Embed Size (px)
DESCRIPTION
WELCOME! Region IX Discussion on Gonorrhea Control Hosted by CDC and Region IX IPP Coordinator. The disseminated findings and conclusions in this presentation have not been formally reviewed by CDC and should not be construed to represent any agency determination or policy. - PowerPoint PPT Presentation
Citation preview

WELCOME!
Region IX Discussion on Gonorrhea Control
Hosted by CDC and Region IX IPP Coordinator
The disseminated findings and conclusions in this presentation have not been formally reviewedby CDC and should not be construed to represent
any agency determination or policy.

Regional Meetings Smaller meeting → more discussion
Learn from peers
Emphasize program improvement
Accommodate regional similarities (morbidity, resources, infrastructure, populations)

Meeting Objectives
Increase understanding of gonorrhea epidemiology, health disparities, and ability to develop antimicrobial resistance
Increase understanding of gonorrhea control strategies
Increase knowledge of gonorrhea control activities conducted in the region
Develop action plans for targeted, and more robust GC control efforts

Gonorrhea Control: Gonorrhea Control:
A Historical A Historical PerspectivePerspective
Kevin O’ConnorKevin O’ConnorDSTDPDSTDP
January 14, 2010January 14, 2010

Epidemiology 101

Why talk about GONORRHEA
now?

Why now?Why now?• GC in the west
• Loss of fluoroquinolones (and GC’s ability to develop antimicrobial resistance)
• Health disparities• ID populations at risk for other STDs and conditions
• Opportunities:• reaching those at-risk for GC also addresses CT• learn from our historic successes• success might not be that far away

* Not Anymore
*

After Cephalosporins: What Next?
Penicillin (in increasing doses) gone Tetracyclines gone Spectinomycin gone Fluoroquinolones gone
Oral cephalosporins going?
Injectable cephalosporins (Ceftriaxone)

This is the second MMWR in the past month that addresses gonorrhea... It is important we use this heightened awareness to reconsider what we are doing to prevent gonorrhea transmission and its sequelae and to begin new discussions about improving gonorrhea prevention. We will continue to keep you updated on developments as they occur and will work with you to address the growing urgency of this serious health concern.
John M. Douglas, Jr., MD Director, Division of STD Prevention National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention
April 12, 2007 DCL announcing that fluoroquinolones are no longer recommended for the treatment of GC; shortly after ‘GC in the West’ MMWR article

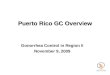
Gonorrhea rates, U.S., 1941-2007
Rate (per 100,000 population)
Gonorrhea2010 Target
0
100
200
300
400
500
1941 46 51 56 61 66 71 76 81 86 91 96 2001 06

Gonorrhea rates, U.S., 1941-2007
Rate (per 100,000 population)
Gonorrhea2010 Target
0
100
200
300
400
500
1941 46 51 56 61 66 71 76 81 86 91 96 2001 06
GC Control Program

Rate (per 100,000 population)
Gonorrhea
2010 Objective 0
100
200
300
400
500
1970 73 76 79 82 85 88 91 94 97 2000
Note: The Healthy People 2010 (HP2010) objective for gonorrhea is 19.0 cases per 100,000 population
Gonorrhea Control Milestones
Gonorrhea Control Program
GC Culture DNA probe
GISP IPP
PCR
D/C TetracyclineD/C PCN
D/C Fluroquinolones in HI, PI, Asia

National Gonorrhea Control Program
Implemented in 1972 Federal funding to state and local agencies Establish screening programs for the
detection of gonorrhea in asymptomatic women
Screening facilities included public and private agencies
Partner services

Gilbert Gonorrhea - 1973

Female Screening VD clinicScreening/testing 4,356,670 582,922GC + 132,387 (3%) 109,889 (19%)
Partner Services 3 mos. Annual est.Interviews 64,154 ~259,000 (3 mos. only: April – June 1973)Contacts 61,439 ( 0.96 CI )Ct. examined 39,409 (~2/3)
Infected/treated 15,928 (.40) ~64,000Epi Rx 18,063
National Gonorrhea Control Program1973

Historic GC Control of Program
1973STD Clinic
842,000Cases reported in 1973
Targeted Screening
Partner Services109,000
females~ 13 % 64,000
~ 7 %110,000females~ 13%

Case Finding Sources and their Contribution to Overall
MorbiditySTD Clinic Private
Providers
TotalReported Cases
Targeted Screening
Partner Services
ER JDC

Your Jurisdiction:Where/how are cases
identified?STD Clinic Private
Providers
TotalAnnual
Morbidity
Targeted Screening
Partner Services
ER
Jail

GONORRHEAin
PITTSBURGH


Allegheny CountyGonorrhea
Gc control strengths: 5-day full service STD clinic w/ 6 DIS Low syphilis morbidity Males come to you & receive prompt dx/Rx Straightforward, quick interviews Named contacts very likely to be infected Existing female screening program Existing partnerships: community & providers
CT: No dx while in the clinic: PS more labor-
intensive Contacts not likely to test positive

Allegheny CountyGonorrhea
Gonorrhea control plan: Interview Gc+ males in the clinic Traditional contact tracing of partners Regularly audit GC screening sites; redirect
screening as needed Build on local partnerships
Hospitals, screening sites, JDC, community clinics, school-based clinics, MCH, healthy start
Annual STD update meeting & report, letters to GSP sites, medical bulletin

O = Other (Previous Rx) A = Epi treat C = Infected, brought to treatment

Allegheny County 1993 1994 2000# Total Cases 3,730 2,602 1,510# F Cases 1,847 1,335 827
GC Screening Program# F Tests 70,000+ 60,000+ 38,672# F Tests + 1,229 (66%) 856 (64%) 347
(42%)PS# Female cases ID’d by PS (partners brought to treat)
359 (20%) 235 (18%) ??

Allegheny CountyGonorrhea
Annual STD Progress Report (1993)
The decline in Gc is likely the result of several factors:
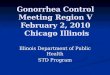
66% female GC cases identified by Gc Screening Program (1,229 of 1847)
1,050 STD clinic males interviewed, and…
359 female sex partners are infected, ‘brought to treatment’ 20% of reported female cases ( N = 1,847) 20% of female cases ‘brought’ every year after 1990

Female GC Case Finding in Allegheny County, 1993
1847Female
GC Cases
GC ScreeningProgram1,229
Partner Services
359
20%66%

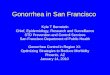
Gonorrhea Morbidity Allegheny County, PA 1990-
2002
0500100015002000250030003500400045005000
1990 1992 1994 1996 1998 2000 2002
New PS strategy; ongoing screening
Focused PS effort ends
Screening reduced

END