Embed Size (px)
Citation preview
Welcome!Welcome!
The QPR Suicide Triage The QPR Suicide Triage Training ProgramTraining Program
Instructor: Instructor:
QPR Suicide Triage Training QPR Suicide Triage Training AgendaAgenda
IntroductionsIntroductionsScope of the problem Scope of the problem Introduction to risk factorsIntroduction to risk factorsMental illness and suicideMental illness and suicideSuicide Risk Rating ExerciseSuicide Risk Rating ExerciseLunchLunchIntroduction to the QPR Triage protocolIntroduction to the QPR Triage protocolRole plays and practiceRole plays and practice
Source of the QPR Suicide Source of the QPR Suicide Triage Training ProgramTriage Training Program
TThe QPR Suicide triage training program is derived from he QPR Suicide triage training program is derived from the QPRT Suicide Risk Management Inventory and the QPRT Suicide Risk Management Inventory and training program used by thousands of healthcare training program used by thousands of healthcare professionals.professionals.
The foundation materials are identical and at the end of The foundation materials are identical and at the end of training you will know about suicide than most healthcare training you will know about suicide than most healthcare professionals.professionals.
Note: where you see or hear the word “patient” remember that the person Note: where you see or hear the word “patient” remember that the person you are trying to help out of a crisis may, or may not be, your patient.you are trying to help out of a crisis may, or may not be, your patient.
Training goalsTraining goals
Describe the scope of the problemDescribe the scope of the problemAddress social policy/impact on practiceAddress social policy/impact on practiceRelationship of mental illness and Relationship of mental illness and substance abuse to suicidesubstance abuse to suicideCurrent status of suicide risk assessmentCurrent status of suicide risk assessmentLearn how to determine immediate risk of Learn how to determine immediate risk of suicide and what safety measures can be suicide and what safety measures can be taken to reduce risktaken to reduce risk
General approach for today…General approach for today…
Emphasis is knowledge gain and skill Emphasis is knowledge gain and skill acquisition verses interesting statisticsacquisition verses interesting statistics
Teach a tested suicide risk assessment Teach a tested suicide risk assessment documentation protocol documentation protocol
Address strategies for immediate suicide Address strategies for immediate suicide risk reduction risk reduction
From the Surgeon GeneralFrom the Surgeon General
““Suicide is our most preventable Suicide is our most preventable form of death.”form of death.”
Why now?Why now?
National movement has begun…National movement has begun…
National Strategy for Suicide Prevention National Strategy for Suicide Prevention
Public health is marketing “suicide is Public health is marketing “suicide is preventable”preventable”
Public expectations that suicide is a Public expectations that suicide is a preventable form of death are risingpreventable form of death are rising
How big is the problem?How big is the problem?Global Violence-Related DeathsGlobal Violence-Related Deaths1 million people die by suicide1 million people die by suicide10-20 million attempt10-20 million attemptLeading cause of death in 1/3 of all Leading cause of death in 1/3 of all countriescountries54% of all violence-related deaths54% of all violence-related deathsGlobal rates are climbing, esp. menGlobal rates are climbing, esp. men
More die by suicide each year than from all More die by suicide each year than from all armed conflicts around the worldarmed conflicts around the world
American NumbersAmerican Numbers(averaged over past 10 years)(averaged over past 10 years)
31,000 + die each year (39,000 in 2010)31,000 + die each year (39,000 in 2010)Rate: 12 -15 per 100,000/YearRate: 12 -15 per 100,000/Year105+ per day now (1 commercial jet per day)105+ per day now (1 commercial jet per day)One person every 15-20 minutesOne person every 15-20 minutesOf these deathsOf these deaths- 4 X male completions to female4 X male completions to female- 3 X females to male attempts3 X females to male attempts
Suicide is no respecter of age, race, religion, Suicide is no respecter of age, race, religion, social or economic status; its an equal social or economic status; its an equal opportunity mode of death.opportunity mode of death.
Scope of the problem USAScope of the problem USA
Range: ideations, attempts, deaths Range: ideations, attempts, deaths 31,483 completed suicides in US (2003)31,483 completed suicides in US (2003)US suicide rates are trending down, not risingUS suicide rates are trending down, not risingExceptions: AI/NA youth are risingExceptions: AI/NA youth are risingRates vary widely by race, gender, Rates vary widely by race, gender, geography, ethnicity, but all deaths have geography, ethnicity, but all deaths have commonalitiescommonalities
Am. Journal of Public Health, McKeown, 2006Am. Journal of Public Health, McKeown, 2006
Big picture adult numbersBig picture adult numbers
Think, plan, attempt, dieThink, plan, attempt, die10 million adults think about suicide each year 10 million adults think about suicide each year 1.2 million plan a method (gun, MVA, etc)1.2 million plan a method (gun, MVA, etc)750,000 attempt (minimum count).750,000 attempt (minimum count).Approximately 30,000 dieApproximately 30,000 dieSuicide is 11Suicide is 11thth cause of death overall cause of death overall- 3- 3rdrd for young people (rate has almost tripled for young people (rate has almost tripled since 1950s – unexpected upturn 2003-2004.since 1950s – unexpected upturn 2003-2004.- first for young people in some states- first for young people in some statessource: National Co morbidity study, CDC and NIMHsource: National Co morbidity study, CDC and NIMH
American NumbersAmerican Numbers(averaged over past 10 years)(averaged over past 10 years)
31,000 + die each year31,000 + die each yearRate: 11-12 per 100,000/YearRate: 11-12 per 100,000/Year80+ per day (1 commercial jet every other day)80+ per day (1 commercial jet every other day)One person every 15-20 minutesOne person every 15-20 minutesOf the 31,000 deathsOf the 31,000 deaths- 4 X male completions to female4 X male completions to female- 3 X females to male attempts3 X females to male attempts
Suicide is no respecter of age, race, religion, Suicide is no respecter of age, race, religion, social or economic status; its an equal social or economic status; its an equal opportunity mode of death.opportunity mode of death.
States with highest rates for past States with highest rates for past decade (not ordered)decade (not ordered)
The following states have completed suicide The following states have completed suicide rates above 15/100,000rates above 15/100,000
Nevada - New Mexico – Montana – Nevada - New Mexico – Montana – Wyoming – Colorado – Alaska – Idaho Wyoming – Colorado – Alaska – Idaho
What do these states have in common?What do these states have in common?
States with the lowest rates for the States with the lowest rates for the past decadepast decade
The following states (and DC) have completed The following states (and DC) have completed suicide rates below 9/100,000suicide rates below 9/100,000
Rhode Island - California - Connecticut - Rhode Island - California - Connecticut - District of Columbia - New Jersey – District of Columbia - New Jersey – Massachusetts - New York Massachusetts - New York
What do these states have in What do these states have in common?common?
Would access to care save lives?Would access to care save lives?
• Over 90% of all people who die by suicide are suffering from Over 90% of all people who die by suicide are suffering from a major psychiatric illness or substance abuse disorder, or a major psychiatric illness or substance abuse disorder, or both.both.
• More teenagers and young adults die from suicide than from More teenagers and young adults die from suicide than from cancer, heart disease, AIDS, birth defects, stroke, cancer, heart disease, AIDS, birth defects, stroke, pneumonia and influenza, and chronic lung disease, pneumonia and influenza, and chronic lung disease, COMBINED.COMBINED.
• Effective, accessible, competent care could save thousands Effective, accessible, competent care could save thousands of lives.of lives.
Intention and SuicideIntention and Suicide
““There are ways of killing yourself without killing There are ways of killing yourself without killing yourself.”yourself.”
Tony Manero, Tony Manero, Saturday Night FeverSaturday Night Fever,, on the “suicide” of his friend.on the “suicide” of his friend.
ILTB = Intentional life threatening behaviorILTB = Intentional life threatening behavior
Need for surveillance dataNeed for surveillance data
We really do not know the full scope of suicidal We really do not know the full scope of suicidal behaviors, self-inflicted injuries, risk-taking behaviors, self-inflicted injuries, risk-taking activities that lead to premature morbidity and activities that lead to premature morbidity and mortality.mortality.New! National Violent Death Surveillance New! National Violent Death Surveillance System is now in place in 17 states and is System is now in place in 17 states and is collecting critical data on 50,000 violent deaths collecting critical data on 50,000 violent deaths per year, including suicide.per year, including suicide.
We do know where those identified end up…. In We do know where those identified end up…. In our care and we must do the best we can to our care and we must do the best we can to keep them safe.keep them safe.
Suicide AttemptSuicide Attempt
““Any potentially self-injurious action, with a Any potentially self-injurious action, with a nonfatal outcome, for which there is nonfatal outcome, for which there is evidence, either explicit or implicit, that the evidence, either explicit or implicit, that the individual intended to kill himself or individual intended to kill himself or herself.”herself.”
From Carol, Berman, Maris, et. Al., From Carol, Berman, Maris, et. Al., Journal of Suicide and Life-Threatening Journal of Suicide and Life-Threatening Behavior, 1996Behavior, 1996
Lethality of Suicide AttemptsLethality of Suicide Attempts
Suicide attempts vary in lethality. Death can be an impossible result of Suicide attempts vary in lethality. Death can be an impossible result of
some action, or almost a certaintysome action, or almost a certainty..
Smith et. al., The Menninger Foundation, scales Smith et. al., The Menninger Foundation, scales from 1 to 10 (good inter rater reliability). from 1 to 10 (good inter rater reliability). Examples:Examples:
0.0 Death is an impossible result of “suicidal 0.0 Death is an impossible result of “suicidal behavior,” e.g., light scratches to the skin behavior,” e.g., light scratches to the skin Wounds that do not require suturing. Swallowing Wounds that do not require suturing. Swallowing paper clips, coins, 10 or fewer aspirins or clearly paper clips, coins, 10 or fewer aspirins or clearly ineffective acts which are shown to others.ineffective acts which are shown to others.
Lethality of Attempt ScaleLethality of Attempt Scale3.5 Death is improbable so long as first aid is 3.5 Death is improbable so long as first aid is administered by victim or other agent. No effort to administered by victim or other agent. No effort to hide attempt. Rescue is likely.hide attempt. Rescue is likely.5.0 Death is a 50-50 probability directly or indirectly. 5.0 Death is a 50-50 probability directly or indirectly. Severe cutting with sizable blood loss. Hanging Severe cutting with sizable blood loss. Hanging efforts with chance of discovery high. Vague drug efforts with chance of discovery high. Vague drug overdose.overdose.7.0 Death is the probable outcome unless there is 7.0 Death is the probable outcome unless there is immediate and vigorous first aid or medical attention. immediate and vigorous first aid or medical attention. Large doses drugs with fifth of whisky and suicide Large doses drugs with fifth of whisky and suicide note. Hanging attempt, with patient found cyanotic.note. Hanging attempt, with patient found cyanotic.10.0 Death almost certain. Use of shotgun. Drowning 10.0 Death almost certain. Use of shotgun. Drowning self at midnight in a lake. Survival is accidental.self at midnight in a lake. Survival is accidental.
Suicide AttemptsSuicide Attempts
Most don’t die in their attemptMost don’t die in their attemptYouth: 100 -200 attempts per 1 completionYouth: 100 -200 attempts per 1 completionElder: 4 attempts per 1 completionElder: 4 attempts per 1 completionAverage: 25 attempts per 1 completionAverage: 25 attempts per 1 completion5 million Americans have attempted (est.)5 million Americans have attempted (est.)Reporting problem Reporting problem - under reporting- under reporting- unknown (don’t ask, don’t tell)- unknown (don’t ask, don’t tell)
Suicide and HomicideSuicide and Homicide
More homicides or suicides More homicides or suicides per year in the US?per year in the US?
Is there any overlap between Is there any overlap between homicide and suicide?homicide and suicide?
Facts you Need to KnowFacts you Need to Know
If a man calls, take him seriously, he may have a If a man calls, take him seriously, he may have a gun in his hand..gun in his hand..
Boys, teenaged boys, young men 18-25Boys, teenaged boys, young men 18-25Highest tally of total death: men in middle yearsHighest tally of total death: men in middle yearsOld white males are the highest risk groupOld white males are the highest risk group- 79% use a firearm (lethal planners)- 79% use a firearm (lethal planners)- They know how to do it and plan carefullyThey know how to do it and plan carefully- They avoid rescueThey avoid rescue
““If a woman calls about a man, take her even more If a woman calls about a man, take her even more seriously.”seriously.”
Our Older VeteransOur Older Veterans
70% of older males are vets70% of older males are vets
Vet status adds suicide risk independent Vet status adds suicide risk independent of any other problemof any other problem
Of all psych problems, depression is self- Of all psych problems, depression is self- or other reported in 50% of the suicides at or other reported in 50% of the suicides at time of deathtime of death
Of these, only 22% were in care, 78% Of these, only 22% were in care, 78% were not - ID and Rx MDD = saved lives!were not - ID and Rx MDD = saved lives!
Cold Sober SuicideCold Sober Suicide
Where alcohol and other drugs on board Where alcohol and other drugs on board contribute to greatly to suicide risk in contribute to greatly to suicide risk in younger people, among men over 65 only younger people, among men over 65 only 9% had a BAC greater than .89% had a BAC greater than .8
Source:Source: National Violent Death Surveillance SystemNational Violent Death Surveillance System
Annie get your gun…Annie get your gun…
In late life a firearm is the #1 method used In late life a firearm is the #1 method used by women….36% of all suicides, OD by women….36% of all suicides, OD second.second.
Now imagine a trend line into the future for Now imagine a trend line into the future for our women warriors…. our women warriors….
Facts you need to know…Facts you need to know…
Suicide risk rises with age for white males, not Suicide risk rises with age for white males, not for men of colorfor men of colorResponsibility for one or more children is a Responsibility for one or more children is a powerful protective factor against suicide in powerful protective factor against suicide in women (Sweden)women (Sweden)Contact with a healthcare provider does not Contact with a healthcare provider does not confer protection…. and neither does recent confer protection…. and neither does recent psychiatric hospitalization.psychiatric hospitalization.Most suicides occur with weeks to months of last Most suicides occur with weeks to months of last contact AND risk rises after discharge!contact AND risk rises after discharge!
Suicide PreventionSuicide Prevention is is Violence Violence PreventionPrevention
DOMESTIC VIOLENCE, SUICIDE AND HOMICIDEDOMESTIC VIOLENCE, SUICIDE AND HOMICIDE
* DV victims make more suicide attempts (20 to * DV victims make more suicide attempts (20 to 26%).26%).
* Violent families contribute to youth suicide. * Violent families contribute to youth suicide. * Violent people have a history of self-destructive * Violent people have a history of self-destructive
behavior (30%).behavior (30%).* Double suicides are often motivated by the * Double suicides are often motivated by the
couples fear of separation and the fantasy that couples fear of separation and the fantasy that they can remain together in death.they can remain together in death.
* Abusive men who kill their wives and lovers * Abusive men who kill their wives and lovers usually do so in response to the woman’s usually do so in response to the woman’s attempt to leave.attempt to leave.
Intimate Partner ViolenceIntimate Partner Violence• Males who threaten suicide in an intimate partner Males who threaten suicide in an intimate partner
violence situation are at greater risk for murder-suicide.violence situation are at greater risk for murder-suicide.
WSDVFR finding: WSDVFR finding: ““Abusers were suicidal in 35% of Abusers were suicidal in 35% of domestic violence fatalities overall (this includes cases domestic violence fatalities overall (this includes cases where no homicide occurred), and in 31% of the cases in where no homicide occurred), and in 31% of the cases in which a homicide was committed.which a homicide was committed.””
US AIR FORCE: US AIR FORCE: • Suicide rate down 33%,Suicide rate down 33%,• Homicide rate down 52%Homicide rate down 52%• Serious DV rate down 54%Serious DV rate down 54%
Suicide Prevention IS violence prevention! Suicide Prevention IS violence prevention!
Survivors of SuicideSurvivors of Suicide
6 blood relatives directly affected by each suicide6 blood relatives directly affected by each suicide1 of every 62 of us is a survivor1 of every 62 of us is a survivorThis number does not include colleagues, co-workers, This number does not include colleagues, co-workers, friends, team or school mates and ex spousesfriends, team or school mates and ex spousesOne suicide every 18 minutes = 6 new survivors One suicide every 18 minutes = 6 new survivors Suicide risk is greater in survivors (e.g., 4-fold increase Suicide risk is greater in survivors (e.g., 4-fold increase in children when a parent dies by suicide)in children when a parent dies by suicide)If 30,000+ Americans die by suicide each year leaving If 30,000+ Americans die by suicide each year leaving 180,000 blood relative survivors, how many have died by 180,000 blood relative survivors, how many have died by suicide since 9/11, and how many new survivors are suicide since 9/11, and how many new survivors are there?there?
GOOD NEWS!GOOD NEWS!
Research, medicine and political will are buildingResearch, medicine and political will are buildingStigma, funding, and lack of awareness remainStigma, funding, and lack of awareness remainLeadership has emerged: NIMH, CDC, National Leadership has emerged: NIMH, CDC, National Council for Suicide PreventionCouncil for Suicide PreventionU.S. Air Force success story is outU.S. Air Force success story is outThe majority of Americans believe we should The majority of Americans believe we should fund more research and believe many suicides fund more research and believe many suicides are preventable (SPANUSA research)are preventable (SPANUSA research)
End ModuleEnd Module
QuestionsQuestions
Suicide Risk and Risk Suicide Risk and Risk ManagementManagement
What you need to What you need to know….know….
Suicide Risk AssessmentSuicide Risk Assessment
Prediction is complex and difficultPrediction is complex and difficultPrognosis vs. predictionPrognosis vs. predictionChallenge of a low probability eventChallenge of a low probability eventBehavior is threshold sensitiveBehavior is threshold sensitiveBehavior is context sensitiveBehavior is context sensitiveBehavior relationship sensitiveBehavior relationship sensitiveSummation of risk factors not helpfulSummation of risk factors not helpfulScreening tools can get you in trouble Screening tools can get you in trouble
(prediction is best done in reverse)(prediction is best done in reverse)
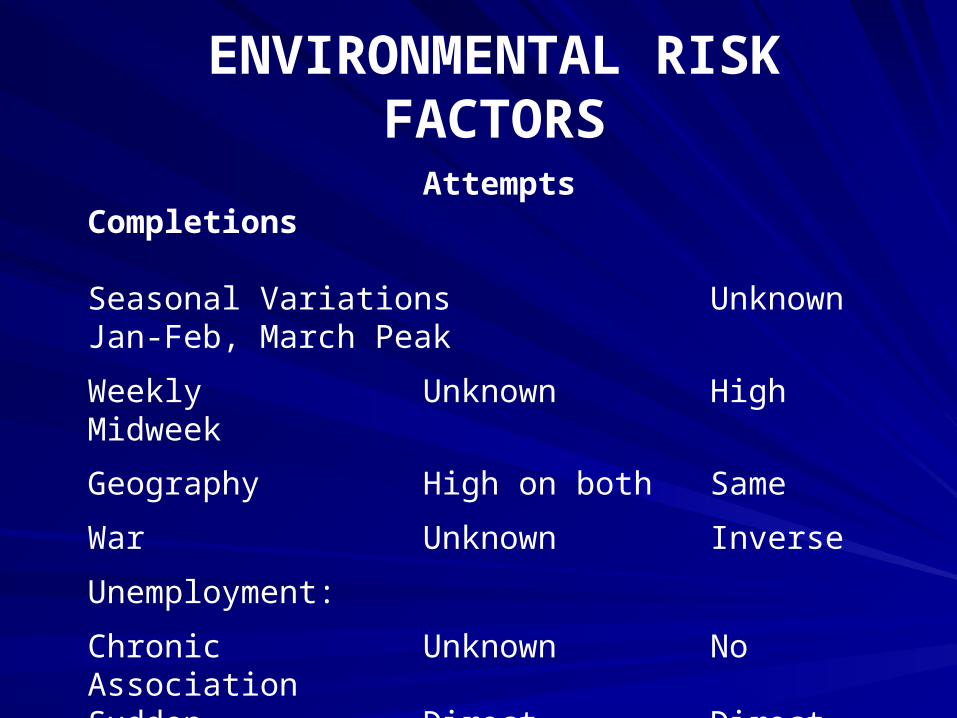
ENVIRONMENTAL RISK
FACTORSAttempts Completions
Seasonal Variations Unknown Jan-Feb, March Peak
Weekly Unknown High Midweek
Geography High on both Same
War Unknown Inverse
Unemployment:
Chronic Unknown No AssociationSudden Direct Direct
* Source: Harvard School of Public Health, 1998
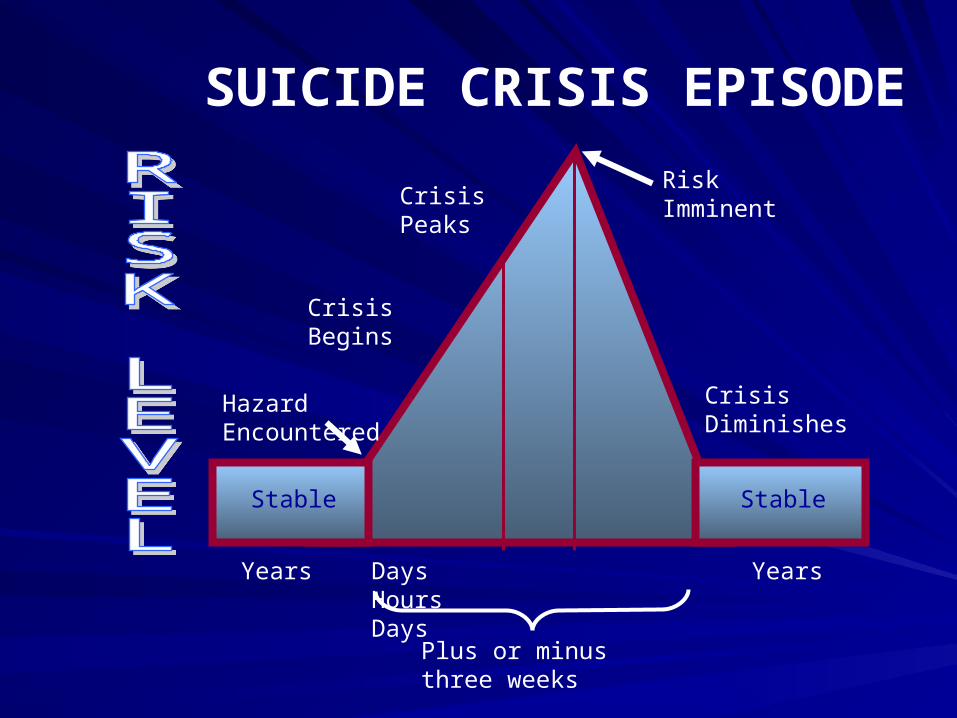
SUICIDE CRISIS EPISODE
Stable Stable
Days Hours Days
Years Years
Crisis Peaks
Crisis Begins
Hazard Encountered
Risk Imminent
Crisis Diminishes
Plus or minus three weeks
THE LETHAL TRIAD
UPSET PERSON
FIREARM ALCOHOL
When these three are present-the risk of violence is high.
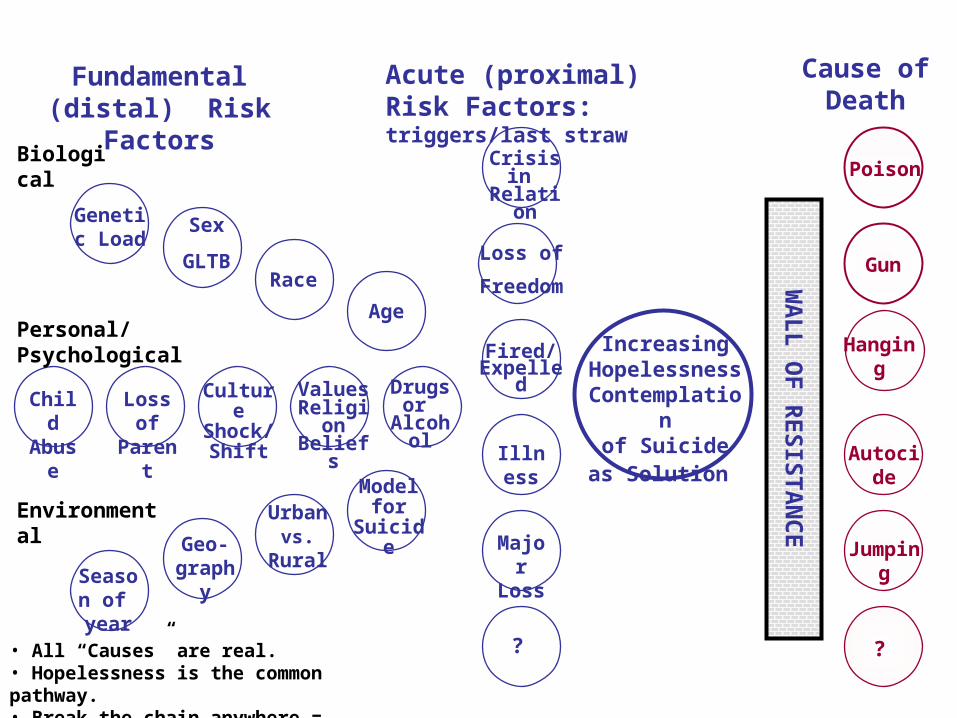
The Many Paths to SuicideFundamental (distal)
Risk FactorsAcute (proximal) Risk Factors: triggers/last straw
Cause of Death
Crisis in Relation
Loss of Freedom
Fired/ Expelled
Illness
Major Loss
?
Poison
Gun
Hanging
Autocide
Jumping
?
Increasing Hopelessness
Contemplationof Suicide
as Solution
WA
LL
OF
RE
SISTA
NC
E
Genetic Load
Sex
GLTBRace
Age
Drugs or
Alcohol
Biological
Child Abuse
Loss of Parent
Culture Shock/Shift
ValuesReligionBeliefs
Season of year
Geo-graphy
Model for
Suicide
Personal/Psychological
• All “Causes” are real.• Hopelessness is the common pathway.• Break the chain anywhere = prevention.
Environmental Urbanvs.
Rural
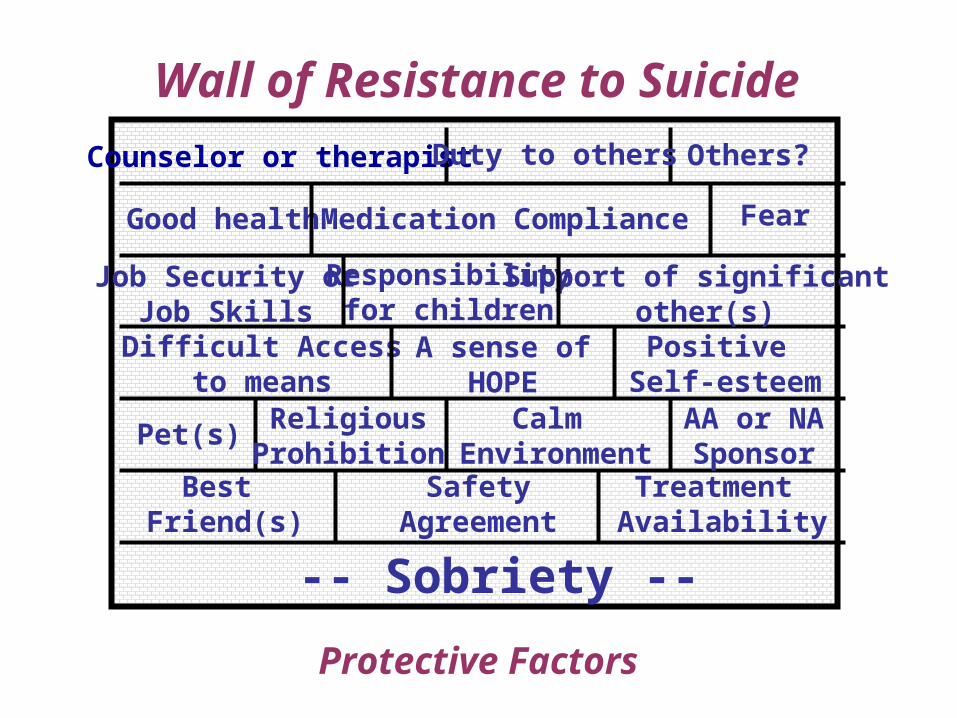
-- Sobriety --
Best Friend(s)
SafetyAgreement
Treatment Availability
Pet(s) Calm Environment
ReligiousProhibition
AA or NASponsor
Difficult Accessto means
A sense ofHOPE
Positive Self-esteem
Fear
Job Security orJob Skills
Support of significant other(s)
Counselor or therapist
Medication ComplianceGood health
Responsibilityfor children
Others?
Wall of Resistance to Suicide
Protective Factors
Duty to others
Nature of the suicideNature of the suicide
Psychic suffering (Psycheache)Psychic suffering (Psycheache)HopelessnessHopelessnessUnbearable mental anguishUnbearable mental anguishCognitive constrictionCognitive constrictionGrossly impaired problem solving abilityGrossly impaired problem solving abilityFeeling a burden to others Feeling a burden to others Thwarted belongingnessThwarted belongingnessAcquired capacity for self-injuryAcquired capacity for self-injury
BASIC CONCEPTS ABOUT SUICIDESuicide is always multi-determined.
Suicide prevention must involve multiple approaches.
Most suicidal people do not want to die.
Suicidal people want to find a way to live.
Ambivalence exists until the moment of death.
The final decision rests with the individual.
Reduce risk factors and you reduce risk.
Enhance protective factors and you reduce risk.
The Relationship of Mental The Relationship of Mental Illness and Substance Abuse to Illness and Substance Abuse to
Suicide…Suicide…
Preventing suicide is largely about Preventing suicide is largely about identifying and treating mood disorders, identifying and treating mood disorders, alcoholism and co-occurring disordersalcoholism and co-occurring disorders
WHO aims to target:WHO aims to target:- Mood disorders- Mood disorders- Schizophrenia- Schizophrenia- Alcoholism- Alcoholism
World evidence for treatment effectiveness World evidence for treatment effectiveness suggests suicide rates can be substantially suggests suicide rates can be substantially reduced in all these categories… if we can find reduced in all these categories… if we can find them before they diethem before they die
Is Suicide Primarily:Is Suicide Primarily: “Mental Health Territory?” “Mental Health Territory?”
Lifetime Suicide risk for Schizophrenic, Affective Lifetime Suicide risk for Schizophrenic, Affective and Addiction Disorders:and Addiction Disorders:
Method: review of 83 mortality studies:Method: review of 83 mortality studies:
– Schizophrenia…………4%Schizophrenia…………4%
– Affective Disorders……6%Affective Disorders……6%
– Addiction Disorders…...7%Addiction Disorders…...7%
Inskip HM: Br J Psych 1998Inskip HM: Br J Psych 1998
Epidemiology: Interesting but not Epidemiology: Interesting but not clinically useful…clinically useful…
Suicide rates vary across cultures, racial groups, age Suicide rates vary across cultures, racial groups, age groups, time and by geography. groups, time and by geography.
Major risk factors: Mental disorders, hopelessness, Major risk factors: Mental disorders, hopelessness, impulsive and/or aggressive tendencies, history of impulsive and/or aggressive tendencies, history of trauma or abuse, major physical illnesses, previous trauma or abuse, major physical illnesses, previous suicide attempt, family history of suicide, etc. (see NSSP suicide attempt, family history of suicide, etc. (see NSSP for complete lists of risk and protective factors)for complete lists of risk and protective factors)
What you need to know: 90-95% of all completed suicides What you need to know: 90-95% of all completed suicides have an Axis I disorder…BUT – most people with these have an Axis I disorder…BUT – most people with these illnesses DO NOT die by suicide. illnesses DO NOT die by suicide.
General Neurobiology of Suicide
Reduced serotonin function in suicide, especially in suicides of high lethality or with considerable planning
Depletion of essential neurotransmitters (including dopamine and serotonin) may be the common clinical pathway for suicidal thinking, feeling and behaviors
Genetic studies inconclusive to date
Familial patterns of suicide suggest biological factors may influence risk.
From Joseph Coyle, MD,Harvard Medical School, 1997
Specific neurobiological changes in Specific neurobiological changes in severe suicidal depressionsevere suicidal depression
Loss of gray matterLoss of gray matterImpaired prefrontal cortical response to Impaired prefrontal cortical response to serotonin releaseserotonin releaseDopamine deficitDopamine deficitSerotonin hypofunction in the PFC Serotonin hypofunction in the PFC correlates to higher suicidal intent and correlates to higher suicidal intent and planning and lethality of suicide attemptplanning and lethality of suicide attempt
MDD AND SUICIDE
Lifetime risk: 2- 6% (lifetime risk)98 % of completers are seriously depressed Most die while off medication.Adherence to meds is essential to safety.For severe, agitated and suicidal depressions, electroconvulsive therapy may be the best choice.
Family/patient education: MMD is a potentially fatal illness and death is a possible result of not following medical advise.
Benzodiazepines are often underutilized (more later)
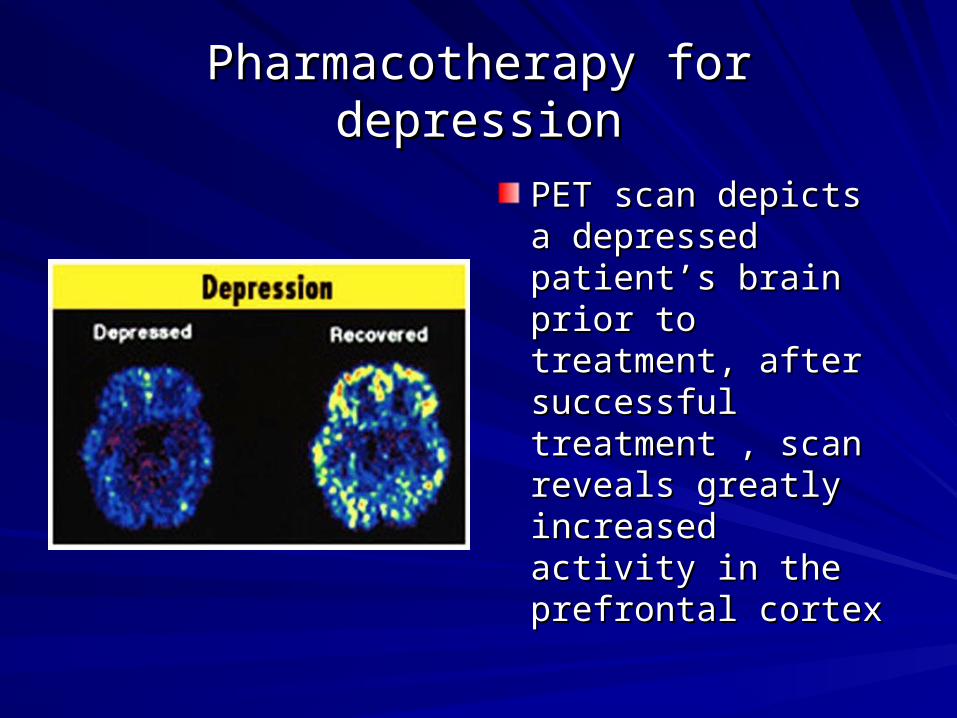
Pharmacotherapy for depressionPharmacotherapy for depression
PET scan depicts a PET scan depicts a depressed patient’s depressed patient’s brain prior to brain prior to treatment, after treatment, after successful treatment , successful treatment , scan reveals greatly scan reveals greatly increased activity in increased activity in the prefrontal cortexthe prefrontal cortex
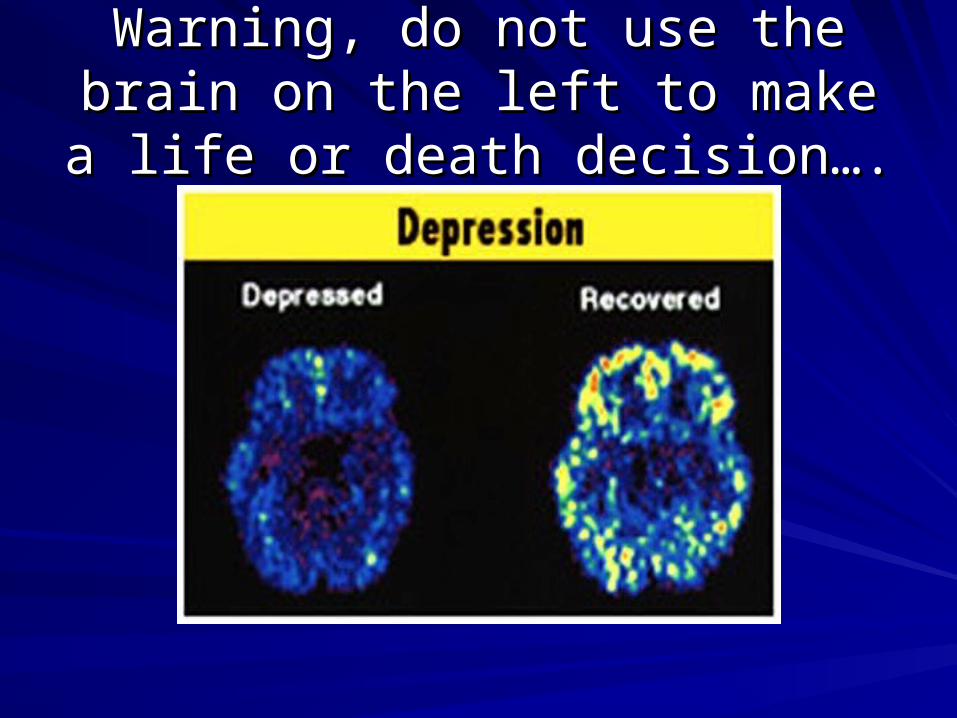
Warning, do not use the brain on Warning, do not use the brain on the left to make a life or death the left to make a life or death
decision….decision….
A note on antidepressantsA note on antidepressants
TCAs deadly in overdoseTCAs deadly in overdose
SSRI’s not deadly in overdoseSSRI’s not deadly in overdose
Lot’s of TCAs prescriptions = more suicidesLot’s of TCAs prescriptions = more suicides
Lot’s of SSRIs prescriptions = fewer suicidesLot’s of SSRIs prescriptions = fewer suicides
(EU, Australia, Scandinavia, USA)(EU, Australia, Scandinavia, USA)Sources:Sources:
Grunebaum, et al, J. Clin. Psychiatry, 2004Grunebaum, et al, J. Clin. Psychiatry, 2004
Gibbons, et al, Arch Gen Psychiatry, 2005Gibbons, et al, Arch Gen Psychiatry, 2005
Gibbons, et al, Am J. Psychiatry, 2006Gibbons, et al, Am J. Psychiatry, 2006
BIPOLAR DISORDER & SUICIDE
#1 cause of death, 1 to 2% per year.30 studies 9 to 46% x = 19%.Attempts
Major Depressive Disorder = 20%Bipolar Disorder = 25%-50%General Population = 1%
Highest risk windowsEarly in illnessIn denial phaseDuring mixed statesWhile experiencing depressive mania
K. R. Jamison, 1997John Hopkins University
11stst line intervention for suicidal line intervention for suicidal bi-polar patientsbi-polar patients
- Lithium appears to decrease aggression and impulsivity
- Psychotherapy and mood stabilizers prevent suicide better than mood stabilizers alone.
- Lithium has pronounced anti-suicide effect (600 fold impact)
Lithium works best for those who won’t take it; when they do take it, therapeutic impact is significant
SUICIDE AND SCHIZOPHRENIA- Ten to 15% complete suicide (best estimated
of Lifetime risk: 5%). Leading cause of death in patients under 35.
- Negative symptoms associated with increased risk.
- 20 to 40% make a suicide attempt.
- Finland National Study (1997) - 7% of all suicides met DSM-IV criteria for schizophrenia (N=92). Of these 92, 64 were also depressed.
- Suicides occur during active phases of the illness
M.T. Tsuang, MD,
Harvard Medical School, 1998
Suicide and SchizophreniaSuicide and Schizophrenia
Inadequate pharmacotherapy contributes to higher suicide rates for schizophrenics.
Major risk factors: young age, early stage of illness, substance abuse present, college education, multiple episodes of psychosis, living alone, history of previous attempt.
Improving on medications is the most dangerous time.
Suicides occur after discharge and in the first year of follow-up from index illness.
A note on ClozapineA note on Clozapine
Most effective for negative symptomsMost effective for negative symptomsBest for Rx resistant, has antidepressant and Best for Rx resistant, has antidepressant and mood stabilizing effectmood stabilizing effectClozapine reduced suicide events by 25% Clozapine reduced suicide events by 25% compared to olanzapinecompared to olanzapineClozapine 2 yr NNT of 13 to prevent 1 attemptClozapine 2 yr NNT of 13 to prevent 1 attempt
Source: Meltzer et. al. 2003/Health study research Source: Meltzer et. al. 2003/Health study research NEJM,1989.NEJM,1989.
Or is Suicide also:Or is Suicide also:Addictions Territory?Addictions Territory?
Alcohol strongest predictor of completed suicide over 5-Alcohol strongest predictor of completed suicide over 5-10 years after attempt, OR= 5.18…vs. demog or psych 10 years after attempt, OR= 5.18…vs. demog or psych disorders ( Beck J Stud Alc 1989)disorders ( Beck J Stud Alc 1989)
40-60% of completed suicides across USA/Europe are 40-60% of completed suicides across USA/Europe are alcohol/drug affected (state variable). Editorial: Dying for alcohol/drug affected (state variable). Editorial: Dying for a Drink: Brit Med J. 2001a Drink: Brit Med J. 2001
Higher suicide rates (+8%) in 18 vs. 21yo legal drinking Higher suicide rates (+8%) in 18 vs. 21yo legal drinking age states for those ages (Birckmayer J: Am J Pub age states for those ages (Birckmayer J: Am J Pub Health 1999)Health 1999)
Alcohol Abuse and Suicide
Major risk factors: male, long-term drinker, co-morbid psychiatric disorder.
Intoxication impairs judgment and increases impulsivity and aggressiveness
Co-morbidity increases risk
Highest risk group: MDD and alcoholism.
Alcoholism erodes protective factors: loss of job, health, home, money, family & friends
Alcohol myopia: inability to access the consequences of one’s actions (the stupid effect)
Sources: NIMH, Dying for a Drink, BMJ Oct 2001
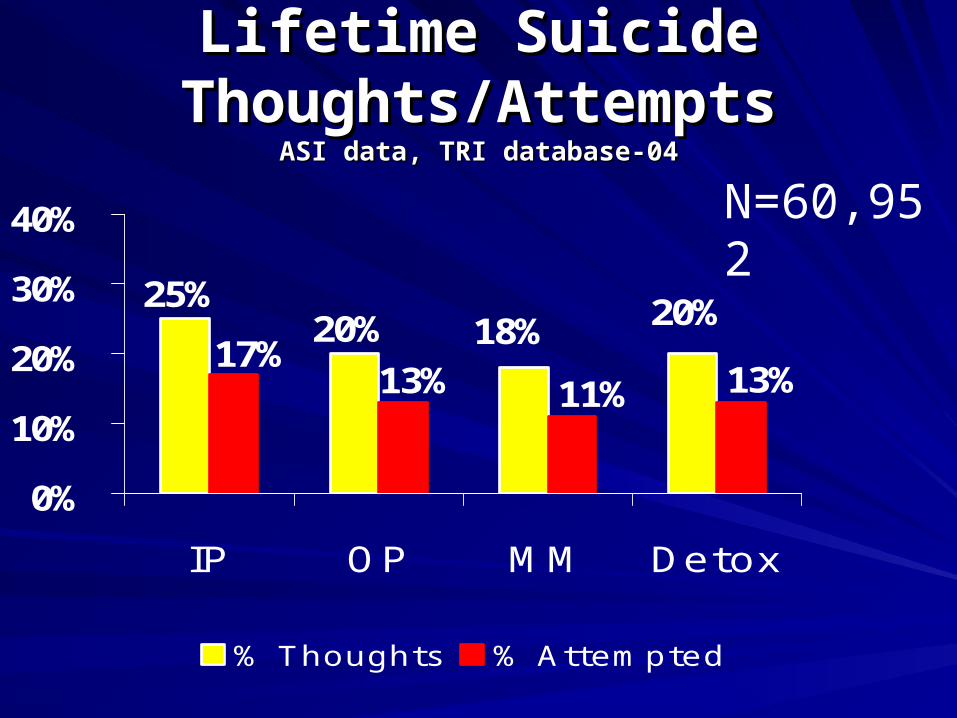
25%20% 18% 20%
17%13% 11% 13%
0%
10%
20%
30%
40%
IP OP MM Detox
% Thoughts % Attempted
Lifetime Suicide Lifetime Suicide Thoughts/AttemptsThoughts/Attempts
ASI data, TRI database-04ASI data, TRI database-04
N=60,952

Skip the booze and junkSkip the booze and junk
Copyright, 2004, CNS Productions, Inc.
28
Chronic Alcohol Abuse Heroin AbuseChronic Alcohol Abuse Heroin Abuse
Refer them all?Refer them all?
If you treat addictive disorders, do you If you treat addictive disorders, do you intend to refer every consumer who intend to refer every consumer who screens positive for suicide to mental screens positive for suicide to mental health?health?
If yes, are you prepared to send 25% of If yes, are you prepared to send 25% of your budget to mental health providers?your budget to mental health providers?
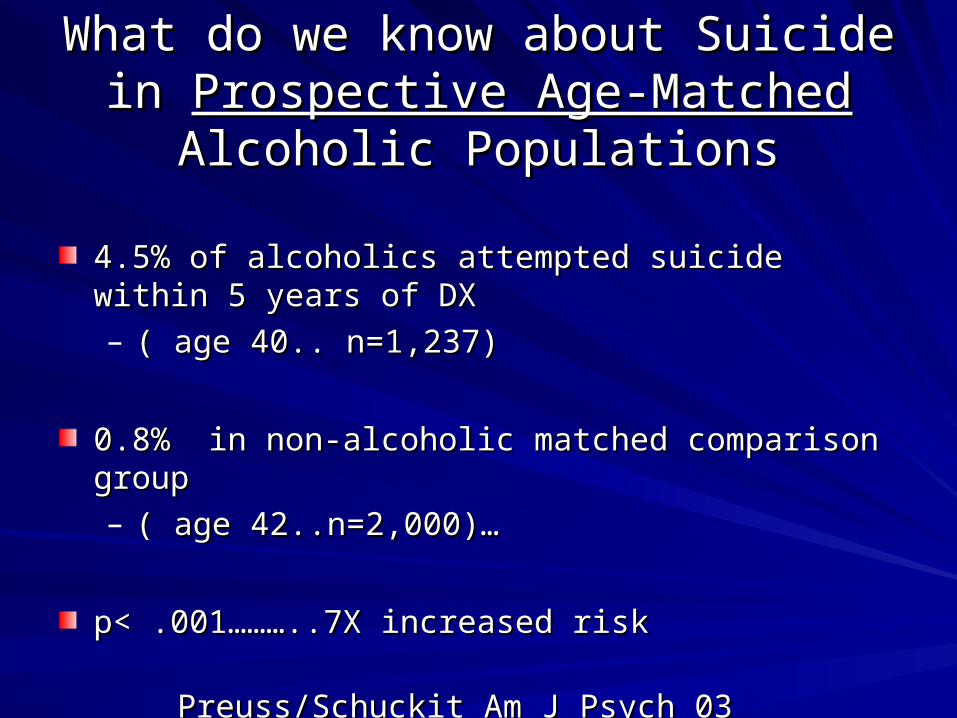
What do we know about Suicide in What do we know about Suicide in Prospective Age-MatchedProspective Age-Matched Alcoholic Alcoholic
PopulationsPopulations
4.5% of alcoholics attempted suicide within 5 years of DX 4.5% of alcoholics attempted suicide within 5 years of DX – ( age 40.. n=1,237)( age 40.. n=1,237)
0.8% in non-alcoholic matched comparison group 0.8% in non-alcoholic matched comparison group – ( age 42..n=2,000)…( age 42..n=2,000)…
p< .001………..7X increased riskp< .001………..7X increased risk
Preuss/Schuckit Am J Psych 03 Preuss/Schuckit Am J Psych 03

VITAL STATUS: Cumulative Survival after VITAL STATUS: Cumulative Survival after State Hosp Admission- State Hosp Admission- WA StateWA State
70%
80%
90%
100%
110%
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6
Mental Illness OnlyMental Illness, secondary drug/alcoholPrimary drug/alcohol, secondary major mental illnessPrimary drug/alcohol, secondary minor mental illnessDrug/alcohol only
Maynard & Cox, 2003
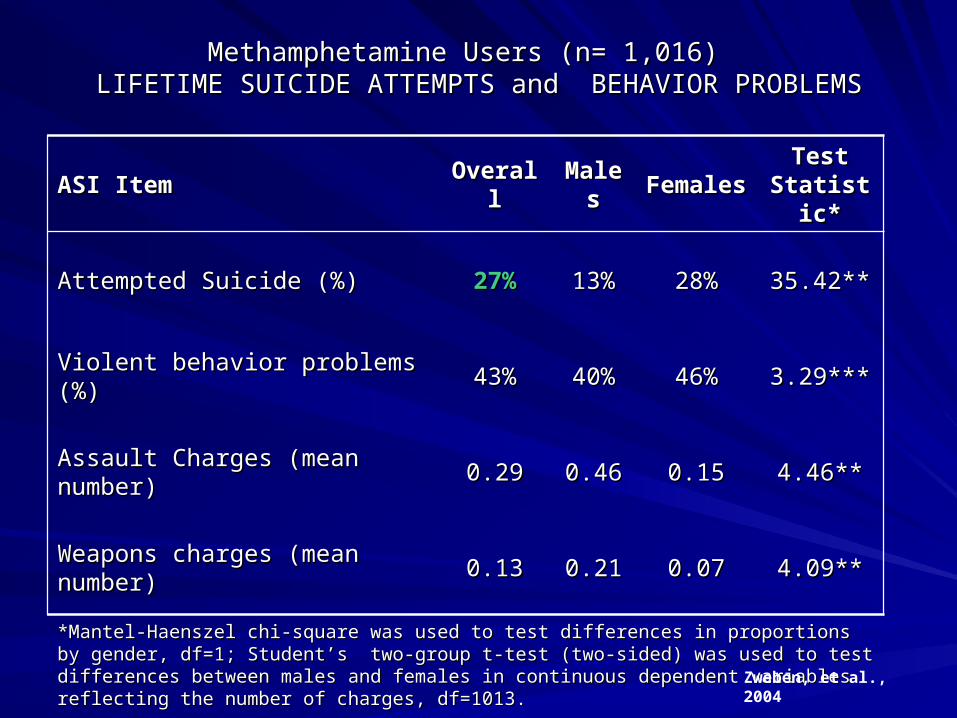
Methamphetamine Users (n= 1,016) Methamphetamine Users (n= 1,016) LIFETIME SUICIDE ATTEMPTS and BEHAVIOR PROBLEMSLIFETIME SUICIDE ATTEMPTS and BEHAVIOR PROBLEMS
ASI ItemASI Item OverallOverall MalesMales FemalesFemales Test Test Statistic*Statistic*
Attempted Suicide (%)Attempted Suicide (%) 27%27% 13%13% 28%28% 35.42**35.42**
Violent behavior problems (%)Violent behavior problems (%) 43%43% 40%40% 46%46% 3.29***3.29***
Assault Charges (mean number)Assault Charges (mean number) 0.290.29 0.460.46 0.150.15 4.46**4.46**
Weapons charges (mean number)Weapons charges (mean number) 0.130.13 0.210.21 0.070.07 4.09**4.09**
*Mantel-Haenszel chi-square was used to test differences in proportions by gender, df=1; *Mantel-Haenszel chi-square was used to test differences in proportions by gender, df=1; Student’s two-group t-test (two-sided) was used to test differences between males and females in Student’s two-group t-test (two-sided) was used to test differences between males and females in continuous dependent variables reflecting the number of charges, df=1013. continuous dependent variables reflecting the number of charges, df=1013.
**p < 0.00001 ***0.1 **p < 0.00001 ***0.1 << p <0.05 p <0.05 Zweben, et al., 2004
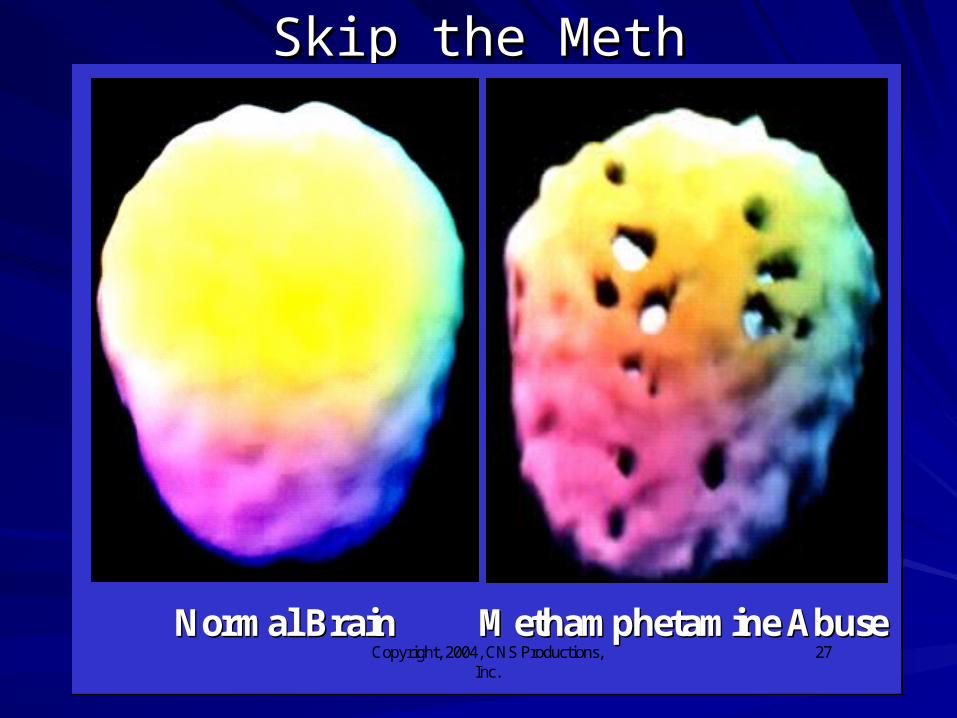
Skip the MethSkip the Meth
Copyright, 2004, CNS Productions, Inc.
27Normal BrainNormal Brain Methamphetamine AbuseMethamphetamine Abuse
Substance Induced Depression: Substance Induced Depression: Severity/DangerousnessSeverity/Dangerousness
Henriksson, et al (1993)-Henriksson, et al (1993)- 43% of completed suicides had 43% of completed suicides had alcohol dependence. 48% of these were also depressed. alcohol dependence. 48% of these were also depressed. 42% had a personality disorder.42% had a personality disorder.
Elliot, et al (1996)-Elliot, et al (1996)- patients with medically severe suicide patients with medically severe suicide attempts had a statistically higher prevalence or substance-attempts had a statistically higher prevalence or substance-induced mood disorder.induced mood disorder.
Pages K et al (1997)-Pages K et al (1997)- Higher degrees of Sub + Dep related Higher degrees of Sub + Dep related to higher severity suicide ratingsto higher severity suicide ratings
Traumatic brain injuryTraumatic brain injury
Blast is the most common wounding etiology our Blast is the most common wounding etiology our returning war fightersreturning war fighters50-60% of those exposed to blasts sustain a 50-60% of those exposed to blasts sustain a brain injury (Walter Reed Army Medical Center)brain injury (Walter Reed Army Medical Center)Depression, PTSD and alcohol use commonDepression, PTSD and alcohol use commonSimpson & Tate post-injury TBI community Simpson & Tate post-injury TBI community sample study (2002):sample study (2002):
- 23% had significant suicidal ideation - 23% had significant suicidal ideation - 18% made a suicide attempt- 18% made a suicide attempt
Life time risk of suicide 3-4 times higherLife time risk of suicide 3-4 times higher
PTSD and SuicidePTSD and Suicide
Research: Positive cResearch: Positive correlation between orrelation between PTSD and suicide PTSD and suicide
Some studies suggest that suicide risk is Some studies suggest that suicide risk is higher due to the symptoms of PTSD; higher due to the symptoms of PTSD; others claim risk is higher due related others claim risk is higher due related psychiatric conditions psychiatric conditions
Intrusive memories, high arousal & low Intrusive memories, high arousal & low avoidance increase risk of suicide ?avoidance increase risk of suicide ?
PTSDPTSD
Or, is it the co-occurring depression and/or Or, is it the co-occurring depression and/or alcohol use?alcohol use?Risk factors: male, alcohol abuse, older, Risk factors: male, alcohol abuse, older, family history of suicide, homeless, single, family history of suicide, homeless, single, with firearmwith firearmHighest risk: multiple combat wounds Highest risk: multiple combat wounds and/or hospitalized for injury + guilt over and/or hospitalized for injury + guilt over combat behaviorcombat behavior
Source: The Relationship Between PTSD and Suicide, Source: The Relationship Between PTSD and Suicide, William William Hudenko, Ph.D.Hudenko, Ph.D. VA – National Center for PTSD VA – National Center for PTSD
FIVE ACUTE SUICIDE RISK FACTORS
Severe psychic anxiety/turmoil
Incessant rumination
Global insomnia
Delusions of gloom and doom
Recent alcohol use (with or without alcoholism)
Jan Fawcett, M.D., 1997 (replicated in 2003 with 76 inpatient deaths)
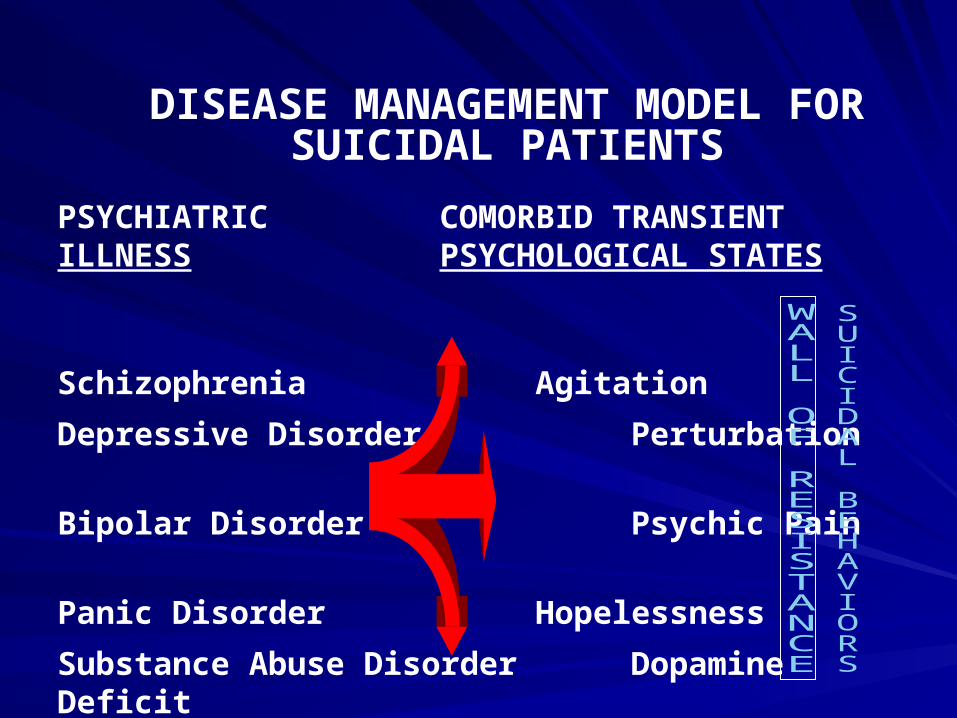
PSYCHIATRIC COMORBID TRANSIENT ILLNESS PSYCHOLOGICAL STATES
Schizophrenia Agitation
Depressive Disorder Perturbation
Bipolar Disorder Psychic Pain
Panic Disorder Hopelessness
Substance Abuse Disorder Dopamine Deficit
Personality Disorder Serotonin Deficit
Co-morbid Physical Illness Alcohol Myopia
DISEASE MANAGEMENT MODEL FOR SUICIDAL PATIENTS
Common Chemical Pathways for Common Chemical Pathways for Suicidal Acts?Suicidal Acts?
Alcohol in the bloodstreamAlcohol in the bloodstream
Low serotonin levelsLow serotonin levels
Impaired dopamine Impaired dopamine functionfunction
What can we do?What can we do?
Do we know how to sober people up?Do we know how to sober people up?Do we know how to treat anxiety?Do we know how to treat anxiety?Do we know how reduce psychic pain?Do we know how reduce psychic pain?Are there effective treatments for Are there effective treatments for agitation?agitation?Do we know what to do about serotonin Do we know what to do about serotonin deficits?deficits? CBT for depressive hopelessness?CBT for depressive hopelessness?DBT for Axis II consumersDBT for Axis II consumers
Good news! Treatment worksGood news! Treatment works
Cognitive therapy reduces youth suicide Cognitive therapy reduces youth suicide attempts by 50% (Brown, et al, Aug 3, attempts by 50% (Brown, et al, Aug 3, 2005 2005 JAMA)JAMA). . Youth Suicide Rates Lower in Counties Youth Suicide Rates Lower in Counties with High SSRI Use (Gibbons, et al, with High SSRI Use (Gibbons, et al, Am. J. Am. J. PsychiatryPsychiatry 2006) 2006)Several therapies are being adapted Several therapies are being adapted specifically for suicidal patients.. MI, CBT, specifically for suicidal patients.. MI, CBT, IMPACT and Problem Solving TherapyIMPACT and Problem Solving Therapy
Limitations: 18-month follow up and correlational data onlyLimitations: 18-month follow up and correlational data only
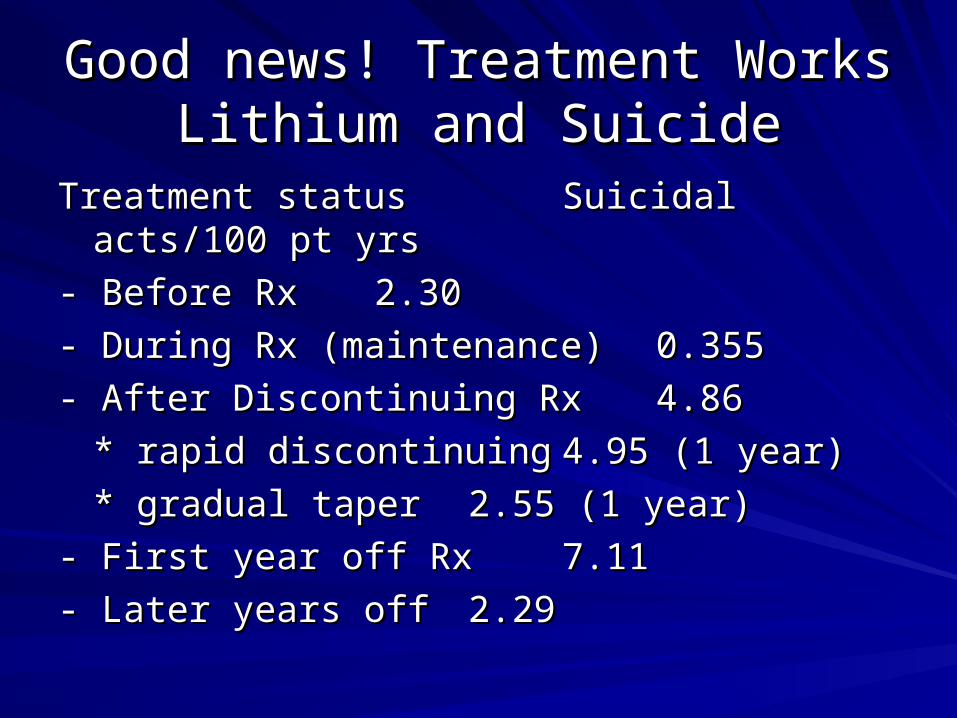
Good news! Treatment Works Good news! Treatment Works Lithium and SuicideLithium and Suicide
Treatment status Treatment status Suicidal acts/100 pt yrsSuicidal acts/100 pt yrs
- Before Rx- Before Rx 2.302.30
- During Rx (maintenance)- During Rx (maintenance) 0.3550.355
- After Discontinuing Rx- After Discontinuing Rx 4.864.86
* rapid discontinuing* rapid discontinuing 4.95 (1 year)4.95 (1 year)
* gradual taper* gradual taper 2.55 (1 year)2.55 (1 year)
- First year off Rx- First year off Rx 7.117.11
- Later years off - Later years off 2.292.29
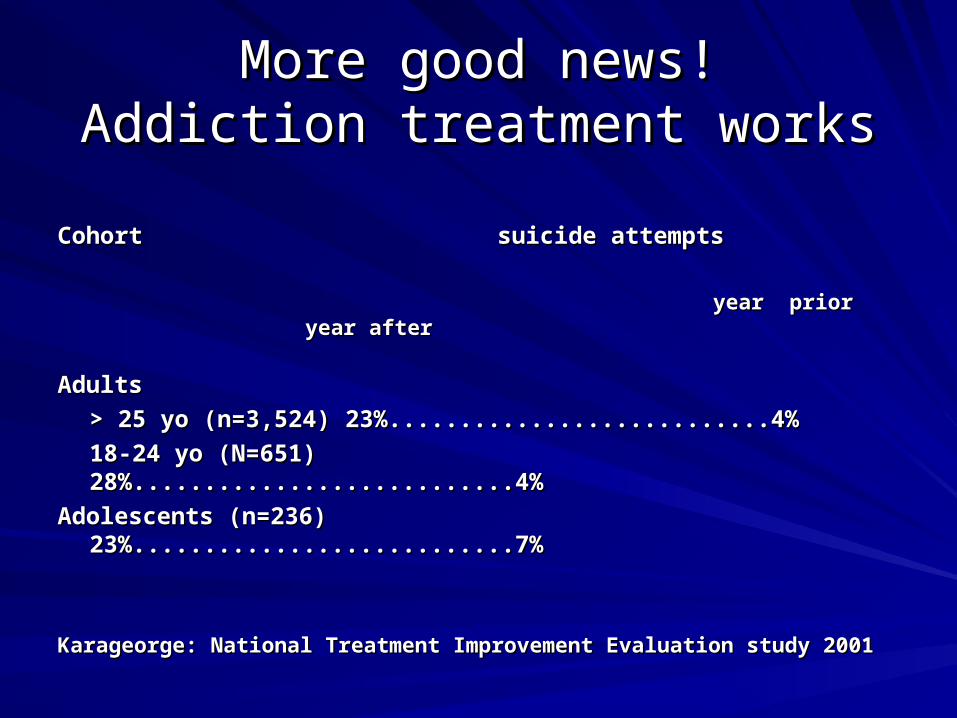
More good news!More good news!Addiction treatment worksAddiction treatment works
Cohort suicide attemptsCohort suicide attempts
year prior year afteryear prior year after
Adults Adults
> 25 yo (n=3,524)> 25 yo (n=3,524) 23%...........................4%23%...........................4%
18-24 yo (N=651) 28%...........................4% 18-24 yo (N=651) 28%...........................4%
Adolescents (n=236) 23%...........................7% Adolescents (n=236) 23%...........................7%
Karageorge: National Treatment Improvement Evaluation study 2001 Karageorge: National Treatment Improvement Evaluation study 2001
Take home messages….Take home messages….
Most dangerous diagnosis: alcoholism and Most dangerous diagnosis: alcoholism and major depressive disorder… Am. Journal of major depressive disorder… Am. Journal of Psychiatry, 1998.Psychiatry, 1998.
3 Common clinical pathways: serotonin deficit, 3 Common clinical pathways: serotonin deficit, dopamine deficit, and alcohol in blood streamdopamine deficit, and alcohol in blood stream
Co-occurring disorders kill Co-occurring disorders kill
There is no safety without sobriety…There is no safety without sobriety…
Treatment works!Treatment works!
DiscussionDiscussion
Questions?Questions?
Risk Rating ExerciseRisk Rating Exercise
Compare yourself with other Compare yourself with other judgesjudges
Rate each of the following on a Rate each of the following on a scale of 1 to scale of 1 to
(1= no risk; 7 = high risk)(1= no risk; 7 = high risk)StecklemeyerStecklemeyer
CASE #1CASE #1
A 21 year old male, foreign graduate student A 21 year old male, foreign graduate student was brought to Crisis Intervention Center by was brought to Crisis Intervention Center by friends and a pastor. After informing his friends and a pastor. After informing his friends that he planned to jump off a bridge, he friends that he planned to jump off a bridge, he actually went there and had to be physically actually went there and had to be physically restrained from jumping. He had written restrained from jumping. He had written several suicide notes, one willing his computer several suicide notes, one willing his computer to a friend, another to a different friend stating to a friend, another to a different friend stating that the patient would be dead by the time his that the patient would be dead by the time his note was opened.note was opened.
CASE # 1 ContinuedCASE # 1 Continued
The patient described himself as being quite The patient described himself as being quite depressed, with low energy, poor sleep and depressed, with low energy, poor sleep and appetite, and persistent suicidal ideation. The appetite, and persistent suicidal ideation. The precipitant seems to have been his girlfriend’s precipitant seems to have been his girlfriend’s breaking off their engagement four days ago. breaking off their engagement four days ago. He has a psychiatric history of several years, but He has a psychiatric history of several years, but refuses to reveal any details. He exhibits some refuses to reveal any details. He exhibits some grandiosity, paranoid mentation, anger, agitation grandiosity, paranoid mentation, anger, agitation and irritability. He appears somewhat manic but and irritability. He appears somewhat manic but not depressed. He denies any acute plan to not depressed. He denies any acute plan to commit suicide and is threatening to sue the CID commit suicide and is threatening to sue the CID for having been detained.for having been detained.
Risk RatingRisk Rating
Rating: High RiskRating: High Risk
Mean 6.21Mean 6.21
SD. 0.86SD. 0.86
Case # 2Case # 2
A 16-year-old Native America female presented A 16-year-old Native America female presented as a self-referral following an overdose of 12 as a self-referral following an overdose of 12 aspirin tables. Patient reports that she could not aspirin tables. Patient reports that she could not tolerate the rumors at school that she and tolerate the rumors at school that she and another girl are sharing the same boyfriend.another girl are sharing the same boyfriend.The patient denies being suicidal at this time (“I The patient denies being suicidal at this time (“I won’t do it again; I learned my lesson.”)won’t do it again; I learned my lesson.”)
She reports that she has always had difficulty She reports that she has always had difficulty expressing her feelings. In the interview she is expressing her feelings. In the interview she is quiet, guarded and initially reluctant to talk.quiet, guarded and initially reluctant to talk.
Diagnostic impression: adjustment disorderDiagnostic impression: adjustment disorder
Risk RatingRisk Rating
Rating: Low RiskRating: Low Risk
Mean: 2.25Mean: 2.25
SD: 1.29SD: 1.29
Case # 3Case # 3
A 39 year old white male was referred from A 39 year old white male was referred from the Emergency room. Patient was in the the Emergency room. Patient was in the process of overdosing when he was called by process of overdosing when he was called by a friend, who arranged for the ambulance to a friend, who arranged for the ambulance to bring him to the CIC. The patient took 10 or bring him to the CIC. The patient took 10 or 15 aspirin tablets and 72 over the counter 15 aspirin tablets and 72 over the counter sleeping pills. He had written a long suicide sleeping pills. He had written a long suicide note bequeathing belongings, expressing note bequeathing belongings, expressing guilt about not doing well on his job and guilt about not doing well on his job and feeling hopeless about a “hereditary thinking feeling hopeless about a “hereditary thinking disorder.”disorder.”
Case # 3 continuedCase # 3 continued
He feels that no one can help him and He feels that no one can help him and suffers from low self esteem. Says, “I’m a suffers from low self esteem. Says, “I’m a misfit.”misfit.”
Three nights ago he had also made a Three nights ago he had also made a suicide attempt with Navane and aspirin suicide attempt with Navane and aspirin but woke up by himself in the morning. He but woke up by himself in the morning. He lives by himself. There was no obvious lives by himself. There was no obvious immediate precipitant, but the patient’s immediate precipitant, but the patient’s mother had died six months ago. He is mother had died six months ago. He is currently in therapy and has a psychiatrist.currently in therapy and has a psychiatrist.
Risk RatingRisk Rating
Rating: High RiskRating: High Risk
Mean: 6.58Mean: 6.58
SD: 0.61SD: 0.61
Case # 4Case # 4
A 38-year-old man with a chronic and persistent, A 38-year-old man with a chronic and persistent, severe infection in his right hand is evaluated to severe infection in his right hand is evaluated to be moderately depressed. Prognosis for his be moderately depressed. Prognosis for his infection is not good and he has been struggling infection is not good and he has been struggling with feelings of hopelessness regarding his hand.with feelings of hopelessness regarding his hand.
There is no family history for suicide, mental illness, There is no family history for suicide, mental illness, mood disorders or alcoholism. This man is mood disorders or alcoholism. This man is neither alcoholic nor drug dependent, has a high neither alcoholic nor drug dependent, has a high IQ and has never been in trouble emotionally. He IQ and has never been in trouble emotionally. He is cooperative during the interview, but distant. is cooperative during the interview, but distant. His family remains greatly concerned.His family remains greatly concerned.
What you need to know….What you need to know….
This troubled man has been training to be This troubled man has been training to be a concert pianist for the past 25 years.a concert pianist for the past 25 years.
Case # 5Case # 5
A 30-year-old married female is discovered to be A 30-year-old married female is discovered to be having an affair by her husband (a minister). After having an affair by her husband (a minister). After her husband’s learning of her indiscretions, she her husband’s learning of her indiscretions, she requests an emergency evaluation for treatment. requests an emergency evaluation for treatment. She states she has not been depressed, but does She states she has not been depressed, but does feel panicky. She states her husband has a feel panicky. She states her husband has a history of losing his temper and she is afraid of history of losing his temper and she is afraid of him. However, she seems resourceful, intelligent him. However, she seems resourceful, intelligent and articulate. There are no children in the family. and articulate. There are no children in the family. She does not have a history of prior suicide She does not have a history of prior suicide attempts, but reports she is now thinking about it. attempts, but reports she is now thinking about it. She reports she and her husband have continued She reports she and her husband have continued having sexual relations throughout the period of having sexual relations throughout the period of her affair.her affair.

What you can’t know, but should What you can’t know, but should always plan for….always plan for….
Two days before her scheduled Two days before her scheduled counseling appointment, her lover tests counseling appointment, her lover tests positive for HIV and calls her husband to positive for HIV and calls her husband to inform him of his exposure….inform him of his exposure….
Things to Keep in MindThings to Keep in Mind
The absence of suicidal ideation does not equal The absence of suicidal ideation does not equal no suicide riskno suicide risk
The denial of suicide ideation does not equal no The denial of suicide ideation does not equal no suicide risksuicide risk
Managed care companies don’t pay death Managed care companies don’t pay death benefitsbenefits
Managed care admission criteria often require Managed care admission criteria often require specific suicide planning and/or a previous specific suicide planning and/or a previous attempt – these requirements are not based on attempt – these requirements are not based on scientific standards scientific standards
Things to keep in mind….Things to keep in mind….
Wall, Platt and Hall, 1999 study of 100 Wall, Platt and Hall, 1999 study of 100 successive suicide attempters:successive suicide attempters:- 83 had been seen within one month by - 83 had been seen within one month by healthcare providers (PCP and mental health), healthcare providers (PCP and mental health), yet only 28 had be asked about suicide.yet only 28 had be asked about suicide.
You can’t assess risk you don’t know is there, You can’t assess risk you don’t know is there, and your referral source PROBABLY hasn’t and your referral source PROBABLY hasn’t asked!asked!
Don’t ask, don’t tell, don’t work….Don’t ask, don’t tell, don’t work….
If you are not a healthcare If you are not a healthcare professional…professional…
Do not assume a recent doctor visit led to Do not assume a recent doctor visit led to a suicide risk assessment.a suicide risk assessment.
Do not assume a recent visit to a mental Do not assume a recent visit to a mental health professional led to a suicide risk health professional led to a suicide risk assessment.assessment.– Remember – the odds of being asked if you Remember – the odds of being asked if you
are suicidal by a healthcare professional is are suicidal by a healthcare professional is less than 50% - even when you are actively less than 50% - even when you are actively suicidal!suicidal!
If you are a healthcare provider, 10 top If you are a healthcare provider, 10 top reasons never to ask about suicide…reasons never to ask about suicide…
Reason # 10: My schedule is already full Reason # 10: My schedule is already full next week if they need extra sessions.next week if they need extra sessions.
The 10 Top Reasons never to ask The 10 Top Reasons never to ask your patient if they’re suicidalyour patient if they’re suicidal
Reason # 10: My schedule is already full Reason # 10: My schedule is already full next week if they need extra sessions.next week if they need extra sessions.
Reason # 9: If they were really suicidal, they Reason # 9: If they were really suicidal, they would say so.would say so.
The 10 Top Reasons never to ask The 10 Top Reasons never to ask your patient if they’re suicidalyour patient if they’re suicidal
Reason # 10: My schedule is already full Reason # 10: My schedule is already full next week if they need extra sessions.next week if they need extra sessions.
Reason # 9: If they were really suicidal, they Reason # 9: If they were really suicidal, they would say so.would say so.
Reason# 8: There’s no room on the form.Reason# 8: There’s no room on the form.
The 10 Top Reasons never to ask The 10 Top Reasons never to ask your patient if they’re suicidalyour patient if they’re suicidal
Reason # 10: My schedule is already full Reason # 10: My schedule is already full next week if they need extra sessions.next week if they need extra sessions.
Reason # 9: If they were really suicidal, they Reason # 9: If they were really suicidal, they would say so.would say so.
Reason# 8: There’s no room on the form.Reason# 8: There’s no room on the form.
Reason # 7: I’m not sure I like this patient Reason # 7: I’m not sure I like this patient very much.very much.
The 10 Top Reasons never to ask The 10 Top Reasons never to ask your patient if they’re suicidalyour patient if they’re suicidal
Reason # 10: My schedule is already full Reason # 10: My schedule is already full next week if they need extra sessions.next week if they need extra sessions.
Reason # 9: If they were really suicidal, they Reason # 9: If they were really suicidal, they would say so.would say so.
Reason# 8: There’s no room on the form.Reason# 8: There’s no room on the form.Reason # 7: I’m not sure I like this patient Reason # 7: I’m not sure I like this patient
very much.very much.Reason # 6: The managed care company Reason # 6: The managed care company
doesn’t want to know.doesn’t want to know.
The 10 Top Reasons never to ask The 10 Top Reasons never to ask your patient if they’re suicidalyour patient if they’re suicidal
Reason # 5: Denial in my line of work is Reason # 5: Denial in my line of work is underrated, what I don’t know can’t hurt underrated, what I don’t know can’t hurt me.me.
The 10 Top Reasons never to ask The 10 Top Reasons never to ask your patient if they’re suicidalyour patient if they’re suicidal
Reason # 5: Denial in my line of work is Reason # 5: Denial in my line of work is underrated, what I don’t know can’t hurt underrated, what I don’t know can’t hurt me.me.
Reason # 4: It’s already 11:45 and I have Reason # 4: It’s already 11:45 and I have plans for lunch.plans for lunch.
The 10 Top Reasons never to ask The 10 Top Reasons never to ask your patient if they’re suicidalyour patient if they’re suicidal
Reason # 5: Denial in my line of work is Reason # 5: Denial in my line of work is underrated, what I don’t know can’t hurt underrated, what I don’t know can’t hurt me.me.
Reason # 4: It’s already 11:45 and I have Reason # 4: It’s already 11:45 and I have plans for lunch.plans for lunch.
Reason # 3: I probably couldn’t get them Reason # 3: I probably couldn’t get them into a hospital anyway. into a hospital anyway.
The 10 Top Reasons never to ask The 10 Top Reasons never to ask your patient if they’re suicidalyour patient if they’re suicidal
Reason # 5: Denial in my line of work is Reason # 5: Denial in my line of work is underrated, what I don’t know can’t hurt me.underrated, what I don’t know can’t hurt me.
Reason # 4: It’s already 11:45 and I have Reason # 4: It’s already 11:45 and I have plans for lunch.plans for lunch.
Reason # 3: I probably couldn’t get them into Reason # 3: I probably couldn’t get them into a hospital anyway.a hospital anyway.
Reason # 2: Nothing I learned in graduate Reason # 2: Nothing I learned in graduate school says I have to.school says I have to.
And the # 1 reason not ask our And the # 1 reason not ask our patient if he or she is suicidal?patient if he or she is suicidal?
MY GOD THEY MIGHT SAY MY GOD THEY MIGHT SAY YES!YES!
True storyTrue story
My son died by suicide in 1993 and in the process of My son died by suicide in 1993 and in the process of suing the hospital and the doctor, the last professional to suing the hospital and the doctor, the last professional to see my son for therapy was a Ph.D. in see my son for therapy was a Ph.D. in Psychology. When this person was deposed, he Psychology. When this person was deposed, he reported that he never asked him if he was suicidal reported that he never asked him if he was suicidal (Todd was two days post discharge from a suicide (Todd was two days post discharge from a suicide attempt) and said that 'he was a bright young adult, if he attempt) and said that 'he was a bright young adult, if he was suicidal, he would have told me.' Two days later, was suicidal, he would have told me.' Two days later, Todd hung himself. I won the case out of court without Todd hung himself. I won the case out of court without going to a jury!going to a jury!
Sherry Bryant, LCSW, CADC, LMFTSherry Bryant, LCSW, CADC, LMFT
New moduleNew module
Break – lunch?Break – lunch?
CURRENT THINKING ON SUICIDE AND RISK
The greater the number of losses, the greater the risk.
Personally humiliating events.
No good evidence for sexual orientation as an independent risk factor for suicide.
Treatment prevents suicide.
Eve Morscicki, NIMH, 1997
Suicide Risk Assessment: What Suicide Risk Assessment: What you Need to Know…you Need to Know…
Screens for suicide produce large Screens for suicide produce large numbers of false positives (will not die by numbers of false positives (will not die by suicide)suicide)Positive screens require assessmentsPositive screens require assessmentsNo useful psychological tests or methods No useful psychological tests or methods to predict suicide attempt (NIMH)to predict suicide attempt (NIMH)Summation of risk factor approach too Summation of risk factor approach too nonspecific and weak in predicting nonspecific and weak in predicting individual suicideindividual suicide
Prediction vs. Standard of CarePrediction vs. Standard of Care
You are not required to predict the future, You are not required to predict the future, but you are required to try (assess risk).but you are required to try (assess risk).
Note: 40% of clinical decisions at major Note: 40% of clinical decisions at major academic medical centers are not based academic medical centers are not based on research evidence (Gray, on research evidence (Gray, Evidence Evidence Based PsychiatryBased Psychiatry, APA 2004), APA 2004)
CURRENT THINKING ON SUICIDE AND RISK
The greater the number of losses, the greater the risk.
No good evidence for sexual orientation as an independent risk factor for suicide.
Personally humiliating events may trigger suicidal behavior in non-mentally ill people
Single greatest risk: untreated mental illness
Eve Morscicki, NIMH, 1997
CURRENT THINKING ON SUICIDE AND RISK
Necessary condition + trigger(s) push suicide threshold.
Distal vs. Proximal & trait vs. State.
Halt (hungry, angry, lonely, tired).
Mental illness and suicide disconnect (90+%).
Absence of a psychiatric diagnosis does not equal mental health.
Co-morbidity is the single greatest risk.
CURRENT STATUS OF SUICIDE RISK ASSESSMENT
National Survey: Almost all clinicians rely on clinical interview (Jobes, Eyman & Yufi, 1995).
No known test will predict suicide.
Screening inventories useful but…. Beck Hopelessness scale the best life long predictor
Risk detection is job one.
75% of suicides see a physician within a week to a month before their death (NIMH: opportunities missed)
Current screening methods produce large numbers of false positives.
Summation of risk factor approach:-not clinically useful-too nonspecific to be helpful-inefficient and weak in predicting
individual suicide
67% - 91% of completers made no previous attempt (Coe, 1963 & Dorpat, 1960).
Lot’s of risk goes unrecognized…
CURRENT STATUS OF SUICIDE RISK ASSESSMENT
UNRECOGNIZED RISK
60% of suicide completers had no contact with a mental health professional and no prior suicide attempt.
60% to 90% of all suicide completers had communicated explicit intent to a significant other during the period prior to death.
75% to 80% had a non-psychiatrist physician contact within six months.
93% of completers had an Axis I diagnosis.
One-sixth of all completers are in current treatment with a mental health provider
Clark and Fawcett 1991
Limitations of the clinical Limitations of the clinical interview in suicide risk interview in suicide risk
assessmentassessment
Update and new researchUpdate and new research
Current practice standardsCurrent practice standards
Clinicians rely on their clinical interviewing skills Clinicians rely on their clinical interviewing skills to understand the patient’s realityto understand the patient’s reality
The patient’s reality is often distorted by CNS The patient’s reality is often distorted by CNS dysfunctiondysfunction
““Facts” elicited from distressed patients may be Facts” elicited from distressed patients may be interesting and useful to plan treatment, but they interesting and useful to plan treatment, but they may not be an accurate reflection of dynamic may not be an accurate reflection of dynamic realityreality
Self-disclosure and suicide risk:Self-disclosure and suicide risk:Why not “tell all?”Why not “tell all?”
Fear that full disclosure will lead to voluntary or even Fear that full disclosure will lead to voluntary or even involuntary hospitalizationinvoluntary hospitalization
Fear that full disclosure will prevent discharge from Fear that full disclosure will prevent discharge from hospitalhospital
Fear that full disclosure will lead to arrest and possibly Fear that full disclosure will lead to arrest and possibly incarcerationincarceration
Fear that full disclosure of suicidal desire and intent will Fear that full disclosure of suicidal desire and intent will lead to unwanted rescuelead to unwanted rescue
Why not “tell all?”Why not “tell all?”
Fear that revelation of access to a firearm or drugs may Fear that revelation of access to a firearm or drugs may implicate personal or third party illegal ownership of implicate personal or third party illegal ownership of samesame
Fear that the interviewer is neither benevolent nor Fear that the interviewer is neither benevolent nor trustworthytrustworthy
Fear that revelation of a suicide plan may expose a Fear that revelation of a suicide plan may expose a double suicide, suicide pact or planned murder-suicidedouble suicide, suicide pact or planned murder-suicide
Fear that disclosure of suicidal desire, intent, rehearsal Fear that disclosure of suicidal desire, intent, rehearsal or past suicide attempts will lead to shame and censure or past suicide attempts will lead to shame and censure or job denial or lossor job denial or loss
Better solutionBetter solution
Do not rely on a single reporterDo not rely on a single reporter
Do not rely on a single data sourceDo not rely on a single data source
Do Do rely on multiple observersrely on multiple observers
Interview everyone possible (conduct a Interview everyone possible (conduct a psychological autopsy in reverse)psychological autopsy in reverse)
What you don’t bother to learn now, you What you don’t bother to learn now, you have to learn later (in court)have to learn later (in court)
It’s what they do, not what they sayIt’s what they do, not what they say
End moduleEnd module
Questions?Questions?
The QPR Triage Risk The QPR Triage Risk Assessment MethodAssessment Method
The QPR Suicide Triage The QPR Suicide Triage interview is not:interview is not:
A substitute for psychiatric diagnosisA substitute for psychiatric diagnosis
A treatment planA treatment plan
A substitute for a comprehensive mental A substitute for a comprehensive mental health examinationhealth examination
Follow along….Follow along….
Please take your sample triage document Please take your sample triage document or one from your folder and follow along or one from your folder and follow along and, if you like, make notes…and, if you like, make notes…
The triage interview is:The triage interview is:
A tactical structured interview protocol A tactical structured interview protocol designed to obtain critical, dynamic suicide designed to obtain critical, dynamic suicide risk and protective factor informationrisk and protective factor informationA tool to help determine near-term suicide A tool to help determine near-term suicide risk risk A strategic intervention designed to reduce A strategic intervention designed to reduce immediate risk of suicide through empathic immediate risk of suicide through empathic inquiry and enhance suicide protective inquiry and enhance suicide protective factorsfactors
The triage interview may not be The triage interview may not be useful with:useful with:
Actively psychotic patientsActively psychotic patients
Patients so depressed they can barely speak, or Patients so depressed they can barely speak, or so manic they cannot be engagedso manic they cannot be engaged
Intoxicated patientsIntoxicated patients
Delusional patientsDelusional patients
Highly impulsive patients, especially if on drugs Highly impulsive patients, especially if on drugs and/or alcoholand/or alcohol
Patients suffering from severe dementia or Patients suffering from severe dementia or obvious cognitive impairmentsobvious cognitive impairments
Asking the S Question: SamplesAsking the S Question: Samples
““You know, when people are as upset as you You know, when people are as upset as you seem to be, they sometimes wish they were seem to be, they sometimes wish they were dead. I’m wondering if you’re feeling that way, dead. I’m wondering if you’re feeling that way, too?”too?”““You seem very unhappy. Have you had any You seem very unhappy. Have you had any thoughts of death or suicide?”thoughts of death or suicide?”““Suicidal thoughts are a common symptom of Suicidal thoughts are a common symptom of depression; have you had been depressed depression; have you had been depressed lately?”lately?”““Have you been suicidal or have you been Have you been suicidal or have you been thinking about suicide?”thinking about suicide?”
Sample S QuestionsSample S Questions
““Are you considering ending your life?”Are you considering ending your life?”
““Have you ever wished that you were Have you ever wished that you were dead?”dead?”
““Are you thinking about killing yourself?”Are you thinking about killing yourself?”
““Have you thought about suicide in the Have you thought about suicide in the past two months?” (Sometimes suicidal past two months?” (Sometimes suicidal people will tell you about how they felt last people will tell you about how they felt last week, but not today.)week, but not today.)
Wrong way to ask S QuestionWrong way to ask S Question
““You’re not thinking of suicide, are you?” You’re not thinking of suicide, are you?”
……or any variant question which asks for a or any variant question which asks for a denial….denial….
WHAT’S WRONG? WHAT’S WRONG?
What You Should Learn:What You Should Learn:
Explanation of the reasons for suicideExplanation of the reasons for suicide
Problem(s) that suicide would solve, such Problem(s) that suicide would solve, such as being a burden on othersas being a burden on others
How this person solves problems How this person solves problems
Sample QuestionsSample Questions
““Okay John, why don’t you tell me what’s Okay John, why don’t you tell me what’s wrong with your life right now?”wrong with your life right now?”
““Audrey, what made you decide to come in Audrey, what made you decide to come in today?” today?”
““We’ve got some time to talk. I’d very We’ve got some time to talk. I’d very much like to hear your version of what’s much like to hear your version of what’s wrong right now.” wrong right now.”
Key Points for What’s Wrong?Key Points for What’s Wrong?
Most suicidal people need to talk. Others Most suicidal people need to talk. Others may not be listening, but now you are. may not be listening, but now you are. Telling their story produces relief.Telling their story produces relief.Active listening without interjecting Active listening without interjecting judgments or opinions is essential to judgments or opinions is essential to encourage full disclosure.encourage full disclosure.Telling one’s story may help restore the Telling one’s story may help restore the person’s ability to think more clearly and person’s ability to think more clearly and cope more successfully.cope more successfully.
Expect Common themes (suicidal Expect Common themes (suicidal desire and intent)desire and intent)
– Feels hopeless and depressed (clinical Feels hopeless and depressed (clinical depression is the most common cause of depression is the most common cause of suicide)suicide)
– Feels isolated and aloneFeels isolated and alone
– Has lost job or major relationship or a multiple Has lost job or major relationship or a multiple of lossesof losses
– Feels overwhelmed, angry and upsetFeels overwhelmed, angry and upset
Common themesCommon themes
– Feels like a burden on othersFeels like a burden on others
– Financial problems with no escapeFinancial problems with no escape
– Fears being humiliated, e.g., arrested for a Fears being humiliated, e.g., arrested for a sex crimesex crime
– Has serious problems at work Has serious problems at work
WHY NOW?WHY NOW?What you should learnWhat you should learn
Recent history of recent or anticipated real or Recent history of recent or anticipated real or imagined losses or rejections. imagined losses or rejections. Trigger event(s) - separation from spouse, loss Trigger event(s) - separation from spouse, loss of home, domestic violence, anticipated loss of of home, domestic violence, anticipated loss of job, any changes creating a sense of job, any changes creating a sense of burdensomeness on others, or that causes burdensomeness on others, or that causes isolation from one’s primary group.isolation from one’s primary group.Onset of sleeplessness, depression, loss of Onset of sleeplessness, depression, loss of appetite, relapse into drug or alcohol use, appetite, relapse into drug or alcohol use, anxiety, panic attacks, or other symptoms of anxiety, panic attacks, or other symptoms of acute psychological distress.acute psychological distress.
Sample QuestionsSample Questions
““Robin, what has changed such that you Robin, what has changed such that you are considering suicide now?”are considering suicide now?”““It sounds as though this relationship has It sounds as though this relationship has been difficult for a long time. What’s been difficult for a long time. What’s different for you now?”different for you now?”““Joe, it sounds like you’ve been unhappy Joe, it sounds like you’ve been unhappy for months and hadn’t contemplated for months and hadn’t contemplated suicide before. Why are things so suicide before. Why are things so unbearable now?”unbearable now?”
Key Points for Why Now?Key Points for Why Now?
Something unacceptable is about to happen.Something unacceptable is about to happen.
Suicide or homicide threats have been made.Suicide or homicide threats have been made.
Ambivalence about living or dying, and both reasons for Ambivalence about living or dying, and both reasons for living and dying may be expressed. living and dying may be expressed.
Listen for both suicide risk and protective factors.Listen for both suicide risk and protective factors.
Are suicidal desire and intent present?Are suicidal desire and intent present?
How is the person’s ability to cope being overwhelmed?How is the person’s ability to cope being overwhelmed?
WITH WHAT? WITH WHAT?
What You Should Learn:What You Should Learn:
The means of suicide under consideration (if The means of suicide under consideration (if any) any)
Lethality of means being consideredLethality of means being considered
Accessibility to the means selected (this requires Accessibility to the means selected (this requires a follow up question – where are the means?)a follow up question – where are the means?)
Whether more than one method is under Whether more than one method is under considerationconsideration
Practice or rehearsal with the means selectedPractice or rehearsal with the means selected
Sample QuestionsSample Questions
““Have you thought about how you would Have you thought about how you would kill yourself? If the person responds with a kill yourself? If the person responds with a ‘yes,’ follow up with:‘yes,’ follow up with:- “Can you tell me how you’ve considered - “Can you tell me how you’ve considered
ending your life?”ending your life?”- “How would you kill yourself?”- “How would you kill yourself?”- “Do you have a method in mind?”- “Do you have a method in mind?”- “Have you practiced with the (means - “Have you practiced with the (means selected)?”selected)?”
Redundant Planning?Redundant Planning?
Sample questions:Sample questions:
““Have you had any other thoughts of how Have you had any other thoughts of how you might kill yourself?”you might kill yourself?”
““If the first method didn’t work what else If the first method didn’t work what else might you try?”might you try?”
Sample questions to determine Sample questions to determine the availability of meansthe availability of means
““Do you have immediate access to Do you have immediate access to (medications, a gun, a razor blade, etc.)?”(medications, a gun, a razor blade, etc.)?”
““Where is the gun (rope, razor, etc.)?”Where is the gun (rope, razor, etc.)?”
““Where would you get the medications Where would you get the medications (gun, rope, razor, etc.)?”(gun, rope, razor, etc.)?”
Key Points for With What?Key Points for With What?
Rehearsal suggests suicide capability is presentRehearsal suggests suicide capability is present
Past self-injury (with any method)Past self-injury (with any method)
Risk increases dramatically with access to meansRisk increases dramatically with access to means
Never suggest another method or meansNever suggest another method or means
Means selection is often influenced by culture, occupation, social Means selection is often influenced by culture, occupation, social contagion (modeling effect), and availabilitycontagion (modeling effect), and availability
Multiple methods under consideration = greater riskMultiple methods under consideration = greater risk
WHERE AND WHEN?WHERE AND WHEN?
What You Should Learn:What You Should Learn:A conditional suicide plan contingent on some A conditional suicide plan contingent on some unacceptable event, “If she leaves me I will kill unacceptable event, “If she leaves me I will kill myself.” “If they fire me, I die.” “If I’m arrested I myself.” “If they fire me, I die.” “If I’m arrested I will have to kill myself.”will have to kill myself.”Possible location of a suicide attemptPossible location of a suicide attemptPlan for rescue or to avoid rescuePlan for rescue or to avoid rescueDegree and details of lethal planningDegree and details of lethal planningPossible anniversary phenomenaPossible anniversary phenomenaPotential for murder-suicide or suicide pactPotential for murder-suicide or suicide pact
Sample QuestionsSample Questions
““Have thought about where you might try Have thought about where you might try to kill yourself?”to kill yourself?”
““Have you decided when?”Have you decided when?”
““Is there something that might happen that Is there something that might happen that would put your plan in motion?”would put your plan in motion?”
Key Points for When and Where?Key Points for When and Where?
Many suicide attempts are impulsive and little or Many suicide attempts are impulsive and little or no planning will be evidentno planning will be evidentGenerally, the more detailed the planning Generally, the more detailed the planning (intent) the greater the risk (intent) the greater the risk Specificity of time and place = greater riskSpecificity of time and place = greater riskDetermination of “anniversary phenomena” may Determination of “anniversary phenomena” may open discussion of opportunities and a referral open discussion of opportunities and a referral for help, e.g., grief counseling for a major lossfor help, e.g., grief counseling for a major lossEfforts to avoid rescue = greater riskEfforts to avoid rescue = greater riskResistance to disclosure of a suicide plan may Resistance to disclosure of a suicide plan may indicate higher riskindicate higher risk
WHEN AND WITH WHAT IN THE WHEN AND WITH WHAT IN THE PAST?PAST?
What You Should LearnWhat You Should LearnPast history of suicidal behaviorsPast history of suicidal behaviorsPast history of intense suicidal ideation and/or planningPast history of intense suicidal ideation and/or planningMethod used in any suicide attempt(s)Method used in any suicide attempt(s)Whether rescue was avoidedWhether rescue was avoidedTiming and precipitants of past attemptsTiming and precipitants of past attemptsSocial response to past attempt(s)Social response to past attempt(s)Treatment, if any, following a suicide attempt or period of severe Treatment, if any, following a suicide attempt or period of severe ideationideationDegree, if any, of medical injuriesDegree, if any, of medical injuriesPotential protective factorsPotential protective factorsComparison of current method under consideration vs. prior method Comparison of current method under consideration vs. prior method usedused
Sample questionsSample questions
““Pat, you’ve been struggling with a lot of different feelings lately and Pat, you’ve been struggling with a lot of different feelings lately and you’re telling me you’ve been considering suicide. Have you ever you’re telling me you’ve been considering suicide. Have you ever had thoughts of suicide in the past?”had thoughts of suicide in the past?”
- If Pat responds “yes,” then ask:- If Pat responds “yes,” then ask:““When was that?When was that?
After learning when a previous episode of suicidality occurred, After learning when a previous episode of suicidality occurred, follow up with:follow up with:
““Did you think about suicide seriously for two or more weeks?”Did you think about suicide seriously for two or more weeks?”““Did you attempt suicide at that time?”Did you attempt suicide at that time?”
Repeat the inquiry until you have the complete historyRepeat the inquiry until you have the complete history
Key Points for When and With Key Points for When and With What?What?
Comprehensive history taking is strongly recommendedComprehensive history taking is strongly recommended
The more detail elicited the better The more detail elicited the better
Suicide attempts while in treatment = greater risk and suggests Suicide attempts while in treatment = greater risk and suggests extraordinary precautionary safety measures are indicated extraordinary precautionary safety measures are indicated
Historical response to a past suicide attempt may provide insights Historical response to a past suicide attempt may provide insights into resolution of the current crisisinto resolution of the current crisis
Attempt to avoid rescue? = greater riskAttempt to avoid rescue? = greater risk
New method under consideration? = greater riskNew method under consideration? = greater risk
WHO IS INVOLVED? WHO IS INVOLVED?
What You Should LearnWhat You Should LearnRole of significant others Role of significant others Names of potentially helpful third partiesNames of potentially helpful third partiesNames of potentially harmful third partiesNames of potentially harmful third partiesNames of persons on whom the suicidal Names of persons on whom the suicidal person feels he or she is a burden (a person feels he or she is a burden (a perceived, not necessarily real burden)perceived, not necessarily real burden)Possible presence of a suicide pact or Possible presence of a suicide pact or murder-suicide planmurder-suicide plan
Sample Questions Sample Questions
““Who are the people or the activities that are important to Who are the people or the activities that are important to you?” you?”
““Who else knows you are in this much pain?”Who else knows you are in this much pain?”
““Who is your main support during times like these?”Who is your main support during times like these?”
““Is there anyone who will be hurt if you take you own Is there anyone who will be hurt if you take you own life?”life?”
““If you feel like a burden on others, who are they?”If you feel like a burden on others, who are they?”
Key PointsKey Points
Most suicidal crises involve at least two people, such as Most suicidal crises involve at least two people, such as a couple in conflict a couple in conflict
Suicide threats made to significant others without Suicide threats made to significant others without producing relief or change may suggest higher riskproducing relief or change may suggest higher risk
Social isolation = greater riskSocial isolation = greater risk
Feeling a burden to significant others = greater riskFeeling a burden to significant others = greater risk
Threats of violence toward others may be part of a Threats of violence toward others may be part of a planned suicide, or murder-suicide plan involving a planned suicide, or murder-suicide plan involving a conflicted relationship, students at school, or co-workersconflicted relationship, students at school, or co-workers
WHY NOT NOW?WHY NOT NOW?
What You Should LearnWhat You Should LearnOne or more protective factors (reasons for One or more protective factors (reasons for living)living)Spiritual or religious prohibitions against suicideSpiritual or religious prohibitions against suicidePersonal or professional responsibilities to Personal or professional responsibilities to others (connectedness)others (connectedness)Plans made for dependent others, such as, “My Plans made for dependent others, such as, “My brother will raise my children.”brother will raise my children.” Meaningfulness of life and purpose for livingMeaningfulness of life and purpose for livingResidual tasks to be completed before the Residual tasks to be completed before the attempt, such as making out a willattempt, such as making out a will

Sample QuestionsSample Questions
““Give me some reasons why you may want to Give me some reasons why you may want to live?”live?”““You’ve shared some reasons why you are You’ve shared some reasons why you are considering suicide. What are some reasons considering suicide. What are some reasons that you should not kill yourself?”that you should not kill yourself?”““Can you give me three reasons to go on living?”Can you give me three reasons to go on living?”““Can you tell me about your core values and Can you tell me about your core values and beliefs?”beliefs?”““Who are you close to? Who matters in your Who are you close to? Who matters in your life”life”““What are your dreams for the future?”What are your dreams for the future?”

Key PointsKey Points
Few or no protective factors = greater riskFew or no protective factors = greater risk
Serious isolation or rejection by others = Serious isolation or rejection by others = greater riskgreater risk
The offer of treatment, rest, hope, relief The offer of treatment, rest, hope, relief from suffering is a powerful protective from suffering is a powerful protective factorfactor
Marshalling protective factors lowers riskMarshalling protective factors lowers risk
Low risk does not equal zero riskLow risk does not equal zero risk

Persuading the Person to Get Persuading the Person to Get HelpHelp
KEY POINTS:KEY POINTS:Expressed anger at you may mean greater riskExpressed anger at you may mean greater riskRefusal to accept help = greater riskRefusal to accept help = greater riskAn abrupt or angry withdrawal from the interview An abrupt or angry withdrawal from the interview may mean greater riskmay mean greater riskUnwillingness to remove the means of suicide = Unwillingness to remove the means of suicide = greater riskgreater riskReassessment of risk may be indicated if help is Reassessment of risk may be indicated if help is refusedrefusedEmergency intervention, consultation and/or Emergency intervention, consultation and/or supervisory input should be readily availablesupervisory input should be readily available

Suicide risk is low to moderateSuicide risk is low to moderate
When:When:
- - Few risk factors are present and several Few risk factors are present and several or many protective factors are present, or many protective factors are present, and the person agrees to:and the person agrees to:
* Not use drugs or alcohol* Not use drugs or alcohol
* Seek help or accept a referral* Seek help or accept a referral
* Remove the means of suicide* Remove the means of suicide
* Commit to a safety plan* Commit to a safety plan

Suicide risk is highSuicide risk is high
When: When: many risk factors are present and few or no many risk factors are present and few or no protective factors are present, and the person:protective factors are present, and the person:- Has been uncooperative- Has been uncooperative- Has said little or nothing about his or her - Has said little or nothing about his or her problemsproblems- Has been distant, evasive and aloof- Has been distant, evasive and aloof- Refuses to go along or agree to the referral - Refuses to go along or agree to the referral and safety planand safety plan- Refuses to remove the mans of suicide- Refuses to remove the mans of suicide

What else would cause you to have What else would cause you to have low confidence in your risk ratinglow confidence in your risk rating
Discussion….Discussion….

SEMANTICS ARE IMPORTANTSEMANTICS ARE IMPORTANT
Poor safety agreement languagePoor safety agreement language
- “I guess I’ll be okay” (vague)- “I guess I’ll be okay” (vague)
- “I’ll call somebody if things get bad.” - “I’ll call somebody if things get bad.” (vague, lacks specificity. How will anyone (vague, lacks specificity. How will anyone know when things “get bad?” What is know when things “get bad?” What is “bad” in this context? Who is “bad” in this context? Who is “somebody?”)“somebody?”)

Real people safety statementsReal people safety statements
““If things get this bad again, I’ll call my If things get this bad again, I’ll call my pastor. Honest, I will.”pastor. Honest, I will.”
““I won’t do it. I promise. I wouldn’t put I won’t do it. I promise. I wouldn’t put Adam through that. I’ll call you back Adam through that. I’ll call you back personally if I need to.”personally if I need to.”
““I can, and do, agree to a safety plan. I I can, and do, agree to a safety plan. I don’t want to die. I honor my word.”don’t want to die. I honor my word.”

KEY POINTS in Safety AgreementsKEY POINTS in Safety Agreements
Set specific times and expectations for crisis Set specific times and expectations for crisis management action steps (work through safety plan management action steps (work through safety plan checklist)checklist)
Recommitment to life; not a “no-suicide contract”Recommitment to life; not a “no-suicide contract”
Clarity of language in a person’s recommitment to life Clarity of language in a person’s recommitment to life and safety plan helps confirm risk is now lowerand safety plan helps confirm risk is now lower
Hard copy directions, phone numbers, and how-to steps Hard copy directions, phone numbers, and how-to steps are helpful and key to avoiding claims of negligenceare helpful and key to avoiding claims of negligence

USE QUOTATIONSUSE QUOTATIONS
For example, “I just couldn’t do that [suicide] to my For example, “I just couldn’t do that [suicide] to my family,” illustrates that, in this case, the family is a strong family,” illustrates that, in this case, the family is a strong protective factor.protective factor.Likewise, the phrase, “I have a five-year-old boy and am Likewise, the phrase, “I have a five-year-old boy and am pregnant right now,” indicates much lower suicide risk pregnant right now,” indicates much lower suicide risk than, say, “I have no children and just had my first than, say, “I have no children and just had my first abortion.”abortion.”If the statement is not clear and unequivocal, try to help If the statement is not clear and unequivocal, try to help the person make the statement more clearly. The greater the person make the statement more clearly. The greater the clarity of this commitment, even over the phone to a the clarity of this commitment, even over the phone to a stranger, the greater the likelihood the person will follow stranger, the greater the likelihood the person will follow through with the recommended referral.through with the recommended referral.

Role play practice sessionsRole play practice sessions
Allow 25-30 minutes per role playAllow 25-30 minutes per role play
Complete sample QPR Triage document Complete sample QPR Triage document as part of the practice sessionas part of the practice session
Process each experienceProcess each experience
All questions answeredAll questions answered

THANK YOU!THANK YOU!
Contact informationContact information
Free book from websiteFree book from website
The Institute does not provide clinical The Institute does not provide clinical consultation….consultation….
My contact information:My contact information:





![QPR SUICIDE PREVENTION TRAINING: A CALIFORNIA STATE ... · Health Association [ACHA], 2013). Suicide is the third leading cause of death of individuals ages 15-24 in the United States,](https://img.pdfslide.net/doc/110x75/5ecd385be758c102e87a8cbd/qpr-suicide-prevention-training-a-california-state-health-association-acha.jpg)























