Embed Size (px)
Citation preview

Welcome
0 to 5 transformation of children’s public health
services – towards a definition of school
readiness

•Dr Dympna Edwards
•Assistant Director of Public Health
•St. Helens Council
Early Years Healthy Child Programme – the journey so far

Policy Context for Early Years
• Extend early education and childcare for most disadvantaged
• Early Years Pupil Premium
• Quality of early education and childcare
• Troubled Families Agenda
• SEND Reforms 0-25
• Future in Mind
• Welfare Reform
• Healthy Child Programme

Health Visitor Offer - National Changes
•Health Visitor Call to Action - 2011
• Increased numbers (to 2015)
• Increased universal visits •New National Specification 15/16
• Move to resident not GP registered population
• Each GP practice to have named Health Visitor
• Family Nurse Partnership

Healthy Child Programme Universal Visit
• Antenatal visit at 28 weeks
(new)
• New baby visit (10-14 days)
• 6-8 week maternal mental
health assessment (new)
• 12 month visit
• 2-2.5 year visit - integrated
with early years setting

Family Nurse Partnership
• Evidence based intensive health visiting programme - pregnancy to 24 months
• First time mothers under 20 years of age
• Work alongside mothers and partners
• Better outcomes for both mothers and babies
• In place in many LAs

Commissioning Responsibilities
• Health & Social Care Act 2012
• LA to commission Health Visitor Service & Family Nurse Partnership
• NHS England to commission:
6-8 week physical health check
Early childhood immunisations
Child Health Information Systems
These are not part of Health Visiting Specification

Early Years Perspective - School Readiness
• Target doesn’t have a clearly articulated
indicator, it is left to local determination.
• EYFS seen as a proxy indicator for
school readiness – but undertaken when
many children have completed first year.
• Children more likely to benefit from their
time in school if they get off to a good
start.
• Recognise that school readiness is part
of cycle – family ready, school ready, life
ready.
• 2.5 check – opportunity to identify
needs/deficits whilst still time to put in
additional help or support.
0
10
20
30
40
50
60
70
80
Pe
rce
nta
ge
of
chil
dre
n a
chie
vin
g a
go
od
leve
l of
de
velo
pm
en
t at
th
e e
nd
of
rece
pti
on
North West
England

The Local Opportunity
• 0-5 Transition Strategic Leadership Group
• Merseyside (and more recently Cheshire) LAs, NHSE & PHE
• Quality assuring transition via a sector led approach plus adding value via transformation
Transition
Transformation
Improved Outcomes

The Challenge • Good educational outcomes are key to a successful future.
• The early years are a crucial time for children’s physical, emotional and
cognitive development. School readiness proxy indicator through
Foundation Stage Profile.
• % of children achieving a Good Level of Development at the end of
Reception:
England best: 75%
England average: 60%
• Across Cheshire and Merseyside (not ranked by deprivation):
Lowest performing Local Authority: 46%
Highest performing Local Authority: 63%
• 20% gap: What could we do better/differently in order to improve on
this measure through the 0-5 HCP?

So what have we got? • 0-5 Public Health commissioning resource
(predominantly pays for Health Visitor
Service)
• A mandatory universal health check for
every child at 2-2.5 years
• Children in early years settings having an
ASQ3 assessment
• An idea/aspiration to introduce an integrated
review of development/school readiness
• PH requirement to improve the health of
those at risk of poorer outcomes faster

National insight on our local focus
• Significant interest from PHE in school readiness as a health and wellbeing priority, as well as a life chances enabler.
• Recognition from DH Health Visitor Task Force of the evidence base to school readiness and how the child later functions as a young person and an adult.
• By both parties Cheshire & Merseyside have been credited for the work done to date.

Some questions…
• Would we benefit from a common framework for school readiness across Cheshire and Merseyside?
• To what extent would this help or hinder local areas to commission services to reflect specific local circumstances?
• Could this support a shared approach to child’s development between public services and parents?

Some questions… • Should school readiness be a priority for
wellbeing as well as attainment?
• Would a common definition and agreed key
attributes of ‘school readiness’ help parents,
educationalists and health and social care
professionals to share a common goal? Would
this help to inform more integrated delivery
models from pregnancy through to school? If
so, what (3 or so) key attributes would we
choose as the crucial ones?
• Can the assessments undertaken at 2.5 years
be a reasonable indicator of a child’s/family’s
readiness for school?

0 to 5 transformation of children’s
public health services – towards a
definition of school readiness

Family Fun and School Success: Introducing the Brief Early Skills and Support Index (BESSI)
•Naomi White,
•Irenee Daly, Sarah Foley, Rory Devine, and Claire Hughes

Foundation Years Report: Preventing Poor Children Becoming Poor Adults
• In 2010 Frank Field, MP, conducted independent review on poverty and life chances
• Recommendation to ‘establish a set of Life Chance Indicators’
• Measures for nursery (age 3) and primary school entry (age 5)

School readiness
• Term means different things to different groups: – Politicians (and many parents): literacy, numeracy etc
– Teachers: socio-emotional development & ‘daily living skills’
are key
• Shifting goals for measurement:
– Traditional: identify the small number of children who need
special education
– Current: identify more common problems, to ensure that curriculum meets the needs of all children

From tasks to questionnaires: the EDI •Janus and Offord (2000; 2007)
• 5 child scales:
– social, emotional, physical, cognitive and communicative
• Administered to large samples in Canada, Australia, China, Scotland
•BUT:
• Not used with children < 4 years
• 104 items (7 pages)

A new measure – The Brief Early Skills & Support Index (BESSI)
• One page (30 items) – with simple response scale (Strongly Disagree / Disagree / Agree / Strongly Agree)
• Includes (as name suggests) items about family support
• Also includes items selected to be relevant to very young children (e.g., ‘enjoys songs and rhymes’)
Developing the BESSI
• Initial grid of 80 items rated by 23 teachers as useful / not useful
• Focus groups with reception teachers and head teachers
• Reduced set of 50 items completed for 185 children
• Filtered out items with poor sensitivity / unclear item wording

The BESSI contains 4 Subscales
Behavioural Adjustment 12 items
Social skills, Self-regulation
‘Trouble sitting still’
Language & Cognition 6 items
Early literacy/numeracy abilities
‘Enjoys songs and rhymes’
Daily Living Skills 6 items
Ability to dress/feed self ‘Does not need help with
fork’
Family Support 6 items
Parental support for learning
‘Talks about fun activities at home’

• 1473 UK nursery and reception children
• Age Range: 2.50 – 5.50 years
• 49% Male and 89% White British
• 25% Eligible for Free School Meals
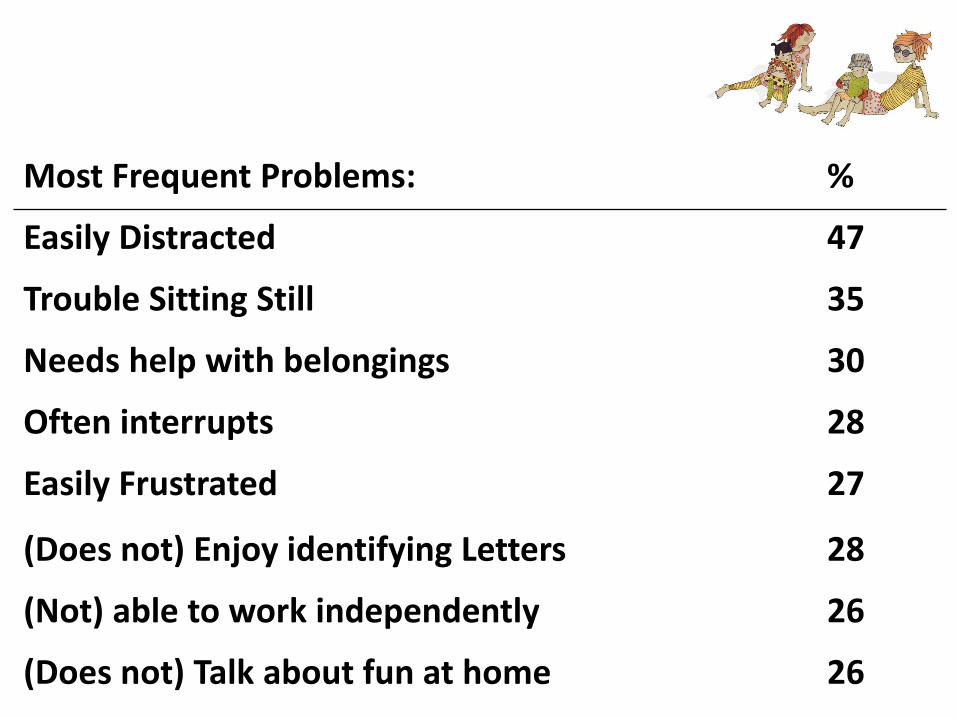
Most Frequent Problems: %
Easily Distracted 47
Trouble Sitting Still 35
Needs help with belongings 30
Often interrupts 28
Easily Frustrated 27
(Does not) Enjoy identifying Letters 28
(Not) able to work independently 26
(Does not) Talk about fun at home 26

Common problems were more frequent in boys than in girls…. Item Boys % Girls %
Easily Distracted 56 38
Trouble Sitting Still 45 25
Needs help with belongings 40 20
Often interrupts 31 24
Easily Frustrated 35 19
(Does not) Enjoy identifying Letters 24 15
(Not) able to work independently 35 17
(Does not) Talk about fun at home 31 21

Gender
Age
Free School Meal
Older Sibling
Ethnicity
Behavioural Adjustment
Language and
Cognition
Daily Living Skills
Family Support
.23
.26
.34
.14
Gender effects on all BESSI subscales

Item FSM Not
Easily Distracted 57 43
Trouble Sitting Still 44 32
Needs help with belongings 37 29
Often interrupts 34 25
Easily Frustrated 35 26
(Not) Enjoy identifying Letters 30 12
(Not) able to work independently 33 24
(Not) Talk about fun at home 47 20
Common problems more frequent in children from low-income families

Gender
Age
Free School Meal
Older Sibling
Ethnicity
Behavioural Adjustment
Language and
Cognition
Daily Living Skills
Family Support
.13
.28
.16
.40
FSM effects on all BESSI subscales

Gender
Age
Free School Meal
Older Sibling
Ethnicity
Behavioural Adjustment
Language and
Cognition
Daily Living Skills
Family Support
.58
.56
.45
Family Support explains FSM differences

Behaviour Adjustment
Language & Cognition
Daily Living Skills
Praise .13 -.61* -.42
Punctuality .02 -.02 -.32*
Misses School -.01 .12 .14
Talks about Fun .22* .68*** .46***
Reads Regularly .03 .27 .45**
Sleepy .13 .29* .39**
A closer look at Family Support
Controlling for effects of age, gender, sibs, income and ethnicity

Key findings from the BESSI
• The BESSI works equally well for boys and girls, and for children from 2.5 to 5.5 years
• Boys show more problems than girls (in behavioural adjustment, cognitive development and daily living skills)
• Reduced family support explains increased problems in children from low income families
• No effect of ethnicity

Current work with the BESSI
• How much do BESSI scores change over 6 months? • How similar or different are parents’ versus teachers’ ratings?
• Does observational coding validate ratings of family support?
• Can the BESSI be used to assess impact of interventions to promote
family support?
• Does the BESSI work in a similar way for ethnic minority children?
• Is the BESSI suitable for use in other countries (first step, Singapore)?

Current work with the BESSI - Can you help?
• We’re developing a user manual and scoring guide for teachers for the BESSI
• This will include a spreadsheet that will provide a profile of each child’s strengths and difficulties
• We’d love to hear from any Foundation Years staff who would be interested in test-driving it for us!

Acknowledgements: Westminster Foundation &
Foundation Years Trust – for funding support www.foundationyearstrust.org.uk
All the schools and nurseries in the Wirral – for taking part. [email protected]

0 to 5 transformation of children’s
public health services – towards a
definition of school readiness

Ensuring Every Child has the
Best Start in Life: Ready to learn at 2 –
2.5yrs, ready for school at 5yrs
Alison Burton – Lead for Maternity and Early Years, PHE

The Best Start in Life - Why is this important?
• Currently 60.4% of children in England (2013/14) achieve a good level of
development at the end of reception as measured by the Foundation Stage Profile. Department of Education
• Around 1 in 10 (9.5%) of children are obese at age 4/5 yrs. National Child Measurement
Programme (2013/14)
• 27% of children have tooth decay at age 5 yrs. Commissioning better oral health for children and
young people . PHE 2013
• 7% of children around five years of age have speech, language and communication
needs. (SLCN) Tomblin JB, et al (1997)
• 1 in 10 women are estimated to experience mild to moderate post natal depression. NICE 2007
• Up to 20% of women develop a mental health problem during pregnancy or within a
year of giving birth. This can lead to disordered early attachment with long term
consequences for mother and baby. The Costs of Perinatal Mental Health Problems, Bauer et al., LSE,
Centre for Mental Health, 2014
• Obesity in childhood increases risks of becoming obese adults. Annual Report of the Chief
Medical Officer 2012. Our Children Deserve Better: Prevention Pays. Department of Health, 2013
• 70% of adults are predicted to be obese or overweight by 2034 From Evidence into Action:
Opportunities to Protect and Improve the Nation’s Health. PHE. 2014
37

Measuring outcomes School readiness: Percentage of children achieving a good level
of development at the end of reception (age 5 years) DfE via PHOF
60.4% in 13/14.
Ranging from
41.2 to 75.3%
1.8X variation
38
FSP DIMENSIONS
• Personal
• Social
• Emotional
• Physical
• Communication
• Language
• Maths
• Literacy

Public health outcome frame work data (1)
PHOF indicators Highest Lowest Period
1.01 Children in poverty(under 16)
London (23.7%) South East (14.2%) 2012
2.02 Breastfeeding (initiation)
South West (78.6%) North East (60.3%) 2013/14 – no figure for London
2.03 Smoking status at time of delivery
North East (18.8%) London (5.1%) 2013/14
2.04 under-18s
conception (inc under-16s)
North East (30.6 per 1,000 pop)
South East (20.5 per 1,000 pop)
2013
Tooth decay in
children aged 5 - % of
children with decay
experience NOT PHOF
North West (34.8%) South East (21.2%) 2011/12
39
Regions

Public health outcome frame work data (2)
PHOF indicators Highest Lowest Period
1.01 Children in poverty(under 16)
Tower Hamlets (37.9%) Wokingham (6.6%) 2012
2.02 Breastfeeding (initiation)
Wandsworth (93.0%) Stoke-on-Trent (36.6%) 2013/14
2.03 Smoking status at time of delivery
Blackpool (27.5%) Westminster (1.9%) 2013/14
2.04 under-18s
conception (inc under-16s)
Stoke-on-Trent (43.9 per 1,000 pop)
Rutland (9.2 per 1,000 pop)
2013
Tooth decay in
children aged 5 - % of
children with decay
experience NOT PHOF
Leicester (53.2%) Brighton and Hove (12.5%)
2011/12
40
Upper tier local authorities (ie counties, UAs and LBs)

Best Start in Life:- Local picture Around 58.9% of children in Cheshire and Merseyside achieve a good level
of development at the end of reception compared with 60.4% across England.
This proportion varies from 45.6% to 62.8% across Cheshire and Merseyside
local authorities.
Nearly 6,200 Cheshire and Merseyside children aged four to five years
have excess weight. This equates to 23.6% of the age group, which is
significantly higher than the England average of 22.5%. In one local authority
in the area, the proportion is as high as 29.5%.
Around 91.4% of five year olds in Cheshire and Merseyside have received
their second dose of the MMR vaccination. This is higher than the England
average of 88.3%. In all local authorities in the area the proportion of children
that have received their second dose is higher than 90%.
Source: Public Health Outcomes Framework
41 Change in Header and Footer

42 Change in Header and Footer
Cheshire & Merseyside: Tooth decay (mean dmft) in
children aged 5
England average
Source: Public Health
Outcomes Framework

From evidence into action: opportunities to protect
and improve the nation’s health (October 2014)
Ensuring every child has the best start in life. Ready to learn at 2 – 2.5yrs, ready for
school at 5yrs
Over the next 18 months PHE will:
• support local authorities in developing integrated children and young people’s
services as they take on commissioning responsibilities for the Healthy Child
Programme for 0-5’s
• promote the importance of high-quality universal services as a foundation for good
health for all our children and as a platform for early intervention and targeted support
• develop and strengthen the evidence, including working with the Early Intervention
Foundation as a ‘What Works Centre for Early Intervention’
• expand the Start4Life Information Service for Parents from 0-2 years to 0-5 years and
sign up over 200,000 more parents
• expand newborn bloodspot screening to include four new inherited metabolic
disorders
• work with NICE on the implementation of the quality standards and pathways for
emotional and social wellbeing in early years
• lead and co-ordinate the Childhood Flu Programme, working with NHS England
• increase coverage of measles, mumps and rubella immunisations for all children at
five years https://www.gov.uk/government/publications/from-evidence-into-action-opportunities-to-protect-and-improve-the-nations-health
43 43

Building on current assets Significant system change and investment in early years over 5 years:
• Health visitor implementation plan – workforce expansion
• Service transformation:
o 4 levels: community, universal, universal plus & universal partnership plus
o 5 mandated reviews: A/N, NBV, 6/8 weeks, 1yr., 2 - 2.5 years old
o 6 high impact areas: transition to parenthood, maternal mental health, obesity,
preventing admissions to hospital, breast feeding, child development
• Family Nurse Partnership – 16 000 places, RCT
• Universal 2 – 2.5 year review
• Transfer of commissioning responsibilities for 0 – 5’s PH to LAs
• ChiMat resources and expertise: analytical capacity, online resources etc
• PHE: Centres’ expertise and local leadership, nursing and midwifery, social
marketing, drugs and alcohol, immunisations, mental health, health equity etc
44 44

Best Start in Life - High level aims • Closing the gap in inequalities in important health outcomes during pregnancy and
early years in particular: transition to parenthood (attachment), maternal mental
health, breast feeding, oral health, child obesity and child development
• Sustaining universal primary prevention services for 0 – 5’s. Able to undertake risk
assessment and early identification of need, including universal assessment and
support to promote sensitive attuned parenting and promote secure attachment
• Ensuring that knowledge and intelligence including evidence of effectiveness, data
and soft intelligence are readily available to inform need, service provision and
targeted support
• Sector led improvement – articulating what “good” looks like, support local systems to
join commissioning of universal public health prevention services with early
intervention and specialist services – a holistic offer
• Workforce development – identify core competencies, shared quality standards,
critical success factors, joint training
45 45

PHE tools • PHE have a number of tools available already which help local areas when they are planning
public health services for children who are aged 0 to 5 years old.
• 2014, published early years profiles which show all local councils how they compare with the
average for England, making it easy for them to identify areas for improvement.
http://atlas.chimat.org.uk/IAS/dataviews/earlyyearsprofile
• in addition, the profiles give trend information so that a council can see whether they have made
an improvement since 2010 on key issues for this age group such as breastfeeding, obesity and
injuries.
• we also published an early years report for each council which gives more background to the
profiles and help with interpreting the data.
• http://atlas.chimat.org.uk/IAS/profiles/profile?profileId=52&geoTypeId=
• alongside these existing tools, we now have estimated data for electoral wards for some of the
key indicators such as teenage mothers, hospital admissions as an emergency in under 5s and
A&E attendances
• http://www.localhealth.org.uk/#v=map4;l=en
• local specialists in child health data
• http://www.chimat.org.uk/default.aspx?QN=CHIMAT_LOCAL
46

Local Authority Child Health Profiles
Official Statistics, 19th March 2014
Standard template
Tailored at a regional level
“We found this information very useful
for setting priorities and assessing
interventions”

A Benchmarking Tool (Outcomes Framework)
for Children & Young People
• See, http://www.fingertips.phe.org.uk/profile/cyphof
• Benchmarked for Local Authorities
• Broken down to greater detail where possible
48 48 48

0 to 5 transformation of
children’s public health
services – towards a
definition of school readiness

School Readiness
www.sefton.gov.uk
The evidence is overwhelming that for optimal effectiveness, intervention should be focused on the earliest years, and ensure that children arrive at school ‘school
ready’ WAVE Trust 2010
“School readiness involves more than just children.
School Readiness, in the broadest sense, is about
children, families, early environments, schools
and communities. Children are not innately
“ready” or “not ready” for school. Their skills and
development are strongly influenced by their
families and through their interactions with other
people and environments before coming to
school.” Maxwell & Clifford 2004
School Readiness

Policy Direction and Drivers
• Sefton’s Early Intervention & Prevention (EIP)
Strategy
• Re-structure of early years services
• Political landscape
• Breadth of partnership work
• Health agenda - Integrated assessment with
health for two year olds
School Readiness

Early childhood services cover integrated provision from pre
birth to the end of the Early Years Foundation Stage
Sefton approach to School Readiness
School Readiness
Education
Health Parenting and family support

School
Readiness
Coherence
Consistency
Collaboration
Challenge

School Readiness
CHILD READY Children happy,
healthy and ready for school
FAMILY READY Effective integrated
working across child and family services with clear
focus on the most vulnerable and earlier
intervention
SCHOOL READY All children
attending good and outstanding
settings
COMMUNICAT ION
F I VE to TH R I VE

Design Fundamentals
• Focus on younger children
• Going beyond education
• Development aware
parenting
• Pedagogical conversations

Toxic Trio Parental
mental health Poor housing
Domestic violence
Family debt
Transient population
Welfare reform
Attachment disorder
Integrated health review
Parental drug and alcohol
misuse Neglect
Family breakdown
CSE LA & Health
re-organisation

• Proportion of children achieving a good level of
development
• Closing the gap between vulnerable children and others
– Gender differences
– Free School Meals
• CHIMAT Child Health Profiles
• Healthy Child Programme
• Integrate services in order to develop, retain and embed
high quality and expertise across the sector
• Parenting programmes
Measures and Performance

Thank you for attending
Presentations will be available at
www.champspublichealth.com
GROUP WORK – KEY ATTRIBUTES
1) Resilient
2) Confidence
3) Empathy
4) Positive
5) Sense of wonder
6) Good communicators
7) Communicators
8) Self worth
9) Sociable
10) Creative
11) Healthy and loved
12) Aspirations
13) Point of difference?
14) Attachment to parents?
15) Independence
16) Able to play
17) Feeling secure with own feelings (internally)
18) Take risk
19) Environment
20) Be happy/joyful
21) Cared for
22) Mindfulness

Four Themes
• Parents
• Communication and Language
• Relationships and Social Interaction
• Self-awareness

![Welcome [champspublichealth.com] · 11th February 2016 . Welcome . NO MORE suicide – time to change 2016 Suicide Prevention Summit Thursday 11. th. February 2016 Everton Football](https://img.pdfslide.net/doc/110x75/5f7da5385536905d0e4d95d7/welcome-11th-february-2016-welcome-no-more-suicide-a-time-to-change-2016.jpg)



























