Embed Size (px)
Citation preview
Weight Management in Patients With Type 2 Diabetes
JOAN TEMMERMAN, MD, MS, FAAFP, CNS
American Association of Diabetic Educators Annual Meeting, Indianapolis, IN August 3,
2012
Objectives
• Describe the obesity epidemic and its impact on diabetes
• Review various options for weight loss and expected results
• Review diabetes weight management studies: Look AHEAD & Why WAIT
• Distinguish among different bariatric surgical procedures
• Summarize the IDF position statement on bariatric surgery in the treatment of obese patients with T2DM
• Examine recommendations for pre-operative and post-operative diabetic care
2

The age of obesity: Inactive lifestyle, poor nutrition, calorie
imbalance
Threatens steady gains in longevity
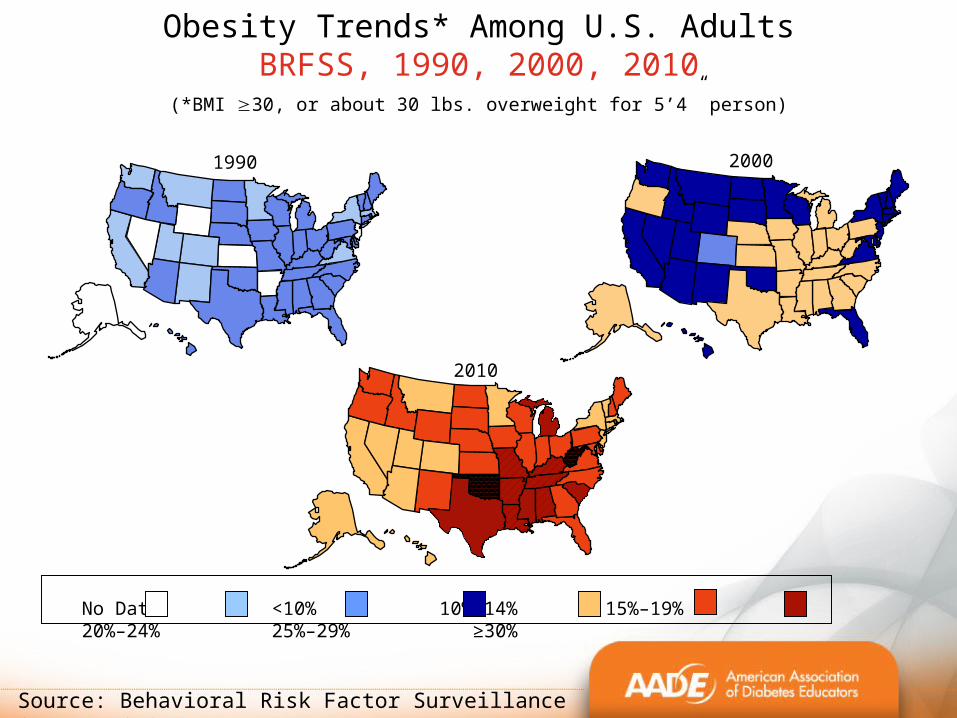
2000
Obesity Trends* Among U.S. AdultsBRFSS, 1990, 2000, 2010
(*BMI 30, or about 30 lbs. overweight for 5’4” person)
2010
1990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Source: Behavioral Risk Factor Surveillance System, CDC
Obesity associated with increased
mortality
• 2-3-fold increased risk of death
• Serious health effects: obesity major risk for DM, CVD, HTN,stroke, and some cancers
James WPT, J Intern Med 2008:336-352
Diabesity: obesity strongly related to the epidemic of type 2 diabetes (T2DM)
Nguyen & El-Serag, Gastroenterol Clin North Am. 2010
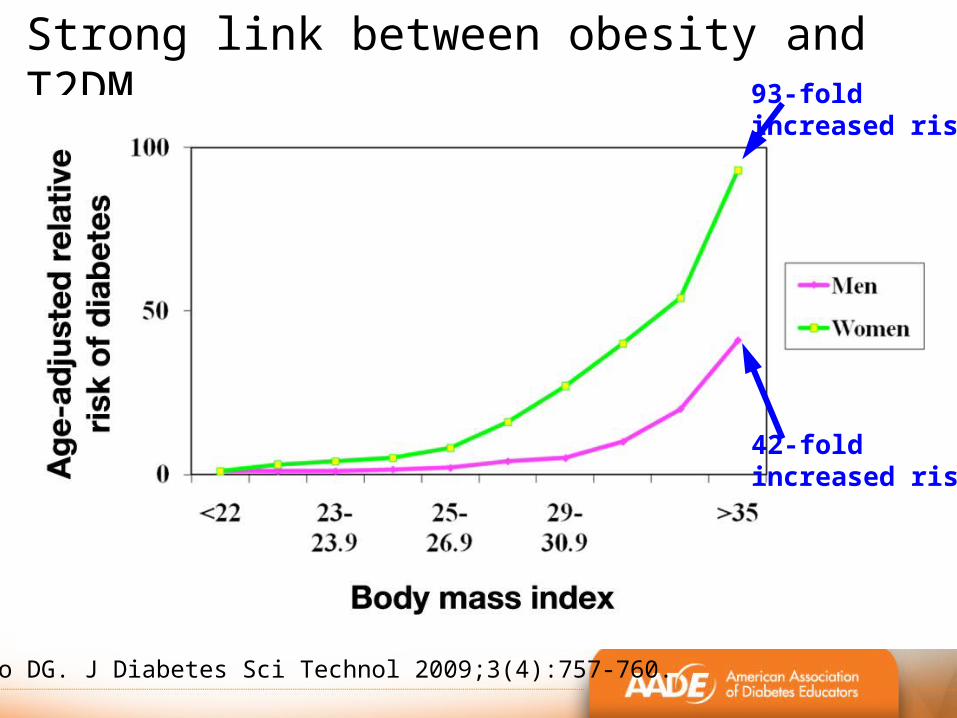
Strong link between obesity and T2DM
Marrero DG. J Diabetes Sci Technol 2009;3(4):757-760.
42-foldincreased risk
93-fold increased risk
Obesity linked to T2DM
• Diabetes primarily caused by obesity: 90% of type 2 diabetes due to excess body weight and lifestyle
• Rapid increases in T2DM parallel rise of obesity• 26 million Americans have Type 2 diabetes• 27% are unaware (7 million people)!• T2DM: 1 in 4 ages ≥ 60 years (27%)• Also occurring at younger ages
CDC 2011 National Diabetes Fact Sheet
Increased Risk for Diabetes (pre-diabetes)
• 79 million people in the US with pre-diabetes in 2010 (35% of adults)
• Up from 57 million 2008
• High risk for developing diabetes
• Prevention urgent
CDC 2011 National Diabetes Fact Sheet
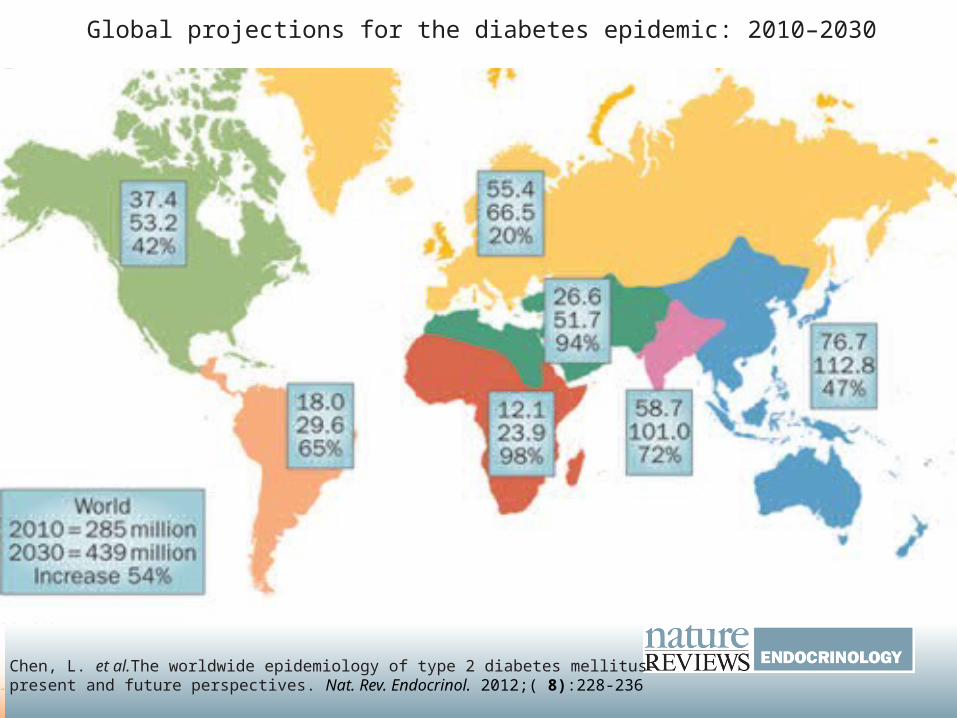
Global projections for the diabetes epidemic: 2010–2030
Chen, L. et al.The worldwide epidemiology of type 2 diabetes mellitus—present and future perspectives. Nat. Rev. Endocrinol. 2012;( 8):228-236
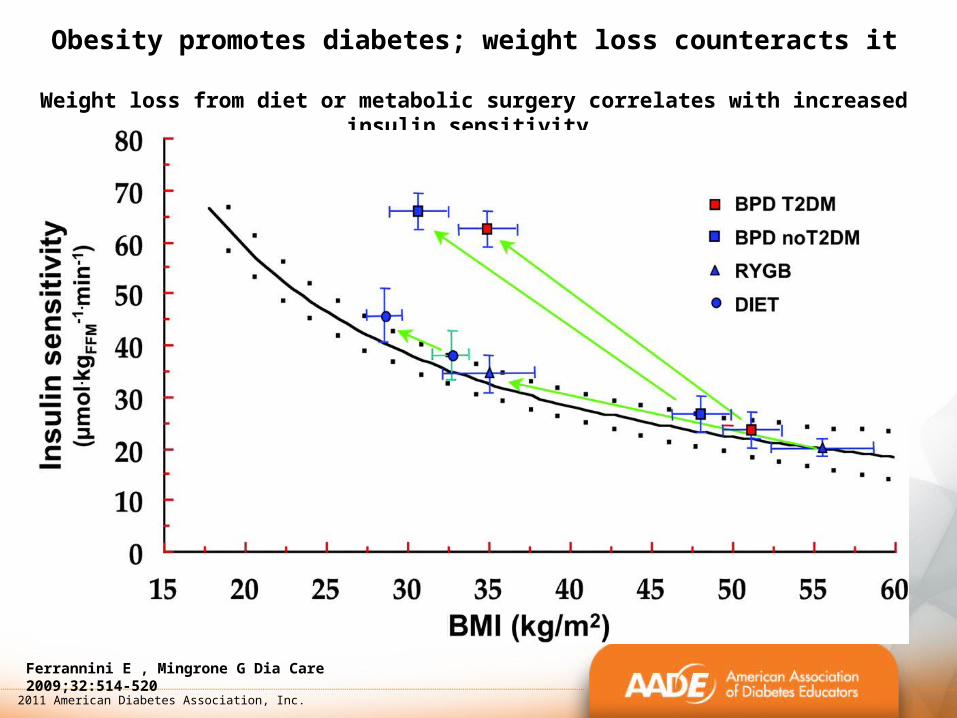
Obesity promotes diabetes; weight loss counteracts it
Weight loss from diet or metabolic surgery correlates with increased insulin sensitivity
Ferrannini E , Mingrone G Dia Care 2009;32:514-520
2011 American Diabetes Association, Inc.
Diabetic patients may have more difficulty losing weight
– Genetic differences– Metabolic factors inflammation, insulin resistance,
adipokines
– Medications: insulin, TZDs, sulfonylureas – Increased food to avoid hypoglycemia– Limited physical activity– Diet fatigue (carbohydrate restriction)
Anderson JW, Kendall CWC, et al. J Am Coll Nutr. 2003;22(5):331-339.
T2DM and Lifestyle interventionLook AHEAD Study (Action for Health in Diabetes) • Multicenter randomized 10 year clinical trial examining lifestyle intervention
• One of largest diabetes weight management studies using meal replacement (MR) strategy for weight reduction
• Weight loss at 1 year directly related to # of MR; addition of MR to lifestyle group increased weight loss to 8.6% (0.7% in usual care/control)
12
Wadden, West, et al. Obesity 2009;17(4):713-722
T2DM and Lifestyle intervention: Why WAIT
• Short-term intensive weight loss program effective for 4 yrs
• 120 patients, weekly group visits for 12 weeks
• Lifestyle intervention: 2 MR, 2 snacks, healthy dinner
• ~50% maintained 10% wt loss (24 #) at 4 years; total group maintained 6.3% at 4 years
• Significant metabolic improvements; 50% reduction in diabetic meds & 27% decrease overall health costs
13
Hamdy O. Diabetes Weight Management in Clinical Practice: Why WAIT Program
Why WAIT Program
• Results more robust than Look AHEAD 4 year results
• Intensive lifestyle modification very valid option to bariatric surgery
• At least as effective as common bariatric surgery (gastric banding), much less costly & fewer side effects
• Comprehensive lifestyle intervention can produce sustainable clinically significant weight loss
14
Hamdy O. Diabetes Weight Management in Clinical Practice: Why WAIT Program
Meal Replacements (MRs) highly effective in T2DM
• MR diet: significantly greater weight loss & less regain after 1 year of maintenance than standard, self-selected, food-based diet
• Statistically significant improvements in: weight loss, BMI, waist/hip measurements, fasting glucose, insulin and HbA1c level, lipids, & BP
• Achieved significantly lower levels of insulin and HbA1c than standard diet group
• 25% reduced diabetic medications
126 overwt/obese adults, T2DM, isocaloric MR vs ADA diet
Cheskin et al; Diabetes Educ 2008;34:118-127
Diabetes and MRs
• MR are viable and cost-effective for weight loss and maintenance in T2DM
• MR diet more effective in reducing metabolic risk factors, insulin & leptin than fat-restricted low-calorie diet
• Superior glycemic control with high-protein VLCD compared to traditional low-fat diet
Hamdy O, Zwiefelhofer D. Curr Diab Rep. 2010;10:159-164
Konig D, et al. Ann Nutr Metab 2008;52:74-78
Wing, Marcus et al; Arch Intern Med 1991;151:1334-40
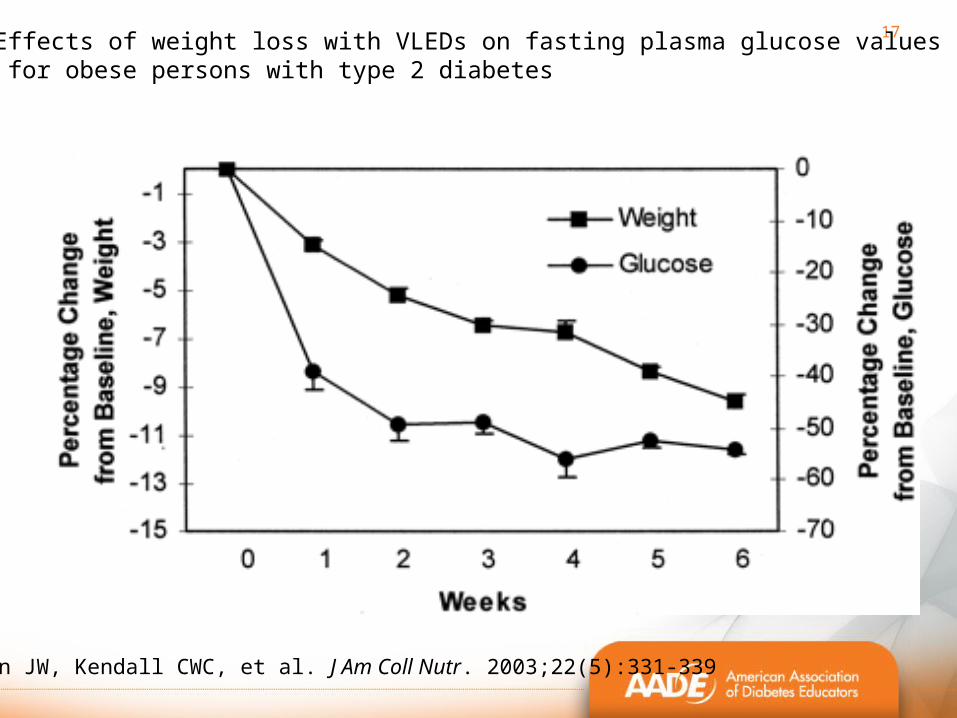
17Effects of weight loss with VLEDs on fasting plasma glucose values for obese persons with type 2 diabetes
Anderson JW, Kendall CWC, et al. J Am Coll Nutr. 2003;22(5):331-339
Joslin New Nutrition Guidelines
• Reduce Daily Caloric Intake by 250-500 calories
• ~40% Carbohydrates, LGI, High Fiber
• 20-30% Protein
• 30% Fat (no TF, 7-10% SF, 20% Mono & Poly UF)
18
www.joslin.org
19
Bariatric Surgery
19
Bariatric surgery
•Most effective treatment for sustained weight loss
•Most patients have complete resolution of T2DM, HTN, OSA, dyslipidemia
•Criteria to qualify:• Ages 16* – 65• BMI ≥ 40• BMI ≥ 35 with serious comorbidities (T2DM, OSA, HTN, cardiovascular disease)
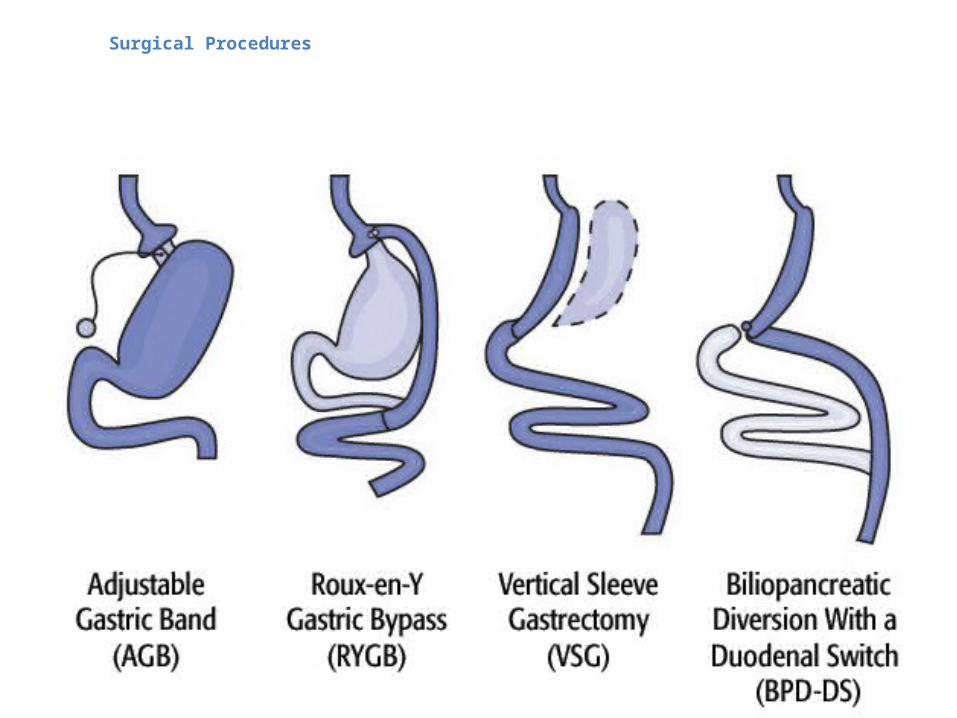
Surgical Procedures
Roux-en-Y gastric bypass (RYGB)
• Gold Standard
• Laparoscopic
• Both restrictive and malabsorptive
• Metabolic effect
• Most common bariatric surgery in US
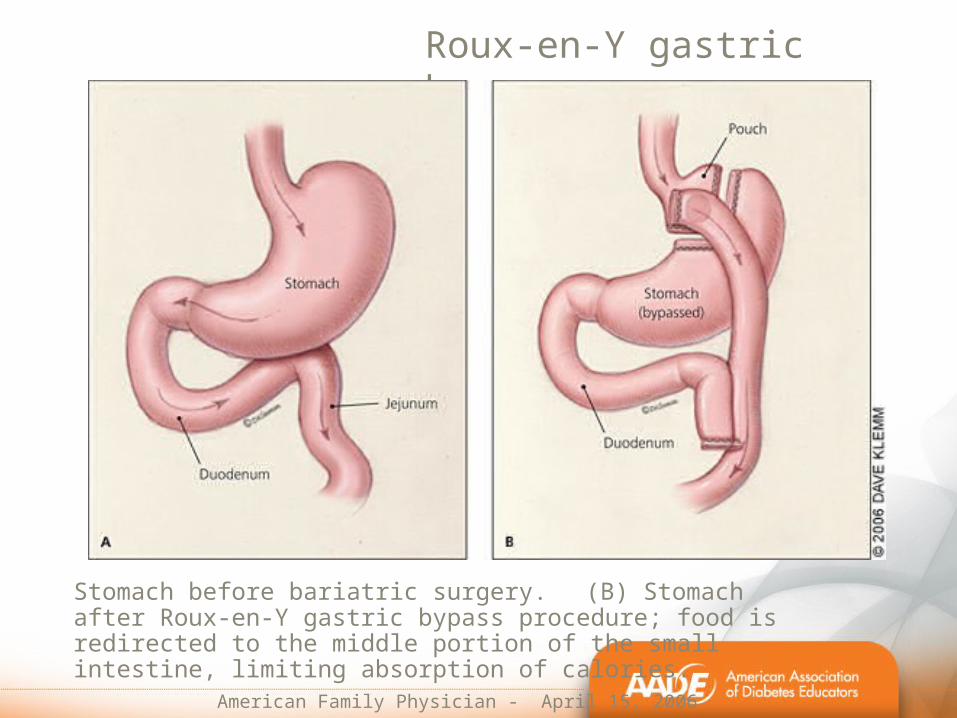
Roux-en-Y gastric bypass
Stomach before bariatric surgery. (B) Stomach after Roux-en-Y gastric bypass procedure; food is redirected to the middle portion of the small intestine, limiting absorption of calories.
American Family Physician - April 15, 2006
Adjustable gastric banding (AGB)
• Laparoscopic
• Primarily restrictive
• Potentially reversible
• Most common bariatric surgery in Australia and Europe
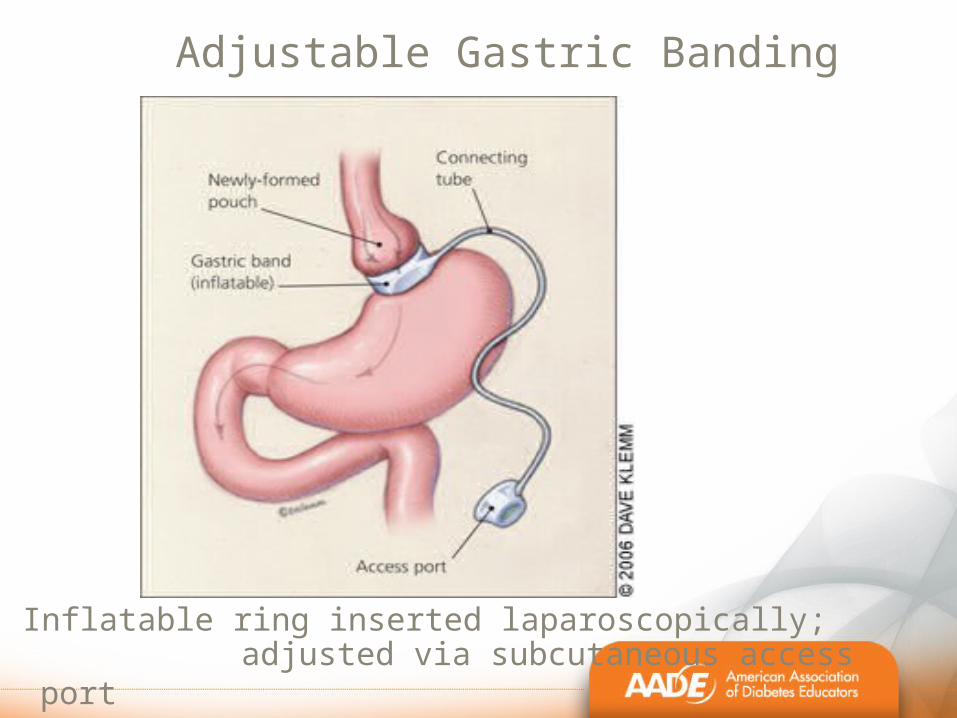
Adjustable Gastric Banding
Inflatable ring inserted laparoscopically; adjusted via subcutaneous access
port American Family Physician – April 15, 2006
AGB: poor long-term outcomes
• 151 consecutive patients 1994-1997; 82 followed:
• Reoperation rate 60%
• 1/3 experienced band erosions
• ~50% require band removal
Himpens, Cadiere et al. Arch Surg. March 22, 2011
RYGB has better risk-benefit profile than LB
• RYGB greater weight loss, increased resolution of diabetes, improved QOL
• Low complication rate similar to LB
• Lower rate late complications (reoperations)
Campos, Rabl et al. Arch Surg. 2011;146(2):149-155.
Vertical Sleeve Gastrectomy (VSG) (Sleeve Gastrectomy; Vertical Gastrectomy)
• 2/3 of stomach removed; remaining stomach 3-4 oz (~ 100 cc)
• Ghrelin not produced (loss of appetite)
• Irreversible
• Purely restrictive although has metabolic effect
• Easy to modify; sometimes done as staged procedure
• Weight loss superior to Band
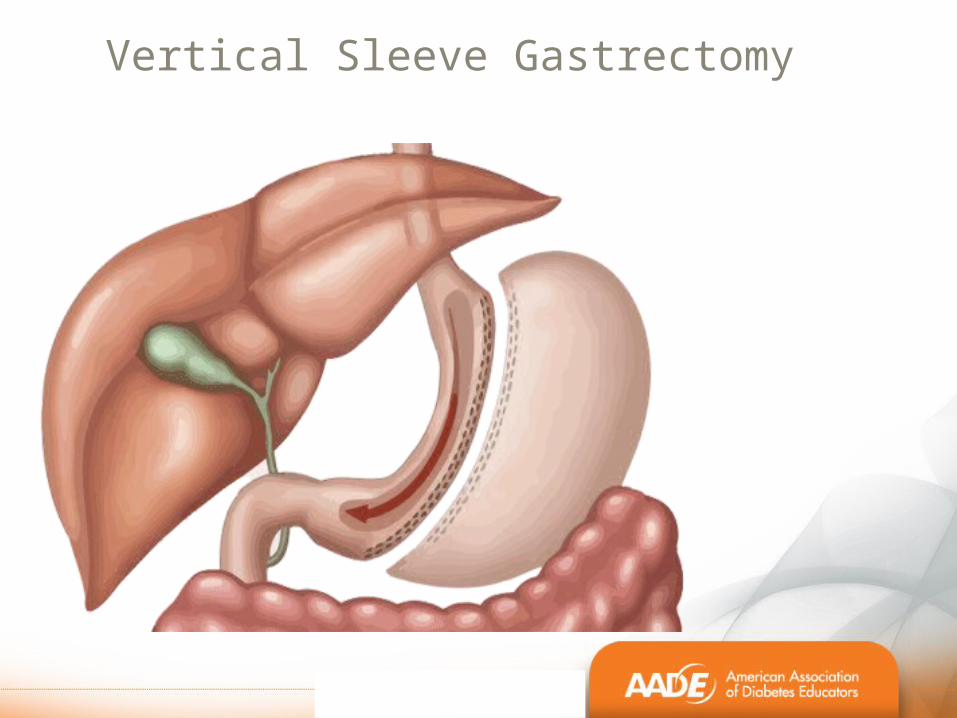
Vertical Sleeve Gastrectomy
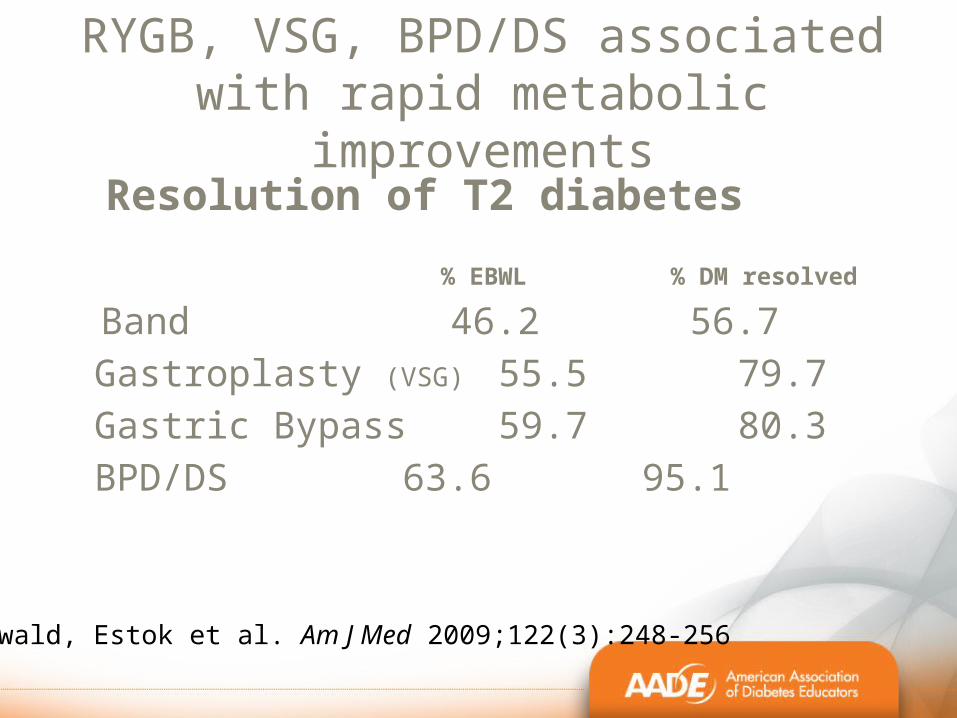
Resolution of T2 diabetes
% EBWL % DM resolved
Band 46.256.7
Gastroplasty (VSG) 55.5 79.7 Gastric Bypass 59.780.3
BPD/DS 63.695.1Buchwald, Estok et al. Am J Med 2009;122(3):248-256
RYGB, VSG, BPD/DS associated with rapid metabolic
improvements
Metabolic improvements
•Metabolic surgery (RYGB, VSG, BPD/DS) state of negative energy balance and rapid weight loss:
– decreased appetite & early satiety, not hunger– Suggests resetting of weight set point to a lower
level
•After metabolic surgery,– rapid improvement in glycemic control in T2DM
patients – diabetes remission occurs almost immediately
before significant weight loss has occurred
– alterations in gut hormones seem to underlie glucose homeostasis
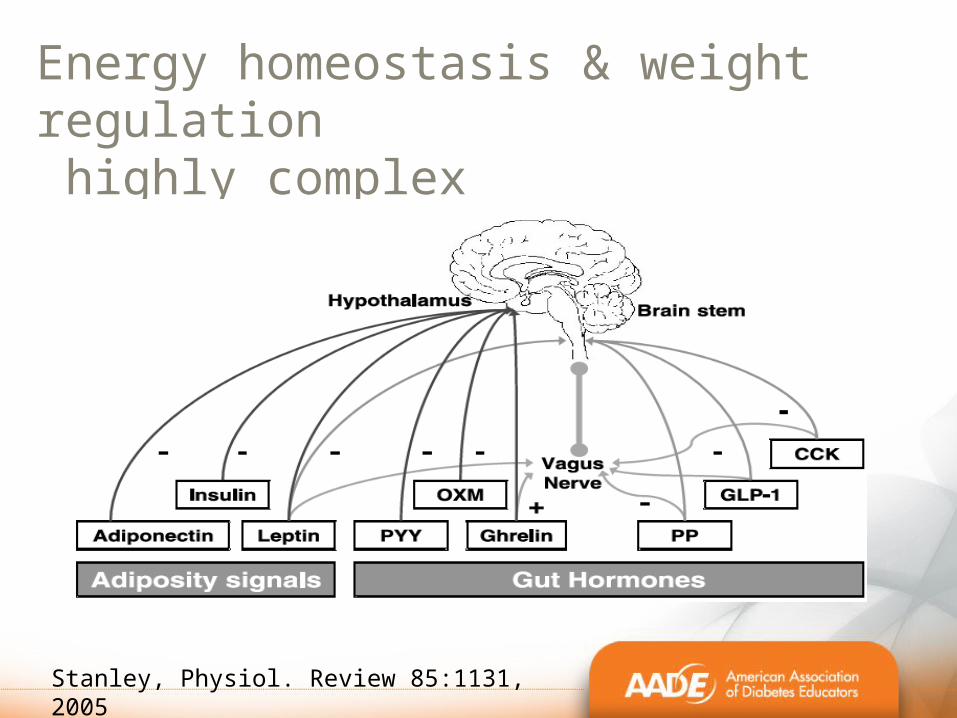
Energy homeostasis & weight regulation highly complex
Stanley, Physiol. Review 85:1131, 2005
Key hormones in energy homeostasis• Hormone expression altered by metabolic surgery:
– Ghrelin– GLP-1– PYY1–36– GIP– Insulin– Leptin– Adiponectin
Metabolic adaptations after RYGB, VSG & BPD/DS
– Ghrelin (appetite stimulating & prodiabetic hormone produced by stomach and duodenum) may decrease *
– Incretin hormones increased (enhance insulin secretion, decrease glucagon secretion, inhibit gastric emptying; exert trophic effects on beta cells in response to meals), CNS effect to reduce food intake
• Glucagon-like peptide-1 (GLP-1)• Gastric inhibitory peptide (GIP)• Peptide YY (PYY)
*early decrease; inconsistent long-term; variable methods used in studies (Harvey et al, 2010)
gut hormones mediate glucose metabolism after bariatric surgery; reduce food intake
.
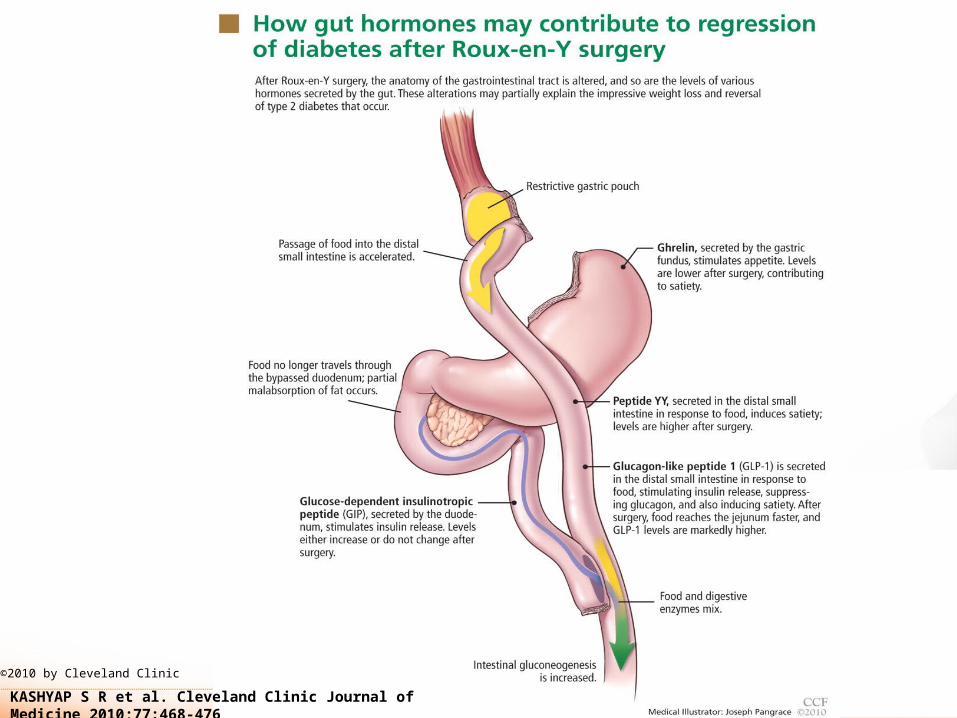
KASHYAP S R et al. Cleveland Clinic Journal of Medicine 2010;77:468-476
©2010 by Cleveland Clinic
Summary of IDF Position Statement for T2DM • Obesity and diabetes epidemics are serious chronic diseases
& major global public health issues
• Prejudices about severe obesity, which also exist within the health care system, should not be a barrier to effective treatment options
• Bariatric surgery can significantly improve T2DM
• Effective, safe, cost-effective therapy
• Bariatric surgery is an appropriate treatment for people with T2DM and obesity not achieving recommended treatment targets with medical therapies especially when there are other major co-morbidities
36
IDF Position Statement for T2DM
• Surgery accepted option in people with T2DM & BMI ≥ 35
• Surgery should be considered as treatment option in persons with BMI 30-35 when diabetes not adequately controlled by optimal medical regimen especially in the presence of other major cardiovascular diseases risk factors
• Procedures must be performed within accepted guidelines
• Requires comprehensive approach and ongoing multidisciplinary care, patient education and follow up
• Surgery should be considered complementary to medical therapies
37
Post-op requirements (Bariatric program requirements vary)
• Maintain good nutrition• 60-80 g protein daily• B12 supplementation:
– 500 mcg SL/d; – 500-1000 mcg oral/d; – 500 mcg/wk nasal; – 1000 mcg/month IM
OR B complex
• Calcium citrate 1200-1800 mg/d (divided doses; separate from iron)
Post-op requirements
• Complete multivitamin (with iron): 1-2/d*
• Menstruating women may need additional iron: 120-200 mg elemental Fe daily divided
– May develop anemia refractory to oral Fe and require parenteral Fe infusions
• Vitamin D if deficient
•Do not recommend prenatal vitamins
• If become pregnant, one complete MV + one PNV daily
•NO GTT!!!
*Ca and Fe need to be separated
Post-op lab parameters
• CBC with differential• CMP• B12• B1 (thiamine)• 25(OH) D• Ferritin• Serum iron• RBC folate (most reliable indicator of folate tissue stores;
steadier value)• Pre albumin (most sensitive laboratory indicator of protein
status) • Lipid profile• PTH intact• *Hgb A1c, TSH (If h/o DM or hypothyroid)
Every 6 months for 1st yr; then yearly
Recommendations for pre- and post-operative diabetic care
• Optimize glycemic control peri-operatively & closely monitor after surgery
• Tips from IU Health Bariatric Center Diabetic Educator Angela Marsden, RD, MS, CHES, CD, CDE:
• Check A1c and lipids pre-op; A1c should be < 8% for surgery
• If A1c > 7.5%, patient contacted and asked what they are doing for BS control
• If A1c ≥ 8%, PCP notified to assist in achieving good control pre-op
41
Pre- and post-operative diabetic careTips from IU Health Bariatric Center Diabetic Educator Angela Marsden, RD, MS, CHES, CD, CDE:
• Patients educated during pre-op class:– Managing glucose during clear liquid diet– Maintaining diabetes self-care behaviors after surgery– How to treat low blood sugar after surgery– Potential causes of hypoglycemia (too many carbs;
poorly timed meals)
• Ongoing support and monitoring
• Data collection following post-op progress: BMI, BP, LDL, A1c
• Address post-op individual concerns: hypoglycemia, dumping syndrome
42
Is there a difference between surgical and medical weight loss?
Weight loss: surgical vs medical
•Surgery is the most effective treatment for sustained weight loss RYBG, VSG metabolic effect
•Surgery is the most effective treatment for diabetes
• Difficult to lose >100# without surgery
• Nonsurgical typical maximum weight loss 1/3:– If 300 #; getting to 200 # good result– if 400 #; 270# best result
Surgical vs. medical weight loss
• Observational study comparing people who lost large amounts of weight through surgery vs non-surgical means (NWCR data)
• Possible to have massive weight loss through intensive lifestyle/behavioral efforts sometimes comparable to surgery
• Marked behavioral differences: non-surgical worked much harder in terms of diet and exercise
Bond DS et al. Int J Obes 2009;33:173-80
What happens after medical weight loss?
•Unfavorable metabolic adaptations occur
• Neuroendocrine changes convey “energy deficit signal”
– Decreased leptin, PYY, cholecystokinin, insulin, amylin (anorexigenic hormones satiety)
– Increased ghrelin, pancreatic peptide (oxeigenic hormones increase appetite
MacLean et al; Am J Physiol Regulatory Integrative Comp Physiol 2009;297
Sumithran et al; NEJM 2011;365;Oct 27, 2011
What happens after medical weight loss?• Increased drive to eat
• Decreased energy expenditure/REE
large energy gap between appetite and expenditure
•~8 kcal/# lost/day less energy
MacLean et al; 2009Sumithran et al; NEJM 2011;365; Oct 27, 2011
ADA position: weight management; J Am Diet Assoc. 2009
Summary
• Weight management is most important therapy for patients with T2DM obesity promotes diabetes; weight loss counteracts it
• Comprehensive lifestyle intervention can produce sustainable clinically significant weight loss
• Metabolic surgery most effective intervention
• Therapeutic lifestyle changes cornerstone of therapy for all approaches
48
49
Marrero DG. J Diabetes Sci Technol 2009;3(4):757-760.
James WPT, J Intern Med 2008:336-352
Nguyen & El-Serag, Gastroenterol Clin North Am. 2010.
Chen, L. et al. The worldwide epidemiology of type 2 diabetes mellitus—present and future perspectives. Nat. Rev. Endocrinol. 2012;( 8):228-236
Wadden TA, West DS, et al. One-year weight losses in the Look AHEAD Study: Factors associated with success. Obesity 2009;17(4):713-72
Joslin Study Shows Short-Term Intensive Weight Loss Program Works For Four Years. Accessed June 14, 2012 at http://www.joslin.org/news/short-term-intensive-weight-loss-program-works-for-four-years.html andhttp://www.joslin.org/care/why_wait.html (description of program)
Diabetes Weight Management in Clinical Practice: Why WAIT Program. Hamdy O. Accessed June 14, 2012 at http://www.joslin.org/docs/WHY_WAIT_2007.pdf
References
50
Wadden TA, Neiberg RH, et al, Four-year weight losses in the Look AHEAD Study: Factors associated with long-term success. Obesity (Silver Spring) 2011;19(10):1987-1998.
Cheskin LJ, Mitchell AM, Jhaveri AD, Mitola AH, Davis LM, Lewis RA, Yep MA, Lycan TW. Efficacy of meal replacements versus a standard food-based diet for weight loss in type 2 diabetes: a controlled clinical trial. Diabetes Educ. 2008 Jan-Feb;34(1):118-27.
Anderson JW, Kendall CWC, et al. Importance of weight management in type 2 diabetes: Review with Meta-analysis of clinical studies. J Am Coll Nutr. 2003;22(5):331-339.
Wing RR, Marcus MD, Salata R, Epstein LH, Miaskiewicz s, Blair EH. Effects of a very-low-calorie diet on long-term glywemic control in obese type-2 diabetic subjects. Arch Intern Med. 1991;151:1334-40.
Hamdy O, Zwiefelhofer D. Weight management using a meal replacement strategy in type 2 diabetes. Curr Diab Rep. 2010;10:159-164.
51
Konig D, et al. Ann Nutr Metab 2008;52:74-78
Himpens, Cadiere et al. Arch Surg. March 22, 2011
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med . 2009 Mar;122(3):248-256.
Kashyap SR et al. Bariatric surgery for type 2 diabetes: Weighing the impact for obese patients. Clev Clin J Med. 2010;77(7):468-476.
Bariatric Surgical and Procedural. Interventions in the Treatment of Obese Patients with Type 2 Diabetes. A position statement from the. International Diabetes Federation Taskforce on Epidemiology and Prevention. Accessed July 17, 2012 at http://www.diabetes.org.br/anexo/idf-position-statement-bariatric-surgery.pdf
Harvey et al; Mount Sinai J of Medicine 2010; 77:446-465).
52
Kohli R, Stefater MA, Inge TH. Rev Endocr Metab Disord 2011.
Bond DS et al. Int J Obes 2009;33:173-80
MacLean PS, Higgins JA, et al. Regular exercise attenuates the metabolic drive to regain weight after long-term weight Loss. Am J Physiol Regulatory Integrative Comp Physiol 2009;297:R793-R802.
Sumithran et al; NEJM 2011;365; Oct 27, 2011
Position of the American Dietetic Association: Weight Management. J Am Diet Assoc. 2009;109(2):330-346. Ferrannini E, Mingrone G. Impact of Different Bariatric Surgical Procedures on Insulin Action and β-Cell Function in Type 2 Diabetes. Diabetes Care March 2009 vol. 32 no. 3 514-520









![The Indianapolis Star - Indianapolis, IN - Publisher ... · The Indianapolis Star - Indianapolis, IN - Publisher, Broadcasting & Media Production | Facebook 1/10/2013 4:09:30 PM]](https://img.pdfslide.net/doc/110x75/5b84ed5a7f8b9a317e8cea29/the-indianapolis-star-indianapolis-in-publisher-the-indianapolis-star.jpg)











![The Indianapolis journal. (Indianapolis [Ind.]) 1899-11-09](https://img.pdfslide.net/doc/110x75/61689f47d394e9041f713c5f/the-indianapolis-journal-indianapolis-ind-1899-11-09-.jpg)