Embed Size (px)
DESCRIPTION
Welcome Everybody To My Presentation On Shoulder joint. Introduction. It is a ball and socket type of synovial joint It is a multiaxial spheroidal jt Roughly hemispheric head of the humerus form the ball and shallow glenoid fossa of scapula form the socket. - PowerPoint PPT Presentation
Citation preview

Welcome
Everybody
To
My
Presentation
On
Shoulder joint
Introduction
It is a ball and socket type of synovial jointIt is a multiaxial spheroidal jtRoughly hemispheric head of the humerus form the ball and shallow glenoid fossa of scapula form the socket.Skeletally jt is weak. It depends for stability and support on it’s surrounding muscle rather than it’s shape and ligaments.Only one third of humeral head is in contact with the glenoid fossa at any time.




Angle of inclination: in the frontal plane, the axis of the head and neck of humerus form an angle of 130°-140° with the long axis of shaft of femur.Because of this angulation, the centre of the humeral head lies about 1cm medial to the long axis.
Angle of retroversion: an angle to the shaft of the humerus, the axis of the head and neck is rotated backwords against the shaft some 30°-40°, this is caled the angle of retroversion.


Articular surfaceTwo articular surface:
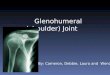
Glenoid fossa:
glenoid fossa is situated at the supero-lateral angle of the scapula
faces laterally, anteriorly and slightly superiorly. Concavity of glenoid fossa is irregular and less deep
than convexity of head of the humerus. The articular surface the fossa is little more than the
head of the humerus It ls covered by hyaline cartilage Hyaline cartilage is thinner centrally and thickest
peripharally


Head of the humerus:
It represents two-fifths of a sphere It faces superiorly, medially and anteriorly Covered by hyaline cartilage On the humerus hyaline cartilage is thickest
centrally and thinner peripherally


Joint capsule
It is like a cylindrical sleeve and situated between two bones Majority fibres of the capsule passes horizontally between scapula and humerus. But some oblique and transversre fibres are also found On the scapula, the capsule attaches just outside the glenoid labrum anteriorly and inferiorlyOn the humerus, capsile attaches to the anatomical neck,medial to the greater and lesser tubercle

Continuation
Anterior part of the capsule is thickened and strengthened by three glenohumeral ligaments.
Superoposterior part is strengthened by coracohumeral ligament
In anatomical position of the arm the lower part of the capsule is lax and forms a redundant fold.
In abduction of arm lower part become s taut


Continuation
It is supported by the: supraspinatus (above) Infraspinatus and teres major (behind) Subscapularis (in front) Long head of triceps (below)
Capsule has two or three openings: Below the coracoid process Between two tubercles Inbursa undea the infraspinatous tendon


Synovial membrane
This lines the capsule and covers parts of the anatomical neck
The synovial membrane is reflected from the margin of the glenoid cavity over the labrum
The tendon of the long head of the Biceps brachii passes through the capsule and is enclosed in a tubular sheath of synovial membrane


Glenonoid labrum
It is lintra-articular structure It is a fibro-cartiliginous rim round the glenoid
fossa It is triangular in section 4mm deep It’s base attaches to the margin of the glenoid
fossa. Outer surface attaches to the joint capsule
superiorly and posteriorly Inner surface is in the contact of head of humerus It protects the joint and assists lubrication


Capsular Ligaments
Glenohumeral ligament: Superior glenohumeral ligament: It is splender shaped It arises from upper part of the glenoid labrum It runs laterally parallel to the biceps tendon to
the upper tendon to the upper surface of the lesser tubercle
Middle glenohumeral ligament:Arises from below the superior glenohumeral
ligamentAttaches to the humerus on the front of the lesser
tubercle below the insertion of subscapularis

Inferior glenohumeral ligamrent:
It is best developed of the three ligaments It arises from the anterior border of the glenoid
labrum It descends slightly obliquely to the
anteroinferior part of the anatomical neckThe antero-superior edge of the inferior ligament
is thickened and known as superior bandThe thickening of the anterior part of the capsule
to which inferior ligament attaches is known as axillary pouch




Function of glenohumeral ligament: They have no stabilizing function Lateral rotation of the humerus put all three
ligaments under tension Medial rotation relaxes them In abduction only the middle and inferior
ligament become taut and superior ligament become relaxed

Transverse humeral ligament: It is formed by some of the transeverse fibres of
the capsule At the upper end of the intertubercular groove,
the transverse humeral ligamentbridges the gap between the greater and lesser tubercles.
It hold the biceps tendon in the intertubercular groove.


Intra- articular ligament
These ligaments are considered as accessory ligamentCoracohumeral ligament:
It is strong and broad It arises from the lateral border of the coracoid
process near its root. It passes laterally above the intertubercular
groove to attach to the anatomical neck to the greater and lesser tubercle
Anterior part of the ligament is free. But laterally it fuses with the tondon of subscapularis
It inserted in lesser tubercle


Coracoacromial ligament: It is not directly associated with the joint It is a strong and triangular ligament It forms with the coracoid and acromion
process, a fibro- osseous arch above the head of the humerus
Its anterior and posterior part is thicker than intermediate part.



Bursae
between the subscapular tendon and articular capsuleSometimes between the infraspinatous tendon and capsuleSubacromial bursa: between deltoid and capsule.On the superior acromial aspectBetween coracoid process and capsuleSometimes behind coracobrachialisBetween teres major and the long head of biceps


Muscle
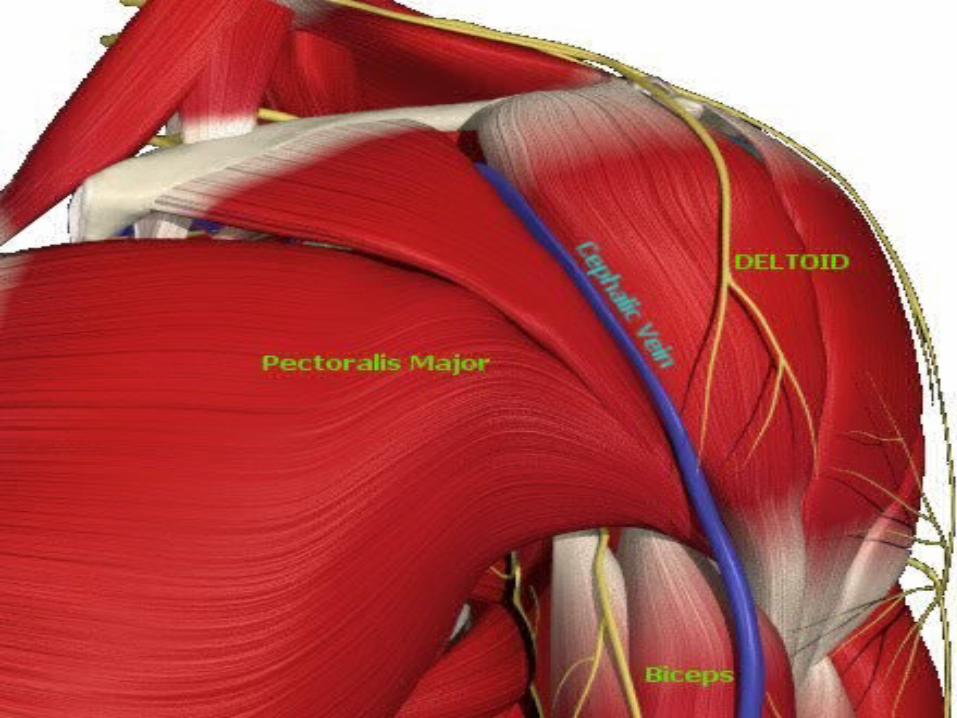
Deltoid (anterior fibre): Origin: Arises from the anterior border
and upper surface of the lateral third of the clavicle
Insertion: Function:

Deltoid (middle fibres): Origin: Arises from the lateral margin and
upper surface of the acromion. Insertion: Function:

Deltoid (posterior fibre): Origin: Arises from the lower lip of the
posterior border of the spine of scapula, as far back as the triangular surface at its medial end.
Insertion: Function:




Pectoralis major: Origin: Insertion; Function:



Coracobrachialis: Origin: Insertion: Function:



Biceps: Origin: Insertion: Function:



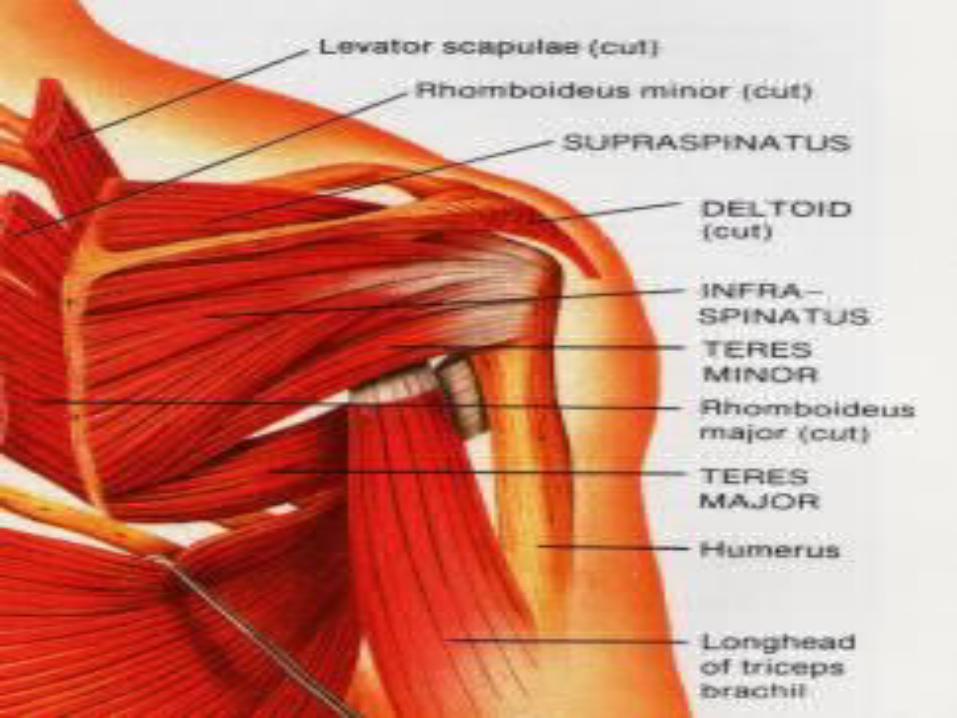
Teres major: origin: Insertion Function;



Latissimus dorsi: Origin: Insertion: Function:



Supraspinatous: Origin: Medial two-thirds of the
supraspinatus fossa of scapula Insertion: Superiorly of the greater tubercle
of the humerus Function:



Serratus anterior: Origin: Originates on the surface of the
upper eight ribs at the side of the chest and inserts along the entire anterior length of themedial border of the scapula
Insertion: Function:


Trapezius: Origin: Arises from theoccipital bone, the
ligamentum nuchae, the spinous process of the seventh cervical, and the spinous processes of all the thoracic vertebrae
Insertion: It inserts on the lateral clavicle, the acromion process, and into the spine of the scapula.
Function:



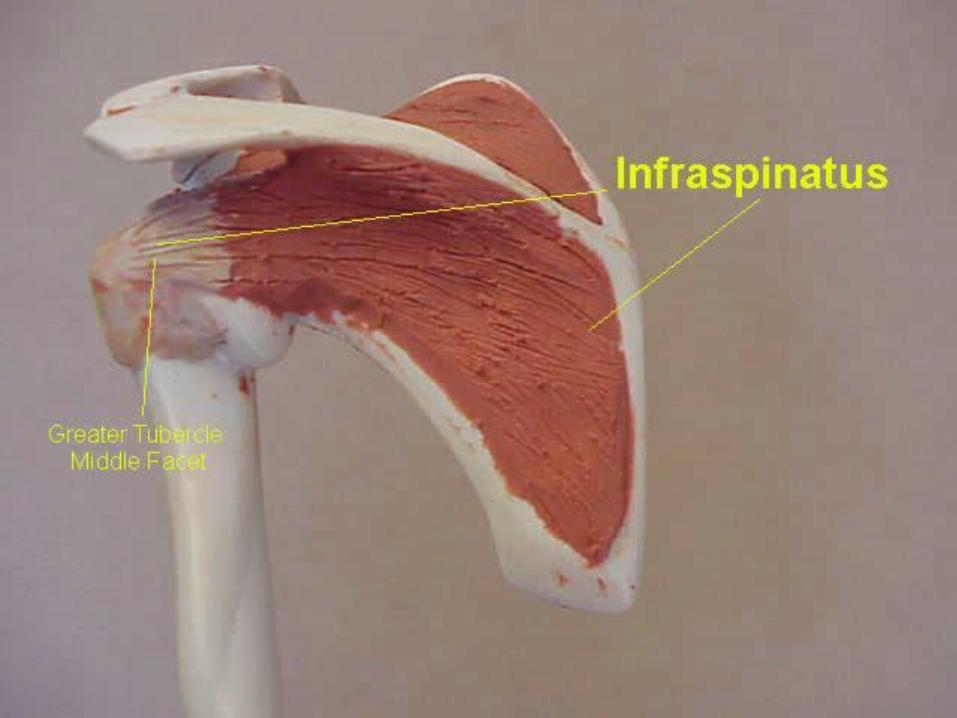
Infraspinatous: Origin: infraspinatus fossa just below the
spine of the scapula Insertion: Posteriorly on the greater tubercle
of the humerus Function:


Teres minor: Origin: Posteriorly on the upper and middle
aspect of the lateral border of the scapula Insertion: Posteriorly on the greater tubercle
of the humerus Function:




Blood and nerve supply
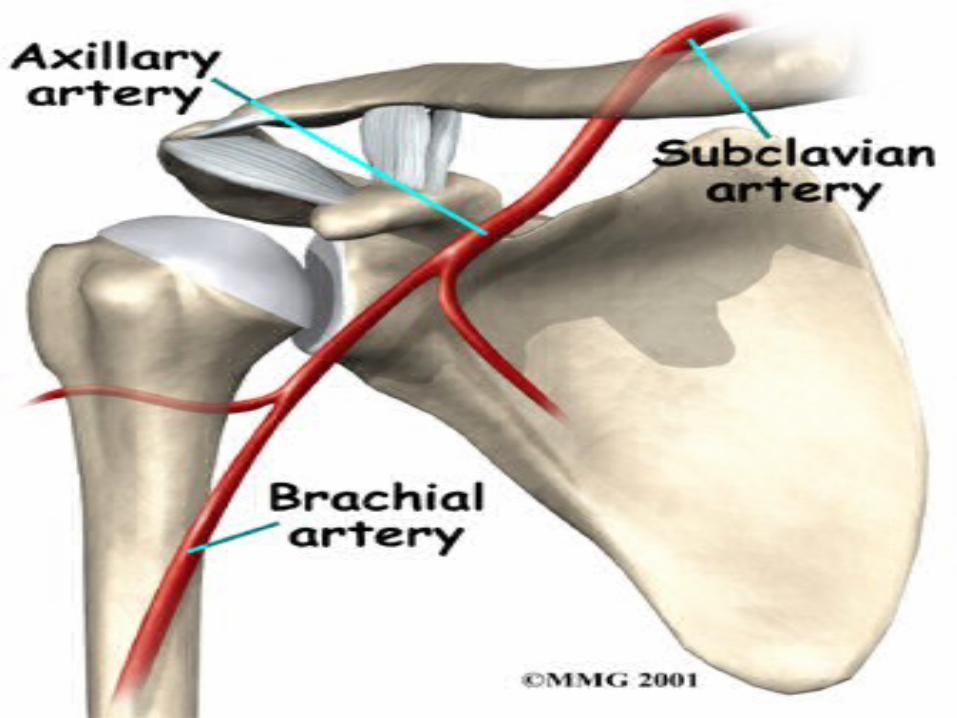
Artial supply: it is from numerous sources around the joint
Suprascapular branch of subclavian artery Acromial branch of thoracoacromial artery Anterior and posterior circumflex humeral
arteries Three are all branches of axillary artery

Venous drainage is by similarly named veins which drains into the external jugular and axillary veinsLymphetic drainage of the joint is to the lymph nodes within the axilla and passes into subclavian lymph trunkNerve supply:
Suprascapular Axillary] Subscapular Lateral pectoral Musculocutaneous Root value of C5,6 and7

Stability Factors responsible for stability:
The glenoid labrum- it deepening the glenoid fossa. And make the joint surface congurent
Rotator cuff- Most important factor Very close it the joint and fuse with lateral part of capsule. They act as ligaments Inferior part of capsule is weak and unsupported. But as
the arm gradually abducted the long head of triceps and teres major support this



Muscle of pectoral girdle and humerus:Long head of biceps: gives support over the
superior part of jointLong head of triceps: gives support below
the joint Coracoacromial arch: it prevent upward
displacement of the head of the humerus


Movement Flexion :
Flexion and extension occur about an axis prependicular to the plane of the glenoid fossa
In flexion the arm moves forward and medially at an angle of 45° to the sagital plane.
Range is 110°-180° It is produced by the anterior fibres of deltoid,
pectoralis major, coracobrachialis and biceps
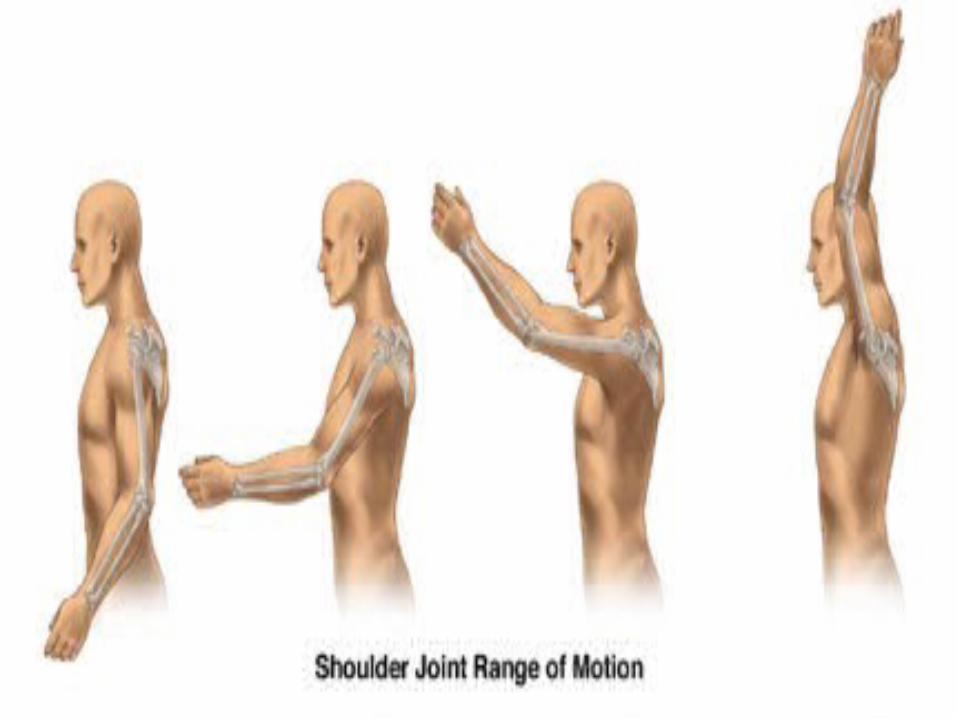

Extension: In extension arm moves backwords and laterally Range is 70°-90° Extension is limited by greater tubercle of the
humerus coming into contact with the coracoacromial arch
Extension is produced by the posterior fibres of deltiod, teres major and latissimus dorsi
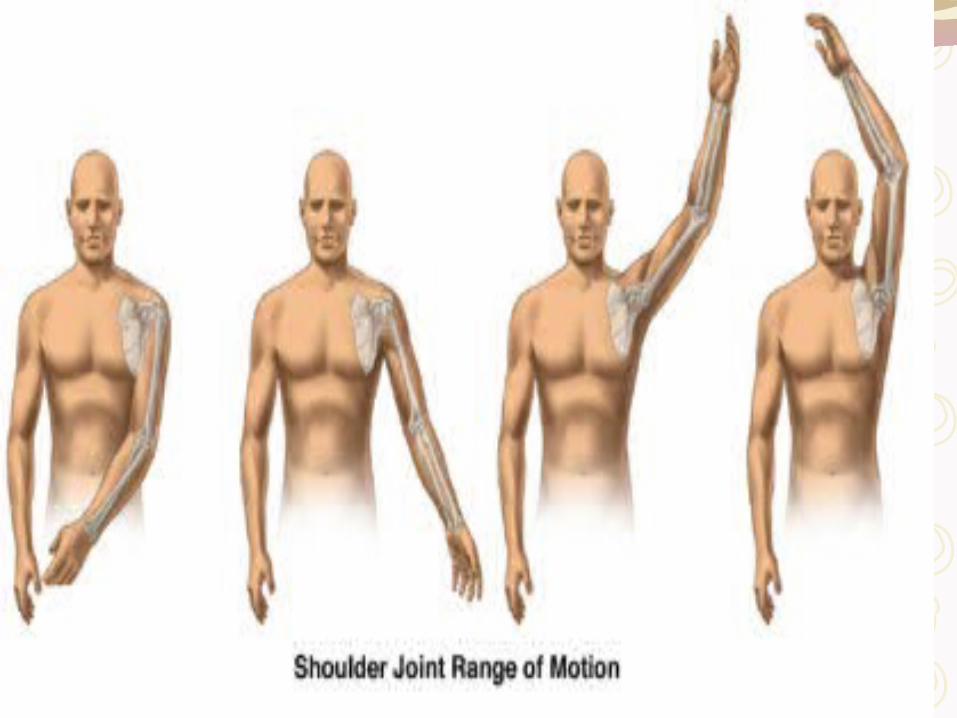
Abduction: In abduction the arm moves anterolaterally away from the
trunk Total range is 120° Only first 30° movement occurs without scapular rotation The terminal part of the shoulder joint abduction is
accompanied by lateral rotation of the humerusIt is due to provide further articular surface on the head of the humerus for the glenoid fossa
Abduction of the medially rotated humerus is limited by tension in the posterior capsule and lateral rotators

First 20° abduction is initiated by supraspinatus muscle and deltoid continues the movement
If deltoid is paralysed, supraspinatus is not strong enough to fully abduct the shoulder.
If supraspinatous is not functioning, deltoid can not initiate abduction

Adduction: In adduction the arm moves anteromedially Adduction is produced by ecentric
contraction of serratus snterior, trapezius, deltoid and supraspinatous

Rotation
Rotation is limited by the extent of articular surface
The range of rotation varies with the position of arm. It is greatest when the arm is by the side. Decreasing to 90° with the arm horizontal. And being negligible as the arm approaches vertical

Medial rotation: Medial rotation causes the anterior surface
of the humerus to be turned medially The maximum range is 90° Medial rotation is produced by
subscapularis, pectoralis major, latissimus dorsi, teres major and anterior fibre of deltoid

Lateral rotation: In lateral rotation the anterior surface of the
humerus is turned laterally The range is 80° It is produced by infraspinatous, teres minor
and posterior fibre of deltoid