Embed Size (px)
Citation preview
2012 ASCO Highlights:Hematologic Malignancies
Wei Ai, M.D., Ph.D.June 2012
A Year of New Agents!
I. Lymphoma: bendamustineII. CLL/SLL: Btk inhibitorIII. Pre-B ALL: Bite biphasic antibodyIV. Multiple Myeloma: Carfilzomib
Lymphomas and CLL/SLL
[TITLE]
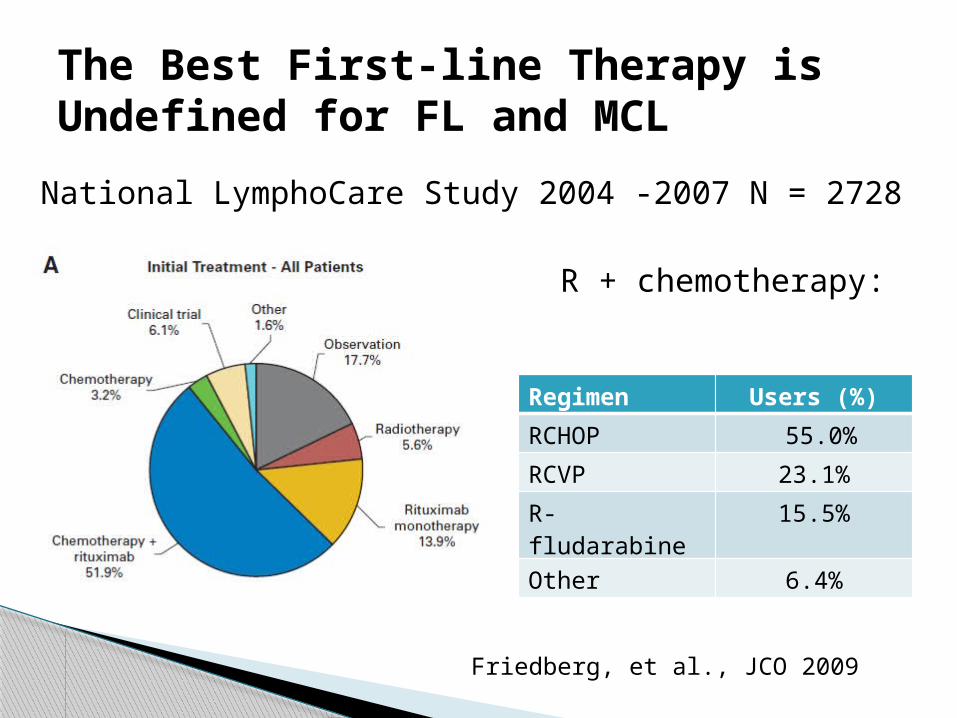
The Best First-line Therapy is Undefined for FL and MCL
National LymphoCare Study 2004 -2007 N = 2728
Friedberg, et al., JCO 2009
R + chemotherapy:
Regimen Users (%)
RCHOP 55.0%
RCVP 23.1%
R-fludarabine 15.5%
Other 6.4%
[TITLE]
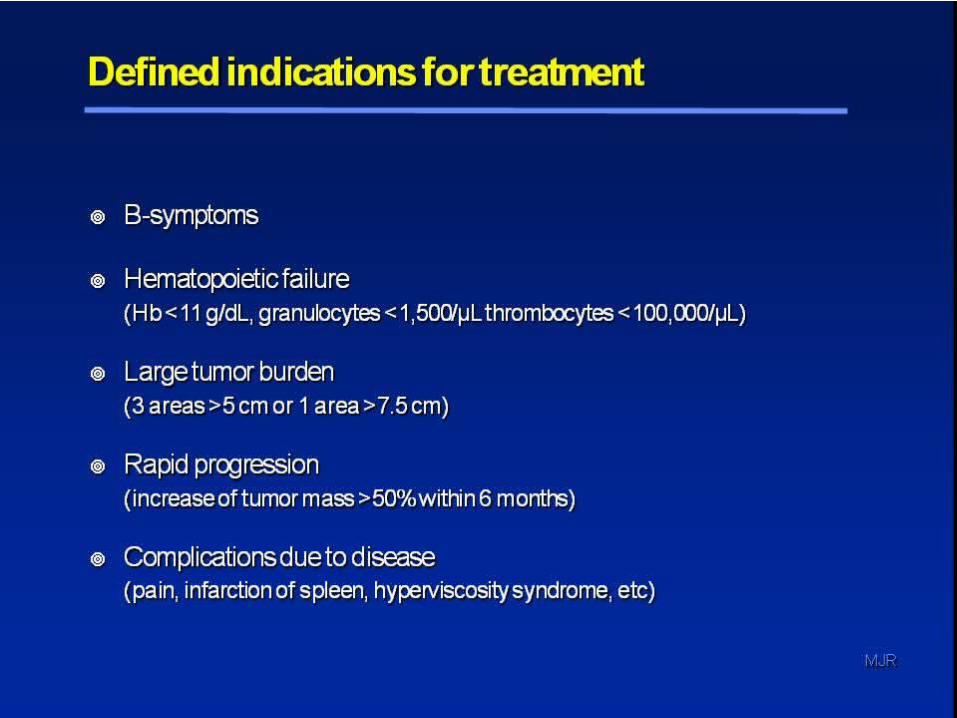
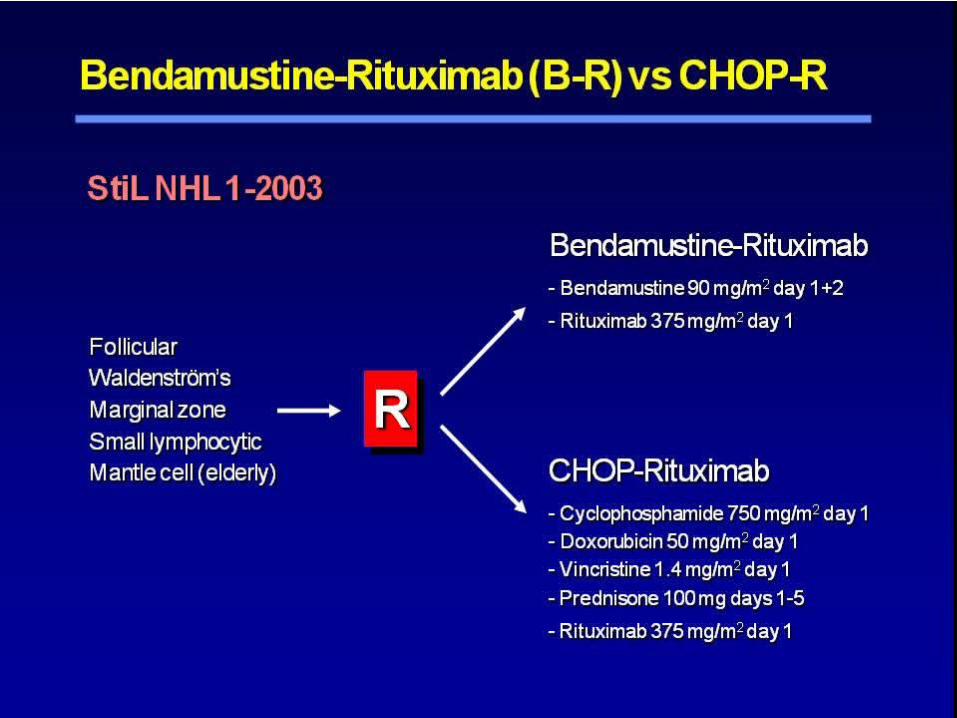
Newly diagnosed indolent lymphoma or mantle cell lymphoma:- Follicular lymphoma (grade 1-3a), small lymphocytic lymphoma, marginal zone lymphoma, wadenstroms, mantle cell lymphoma (elderly)
Stage III and IV Meet criteria for initiating treatment
Major Inclusion Criteria
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
A Phase Ib/II study evaluating activity and tolerability of BTK
inhibitor PIC-32765 and ofatumumab in patients with CLL/SLL and related disease
Samantha Mary Jaglowski, et al.The Ohio State University
BTK inhibitor, an oral agent, showed promising activity as a single agent in untreated elderly pts (>65 yo) with CLL/SLL (John Byrd 2012 ASCO)- N = 26 - ORR 81%, CR 12% with medium f/u 14 mos
Ofatumumab is active in fludarabine- or alemtumumab-refractory CLL/SLL pts: ORR approximately 50%
Background
Wierda, et al., JCO 2010
Ibrutinib 420 mg po qd Oftumumab
- 300 mg C2, day1- 2000 mg C2,days 8, 15, 22- 2000 mg C3, days 1, 8, 15, 22- 2000 mg C4-8, day 1 only
Schema
To determine the toxicity of the combination regimen- Tolerability is defined as no more than 1 DLT in the first 6 pts treated for 2 cycles
To evaluate ORR at one year: N = 27, including the initial 6
Objectives
CLL/SLL or Richter’s transformation Two or more prior therapy, including a
purine analog- containing regimen More than 10% CD20 expression on CLL
cells by flow cytometry Adequate organ functions
Major Eligibility
[TITLE]
[TITLE]
[TITLE]

[TITLE]
[TITLE]
[TITLE]
[TITLE]
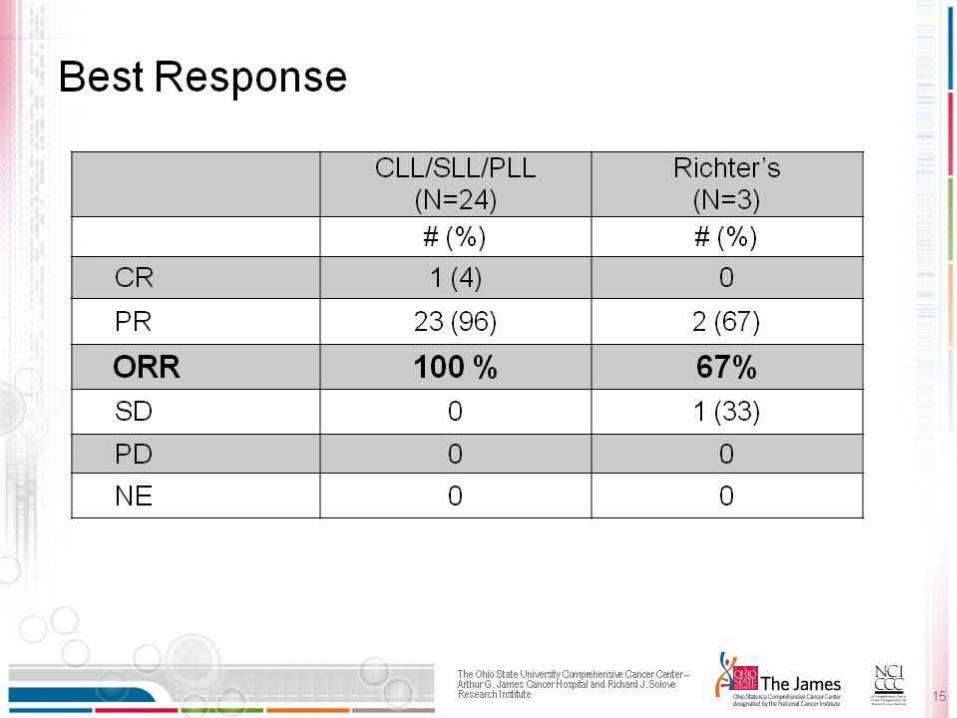
Ibrutinib combined with ofatumumab is a well tolerated and highly active regimen in patients with relapsed and refractory CLL/SLL
Conclusions
Acute Leukemia
Effect of anti-CD19 BiTE blinatumomab on complete remission rate and overall survival in adult patients
with relapsed/refractory pre-B ALL
Max Topp et al.
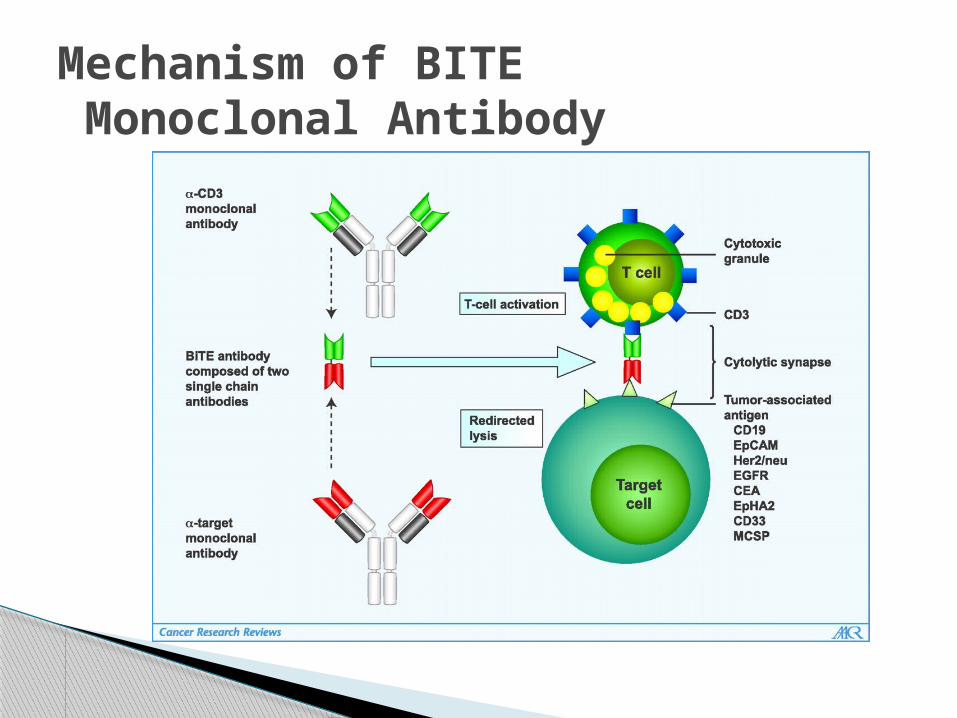
Mechanism of BITE Monoclonal Antibody
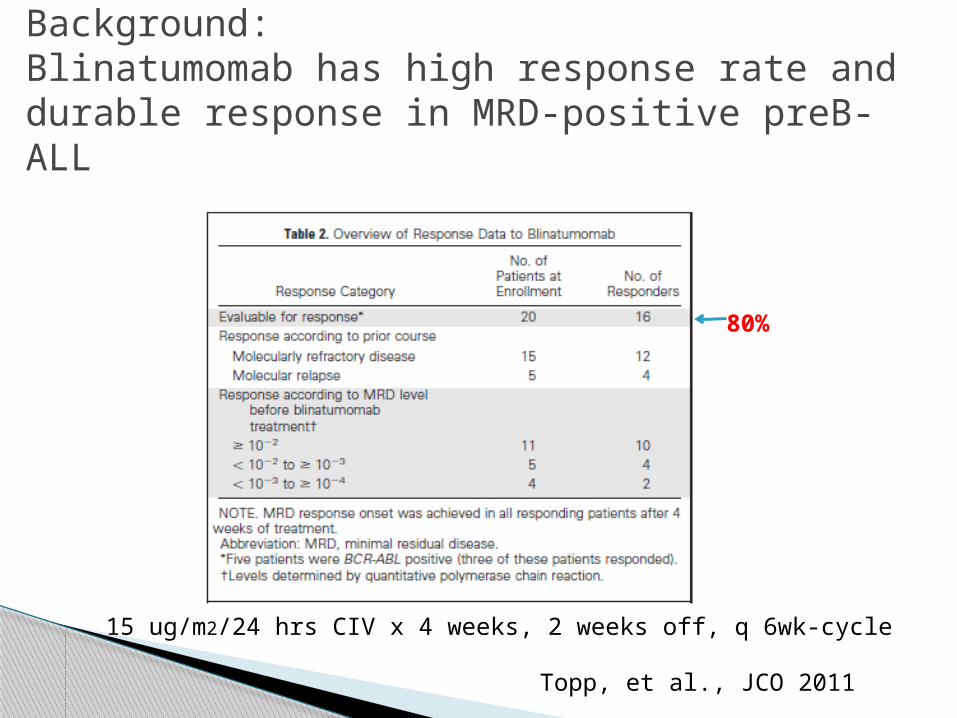
Background:Blinatumomab has high response rate and durable response in MRD-positive preB- ALL
Topp, et al., JCO 2011
80%
15 ug/m2/24 hrs CIV x 4 weeks, 2 weeks off, q 6wk-cycle
Dose-finding Phase:- Cohorts: 1, 2a, 2b
Expansion Phase: Dosing: CIV 4 wks on, 2 wks off, for up to 5
cycles- CR/CRh within the first 2 cycles -> allo
Primary Endpoint: CR/CRh within 2 cycles
Phase II Blinatumumab in R/R ALL: Study Design
R/R ALL, > 5% blasts in BM Ph+ and relapsed after allo were permitted
Key Inclusion Criteria
Selected dose for expansion cohort based on lowest treatment-related AEs (3/5 pts): 5ug/m2/d CIV week 1, then 15ug/m2/d CIV thereafter
Dose-finding Phase
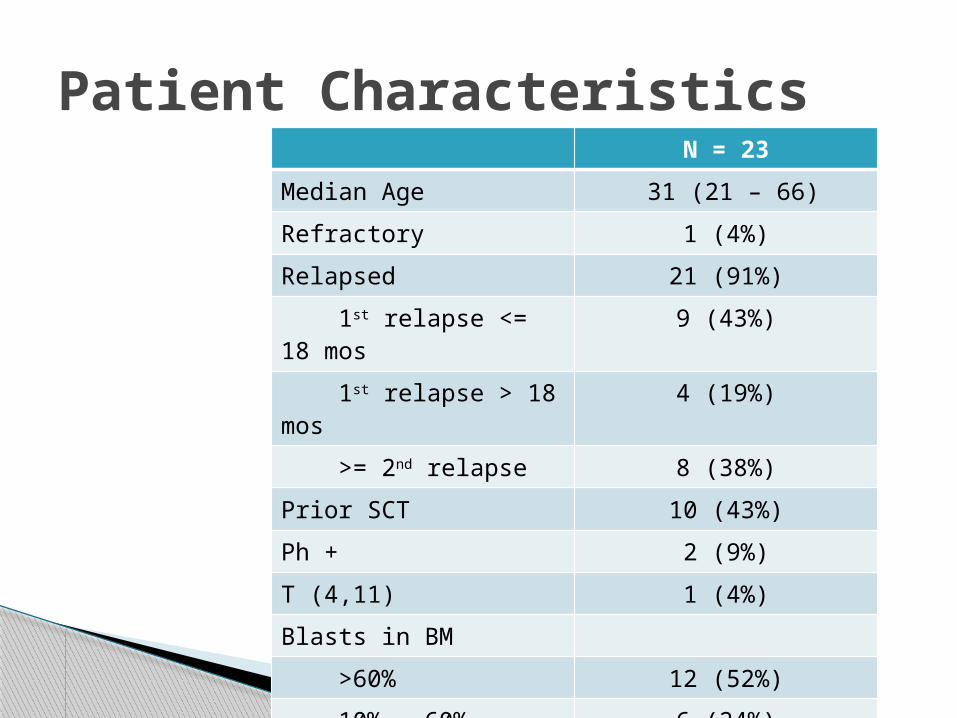
Patient CharacteristicsN = 23
Median Age 31 (21 – 66)
Refractory 1 (4%)
Relapsed 21 (91%)
1st relapse <= 18 mos
9 (43%)
1st relapse > 18 mos 4 (19%)
>= 2nd relapse 8 (38%)
Prior SCT 10 (43%)
Ph + 2 (9%)
T (4,11) 1 (4%)
Blasts in BM
>60% 12 (52%)
10% - 60% 6 (24%)
< 10% 4 (17%)
Cytokine release syndrome- Risks: high tumor burden ans without
cytoreductive phase- Prevention: cytoreduction 5ug/m2 wk 1 and give
Dex for BM>50% CNS Adverse Events:
- 3 seizures and 3 encephalopathy: fully reversible- all 6 pts continued at 5 ug/m2
One pt died of fungal infection
Import Safety Events
CR/CRh: 17/23 pts (74%) All but 2 responders achieved molecular
remission High remission rate in all pt groups,
including Ph+ 13 pts received an allogeneic SCT With a median follow-up of 4.5 months,
median duration of response was 8.9 for all cohorts, not yet reached for the expansion cohort
Results
Well-tolerated at 5 ug/m2/d followed by 15 ug/m2/d CIV, 4 weeks on, 2 weeks off
High hematologic and molecular response rate
Median duration of complete hematologic response was 8.9 months
Median survival was 9 months
Conclusion
Multiple Myeloma
Carfilzomib Coming to the Front-line
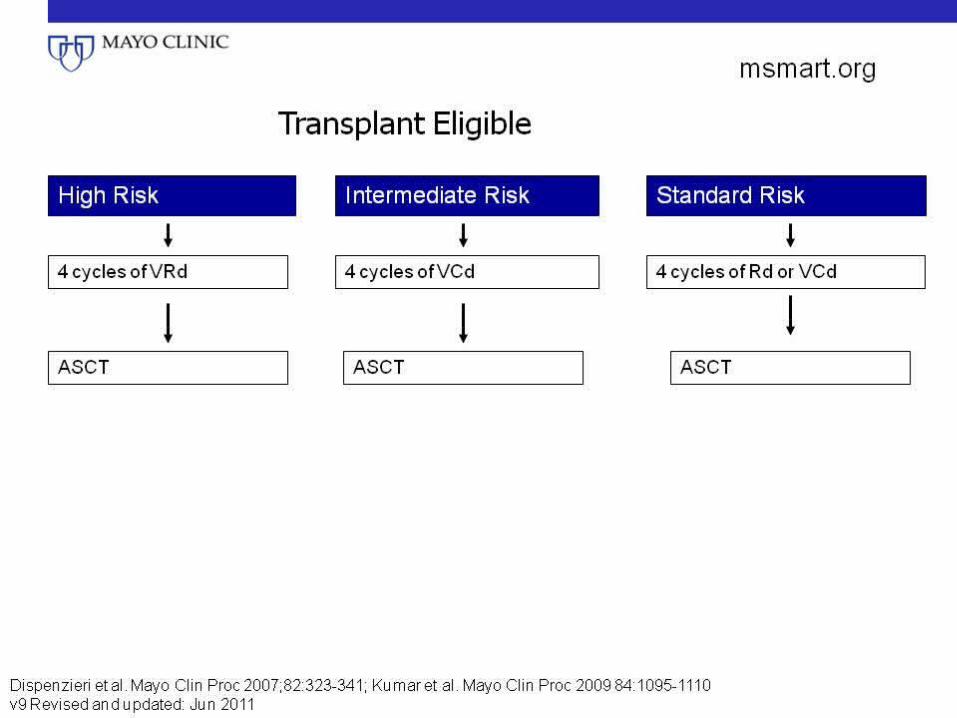
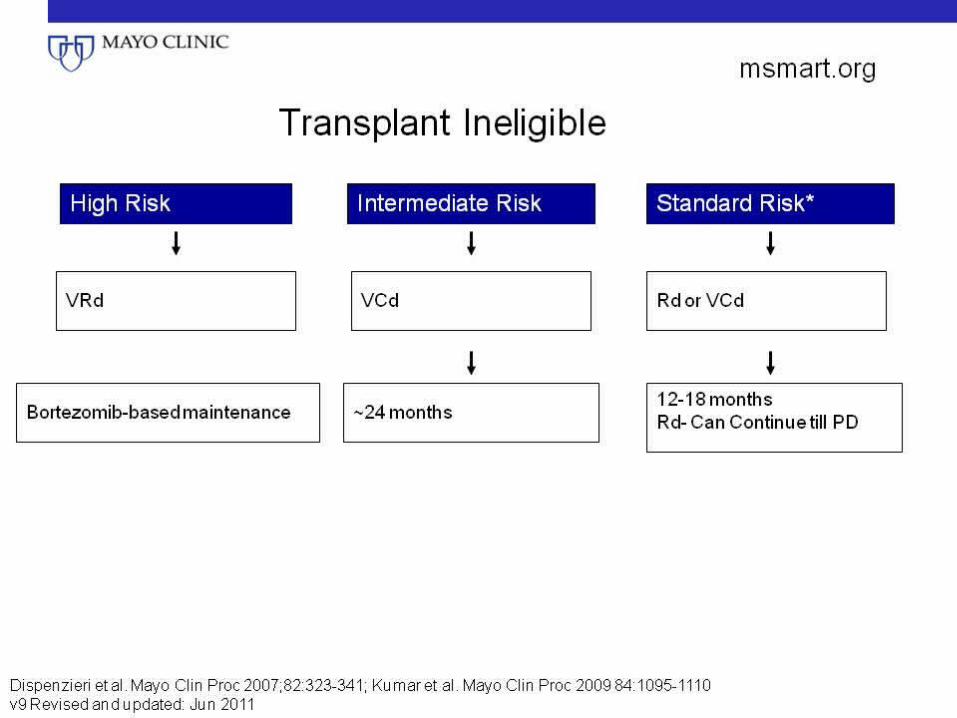
Disease status- High risk, intermediate risk vs low risk- special clinical scenarios: plasma leukemia, renal failure
Patient factors- Transplant eligibility- PS and comorbidity
Clinical benefit- response and OS- QOL
Toxicity and convenience Cost
Principles for Front-line Therapy
[TITLE]
[TITLE]
[TITLE]
[TITLE]
Newly approved second-in-class proteasome inhibitor
Well tolerated, no neurotoxicity Overcome bortezomib resistance in vitro Active alone and in combination regimens
for relapsed/refractory MM
Kuhn et al., Blood 2007, O’Connor Clin Cancer Res 2009, Wang, M et al., JCO 2011 Abstract 8052, Vij, et al., Blood, 2012
Carfilzomaib
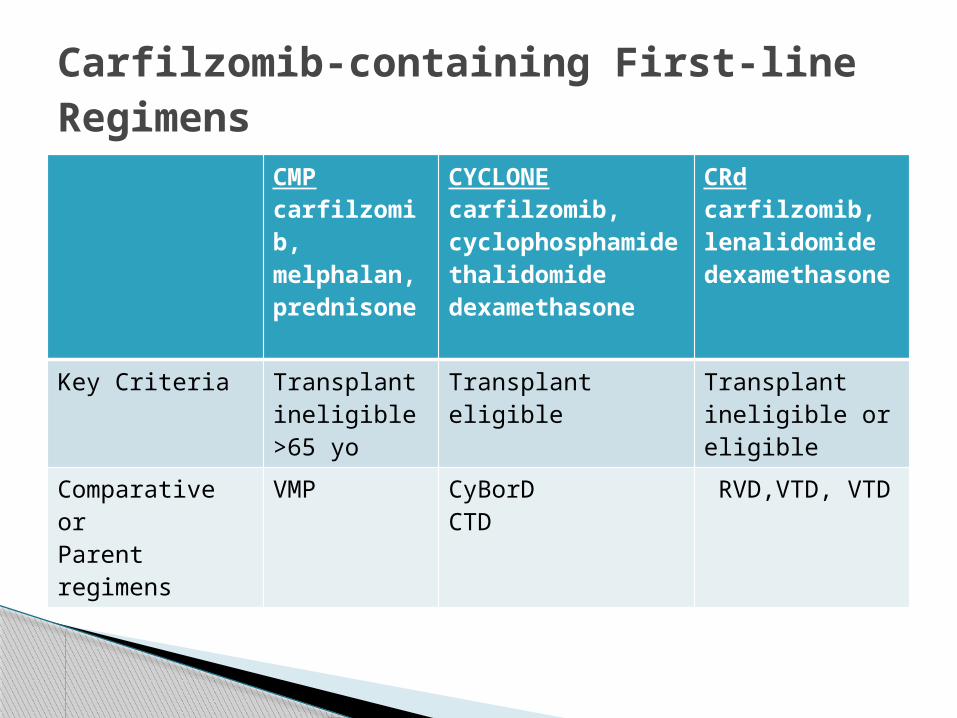
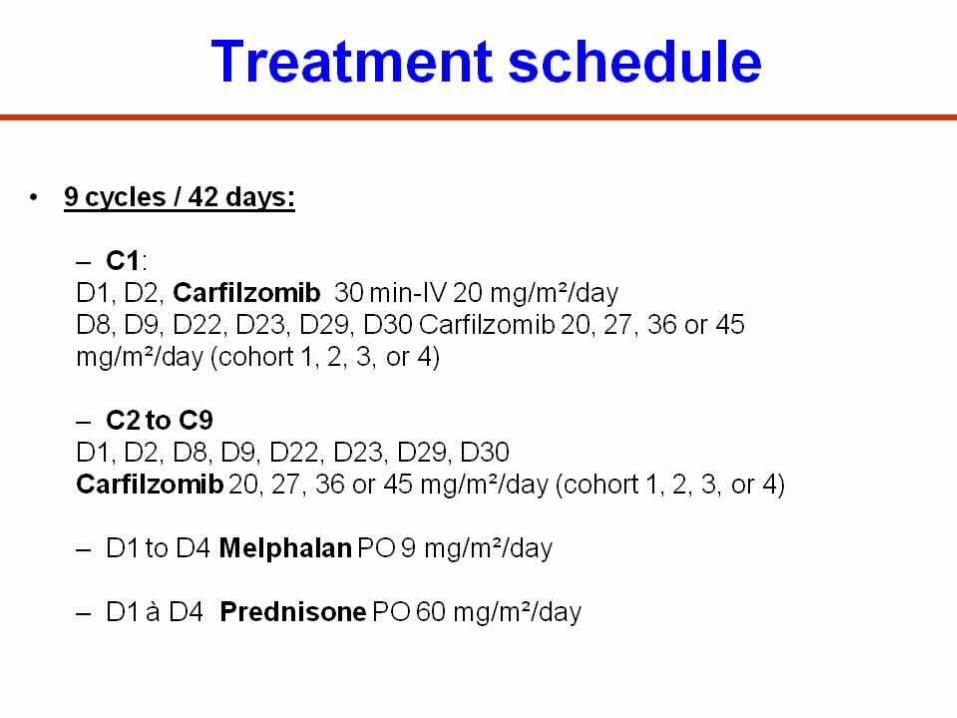
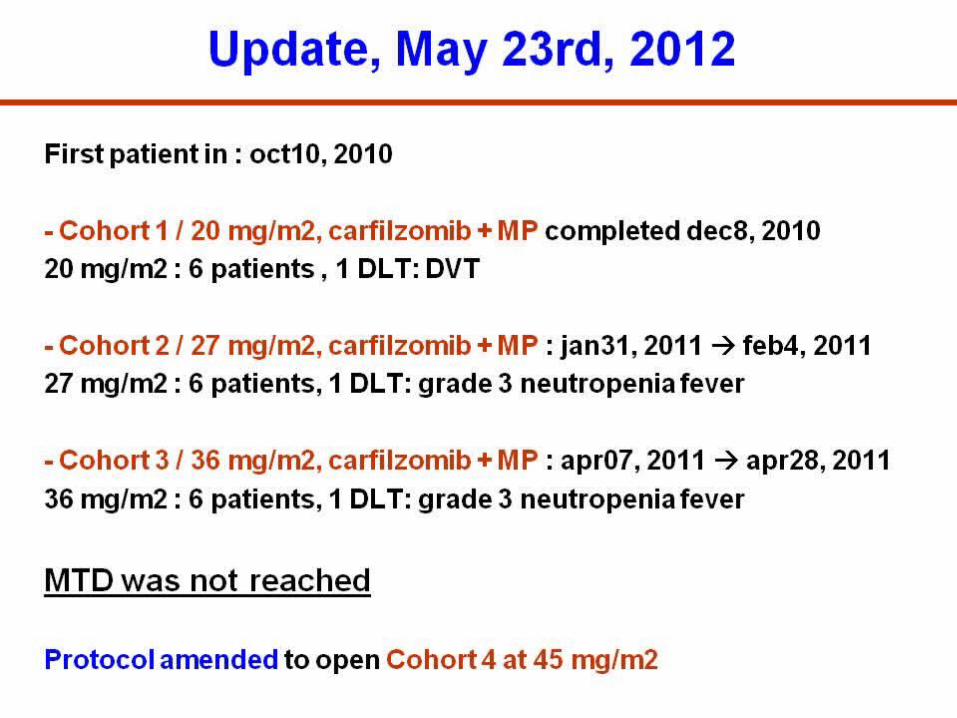
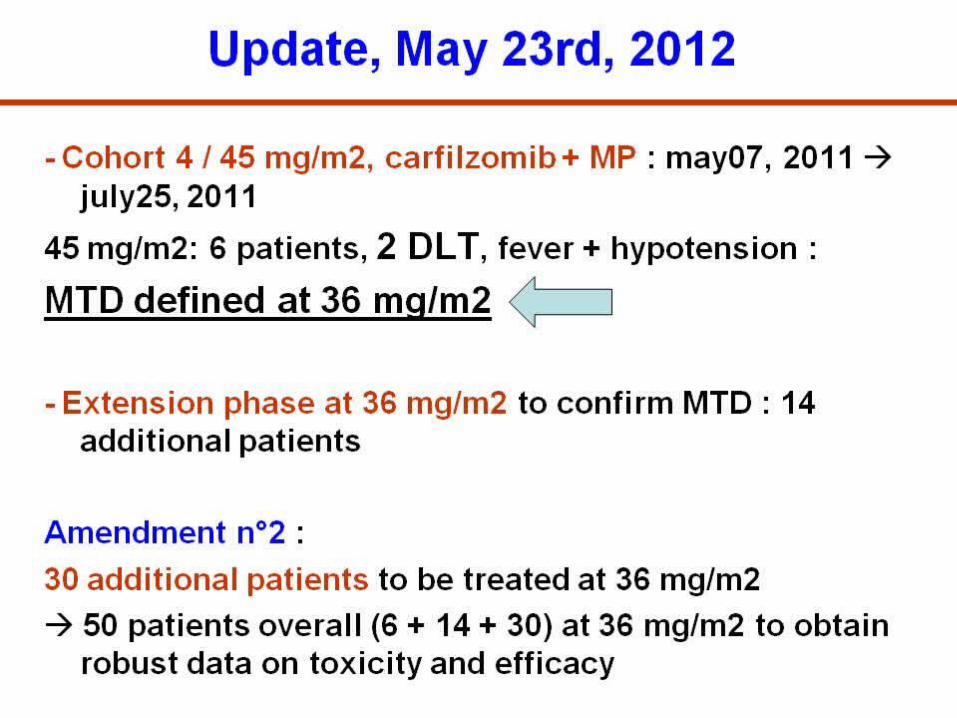
CMPcarfilzomib, melphalan, prednisone
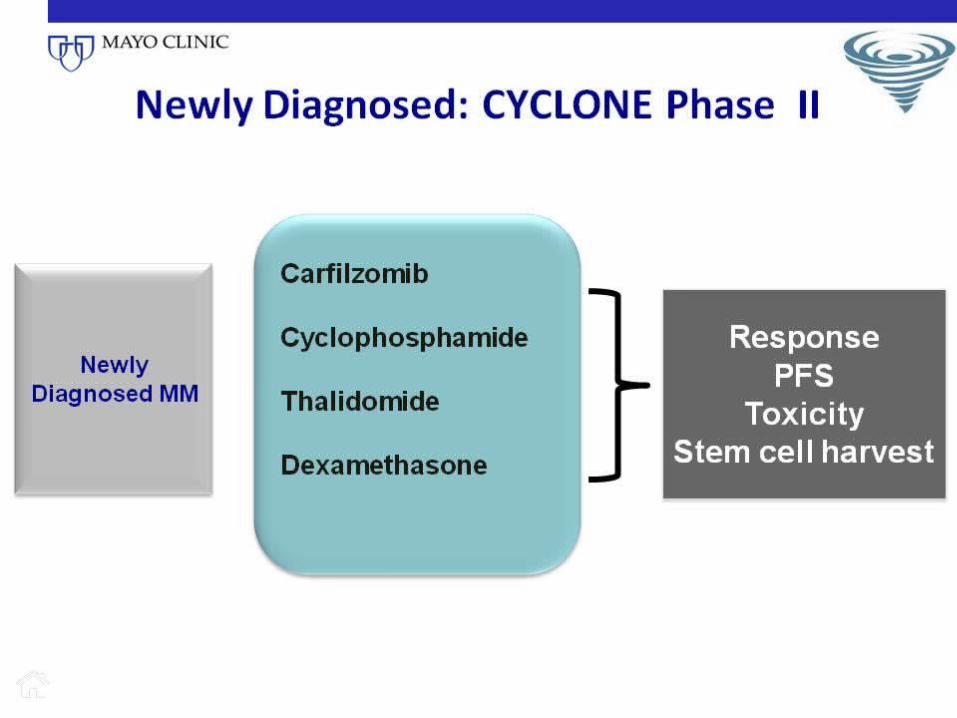
CYCLONEcarfilzomib, cyclophosphamidethalidomidedexamethasone
CRdcarfilzomib,lenalidomidedexamethasone
Key Criteria Transplant ineligible>65 yo
Transplant eligible Transplant ineligible or eligible
Comparative orParent regimens
VMP CyBorDCTD
RVD,VTD, VTD
Carfilzomib-containing First-line Regimens
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
[TITLE]
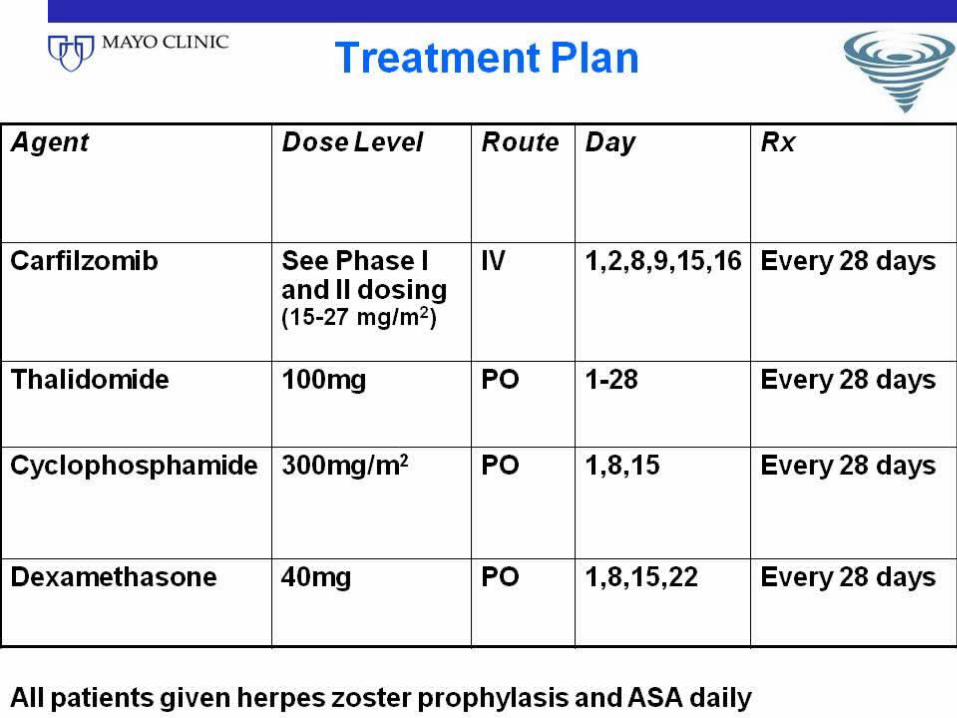
Carfilzomib: 20mg/m2 first week, 27mg/m2 thereafter
Phase II dose
[TITLE]
[TITLE]
[TITLE]
Stringent complete response (sCR) in patients
with newly diagnosed multiple myeloma(NDMM) treated with carfilzomib (CFZ),
lenalidomide (LEN), and dexamethasone (DEX)AJ Jakubowiak,1 K Griffith,2 D Dytfeld,3 DH Vesole,4 S Jagannath,5 T Anderson,2
B Nordgren,2 K Detweiler-Short,2 D Lebovic,2 K Stockerl-Goldstein,6 T Jobkar,2
S Wear, 7 A Al-Zoubi, 2 A Ahmed, 2 M Mietzel, 2 D Couriel, 2 M Kaminski, 2
M Hussein,8 H Yeganegi,9 R Vij6
1University of Chicago, Chicago, IL; 2University of Michigan Comprehensive Cancer Center,Ann Arbor, MI; 3Poznan University of edical Sciences, Poznan, Poland; 4John Theurer CancerCenter, Hackensack, NJ; 5Mount Sinai Medical Center, New York, NY; 6Washington University
School of Medicine, St. Louis, MO; 7Multiple Myeloma Research Consortium, Norwalk, CT;8 Celgene, Inc, Summit, NJ; 9 Onyx Pharmaceuticals, South San Francisco, CA
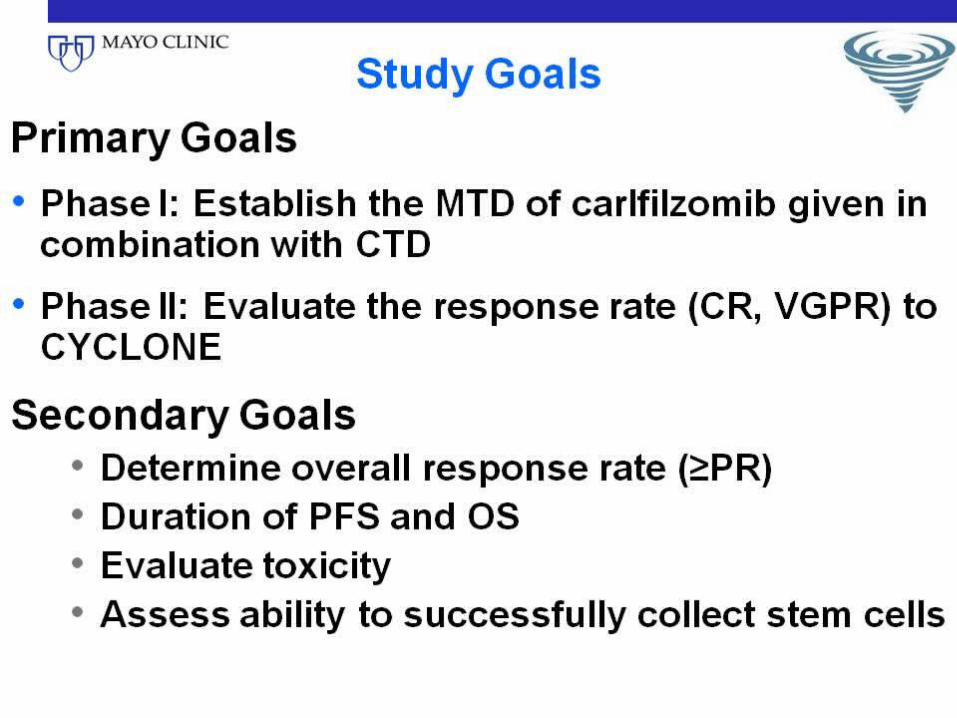
ObjectivesPrimary
• Phase 1: MTD of CRd• Phase 1/2: rate of ≥nCR
Secondary• Overall response rate (≥PR)
• TTP, DOR, PFS, and OS• Tolerability and toxicity
• For transplant candidates, evaluate the impact of CRd onstem cell mobilization• Evaluate prognostic factors and markers of response
4
Eligibility
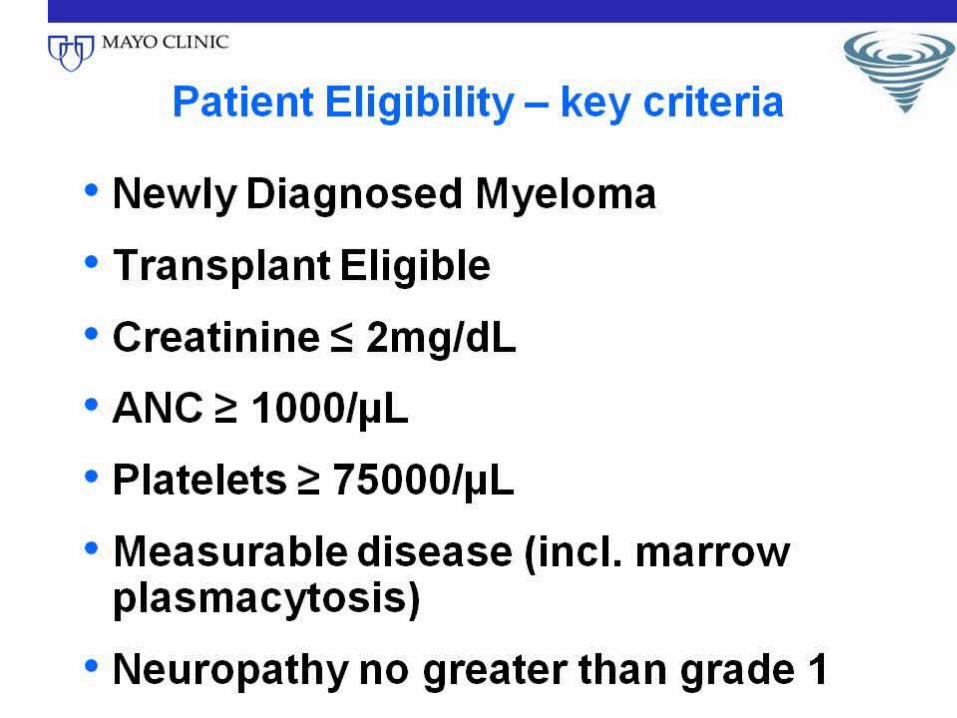
Key inclusion criteria• Newly-diagnosed MM requiring first-line therapy1
- Transplant-eligible and -ineligible
• Measurable disease per IMWG Criteria1
• ECOG performance status 0-2
Key exclusion criteria• Grade 3/4 peripheral neuropathy
• ANC <1.0x109/L, Hgb <8.0 g/dL, platelets <75,000/µL• Creatinine clearance <50 mL/min or serum creatinine ≥2 g/dL
• Serious co-morbidities
1. Durie BGM, et al. Leukemia. 2006;20:1467-1473.5
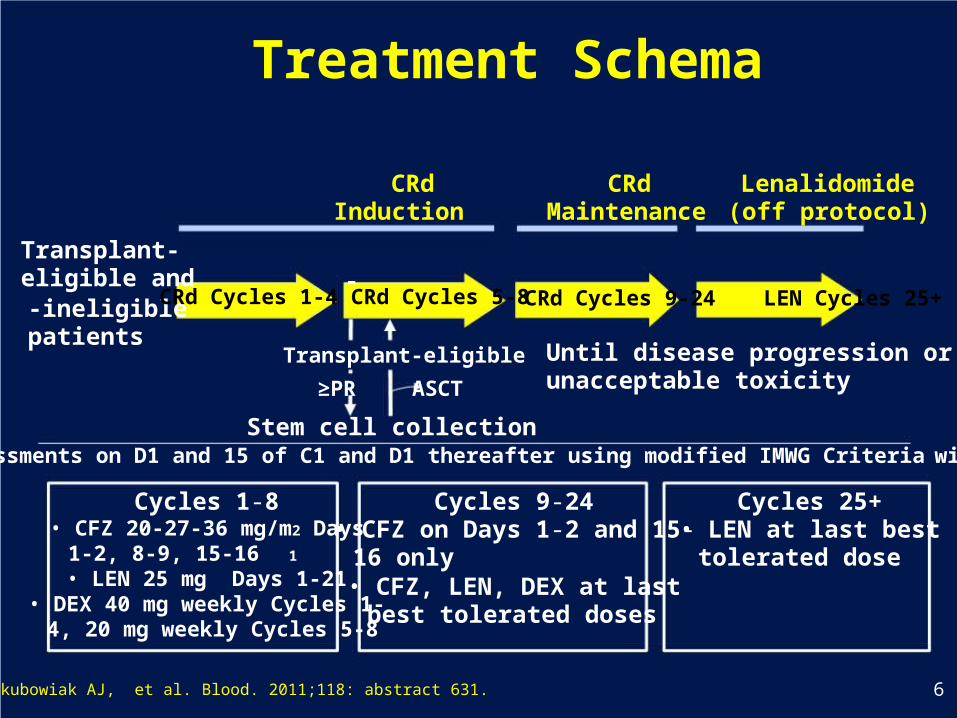
Treatment Schema
Transplant-eligible and-ineligiblepatients
CRdInduction
-CRd Cycles 1-4 CRd Cycles 5-8
Transplant-eligible
≥PR ASCT
Stem cell collection
CRd LenalidomideMaintenance (off protocol)
CRd Cycles 9-24 LEN Cycles 25+
Until disease progression orunacceptable toxicity
• Assessments on D1 and 15 of C1 and D1 thereafter using modified IMWG Criteria with nCR
Cycles 1-8• CFZ 20-27-36 mg/m2 Days
1-2, 8-9, 15-16 1
• LEN 25 mg Days 1-21• DEX 40 mg weekly Cycles 1-
4, 20 mg weekly Cycles 5-8
Cycles 9-24• CFZ on Days 1-2 and 15-
16 only• CFZ, LEN, DEX at last
best tolerated doses
Cycles 25+• LEN at last best
tolerated dose
1. Jakubowiak AJ, et al. Blood. 2011;118: abstract 631. 6
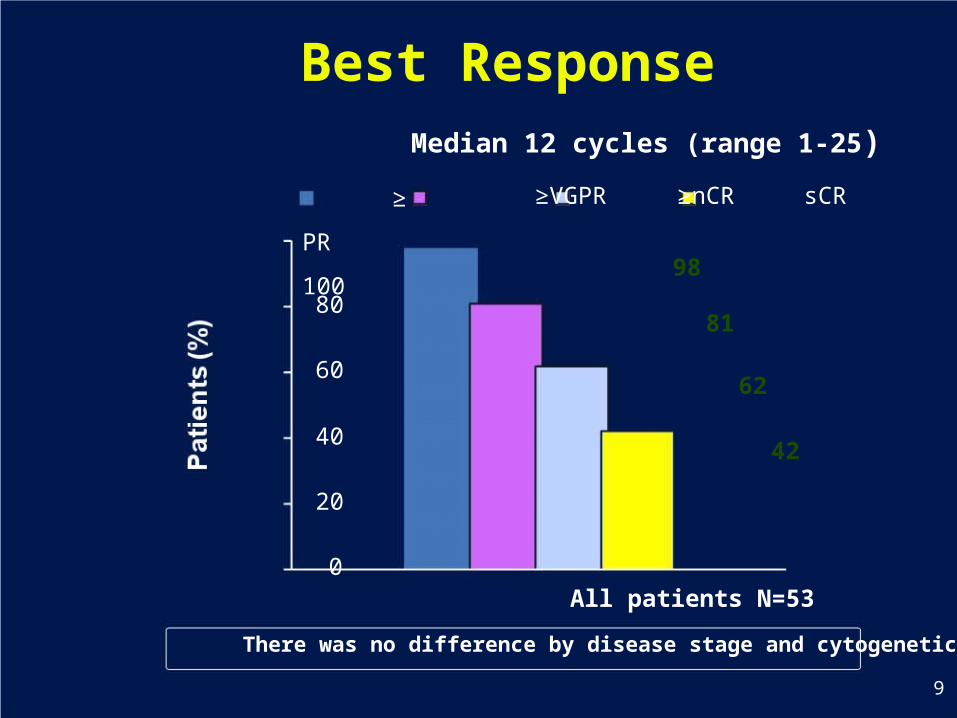
Best ResponseMedian 12 cycles (range 1-25)
≥
PR
10080
60
40
20
0
≥VGPR ≥nCR sCR
98
81
62
42
All patients N=53
There was no difference by disease stage and cytogenetics
9
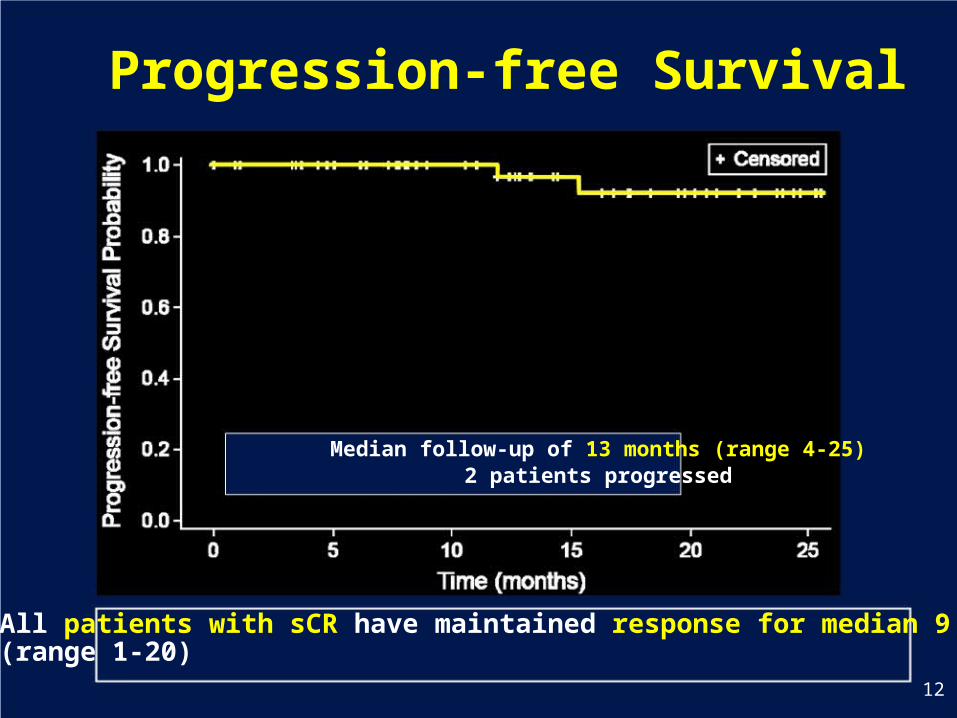
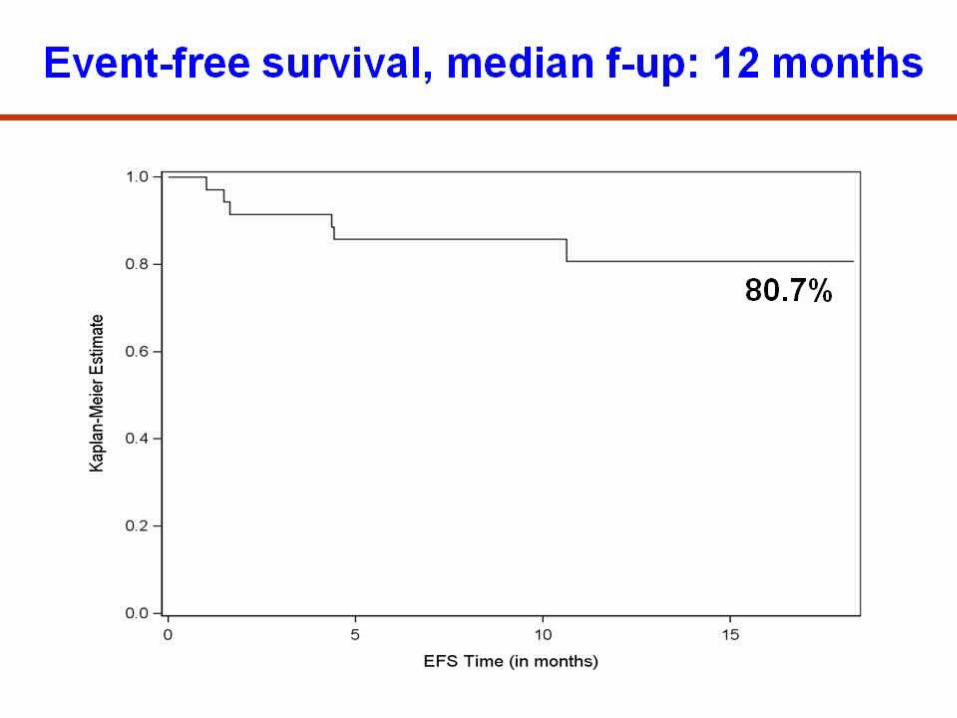
Progression-free Survival
Median follow-up of 13 months (range 4-25)2 patients progressed
All patients with sCR have maintained response for median 9 months(range 1-20)
12
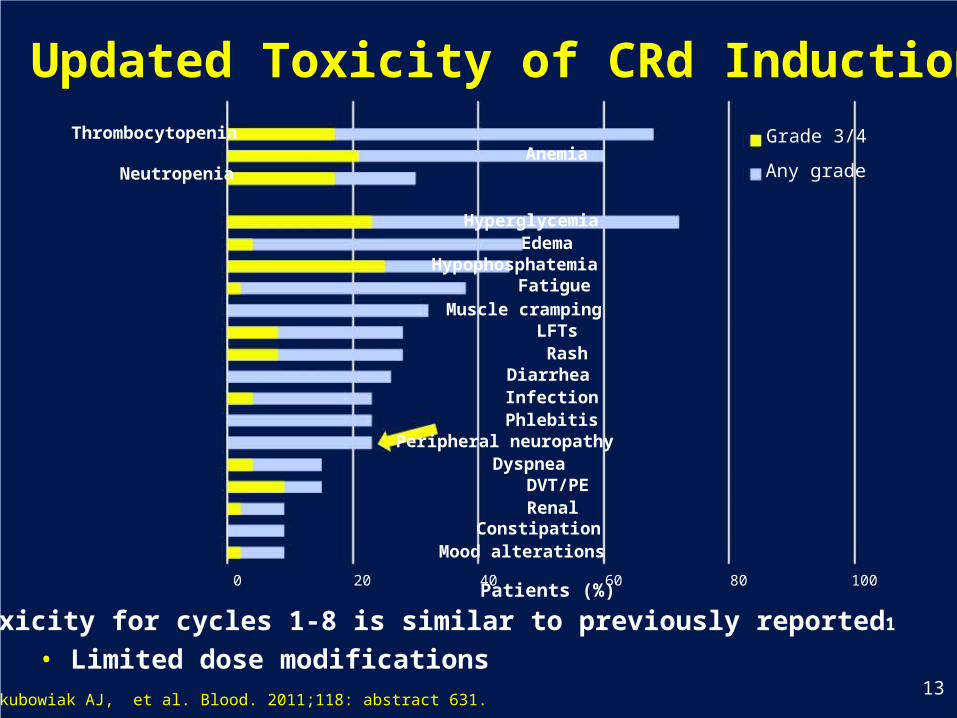
Updated Toxicity of CRd InductionThrombocytopenia Grade 3/4
AnemiaNeutropenia Any grade
HyperglycemiaEdema
HypophosphatemiaFatigue
Muscle crampingLFTsRash
DiarrheaInfectionPhlebitis
Peripheral neuropathyDyspnea
DVT/PERenal
ConstipationMood alterations
0 20 40 60 80 100Patients (%)
• Toxicity for cycles 1-8 is similar to previously reported1
• Limited dose modifications1. Jakubowiak AJ, et al. Blood. 2011;118: abstract 631.
13
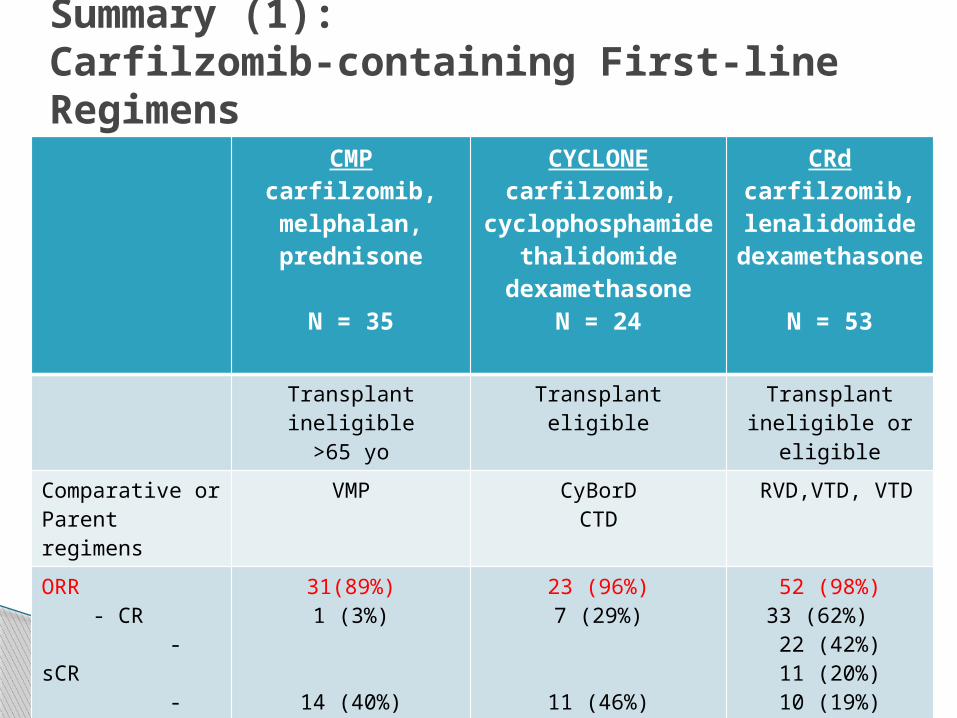
CMPcarfilzomib, melphalan, prednisone
N = 35
CYCLONEcarfilzomib,
cyclophosphamide
thalidomidedexamethasone
N = 24
CRdcarfilzomib,lenalidomidedexamethaso
ne
N = 53
Transplant ineligible>65 yo
Transplant eligible Transplant ineligible or
eligible
Comparative orParent regimens
VMP CyBorDCTD
RVD,VTD, VTD
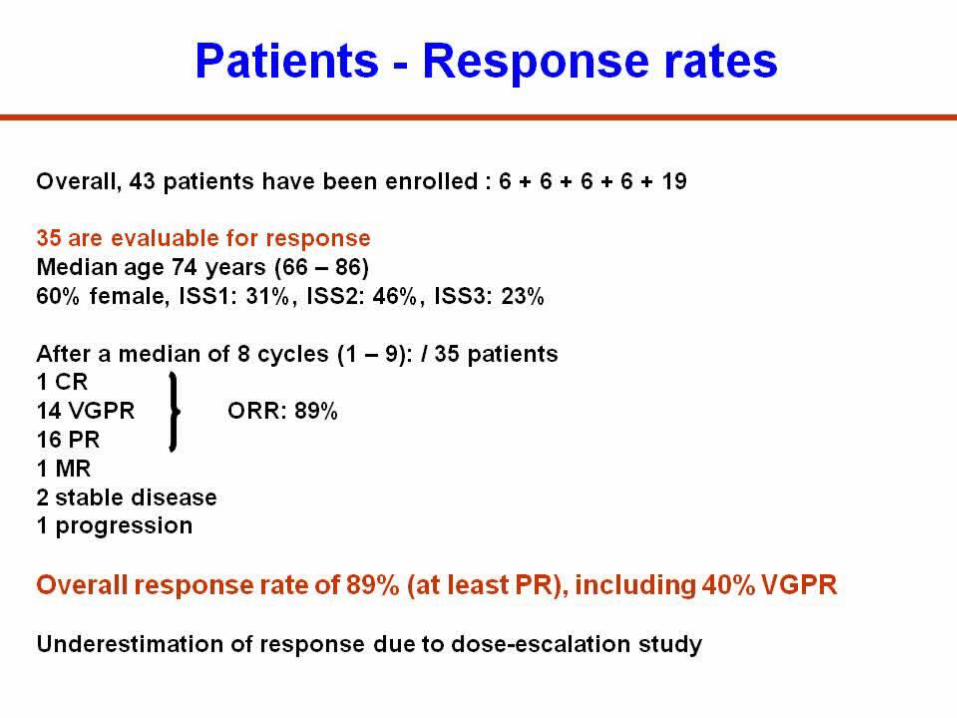
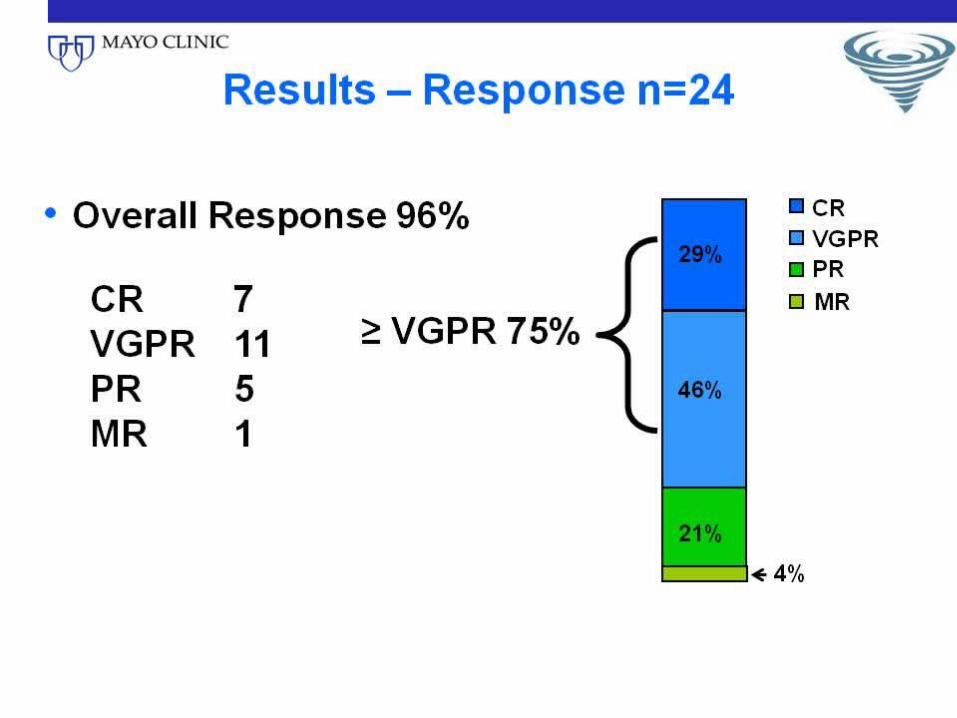
ORR - CR - sCR - nCR - VGPR - PR
31(89%)1 (3%)
14 (40%)16 (46%)
23 (96%)7 (29%)
11 (46%)5 (21%)
52 (98%)33 (62%) 22 (42%)11 (20%)10 (19%)9 (17%)
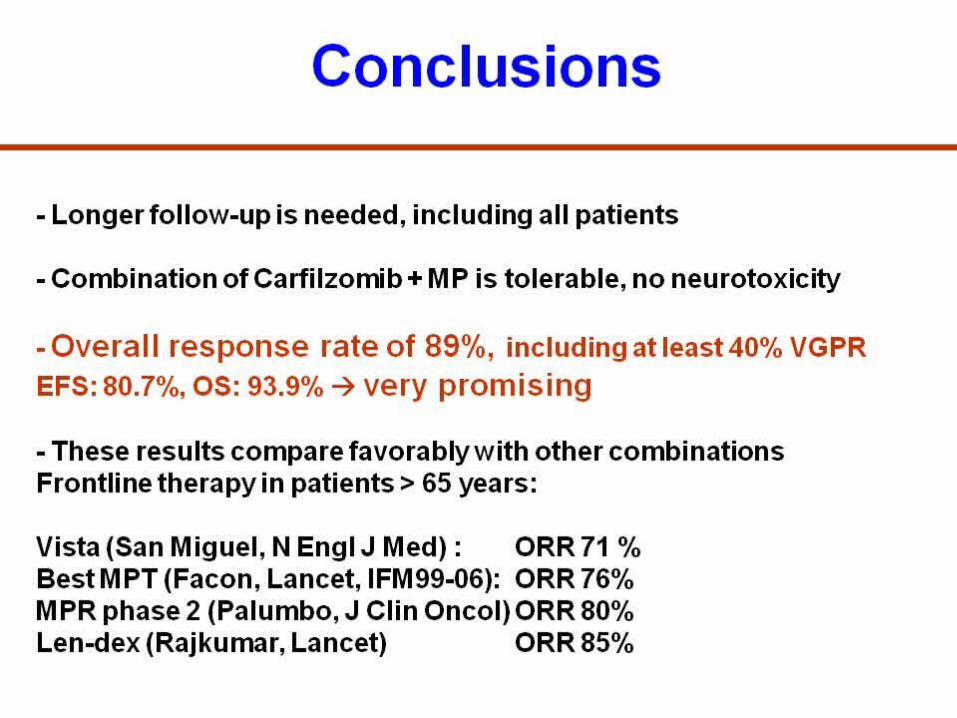
Summary (1):Carfilzomib-containing First-line Regimens
Highly active as a first-line treatment for MM
The quality of response seems improved in some studies
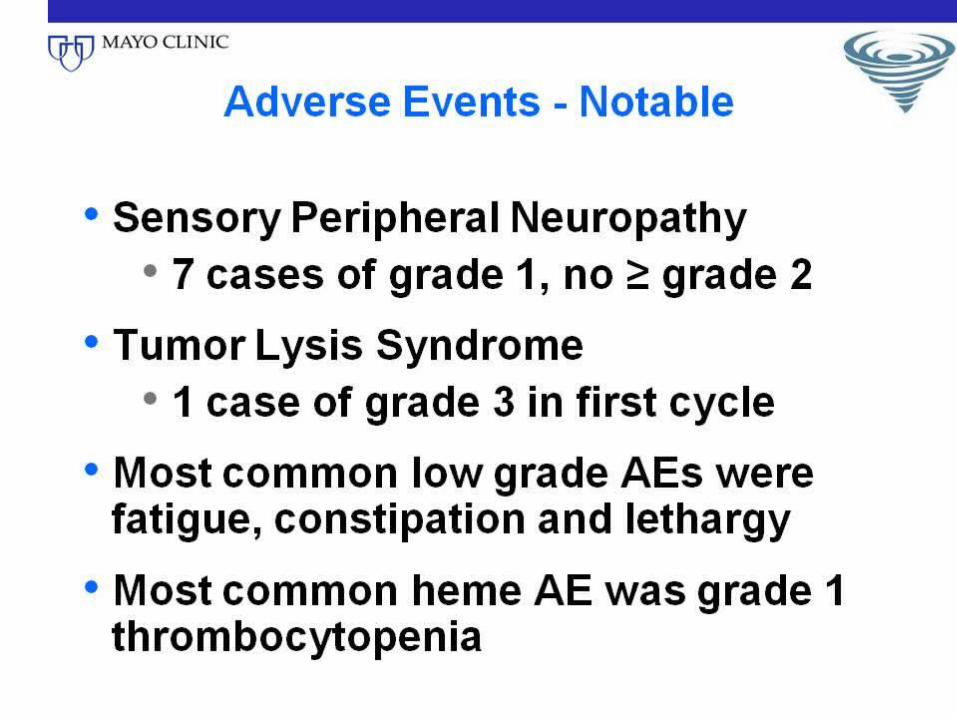
Tolerability seems improved with minimum peripheral neuropathy, although comparison with SQ bortezomib remain to be investigated
Summary (2):Carfilzomib-containing First-line Regimens
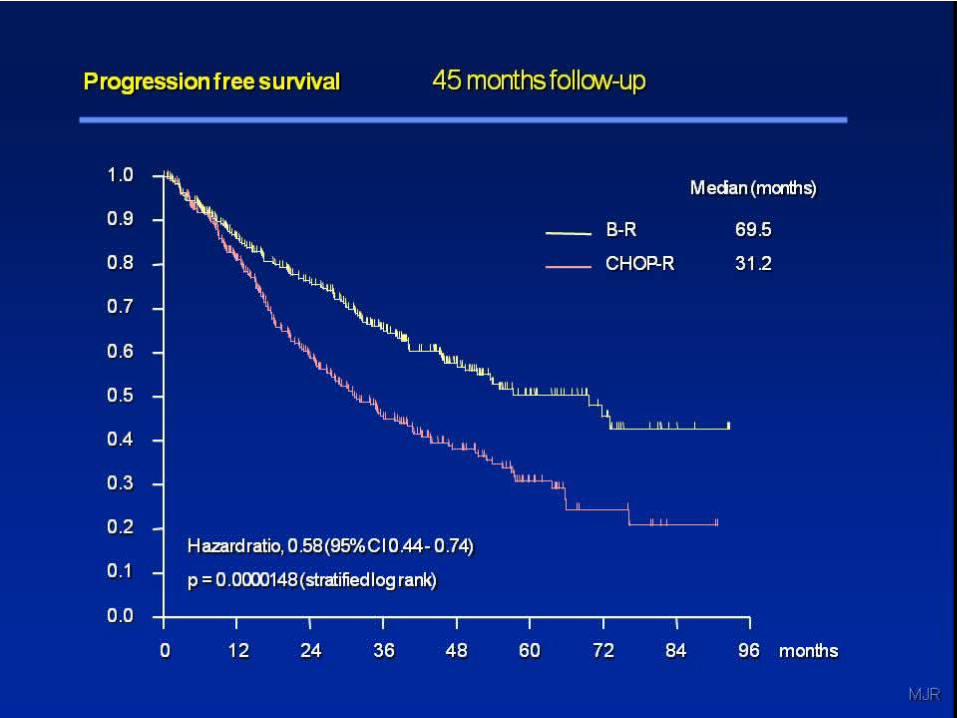
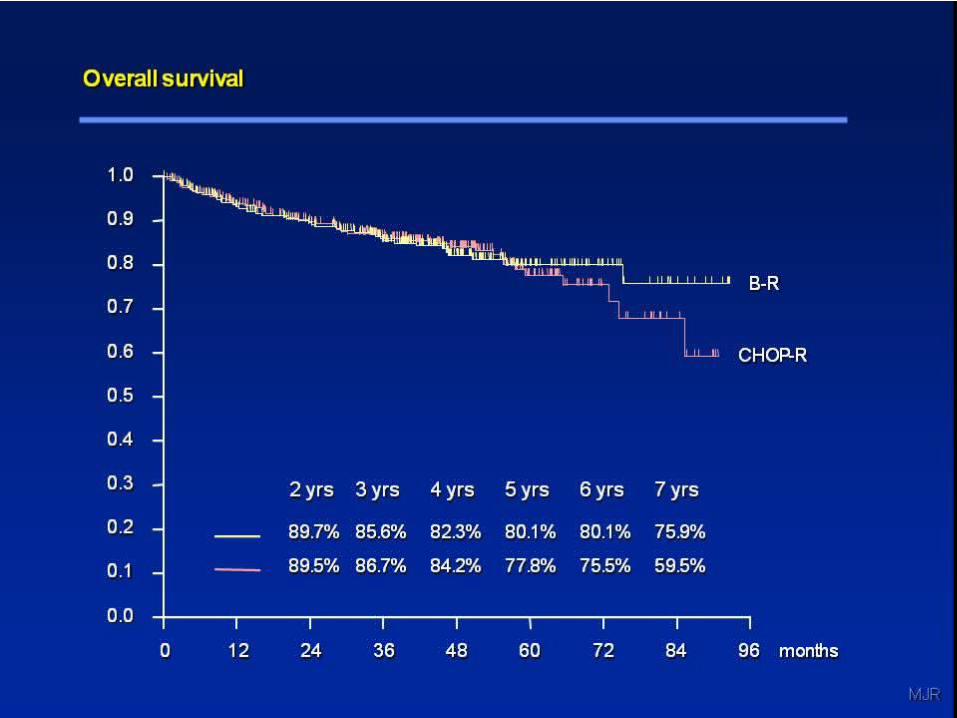
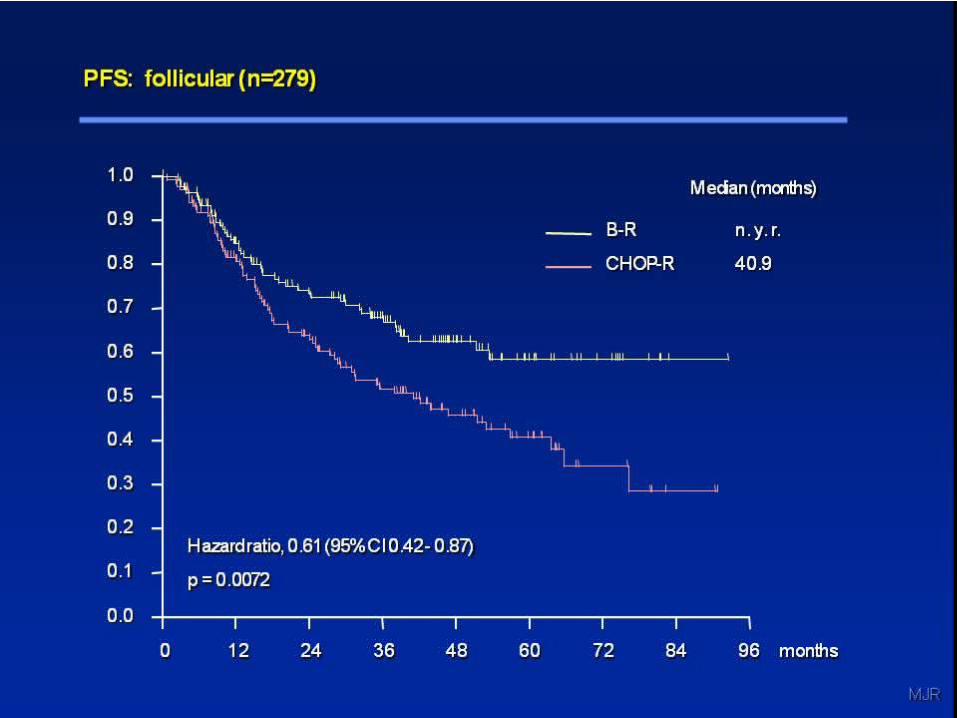
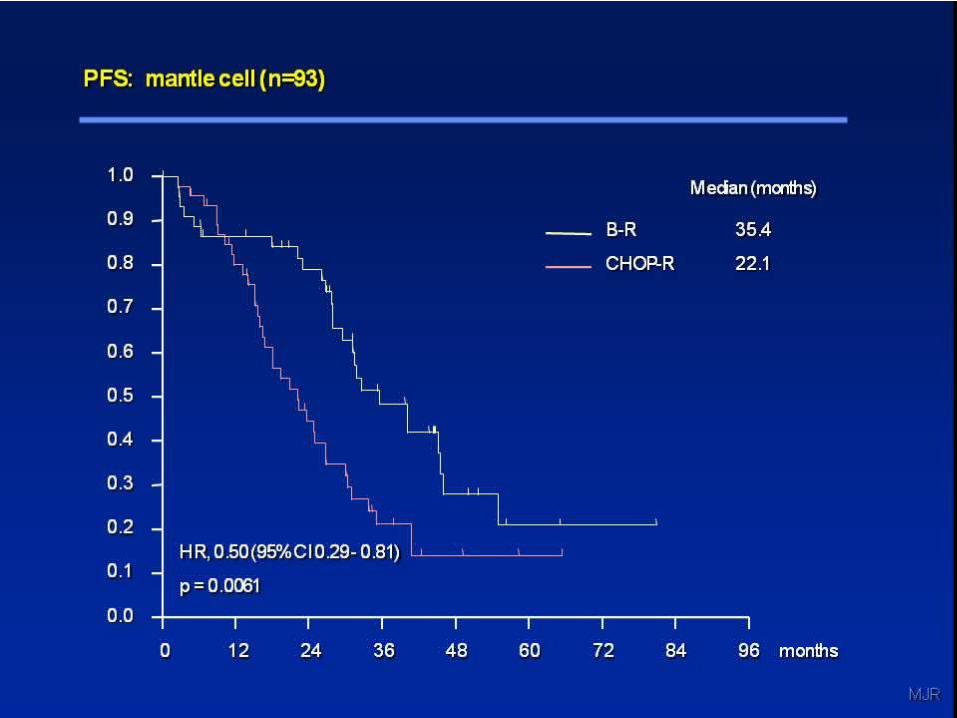
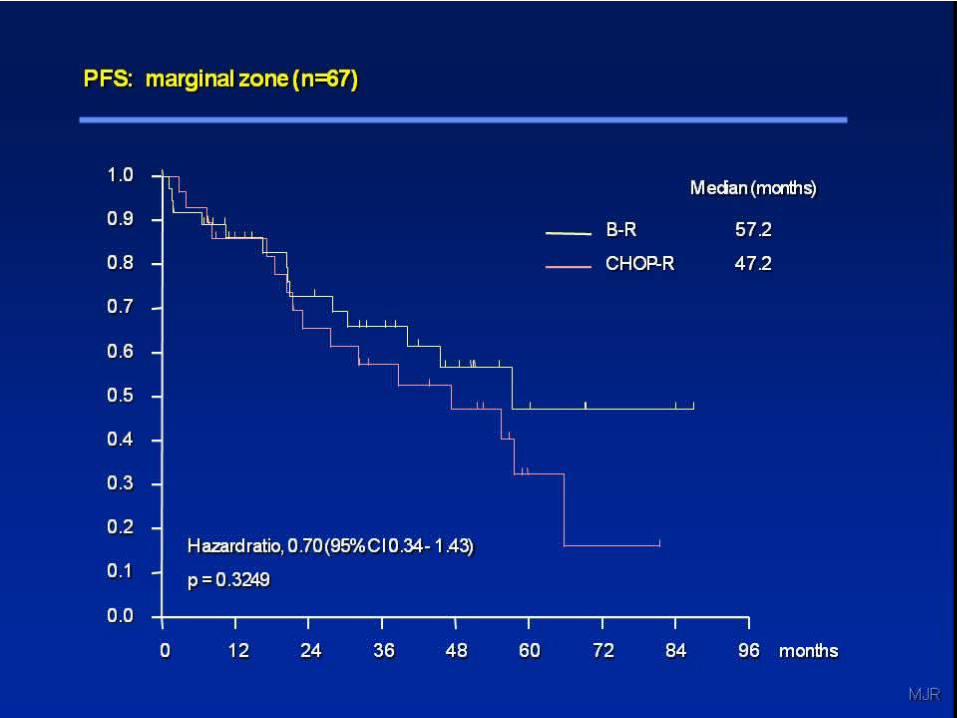
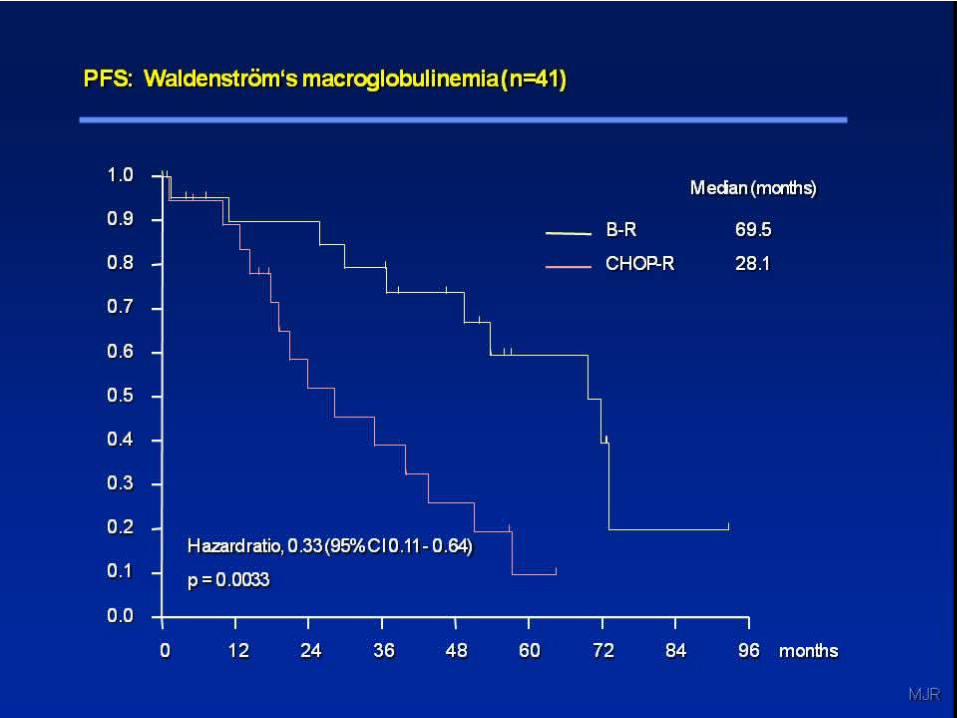
Lymphoma and CLL/SLL The Stil trial established R-Benda as the
preferred first-line treatment for FL and MCL Ofatumumab + ibrutinib (Btk inhibitor) is
highly active in relapsed/refractory CLL/SLL Acute Leukemia
Blinatumumab (Bite biphasic antibody) is highly active in relapsed/refractory ALL
Multiple MyelomaCarfilzomib is moving to the front line
Summary
Thank you
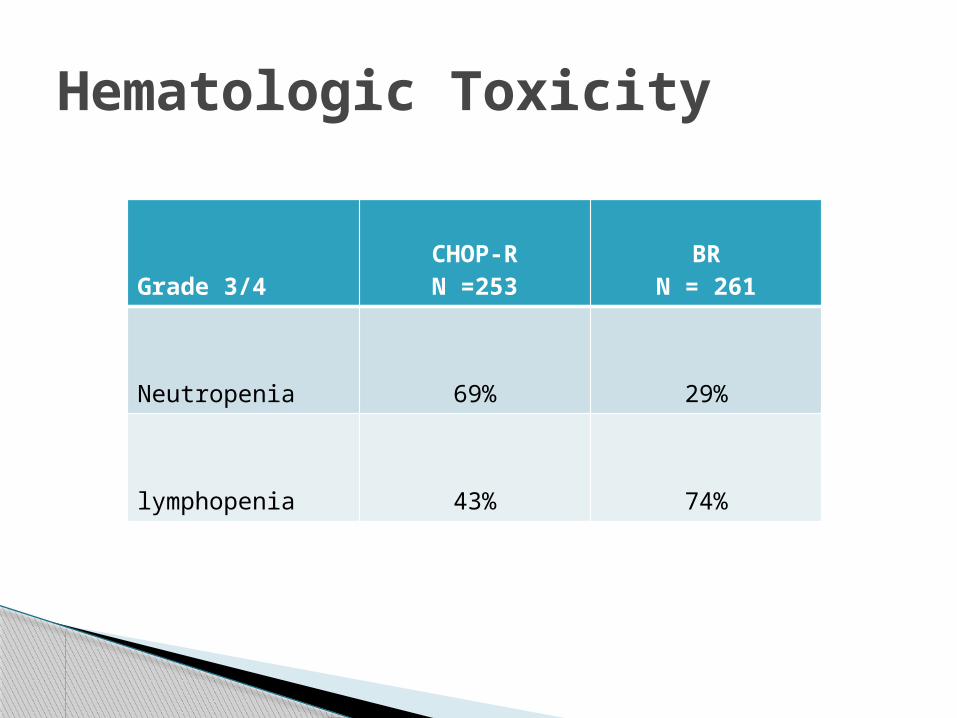
Hematologic Toxicity
Grade 3/4CHOP-RN =253
BRN = 261
Neutropenia 69% 29%
lymphopenia 43% 74%
[TITLE]
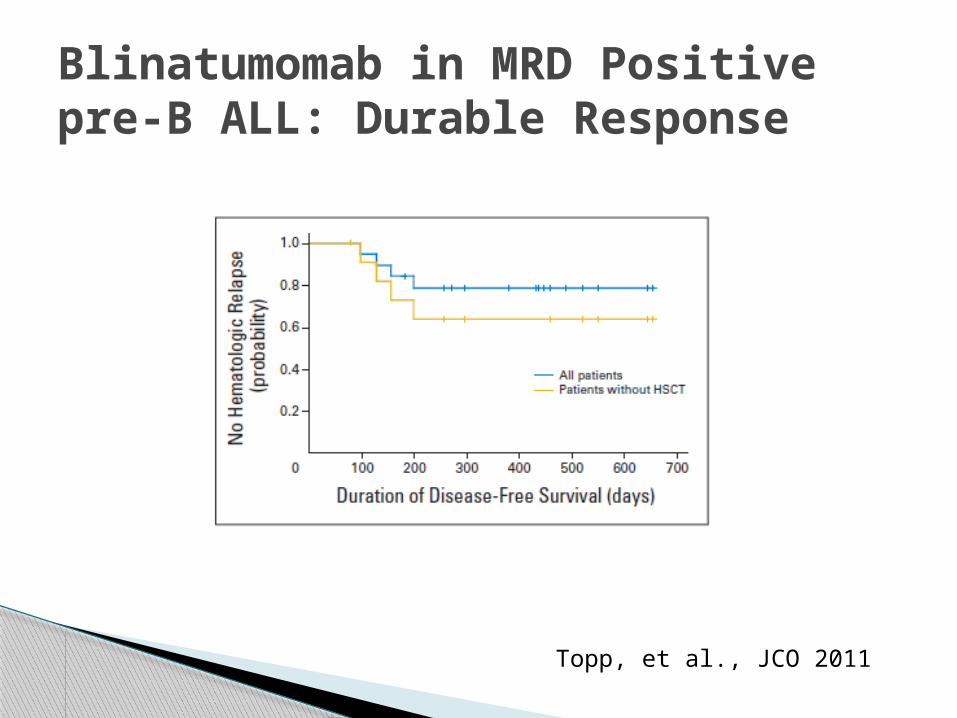
Blinatumomab in MRD Positivepre-B ALL: Durable Response
Topp, et al., JCO 2011