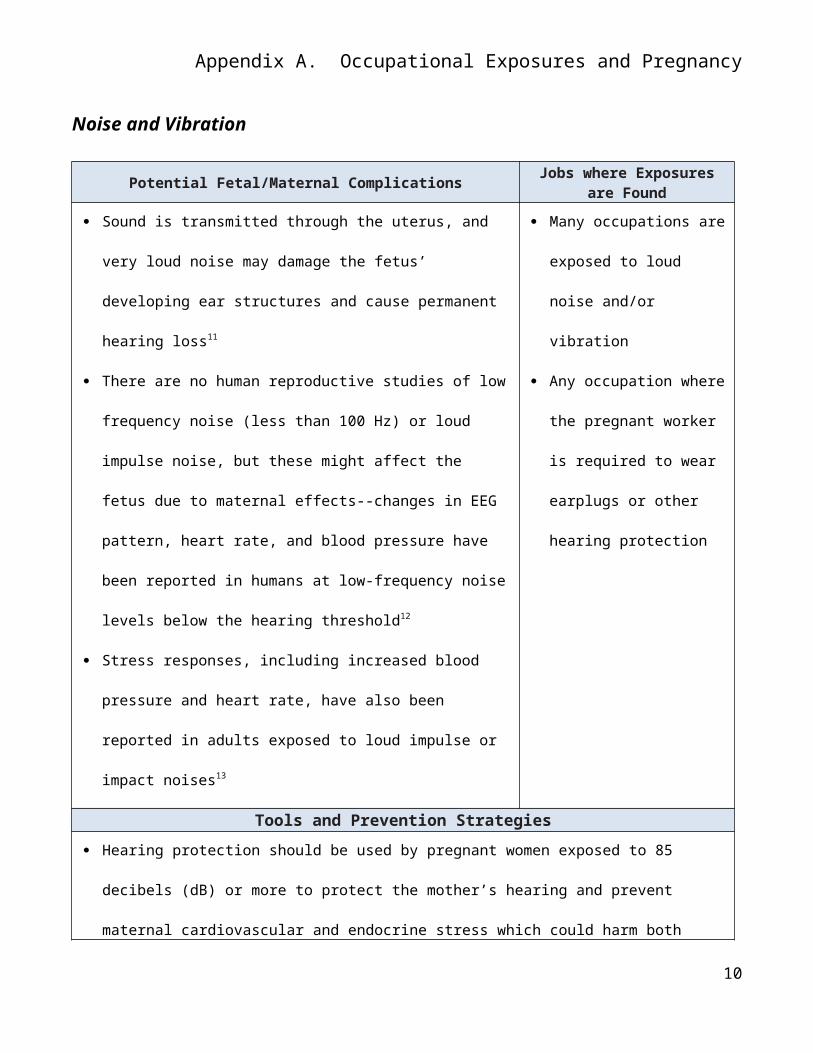
Noise and Vibration
Potential Fetal/Maternal ComplicationsJobs where Exposures are
Found
Sound is transmitted through the uterus, and very loud noise may
damage the fetus’ developing ear structures and cause
permanent hearing loss11
There are no human reproductive studies of low frequency noise
(less than 100 Hz) or loud impulse noise, but these might affect
the fetus due to maternal effects--changes in EEG pattern, heart
rate, and blood pressure have been reported in humans at low-
frequency noise levels below the hearing threshold12
Stress responses, including increased blood pressure and heart
rate, have also been reported in adults exposed to loud impulse
or impact noises13
Many occupations are
exposed to loud noise
and/or vibration
Any occupation where the
pregnant worker is required
to wear earplugs or other
hearing protection
Tools and Prevention Strategies
Hearing protection should be used by pregnant women exposed to 85 decibels (dB) or more to
protect the mother’s hearing and prevent maternal cardiovascular and endocrine stress which could
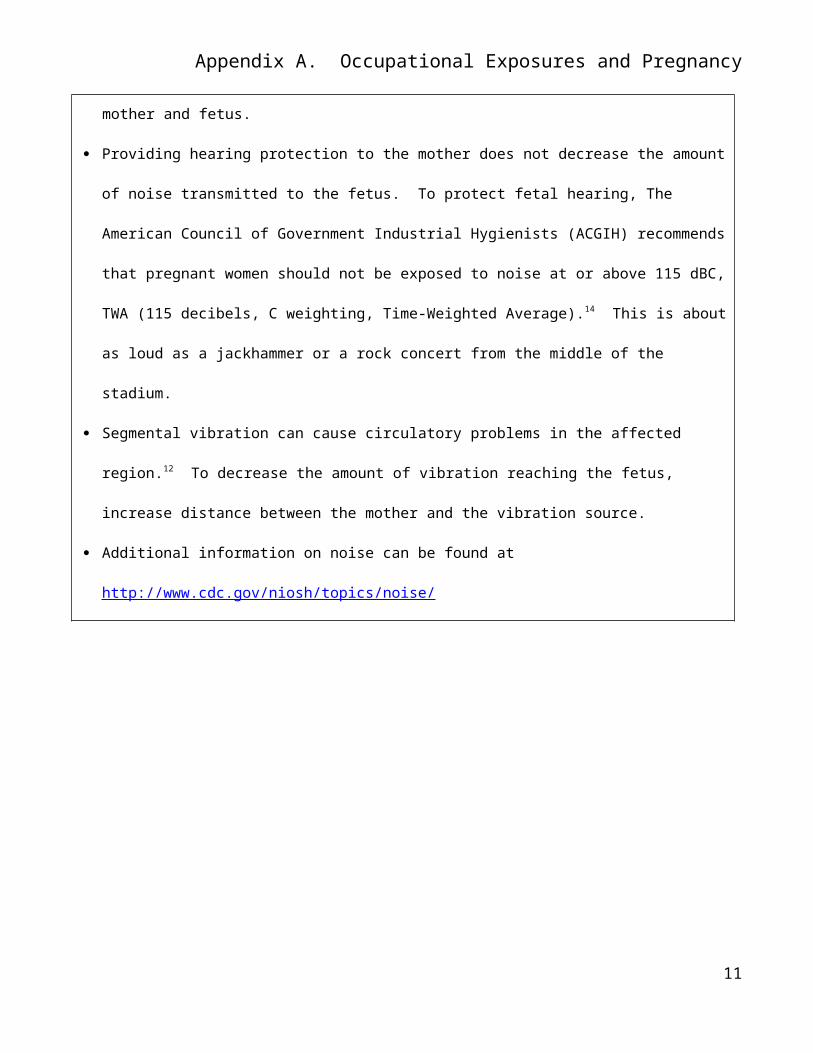
harm both mother and fetus.
Providing hearing protection to the mother does not decrease the amount of noise transmitted to
the fetus. To protect fetal hearing, The American Council of Government Industrial Hygienists
(ACGIH) recommends that pregnant women should not be exposed to noise at or above 115 dBC,
TWA (115 decibels, C weighting, Time-Weighted Average).14 This is about as loud as a jackhammer
or a rock concert from the middle of the stadium.
Segmental vibration can cause circulatory problems in the affected region.12 To decrease the
amount of vibration reaching the fetus, increase distance between the mother and the vibration
7
Appendix A. Occupational Exposures and Pregnancy
source.
Additional information on noise can be found at http://www.cdc.gov/niosh/topics/noise/
8
Appendix A. Occupational Exposures and Pregnancy
Chemicals
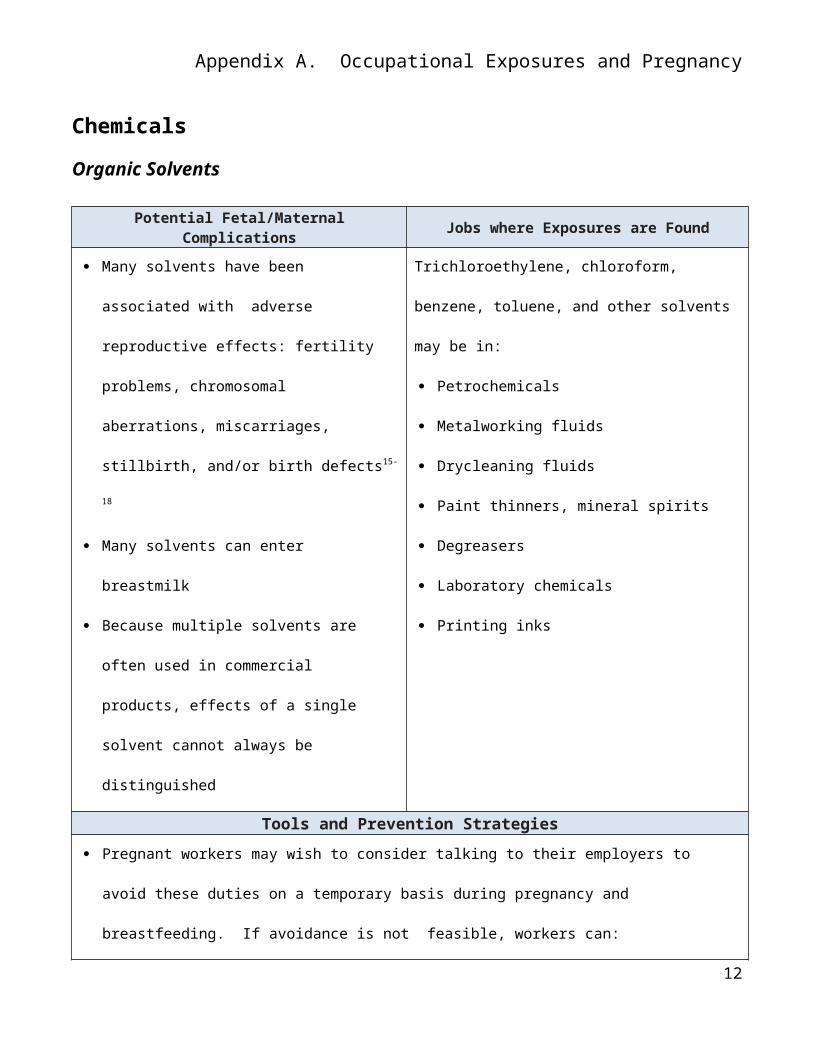
Organic Solvents
Potential Fetal/Maternal Complications Jobs where Exposures are Found
Many solvents have been associated with
adverse reproductive effects: fertility problems,
chromosomal aberrations, miscarriages,
stillbirth, and/or birth defects15-18
Many solvents can enter breastmilk
Because multiple solvents are often used in
commercial products, effects of a single solvent
cannot always be distinguished
Trichloroethylene, chloroform, benzene, toluene,
and other solvents may be in:
Petrochemicals
Metalworking fluids
Drycleaning fluids
Paint thinners, mineral spirits
Degreasers
Laboratory chemicals
Printing inks
Tools and Prevention Strategies
Pregnant workers may wish to consider talking to their employers to avoid these duties on a
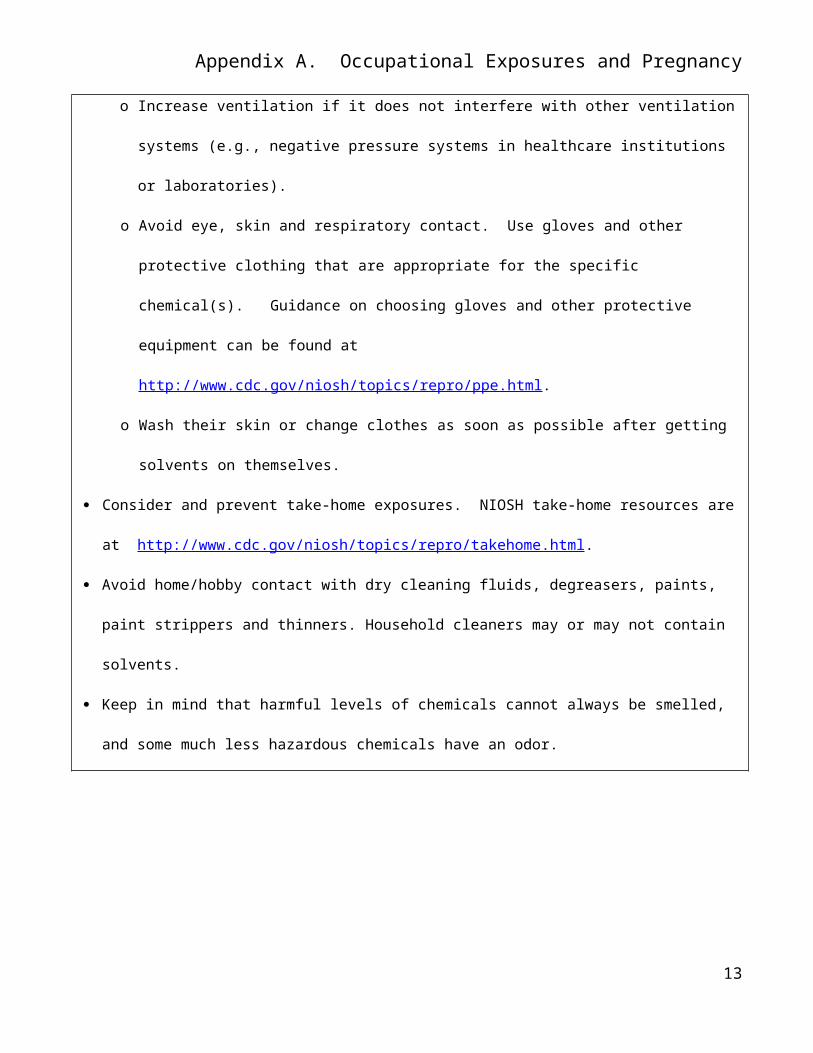
temporary basis during pregnancy and breastfeeding. If avoidance is not feasible, workers can:
o Increase ventilation if it does not interfere with other ventilation systems (e.g., negative
pressure systems in healthcare institutions or laboratories).
o Avoid eye, skin and respiratory contact. Use gloves and other protective clothing that are
appropriate for the specific chemical(s). Guidance on choosing gloves and other protective
equipment can be found at http://www.cdc.gov/niosh/topics/repro/ppe.html.
o Wash their skin or change clothes as soon as possible after getting solvents on themselves.
Consider and prevent take-home exposures. NIOSH take-home resources are at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
Avoid home/hobby contact with dry cleaning fluids, degreasers, paints, paint strippers and thinners.
9
Appendix A. Occupational Exposures and Pregnancy
Household cleaners may or may not contain solvents.
Keep in mind that harmful levels of chemicals cannot always be smelled, and some much less
hazardous chemicals have an odor.
10
Appendix A. Occupational Exposures and Pregnancy
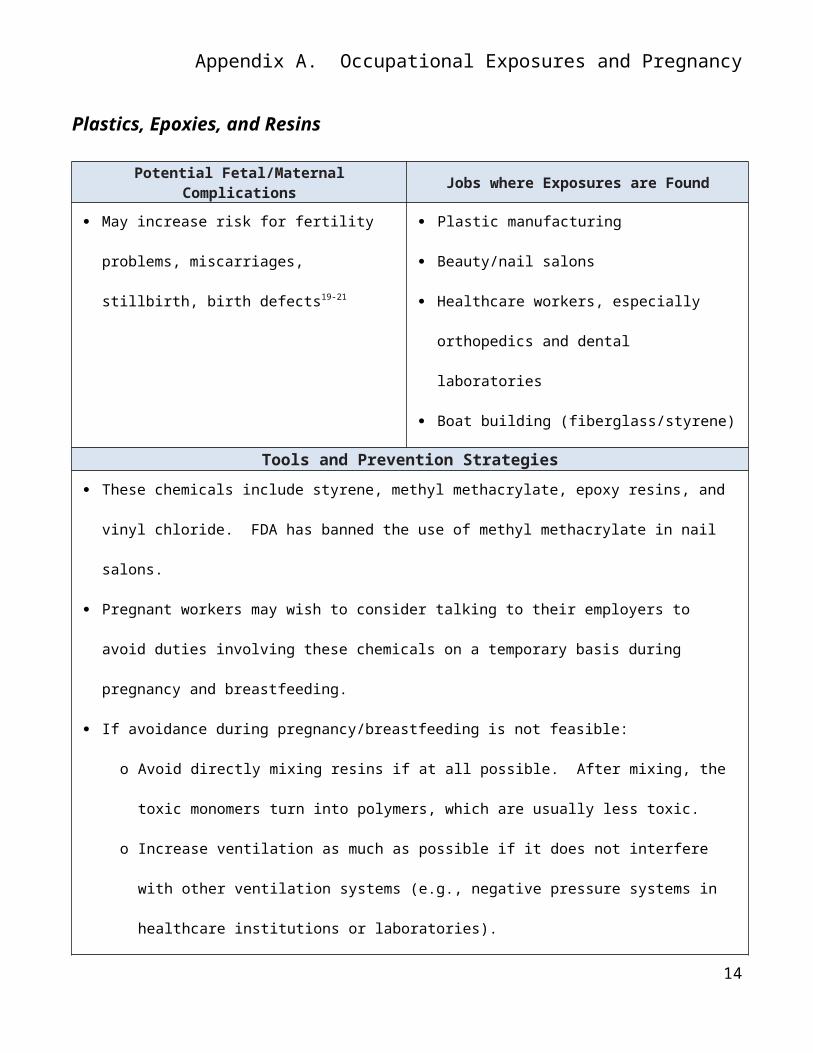
Plastics, Epoxies, and Resins
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May increase risk for fertility problems,
miscarriages, stillbirth, birth defects19-21
Plastic manufacturing
Beauty/nail salons
Healthcare workers, especially orthopedics and
dental laboratories
Boat building (fiberglass/styrene)
Tools and Prevention Strategies
These chemicals include styrene, methyl methacrylate, epoxy resins, and vinyl chloride. FDA has
banned the use of methyl methacrylate in nail salons.
Pregnant workers may wish to consider talking to their employers to avoid duties involving these
chemicals on a temporary basis during pregnancy and breastfeeding.
If avoidance during pregnancy/breastfeeding is not feasible:
o Avoid directly mixing resins if at all possible. After mixing, the toxic monomers turn into
polymers, which are usually less toxic.
o Increase ventilation as much as possible if it does not interfere with other ventilation systems
(e.g., negative pressure systems in healthcare institutions or laboratories).
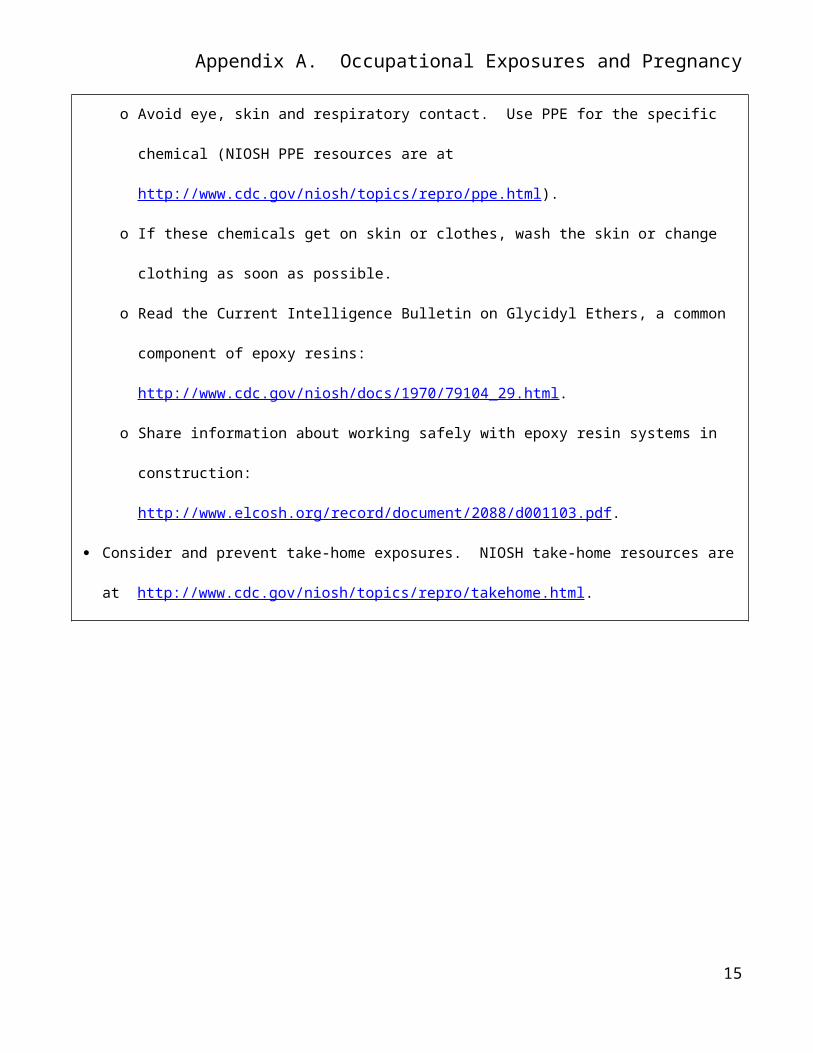
o Avoid eye, skin and respiratory contact. Use PPE for the specific chemical (NIOSH PPE resources
are at http://www.cdc.gov/niosh/topics/repro/ppe.html).
o If these chemicals get on skin or clothes, wash the skin or change clothing as soon as possible.
o Read the Current Intelligence Bulletin on Glycidyl Ethers, a common component of epoxy resins:
http://www.cdc.gov/niosh/docs/1970/79104_29.html.
o Share information about working safely with epoxy resin systems in construction:
http://www.elcosh.org/record/document/2088/d001103.pdf.
11
Appendix A. Occupational Exposures and Pregnancy
Consider and prevent take-home exposures. NIOSH take-home resources are at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
12
Appendix A. Occupational Exposures and Pregnancy
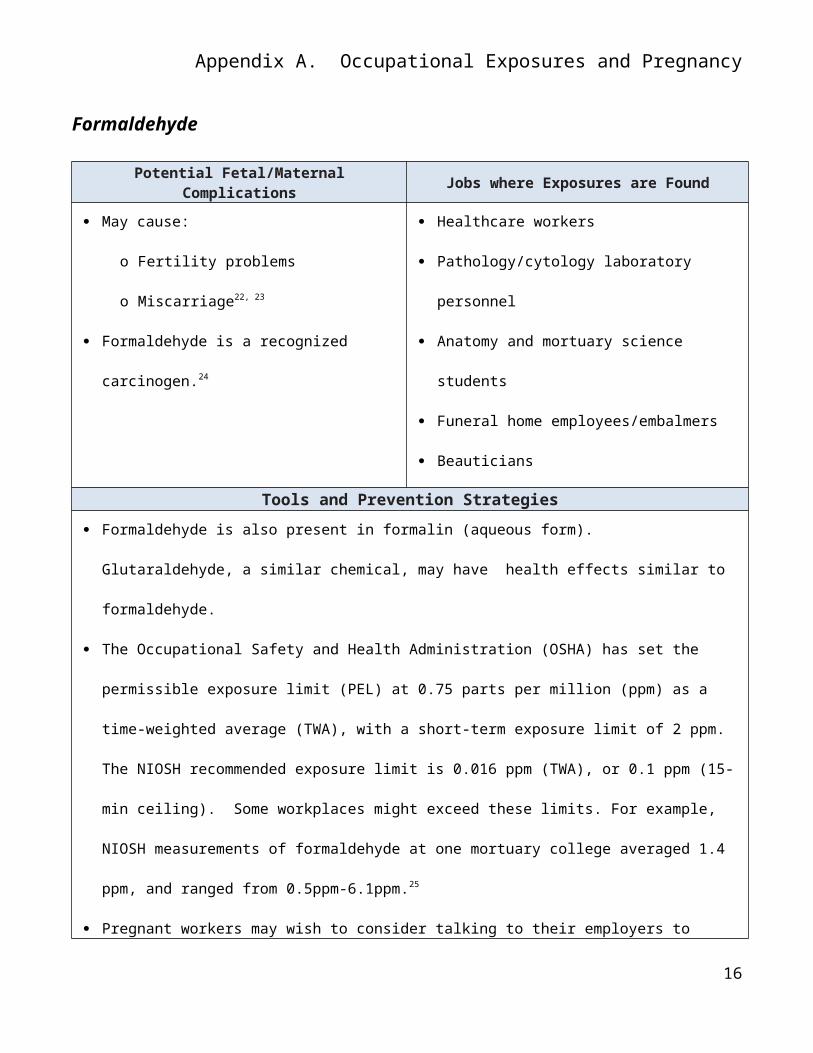
Formaldehyde
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause:
o Fertility problems
o Miscarriage22, 23
Formaldehyde is a recognized carcinogen.24
Healthcare workers
Pathology/cytology laboratory personnel
Anatomy and mortuary science students
Funeral home employees/embalmers
Beauticians
Tools and Prevention Strategies
Formaldehyde is also present in formalin (aqueous form). Glutaraldehyde, a similar chemical, may
have health effects similar to formaldehyde.
The Occupational Safety and Health Administration (OSHA) has set the permissible exposure limit
(PEL) at 0.75 parts per million (ppm) as a time-weighted average (TWA), with a short-term exposure
limit of 2 ppm. The NIOSH recommended exposure limit is 0.016 ppm (TWA), or 0.1 ppm (15-min
ceiling). Some workplaces might exceed these limits. For example, NIOSH measurements of
formaldehyde at one mortuary college averaged 1.4 ppm, and ranged from 0.5ppm-6.1ppm.25
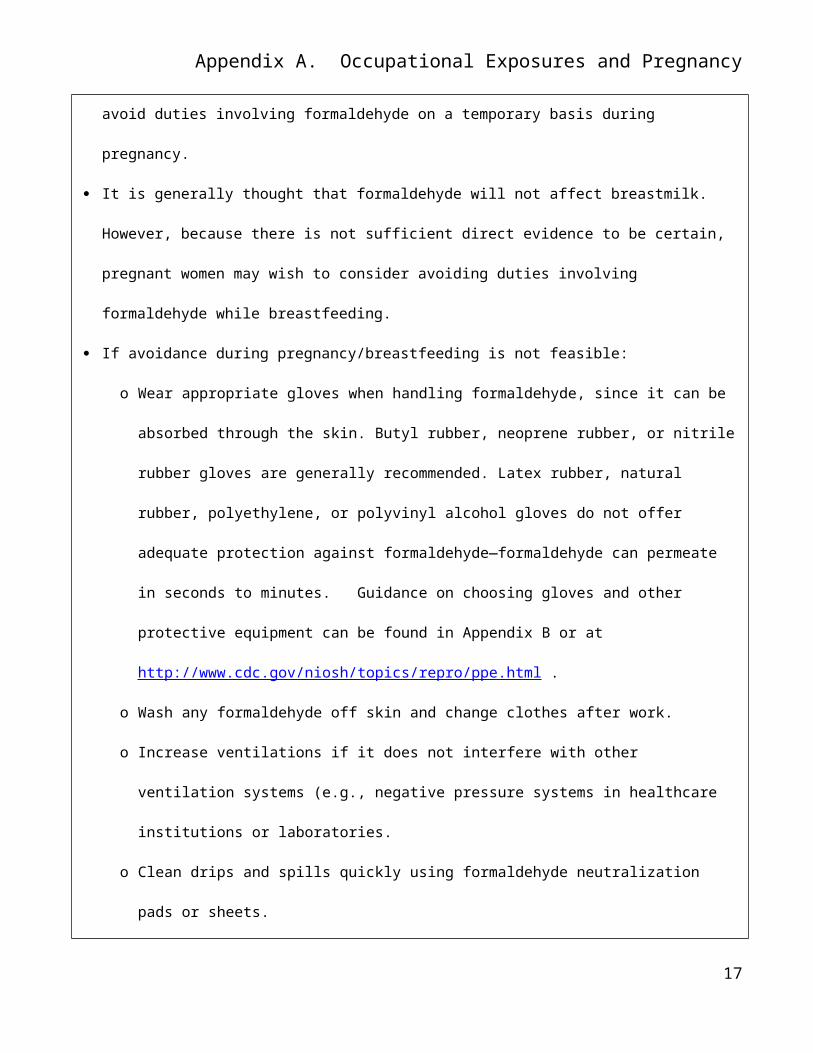
Pregnant workers may wish to consider talking to their employers to avoid duties involving
formaldehyde on a temporary basis during pregnancy.
It is generally thought that formaldehyde will not affect breastmilk. However, because there is not
sufficient direct evidence to be certain, pregnant women may wish to consider avoiding duties
involving formaldehyde while breastfeeding.
If avoidance during pregnancy/breastfeeding is not feasible:
o Wear appropriate gloves when handling formaldehyde, since it can be absorbed through the
skin. Butyl rubber, neoprene rubber, or nitrile rubber gloves are generally recommended. Latex
rubber, natural rubber, polyethylene, or polyvinyl alcohol gloves do not offer adequate
protection against formaldehyde—formaldehyde can permeate in seconds to minutes.
13
Appendix A. Occupational Exposures and Pregnancy
Guidance on choosing gloves and other protective equipment can be found in Appendix B or at
http://www.cdc.gov/niosh/topics/repro/ppe.html .
o Wash any formaldehyde off skin and change clothes after work.
o Increase ventilations if it does not interfere with other ventilation systems (e.g., negative
pressure systems in healthcare institutions or laboratories.
o Clean drips and spills quickly using formaldehyde neutralization pads or sheets.
o If working with tissues, cadavers, or animal specimens preserved using formalin, rinse the
specimen in water to remove excess formalin before beginning dissection. Keep the formalin
solution under a chemical fume hood or in another room while in the lab.
o Some activities will have higher exposures than others. For example, dissections of the chest and
abdomen appear to have higher levels of formaldehyde exposure.
14
Appendix A. Occupational Exposures and Pregnancy
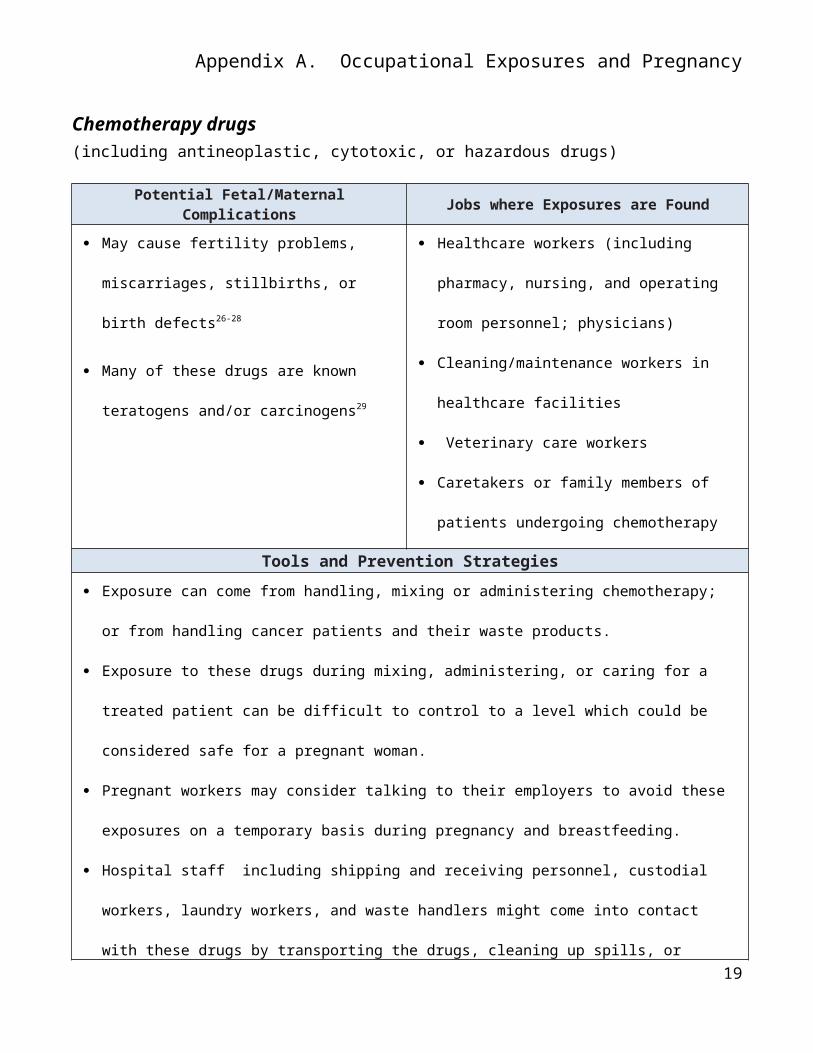
Chemotherapy drugs (including antineoplastic, cytotoxic, or hazardous drugs)
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause fertility problems, miscarriages,
stillbirths, or birth defects26-28
Many of these drugs are known teratogens
and/or carcinogens29
Healthcare workers (including pharmacy,
nursing, and operating room personnel;
physicians)
Cleaning/maintenance workers in healthcare
facilities
Veterinary care workers
Caretakers or family members of patients
undergoing chemotherapy
Tools and Prevention Strategies
Exposure can come from handling, mixing or administering chemotherapy; or from handling cancer
patients and their waste products.
Exposure to these drugs during mixing, administering, or caring for a treated patient can be difficult to
control to a level which could be considered safe for a pregnant woman.
Pregnant workers may consider talking to their employers to avoid these exposures on a temporary
basis during pregnancy and breastfeeding.
Hospital staff including shipping and receiving personnel, custodial workers, laundry workers, and
waste handlers might come into contact with these drugs by transporting the drugs, cleaning up spills,
or handling linens contaminated with bodily fluids from patients receiving antineoplastic drugs.
Guidelines for safe handling and PPE use can be found at NIOSH's Hazardous Drug Alert website,
http://www.cdc.gov/niosh/docs/2014-138/default.html.
Consider and prevent take-home exposures. NIOSH take-home resources are at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
15
Appendix A. Occupational Exposures and Pregnancy
Anesthetic Gases
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause impaired fertility, miscarriage, low
birthweight and/or preterm birth, birth
defects30-33
Healthcare workers in dental offices, hospitals,
and veterinary operating rooms
Tools and Prevention Strategies
Agents include isoflurane, sevoflurane, desflurane, and nitrous oxide.
Historical studies have shown that women who have been exposed to waste anesthetic gases have an
increased risk of miscarriage. More recent studies suggest that hospitals may be getting better at
preventing anesthetic gases from leaking into operating rooms during surgery, which reduces the risk
to workers in operating rooms.
Scavenger systems, devices used to gather and remove waste anesthetic gases from treatment rooms,
must be maintained and monitored to make sure they are working properly.
Workers are most likely to be exposed to waste anesthetic gases in operating facilities with no
automatic ventilation or scavenging systems, operating facilities where these systems are in poor
condition, or recovery rooms where gases exhaled by recovering patients are not properly vented or
scavenged. It may be also harder to control anesthesia leakage if the patient moves (e.g., children,
animals).
Pregnant workers may consider talking to their employers to avoid exposure to these gases during
pregnancy. If this is not possible, patients can be advised that:
o Respirators can be worn to reduce the amount of certain chemicals that workers breathe in.
Charcoal masks or surgical masks will not protect a person from these chemicals. To be effective,
respirators must also be used correctly. Also, effective respiratory protection does not guarantee
a safe environment for the fetus. Learn about respirators and pregnancy at
16
Appendix A. Occupational Exposures and Pregnancy
http://www.cdc.gov/niosh/topics/repro/ppe.html .
o Share NIOSH guidance on waste anesthetic gases, which includes advice for employers on how
to reduce employee exposures: http://www.cdc.gov/niosh/docs/2007-151/ .
17

Appendix A. Occupational Exposures and Pregnancy
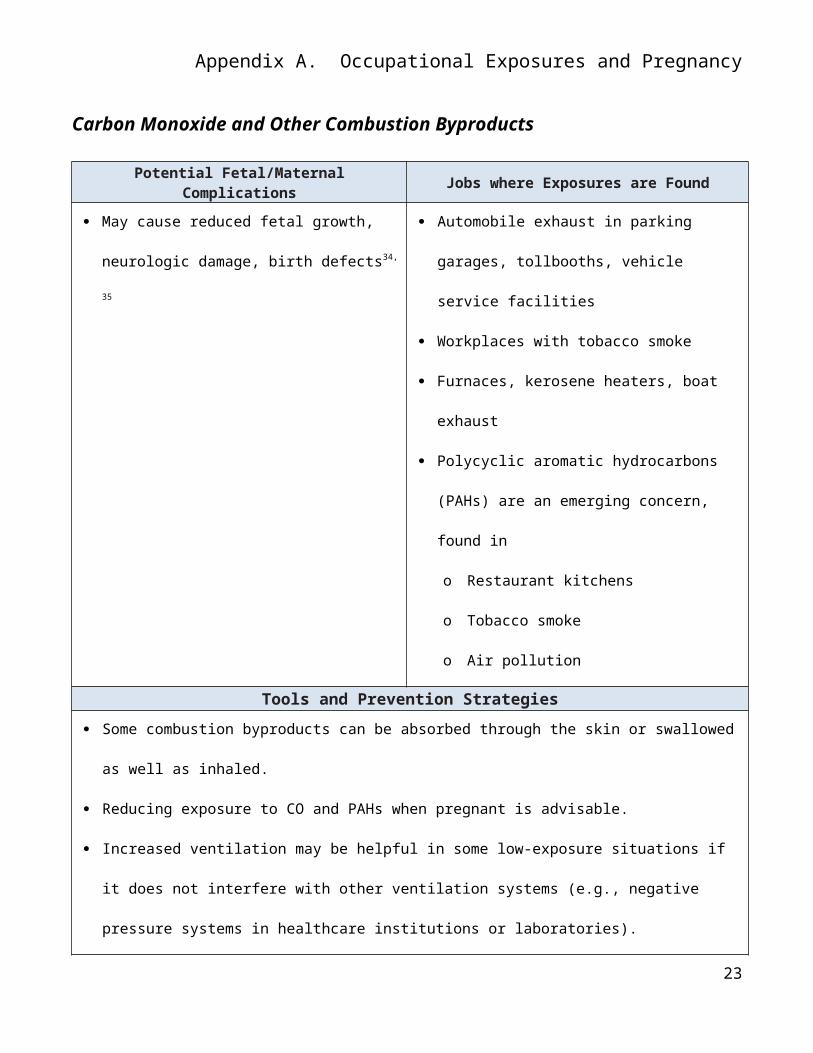
Carbon Monoxide and Other Combustion Byproducts
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause reduced fetal growth, neurologic
damage, birth defects34, 35
Automobile exhaust in parking garages,
tollbooths, vehicle service facilities
Workplaces with tobacco smoke
Furnaces, kerosene heaters, boat exhaust
Polycyclic aromatic hydrocarbons (PAHs) are an
emerging concern, found in
o Restaurant kitchens
o Tobacco smoke
o Air pollution
Tools and Prevention Strategies
Some combustion byproducts can be absorbed through the skin or swallowed as well as inhaled.
Reducing exposure to CO and PAHs when pregnant is advisable.
Increased ventilation may be helpful in some low-exposure situations if it does not interfere with
other ventilation systems (e.g., negative pressure systems in healthcare institutions or laboratories).
Pregnant workers may consider talking to their employers to reduce or avoid exposure on a
temporary basis during pregnancy. If occupational exposure cannot be avoided, respiratory protection
can be evaluated but does not guarantee a safe environment for the fetus.
NIOSH PPE resources are at http://www.cdc.gov/niosh/topics/repro/ppe.html.
New Jersey Fact Sheet on carbon monoxide available at:
http://nj.gov/health/eoh/rtkweb/documents/fs/0345.pdf.
Consider and prevent take-home smoke exposures. NIOSH take-home resources are at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
18
Appendix A. Occupational Exposures and Pregnancy
Be aware of local smog alerts and follow directions.
Pesticides
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause miscarriages, birth defects, cognitive
deficits36-38
Some pesticides may also pass into breast milk.
Farm and greenhouse workers
Florists
Fruit/ vegetable handlers
Veterinarians and veterinary assistants
Landscapers
Anyone who performs pest or weed control.
Tools and Prevention Strategies
Avoiding exposure to pesticides when pregnant is the safest option. If occupational exposure cannot
be avoided, reducing exposure is advisable.
Greenhouse and farm workers must observe re-entry times carefully. Every pesticide has a re-entry
time based on its chemical/s.
In the home, people may be exposed through the use of insect sprays in and around the house, lawn or
garden treatments, or the use of flea and tick treatments or preventatives on pets.
Consider and prevent take-home exposures. NIOSH take-home resources are at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
Use PPE gloves/clothing recommended for the specific pesticide. Guidance on choosing gloves and
other protective equipment can be found in Appendix B or at
http://www.cdc.gov/niosh/topics/repro/ppe.html.
Wash hands after handling pets wearing flea collars or who have received flea and tick drops, and
avoid skin contact with flea, tick, and mite treatments or preventatives.
Pregnant workers may wish to consider talking to their employers to reduce or avoid exposure on a
temporary basis during pregnancy. If occupational exposure cannot be avoided, respiratory
19

Appendix A. Occupational Exposures and Pregnancy
protection can be considered.
Polychlorinated Biphenyls (PCBs)
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause low birthweight, stillbirth39-41 Waste management/recycling
Repair of older electrical capacitors
Tools and Prevention Strategies
Production of PCBs was banned in the U.S. in 1977, but worker exposures continue where PCB
sources are recycled or repaired. PCB contamination of surface waters is widespread.
Pregnant workers may wish to consider talking to their employers to avoid duties with exposure
to PCBs on a temporary basis during pregnancy.
If avoidance during pregnancy is not feasible:
o Increase ventilation as much as possible if it does not interfere with other ventilation
systems (e.g., negative pressure systems in healthcare institutions or laboratories).
o Avoid eye, skin and respiratory contact.
o Use PPE recommended for PCBs. Guidance on choosing gloves and other protective
equipment can be found in Appendix B or at
http://www.cdc.gov/niosh/topics/repro/ppe.html.
Consider and prevent take-home exposures. NIOSH take-home resources are at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
New Jersey Fact Sheet on PCBs available at:
http://nj.gov/health/eoh/rtkweb/documents/fs/1554.pdf.
20
Appendix A. Occupational Exposures and Pregnancy
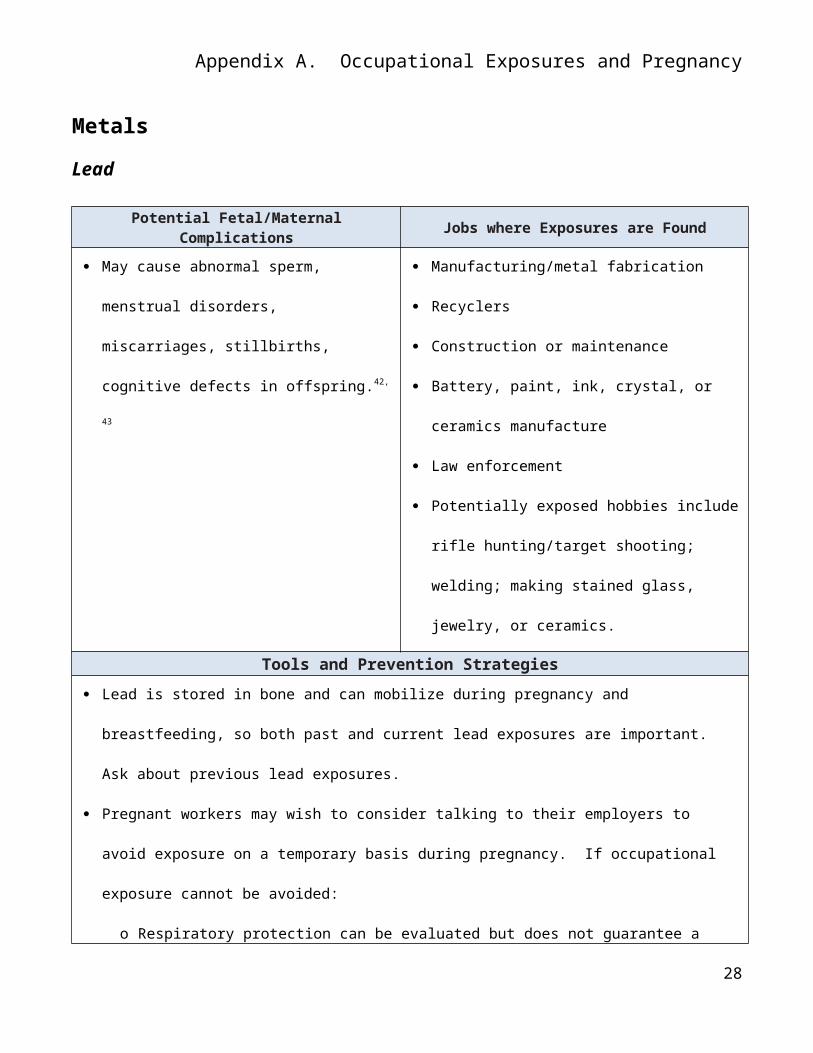
Metals
Lead
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause abnormal sperm, menstrual
disorders, miscarriages, stillbirths, cognitive
defects in offspring.42, 43
Manufacturing/metal fabrication
Recyclers
Construction or maintenance
Battery, paint, ink, crystal, or ceramics
manufacture
Law enforcement
Potentially exposed hobbies include rifle
hunting/target shooting; welding; making
stained glass, jewelry, or ceramics.
Tools and Prevention Strategies
Lead is stored in bone and can mobilize during pregnancy and breastfeeding, so both past and current
lead exposures are important. Ask about previous lead exposures.
Pregnant workers may wish to consider talking to their employers to avoid exposure on a temporary
basis during pregnancy. If occupational exposure cannot be avoided:
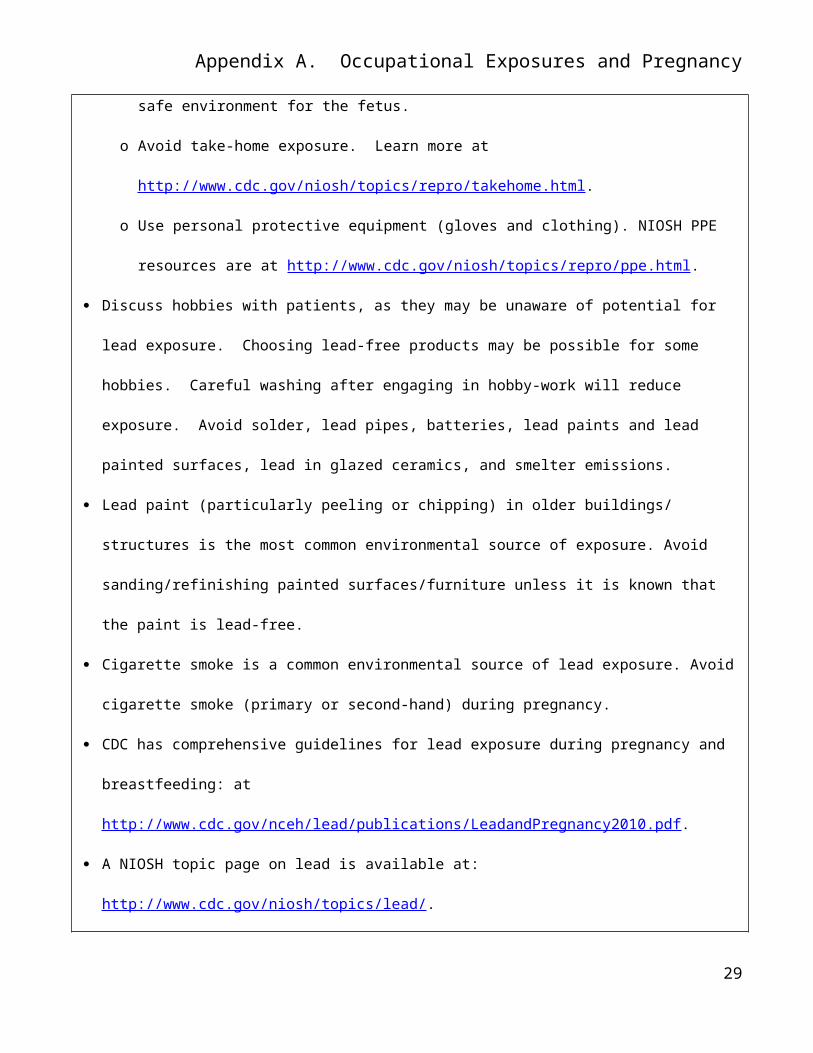
o Respiratory protection can be evaluated but does not guarantee a safe environment for the fetus.
o Avoid take-home exposure. Learn more at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
o Use personal protective equipment (gloves and clothing). NIOSH PPE resources are at
http://www.cdc.gov/niosh/topics/repro/ppe.html.
Discuss hobbies with patients, as they may be unaware of potential for lead exposure. Choosing lead-
free products may be possible for some hobbies. Careful washing after engaging in hobby-work will
reduce exposure. Avoid solder, lead pipes, batteries, lead paints and lead painted surfaces, lead in
21
Appendix A. Occupational Exposures and Pregnancy
glazed ceramics, and smelter emissions.
Lead paint (particularly peeling or chipping) in older buildings/ structures is the most common
environmental source of exposure. Avoid sanding/refinishing painted surfaces/furniture unless it is
known that the paint is lead-free.
Cigarette smoke is a common environmental source of lead exposure. Avoid cigarette smoke (primary
or second-hand) during pregnancy.
CDC has comprehensive guidelines for lead exposure during pregnancy and breastfeeding: at
http://www.cdc.gov/nceh/lead/publications/LeadandPregnancy2010.pdf.
A NIOSH topic page on lead is available at: http://www.cdc.gov/niosh/topics/lead/.
A New Jersey Fact Sheet on lead is available at:
http://nj.gov/health/eoh/rtkweb/documents/fs/1096.pdf.
22
Appendix A. Occupational Exposures and Pregnancy
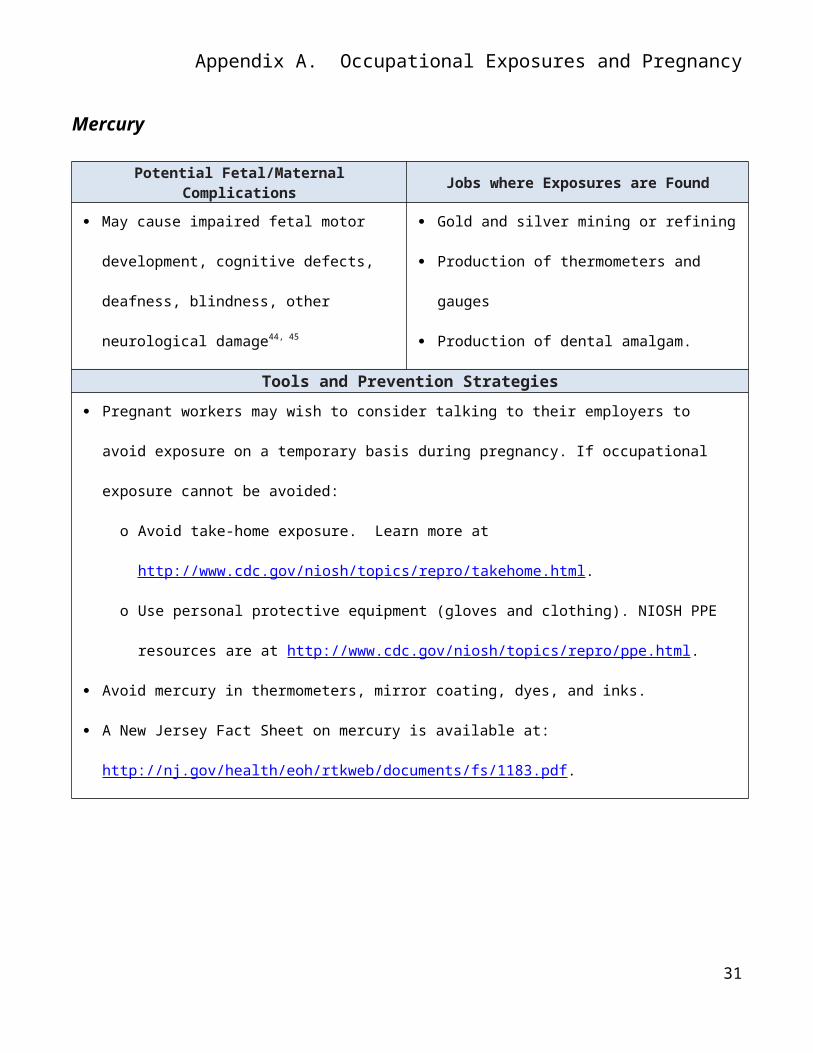
Mercury
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause impaired fetal motor development,
cognitive defects, deafness, blindness, other
neurological damage44, 45
Gold and silver mining or refining
Production of thermometers and gauges
Production of dental amalgam.
Tools and Prevention Strategies
Pregnant workers may wish to consider talking to their employers to avoid exposure on a temporary
basis during pregnancy. If occupational exposure cannot be avoided:
o Avoid take-home exposure. Learn more at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
o Use personal protective equipment (gloves and clothing). NIOSH PPE resources are at
http://www.cdc.gov/niosh/topics/repro/ppe.html.
Avoid mercury in thermometers, mirror coating, dyes, and inks.
A New Jersey Fact Sheet on mercury is available at:
http://nj.gov/health/eoh/rtkweb/documents/fs/1183.pdf.
23
Appendix A. Occupational Exposures and Pregnancy
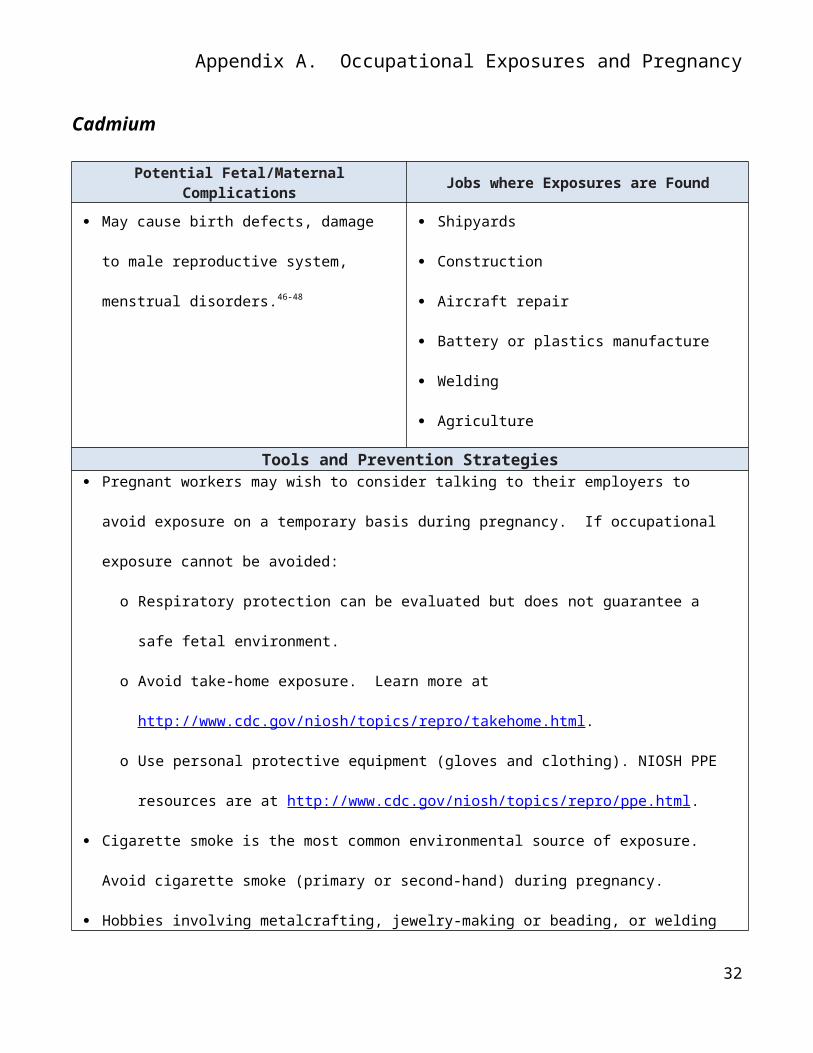
Cadmium
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause birth defects, damage to male
reproductive system, menstrual disorders.46-48
Shipyards
Construction
Aircraft repair
Battery or plastics manufacture
Welding
Agriculture
Tools and Prevention Strategies Pregnant workers may wish to consider talking to their employers to avoid exposure on a temporary
basis during pregnancy. If occupational exposure cannot be avoided:
o Respiratory protection can be evaluated but does not guarantee a safe fetal environment.
o Avoid take-home exposure. Learn more at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
o Use personal protective equipment (gloves and clothing). NIOSH PPE resources are at
http://www.cdc.gov/niosh/topics/repro/ppe.html.
Cigarette smoke is the most common environmental source of exposure. Avoid cigarette smoke
(primary or second-hand) during pregnancy.
Hobbies involving metalcrafting, jewelry-making or beading, or welding create the potential for
exposure to cadmium. Inexpensive metal costume jewelry, jewelry-making products, or beads may
contain cadmium. Careful washing after hobby-work will reduce exposure.
A New Jersey Fact Sheet on cadmium is available at:
http://nj.gov/health/eoh/rtkweb/documents/fs/0305.pdf.
24
Appendix A. Occupational Exposures and Pregnancy
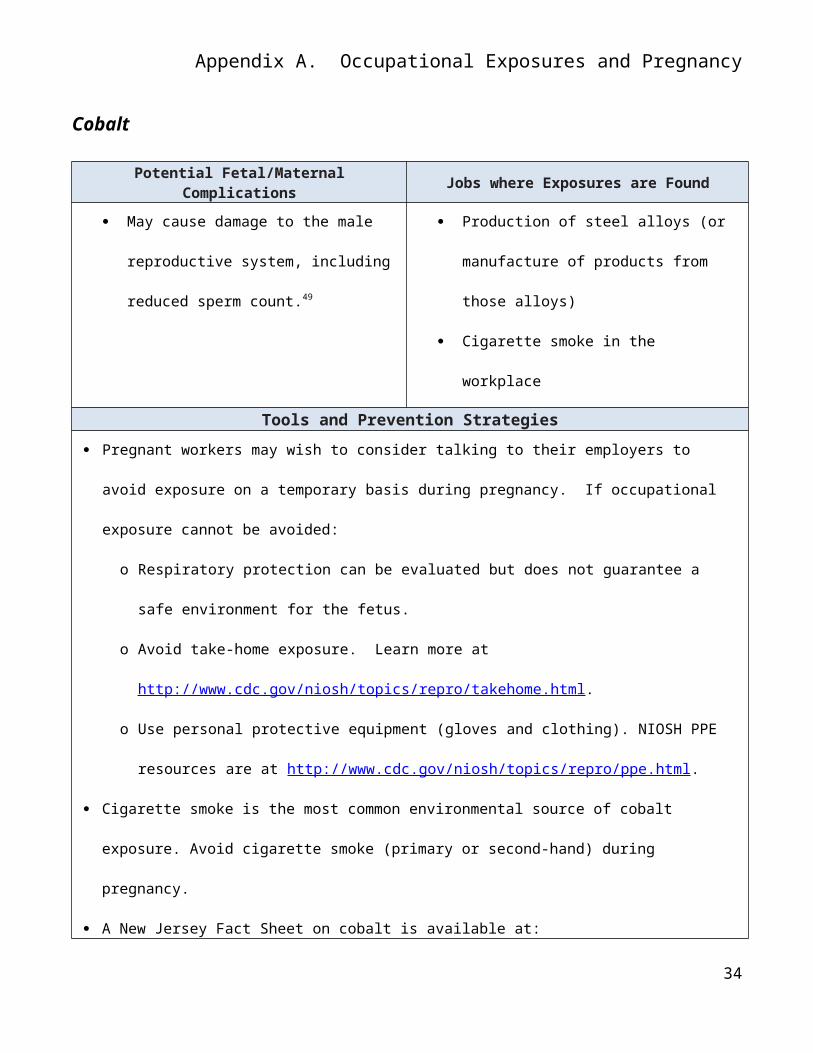
Cobalt
Potential Fetal/Maternal Complications Jobs where Exposures are Found
May cause damage to the male
reproductive system, including reduced
sperm count.49
Production of steel alloys (or manufacture of
products from those alloys)
Cigarette smoke in the workplace
Tools and Prevention Strategies
Pregnant workers may wish to consider talking to their employers to avoid exposure on a temporary
basis during pregnancy. If occupational exposure cannot be avoided:
o Respiratory protection can be evaluated but does not guarantee a safe environment for the fetus.
o Avoid take-home exposure. Learn more at
http://www.cdc.gov/niosh/topics/repro/takehome.html.
o Use personal protective equipment (gloves and clothing). NIOSH PPE resources are at
http://www.cdc.gov/niosh/topics/repro/ppe.html.
Cigarette smoke is the most common environmental source of cobalt exposure. Avoid cigarette smoke
(primary or second-hand) during pregnancy.
A New Jersey Fact Sheet on cobalt is available at:
http://nj.gov/health/eoh/rtkweb/documents/fs/0520.pdf .
25
Appendix A. Occupational Exposures and Pregnancy
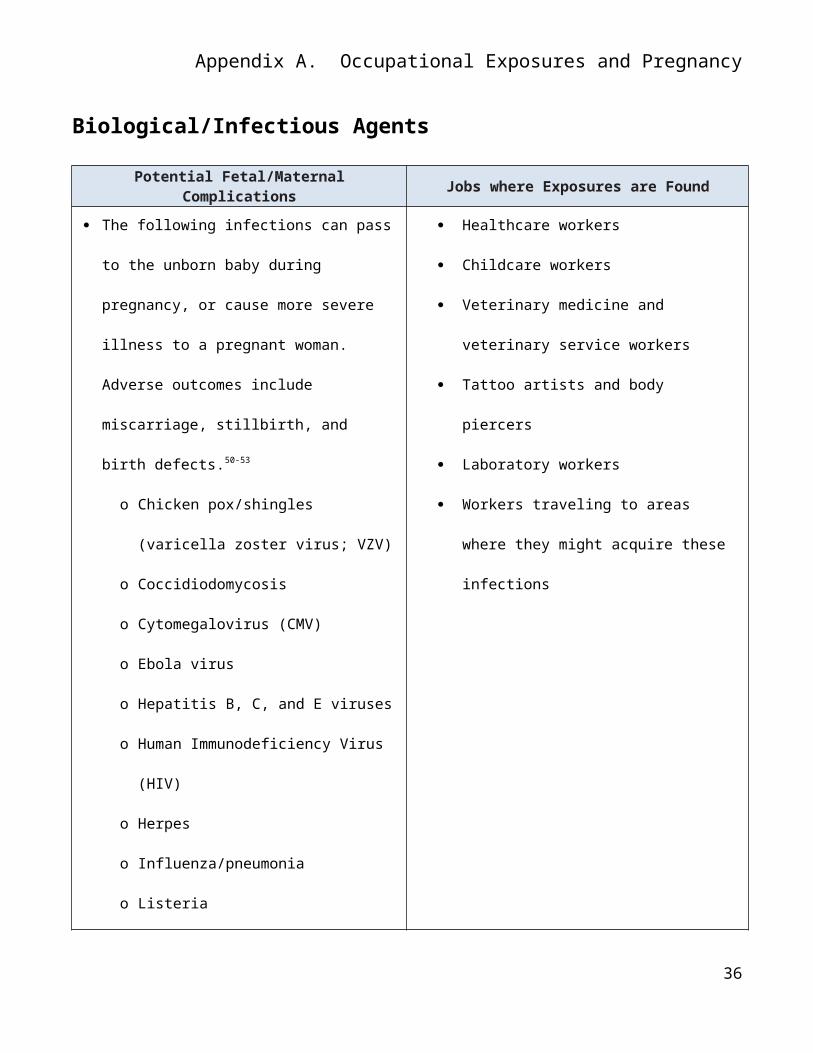
Biological/Infectious Agents
Potential Fetal/Maternal Complications Jobs where Exposures are Found
The following infections can pass to the unborn
baby during pregnancy, or cause more severe
illness to a pregnant woman. Adverse
outcomes include miscarriage, stillbirth, and
birth defects.50-53
o Chicken pox/shingles (varicella zoster
virus; VZV)
o Coccidiodomycosis
o Cytomegalovirus (CMV)
o Ebola virus
o Hepatitis B, C, and E viruses
o Human Immunodeficiency Virus (HIV)
o Herpes
o Influenza/pneumonia
o Listeria
o Malaria
o Measles
o Parvovirus B19 (Fifth disease)
o Rubella (German measles)
o Toxoplasmosis
o Zika Virus
Healthcare workers
Childcare workers
Veterinary medicine and veterinary service
workers
Tattoo artists and body piercers
Laboratory workers
Workers traveling to areas where they
might acquire these infections
26
Appendix A. Occupational Exposures and Pregnancy
Tools and Prevention Strategies Review vaccination history with the patient:
o Pregnant women should get the inactivated (injected) influenza vaccine, instead of the live
attenuated nasal vaccine (LAIV).
o MMR vaccination is contraindicated during pregnancy. Non-immune health care workers (can
be determined by serology) should not work with rubella-infected patients.
o Hepatitis A and B vaccines can be administered during pregnancy
o See immunization recommendations for special HCW conditions, including pregnancy, on Table
3 of: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6007a1.htm.
Pregnant women who carefully follow infection control guidelines (i.e., standard precautions) are
generally at no higher risk of acquiring a harmful infection from a patient than other workers.
Exceptions exist for some pregnant women and some infectious agents:
o See appendix A of the 2007 Guidelines for Isolation Precautions:
http://www.cdc.gov/hicpac/pdf/isolation/Isolation2007.pdf
o See Guidelines for Infection Control in Healthcare Workers, Table 6
http://www.cdc.gov/hicpac/pdf/InfectControl98.pdf.
o Pregnant women are at greater risk of severe illness and death when they contract Ebola virus.
Pregnant healthcare workers should not be required to care for patients with confirmed or
probable Ebola Virus Disease (EVD) or a person under investigation for EVD. They should not
be required to clean and disinfect items or surfaces that are possibly contaminated with Ebola
virus or the blood and/or body fluids of these patients.
o Risks and precautions for CMV can be found at:
http://www.cdc.gov/cmv/clinical/index.html
27
Appendix A. Occupational Exposures and Pregnancy
http://www.cdc.gov/cmv/risk/preg-women.html .
In 1-4% of pregnancies, a mother will develop a primary CMV infection; approximately
one-third will pass the infection to their fetus. Most fetal infections (85-90%) will resolve
prior to birth. These numbers and risks are even lower for seropositive women, but
seropositivity to CMV does not necessarily mean immunity.
o Following precautions for shingles/chicken pox carefully reduces the risk of a pregnant worker
contracting VZV infection. Based on the patient’s circumstances, consider recommending that
pregnant employees avoid working with patients with shingles or chicken pox due to the
potentially severe consequences:
Even among those people who previously contracted chicken pox or had varicella vaccine,
a small group are still not immune.
Approximately 10-20% of pregnant women who contract VZV may develop pneumonia
and, of those women, the chance of death can be as high as 40%.54, 55 Women who are
infected with varicella have a small risk of having a baby with congenital varicella
syndrome.56
o Zika virus is an emerging infectious disease which has been linked to birth defects in pregnant
women. Current guidance for Zika virus is at the CDC Zika website
http://www.cdc.gov/zika/index.html.
Observe safe practices in body modification studios: http://www.cdc.gov/niosh/topics/body_art/.
Guidelines for laboratory workers are intended to prevent laboratory-acquired infection in all
personnel when followed correctly. Some exceptions exist.
o For patient clinical samples, refer to the Guidelines for Safe Work Practices in Human and
Animal Medical Diagnostic Laboratories at: http://www.cdc.gov/mmwr/pdf/other/su6101.pdf.
o For laboratory work with concentrated cultures of pathogens, refer to the Biosafety Manual for
Biomedical Laboratories at: http://www.cdc.gov/biosafety/publications/bmbl5/BMBL.pdf.
28
Appendix A. Occupational Exposures and Pregnancy
o For work involving unusual pathogens, production quantities, emergent infections, or
genetically modified pathogens, CDC-INFO is available at 1-800-CDC-INFO.
Other workplace factors
Shift Work and Long Working Hours
Potential Fetal/Maternal Complications Jobs where Exposures are Found
Have been associated with menstrual
disorders, miscarriages, preterm birth.57-59
Health effects from shiftwork are also relevant
to any kind of work during normal sleep time,
including irregular shifts and jet lag, as well as
long hours of work
Health Care Workers
Law Enforcement and Firefighters
Cleaning/Building Services
Manufacturing Workers
Transportation Workers
Air Crew
Tools and Prevention Strategies
If feasible, avoid working during normal sleep time during pregnancy.
The National Sleep Foundation’s shift work information is found at: http://sleepfoundation.org/shift-
work/content/shift-work-disorder.
Good sleep hygiene is always important, but especially for shiftworkers. General recommendations
can be found at http://www.sleepfoundation.org/article/ask-the-expert/sleep-hygiene.
Sleep hygiene tips for shift workers can be found at
http://my.clevelandclinic.org/disorders/sleep_disorders/hic_shift_work_sleep_disorder.aspx
Because the adverse health effects of long or irregular work schedules may be partially due to stress
responses, measures to reduce stress and improve resilience may help (relaxation, exercise, and
following a healthful diet).
29
Appendix A. Occupational Exposures and Pregnancy
30
Appendix A. Occupational Exposures and Pregnancy
High physical demands
Potential Fetal/Maternal Complications Jobs where Exposures are Found
Pregnant women are at higher risk of an injury
while lifting due to ergonomic stresses
(including altered posture, impaired balance
and agility, and impaired ability to hold objects
close to the body due to the abdomen’s
changing size).60
Risk of injury can also increase in early
pregnancy due to hormonal changes that affect
spinal ligaments and joints.60
Prolonged standing or heavy lifting has been
associated with an increased chance of
miscarriage or preterm delivery57, 60-62
Healthcare workers
Childcare workers
Flight attendants
Construction
Manufacturing
Service workers
Housekeeping/janitorial
Farm and greenhouse workers
Many other jobs
Tools and Prevention Strategies
Normal everyday physical activities aren’t a cause for concern, and moderate exercise during
pregnancy can help promote a healthy pregnancy. Very high physical demands are a concern.
Examples include the following:
o bending at the waist more than 20 times per day
o highly repetitive lifting (more than 3 times a minute)
o standing for many hours without a rest break
Reduce or avoid the following actions:
o Repeated stooping, bending, squatting
o Lifting heavy objects from the floor or below mid-shin, or lifting overhead
31
Appendix A. Occupational Exposures and Pregnancy
o Prolonged standing or sitting
Advise workers to get off their feet when on breaks.
A NIOSH infographic on provisional weight limits for lifting during pregnancy is at:
http://blogs.cdc.gov/niosh-science-blog/files/2013/05/ClinicalGuidelinesImg-NewLogoFinal.jpg.
32
Appendix A. Occupational Exposures and Pregnancy
References Cited
1. DE SANTIS M, CESARI E, NOBILI E, STRAFACE G, CAVALIERE AF, CARUSO A. Radiation effects on development. Birth Defects Res C Embryo Today 2007;81:177-82.
2. GRAJEWSKI B, WHELAN EA, LAWSON CC, et al. Miscarriage among flight attendants. Epidemiology 2015;26:192-203.
3. LAWSON CC, ROCHELEAU CM, WHELAN EA, et al. Occupational exposures among nurses and risk of spontaneous abortion. Am J Obstet Gynecol 2012;206:327 e1-8.
4. SHIRANGI A, FRITSCHI L, HOLMAN CDJ. Maternal occupational exposures and risk of spontaneous abortion in veterinary practice. Occup Environ Med 2008;65:719-25.
5. LARY JM, CONOVER DL. Teratogenic effects of radiofrequency radiation. IEEE Eng Med Biol Mag 1987;6:42-46.
6. ZISKIN MC, MORRISSEY J. Thermal thresholds for teratogenicity, reproduction, and development. International journal of hyperthermia : the official journal of European Society for Hyperthermic Oncology, North American Hyperthermia Group 2011;27:374-87.
7. HITCHCOCK RT. Nonionizing Radiation: Radiofrequency. Patty's Industrial Hygiene. Hoboken, NJ: John Wiley & Sons, Inc., 2001.
8. HU H, BESSER M. Atmospheric variations, noise, and vibration. In: Paul M, ed. Occupational and Environmental Reproductive Hazards: A Guide for Clinicians. Baltimore: Williams & Wilkins, 1993.
9. EDWARDS MJ. Review: Hyperthermia and fever during pregnancy. Birth Defects Res A Clin Mol Teratol 2006;76:507-16.
10. CHAMBERS CD. Risks of hyperthermia associated with hot tub or spa use by pregnant women. Birth Defects Research Part A: Clinical and Molecular Teratology 2006;76:569-73.
11. AMERICAN ACADEMY OF PEDIATRICS COMMITTEE ON ENVIRONMENTAL HEALTH. Noise: A hazard for the fetus and newborn. Pediatrics 1997;100:724-27.
12. PELMEAR PL. Low frequency noise and vibration: role of government in occupational disease. Seminars in perinatology 1990;14:322-8.
13. NIEMTZOW RC. Loud noise and pregnancy. Military medicine 1993;158:10-12.14. AMERICAN CONFERENCE OF GOVERNMENTAL INDUSTRIAL HYGIENISTS. Documentation of the threshold
limit values and biological exposure indices, 7th edition. Cincinnati, Ohio: ACGIH Worldwide; Number of pages.
15. ATTARCHI MS, ASHOURI M, LABBAFINEJAD Y, MOHAMMADI S. Assessment of time to pregnancy and spontaneous abortion status following occupational exposure to organic solvents mixture. International archives of occupational and environmental health 2012;85:295-303.
16. GARLANTEZEC R, CHEVRIER C, CORDIER S. The study of the relation between maternal occupational exposure to solvents and birth defects should include oxygenated solvents. Occup Environ Med 2012;69:933; author reply 33-4.
17. GILBOA SM, DESROSIERS TA, LAWSON C, et al. Association between maternal occupational exposure to organic solvents and congenital heart defects, National Birth Defects Prevention Study, 1997-2002. Occup Environ Med 2012;69:628-35.
18. HEALTH COUNCIL OF THE NETHERLANDS. Occupational exposure to organic solvents: effects on human reproduction. The Hague: Health Council of the Netherlands, 2008.
19. HAUSER R, CALAFAT AM. Phthalates and human health. Occup Environ Med 2005;62:806-18.
33
Appendix A. Occupational Exposures and Pregnancy
20. HOUGAARD KS, HANNERZ H, FEVEILE H, BONDE JP. Increased incidence of infertility treatment among women working in the plastics industry. Reproductive toxicology (Elmsford, NY) 2009;27:186-9.
21. SHELBY MD. NTP-CERHR monograph on the potential human reproductive and developmental effects of bisphenol A. National Toxicology Program 2008:v, vii-ix, 1-64 passim.
22. DUONG A, STEINMAUS C, MCHALE CM, VAUGHAN CP, ZHANG LP. Reproductive and developmental toxicity of formaldehyde: A systematic review. Mutation Research-Reviews in Mutation Research 2011;728:118-38.
23. TASKINEN HK, KYYRONEN P, SALLMEN M, et al. Reduced fertility among female wood workers exposed to formaldehyde. Am J Ind Med 1999;36:206-12.
24. ANONYMOUS. Formaldehyde. IARC Monogr Eval Carcinog Risks Hum 1995;62:217-362.25. NATIONAL INSTITUTE FOR OCCUPATIONAL SAFETY AND HEALTH (NIOSH). NIOSH Health Hazard Evaluation
HHE 79-146-670, Cincinnati College of Mortuary Science, Embalming Laboratory, Cincinnati, Ohio. Cincinnati, Ohio: NIOSH, Department of Health and Human Services, 1980.
26. FRANSMAN W, ROELEVELD N, PEELEN S, DE KORT W, KROMHOUT H, HEEDERIK D. Nurses with dermal exposure to antineoplastic drugs: reproductive outcomes. Epidemiology 2007;18:112-19.
27. LAWSON CC, ROCHELEAU CM, WHELAN EA, et al. Occupational exposure to anesthetic gases, antineoplastic drugs, antiviral drugs, sterilizing agents, and x-rays and risk of spontaneous abortion among nurses. Am J Epidemiol 2011;173:S296.
28. QUANSAH R, JAAKKOLA JJ. Occupational exposures and adverse pregnancy outcomes among nurses: a systematic review and meta-analysis. Journal of women's health (2002) 2010;19:1851-62.
29. SHORTRIDGE-MCCAULEY LA. Reproductive hazards: an overview of exposures to health care workers. AAOHN journal : official journal of the American Association of Occupational Health Nurses 1995;43:614-21.
30. BOIVIN JF. Risk of spontaneous abortion in women occupationally exposed to anaesthetic gases: a meta-analysis. Occup Environ Med 1997;54:541-48.
31. ROWLAND AS, BAIRD DD, SHORE DL, WEINBERG CR, SAVITZ DA, WILCOX AJ. Nitrous oxide and spontaneous abortion in female dental assistants. Am J Epidemiol 1995;141:531-8.
32. SHIRANGI A, FRITSCHI L, HOLMAN CD. Associations of unscavenged anesthetic gases and long working hours with preterm delivery in female veterinarians. Obstetrics and gynecology 2009;113:1008-17.
33. TESCHKE K, ABANTO Z, ARBOUR L, et al. Exposure to anesthetic gases and congenital anomalies in offspring of female registered nurses. Am J Ind Med 2011;54:118-27.
34. WORLD HEALTH ORGANIZATION. Carbon Monoxide, 2nd ed. (Environmental Health Criteria 213) Geneva: World Health Organization, 1999.
35. MCELHATTON P, EASTON T. Environmental and occupational exposure to gases during pregnancy. Reproductive toxicology (Elmsford, NY) 2002;16:441-2.
36. HARARI R, JULVEZ J, MURATA K, et al. Neurobehavioral deficits and increased blood pressure in school-age children prenatally exposed to pesticides. Environ Health Perspect 2010;118:890-6.
37. SNIJDER CA, ROELEVELD N, TE VELDE E, et al. Occupational exposure to chemicals and fetal growth: the Generation R Study. Human reproduction (Oxford, England) 2012;27:910-20.
38. SNIJDER CA, TE VELDE E, ROELEVELD N, BURDORF A. Occupational exposure to chemical substances and time to pregnancy: a systematic review. Human reproduction update 2012;18:284-300.
39. FAROON OM, KEITH S, JONES D, DE ROSA C. Effects of polychlorinated biphenyls on development and reproduction. Toxicology and industrial health 2001;17:63-93.
34
Appendix A. Occupational Exposures and Pregnancy
40. GUO YL, LAMBERT GH, HSU C-C, HSU MML. Yucheng: health effects of prenatal exposure to polychlorinated biphenyls and dibenzofurans. International archives of occupational and environmental health 2004;77:153-58.
41. NIEUWENHUIJSEN MJ, DADVAND P, GRELLIER J, MARTINEZ D, VRIJHEID M. Environmental risk factors of pregnancy outcomes: a summary of recent meta-analyses of epidemiological studies. Environ Health 2013;12:6.
42. NATIONAL TOXICOLOGY PROGRAM. NTP monograph on health effects of low-level lead Research Triangle Park, NC: National Toxicology Program, 2012.
43. JENSEN TK, BONDE JP, JOFFE M. The influence of occupational exposure on male reproductive function. Occupational medicine (Oxford, England) 2006;56:544-53.
44. BHAN A, SARKAR NN. Mercury in the environment: effect on health and reproduction. Reviews on environmental health 2005;20:39-56.
45. SATOH H. Occupational and environmental toxicology of mercury and its compounds. Industrial health 2000;38:153-64.
46. JACKSON LW, HOWARDS PP, WACTAWSKI-WENDE J, SCHISTERMAN EF. The association between cadmium, lead and mercury blood levels and reproductive hormones among healthy, premenopausal women. Human Reproduction 2011;26:2887-95.
47. JURASOVIC J, CVITKOVIC P, PIZENT A, COLAK B, TELISMAN S. Semen quality and reproductive endocrine function with regard to blood cadmium in Croatian male subjects. Biometals : an international journal on the role of metal ions in biology, biochemistry, and medicine 2004;17:735-43.
48. LIN CM, DOYLE P, WANG D, HWANG YH, CHEN PC. Does prenatal cadmium exposure affect fetal and child growth? Occup Environ Med 2011;68:641-6.
49. ELSAMANOUDY AZ, SHAALAN D, GABALLAH MA, EL-ATTA HM, HELALY AMN. Possible effects of metallosis on spermatozoal apoptotic genes expression in individuals with intramedullary nailing prosthesis. Biological Trace Element Research 2014;158:334-41.
50. BOLYARD EA, TABLAN OC, WILLIAMS WW, et al. Guideline for infection control in health care personnel, 1998. Amer J Infect Control 1998;26:269-354.
51. CRUM NF, BALLON-LANDA G. Coccidioidomycosis in Pregnancy: Case Report and Review of the Literature. The American Journal of Medicine 2006;119:993.e11-93.e17.
52. SHEPARD TH. Catalog of Teratogenic Agents, 13th ed. Baltimore: The Johns Hopkins University Press, 2010.
53. SIEGEL JD, RHINEHART E, JACKSON M, CHIARELLO L, THE HEALTHCARE INFECTION CONTROL PRACTICES ADVISORY COMMITTEE. 2007 Guidelines for isolation precautions: Preventing transmission of infectious agents in healthcare settings. Atlanta, GA: Centers for Disease Control and Prevention, 2007.
54. BRUNELL PA. Varicella in Pregnancy, the Fetus, and the Newborn: Problems in Management. The Journal of Infectious Diseases 1992;166:S42-S47.
55. HARRIS RE, RHOADES ER. Varicella pneumonia complicating pregnancy: report of a case and review of literature. Obstetrics and gynecology 1965;25:734-40.
56. CENTERS FOR DISEASE CONTROL AND PREVENTION. Prevention of Varicella: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2007;56.
57. LAWSON CC, WHELAN EA, HIBERT EN, GRAJEWSKI B, SPIEGELMAN D, RICH-EDWARDS JW. Occupational factors and risk of preterm birth in nurses. Am J Obstet Gynecol 2009;200:51.e1-8.
58. WHELAN EA, LAWSON CC, GRAJEWSKI B, HIBERT EN, SPIEGELMAN D, RICH-EDWARDS JW. Work schedule during pregnancy and spontaneous abortion. Epidemiology 2007;18:350-5.
35
Appendix A. Occupational Exposures and Pregnancy
59. LAWSON CC, JOHNSON CY, CHAVARRO JE, et al. Work schedule and physically demanding work in relation to menstrual function: the Nurses' Health Study 3. Scand J Work Environ Health 2015;41:194-203.
60. MACDONALD LA, WATERS TR, NAPOLITANO PG, et al. Clinical guidelines for occupational lifting in pregnancy: evidence summary and provisional recommendations. Am J Obstet Gynecol 2013;209:80-88.
61. FLORACK EI, ZIELHUIS GA, PELLEGRINO JE, ROLLAND R. Occupational physical activity and the occurrence of spontaneous abortion. Int J Epidemiol 1993;22:878-84.
62. VAN BEUKERING MD, VAN MELICK MJ, MOL BW, FRINGS-DRESEN MH, HULSHOF CT. Physically demanding work and preterm delivery: a systematic review and meta-analysis. International archives of occupational and environmental health 2014;87:809-34.
36