Embed Size (px)
Citation preview
Weighing the Options for Anticoagulation in ObesityCaitlin S. Brown, PharmD
Pharmacy Grand RoundsMay 24, 2016
Objectives• Review pharmacokinetic changes in obesity
• Discuss dosing and monitoring strategies when using low molecular weight heparin
• Outline evidence and recommendations for utilization of direct oral anticoagulants

Overweight Adults in the United States
69%
31%
BMI ≥ 25kg/m2 BMI < 25kg/m2
Ogden CL, et al. JAMA. 2014;311:806-814.Overweight & Obesity. CDC. http://www.cdc.gov/obesity/. BMI = Body mass index
Obese Adults in the United States
35%
65%
BMI ≥30kg/m2 BMI <30kg/m2
Ogden CL, et al. JAMA. 2014;311:806-814.
1 in 3 adults you take care of will be obese
Overweight & Obesity. CDC. http://www.cdc.gov/obesity/.

What Will Obesity in the U.S. Be In The Future?
32%37%
41%46%
51%
0%
10%
20%
30%
40%
50%
60%
2010 2015 2020 2025 2030
Obe
se In
divi
dual
s
Year
Finkelstein EA, et al. Am J Prev Med. 2012;42:563-570.
Pharmacokinetics in Obesity
Volume of Distribution
(Vd)
Elimination Half-Life
(T1/2)
Clearance(CL)
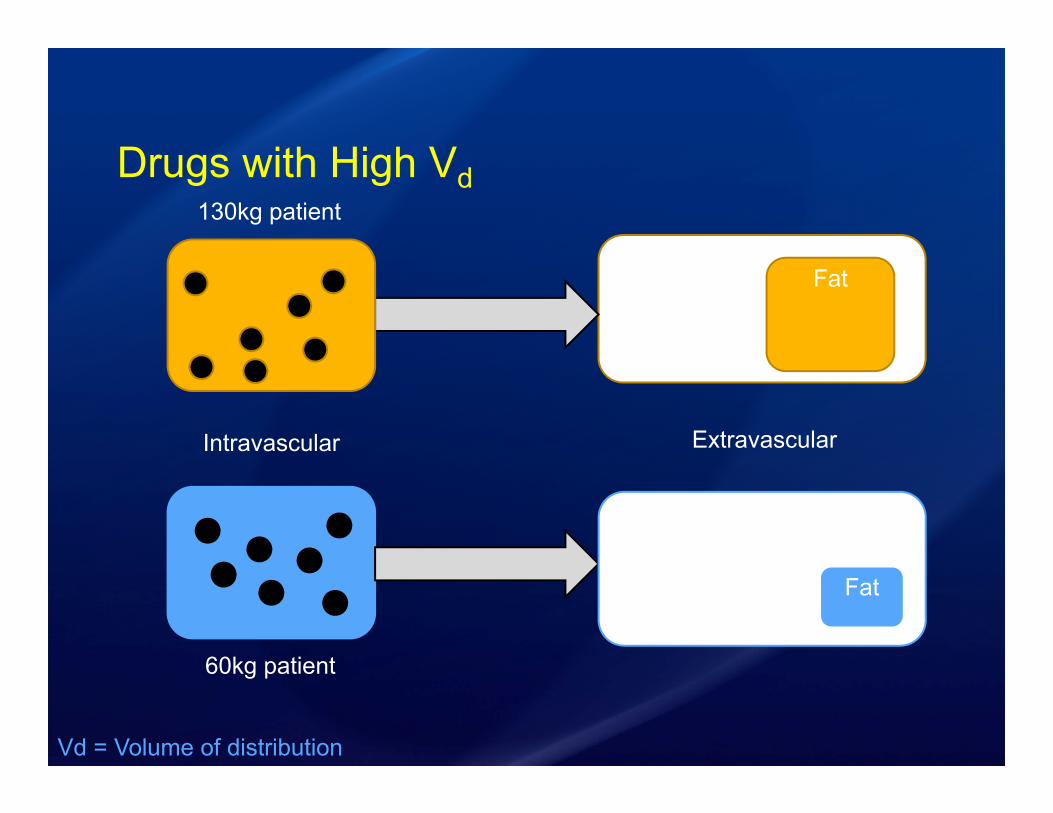
Drugs with High Vd
60kg patient
130kg patient
Intravascular Extravascular
Fat
Fat
Vd = Volume of distribution
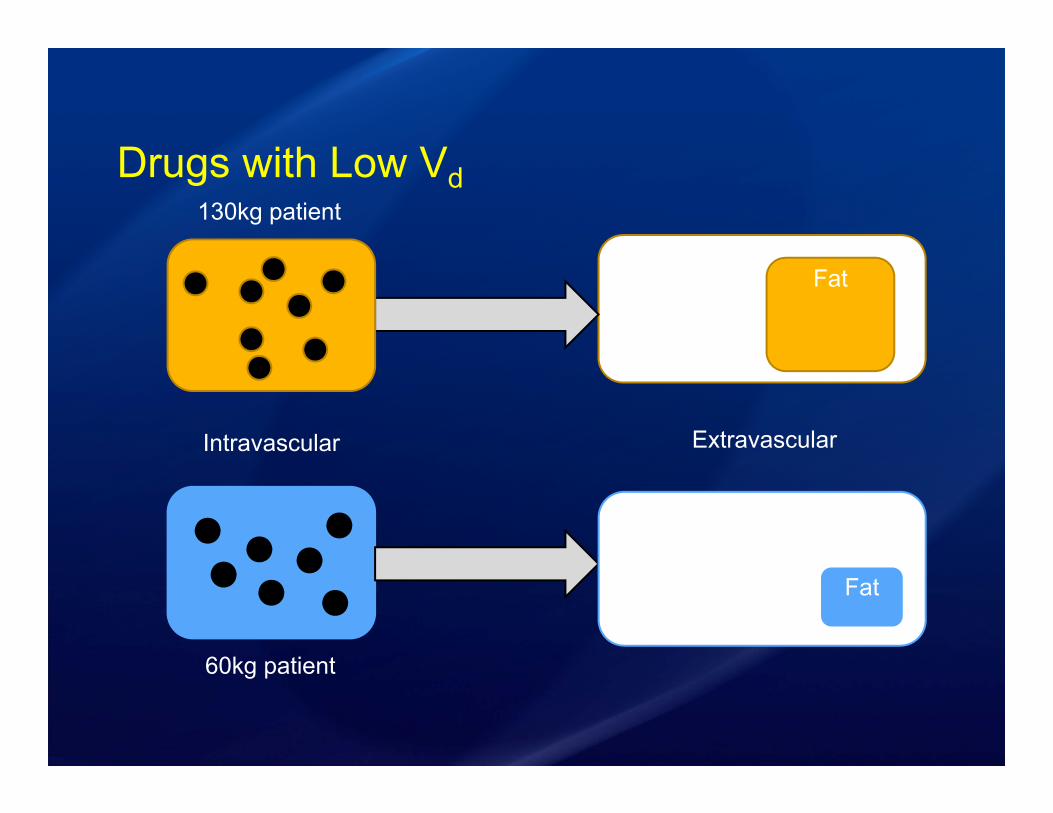
Drugs with Low Vd
60kg patient
130kg patient
Intravascular Extravascular
Fat
Fat
Clearance• Defined as the volume of blood cleared of drug
in a given time
• In obese patients:• Altered hepatic blood flow• Higher absolute clearance
Hanley MJ, et al. Clin Pharmacokinet. 2010;49:71-87.
Elimination Half-Life• Defined as time it takes for concentration to fall
to half its original concentration
Hanley MJ, et al. Clin Pharmacokinet. 2010;49:71-87.
T½ = (ln 2 x Vd) / CL
CL = Clearance
Which of the following statements is true?A. Obese and non-obese patients have similar
PK profilesB. Vd is increased in obese patientsC. T1/2 is equivalent in obese and non-obese
patientsD. Compared to non-obese patients, obese
patients have equivalent CL

Venous Thromboembolism Prophylaxis
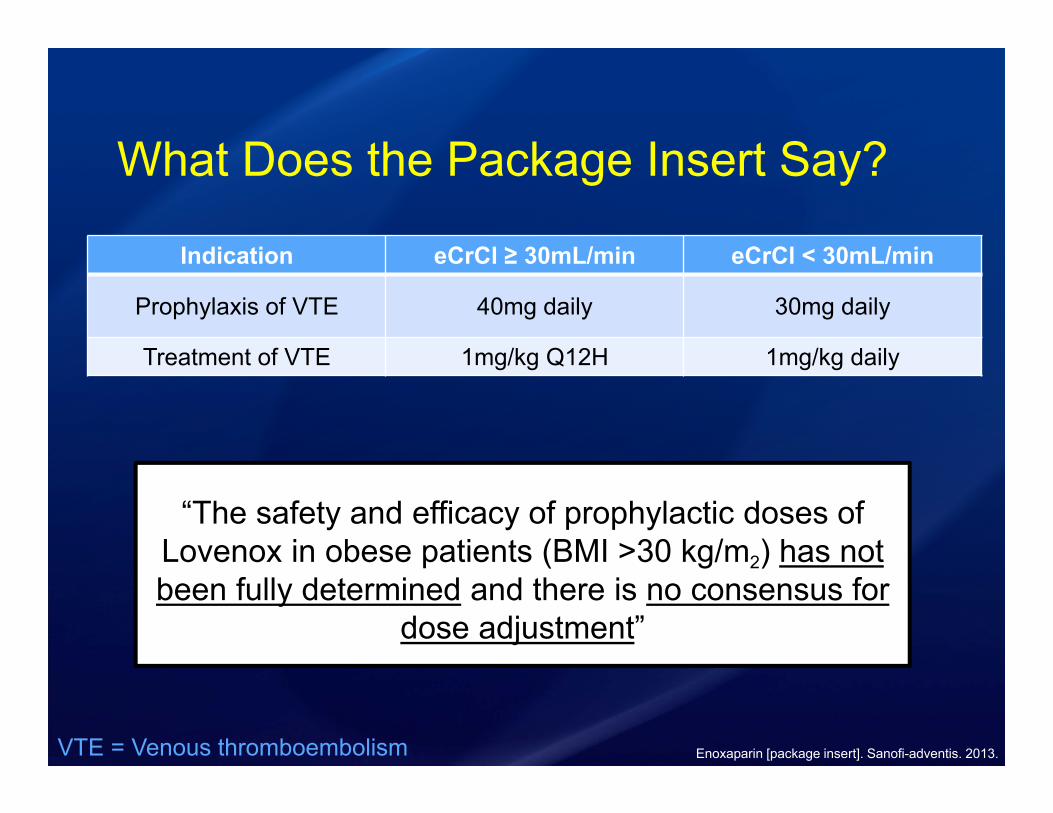
What Does the Package Insert Say?
Indication eCrCl ≥ 30mL/min eCrCl < 30mL/min
Prophylaxis of VTE 40mg daily 30mg daily
Treatment of VTE 1mg/kg Q12H 1mg/kg daily
Enoxaparin [package insert]. Sanofi-adventis. 2013.
“The safety and efficacy of prophylactic doses of Lovenox in obese patients (BMI >30 kg/m2) has not been fully determined and there is no consensus for
dose adjustment”
VTE = Venous thromboembolism
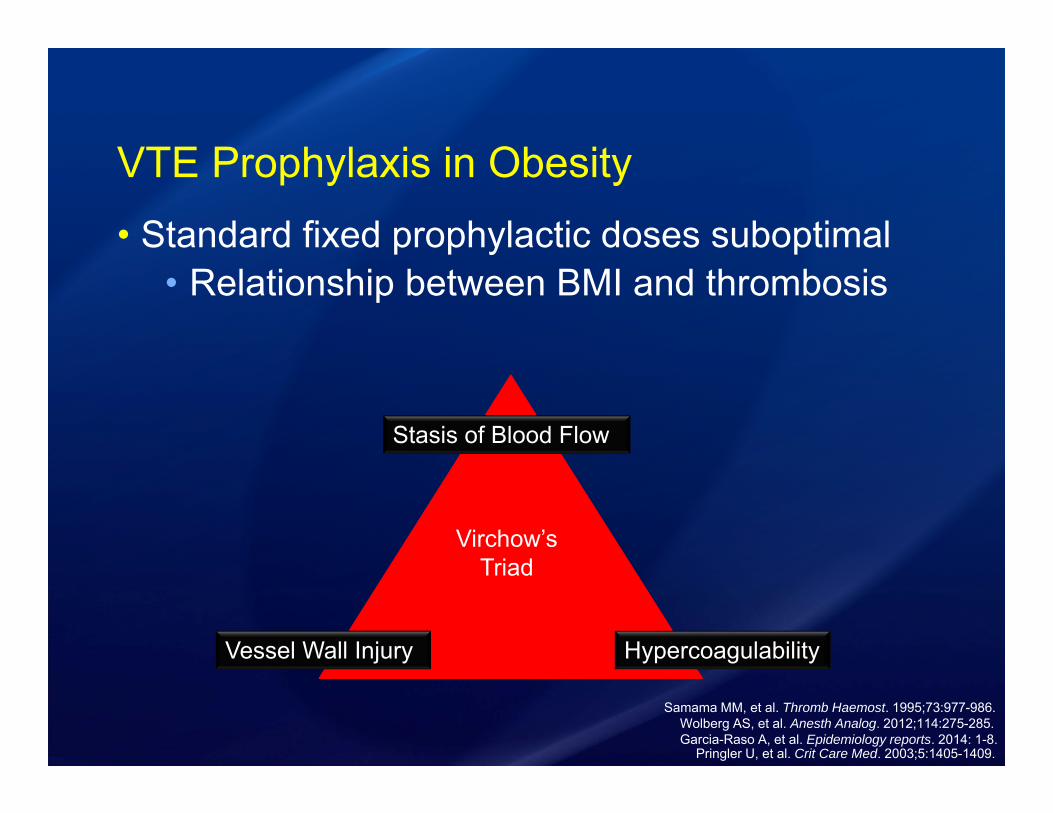
VTE Prophylaxis in Obesity• Standard fixed prophylactic doses suboptimal
• Relationship between BMI and thrombosis
Garcia-Raso A, et al. Epidemiology reports. 2014: 1-8. Wolberg AS, et al. Anesth Analog. 2012;114:275-285.
Pringler U, et al. Crit Care Med. 2003;5:1405-1409.
Stasis of Blood Flow
HypercoagulabilityVessel Wall Injury
Virchow’s Triad
Samama MM, et al. Thromb Haemost. 1995;73:977-986.

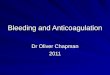
Unfractionated Heparin and Low Molecular Weight Heparin for VTE Prophylaxis
Wang TF, et al. Thrombosis and Haemostasis. 2014;111:88-93.
Study Design Retrospective cohort study at 3 hospitals
Population Adult obese (> 100kg) inpatients (> 48 hours) who received thromboprophylaxis with UFH or enoxaparin
InterventionStandard - UFH 5,000 units BID/TID or enoxaparin 40mg daily vsHigh-dose - UFH 7,500 units TID or enoxaparin 40mg BID
PrimaryEndpoint Rates of VTE in the standard vs high-dose groups
SecondaryEndpoints
-VTE rates stratified by BMI-Hemorrhage
UFH = Unfractionated heparin
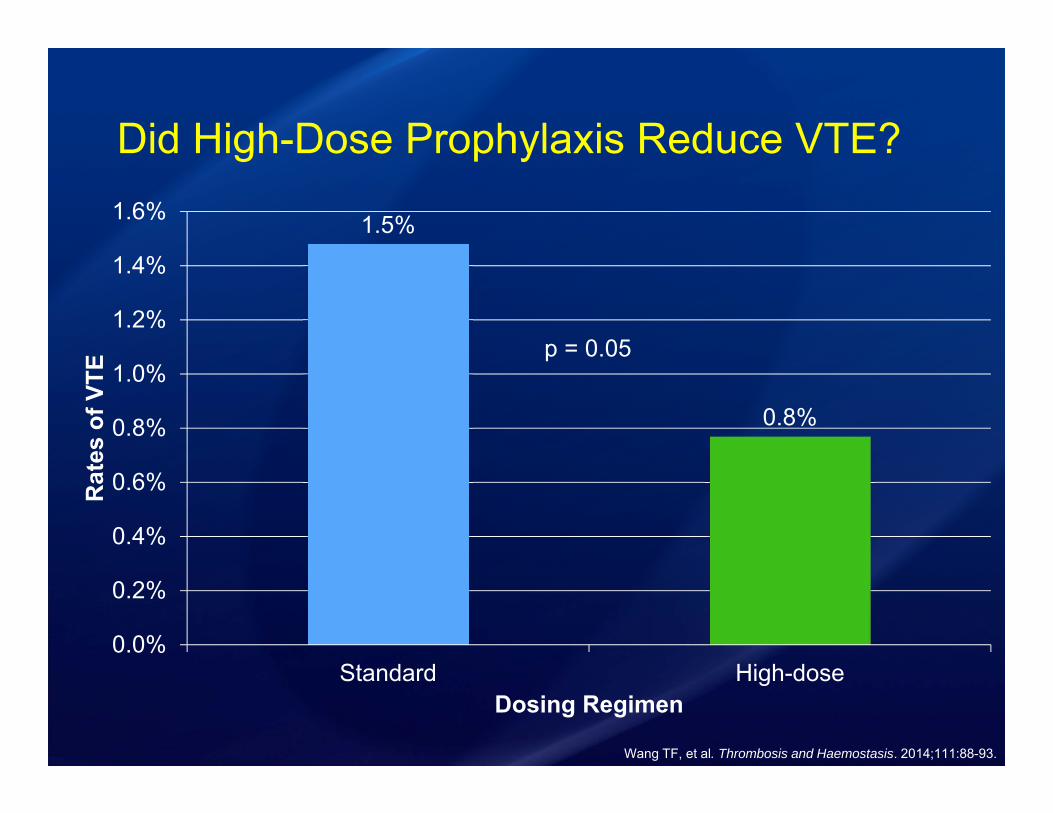
Did High-Dose Prophylaxis Reduce VTE?
1.5%
0.8%
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
1.6%
Standard High-dose
Rat
es o
f VTE
Dosing Regimen
p = 0.05
Wang TF, et al. Thrombosis and Haemostasis. 2014;111:88-93.
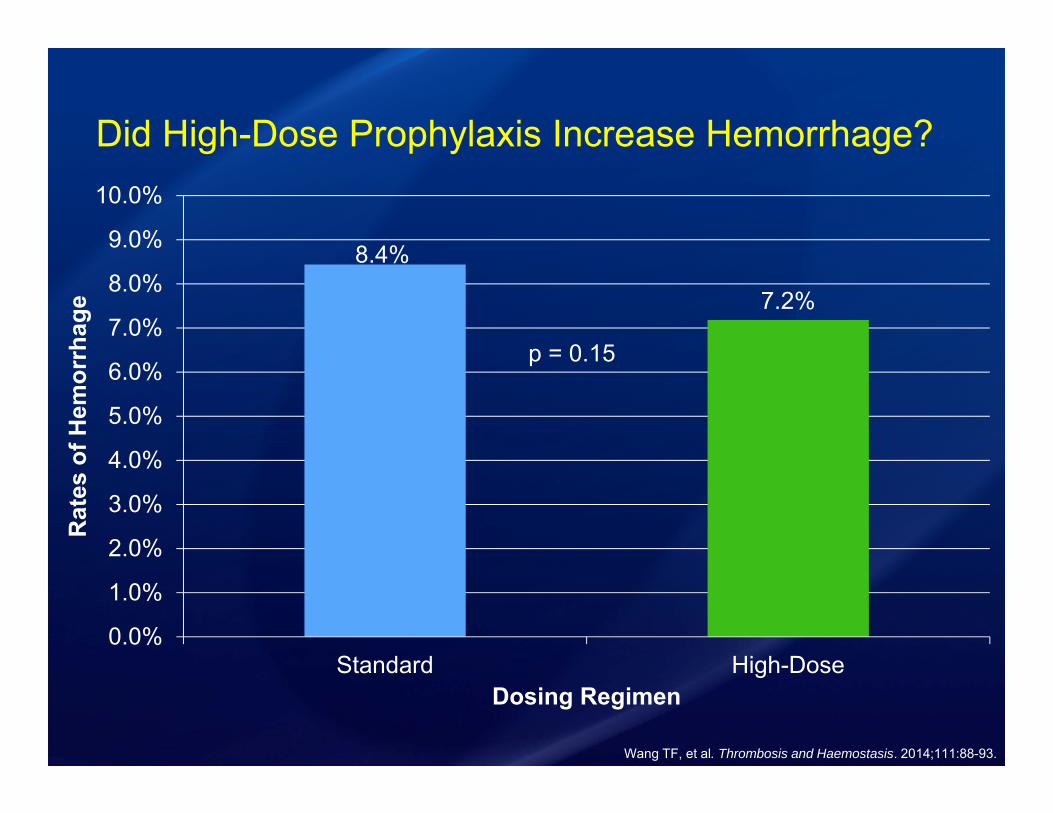
Did High-Dose Prophylaxis Increase Hemorrhage?
8.4%
7.2%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
Standard High-Dose
Rat
es o
f Hem
orrh
age
Dosing Regimen
Wang TF, et al. Thrombosis and Haemostasis. 2014;111:88-93.
p = 0.15

VTE Prophylaxis RecommendationsWeight ≥ 100kg
And/orBMI ≥ 40 kg/m2
eCrCl < 30mL/min eCrCl ≥ 30mL/min
Heparin 7,500 units TID
Enoxaparin 40mg BID
Heparin 7,500 units TID
Treatment Dosing of Low Molecular Weight Heparin
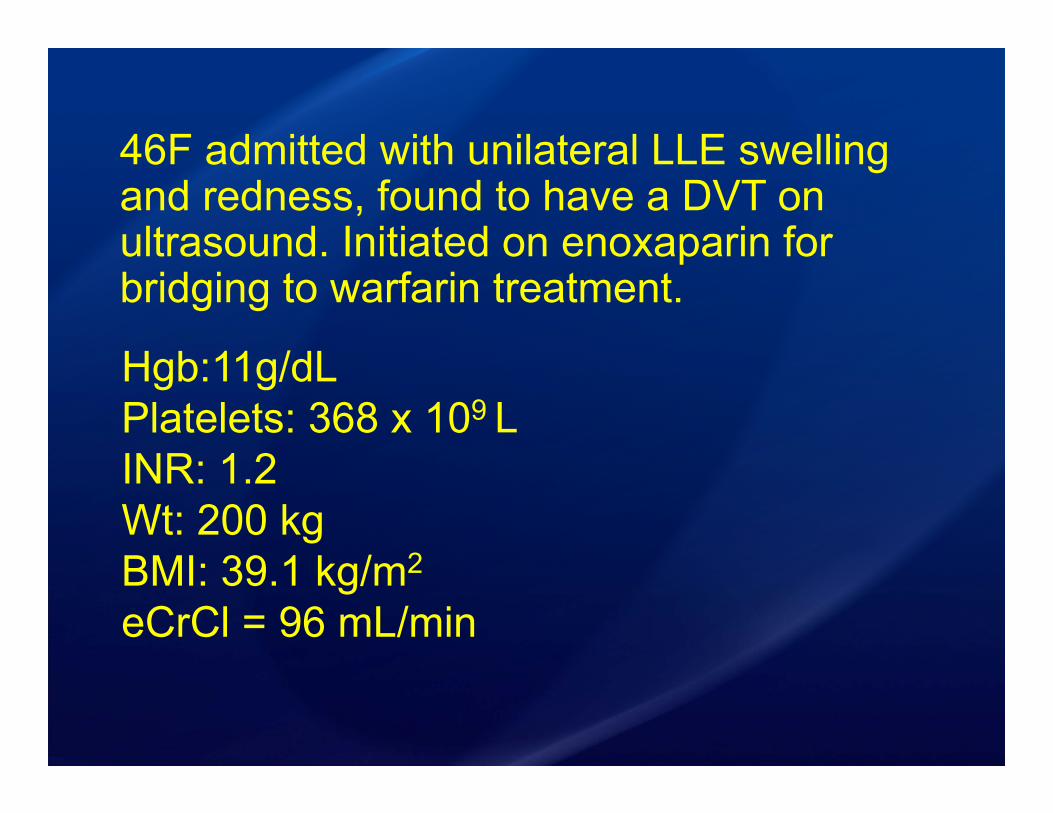
46F admitted with unilateral LLE swelling and redness, found to have a DVT on ultrasound. Initiated on enoxaparin for bridging to warfarin treatment.
LLE = Left lower extremity DVT = Deep vein thrombosiseCrCl = Estimated creatinine clearance
Hgb:11g/dLPlatelets: 368 x 109 LINR: 1.2 Wt: 200 kgBMI: 39.1 kg/m2
eCrCl = 96 mL/min
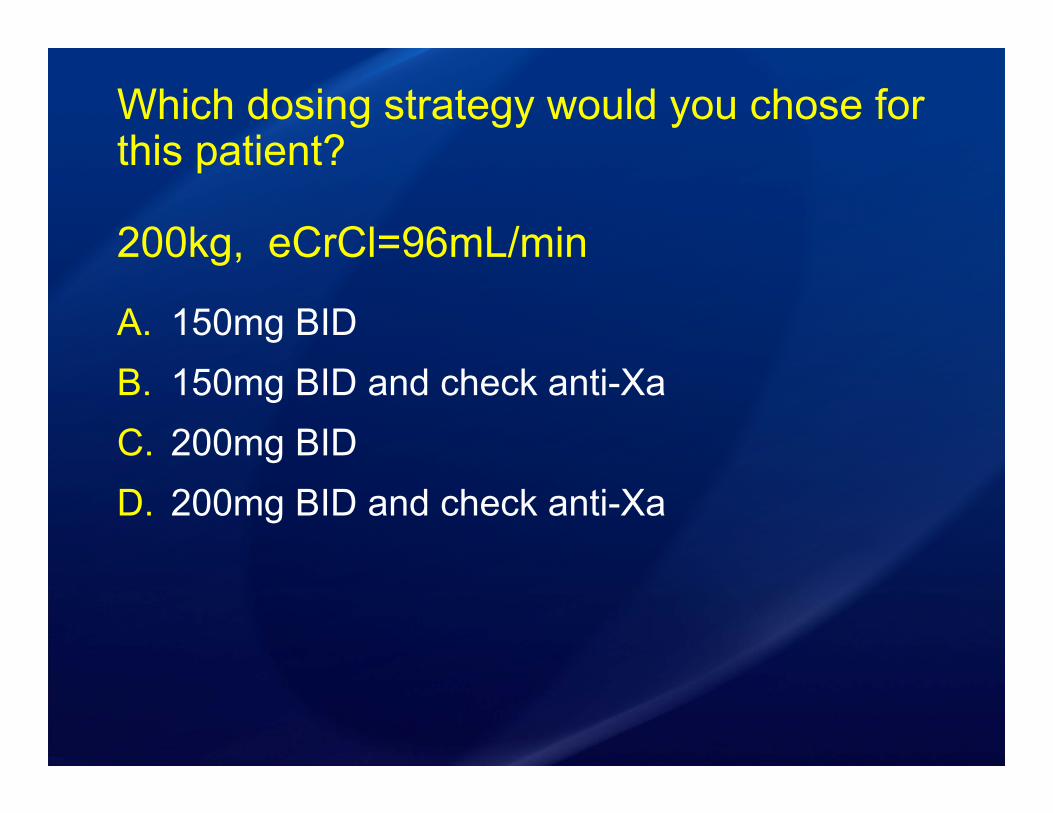
Which dosing strategy would you chose for this patient?
200kg, eCrCl=96mL/min
A. 150mg BIDB. 150mg BID and check anti-XaC. 200mg BIDD. 200mg BID and check anti-Xa

Anti-Xa Monitoring• Peak levels drawn 3 – 5 hours after steady
state
• LMWH therapeutic range• 0.5 – 1.00 IU/mL for BID dosing• 1.00 – 2.00 IU/mL for once daily dosing
• Low antithrombin III (AT III) levels can decrease the efficacy of heparins
Heparin Anti-Xa Assay. Mayo Medical Laboratories. Accessed May 18, 2016.Houbouyan L, et al. Clin Chem. 1996;42:1223-1230.
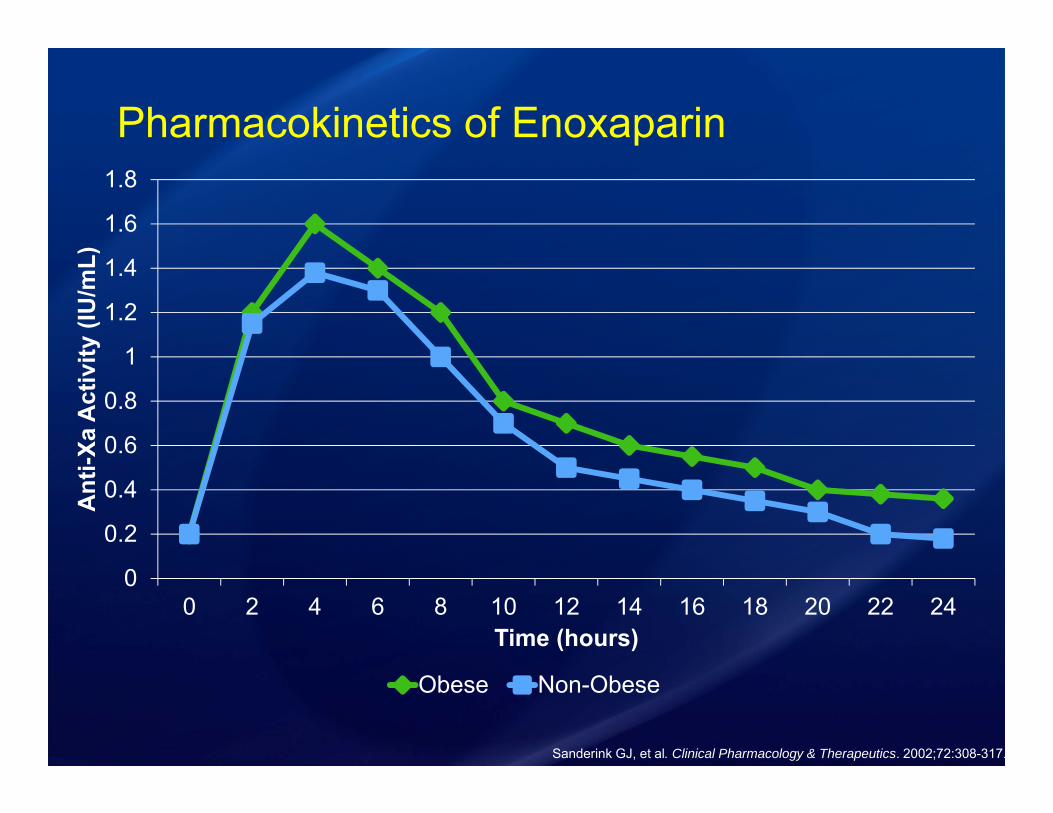
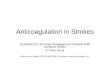
Pharmacokinetics of Enoxaparin
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
0 2 4 6 8 10 12 14 16 18 20 22 24
Ant
i-Xa
Act
ivity
(IU
/mL)
Time (hours)
Obese Non-Obese
Sanderink GJ, et al. Clinical Pharmacology & Therapeutics. 2002;72:308-317.
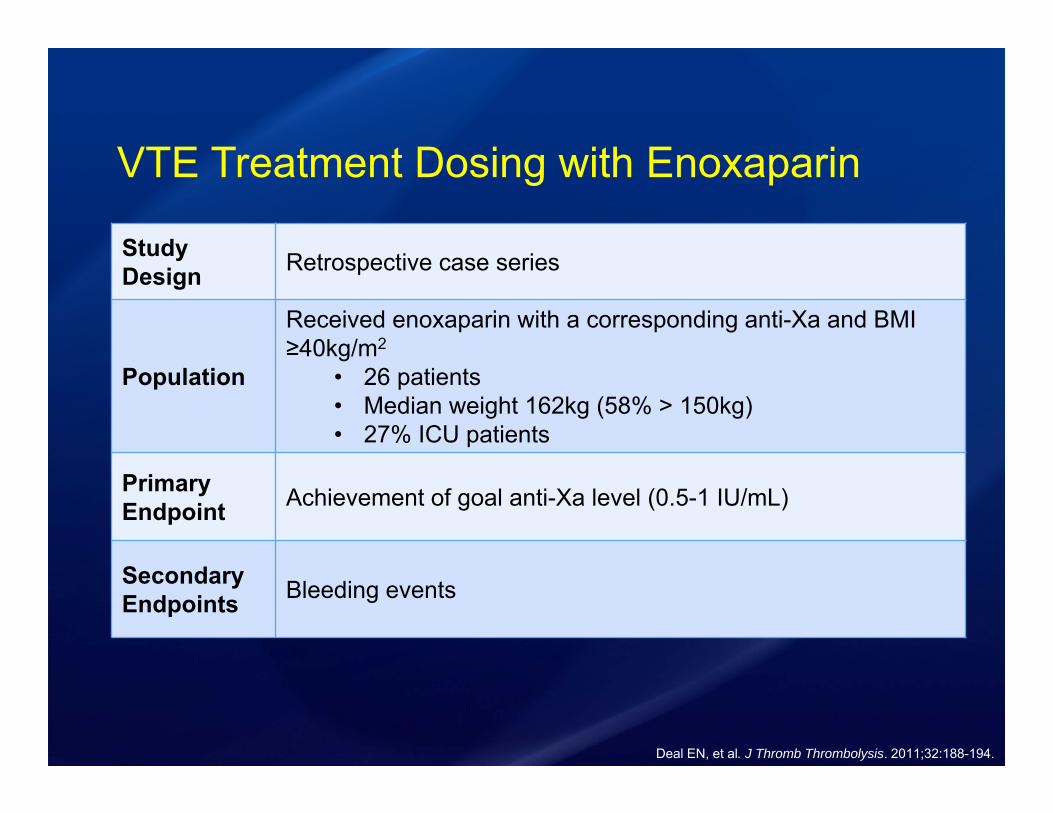
VTE Treatment Dosing with Enoxaparin
Deal EN, et al. J Thromb Thrombolysis. 2011;32:188-194.
Study Design Retrospective case series
Population
Received enoxaparin with a corresponding anti-Xa and BMI ≥40kg/m2
• 26 patients• Median weight 162kg (58% > 150kg)• 27% ICU patients
PrimaryEndpoint Achievement of goal anti-Xa level (0.5-1 IU/mL)
SecondaryEndpoints Bleeding events

Anti-Xa Levels
15%
46%
38%
0%5%
10%15%20%25%30%35%40%45%50%
Perc
enta
ge o
f Pat
ient
s
Anti-Xa Level
• No patient had subtherapeutic levels
• No thrombotic events occurred in the study
• 40% of patients with a supratherapeutic level had bleeding events
• Median starting dose was 0.8mg/kg
• Doses ranged from 80mg – 150mg BID
Deal EN, et al. J Thromb Thrombolysis. 2011;32:188-194.

Enoxaparin AlgorithmWeight ≥ 100kg
and/orBMI ≥ 40 kg/m2
eCrCl<30mL/min eCrCl>30mL/min
1mg/kg Q24HMax: 150mg
0.8mg/kg Q12HMax: 150mg
Check anti-Xa 3-5 hours after 4th dose
46F admitted with unilateral LLE swelling and redness, found to have a DVT on ultrasound. Initiated on enoxaparin for bridging to warfarin treatment.
Hgb:11g/dLPlatelets: 368 x 109 LINR: 1.2 Wt: 200 kgBMI: 39.1 kg/m2
eCrCl = 96 mL/min
Which dosing strategy would you chose for this patient?
200kg, eCrCl=96mL/min
A. 150mg BIDB. 150mg BID and check anti-XaC. 200mg BIDD. 200mg BID and check anti-Xa
Direct Oral Anticoagulants (DOACS)
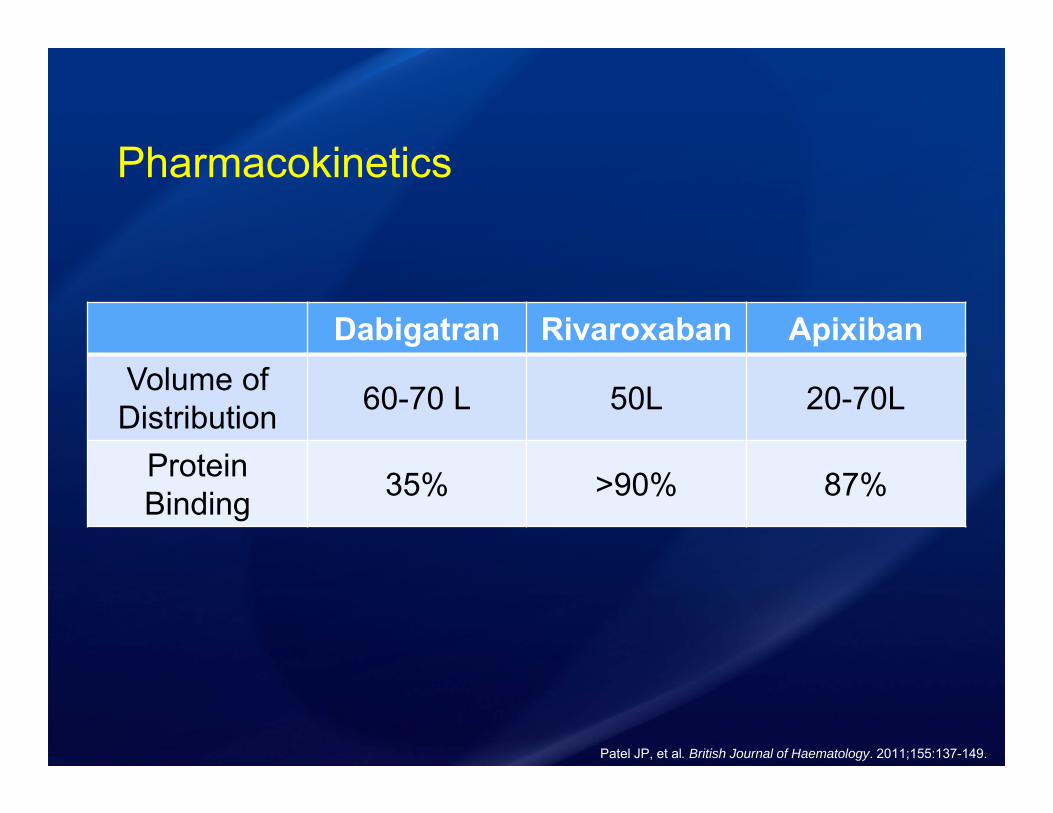
Pharmacokinetics
Dabigatran Rivaroxaban ApixibanVolume of Distribution 60-70 L 50L 20-70L
Protein Binding 35% >90% 87%
Patel JP, et al. British Journal of Haematology. 2011;155:137-149.
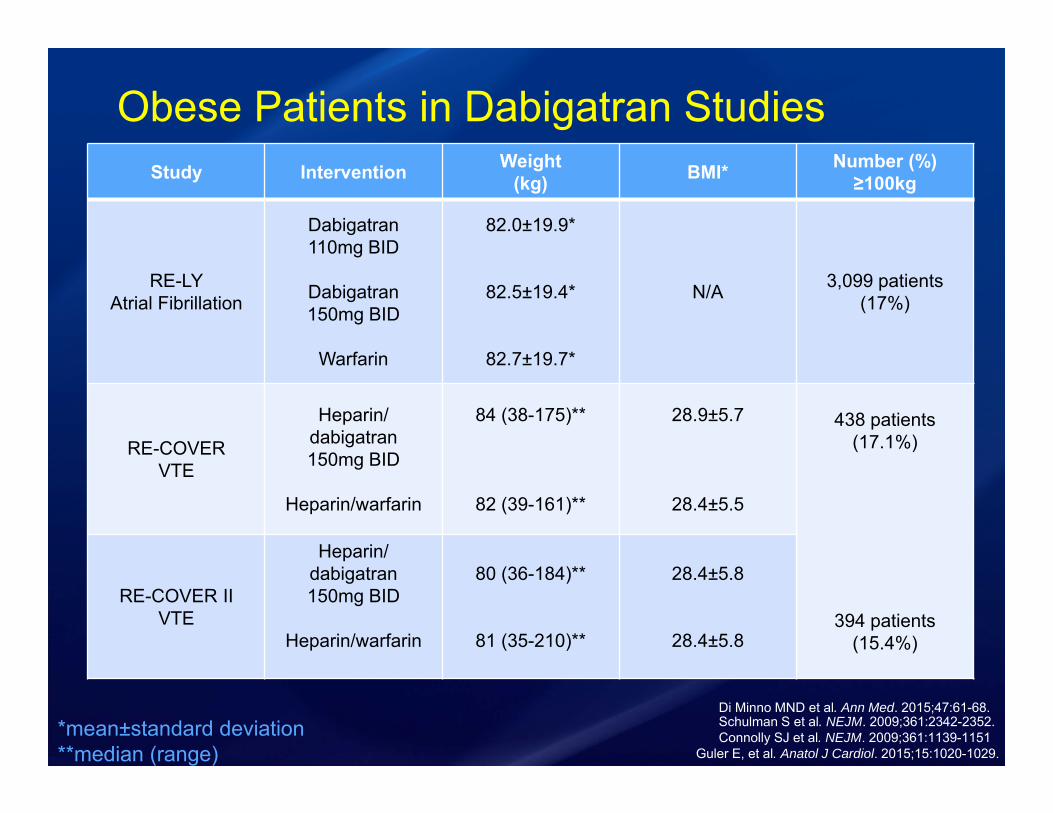
Obese Patients in Dabigatran StudiesStudy Intervention Weight
(kg) BMI* Number (%)≥100kg
RE-LYAtrial Fibrillation
Dabigatran110mg BID
Dabigatran150mg BID
Warfarin
82.0±19.9*
82.5±19.4*
82.7±19.7*
N/A 3,099 patients(17%)
RE-COVERVTE
Heparin/ dabigatran150mg BID
Heparin/warfarin
84 (38-175)**
82 (39-161)**
28.9±5.7
28.4±5.5
438 patients (17.1%)
394 patients(15.4%)
RE-COVER IIVTE
Heparin/ dabigatran150mg BID
Heparin/warfarin
80 (36-184)**
81 (35-210)**
28.4±5.8
28.4±5.8
Guler E, et al. Anatol J Cardiol. 2015;15:1020-1029.Connolly SJ et al. NEJM. 2009;361:1139-1151Schulman S et al. NEJM. 2009;361:2342-2352.*mean±standard deviation
**median (range)
Di Minno MND et al. Ann Med. 2015;47:61-68.
Dabigatran• RE-LY subgroup analysis
• Case reports of stroke in obese patients • 153kg (BMI 44.7kg/m2) peak level was less
than the 25th percentile of therapeutic trough
Guler E, et al. Anatol J Cardiol. 2015;15:1020-1029.Bruer L, et al. NEJM. 2013;25:2440-2442.
Connolly SJ et al. NEJM. 2009;361:1139-1151.

Dabigatran Pharmacokinetics in Obesity
020406080
100120140160180200220240260280
8 a.m. 10 a.m. Noon 2 p.m. 4 p.m. 6 p.m. 8 p.m.
Plas
ma
Leve
l of D
abig
atra
n (n
g/m
L)
Daytime Hours
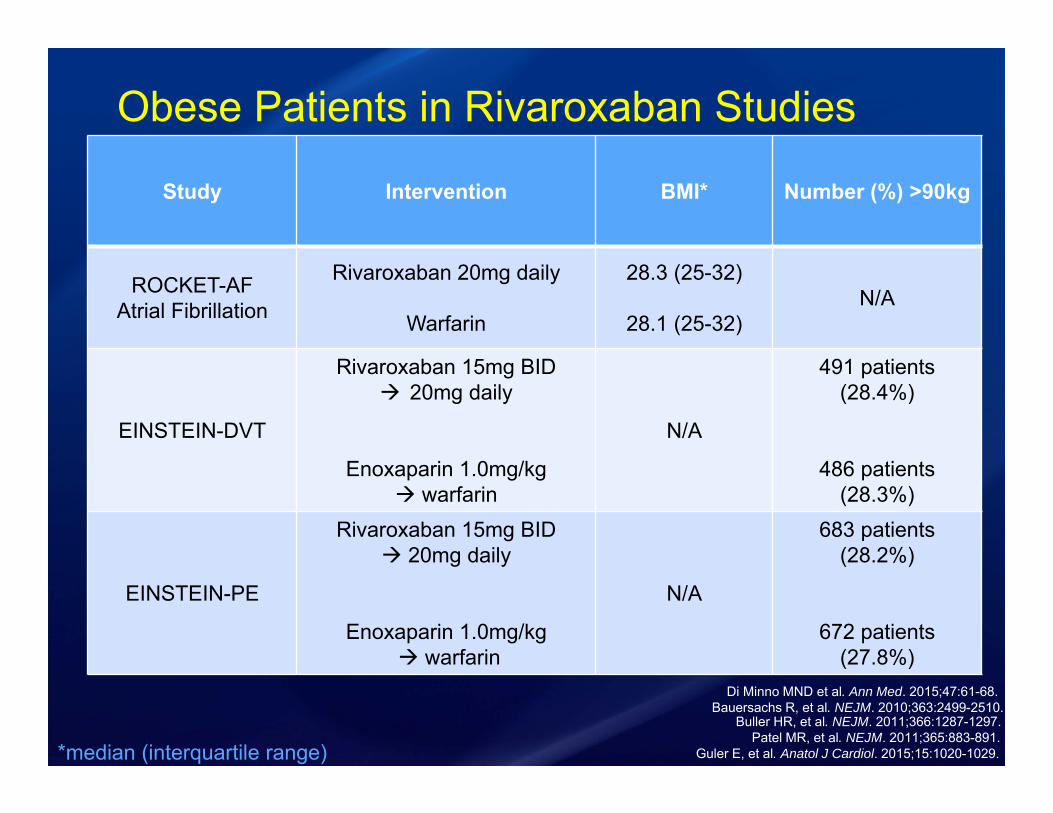
Obese Patients in Rivaroxaban Studies
Study Intervention BMI* Number (%) >90kg
ROCKET-AFAtrial Fibrillation
Rivaroxaban 20mg daily
Warfarin
28.3 (25-32)
28.1 (25-32)N/A
EINSTEIN-DVT
Rivaroxaban 15mg BID 20mg daily
Enoxaparin 1.0mg/kg warfarin
N/A
491 patients(28.4%)
486 patients(28.3%)
EINSTEIN-PE
Rivaroxaban 15mg BID 20mg daily
Enoxaparin 1.0mg/kg warfarin
N/A
683 patients(28.2%)
672 patients(27.8%)
Guler E, et al. Anatol J Cardiol. 2015;15:1020-1029.Patel MR, et al. NEJM. 2011;365:883-891.
Buller HR, et al. NEJM. 2011;366:1287-1297.Bauersachs R, et al. NEJM. 2010;363:2499-2510.
Di Minno MND et al. Ann Med. 2015;47:61-68.
*median (interquartile range)
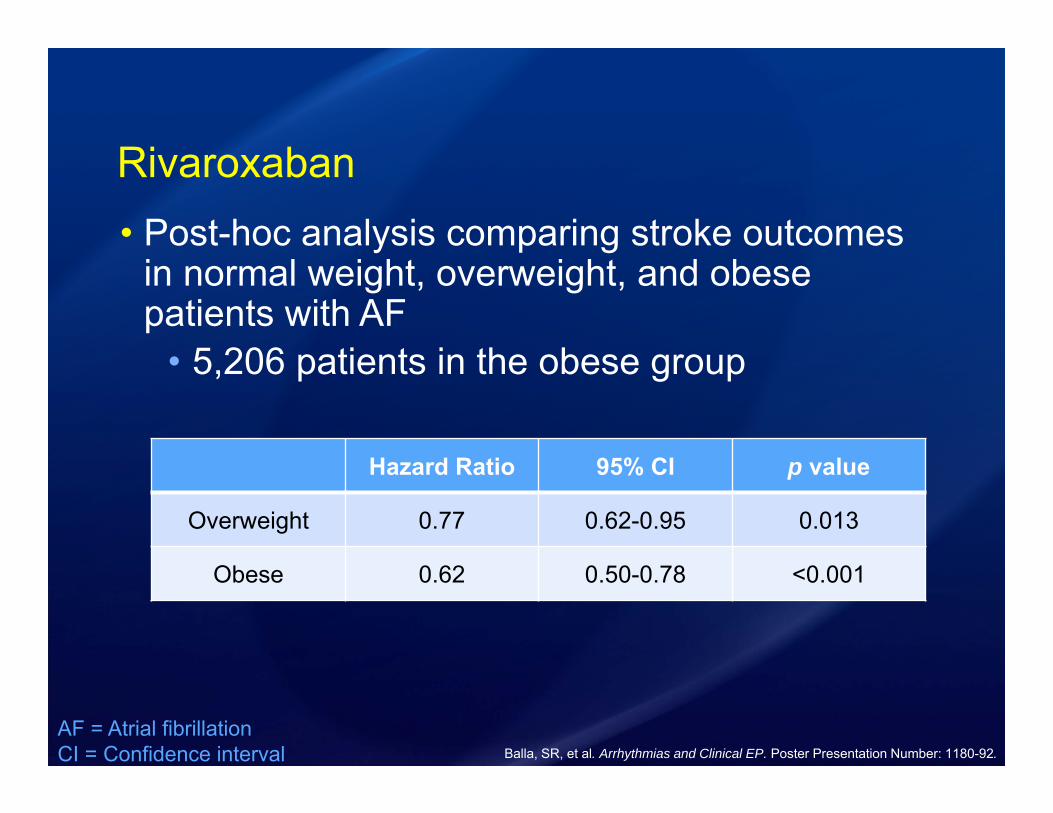
Rivaroxaban• Post-hoc analysis comparing stroke outcomes
in normal weight, overweight, and obese patients with AF
• 5,206 patients in the obese group
AF = Atrial fibrillationCI = Confidence interval Balla, SR, et al. Arrhythmias and Clinical EP. Poster Presentation Number: 1180-92.
Hazard Ratio 95% CI p value
Overweight 0.77 0.62-0.95 0.013
Obese 0.62 0.50-0.78 <0.001
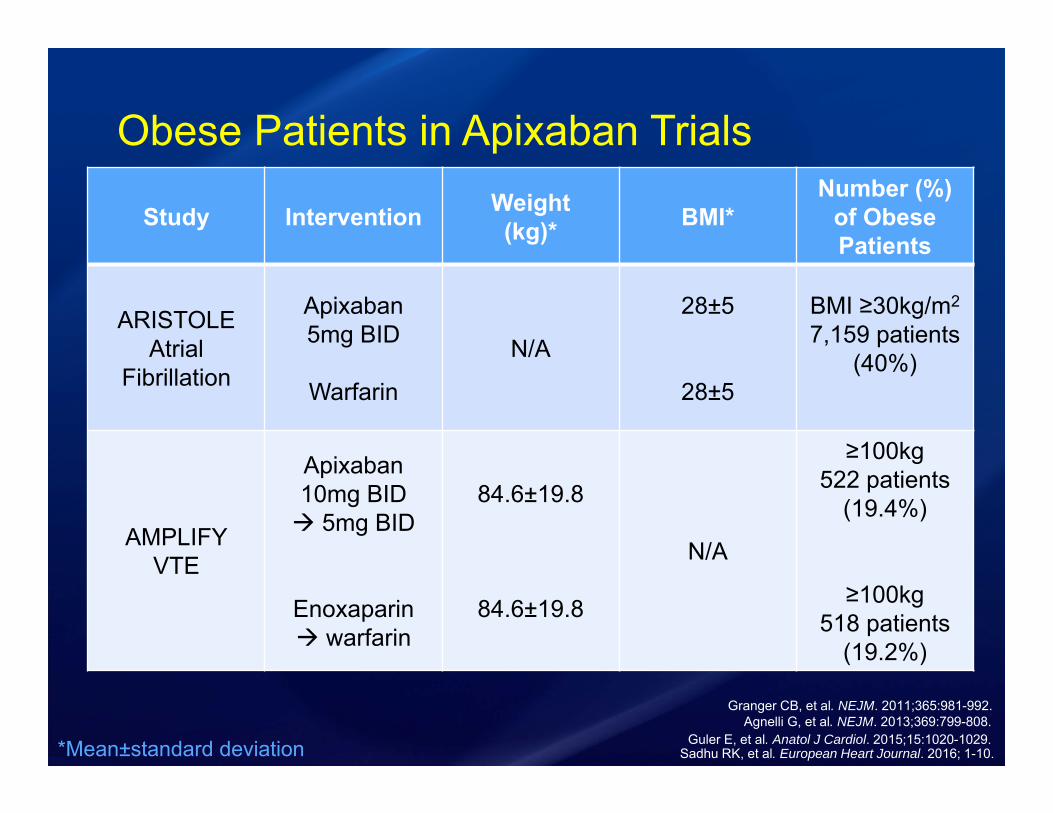
Obese Patients in Apixaban Trials
Guler E, et al. Anatol J Cardiol. 2015;15:1020-1029.
Study Intervention Weight(kg)* BMI*
Number (%) of ObesePatients
ARISTOLEAtrial
Fibrillation
Apixaban5mg BID
Warfarin
N/A
28±5
28±5
BMI ≥30kg/m2
7,159 patients(40%)
AMPLIFYVTE
Apixaban 10mg BID 5mg BID
Enoxaparin warfarin
84.6±19.8
84.6±19.8
N/A
≥100kg522 patients
(19.4%)
≥100kg518 patients
(19.2%)
Agnelli G, et al. NEJM. 2013;369:799-808.Granger CB, et al. NEJM. 2011;365:981-992.
*Mean±standard deviation Sadhu RK, et al. European Heart Journal. 2016; 1-10.
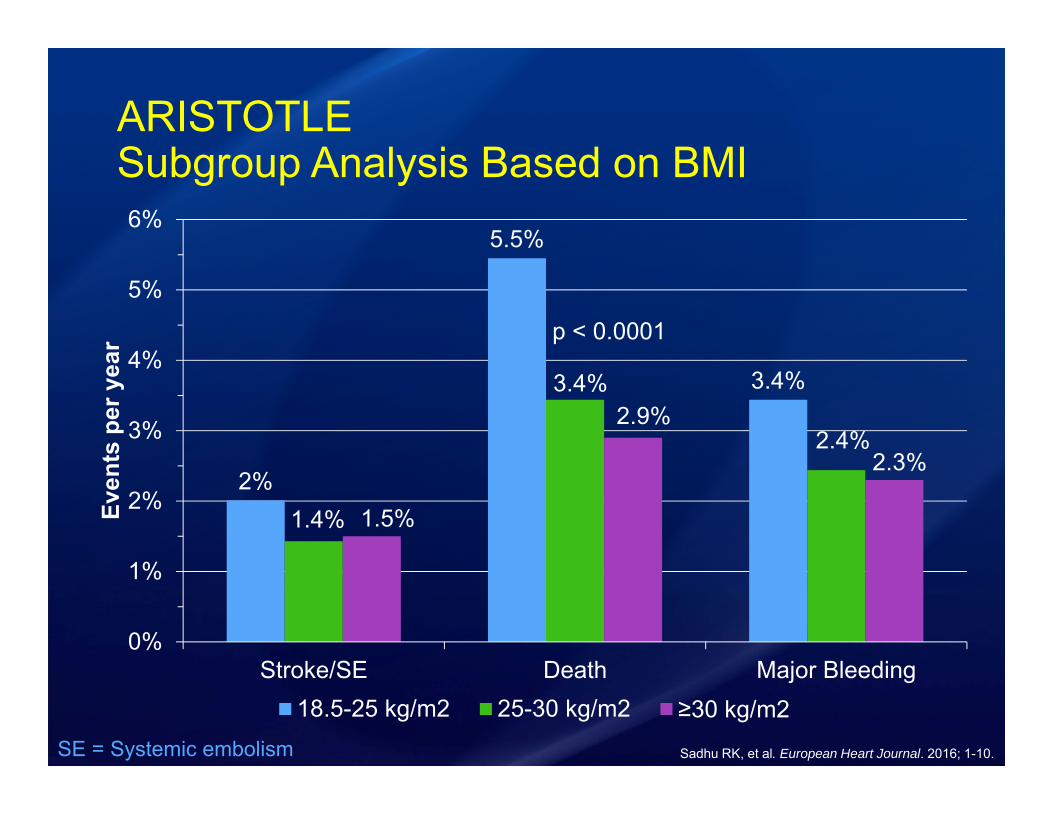
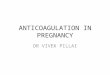
ARISTOTLESubgroup Analysis Based on BMI
2%
5.5%
3.4%
1.4%
3.4%
2.4%
1.5%
2.9%
2.3%
0%
1%
2%
3%
4%
5%
6%
Stroke/SE Death Major Bleeding
Even
ts p
er y
ear
18.5-25 kg/m2 25-30 kg/m2 ≥30 kg/m2
p < 0.0001
SE = Systemic embolism Sadhu RK, et al. European Heart Journal. 2016; 1-10.

How Does Apixaban Compare to Warfarin in Obese Patients with Atrial Fibrillation?
0.5 1 2 3
OutcomeBMI ≥30kg/m2
Hazard Ratio(95% CI)
Stroke/SE 0.76 (0.55-1.05)
Death 0.81 (0.67-0.99)
Major Bleeding 0.84 (0.67-1.07)
Favors Apixaban Favors WarfarinSadhu RK, et al. European Heart Journal. 2016; 1-10.
DOACS for VTE
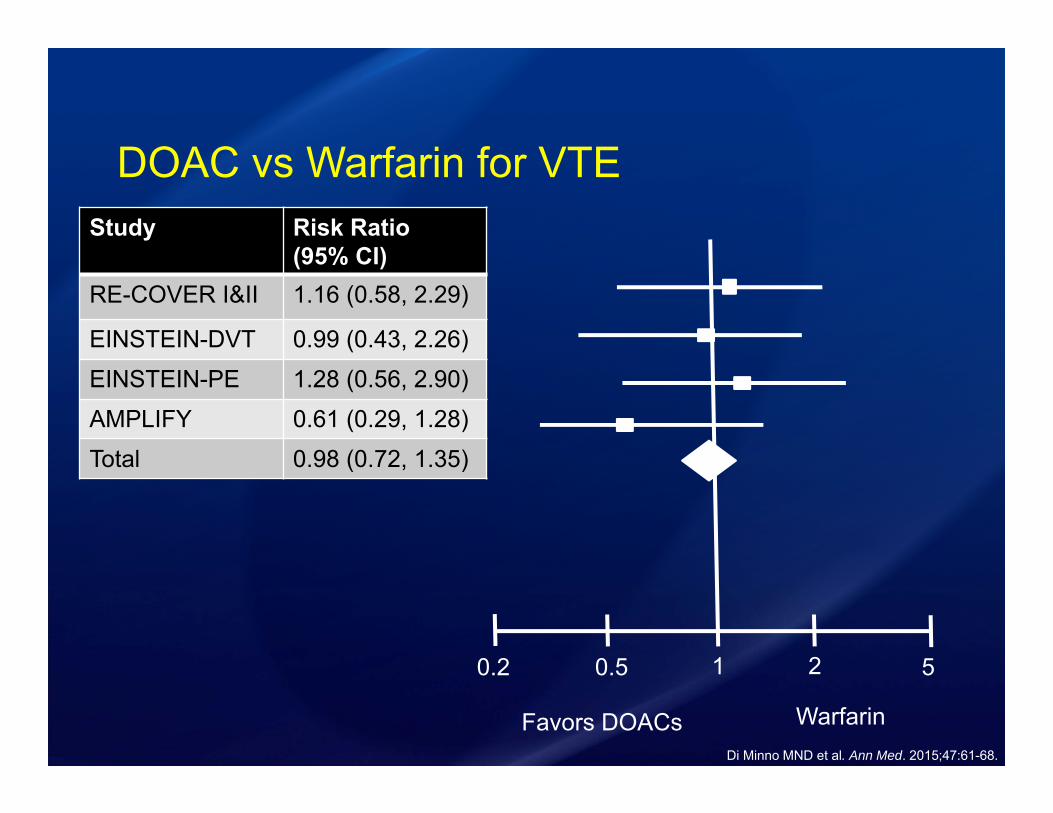
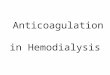
DOAC vs Warfarin for VTE
0.2 0.5 1 52
Favors DOACs WarfarinDi Minno MND et al. Ann Med. 2015;47:61-68.
Study Risk Ratio (95% CI)
RE-COVER I&II 1.16 (0.58, 2.29)
EINSTEIN-DVT 0.99 (0.43, 2.26)
EINSTEIN-PE 1.28 (0.56, 2.90)
AMPLIFY 0.61 (0.29, 1.28)
Total 0.98 (0.72, 1.35)

DOACs Recommendations in Obesity• Avoid dabigatran in obese patients
• Rivaroxaban may be considered in obese patients
• Apixaban has the best evidence for utilization of DOACs in obese patients

In a post-hoc analysis comparing apixaban vs warfarin in obese patients (BMI≥30kg/m2) with atrial fibrillation warfarin prevented more strokes and systemic embolism?A. TrueB. False
Summary• Evaluate pharmacokinetics when dosing medications in
obese patients
• For VTE prophylaxis “high-dose” heparin or LMWH is recommended for patients ≥100kg and BMI ≥40kg/m2
• For VTE treatment dose adjustments are warranted and anti-Xa levels should be monitored
• Apixiban may be considered for anticoagulation in obese patients

Questions & Discussion
Dose Capping with Unfractionated Heparin• NSTEMI
• Obese patients took longer to reach goal aPTT
• No dose cap • Higher doses achieves therapeutic
anticoagulation more rapidly
• VTE• Weight-based nomograms with no cap• Studies have shown relationship between
patients’ weight and heparin requirement
Joncas, SX, et al. Obesity Journal. 2013;21:1753-1758.Patel JP, et al. BJH. 2011;155:137-149.
Fondaparinux• Vd = 8.2L
• Largely resides in the intravascular space• >94% protein bound
• Treatment of VTE based on the MATISSE trials• 10mg if >100kg
Patel JP, et al. British Journal of Haematology. 2011;155:137-149.Fondaparinux [package insert]. GlaxoSmithKline. 2001.

Anti-Xa Monitoring Cost• Mayo Clinic Hospital – Rochester
• $207.50
• Vancomycin trough level cost $150.00
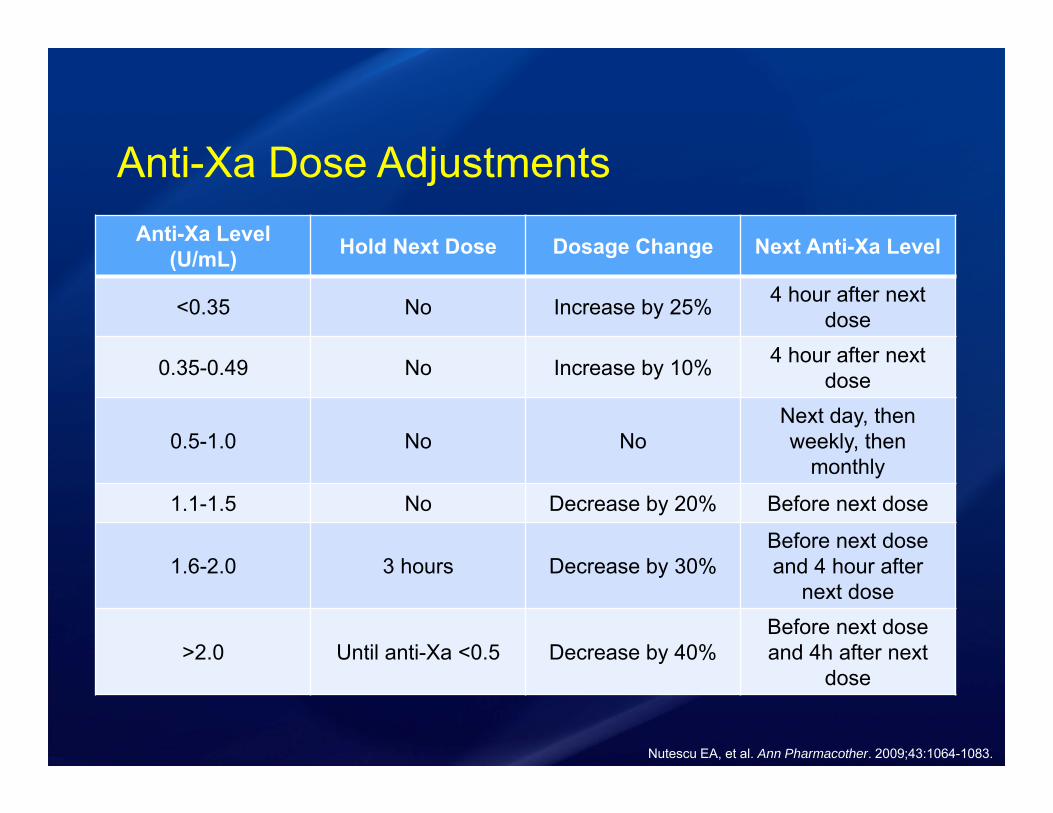
Anti-Xa Dose AdjustmentsAnti-Xa Level
(U/mL) Hold Next Dose Dosage Change Next Anti-Xa Level
<0.35 No Increase by 25% 4 hour after next dose
0.35-0.49 No Increase by 10% 4 hour after next dose
0.5-1.0 No NoNext day, then weekly, then
monthly
1.1-1.5 No Decrease by 20% Before next dose
1.6-2.0 3 hours Decrease by 30%Before next dose and 4 hour after
next dose
>2.0 Until anti-Xa <0.5 Decrease by 40%Before next dose and 4h after next
dose
Nutescu EA, et al. Ann Pharmacother. 2009;43:1064-1083.

ARISTOTLESubgroup Analysis Based on BMI
2%
5.1%
2.2%
1.4%
3.4%
2%
1%
2.6%2.1%
1.3%
3.2%
2.5%
0%
1%
2%
3%
4%
5%
6%
Stroke/SE Death Major Bleeding
Even
ts p
er y
ear
18.5-25 kg/m2 25-30 kg/m2 ≥30 kg/m2 WarfarinSE = Systemic embolism Sadhu RK, et al. European Heart Journal. 2016; 1-10.