Embed Size (px)
Citation preview

This webinar on “HER2 Testing Revision” is presented
by David G. Hicks, MD, FCAP and Stephen J.
Sarewitz, MD, FCAP
Your host is Jill Kaufman, PhD. For comments about
this webinar or suggestions for upcoming
webinars, please contact Jill Kaufman at
THE WEBINAR WILL BEGIN MOMENTARILY. ENJOY!
Welcome to CAP’s “Hot Topics in Pathology”
Webinar Series sponsored by the
Personalized Health Care Committee
© 2013 College of American Pathologists. All rights reserved. 1

cap.org v. #
HER2 Testing Revision David G Hicks, MD, FCAP, and Stephen J. Sarewitz, MD, FCAP
December 3, 2013
Hot Topics in
Pathology

• Professor of Pathology and Laboratory
Medicine, University of Rochester
School of Medicine
• Director of Surgical Pathology at the
University of Rochester Medical Center
• Current research interests focus on the
molecular genetic profiling of clinical
samples from patients with cancer
• Authored or co-authored over 140
peer reviewed articles
• Member of the CAP’s Breast Pathology
Certificate Program Work Group and
Breast Predictive Factors Testing
Program Group
David G. Hicks, MD, FCAP
© 2013 College of American Pathologists. All rights reserved. 3

• Current CAP Board of
Governors
• Vice-chair for CAP’s Council
on Accreditation
• Member of CAP’s Risk
Management Committee,
Council on Education and
Constitution and Bylaws
Committee
Stephen J. Sarewitz, MD, FCAP
© 2013 College of American Pathologists. All rights reserved. 4

Disclaimer
The College does not permit reproduction of any substantial portion of the material in this Webinar without its written
authorization. The College hereby authorizes attendees of the
CAP Webinar to use the pdf presentation solely for educational
purposes within their own institutions. The College prohibits use of the material in the Webinar – and any unauthorized use of
the College’s name or logo – in connection with promotional
efforts by marketers of laboratory equipment, reagents,
materials, or services.
Opinions expressed by the speaker are the speaker’s own and
do not necessarily reflect an endorsement by CAP of any
organizations, equipment, reagents, materials or services used
by participating laboratories.
© 2013 College of American Pathologists. All rights reserved. 5

• Dr. Hicks – member of a speaker’s bureau
sponsored by Genentech BioOncology that support
educational programs on breast cancer testing
• Dr. Sarewitz – no disclosures
Disclosure
© 2013 College of American Pathologists. All rights reserved. 6

Why is HER2 Testing Different?
• HER2 testing is more like doing a frozen section than looking at a special stain:
– A single observation leads to a critical treatment decision
• The test is assumed to be accurate and precise every time by both clinician and patient
• ASCO/CAP HER2 testing guidelines have provided standards for improving the accuracy and reliability for testing
To address ongoing testing needs and challenges in light of new published literature, the 2007 ASCO/CAP HER2 guideline have been updated in 2013

2013 HER2 Testing Guidelines Update, What Changed?
Updates From 2007
8
Wolff AC et al. J Clin Oncol. 2013; Oct 7. [Epub ahead of print]
2013 Updates
2013 Recommendations
• All new tumors should be tested (including
metastatic tumors)
• Highlights the need for enhanced communication
between pathologists and oncologists
• Guidance for communicating with patients
• Optimal tissue specimen handling procedures
• Maximum time in fixative: 72 hours
• New algorithms for test interpretation and reporting
• Language on repeat testing (reflex and new tests)

2013 HER2 Testing Guidelines Update: What Remains the Same From 2007
9
1. Wolff AC et al. J Clin Oncol. 2007;25:118-145; 2. Wolff AC et al. J Clin Oncol. 2013; Oct 7. [Epub ahead of print]
No Change
From 20071
Recommendations1,2
• Optimal tissue specimen handling procedures
• Tissue acquisition (ie, minimize cold
ischemic time): <1 hour
• Fixative: 10% neutral buffered formalin
(NBF)
• Minimum duration of fixation: 6 hours
• Must document fixation time points in
accession or report
• Laboratory quality assurance processes,
including proficiency testing and lab
accreditation

2013 HER2 Testing in BC Guidelines Update: Tumor Specimens to be Tested
10
1. Wolff AC et al. J Clin Oncol. 2007;25:118-145; 2. Wolff AC et al. J Clin Oncol. 2013; Oct 7. [Epub ahead of print]
2007 Guidelines1
• All primary breast cancer
specimens and metastases should
have at least one HER2 test
performed
• Perform HER2 testing on every
• Primary invasive tumor
• Metastatic sites
2013 Guideline Update2

2007 Guidelines
• Resection specimens preferred
sample for HER2 testing
• More representative sample of
the patient’s tumor, more
tumor tissue for evaluation
2013 Guideline update
• Increasing use of core for testing
• Core biopsies can be used for initial
test (likely better pre-analytics)
• However, repeat testing on the
excision may be necessary if a HER2
result is negative on the core in
certain circumstances
2013 HER2 Testing in BC Guidelines Update: Recommended Tumor Specimens to be Tested

2013 HER2 Testing in BC Guidelines Update: Tumor Specimen Selection
Core samples may not be optimal in some situations
Crushing and surface artifacts in cores may hamper interpretation
Tumor on resection may show morphologic heterogeneity
Tumor on resection may show intratumoral heterogeneity
Tissue is not fixed for adequate length of time
12
Heterogeneity HER2 IHC stain obtained
by core needle biopsy
Edge Artifact Crush Intratumoral heterogeneity
If core results are questionable, test the excision specimen

• Breast tissue undergoes ischemic changes from the minute it is
removed from a patient
• Enzymatic activity in the tissue is not stopped until fixation begins
(stabilizing tissue)
• Unabated enzymatic degradation of tissue may lead to false
results
– Critical antigens may be altered or lost.
– Test results may be indeterminate because of artifacts caused
by improper handling.
– Breast tissue should be incised and placed into an appropriate
fixative (10% NBF) within <1 hr from removal from the patient
13
Specimen Handling is Critical!

Tumor stained as ‘2+’ for HER2 at 0.5 h of delayed fixation (a), but
demonstrated reduction in staining at 3 h (b) and was completely negative
at 24 h (c) and 48 h (d). Yildiz-Aktas IZ, et al. Mod Pathol. 2012 Aug;25(8):1098-105.

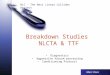
Time to Fixation: HER2 Testing IHC and FISH
15 a, 30 min IHC; b, 30 min FISH; c, 4 h immunohistochemistry; d, 4 h FISH
HER2/CEP17 = 0.98
HER2/CEP17 = 0.29
Khoury T, et al., Mod Pathol. 2009 Nov;22(11):1457-67
30
min
ute
s 4
ho
urs

736 breast cancer specimens, the mean TTF was 53.8 min (SD=37.8min). 453 (61.5%) cases had an TTF less than 1 hour and 283 (38.5%) had TTF greater than an hour

2013 HER2 Testing Guidelines Updates: Duration of Fixation
17
1. Wolff AC et al. J Clin Oncol. 2007;25:118-145; 2. Wolff AC et al. J Clin Oncol. 2013; Oct 7. [Epub ahead of print]
2013 Guideline Update2
• Time in fixative
• 6 – 72 hours
2007 Guidelines1
• Time in fixative
• 6 – 48 hours
Both the ASCO/CAP HER21 and ER/PgR3 Testing Guidelines now share the same recommendation for the duration of fixation
IHC 2+ with appropriate fixation time
IHC 0 after extended fixation time
Core require same fixation time as excisions

2013 HER2 Testing Guidelines Update: Summary of Changes to the Testing Algorithm
18 Wolff AC et al. J Clin Oncol. 2013; Oct 7. [Epub ahead of print]
HER2 Result
IHC ISH
Positive
•> 10% of invasive tumor cells display strong circumferential membrane staining
•Amplified ratio of HER2/CEP17 of ≥ 2.0 or average HER2 signals ≥6
signals/cell (regardless of ratio) in population of >10% of tumor cells
Negative
•IHC 0: No staining observed or membrane staining
that is incomplete, faint/barely perceptible and within ≤10% of the invasive tumor cells
•IHC 1+: Incomplete membrane staining that is faint/barely perceptible and within >10% of the invasive tumor cells
•HER2/CEP17 ratio < 2 and
HER2 signals/cell < 4, regardless of ratio
Equivocal Must reflex test
•2+ based on circumferential membrane staining, incomplete, weak, or moderate within >10% of the
invasive tumor cells; or complete & circumferential
membrane intense staining within ≤10% of the invasive tumor cells
•Dual Probe HER2/CEP17
ratio <2.0 with an average
HER2 copy number ≥4.0 and <6.0 signals/cell
Indeterminate
• Technical issues prevent assay from being conclusive (e.g., issues with controls, specimen handling, artifacts, or analytical failure)
• Assay must be repeated before diagnosis can be rendered

2013 HER2 Testing in BC Guidelines Update: IHC HER2 Positive Interpretation Criteria Redefined
19
HER2 (3+) in
10% of tumor
(HER2 Positive)
If the pathologist or oncologist observes an apparent histopathologic discordance after HER2 testing, the need for additional HER2 testing should be discussed.
1. Wolff AC et al. J Clin Oncol. 2007;25:118-145; 2. Wolff AC et al. J Clin Oncol. 2013; Oct 7. [Epub ahead of print]
*Readily appreciated at low power.
2007 Guidelines1
• Positive for HER2 is 3+ (defined as
uniform intense membrane staining
of > 30% of invasive tumor cells)
• Positive for HER2 is 3+ (defined as
uniform intense membrane staining
of >10% of invasive tumor cells*
2013 Guideline Update2
HER2 (3+) in
>90% of tumor
(HER2 Positive)

2013 HER2 Testing in BC Guidelines Update: IHC HER2 Negative Interpretation Criteria
20
2007 Guidelines1
Negative result for HER2 IHC is 0 or 1+ • IHC 0: no staining
• IHC 1+: weak, incomplete
membrane staining in any
proportion of tumor cells or weak, complete staining in <10% of cells
Negative result for HER2 IHC is 0 or 1+
• IHC 0: No staining* or incomplete
membrane staining (faint/barely
perceptible) and within ≤ 10% of
tumor cells
• IHC 1+: Incomplete membrane
staining (faint/barely perceptible)
and within > 10% of tumor cells*
2013 Guideline Update2
If the pathologist or oncologist observes an apparent histopathologic discordance after HER2 testing, the need for additional HER2 testing should be discussed.

2013 HER2 Testing in BC Guidelines Update: HER2 Testing of the Invasive Component by IHC
21
Wolff AC et al. J Clin Oncol. 2013; Oct 7. [Epub ahead of print]
*Readily appreciated at low power.
If the pathologist or oncologist observes an apparent histopathologic discordance after
HER2 testing, the need for additional HER2 testing should be discussed.

2007 Guidelines
Positive for HER2 is FISH amplified
(ratio of HER2 to CEP17 of > 2.2
or average HER2 gene copy
number > six signals/nucleus for
those test systems without an
internal control probe)
2013 Guideline update
Positive for HER2 is amplified ratio of
HER2/CEP17 of ≥ 2.0 (with
average HER2 signals >4*) or if
average HER2 signals are ≥6
signals/cell (regardless of ratio) in
population of >10% of tumor cells.
*Patient’s with ratio of >2 where eligible
for the adjuvant trial, even if HER2< 4.
no good data on benefit
2013 HER2 Testing in BC Guidelines Update: ISH HER2 Positive Interpretation Criteria, Redefined
If the pathologist or
oncologist observes an
apparent histopathologic
discordance after HER2
testing, the need for
additional HER2 testing
should be discussed.

2013 HER2 Testing in BC Guidelines Update: ISH HER2 Negative Interpretation Criteria, Redefined
2007 Guidelines
Negative for HER2 ISH is FISH
HER2/CEP17 ratio of < 1.8 or
average HER2 gene copy
number of < 4 signals/nucleus
for test systems without an
internal control probe
2013 Guideline update
Negative for HER2 ISH is
HER2/CEP17 ratio < 2 and
HER2 signals/cell < 4*,
regardless of ratio
*Patient’s with ratio of >2 where eligible for the
adjuvant trial, even if HER2< 4, however no
good data on benefit
If the pathologist or oncologist observes an apparent histopathologic discordance after HER2 testing, the need for additional HER2 testing should be discussed.

2013 HER2 Testing in BC Guidelines Update: HER2 Testing of the Invasive Component by Dual Probe ISH
24
Wolff AC et al. J Clin Oncol. 2013; Oct 7. [Epub ahead of print]
Look at ratio,
then HER2#
If the pathologist or oncologist observes an apparent histopathologic discordance after HER2 testing, the need for additional HER2 testing should be discussed.

2013 HER2 Testing in BC Guidelines Update: HER2 Equivocal Results Require a Reflex or Repeat Test
2007 Guidelines
Equivocal for HER2 IHC is 2+
ISH: FISH HER2/CEP17 ratio of 1.8-
2.2 or average HER2 gene
copy number 4-6 HER2
signals/nucleus for test systems
without an internal control
probe
2013 Guideline update
Must report HER2 test result as
Equivocal (HER2 tumor status
Unknown) and order reflex test
using the alternative test if:
IHC: (2+) circumferential membrane
staining, incomplete and/or weak/
moderate in >10% of the invasive
tumor cells; or complete and
circumferential membrane intense
staining within ≤10% of the invasive
tumor cells
ISH: Dual Probe HER2/CEP17 ratio <2.0
with an average HER2 copy
number ≥4.0 and <6.0 signals/cell
If a reflex test on a HER2 Equivocal result
does not render a (+) or (-) HER2 result, must
review clinical and pathologic features of case
and should confer with the oncologist about
additional testing

• New ISH algorithm and interpretive guideline address
unusual cases with:
o Intratumoral heterogeneity
o Chromosomal abnormalities involving CEP17
(aneusomy)
2013 HER2 Testing Guidelines Update: Changes to the Testing Algorithm Help Address:
Some illustrative cases
•New language on repeat HER2 testing

Case#1 History (Heterogeneity)
• 71 year old female
• Palpable mass lesion
• Left breast @ 11:00
• Core needle biopsy
performed
• ER: Negative
• PR: Negative
• HER2 IHC: Shown on
next slide

H&E Stain

HER2 Immunohistochemistry
~10-20% on invasive tumor IHC (3+)

Low Power Scan, HER2 FISH

Low power scan for HER2 IHC versus FISH
*observed in a homogeneous and
contiguous population of at least 10%

HER2 IHC versus FISH
HER2/CEP17 = 1.7
HER2/CEP17 = 7.5
HER2/CEP17 combined = 2.9

33
Reporting Consideration with Heterogeneity
• This case should be reported as HER2
positive, and the percentage of the invasive
tumor involved should be provided on the
report.
• Do not combine the ratios!
• Could result in an equivocal or even negative
result depending on which cells counted
• HER2 signals (and ratio) should be reported for both
the minority amplified (>10%) and the majority non-
amplified portions of the tumor.

Patterns of Intratumor
Heterogeneity for HER2
Mixed Histology
Homogeneous Histology
clusters of HER2+ cells vs scattered + cell

Intratumor Heterogeneity for HER2: IHC vs FISH
Mean score/ratio depends on the
number of amplified cells counted
and gene copy number after dilution
with the non-amplified cells
Fields selected for evaluation will
determine whether or not the tumor is
reported as amplified
Heterogeneity easier to detect by IHC
IHC can be used to target “hot-spots” for FISH analysis
Heterogeneity has implications for core versus excisional biopsies

H&E
Slides courtesy of Dr. Ken Bloom
Core needle biopsy 53 year old female
An Illustrative Case

HER2 IHC
Slides courtesy of Dr. Ken Bloom
An Illustrative Case (cont)

Clinical Significance of Heterogeneity???
• Perez EA, et al, Predictability of adjuvant trastuzumab benefit in N9831
patients using the ASCO/CAP HER2-positivity criteria. JNCI 2012 Jan
18;104(2):159-62
– 107 [3.7%] of 2904 patients on trial HER2 (3+) in 10-30% of tumor
10% threshold (FDA)
30% threshold (ASCO/CAP)
Conclusion:
Following the 2007
ASCO/CAP 30% criteria
for HER2 positivity would
potentially negate the
option of possible life-
saving trastuzumab
therapy for a small but
meaningful group of
patients.

• Intratumoral heterogeneity for HER2 can be seen in breast cancer by IHC and FISH – Can lead to discordant results for HER2 analysis
• Between IHC and FISH, cores vs excision, between blocks
– Easier to detect with IHC (can be used to target FISH)
• Clinical significance of heterogeneity remains unclear however: – Patients with HER2 IHC 3+ (10-30%) and FISH ratio (2-2.2)
appear to benefit from treatment with HER2-targeted therapy
• ASCO/CAP updated HER2 guideline definition for HER2+ – HER2 IHC - >10% of tumor cells with strong circumferential
membrane staining (readily appreciated at low power) – HER2/CEP17 ratio of >2, observed in a homogenous
contiguous population of at least 10% of tumor cells
Pearls of Pathology: Heterogeneity

Case #2: Repeat Testing
• 50 year-old woman, core biopsy for mass, Jan 2011
• Diagnosis: Grade 3, triple negative invasive ductal carcinoma,
positive lymphovascular invasion, negative for DCIS
Case provided by
Stephen Naber, MD, PhD

Core Biopsy IHC Markers
Estrogen Receptor HER2 (Score 1+)
• Progesterone receptor negative
• Cold ischemic and fixation times within CAP/ASCO guidelines • HER2 FISH not performed at this time

Mastectomy and Lymphadenectomy
• Primary tumor: 0.8 cm, Grade 3, triple negative (September 2011)
• 8 of 13 lymph nodes positive for metastasis
Estrogen Receptor HER2 (Score 0)
• Cold ischemic and fixation times within CAP/ASCO guidelines
• HER2 FISH not performed at this time

Contralateral Axillary Node Biopsy
Estrogen Receptor HER2 (Score 1+)
• Core needle biopsy of contralateral axillary node (Jan 2012)
• Cold ischemic and fixation times within CAP/ASCO guidelines
•HER2 FISH assay ordered: • HER2:CEP17 = 2.6 at reference lab
• HER2:CEP17 = 2.7 at hospital lab

Follow-up HER2 FISH
• HER2 FISH then performed in-house on tumor from
mastectomy: HER2:CEP17 = 2.3
• Dual ISH for HER2 performed in-house on tumor from core biopsy:
Numerous HER2 amplified
cells present
Black signals = HER2
Red signals = CEP17

HER2-Negative (1+) Breast Cancer with Unfavorable
Prognostic Features: to FISH or not to FISH? (Viale 2012)
Concordance study IHC vs FISH for
HER2
IHC Score % of case amplified
by FISH
0 3.2%
1+ 6.7%
2+ 23.9%
3+ 89.3%
Overall Concordance, IHC vs FISH
82%
• Given possible association between HER2 positive disease and unfavorable prognostic tumor characteristics
• Conducted a prospective study to assess
the incidence of HER2 gene amplification in selected tumors with adverse prognostic features scored (1+) IHC
• 492 invasive breast cancer IHC (1+)
• 84 cases selected for FISH with one or more of the following histopathologic features
– High grade, high Ki67 (>14%), LVI, LN+
– 13% these cases amplified by FISH (confidence interval 7% to 22%)
– 2 fold higher than what was observed in previous study (6.7%)
• Authors recommended considering FISH for IHC (1+) cancers with adverse prognostic features

• A new HER2 test should be considered following a HER2 negative result, if the following suspicious pathologic findings are observed
– Tumor with a high nuclear grade or Nottingham score
• A new HER2 test should not be ordered if the following histopathologic findings occur and the initial HER2 test was negative:
– Histologic grade 1 carcinoma of the following types:
• Infiltrating ductal or lobular carcinoma, grade 1, ER and PgR positive
• Tubular (at least 90% pure)
• Mucinous (at least 90% pure)
• Cribriform (at least 90% pure)
• Adenoid cystic carcinoma (90% pure) and often triple negative
2013 HER2 Testing Guidelines Update:
Histopathologic Discordance and Repeat Testing
If the pathologist or oncologist observes an apparent histopathologic discordance after HER2 testing, the need for additional HER2 testing should be discussed.

Pearls of Pathology: Repeat Testing
• Under what circumstances should you consider reflex testing an invasive breast cancer that is IHC HER2 (0) or (1+) by FISH?
– Cases with high risk, unfavorable histopathologic features
(increased likelihood of HER2+ disease)
• 50 years of age or less
• ER negative
• ER positive & PR low/negative
• High proliferative index (Ki-67 > 20%)
• Grade II or III
• Peritumoral lymphatic invasion
The yield will be low, however the magnitude of the benefit of Trastuzumab justifies dual
testing for those patients who are at increase risk of HER2+ disease. Patient’s who have a
primary (-) FISH test with these characteristic should be consider for reflex IHC testing

Clinical History Case 3: Aneusomy
• 68 year old male presents
with palpable right sided breast mass
• calcifications seen on
mammographic imaging
• US guided core needle biopsy performed

• Invasive ductal carcinoma
– Size: 2.5 cm
– Nottingham grade: 3 of 3
– LVI: Present
– Margins: Negative
– Axillary nodes: (7/31)
– ER: (+), 70% of cells, strong
– PR: (+), 5% of cells, moderate
– Ki67: 40% of cell positive
– HER2 IHC: (image on next slide)
• pT2 pN2, cMx
• Standardized tissue handling, fixation and processing was
followed
Right Breast, Mastectomy:

HER2 Immunohistochemistry
How would you interpret the HE2 IHC results? Are any further steps needed?

HER2 FISH Assay Results
HER2/CEP17 ratio 1.7
Total # of tumor cells
counted
40 + 40
Average # HER2
signals/nucleus
7.5
Average # CEP17
signals/nucleus
4.5
By ratio, this tumor would be interpreted as non-amplified. What is the
most appropriate interpretation of the HER2 status for this patient?
HER2 FISH

52
• A result like this will be confusing to clinicians (ratio <2, HER2#
>6 = amplified)
• Include a comment to help guide communication between
the clinician and patient.
– For example “Although the ratio is < 2, there are more than
6 HER2 gene signals per cell. The data indicates that this
case is HER2 amplified based on the HER2 copy number.”
Reporting Considerations – Case #3

Aneusomy of Chromosome 17
53
HER2 amplification defined by
Ratio criterion (≥2)
HER2 copy number criterion (≥6)
Both ratio and copy number
criteria
Co-amplification of CEP17 may
lead to HER2/CEP17 <2.0,
suggesting lack of HER2
amplification
If the HER2 copy number is ≥6, the
test is positive regardless of the
HER2/CEP17 ratio HER2 copy number 10.1
CEP17 copy number 7.4
HER2/CEP17 ratio 1.34
Some labs may choose to repeat HER2 testing in the same specimen and using an alternative chromosome 17 reference probe (another gene on chromosome 17 not expected to co-amplified with HER2)

Patient Communication Issues
54
• Clinicians or pathologists should understand and be able to
explain:
– Importance of tumor biologic characteristics
– Importance of HER2 testing
– Types of tissue used for HER2 testing
– Types of tests used for HER2 testing
– Various test results and their significance and requirements
for further action
– Importance of evaluating the HER2 status on each new
tumor (primary or metastasis)
– Value of guidelines being followed to assure accuracy

55
2007 Guidelines
• Initial test validation requires
25-100 samples tested by alternative validated method in the same laboratory or by validated method in another laboratory
2013 Guideline update
• Initial test validation*: 20 negative and 20 positive for FDA-approved assays and 40 negative and 40 positive for LDTs
Note: Requirement does not apply to assays that were previously validated in conformance with the 2007 HER2 testing guideline, and routinely participating in external proficiency testing for HER2 tests, such as the program offered by CAP.
*Conforms to the published 2010 ASCO/CAP Validation Recommendations for
IHC Testing of ER and PgR Guideline (Fitzgibbons, Arch Pathol and Lab Med, 2010)
2013 HER2 Testing in BC Guidelines Update:
Initial Test Validation

2013 HER2 Testing in BC Guidelines Update: Guideline Update Addresses QA
• Specimen handling
• Lab validation
• Test Interpretation
and diagnosis
• Test reporting
requirements
• Proficiency testing
• Laboratory accreditation
56
QA elements will be specified and monitored.

Pearls of Pathology: Guidelines
• Guidelines are living document which change
– From user feedback
– From new publications and data
• Iteration of guidelines leads to greater clarity
• Algorithm changes in the guideline update provide better safety
for patients
– Positive patients will be found and treated
– Equivocal patients will have further work done to better define
their HER2 status
– Negative patients will be spared unnecessary treatment
– Close scrutiny of cases by physicians (oncologists &
pathologists) will find patients with unusual situations
57

Suggested Action Items for Labs Performing HER2 Testing
(Check-List)
Review your lab’s algorithms for HER2 testing and adjust them to
fit the new guideline.
Change length of fixation policies to 72 hours maximum.
Educate other pathologists at your location about the new
interpretation criteria, look at sample cases together.
Review the issues of polysomy, monosomy and tumor heterogeneity with other pathologists and oncologists
interpreting or acting on HER2 tests at your location.
Plan how ISH slides will be optimally handled and interpreted by pathologists
58

• ASCO Guideline Disclaimer:
o “Use of the information is voluntary.”
• CAP Guideline Disclaimer:
o “…adherence to any practice guideline…is
voluntary…”
• A CAP accreditation checklist requirement is NOT
voluntary
o Checklist requirements reflect essence of
guideline but may not exactly = guideline
Guidelines vs. CAP Checklist Requirements
© 2013 College of American Pathologists. All rights reserved. 59

CAP Checklist, in contrast to Guideline
• Requirements must be
o Practical for labs to implement
o Readily evaluable by inspector
o Consistent with FDA for cleared/approved tests
• A guideline element based purely on expert
opinion may not be appropriate as a checklist
requirement
• Some details in a guideline may not be appropriate
for checklist
© 2013 College of American Pathologists. All rights reserved. 60

o Some guideline elements may be gradually
introduced as checklist requirements
− Phase I, then phase II
− Progressive changes in wording (“consider”,
“should”, “must”)
CAP Checklist, in contrast with Guideline, cont.
© 2013 College of American Pathologists. All rights reserved. 61

• ANP.22969 (II) Information on report
o Fixation, antibody clone or probe, scoring system
• ANP.22970 (II) Annual result comparison with
published benchmarks, & interobserver variability
(95% concordance)
• ANP.22973 (II) Proficiency testing
o “Interpretation-only” PT: OK for IHC…NOT for
(F)ISH!
Checklist elements applicable to HER2
© 2013 College of American Pathologists. All rights reserved. 62

• ANP.22978 (II) Validation / CYG.48399 / MOL.39323
o REVISED
• ANP.22983 (II) Fixation / CYG.48932 / MOL.39358
o REVISED
• ANP.22985 (I) Decalcified tissue
Checklist elements applicable to HER2, cont.
© 2013 College of American Pathologists. All rights reserved. 63

• ANP.22999 (II) IHC scoring
o REVISED
• ANP.23002 (II) / CYG.49465 / MOL.39393 ISH/FISH
scoring
o REVISED
• NEW: Testing on primary and metastatic lesions
o Additional testing for histologic discordance /
limited samples
Checklist Elements Applicable to HER2, cont.
© 2013 College of American Pathologists. All rights reserved. 64

• ANP.22978 (II) / CYG.48399 / MOL.39323
o 2013 checklist edition: minimum 25 cases;
recommended 25-100.
o CHANGED in 2014 to:
− 20 + / 20 neg samples for FDA
cleared/approved tests
− 40 + / 40 neg samples for lab-developed tests
o No required concordance level of new test vs
comparative test
Analytic validation
© 2013 College of American Pathologists. All rights reserved. 65

• Data should show concordance between methods
for each possible result
o IHC: 0, 1+, 2+, 3+
o (F)ISH: +, neg, indeterminate (if applicable),
equivocal [new]
• Compare new test to validated alternative method
in same lab, or same validated method in another
lab, using same set of cases
• If fixative other than 10% NBF used, must validate
with NBF-fixed samples
Analytic validation detail – 2013 checklist edition,
unchanged for 2014, except as noted below
© 2013 College of American Pathologists. All rights reserved. 66

• For previous validations not meeting the current
requirements: data from previous PT samples may
be used; or unstained slides from recent cases may
be sent to reference laboratory
o Lab should document the additional data (PT or
reference laboratory studies)
Validation – 2013 checklist edition – no change
© 2013 College of American Pathologists. All rights reserved. 67

• ANP.22983 / MOL.39358 / CYG.48932 / 2013 edition
o Current: 6 – 48 hours
o CHANGED to 6 – 72 hours for 2014 (now = ER /
PgR fixation requirement)
o Lab should communicate fixation guidelines to
clinical personnel
− Record time of tissue removal / time of
immersion in formalin
o Lab should consider monitoring compliance &
contacting clients if these guidelines not met
Fixation
© 2013 College of American Pathologists. All rights reserved. 68

• ANP.22999
o Lab uses ASCO/CAP criteria or mfg’s instructions
o NEW: Laboratories using FDA approved/cleared
tests should follow interpretation criteria in mfg
instructions, unless the lab has performed a
validation study to allow use of the ASCO/CAP
criteria
o NEW: If using ASCO/CAP criteria, report indicates
year of guideline publication
IHC Scoring – additional wording for 2014 edition
as noted below
© 2013 College of American Pathologists. All rights reserved. 69

• Specific IHC scoring not in checklist, but guideline is
referenced:
o Current positive: > 30% invasive tumor cells
stained
o CHANGED to: positive is > 10% of invasive tumor
cells stained
o Intense, complete staining in >10% and <= 30% is
rare (as few as 0.15% of patients)
IHC scoring
© 2013 College of American Pathologists. All rights reserved. 70

• Equivocal…= 2+: complete weak or nonuniform
circumferential membrane staining in >= 10% of
cells; OR intense, complete staining in <= 30% of
cells Order F(ISH)
• Negative…= 0 and 1+, 0 = no staining; 1+ = weak,
incomplete membrane staining in any % of cells
IHC Scoring, 1st edition of Guideline
© 2013 College of American Pathologists. All rights reserved. 71

• Positive HER2 = 3+
o Circumferential, intense, complete membrane
staining in > 10% of invasive tumor cells
• Equivocal HER2 = 2+
o Incomplete and/or weak/moderate
circumferential staining in >10 % of cells OR
o Complete, intense, circumferential staining in
<= 10% of cells
o Order (F)ISH
New Guideline: IHC Scoring (Referenced in
Checklist)
© 2013 College of American Pathologists. All rights reserved. 72

• Negative HER2: = 1+ or 0
o 1+: faint, incomplete membrane staining in >10%
of cells
o 0: no staining, or faint, incomplete membrane
staining in <= 10% of cells
New Guideline, IHC Scoring, cont.
© 2013 College of American Pathologists. All rights reserved. 73

• ANP.23002 / CYG.49465 / MOL.39393
o Current, with internal control probe:
− + HER2/CEP17 > 2.2, neg HER2/CEP17 < 1.8
− Equivocal: ratio 1.8 – 2.2
o Current, no internal control probe
− +: > 6 signals/nucleus; neg: < 4 signals/nucleus
− Equivocal: 4-6 signals/nucleus
ISH scoring…current 2013 checklist
© 2013 College of American Pathologists. All rights reserved. 74

• Positive: HER2/CEP17 >= 2.0 or average HER2 copy
number >= 6.0 signals / cell
• Negative:
o Dual probe: HER2/CEP17 < 2.0 and average HER2
copy number < 4.0 signals / cell
o Single probe: avg. <4.0 signals/cell
• Equivocal:
o Dual probe: HER2/CEP17 < 2.0 with avg. HER2
copy no. >= 4.0 and < 6.0 signals / cell
o Single probe: avg. copy no. >=4.0 and < 6.0
REVISED ISH scoring for 2014 (in checklists ANP,
CYG, MOL):
© 2013 College of American Pathologists. All rights reserved. 75

• ADDITION: Variable positivity (tumor heterogeneity)
in (F)ISH testing
o Scan ISH slides at low power
o If there is subpopulation of >=10% of tumor cells
with amplified HER2: report case as HER2-positive
o Count at least 20 cells in the subpopulation
• No change: For FDA cleared/approved tests
without an equivocal category, follow mfg.
instructions
Revised ISH Scoring (in ANP, CYG, MOL), cont.:
© 2013 College of American Pathologists. All rights reserved. 76

• At least one tumor sample from all patients (early-
stage, recurrent or metastatic disease) is tested for
either HER2 protein expression (IHC) or HER2 gene
expression ([F]ISH)) using a validated HER2 test if
tissue is available.
NEW checklist element for 2014 – Phase I
© 2013 College of American Pathologists. All rights reserved. 77

• Repeat HER2 test for:
o Histologic discordance (ex., + test, Gr I ER+/Pgr+
tumor)
o Core biopsy—repeat test on excisional spec. if:
− Negative test with limited amount of tumor in
core
− Equivocal test by IHC and ISH
Note to NEW checklist element for 2014 – Phase I,
cont.
© 2013 College of American Pathologists. All rights reserved. 78

• “Practical Issues in Surgical Pathology that Enhance
Ancillary Molecular Testing”
o January 23 at 11 am Central
o Presented by John Pfeifer, MD, PhD, FCAP
• “Molecular and Diagnosis of Respiratory Viruses”
o February 27 at 10 am Central
o Presented by Frederick L Kiechle MD, PhD, FCAP
View all past webinars by going to www.cap.org/webinars
Upcoming Free Webinars
© 2013 College of American Pathologists. All rights reserved. 79

• Pathology SPECs are:
o short PowerPoint presentations, created for pathologists, focused on
selected diseases where molecular tests play a key role in patient
management.
o valuable resource for your discussions with Tumor Boards or other
physician colleagues.
• Now Available:
― Emerging Concepts in the Diagnosis of Respiratory Viruses (NEW)
― Emerging Concepts in Molecular Testing in Breast Cancer (NEW)
― Emerging Concepts in the Workup of Colorectal Cancer
― Emerging Concepts in Therapeutic Guidance for Metastatic Melanoma
― Emerging Concepts in the Diagnosis and Workup of Thyroid Cancer
― Emerging Concepts in Colorectal Cancer Hereditary Non-Polyposis
Cancer (Lynch Syndrome)
― Emerging Concepts in the Workup of Polycythemia and
Thrombocythemia: JAK2
To register, go to the CAP Member tab on cap.org 80
Short Presentations on Emerging Concepts
(SPECS)

The CAP has created the Pathology Resource Guides, a tool
(updated Oct 2013) to assist pathologists in understanding key
emerging technologies. These Resource Guides are a CAP member
benefit available at no charge.
Molecular Pathology (single gene, small panel)
Genomic Analysis (large panels, exome, genome)
Digital Pathology
In Vivo Microscopy
Register through the CAP member tab. Once registered, you will be
notified when a new issue is released.
Questions? Contact [email protected].
CAP’s Pathology Resource Guides
81 © 2013 College of American Pathologists. All rights reserved.

CAP Learning – HER2 Revision by ASCO and CAP
82
Course Learning Objectives
ASCO/CAP HER2 Guidelines
CE/CME/SAM – 0.0
Recommendations in the 2007 ASCO/CAP Guideline for HER2 Testing have
been reconciled with the April 2010 ASCO/CAP ER PgR Guideline so that
cancer specimens will be handled in a uniform manner for ER, PgR and HER2 in
breast cancer specimens.
Genomic Aberrations in Salivary
Duct Carcinoma Arising in
Warthin Tumor of Parotid Gland:
DNA Microarray and HER2
Fluorescence In Situ Hybridization
CE/CME/SAM – 0.0
Carcinoma arising from Warthin tumor is extremely rare. A 79-year-old man was
admitted for a firm, well-defined, 5-cm left infra-auricular mass. Aspiration
cytology showed many lymphohistiocytes and oncocytes in a proteinaceous
background, compatible with Warthin tumor. A left superficial parotidectomy
showed a solid mass around the cyst wall. The tumor cells of the solid area were
arranged as infiltrative ducts with a few foci of malignant transformation. Virtual
karyotyping disclosed a complex pattern of genetic aberrations with a focal
amplification in 12q14–q21.2. This chromosomal region contains the MDM2
(murine double minute) gene, which regulates p53 inactivation. HER2
fluorescence in situ hybridization showed a focal amplification. Subsequently,
the patient underwent total parotidectomy and ipsilateral neck dissection for a
recurrence. To our knowledge, this is the first case of salivary duct carcinoma
arising from Warthin tumor. The essential molecular pathway has not been
reported, we presume an important role of MDM2 amplification–P53
inactivation.
© 2013 College of American Pathologists. All rights reserved.

CAP Learning – HER2 Revision by ASCO and CAP
83
Course Learning Objectives
Herceptin HER2+ Breast Cancer
Treatment Information
CE/CME/SAM – 0.0
Herceptin is approved for the treatment of early-stage breast cancer that is
Human Epidermal growth factor Receptor 2-positive (HER2+) and has spread
into the lymph nodes, or is HER2+ and has not spread into the lymph nodes. If it
has not spread into the lymph nodes, the cancer needs to be estrogen
receptor/progesterone receptor (ER/PR)-negative or have one high risk feature.
Standardized Assessment of the
HER2 Status in Breast Cancer by
Immunohistochemistry
CE/CME/SAM – 0.0
Immunohistochemistry (IHC) is widely used in surgical pathology, but it has been
plagued by problems with reproducibility and lack of standardization resulting
in poor concordance between laboratories. In particular, inaccuracy of routine
human epidermal growth factor receptor 2 (HER2) testing in breast cancer
patients has been a major issue. In 2006 this led the American Society of
Clinical Oncologists (ASCO) and College of American Pathologists (CAP) to
charge an expert panel with developing recommendations for HER2 testing.
After subsequent publication and adoption of these guideline
recommendations through dissemination of best practices, variation in clinical
practice is expected to diminish and result in improved accuracy.
In this article, we review the role of genomic HER2 alterations in the
development and treatment of breast cancer, highlight the importance of
accurate and reproducible HER2 testing, and discuss practical approaches to
standardize HER2 testing by IHC. Pre-analytic and analytic variables are
addressed, and a practical algorithm for test interpretation is introduced.
© 2013 College of American Pathologists. All rights reserved.

CAP Learning Portal
84
CAP Learning Portal
• The CAP Learning Portal includes content and tools designed to support the learning needs of pathologists . A user must login to cap.org in order to access the portal. In the portal, you will find: o Learning Options search/catalog
o Competency Model for Pathologists
o Personal Progress Check
o My Learning Plan
o Help Center (Guides, Video, FAQs)
• Benefits Increase effectiveness to plan and manage learning
Increase efficiency to target learning needs and identify premium learning solutions Increase satisfaction with learning solutions that meet specific learner needs Increase capability to maintain professional certifications
© 2013 College of American Pathologists. All rights reserved.

To learn more…
85
• For more details and to register for/access educational offerings:
1. Log in to the cap.org website
2. Click on the “Learning Portal” tab.
3. Click on the “Browse Our Learning Catalog” tab
4. Type your desired topic in the “Search” box or make a selection from the list provided.
A list of available learning options displays
© 2013 College of American Pathologists. All rights reserved.


© 2013 College of American Pathologists. All rights reserved.

THANK YOU!
Thank you for attending our webinar
““HER2 Testing Revision” by David G. Hicks, MD, FCAP and
Stephen J. Sarewitz, MD, FCAP
For comments about this webinar
or suggestions for upcoming
webinars, please contact
Jill Kaufman, PhD,
Director of Personalized Health Care at [email protected]
NOTE: There is no CME/CE credit available for
today’s free webinar.
88