Embed Size (px)
Citation preview

Welcome to
• five inpatient hospitals:
• Tisch Hospital
• Rusk Rehabilitation
• NYU Langone Orthopedic Hospital
• NYU Langone Hospital - Brooklyn
• Hassenfeld Childrens Hospital
• with locations in
• New York City’s five boroughs
• Long Island
• New Jersey
• Westchester, Putnam, and Dutchess counties
• affiliation with
• Winthrop University Hospital
Over 200ambulatory sites

THE JOINT
COMMISSIONNATIONAL QUALITY APPROVAL
Ranked #1 & #2 – Third
Year in a Row for Overall
Patient Safety & Quality
140 Physicians Listed in
New York Magazine’s
“Best Doctors”
Gold Seal of Approval by
the Joint Commission for
Commitment to High
Quality Care
Magnet Recognized
Hospital for Excellence
in Nursing
Clinical Care
Modern
Healthcare
Modern Healthcare
Top HospitalMost Wired Hospital -
2017

RESEARCH
#1 in licensing
revenue among U.S.
universities
A Top 11
U.S. News & World
Report’s Best
Medical School
$189 million
in new NIH
funding for 2016
435 research
faculty
Among the
fastest growing
NIH portfolios
in the U.S.
4,187 peer reviewed
publications as of
2016
Education
175 Years of Training Physicians and Scientists
75+ Residency and Fellowship Training Programs
5,000 Voluntary, full and part-time faculty
3 -year medical degree program
80 MD/PhD students
233PhD Students
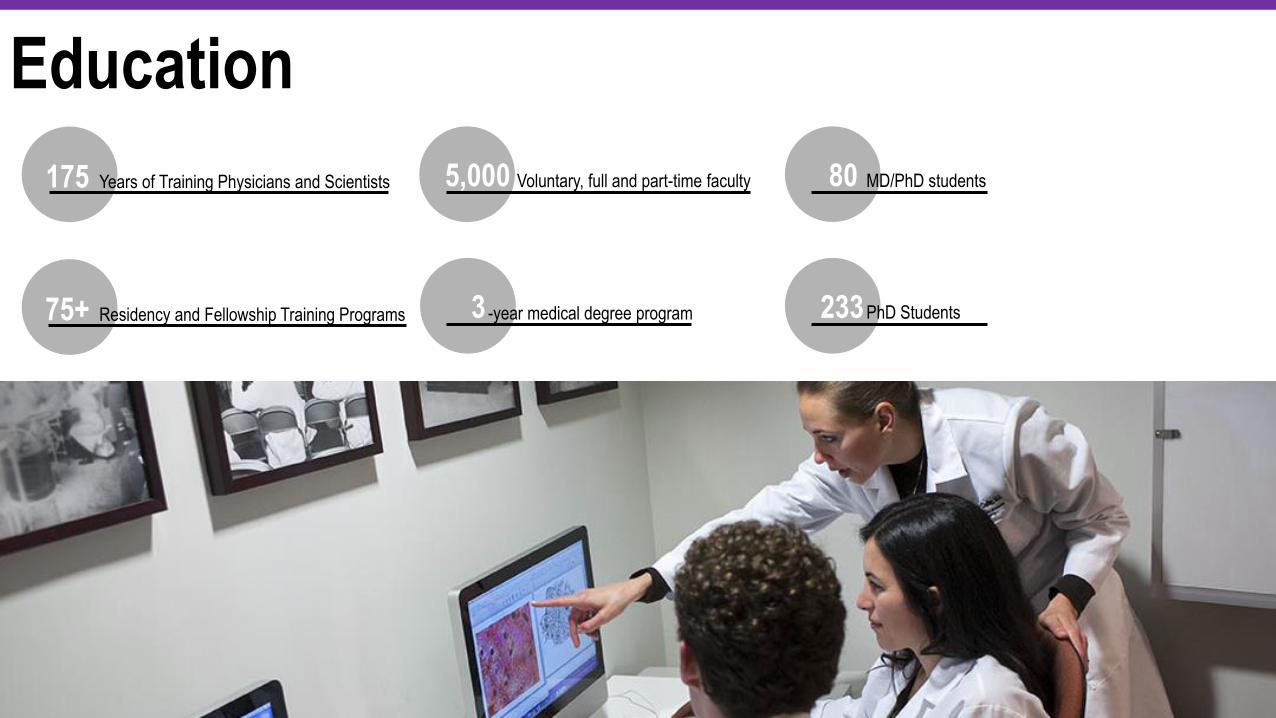
Stage 7
Stage 7 Non-Stage 7
4% of over 5,000
hospitals
evaluated are
Stage 7
Healthcare Information and Management Systems Society (HIMSS) Analytics Electronic
Medical Records (EHR) Adoption Model
Stage 7 Award.
Leverage and govern health data and analytics
Execute computer order entry and electronic documentation
Measure and analyze patient engagement
Demonstrate advanced implementation
and augmentation of EHR
only
Based On Ability To
we’ve achieved

Top 20 in the Nationwith 12 nationally ranked and
8 high performing specialties
Frank Volpicelli, MD
Chief of Medicine, NYU Langone Hospital – Brooklyn
Clinical Lead Value Based Management
Jonathan Austrian, MD
Medical Director, Inpatient Clinical Informatics, NYU Langone Health
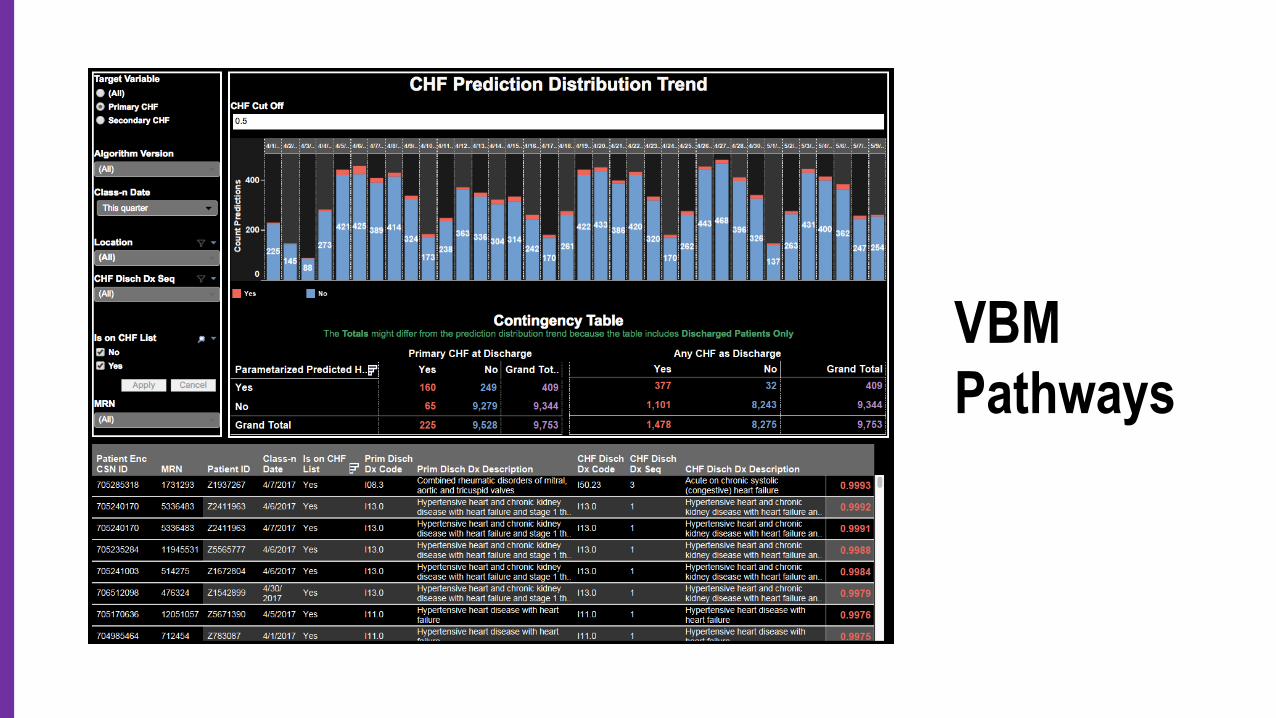
VBM Pathways

166%
210%
0%
50%
100%
150%
200%
250%
FY10 FY11 FY12 FY13 FY14 (6-month annualized)
% Increase in Medicare Loss Since 2010Inpatient & Outpatient Inpatient Only
In 2014, our Inpatient Medicare Loss was increasing
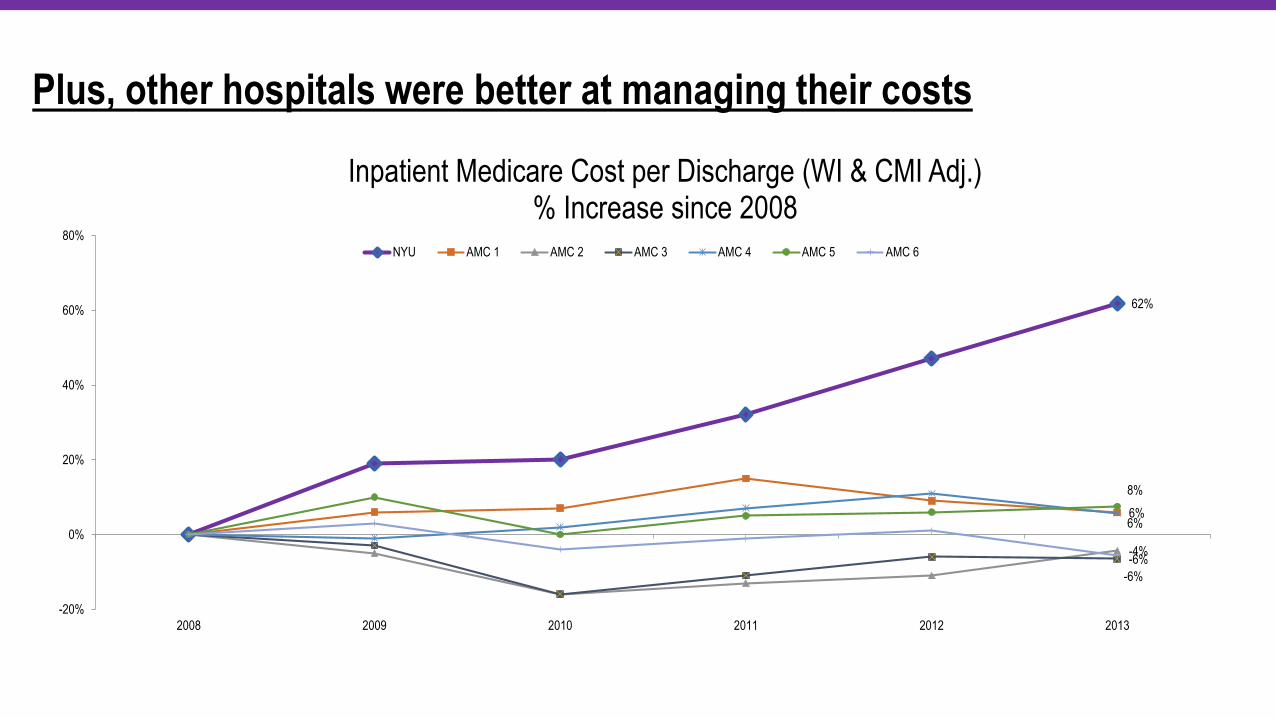
62%
6%
-4%-6%
6%
8%
-6%
-20%
0%
20%
40%
60%
80%
2008 2009 2010 2011 2012 2013
Inpatient Medicare Cost per Discharge (WI & CMI Adj.) % Increase since 2008
NYU AMC 1 AMC 2 AMC 3 AMC 4 AMC 5 AMC 6
Plus, other hospitals were better at managing their costs
Value
Based
Management
Value =Quality
Cost
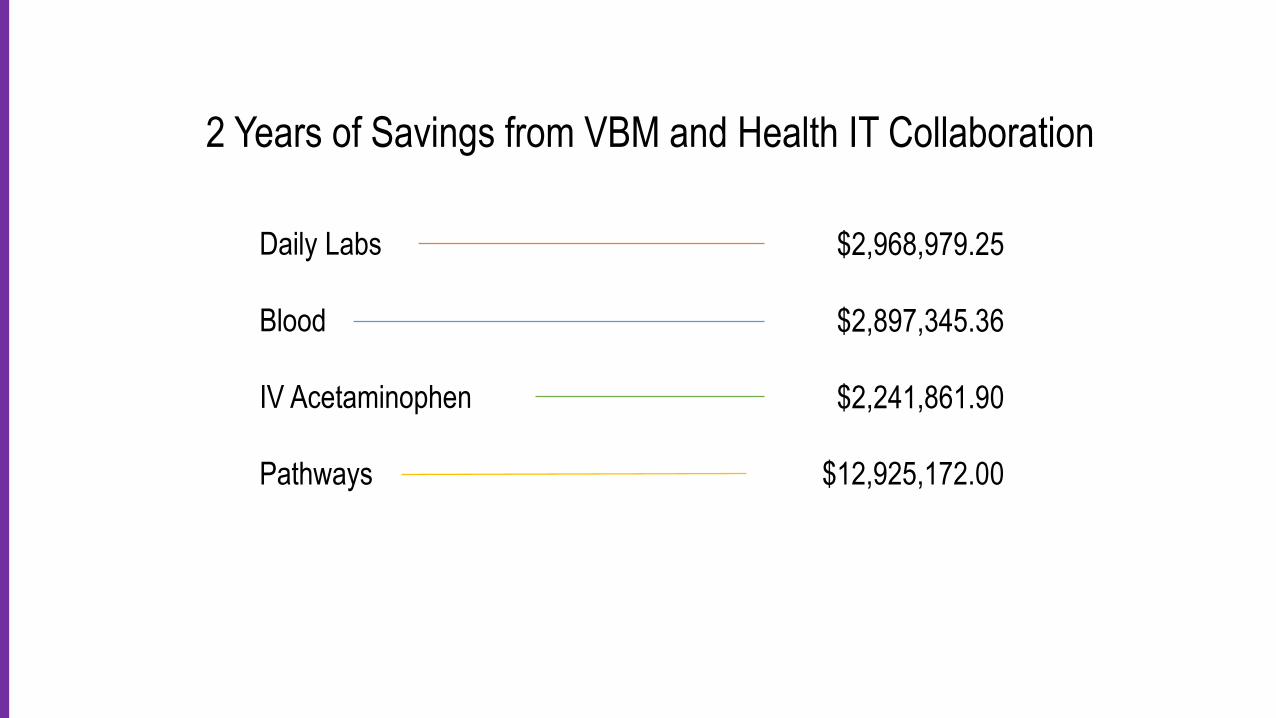
2 Years of Savings from VBM and Health IT Collaboration
Daily Labs
Blood
IV Acetaminophen
Pathways
Daily Labs
Blood
IV Acetaminophen
Pathways
$2,968,979.25
$2,897,345.36
$2,241,861.90
$12,925,172.00
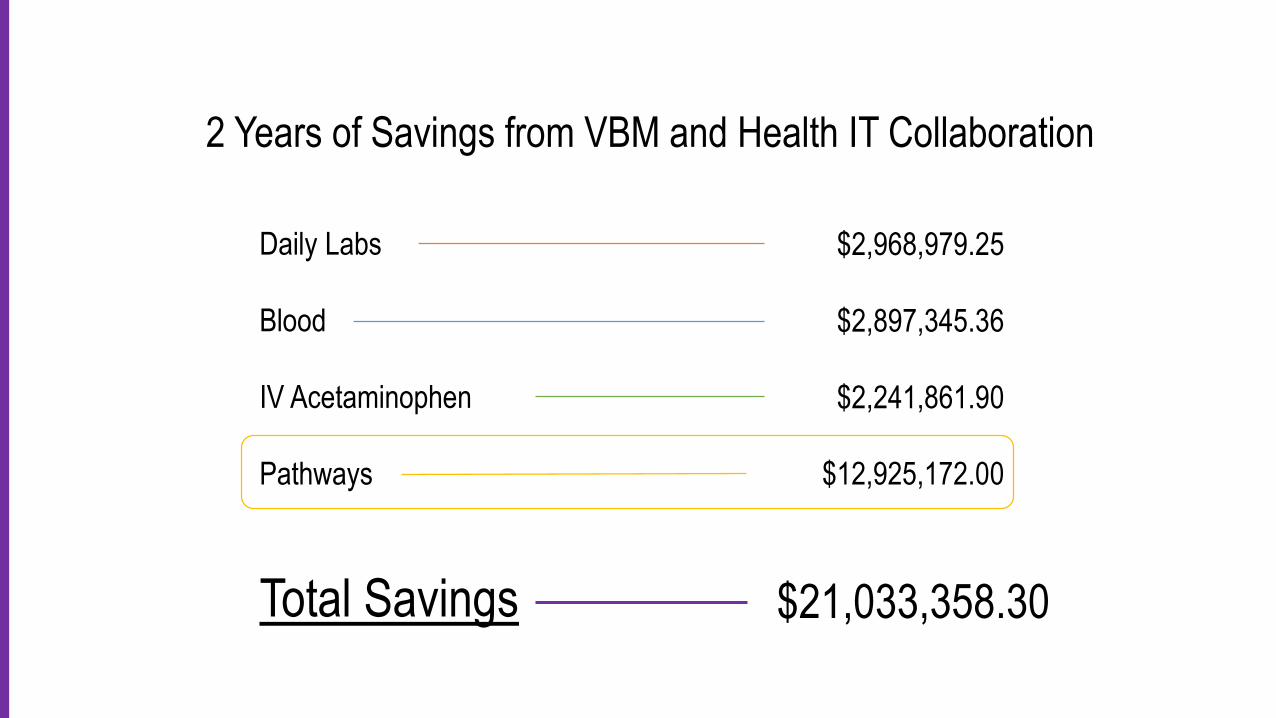
2 Years of Savings from VBM and Health IT Collaboration

Total Savings $21,033,358.30
Daily Labs
Blood
IV Acetaminophen
Pathways
$2,968,979.25
$2,897,345.36
$2,241,861.90
$12,925,172.00
2 Years of Savings from VBM and Health IT Collaboration
Total Savings $21,033,358.30
Daily Labs
Blood
IV Acetaminophen
Pathways
$2,968,979.25
$2,897,345.36
$2,241,861.90
$12,925,172.00
2 Years of Savings from VBM and Health IT Collaboration

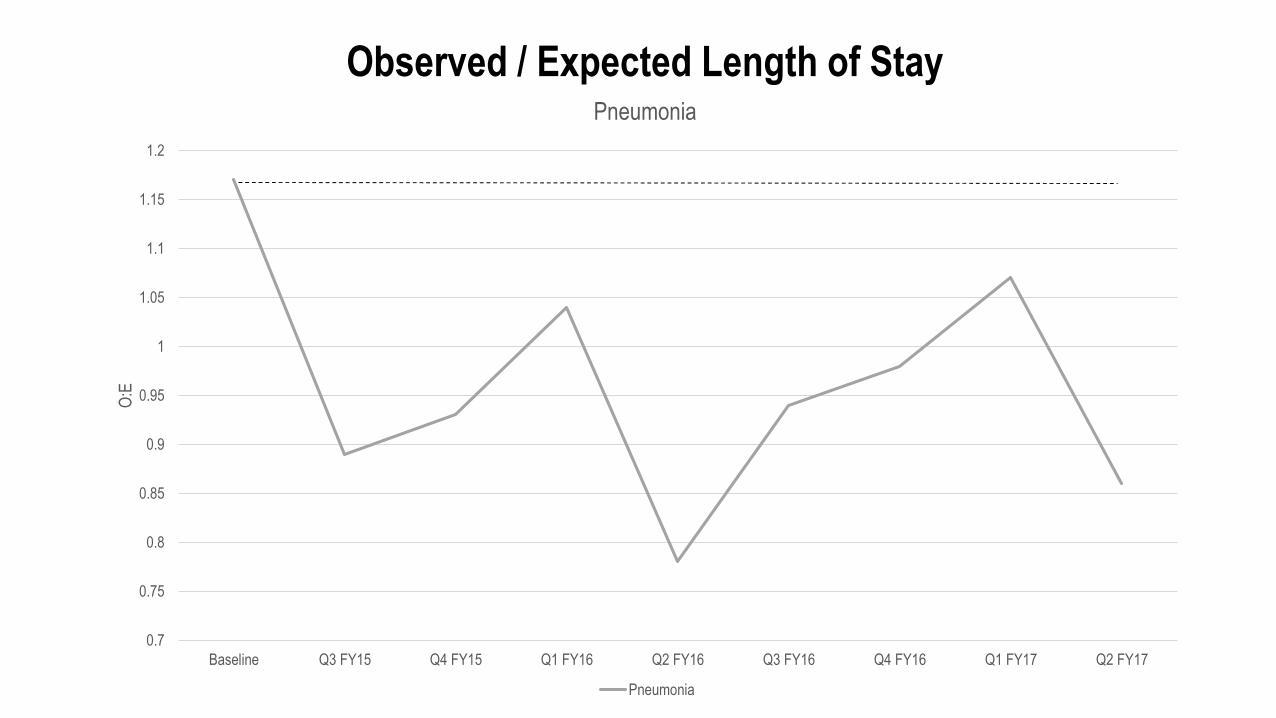
Pneumonia
Heart Failure
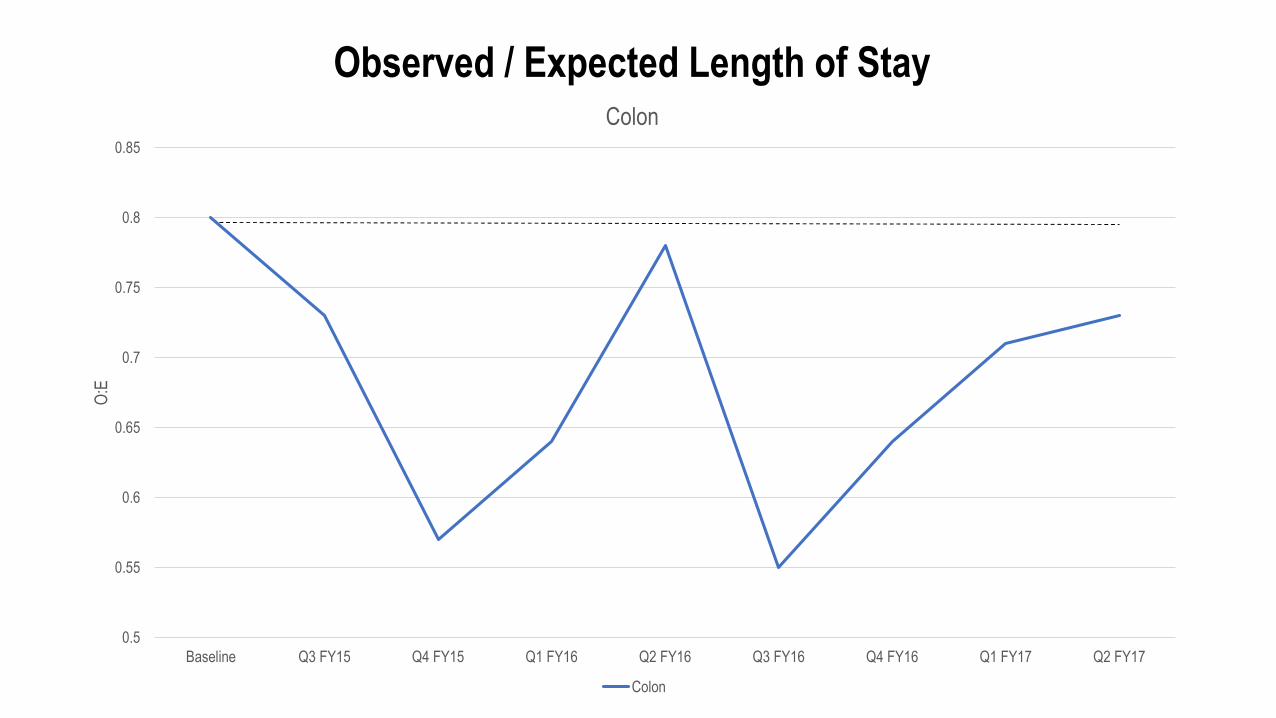
Colon Surgery
Baseline
Pathway
Data
O/E – 1.17
O/E – 1.16
O/E – 0.8
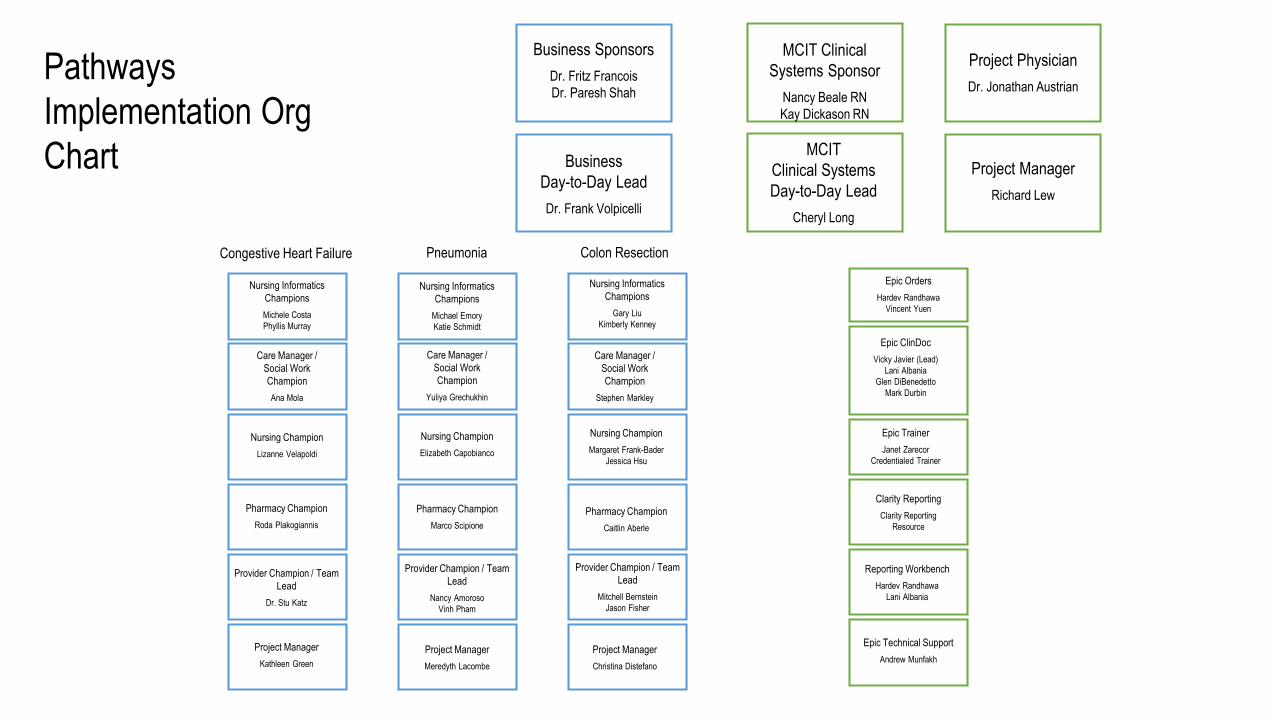
Business Sponsors
Dr. Fritz Francois
Dr. Paresh Shah
Business
Day-to-Day Lead
Dr. Frank Volpicelli
Nursing Informatics
Champions
Michele Costa
Phyllis Murray
Care Manager /
Social Work
Champion
Ana Mola
Nursing Champion
Lizanne Velapoldi
Pharmacy Champion
Roda Plakogiannis
Provider Champion / Team
Lead
Dr. Stu Katz
Project Manager
Kathleen Green
Nursing Informatics
Champions
Michael Emory
Katie Schmidt
Care Manager /
Social Work
Champion
Yuliya Grechukhin
Nursing Champion
Elizabeth Capobianco
Pharmacy Champion
Marco Scipione
Provider Champion / Team
Lead
Nancy Amoroso
Vinh Pham
Project Manager
Meredyth Lacombe
Nursing Informatics
Champions
Gary Liu
Kimberly Kenney
Care Manager /
Social Work
Champion
Stephen Markley
Nursing Champion
Margaret Frank-Bader
Jessica Hsu
Pharmacy Champion
Caitlin Aberle
Provider Champion / Team
Lead
Mitchell Bernstein
Jason Fisher
Project Manager
Christina Distefano
Congestive Heart Failure Pneumonia Colon Resection
Project Physician
Dr. Jonathan Austrian
Project Manager
Richard Lew
Epic Orders
Hardev Randhawa
Vincent Yuen
Epic ClinDoc
Vicky Javier (Lead)
Lani Albania
Glen DiBenedetto
Mark Durbin
Epic Trainer
Janet Zarecor
Credentialed Trainer
Clarity Reporting
Clarity Reporting
Resource
Reporting Workbench
Hardev Randhawa
Lani Albania
Epic Technical Support
Andrew Munfakh
Pathways
Implementation Org
Chart
MCIT Clinical
Systems Sponsor
Nancy Beale RN
Kay Dickason RN
MCIT
Clinical Systems
Day-to-Day Lead
Cheryl Long
Nursing Informatics
Champions
Michele Costa
Phyllis Murray
Care Manager /
Social Work
Champion
Ana Mola
Nursing Champion
Lizanne Velapoldi
Pharmacy Champion
Roda Plakogiannis
Provider Champion / Team
Lead
Dr. Stu Katz
Project Manager
Kathleen Green
Nursing Champion
Elizabeth Capobianco
Pharmacy Champion
Marco Scipione
Provider Champion / Team
Lead
Nancy Amoroso
Vinh Pham
Project Manager
Meredyth Lacombe
Nursing Informatics
Champions
Gary Liu
Kimberly Kenney
Care Manager /
Social Work
Champion
Stephen Markley
Nursing Champion
Margaret Frank-Bader
Jessica Hsu
Pharmacy Champion
Caitlin Aberle
Provider Champion / Team
Lead
Mitchell Bernstein
Jason Fisher
Project Manager
Christina Distefano
Care Manager /
Social Work
Champion
Yuliya Grechukhin
Nursing Informatics
Champions
Michael Emory
Katie Schmidt
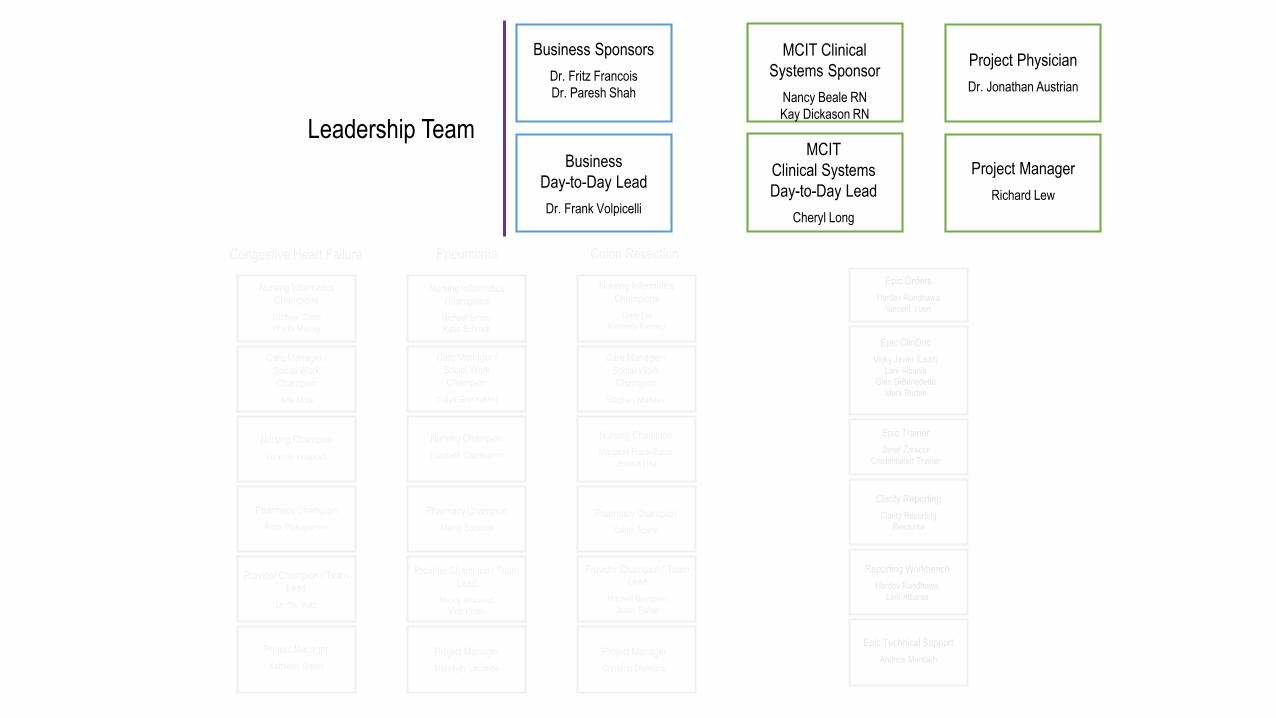
Business Sponsors
Dr. Fritz Francois
Dr. Paresh Shah
Business
Day-to-Day Lead
Dr. Frank Volpicelli
Project Physician
Dr. Jonathan Austrian
Project Manager
Richard Lew
MCIT Clinical
Systems Sponsor
Nancy Beale RN
Kay Dickason RN
MCIT
Clinical Systems
Day-to-Day Lead
Cheryl Long
Leadership Team
Epic Orders
Hardev Randhawa
Vincent Yuen
Epic ClinDoc
Vicky Javier (Lead)
Lani Albania
Glen DiBenedetto
Mark Durbin
Epic Trainer
Janet Zarecor
Credentialed Trainer
Clarity Reporting
Clarity Reporting
Resource
Reporting Workbench
Hardev Randhawa
Lani Albania
Epic Technical Support
Andrew Munfakh
Congestive Heart Failure Pneumonia Colon Resection
Business Sponsors
Dr. Fritz Francois
Dr. Paresh Shah
Business
Day-to-Day Lead
Dr. Frank Volpicelli
Nursing Informatics
Champions
Michele Costa
Phyllis Murray
Care Manager /
Social Work
Champion
Ana Mola
Nursing Champion
Lizanne Velapoldi
Pharmacy Champion
Roda Plakogiannis
Provider Champion / Team
Lead
Dr. Stu Katz
Project Manager
Kathleen Green
Nursing Informatics
Champions
Michael Emory
Katie Schmidt
Care Manager /
Social Work
Champion
Yuliya Grechukhin
Nursing Champion
Elizabeth Capobianco
Pharmacy Champion
Marco Scipione
Provider Champion / Team
Lead
Nancy Amoroso
Vinh Pham
Project Manager
Meredyth Lacombe
Nursing Informatics
Champions
Gary Liu
Kimberly Kenney
Care Manager /
Social Work
Champion
Stephen Markley
Nursing Champion
Margaret Frank-Bader
Jessica Hsu
Pharmacy Champion
Caitlin Aberle
Provider Champion / Team
Lead
Mitchell Bernstein
Jason Fisher
Project Manager
Christina Distefano
Congestive Heart Failure Pneumonia Colon Resection
Project Physician
Dr. Jonathan Austrian
Project Manager
Richard Lew
Epic Orders
Hardev Randhawa
Vincent Yuen
Epic ClinDoc
Vicky Javier (Lead)
Lani Albania
Glen DiBenedetto
Mark Durbin
Epic Trainer
Janet Zarecor
Credentialed Trainer
Clarity Reporting
Clarity Reporting
Resource
Reporting Workbench
Hardev Randhawa
Lani Albania
Epic Technical Support
Andrew Munfakh
MCIT Clinical
Systems Sponsor
Kay Dickason
MCIT
Clinical Systems
Day-to-Day Lead
Cheryl Long
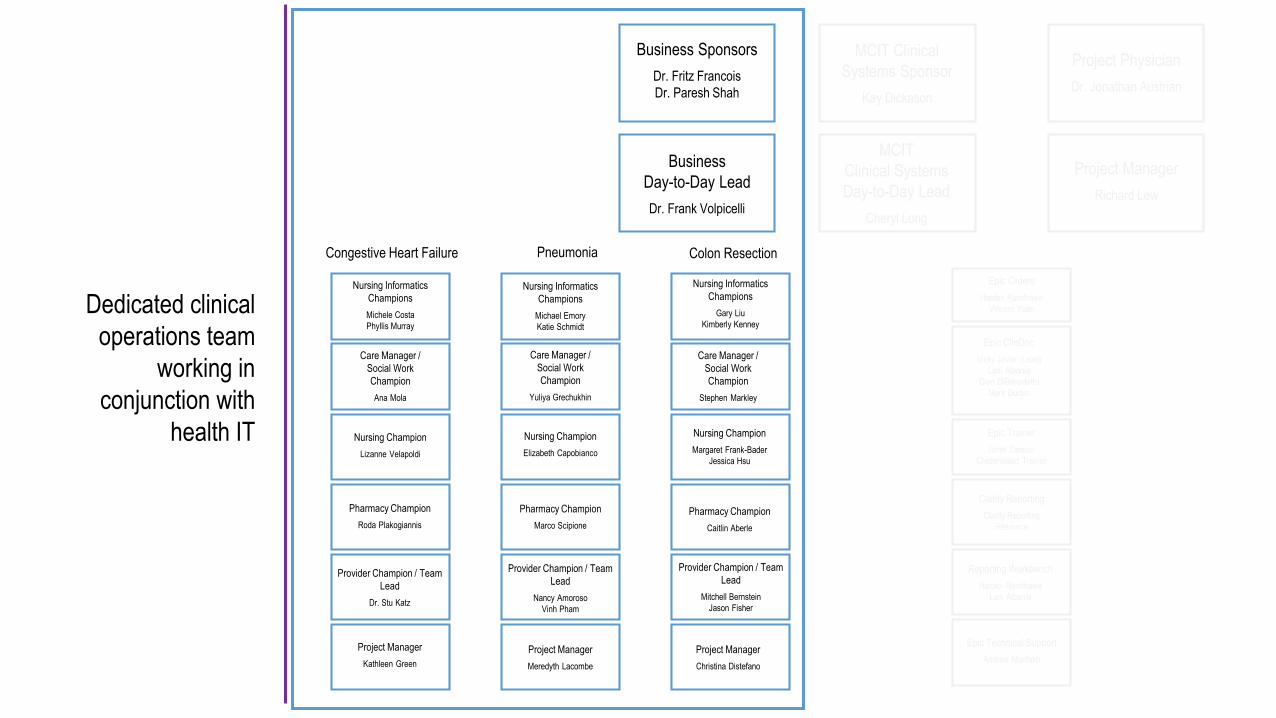
Dedicated clinical
operations team
working in
conjunction with
health IT
Business Sponsors
Dr. Fritz Francois
Dr. Paresh Shah
Business
Day-to-Day Lead
Dr. Frank Volpicelli
Nursing Informatics
Champions
Michele Costa
Phyllis Murray
Care Manager /
Social Work
Champion
Ana Mola
Nursing Champion
Lizanne Velapoldi
Pharmacy Champion
Roda Plakogiannis
Provider Champion / Team
Lead
Dr. Stu Katz
Project Manager
Kathleen Green
Nursing Champion
Elizabeth Capobianco
Pharmacy Champion
Marco Scipione
Provider Champion / Team
Lead
Nancy Amoroso
Vinh Pham
Project Manager
Meredyth Lacombe
Nursing Informatics
Champions
Gary Liu
Kimberly Kenney
Care Manager /
Social Work
Champion
Stephen Markley
Nursing Champion
Margaret Frank-Bader
Jessica Hsu
Pharmacy Champion
Caitlin Aberle
Provider Champion / Team
Lead
Mitchell Bernstein
Jason Fisher
Project Manager
Christina Distefano
MCIT Clinical
Systems Sponsor
Nancy Beale RN
Kay Dickason RN
MCIT
Clinical Systems
Day-to-Day Lead
Cheryl Long
Project Physician
Dr. Jonathan Austrian
Project Manager
Richard Lew
Epic Orders
Hardev Randhawa
Vincent Yuen
Epic ClinDoc
Vicky Javier (Lead)
Lani Albania
Glen DiBenedetto
Mark Durbin
Epic Trainer
Janet Zarecor
Credentialed Trainer
Clarity Reporting
Clarity Reporting
Resource
Reporting Workbench
Hardev Randhawa
Lani Albania
Epic Technical Support
Andrew Munfakh
Congestive Heart Failure Pneumonia Colon Resection
Care Manager /
Social Work
Champion
Yuliya Grechukhin
Nursing Informatics
Champions
Michael Emory
Katie Schmidt
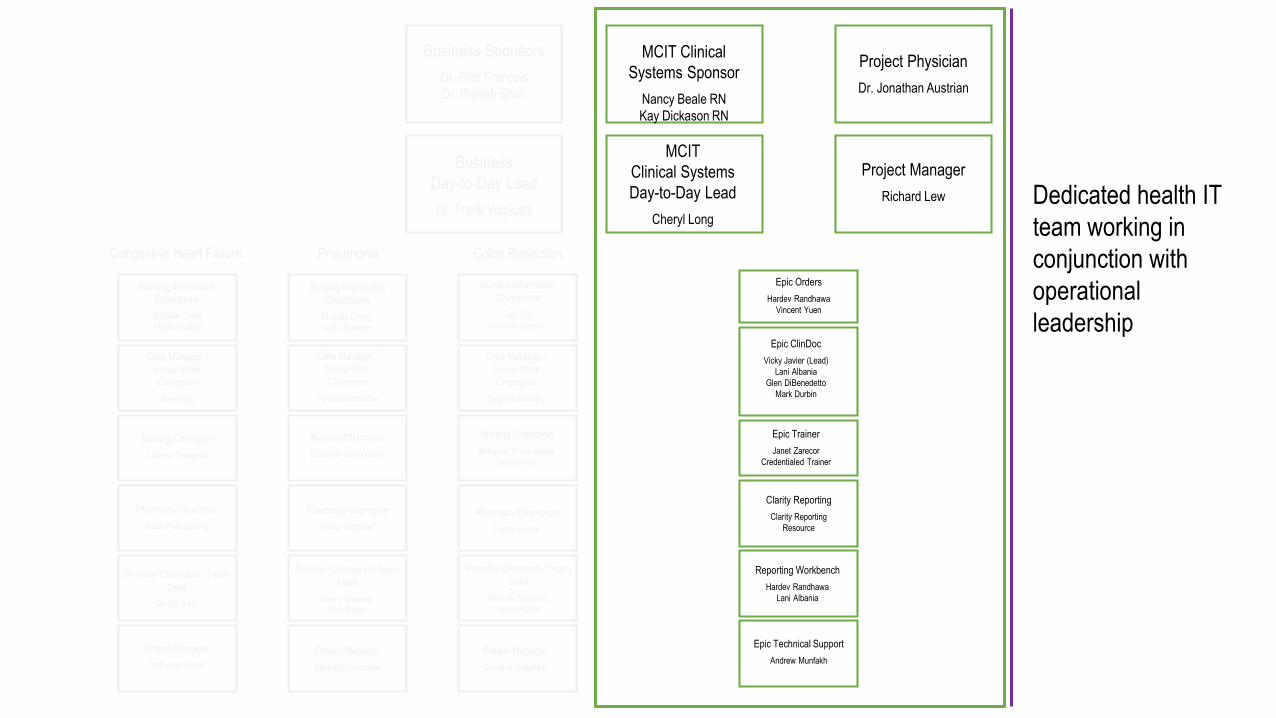
Dedicated health IT
team working in
conjunction with
operational
leadership
Formal project charter with cross-
institutional buy-in

Document approval with
cross-departmental
stakeholder buy-in
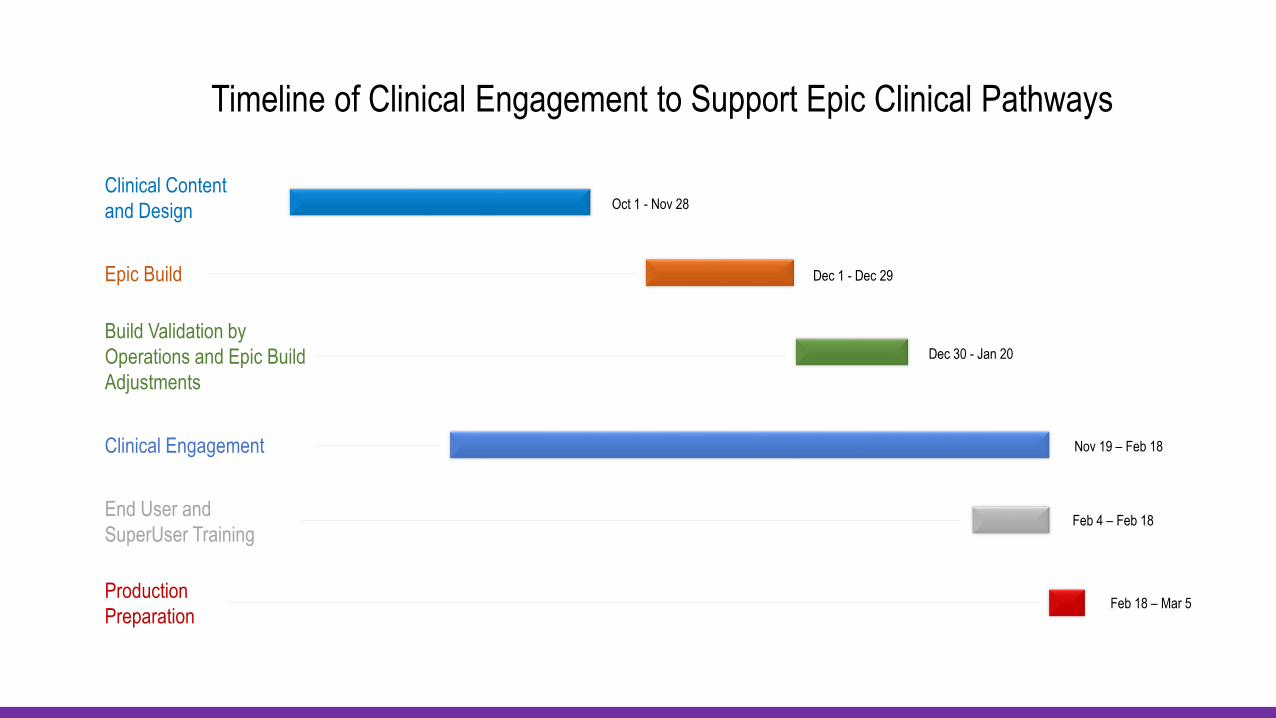
Timeline of Clinical Engagement to Support Epic Clinical Pathways
Production
Preparation
End User and
SuperUser Training
Clinical Engagement
Build Validation by
Operations and Epic Build
Adjustments
Dec 30 - Jan 20
Epic Build Dec 1 - Dec 29
Clinical Content
and Design Oct 1 - Nov 28
Nov 19 – Feb 18
Feb 4 – Feb 18
Feb 18 – Mar 5
Decision
strategy
IT Intervention
Selection ProcessGuiding
Principlesa. b. c.
Workflow Development
Guiding Principles
Start with Barriers
Interdisciplinary
Consistency amongst Pathways
Keep it simple
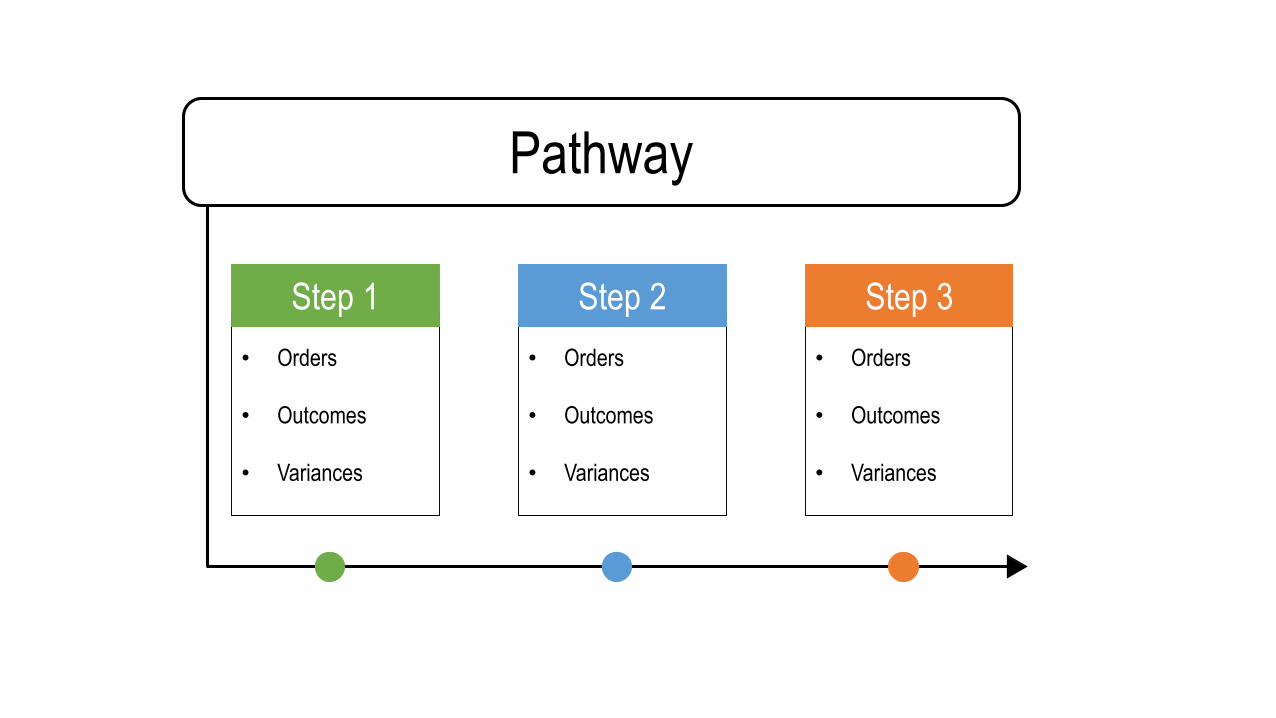
Pathway
• Orders
• Outcomes
• Variances
• Orders
• Outcomes
• Variances
• Orders
• Outcomes
• Variances
Step 1 Step 2 Step 3
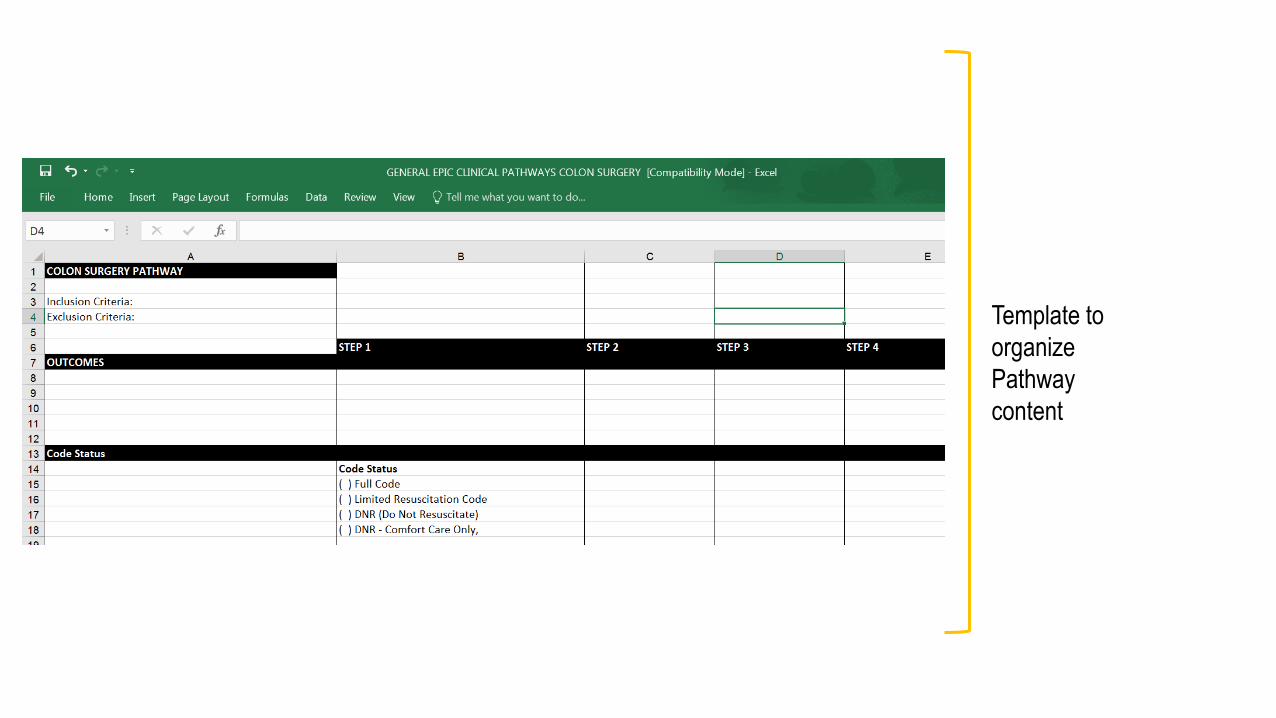
Template to
organize
Pathway
content
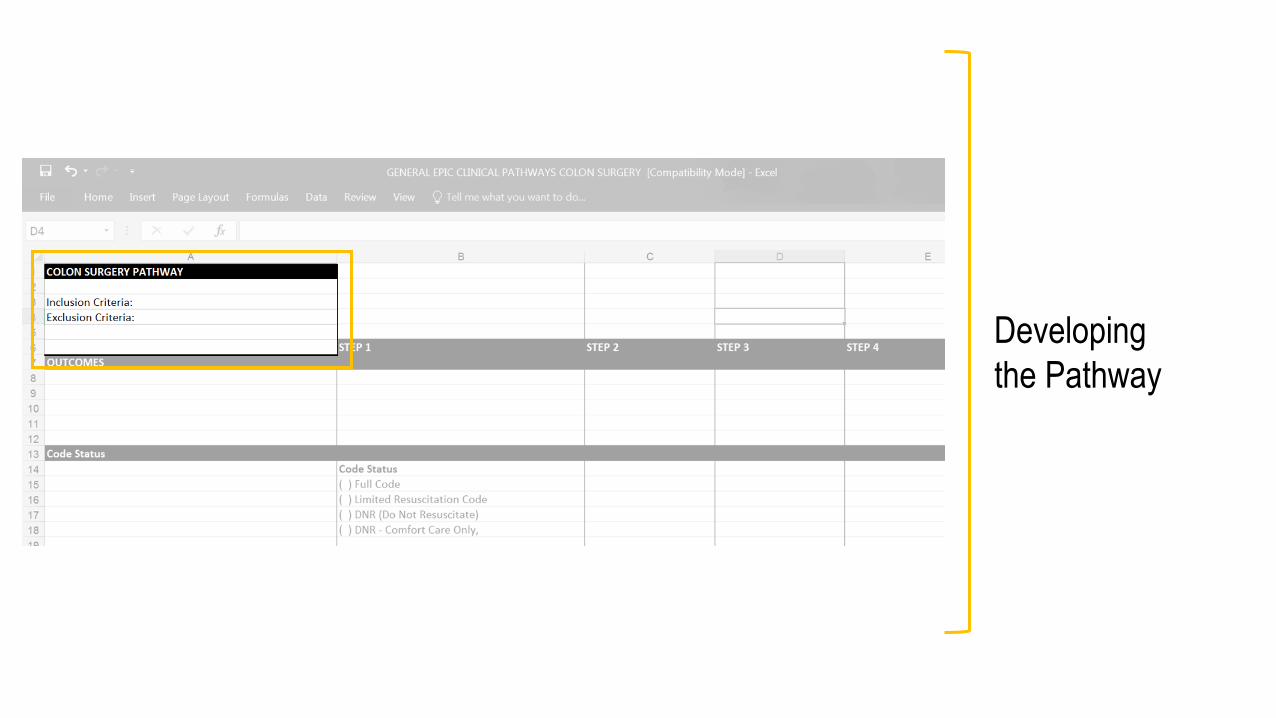
Developing
the Pathway
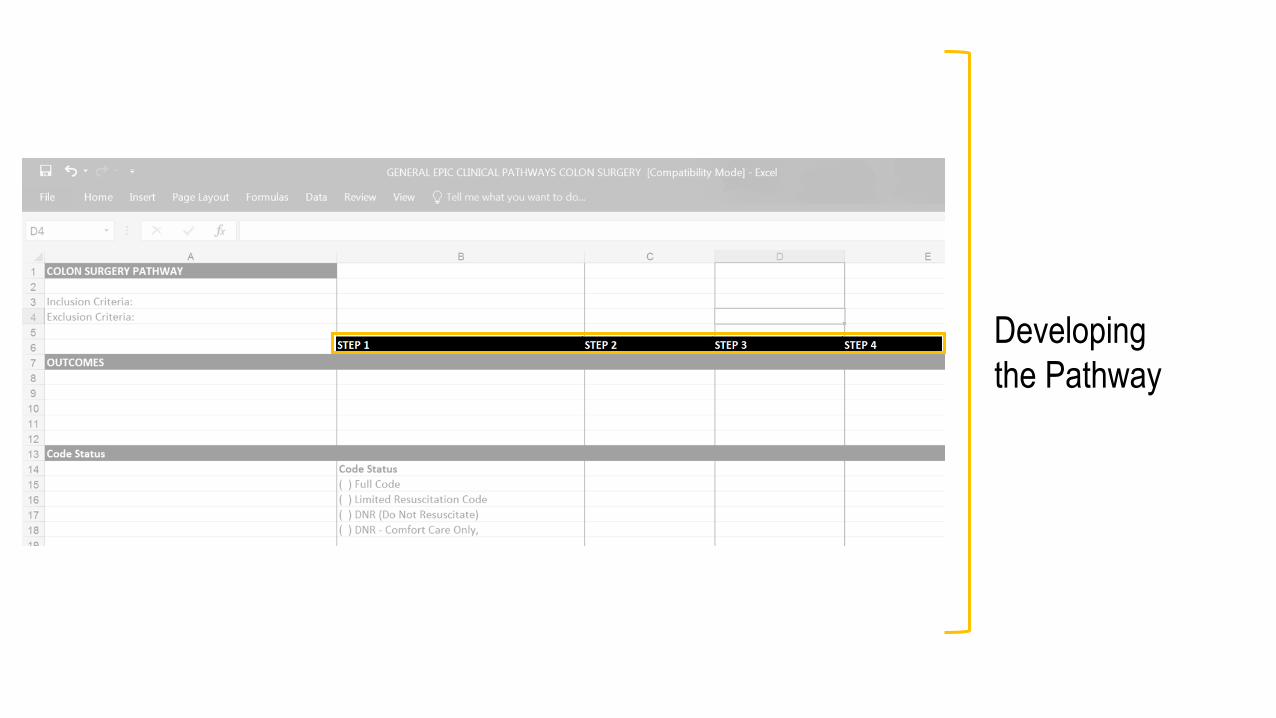
Developing
the Pathway
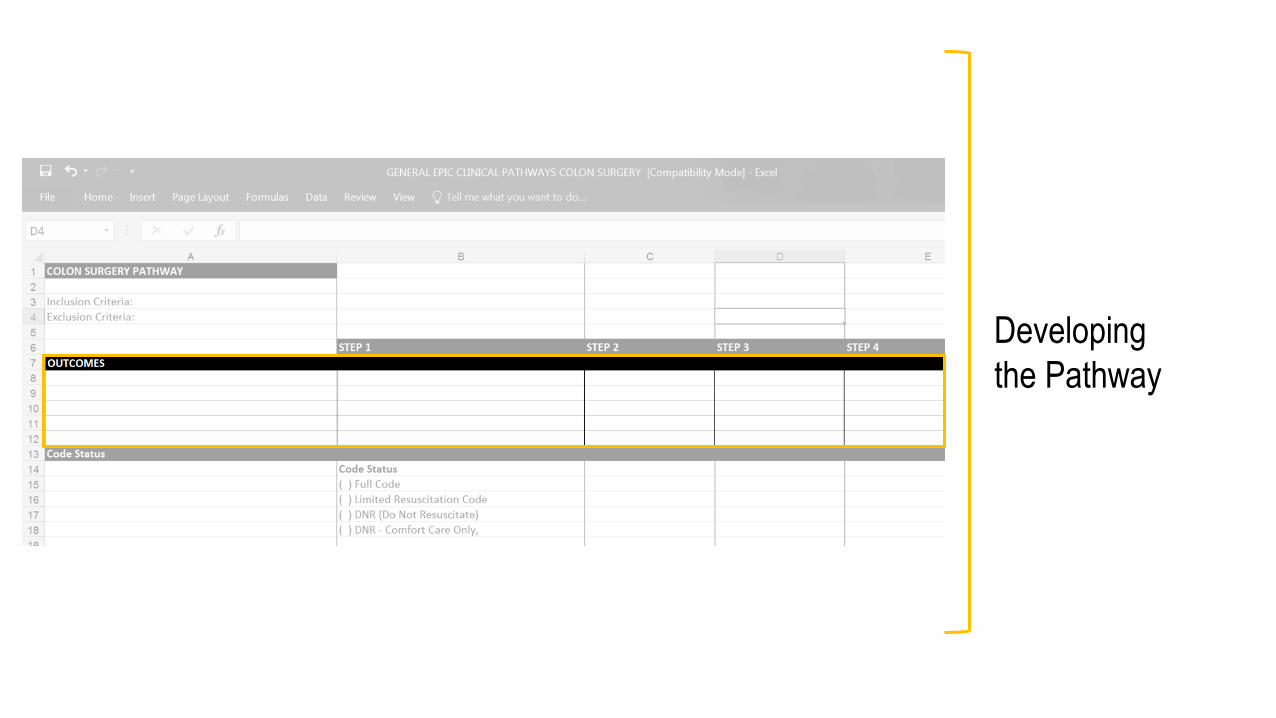
Developing
the Pathway
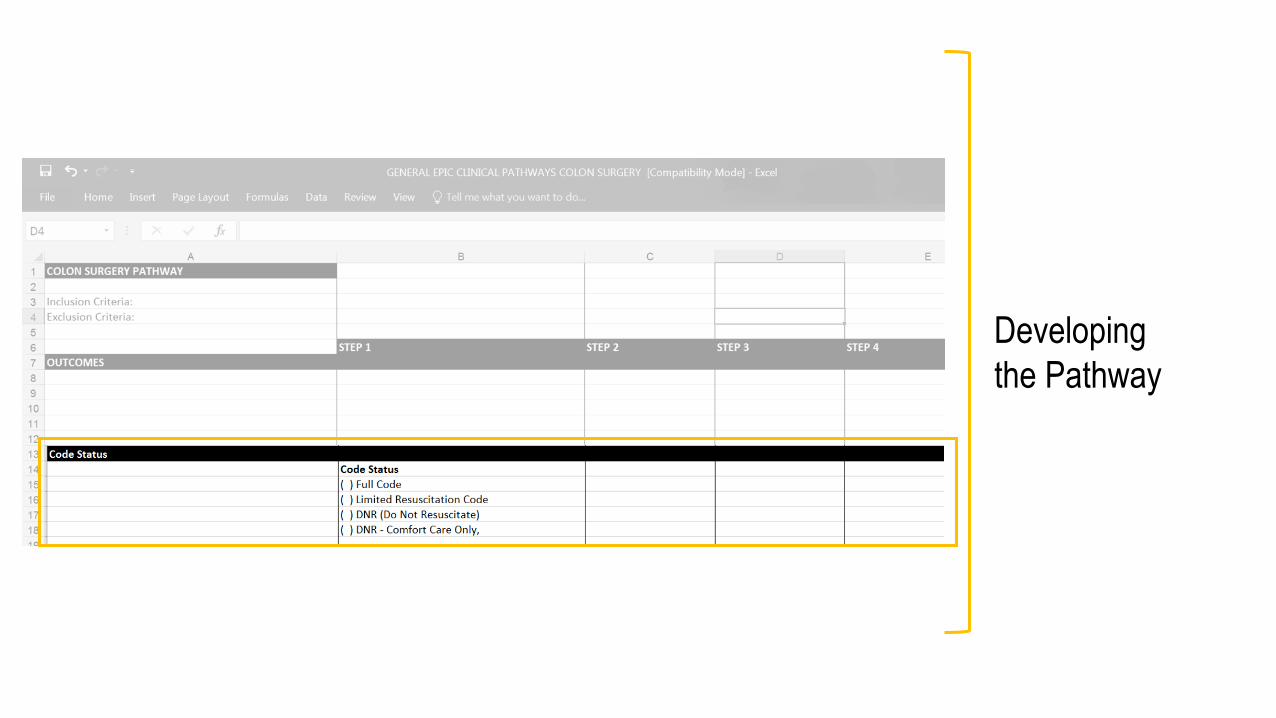
Developing
the Pathway
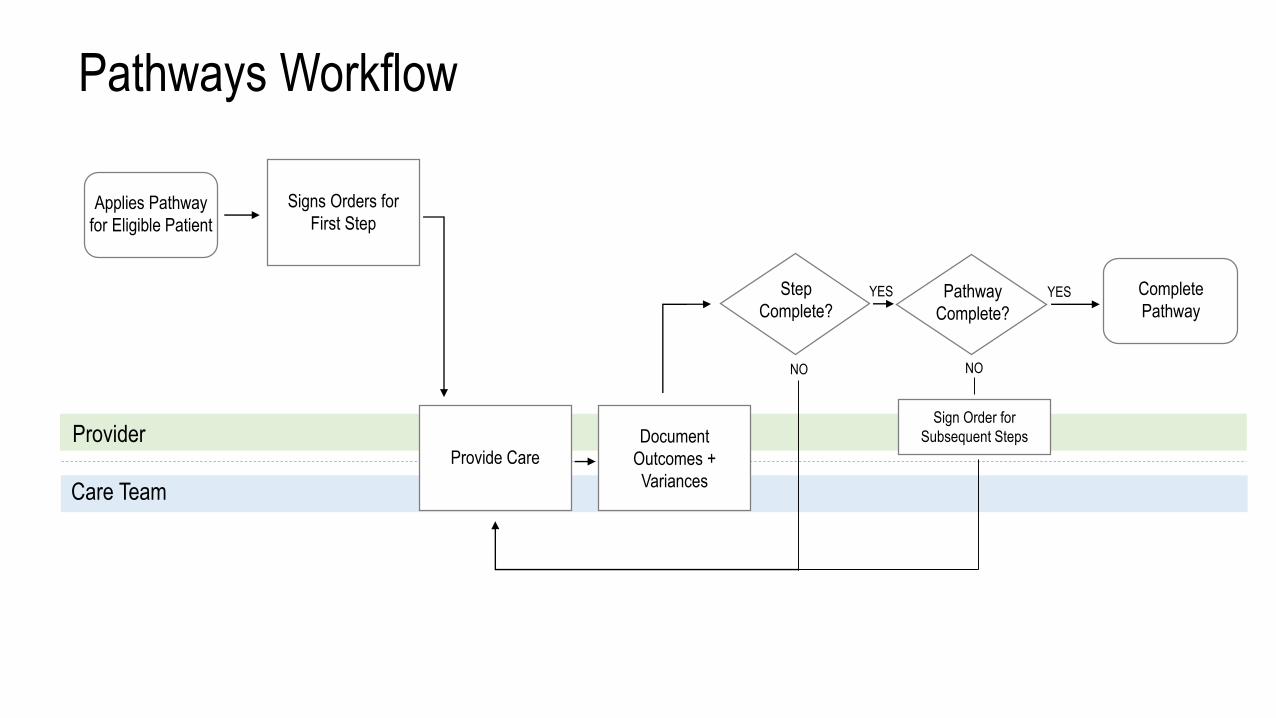
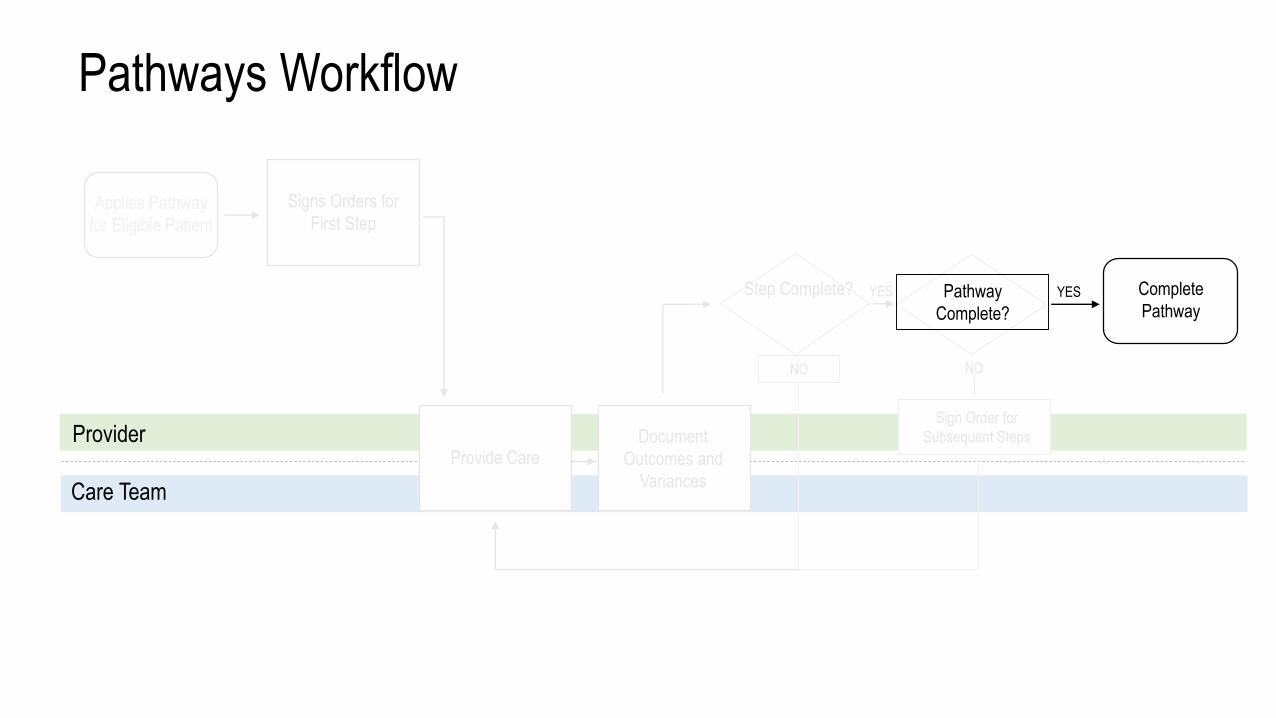
NO
YES
Applies Pathway
for Eligible Patient
Signs Orders for
First Step
Provide CareDocument
Outcomes +
Variances
Step
Complete?Pathway
Complete?
Sign Order for
Subsequent Steps
Complete
PathwayYES
Pathways Workflow
Provider
Care Team
NO

NO
YES
Signs Orders for
First Step
Provide Care
Pathway
Complete?
YES
Pathways Workflow
Provider
Care Team
NO
Document
Outcomes and
Variances
Step Complete?
Sign Order for
Subsequent Steps
Applies Pathway
for Eligible Patient
Complete
Pathway
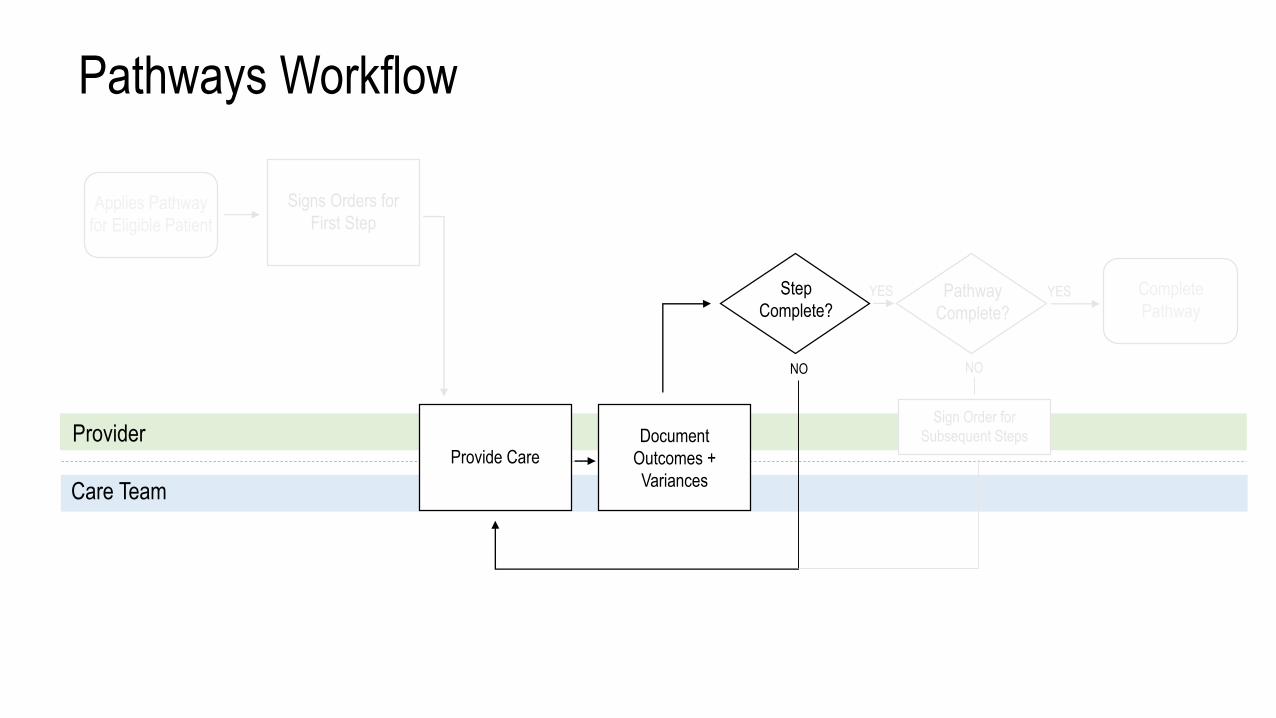
NO
YES
Signs Orders for
First Step
Provide CareDocument
Outcomes +
Variances
Step
Complete?Pathway
Complete?
Sign Order for
Subsequent Steps
YES
Pathways Workflow
Provider
Care Team
NO
Applies Pathway
for Eligible Patient
Complete
Pathway
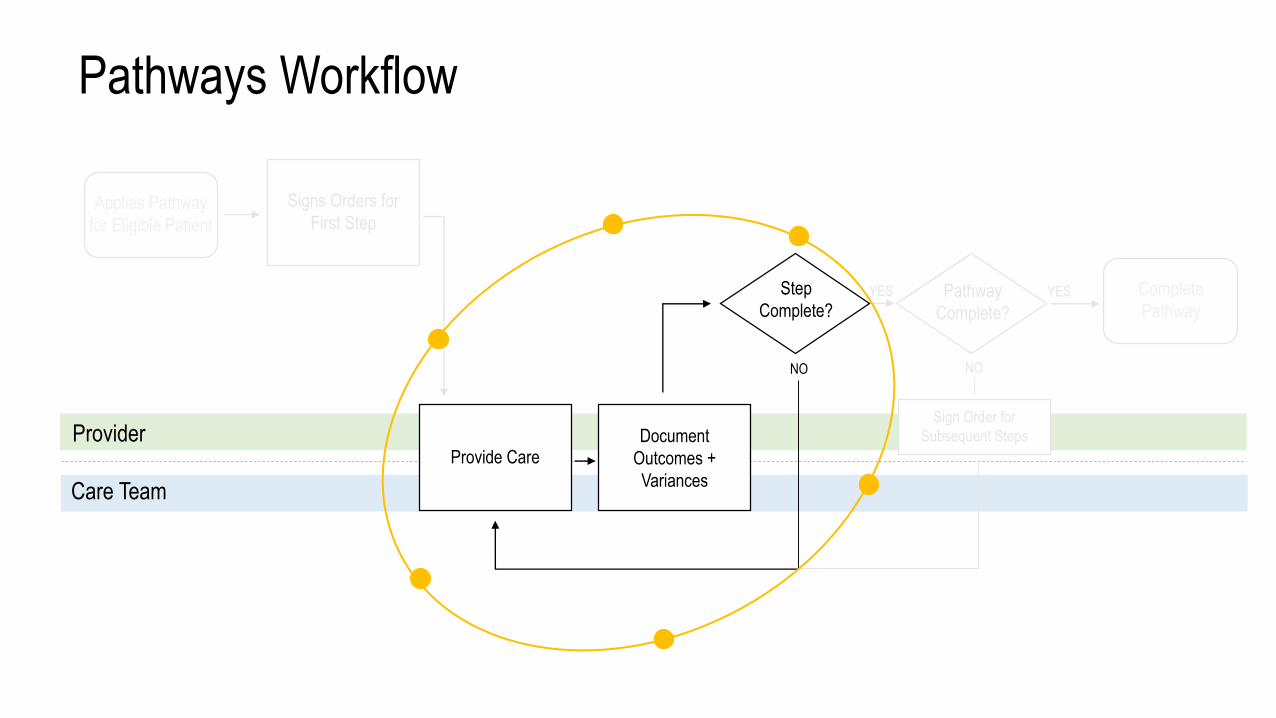
NO
YES
Signs Orders for
First Step
Provide CareDocument
Outcomes +
Variances
Step
Complete?Pathway
Complete?
Sign Order for
Subsequent Steps
YES
Pathways Workflow
Provider
Care Team
NO
Applies Pathway
for Eligible Patient
Complete
Pathway
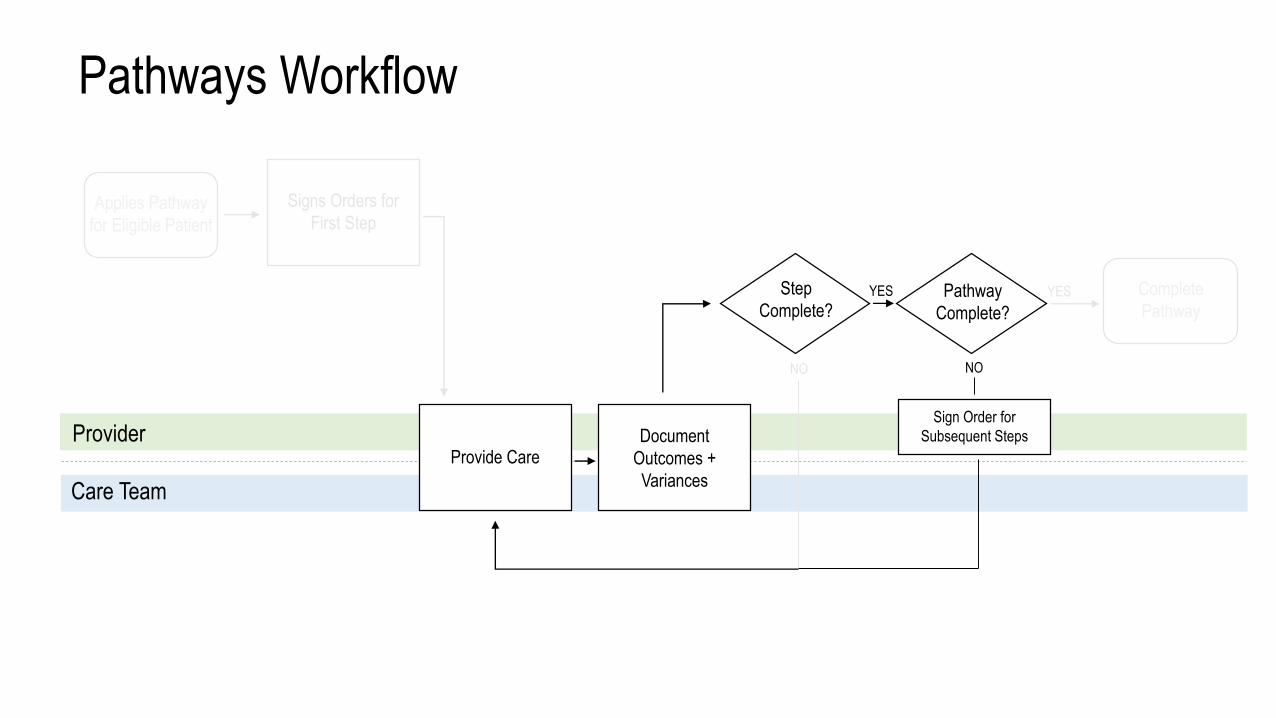
NO
YES
Signs Orders for
First Step
Provide CareDocument
Outcomes +
Variances
Step
Complete?Pathway
Complete?
Sign Order for
Subsequent Steps
YES
Pathways Workflow
Provider
Care Team
NO
Applies Pathway
for Eligible Patient
Complete
Pathway

NO
YES
Signs Orders for
First Step
Provide CareDocument
Outcomes +
Variances
Step
Complete?Pathway
Complete?
Sign Order for
Subsequent Steps
YES
Pathways Workflow
Provider
Care Team
NO
Applies Pathway
for Eligible Patient
Complete
Pathway
NO
YES
Signs Orders for
First Step
Provide Care
Pathway
Complete?
YES
Pathways Workflow
Provider
Care Team
NO
Document
Outcomes and
Variances
Step Complete?
Sign Order for
Subsequent Steps
Applies Pathway
for Eligible Patient
Complete
Pathway

NO
YES
Signs Orders for
First Step
Provide CareDocument
Outcomes +
Variances
Step
Complete?Pathway
Complete?
Sign Order for
Subsequent Steps
YES
Pathways Workflow
Provider
Care Team
NO
Discontinue
Pathway
Applies Pathway
for Eligible Patient
Complete
Pathway
Converting Paper into an Electronic Pathway
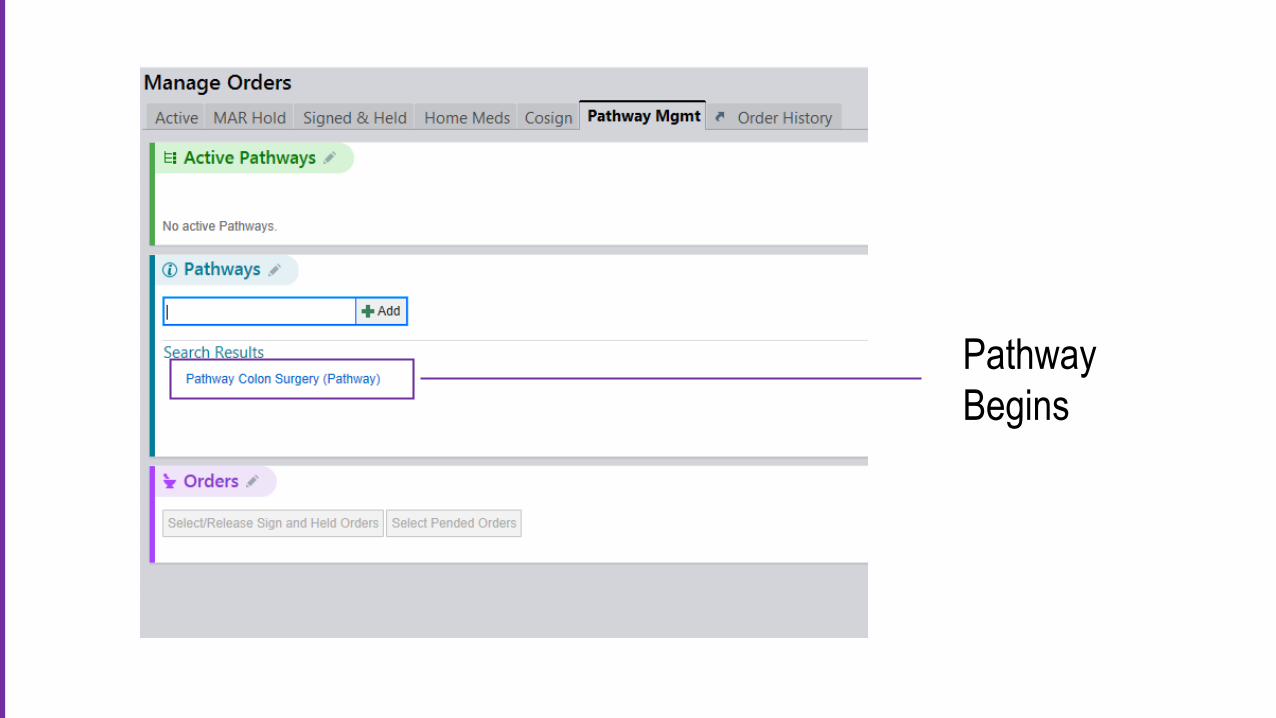
Pathway
Begins
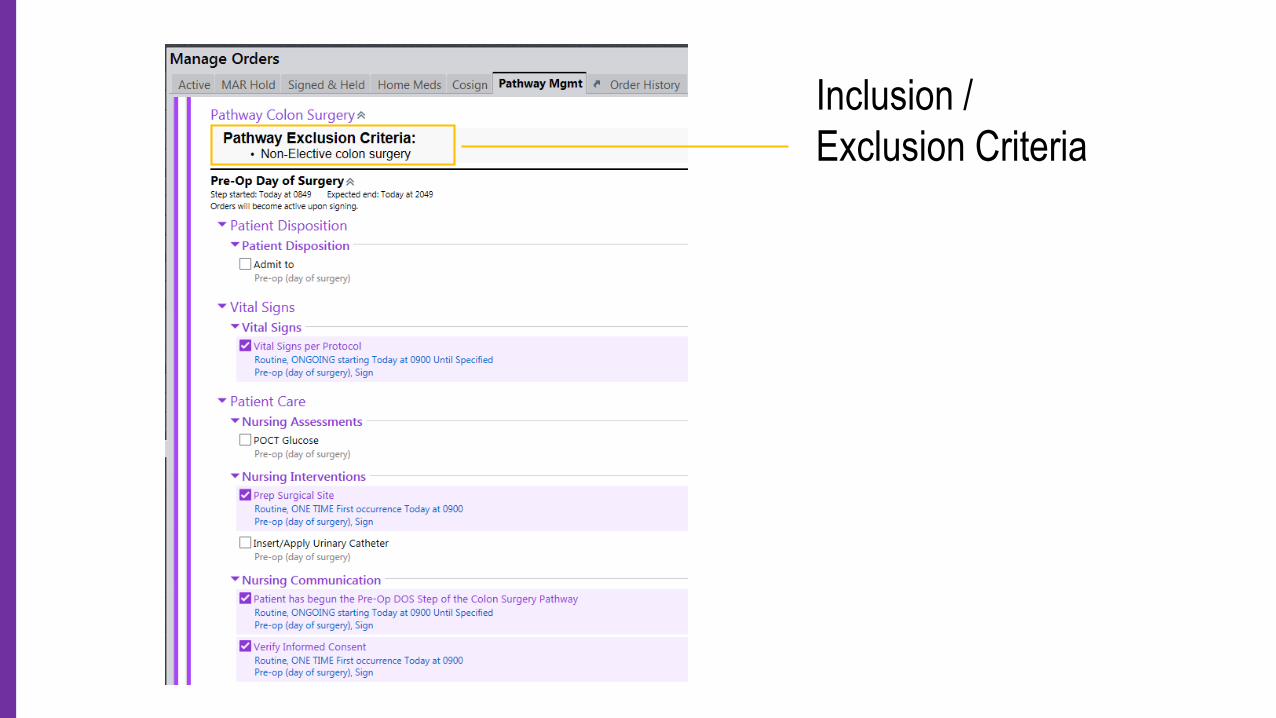
Inclusion /
Exclusion Criteria
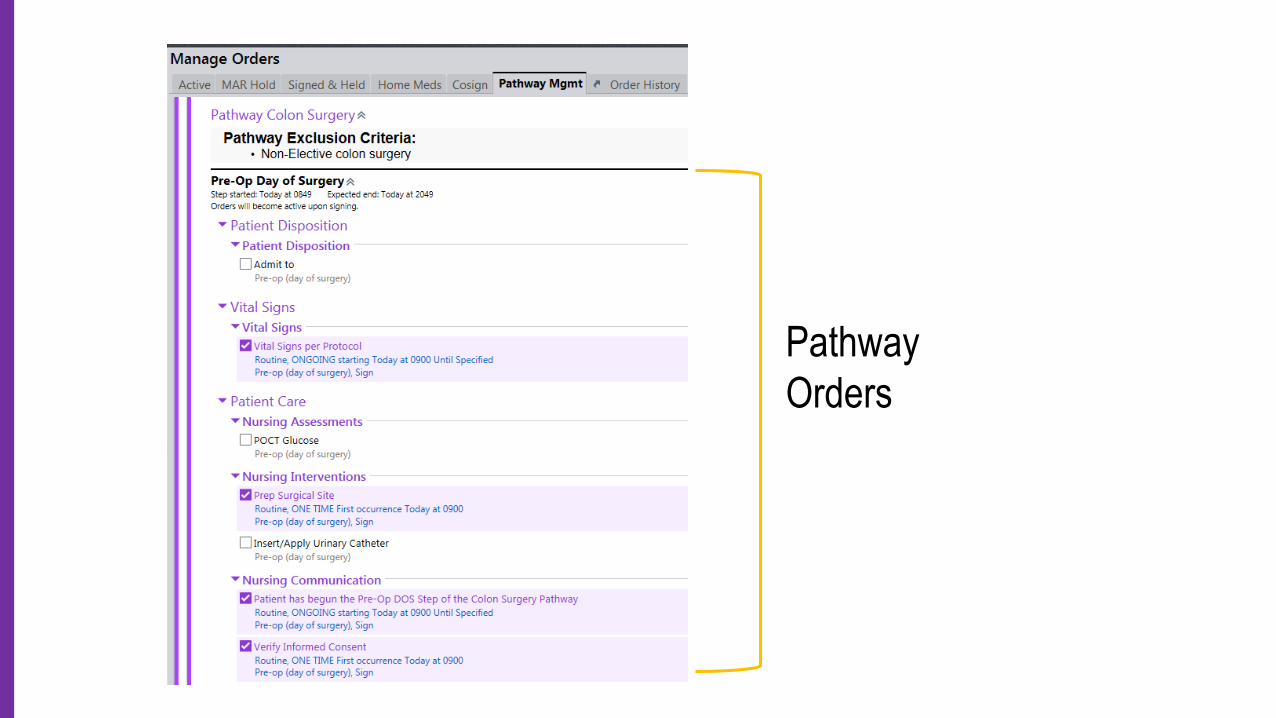
Pathway
Orders
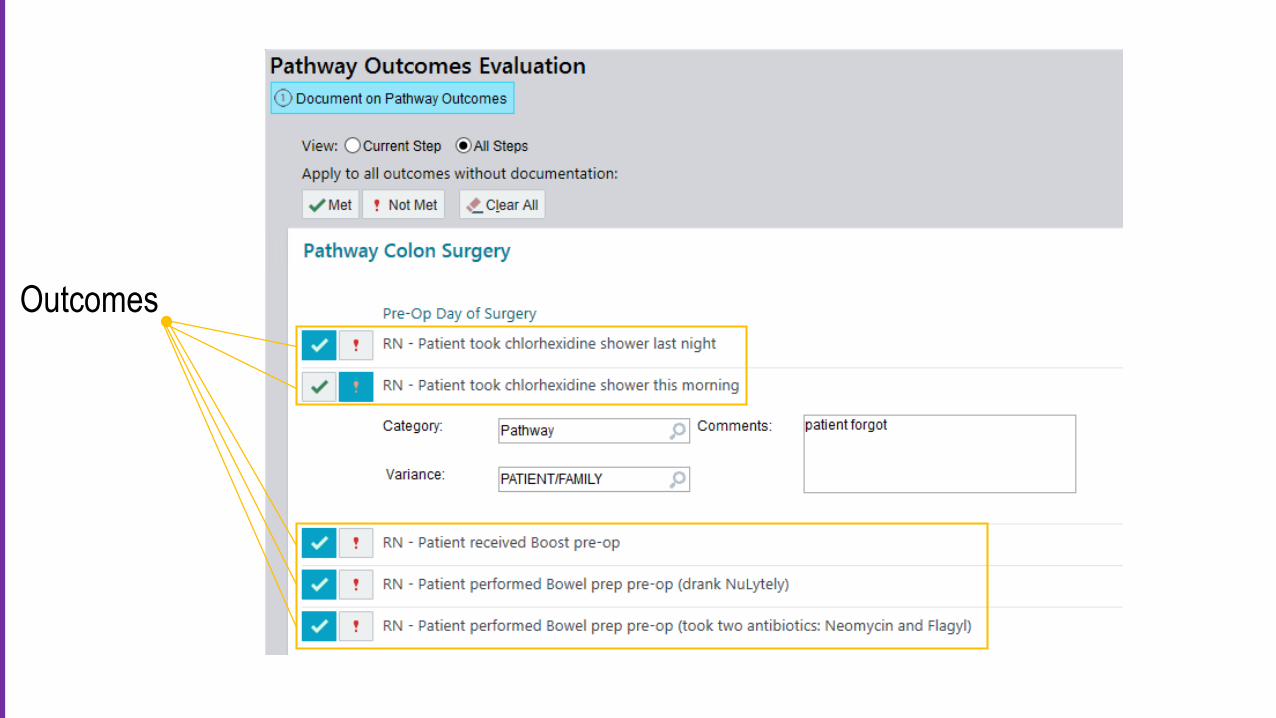
Outcomes

Variance
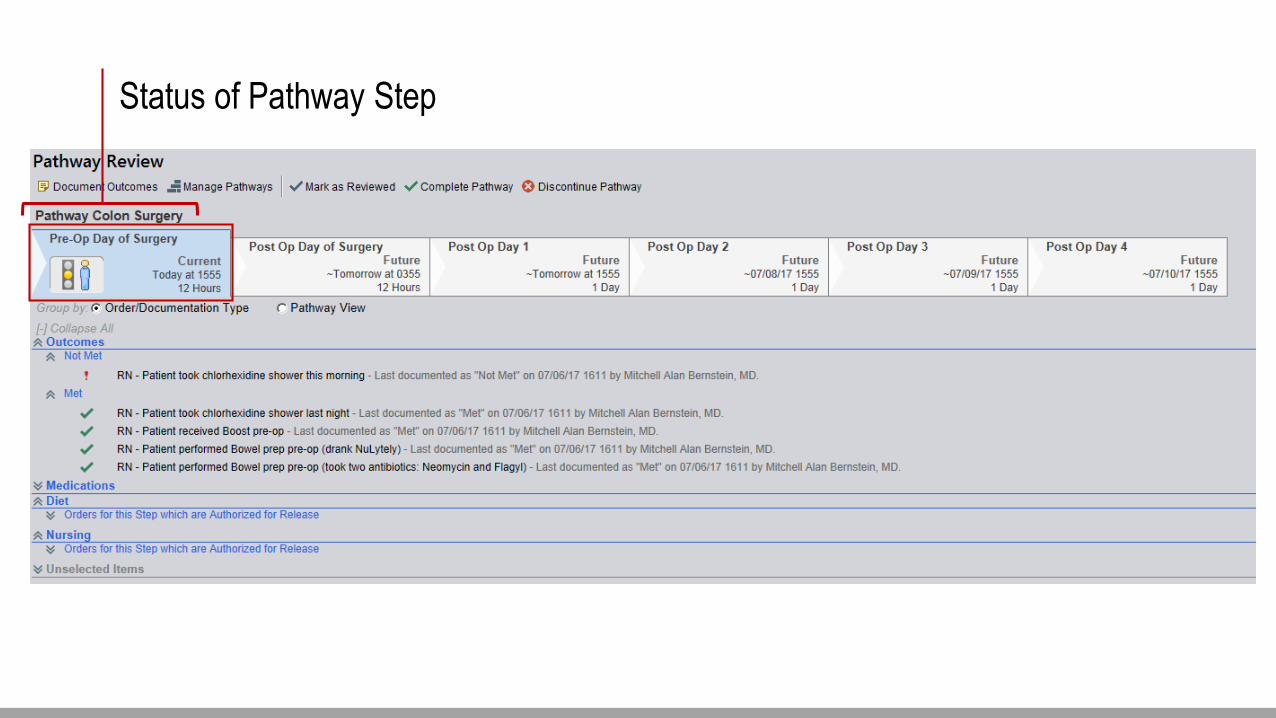
Status of Pathway Step

Pathway
Dashboard
Change
Management &
Implementation
Content
Changes
Functionality
Changes
Functionality
Changes
Continuous Process
Improvement

Suggested
Outcome
Values
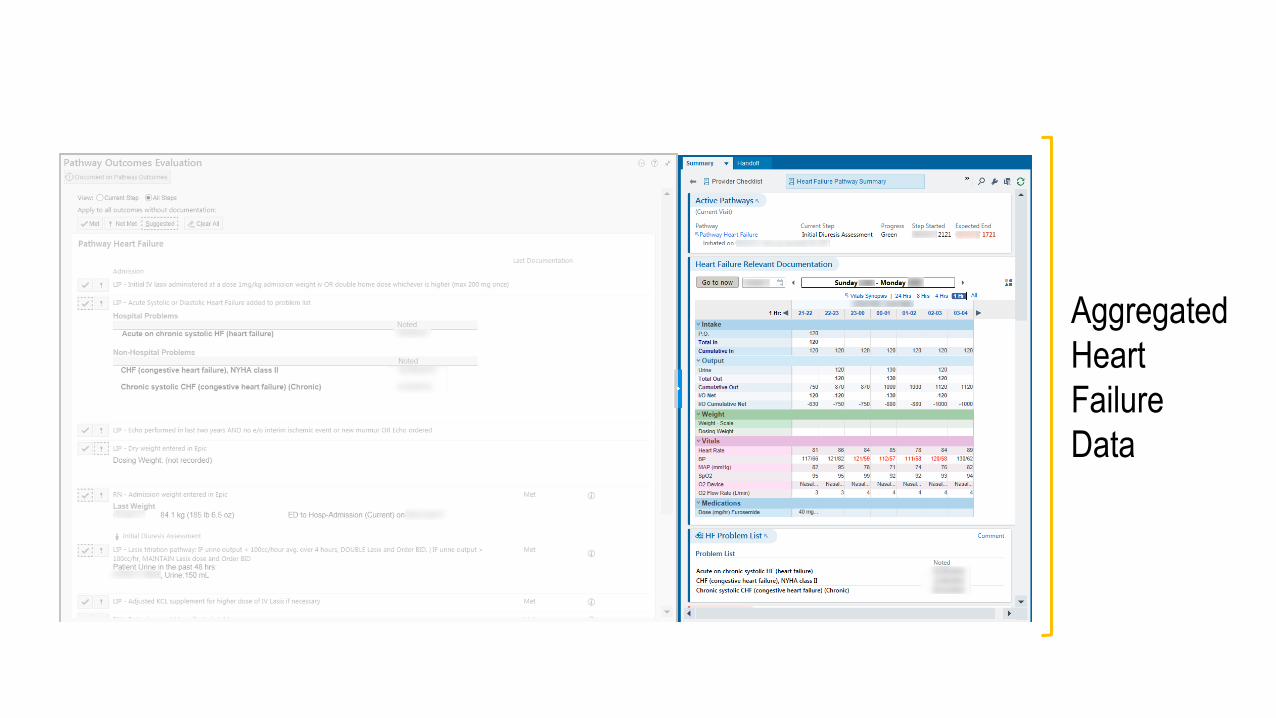
Aggregated
Heart
Failure
Data
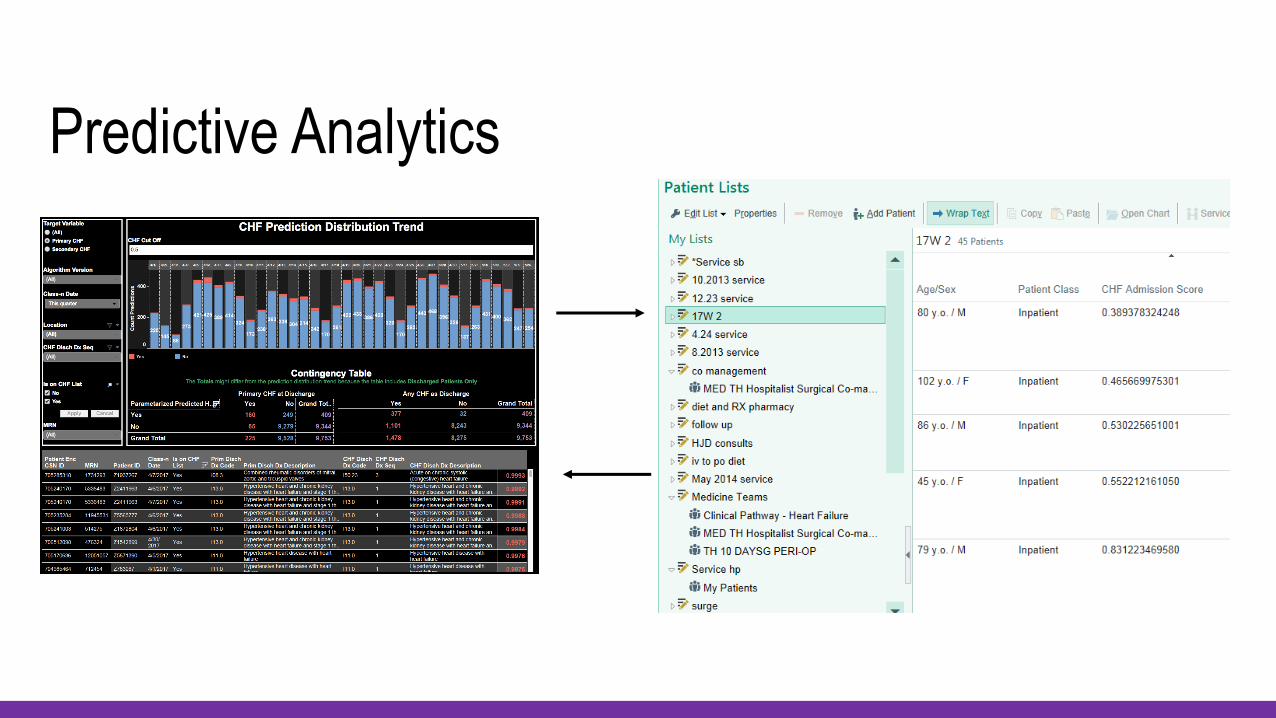
Predictive Analytics
$ Realized
Value
0.7
0.75
0.8
0.85
0.9
0.95
1
1.05
1.1
1.15
1.2
Baseline Q3 FY15 Q4 FY15 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY16 Q1 FY17 Q2 FY17
O:E
Pneumonia
Pneumonia
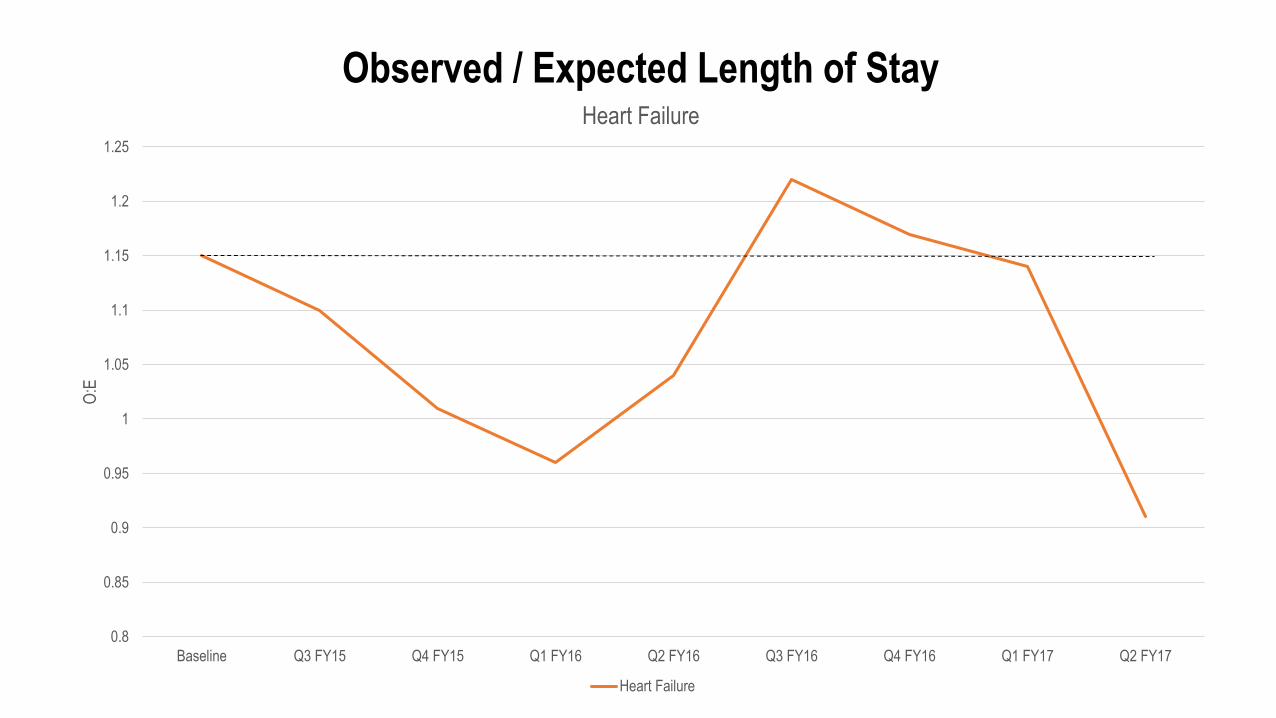
Observed / Expected Length of Stay
-70
-60
-50
-40
-30
-20
-10
0
10
Baseline Q3 FY15 Q4 FY15 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY16 Q1 FY17 Q2 FY17
Per
cent
age
Dec
reas
e
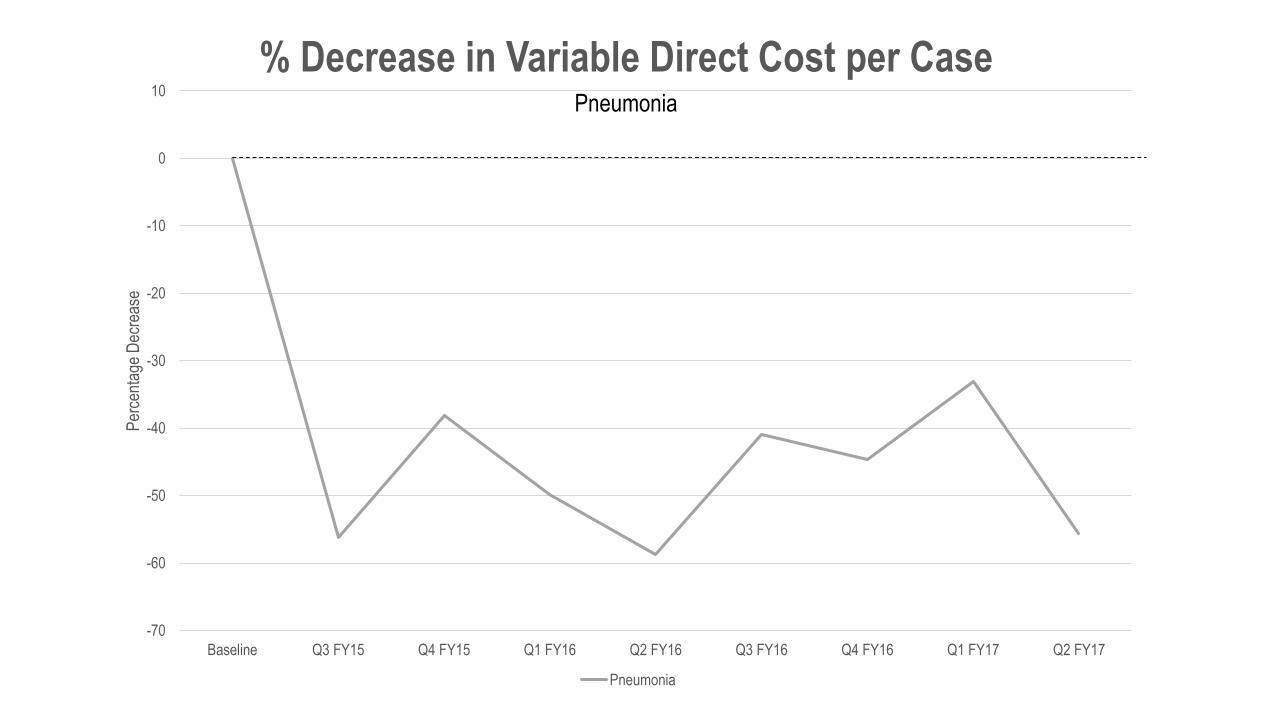
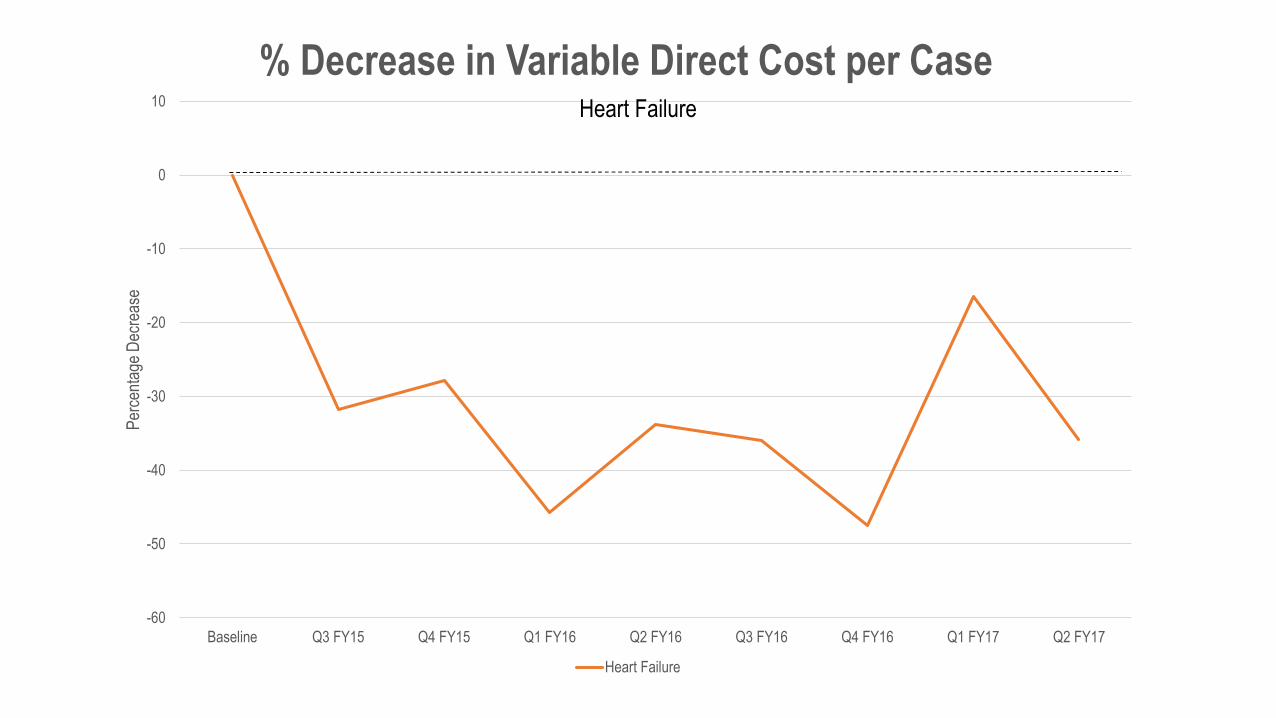
% Decrease in Variable Direct Cost per Case
Pneumonia
Pneumonia
0.5
0.55
0.6
0.65
0.7
0.75
0.8
0.85
Baseline Q3 FY15 Q4 FY15 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY16 Q1 FY17 Q2 FY17
O:E
Colon
Colon
Observed / Expected Length of Stay
-40
-35
-30
-25
-20
-15
-10
-5
0
5
10
Baseline Q3 FY15 Q4 FY15 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY16 Q1 FY17 Q2 FY17
Per
cent
age
Dec
reas
e
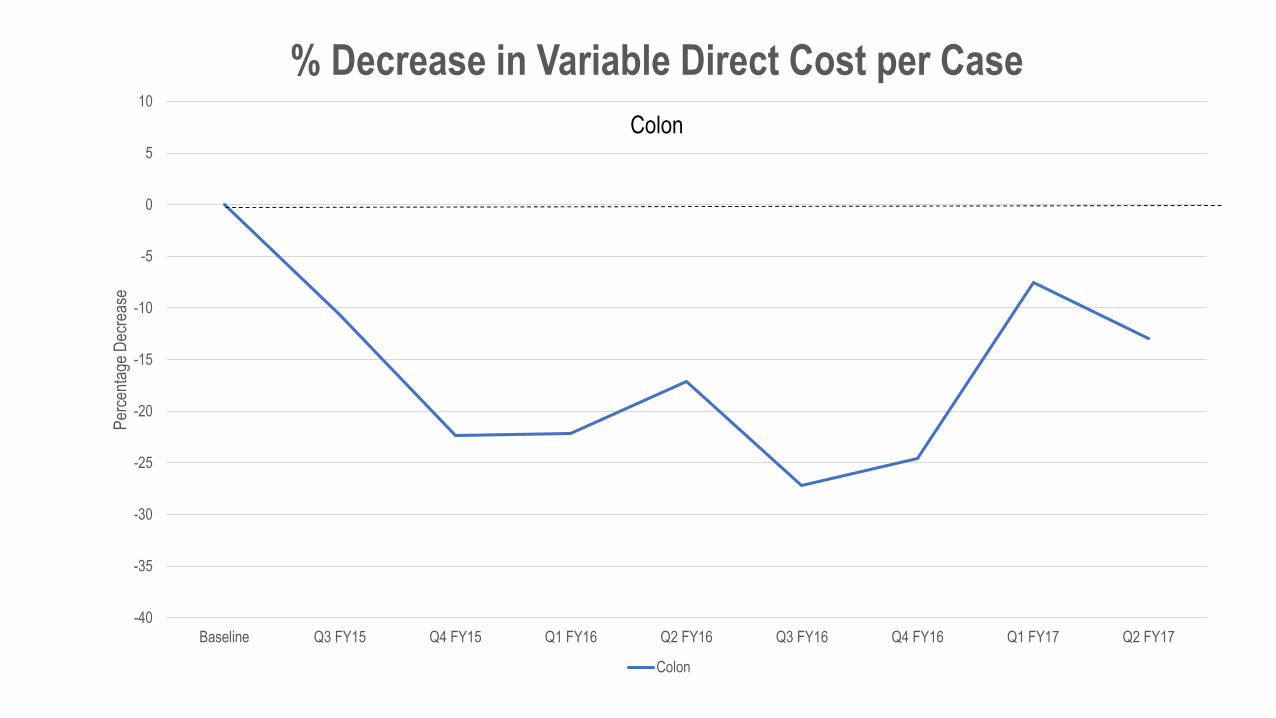
% Decrease in Variable Direct Cost per Case
Colon
Colon
0.8
0.85
0.9
0.95
1
1.05
1.1
1.15
1.2
1.25
Baseline Q3 FY15 Q4 FY15 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY16 Q1 FY17 Q2 FY17
O:E
Heart Failure
Heart Failure
Observed / Expected Length of Stay
-60
-50
-40
-30
-20
-10
0
10
Baseline Q3 FY15 Q4 FY15 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY16 Q1 FY17 Q2 FY17
Per
cent
age
Dec
reas
e
% Decrease in Variable Direct Cost per Case
Heart Failure
Heart Failure
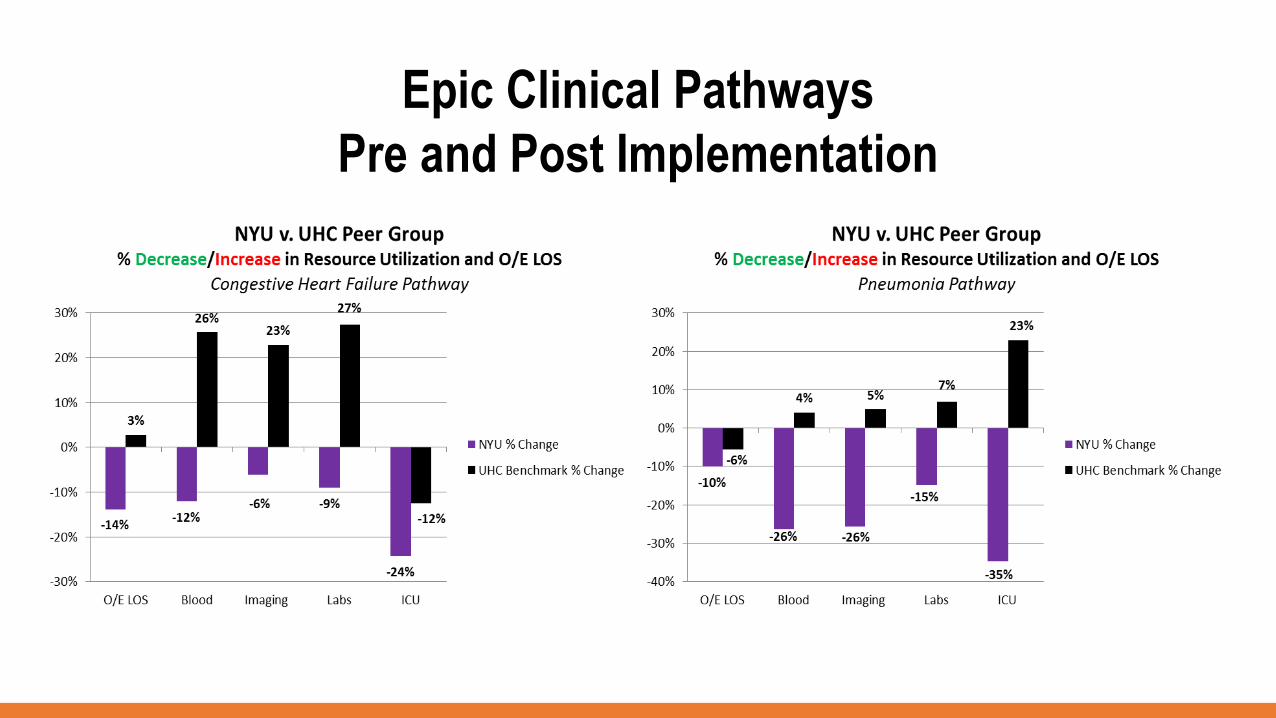
Epic Clinical Pathways
Pre and Post Implementation

0
500000
1000000
1500000
2000000
2500000
3000000
Q3 FY15 Q4 FY15 Q1 FY16 Q2 FY16 Q3 FY16 Q4 FY16 Q1 FY17 Q2 FY17
Quarterly Savings for Pathway Cases
Colon Heart Failure Pneumonia
Total Savings
Colon
Heart Failure
Pneumonia
$2,579,211
$3,951,855
$6,394,106
$12,925,172

691 Project Team Hours
$79,465Costs
Lessons Learned
• Pathway analytics drive change
• Project management handoff key
• Pathways need to be lean.
• Electronic pathways demonstrate value

Thank You
Dana Ostrow
Senior Director of Clinical Systems, NYU Langone Health
Gabriela Grygus, MBA, RHIA
Senior Director, Health Information Management, NYU Langone Health
Paperless Registration
In the past, our registration process
involved lots of paper.

In 2014, we had over
1.25 million paper
registration
documents signed and
scanned into Epic.
Average registration
time with PAPER took
10 minutes
3,897,690 pieces of paper
were used, costing over
$428,745.90
That’s about
527 trees.
And we spent over $93,986
annually on scanning services
before paperless registration.
Registration
We mapped the
Digital Patient Experience
to better understand the needs of our
patients across the continuum of care
beginning end
In the first half of
2017, over 1.3
million documents
were digitally
signed.
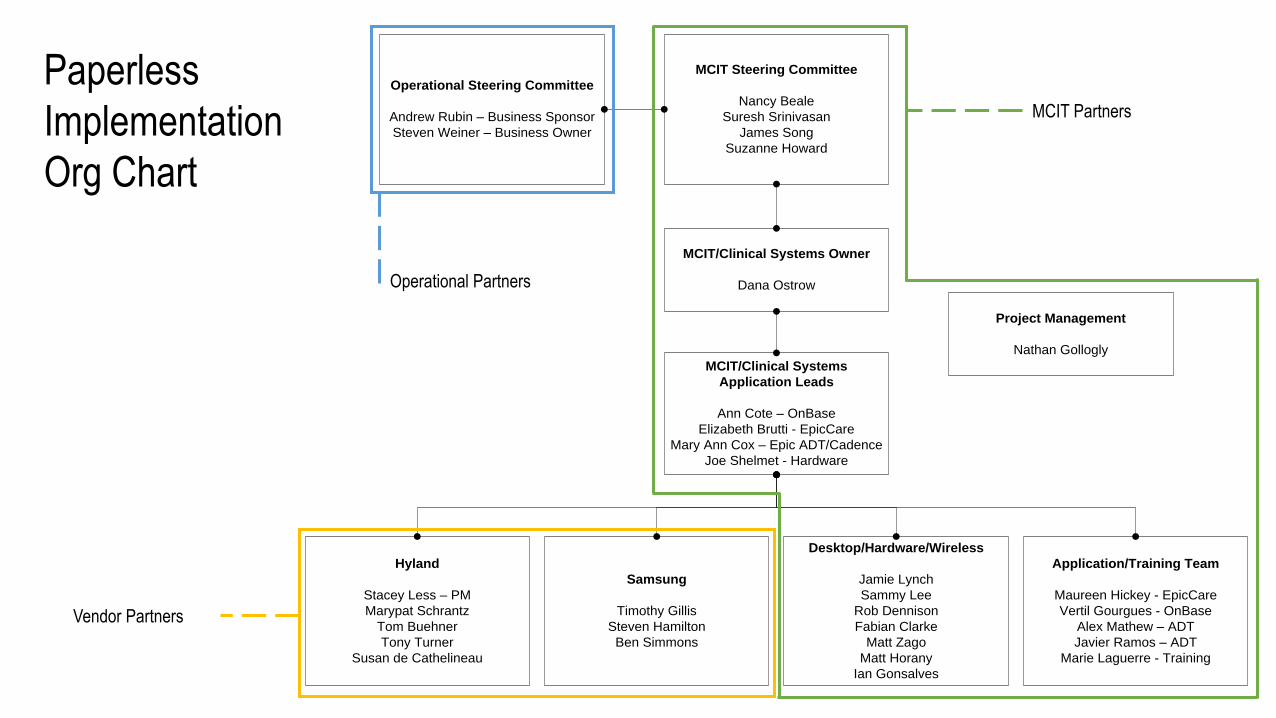
MCIT/Clinical Systems Owner
Dana Ostrow
Hyland
Stacey Less – PM
Marypat Schrantz
Tom Buehner
Tony Turner
Susan de Cathelineau
MCIT/Clinical Systems
Application Leads
Ann Cote – OnBase
Elizabeth Brutti - EpicCare
Mary Ann Cox – Epic ADT/Cadence
Joe Shelmet - Hardware
Samsung
Timothy Gillis
Steven Hamilton
Ben Simmons
Desktop/Hardware/Wireless
Jamie Lynch
Sammy Lee
Rob Dennison
Fabian Clarke
Matt Zago
Matt Horany
Ian Gonsalves
Project Management
Nathan Gollogly
Application/Training Team
Maureen Hickey - EpicCare
Vertil Gourgues - OnBase
Alex Mathew – ADT
Javier Ramos – ADT
Marie Laguerre - Training
MCIT Steering Committee
Nancy Beale
Suresh Srinivasan
James Song
Suzanne Howard
Operational Steering Committee
Andrew Rubin – Business Sponsor
Steven Weiner – Business Owner
Paperless
Implementation
Org Chart
Operational Partners
MCIT Partners
Vendor Partners
Design + Implementation Timeline
September 2014 –
Discovery process for tool selection began
Guiding
Principles for
Tool
Selection
enable positive experience for both employee and patient
leverage existing partnerships if possible
work seamlessly with other registration technologies such as Patient Secure
integrate with Epic
offer a flexible platform that would allow for more than just paperless registration
We counted clicks to ensure that the registrar was
in fact able to work faster.
We timed patients to ensure that registration was in
fact quicker.

Topaz eCapture Access Welcome Kiosk
Patient can see/ complete
form independently
Form is interactive
Error checking on the form
Data Captured Discretely
Signature Embedded on
Saved Form
Can be used for
Questionnaires
Can be used for Clinical
Consents
?
We considered a
wide variety of
platforms and
their capabilities
We tested devices and
platforms and found that
some didn’t meet our
needs.
Design + Implementation Timeline
September 2014 –
Discovery process for
tool selection began
October – November 2014 –
Initial development in coordination with Epic, Samsung
and Hyland

We chose to develop a
paperless platform with these
partners.
The QR Code – what makes our
paperless platform dynamic.
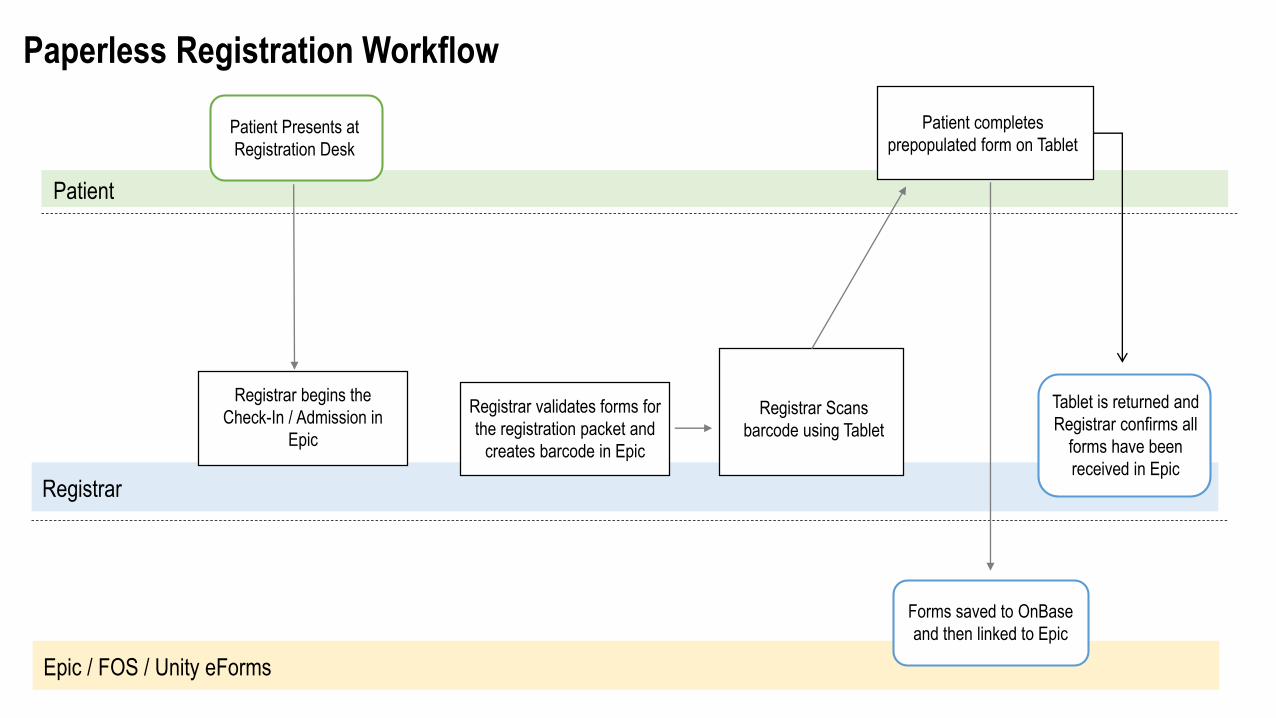
Epic / FOS / Unity eForms
Patient Presents at
Registration Desk
Registrar validates forms for
the registration packet and
creates barcode in Epic
Registrar Scans
barcode using Tablet
Patient completes
prepopulated form on Tablet
Forms saved to OnBase
and then linked to Epic
Patient
Registrar
Paperless Registration Workflow
Registrar begins the
Check-In / Admission in
Epic
Tablet is returned and
Registrar confirms all
forms have been
received in Epic



• Bi-monthly Iterative testing
with each release for a week,
including integrated end to end
testing
• Usability with staff
• Usability with patients
• Trials with multiple types of
tablets and styluses
Testing
• Devices are enrolled in Airwatch, which allows us to manage
them remotely
• Updates can be pushed to devices through Airwatch
• Airwatch Secure Launcher is installed on the devices which
allows us to lock down the home screen of the device to the
Paperless application
Change Management

Infection Control
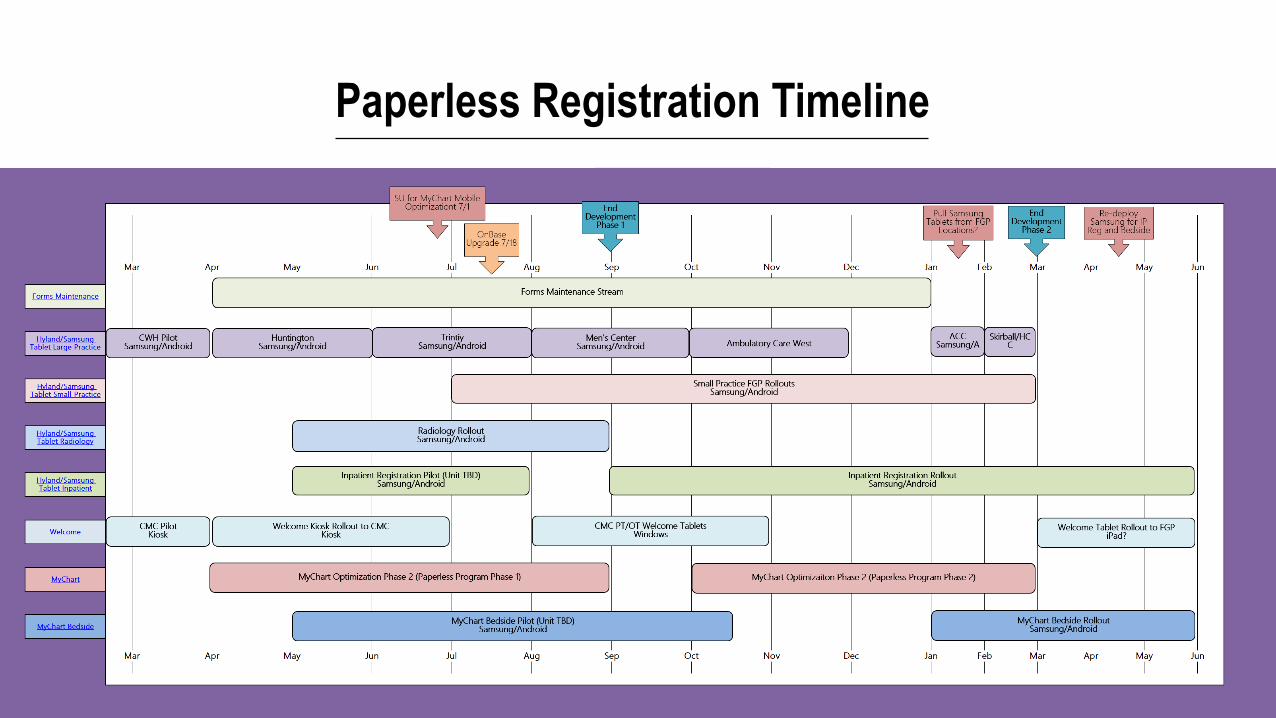
Paperless Registration Timeline
Design + Implementation Timeline
September 2014 –
Discovery process for
tool selection began
October – November
2014 –
Initial development in
coordination with Epic,
Samsung and Hyland
February 2015 –
First Go-Live at NYU Langones Center
for Womens Health
First Test Site –
NYU Health:
Center for Women’s Health
23 providers

Design + Implementation Timeline
September 2014 –
Discovery process for
tool selection began
October – November
2014 –
Initial development in
coordination with Epic,
Samsung and Hyland
February 2015 –
First Go-Live at NYU
Langones Center for
Womens Health
June 2015 –
Rolled out to large ambulatory location –
Huntington Medical Center – ensuring
enterprise readiness

Design + Implementation Timeline
September 2014 –
Discovery process for
tool selection began
October – November
2014 –
Initial development in
coordination with Epic,
Samsung and Hyland
February 2015 –
First Go-Live at NYU
Langones Center for
Womens Health
June 2015 –
Rolled out to large
ambulatory location –
Huntington Medical
Center – ensuring
enterprise readiness
December 2015 –
Paperless registration
rolled out to 95% of
enterprise
Continuous Improvement
MyChart ID creation in registration
Multilanguage capabilities
Research Consents
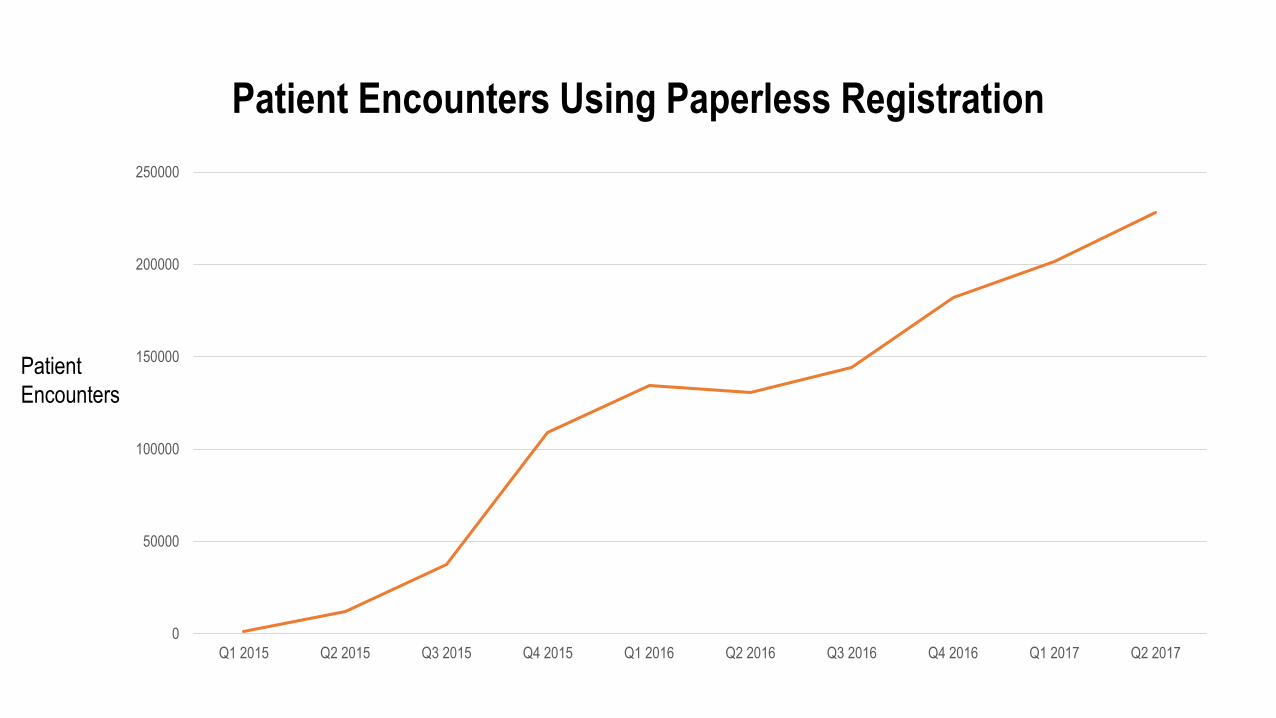
Patient Encounters Using Paperless Registration
0
50000
100000
150000
200000
250000
Q1 2015 Q2 2015 Q3 2015 Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017 Q2 2017
Patient
Encounters

Average registration
time with TABLET – 5
minutes
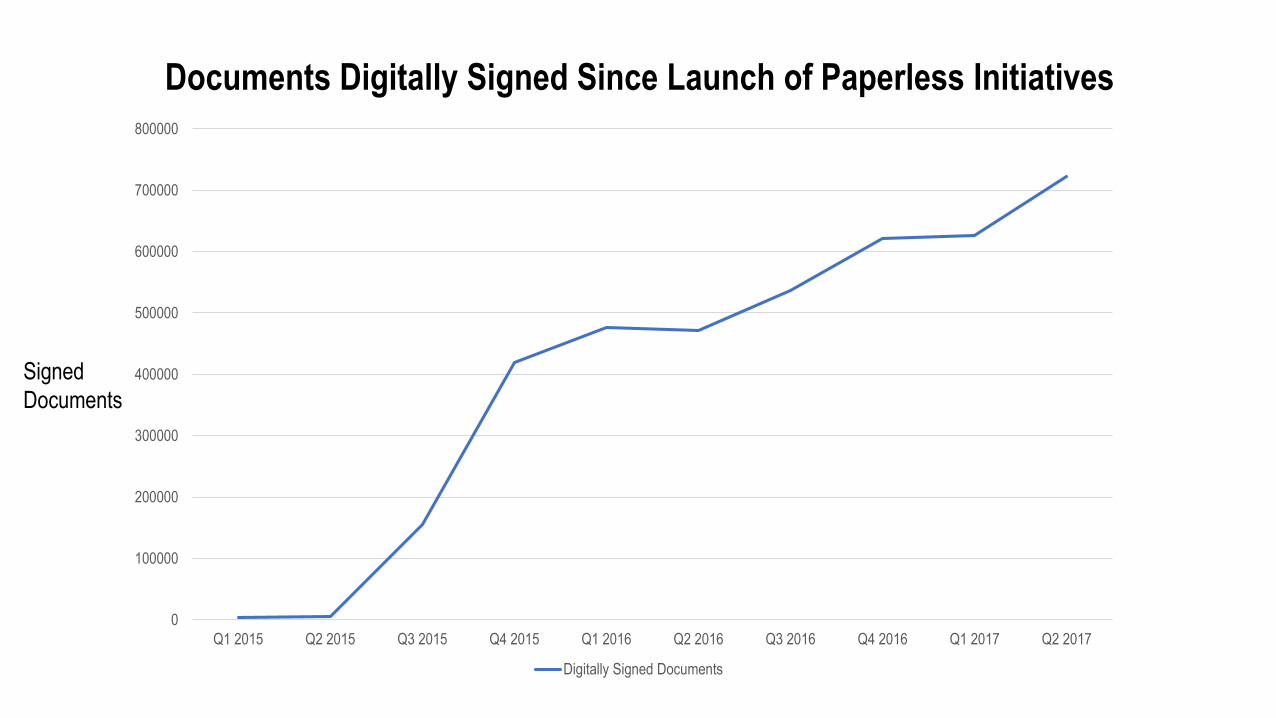
Documents Digitally Signed Since Launch of Paperless Initiatives
0
100000
200000
300000
400000
500000
600000
700000
800000
Q1 2015 Q2 2015 Q3 2015 Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017 Q2 2017
Digitally Signed Documents
Signed
Documents
0
200000
400000
600000
800000
1000000
1200000
Q1 2015 Q2 2015 Q3 2015 Q4 2015 Q1 2016 Q2 2016 Q3 2016 Q4 2016 Q1 2017 Q2 2017
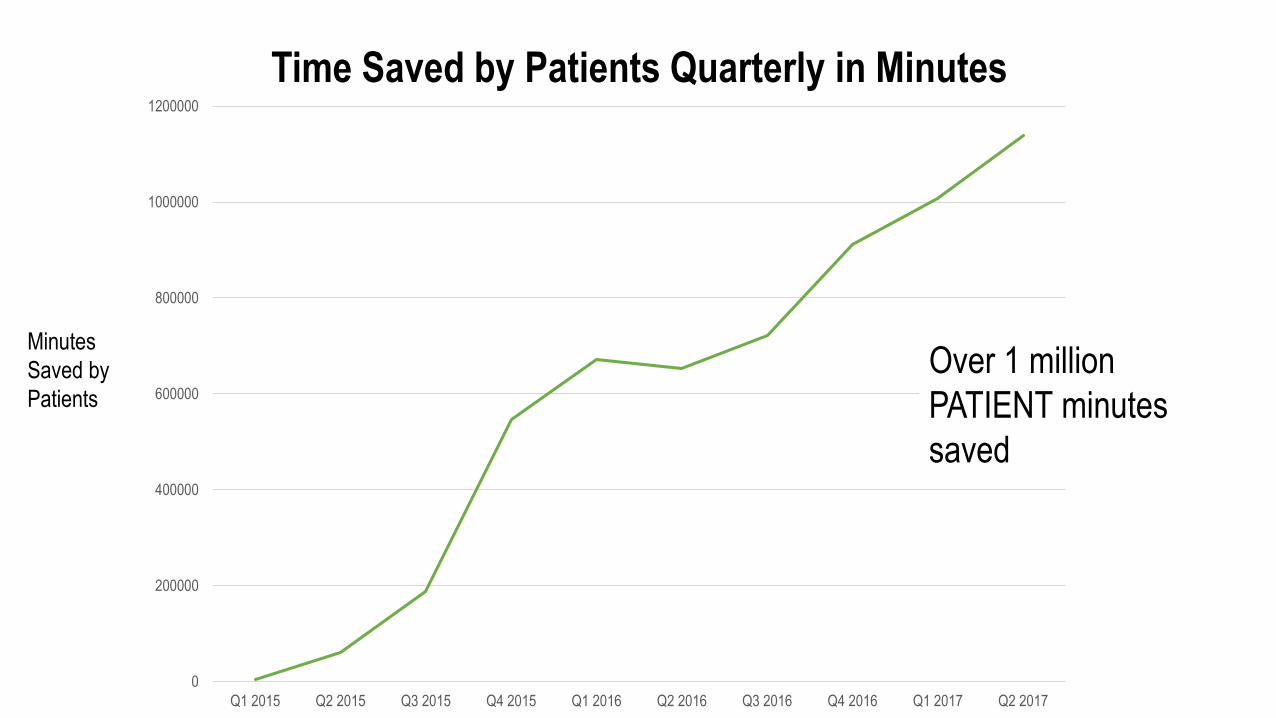
Time Saved by Patients Quarterly in Minutes
Over 1 million
PATIENT minutes
saved
Minutes
Saved by
Patients

0
10000
20000
30000
40000
50000
60000
Monthly MyChart Activation Since Paperless Registration Launch
Patients
New
My Chart
Activations
Not using paper saved us nearly
$450,000 a year.
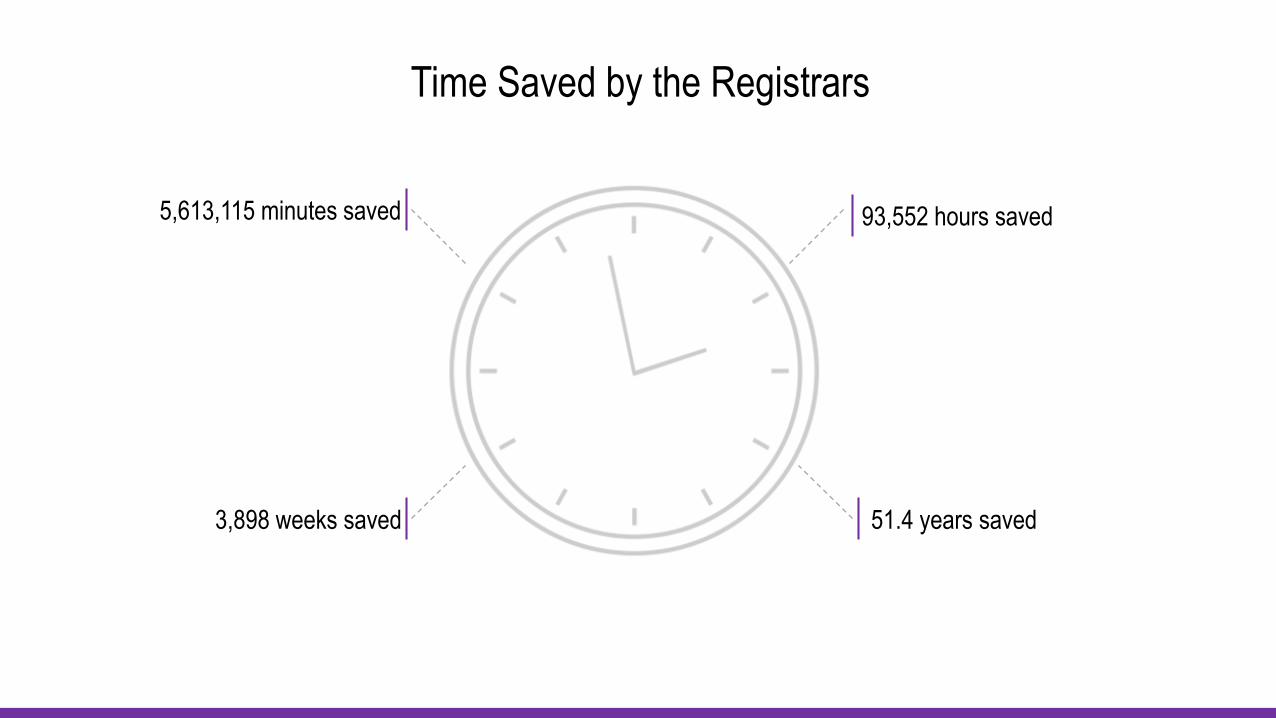
5,613,115 minutes saved 93,552 hours saved
3,898 weeks saved 51.4 years saved
Time Saved by the Registrars
Soft savings of
$1.7 million
in FTE costs
Tablet Replacement budget - $30,000
Annual CostsSoftware Maintenance - $30,000
FTEs to Support- ½ an FTE in steady state. Additional
support as needed for roll outs and forms in other languages
Desktop FTEs to Support- ½ an FTE in steady state
across all locations
Lessons Learned
- Ensure that documents format correctly on tablet and are not merely copies of paper documents
- Ensure that signature requests on electronic forms are in the appropriate place
- Turn on certain interfacing early enough to allow all pieces of the platform to function properly at go-live
- Create an FAQ document for go-live to easily address common questions
- Find secure locations for use of tablets to ensure that they are not taken
- Do not assume that registrars already have full understanding of the registration process before implementation
• In 2016 we signed more then 125,000 surgical/ procedural clinical
consents.
• By the first quarter of 2018 we will be fully digital with all consents.
Next Steps

Questions
Kathleen Mullaly, MSN, RN
Senior Director MCIT, Care Delivery Transformation, NYU Langone Health
Lily Pazand
Director, Managed Care Payment Reform Analytics, NYU Langone Health
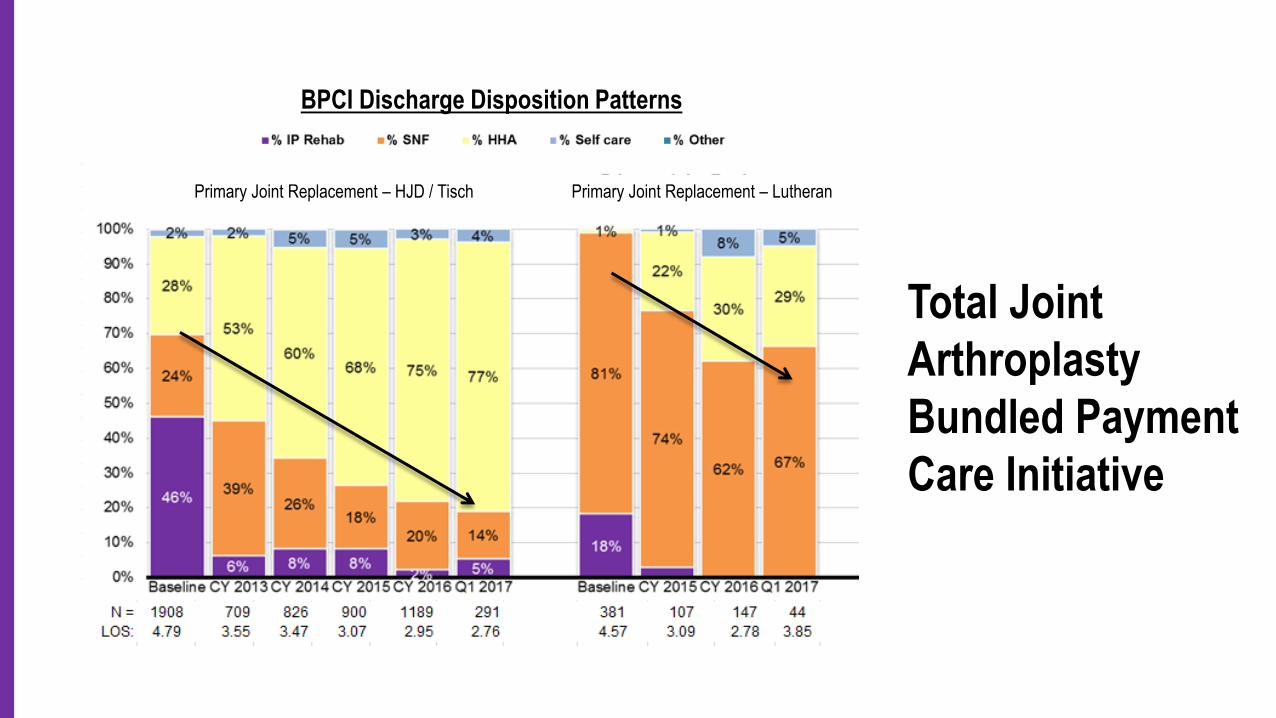
Total Joint Arthroplasty Bundled
Payment Care Initiative
CARE
Bundled Payment
for Care
Improvement
(BPCI)
NYUPN
Commercial
Shared SavingsMedicaid IPA United
Delivery System
Reform Incentive
Payment (DSRIP)
Clinically Integrated Network – Risk Programs
NYUPN
Medicaid IPA UnitedDelivery System
Reform Incentive
Payment (DSRIP)
Clinically Integrated Network – Risk Programs
CARE
Bundled Payment
for Care
Improvement
(BPCI)
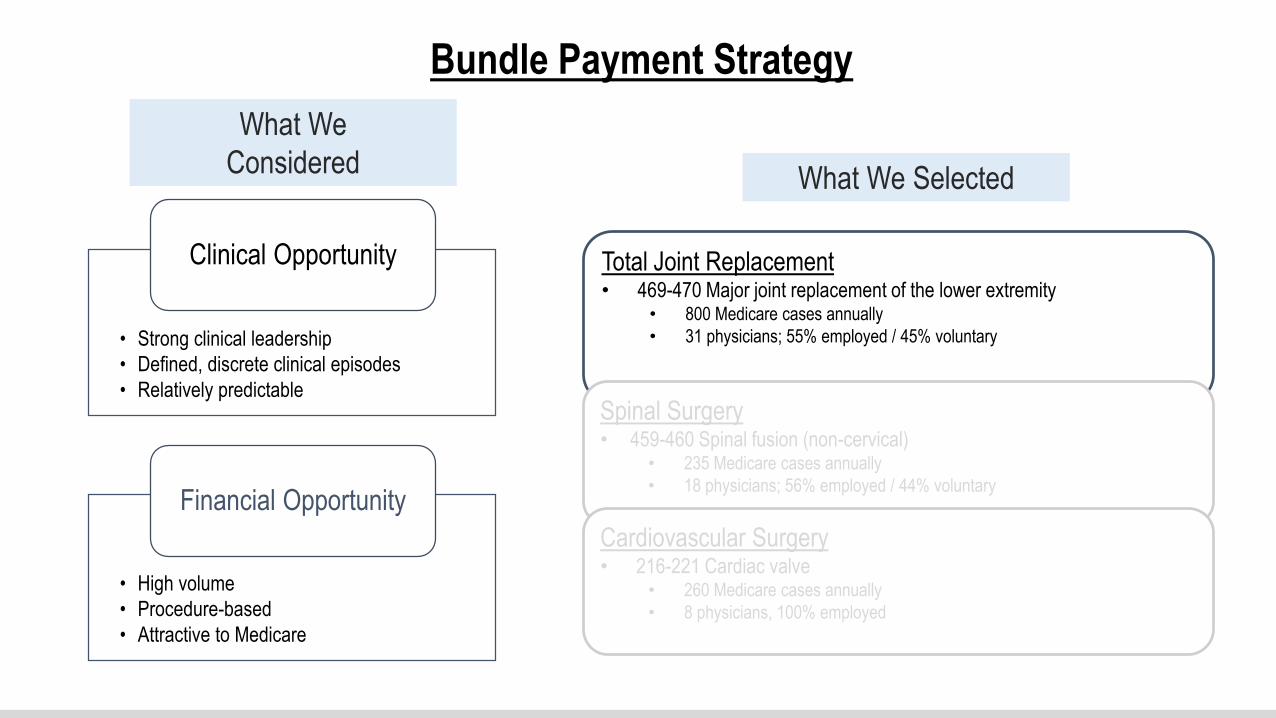
What We
Considered
• Strong clinical leadership
• Defined, discrete clinical episodes
• Relatively predictable
Clinical Opportunity
• High volume
• Procedure-based
• Attractive to Medicare
Financial Opportunity
Total Joint Replacement• 469-470 Major joint replacement of the lower extremity
• 800 Medicare cases annually
• 31 physicians; 55% employed / 45% voluntary
Spinal Surgery• 459-460 Spinal fusion (non-cervical)
• 235 Medicare cases annually
• 18 physicians; 56% employed / 44% voluntary
Cardiovascular Surgery• 216-221 Cardiac valve
• 260 Medicare cases annually
• 8 physicians, 100% employed
Bundle Payment Strategy
What We Selected
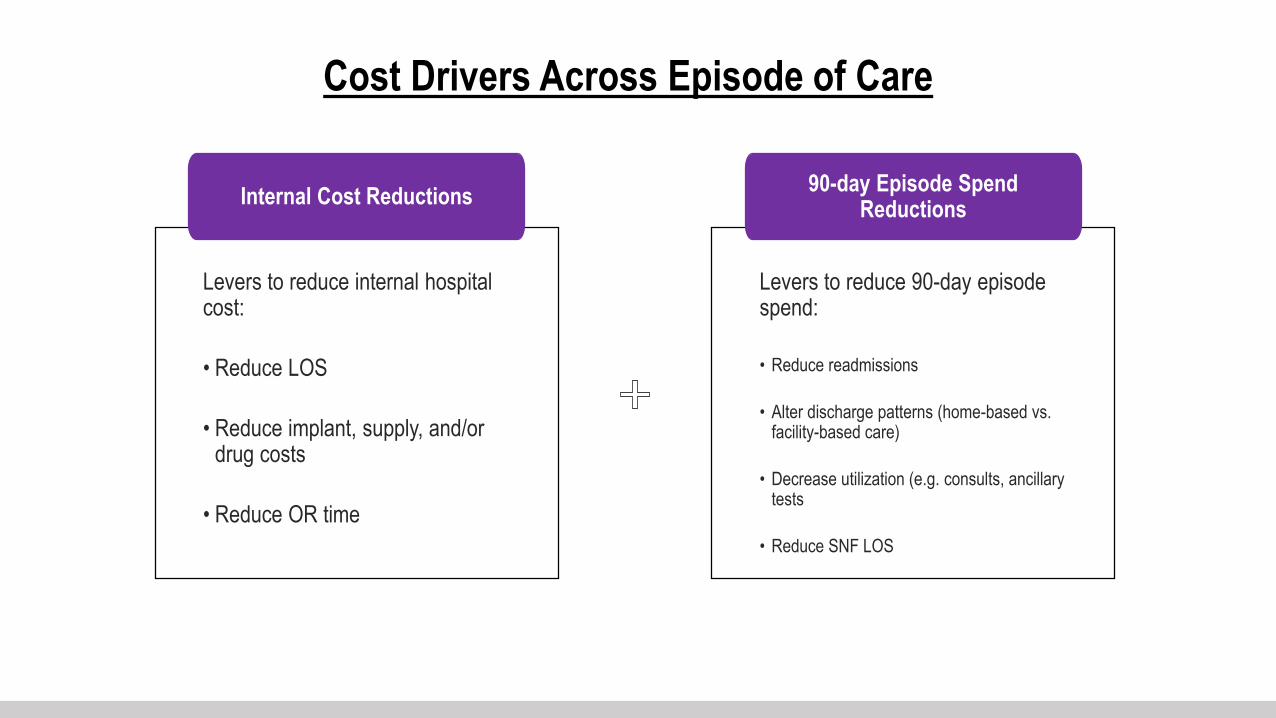
Cost Drivers Across Episode of Care
Levers to reduce internal hospital cost:
• Reduce LOS
• Reduce implant, supply, and/or drug costs
• Reduce OR time
Internal Cost Reductions
Levers to reduce 90-day episode spend:
• Reduce readmissions
• Alter discharge patterns (home-based vs. facility-based care)
• Decrease utilization (e.g. consults, ancillary tests
• Reduce SNF LOS
90-day Episode Spend Reductions

Baseline Metrics – Total Joint Replacement
Initial Post-acute Setting 90 Day Readmission Rate AVG 90-Day Episode Payment
Inpatient Rehab 15% $40,095
Skilled Nursing Facility 18% $43,466
Home Health 10% $23,462
Outpatient Therapy 18% $27,267
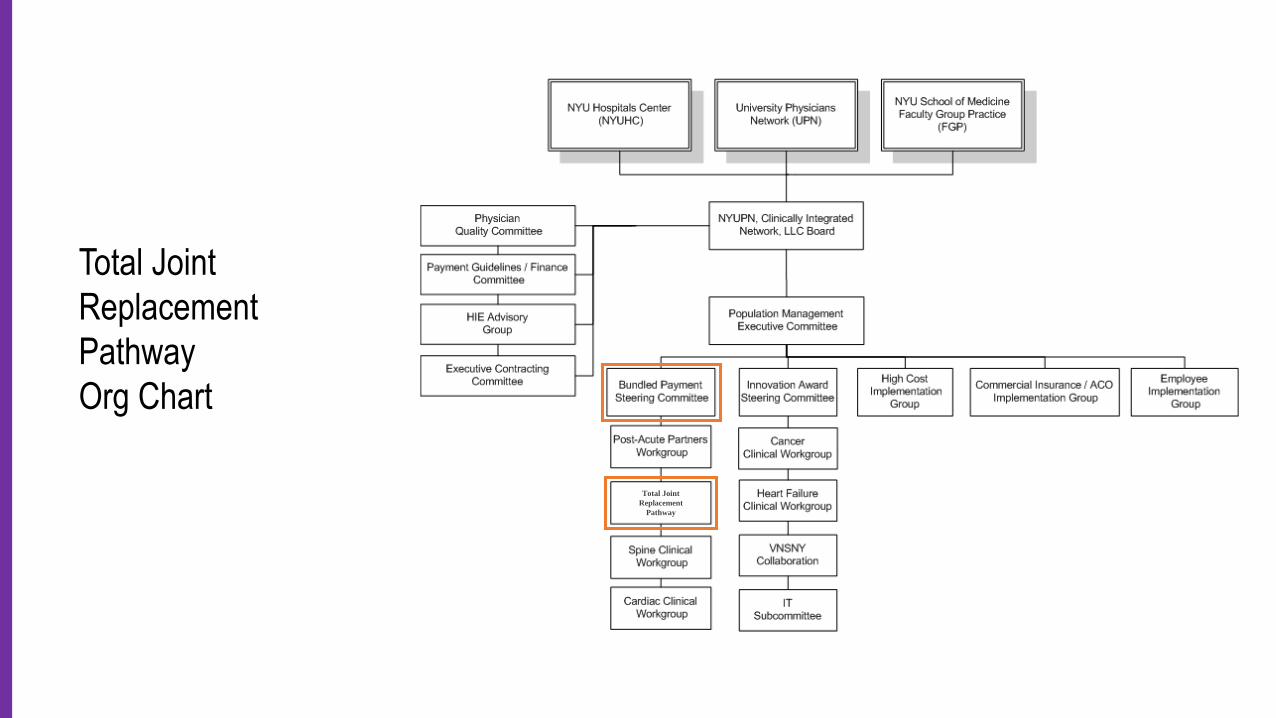
Total Joint
Replacement
Pathway
Org Chart
Total Joint
Replacement
Pathway
Implementation
MCIT Reporting
Epic Workflow
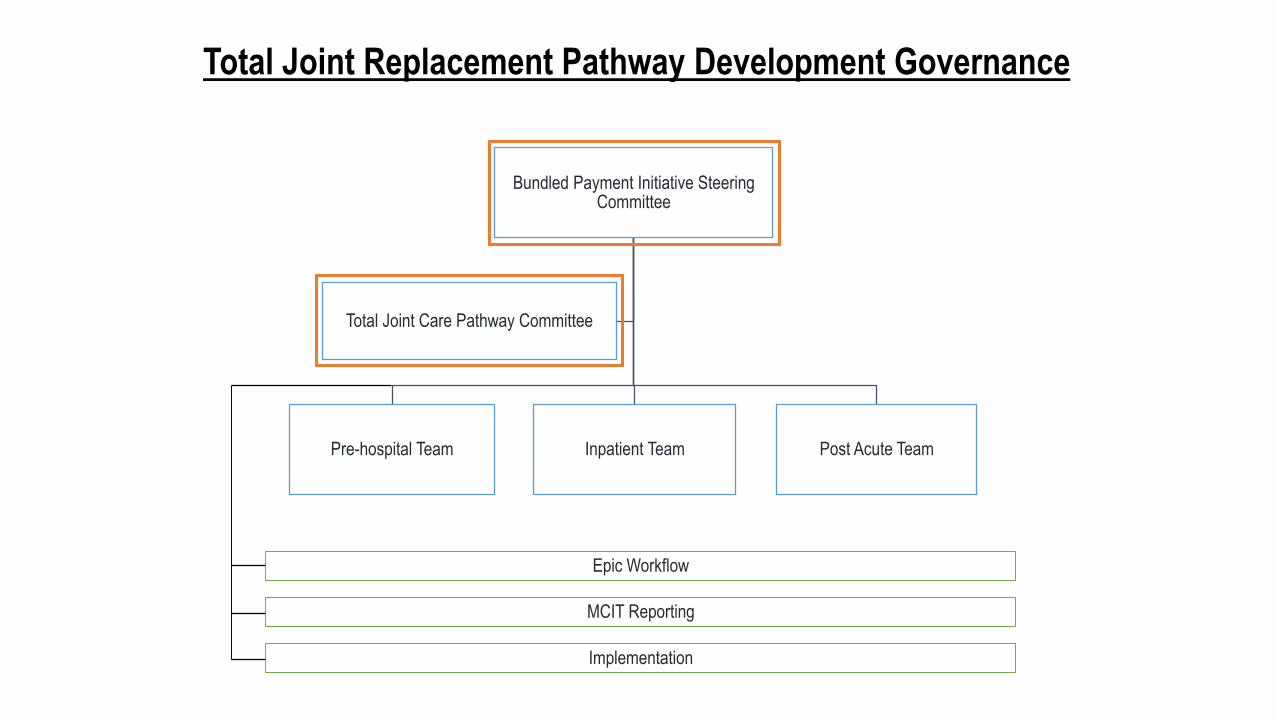
Bundled Payment Initiative Steering Committee
Pre-hospital Team Inpatient Team Post Acute Team
Total Joint Care Pathway Committee
Total Joint Replacement Pathway Development Governance
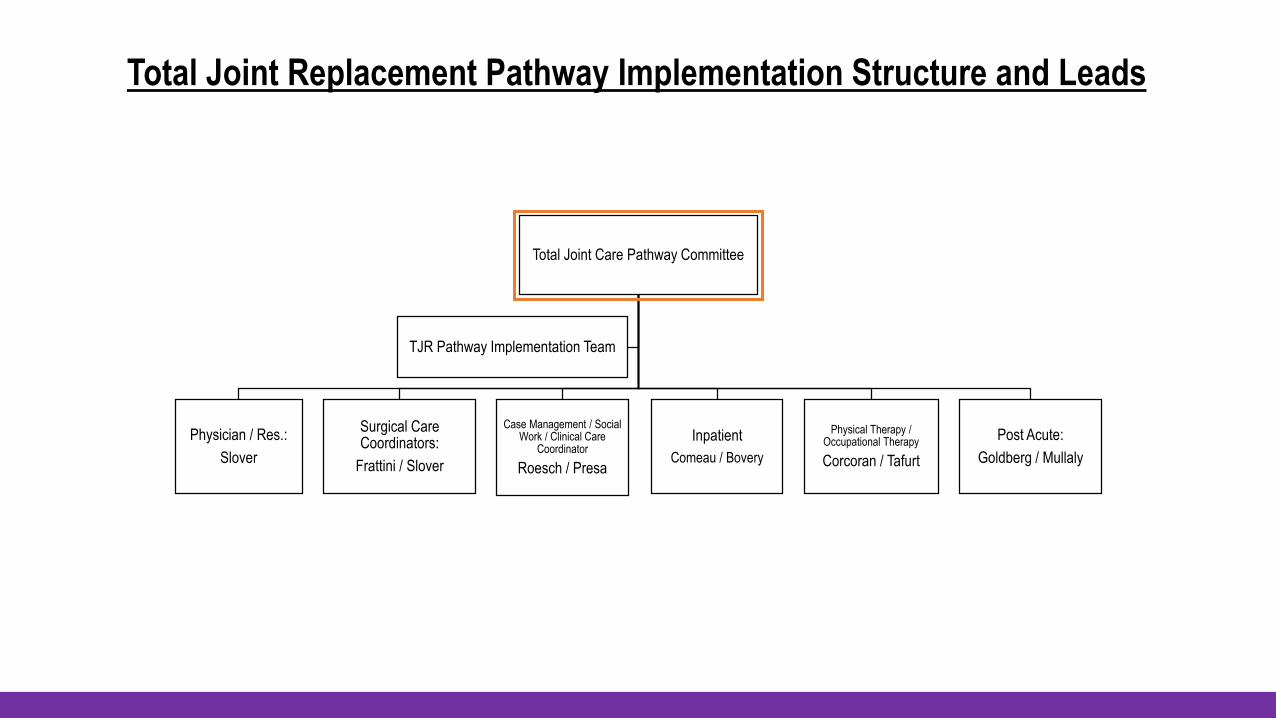
Total Joint Replacement Pathway Implementation Structure and Leads
Total Joint Care Pathway Committee
Physician / Res.:
Slover
Surgical Care Coordinators:
Frattini / Slover
Case Management / Social Work / Clinical Care
Coordinator
Roesch / Presa
Inpatient
Comeau / Bovery
Physical Therapy / Occupational Therapy
Corcoran / Tafurt
Post Acute:
Goldberg / Mullaly
TJR Pathway Implementation Team
Clinical Management Throughout the Pathway
Standardization
Systematization and standardizing
are the foundations of good
operational routines that can be
measured and facilitate
improvements, outcomes, and
ever-greater efficiency.
Advantages of Standardization
1. Increases efficiency
2. Improves ability to monitor and study individual factors
3. Improves communication
4. Allows for identification of outliers or modifiable factors
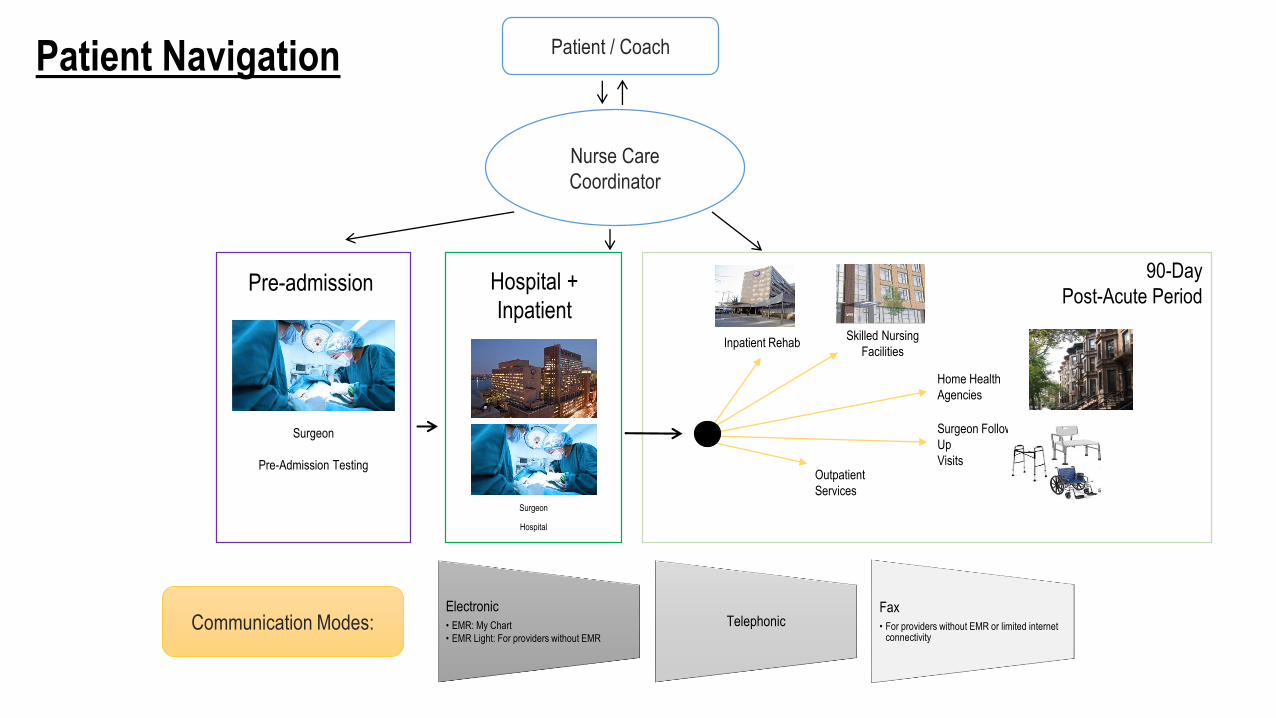
Home Health
Agencies
Surgeon Follow-
Up
Visits
Skilled Nursing
FacilitiesInpatient Rehab
90-Day
Post-Acute Period
Surgeon
Pre-Admission TestingOutpatient
Services
Nurse Care
Coordinator
Patient / Coach
Electronic
• EMR: My Chart
• EMR Light: For providers without EMR
TelephonicFax
• For providers without EMR or limited internet connectivity
Communication Modes:
Pre-admission Hospital +
Inpatient
Patient Navigation
Surgeon
Hospital
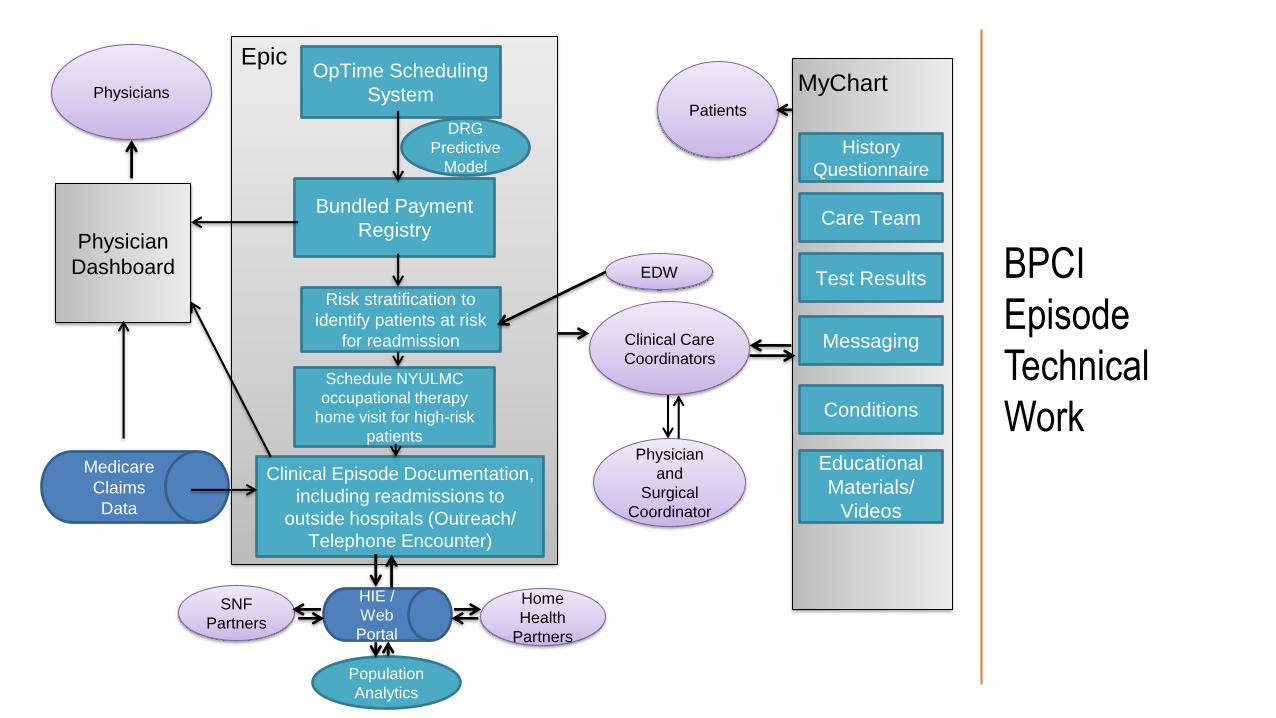
MyChartEpic
Physician
Dashboard
Bundled Payment
Registry
OpTime Scheduling
System
DRG
Predictive
Model
Clinical Episode Documentation,
including readmissions to
outside hospitals (Outreach/
Telephone Encounter)
Clinical Care
Coordinators
HIE /
Web
Portal
Medicare
Claims
Data
Physician
and
Surgical
Coordinator
History
Questionnaire
Test Results
Conditions
Care Team
Messaging
Educational
Materials/
Videos
PhysiciansPatients
Schedule NYULMC
occupational therapy
home visit for high-risk
patients
Risk stratification to
identify patients at risk
for readmission
SNF
Partners
Home
Health
Partners
EDW
Population
Analytics
BPCI
Episode
Technical
Work
Reporting and Monitoring Tools –
Pre-Care Outcomes Improvement
∴ DRG Predictor
∴ Reporting
∴ Care Coordinator Dashboard
∴ High Risk Readmission Identifier

Surgery
Date
Pre-
Testing
Date
Patient
Name
Patient Age on
Surgery Date Surgeon Name Procedure Home Phone Email Address Birth Date
Patient
PCP Name
PCP Office
Phone Num Schedule Status
10/15/2013 5/8/2013 Patient 1 69.5 Surgeon 1 ROBOTIC MITRAL VALVE ANNULOPLASTY Phone 1 Email 1 DOB 1 PCP 1 PCP 1 Scheduled
10/15/2013 10/1/2013 Patient 2 62.2 Surgeon 2 REVISION FUSION SPINAL POSTERIOR Phone 2 Email 2 DOB 2 PCP 2 PCP 2 Scheduled
10/15/2013 10/2/2013 Patient 3 70.9 Surgeon 3 REPLACEMENT HIP TOTAL Phone 3 Email 3 DOB 3 PCP 3 PCP 3 Scheduled
10/15/2013 10/4/2013 Patient 4 88.6 Surgeon 4 REPLACEMENT KNEE TOTAL Phone 4 Email 4 DOB 4 PCP 4 PCP 4 Scheduled
10/15/2013 10/4/2013 Patient 5 71.5 Surgeon 5 REPLACEMENT HIP TOTAL Phone 5 Email 5 DOB 5 PCP 5 PCP 5 Scheduled
DRG Predictor - Scheduled procedure report kicks off
outreach efforts pre-surgery
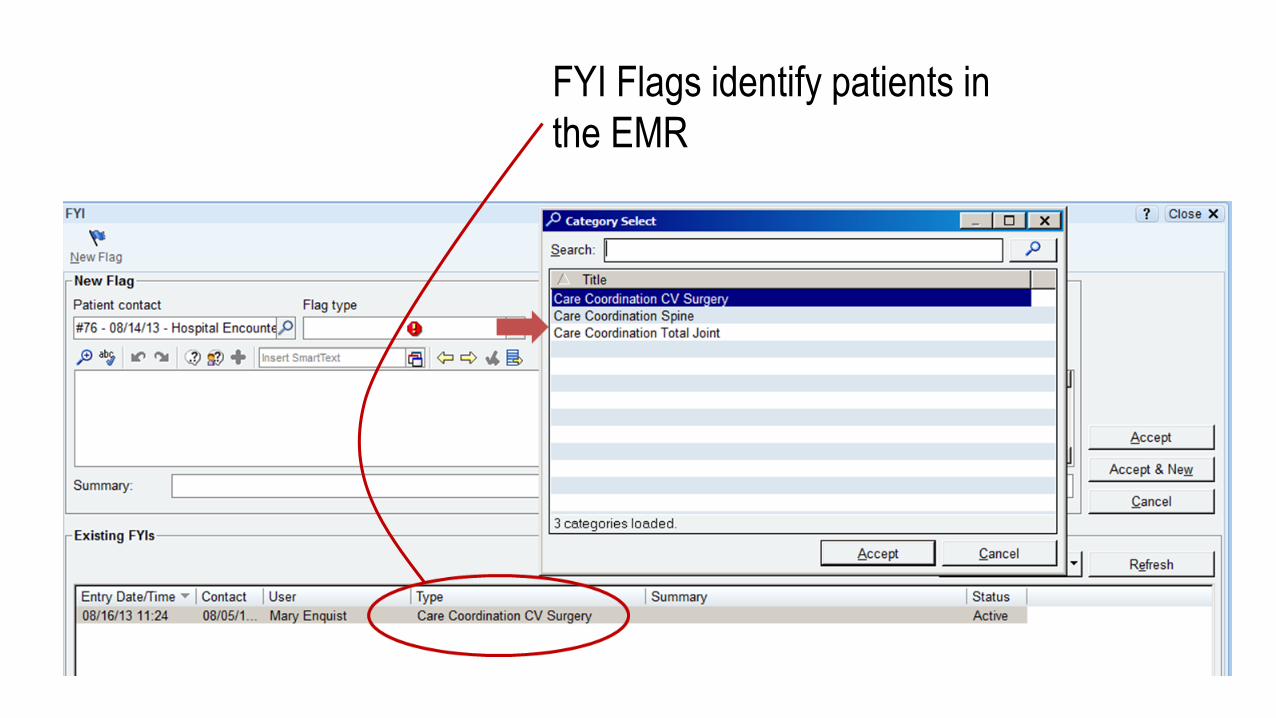
FYI Flags identify patients in
the EMR
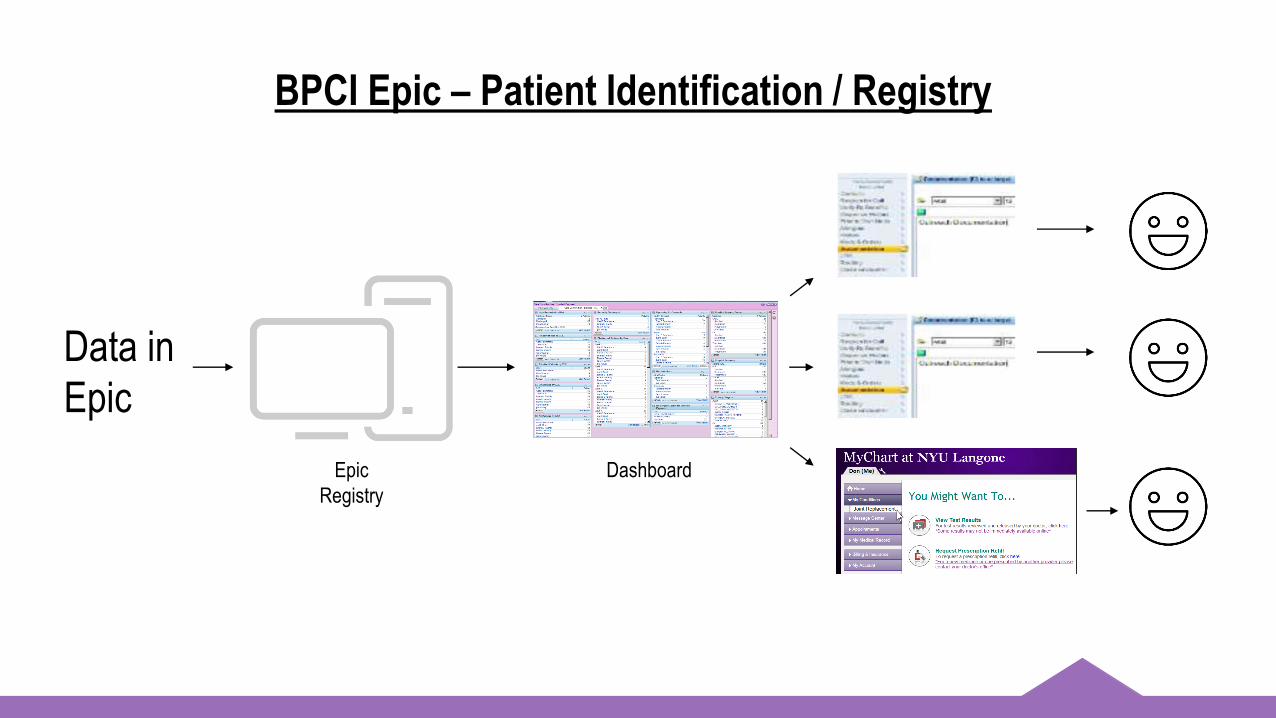
Data in
Epic
Epic
Registry
Dashboard
BPCI Epic – Patient Identification / Registry

EMR Care Coordination Tools and Patient Registries
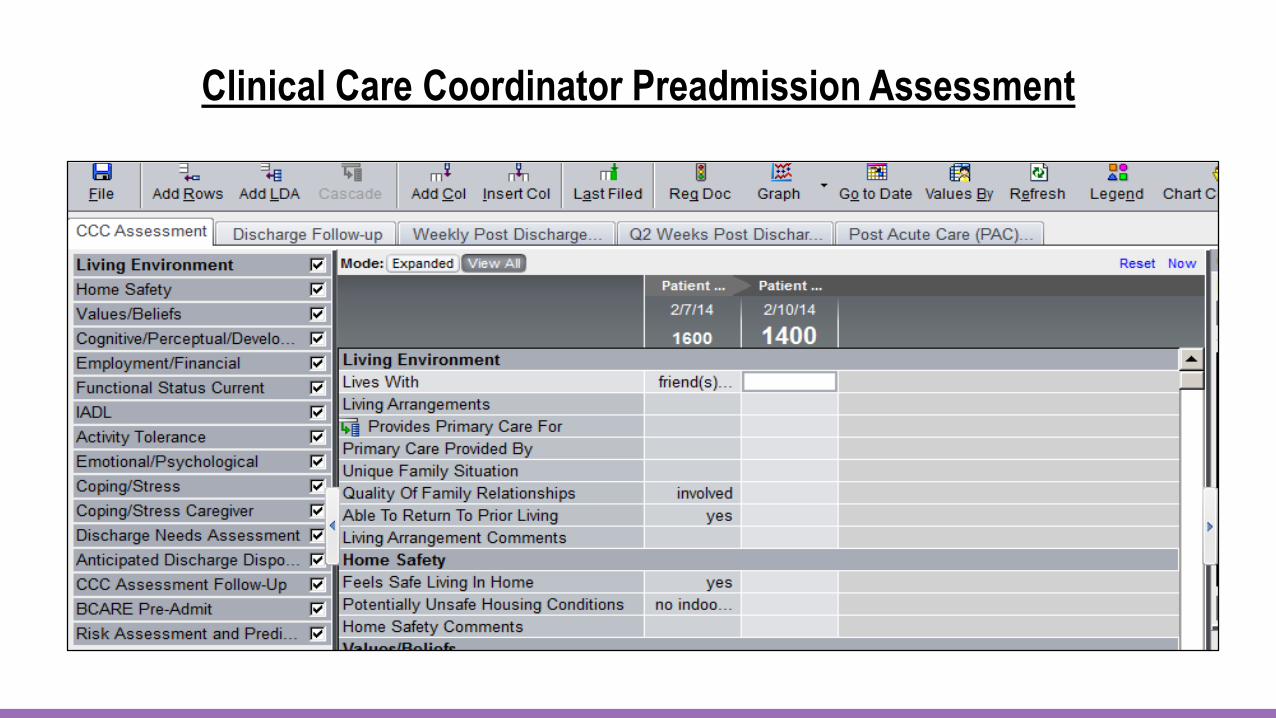
Clinical Care Coordinator Preadmission Assessment
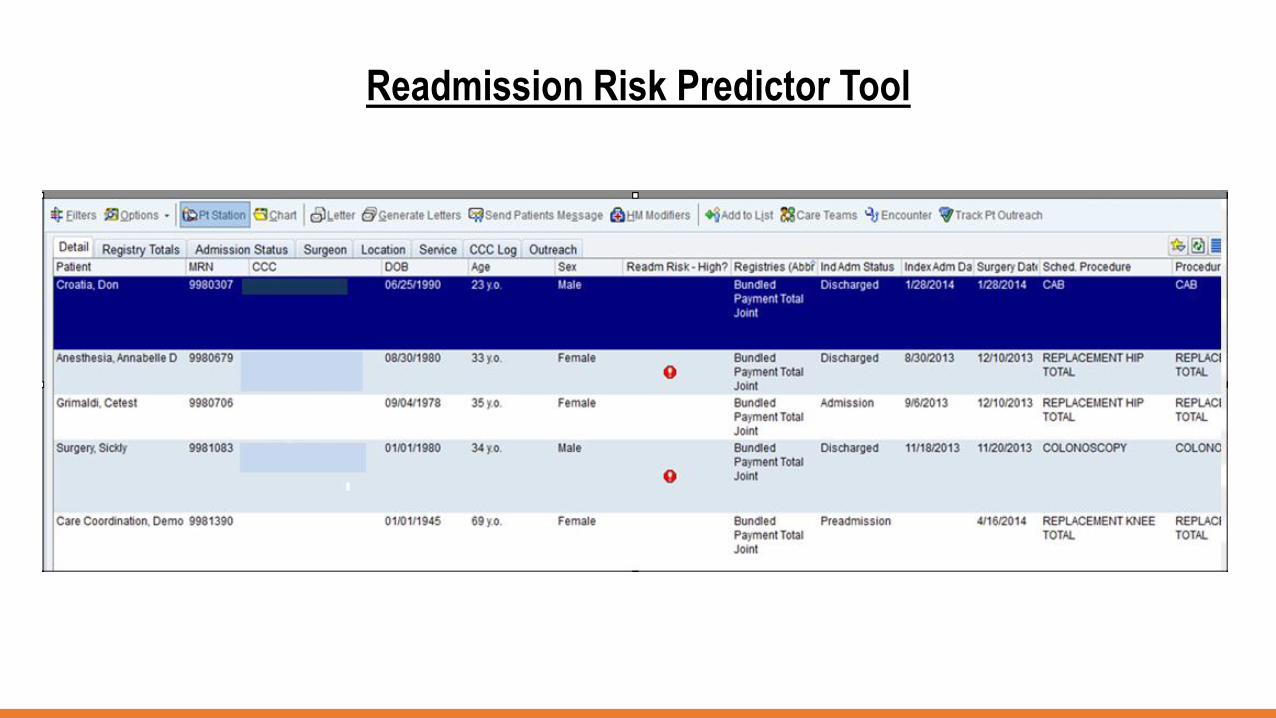
Readmission Risk Predictor Tool
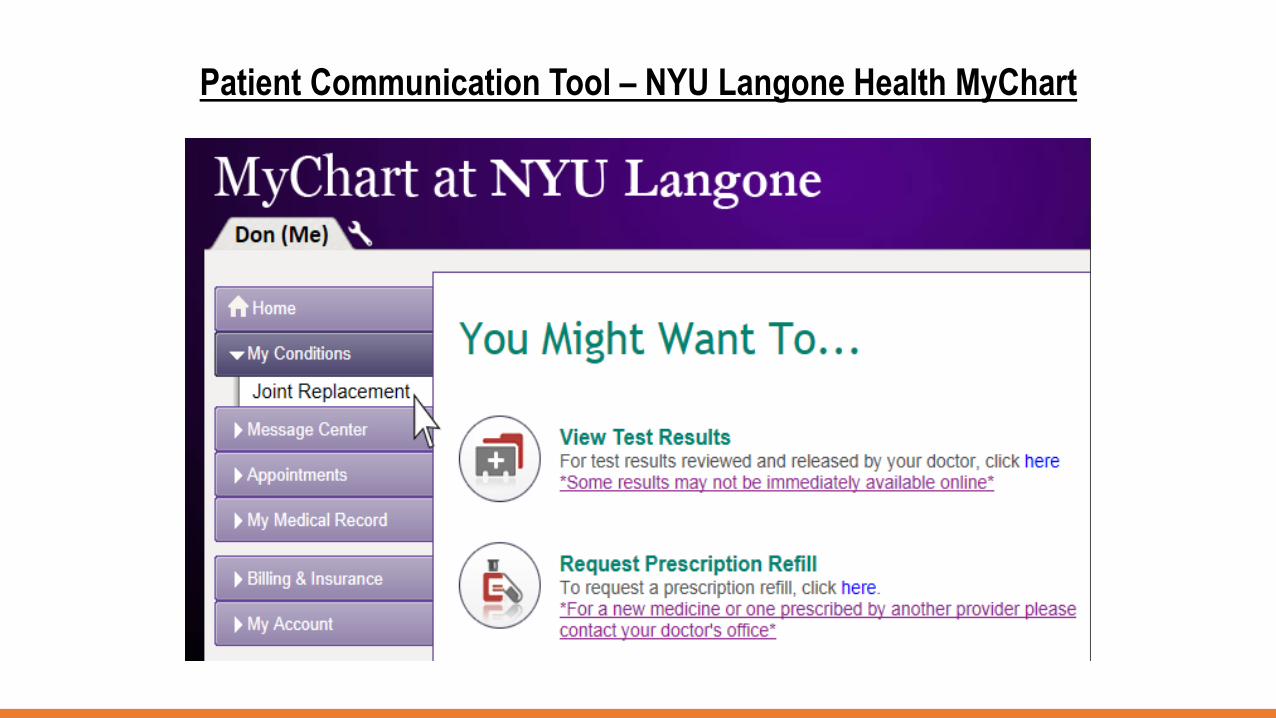
Patient Communication Tool – NYU Langone Health MyChart

Inpatient Workflow + Order Sets –
During-Care Outcomes Improvement
∴ Order Sets
∴ Epic Dashboard
∴ Reporting
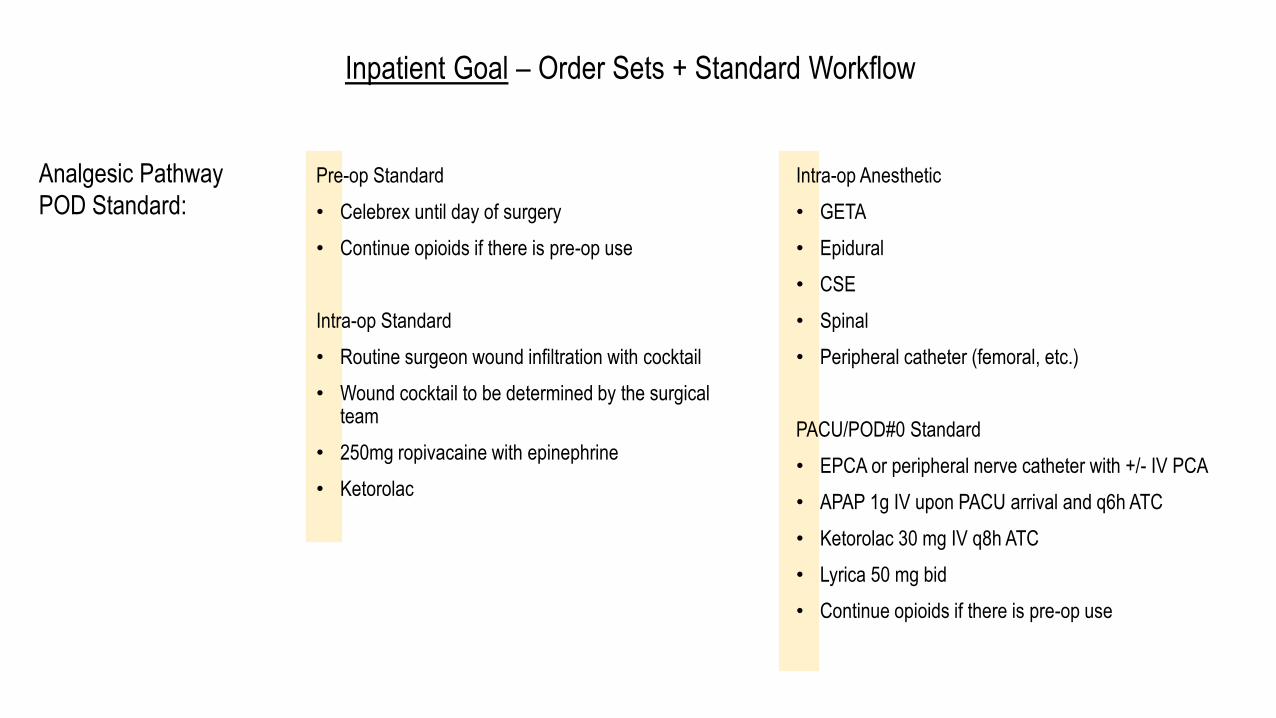
Pre-op Standard
• Celebrex until day of surgery
• Continue opioids if there is pre-op use
Intra-op Standard
• Routine surgeon wound infiltration with cocktail
• Wound cocktail to be determined by the surgical team
• 250mg ropivacaine with epinephrine
• Ketorolac
Inpatient Goal – Order Sets + Standard Workflow
Analgesic Pathway
POD Standard:
Intra-op Anesthetic
• GETA
• Epidural
• CSE
• Spinal
• Peripheral catheter (femoral, etc.)
PACU/POD#0 Standard
• EPCA or peripheral nerve catheter with +/- IV PCA
• APAP 1g IV upon PACU arrival and q6h ATC
• Ketorolac 30 mg IV q8h ATC
• Lyrica 50 mg bid
• Continue opioids if there is pre-op use

Analgesic
Workflow
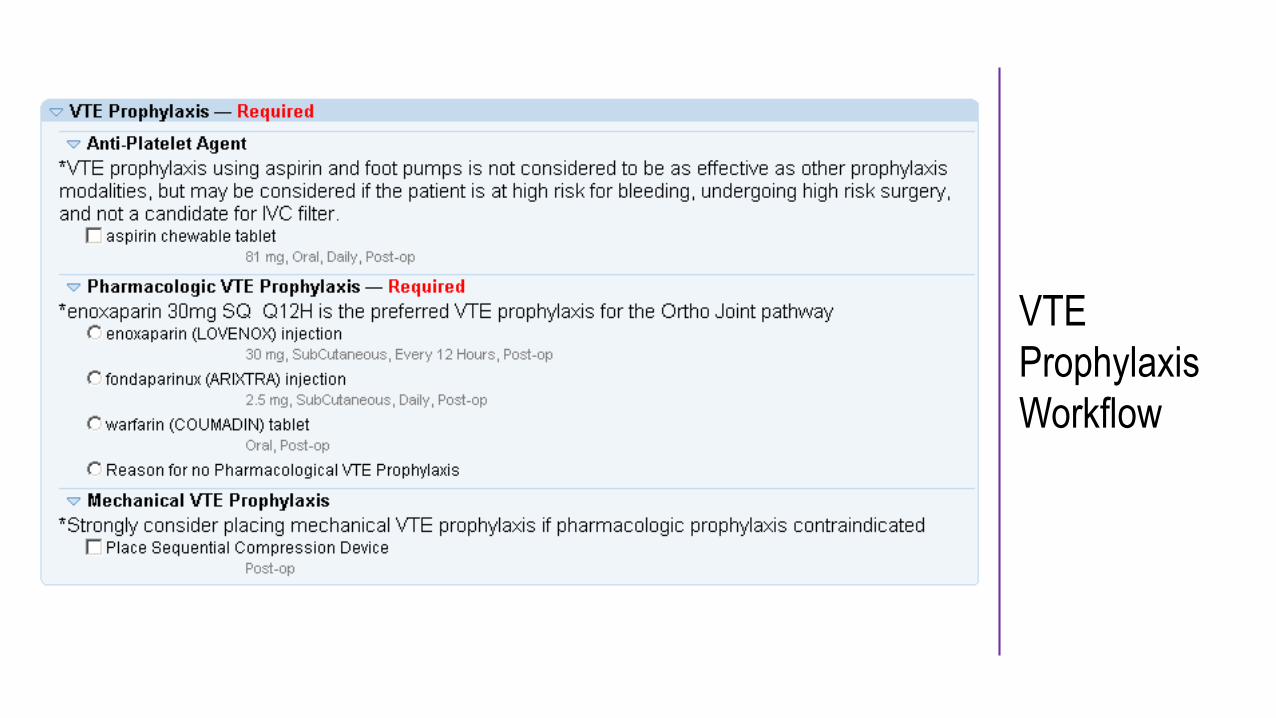
VTE
Prophylaxis
Workflow
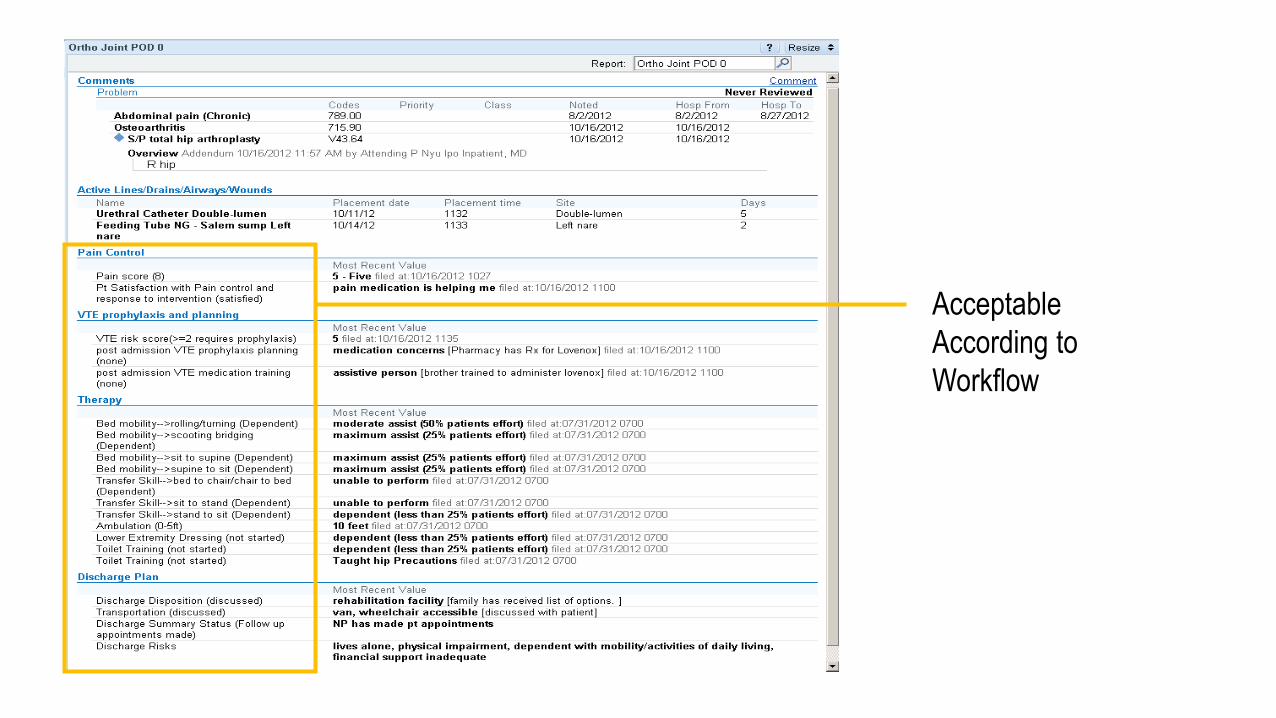
Acceptable
According to
Workflow
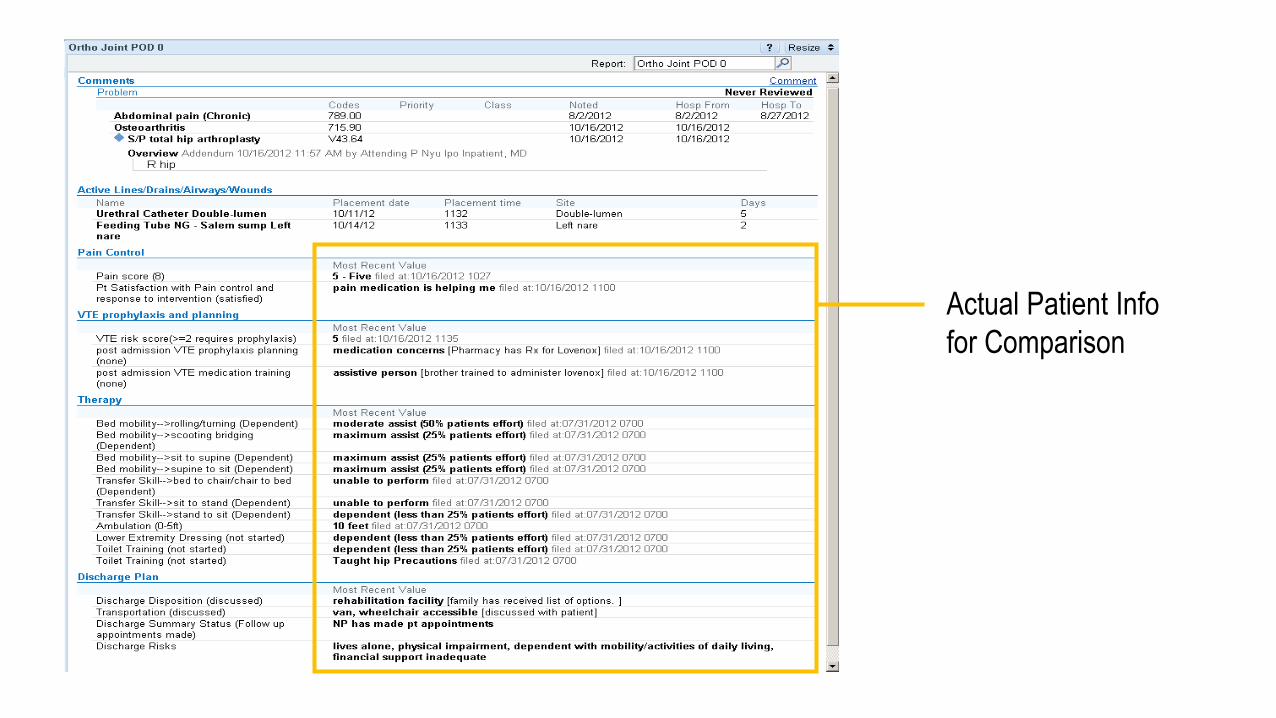
Actual Patient Info
for Comparison

Daily Inpatient Census Report

Homecare Workflow–
Post-Care Outcomes Improvement
∴ Care Coordinator Post-Acute Documentation
∴ Transitional Care Document
∴ Analytics
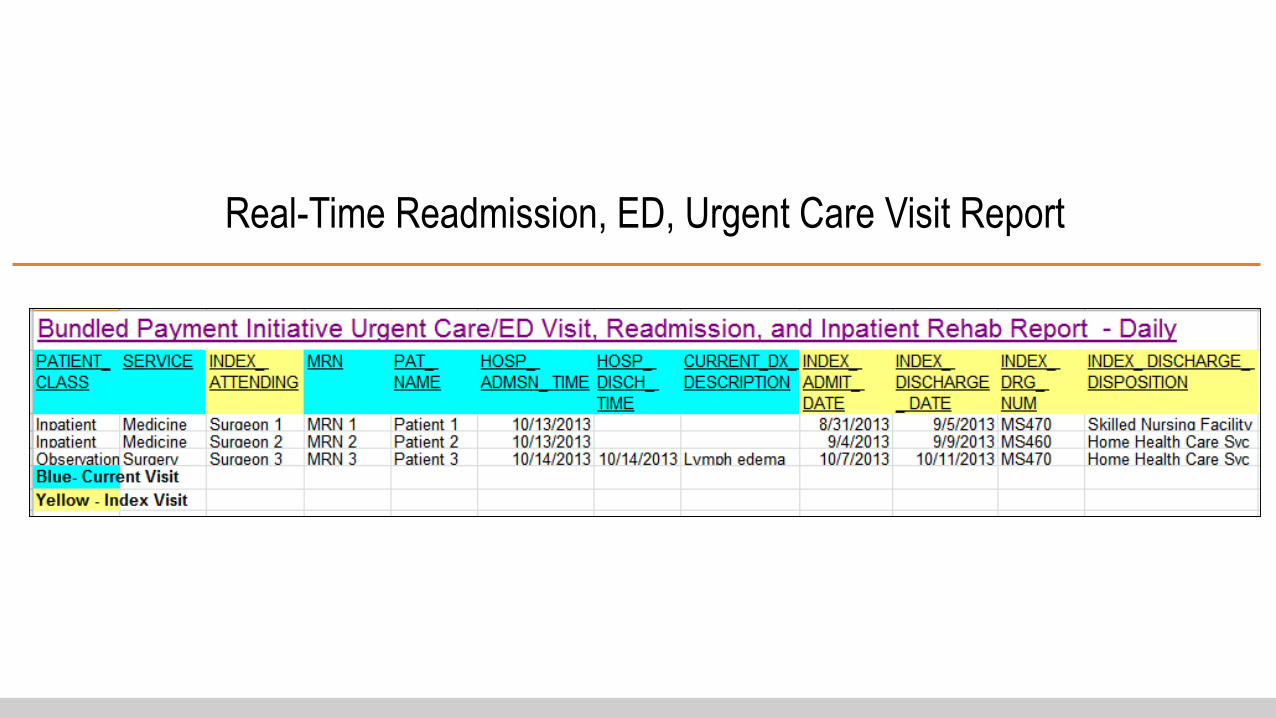
Real-Time Readmission, ED, Urgent Care Visit Report
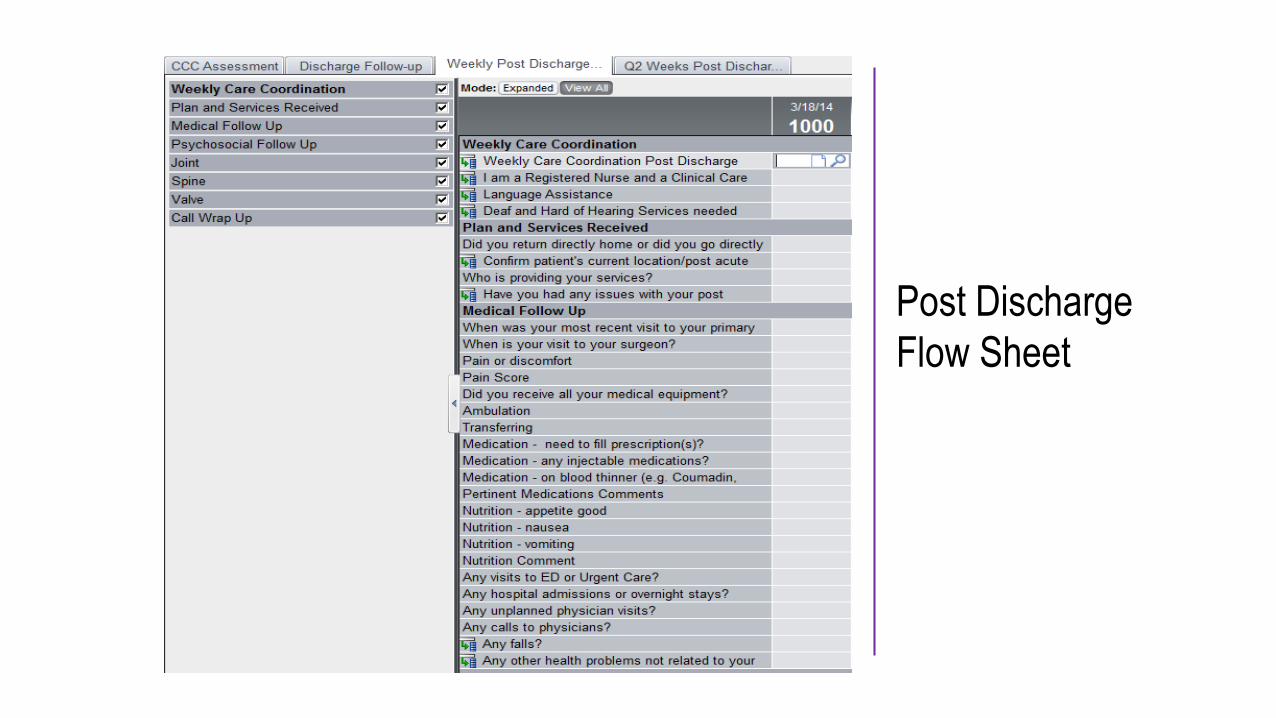
Post Discharge
Flow Sheet

Post Acute Care Provider Contact
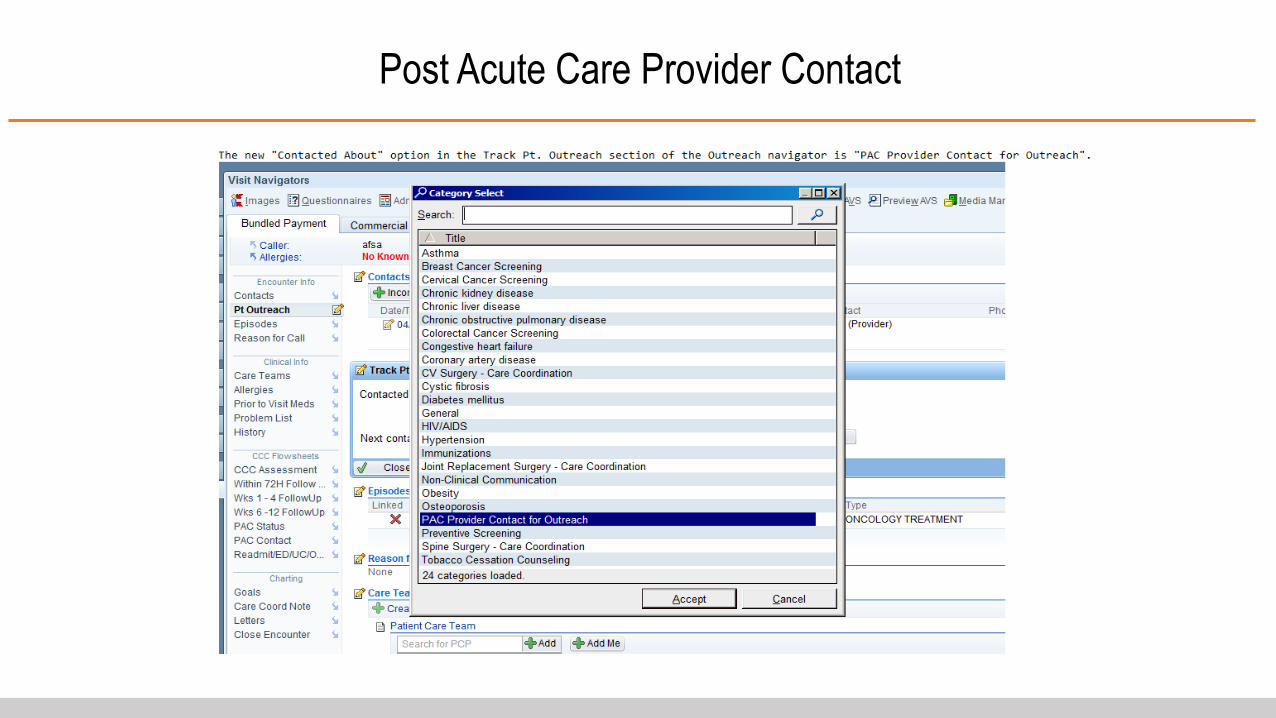
Post Acute Care Provider Contact
• Focus on bi-directional exchange of information
• Twice weekly updates on high risk patients
• Interdisciplinary weekly call
• PAC Report card
• Quarterly PAC Committee Meeting
Developed in collaboration with Partners
Standard Post Acute Pathways
Post Acute Goal –Improved Outcomes and Patient Experience NYULMC Post-Acute Partners
8
12
8
6
7
9
3
5
4
3
3
• Two Home Care Pathways
• Standard Pathway
• Enhanced Support Pathway
• VNSNY/TJR Enhanced Support Pathway Pilot Criteria
• Single Joint replacement
• Caregiver able to participate in therapy prior to DC
• Stairs before discharge / No more that 1 flight in home
• If private home bed/bath cant be longer than a flight of stairs
• Eligible for SNF / Complex Needs
• Established risk profile to assist in determining appropriate disposition
• Focus on bi-directional electronic exchange of information
Criteria for
Homecare
Transitional Care Document –
Post-Care Outcomes Improvement
∴ Transfer Document
∴ Follow-up Form
∴ Continuity of Care Document
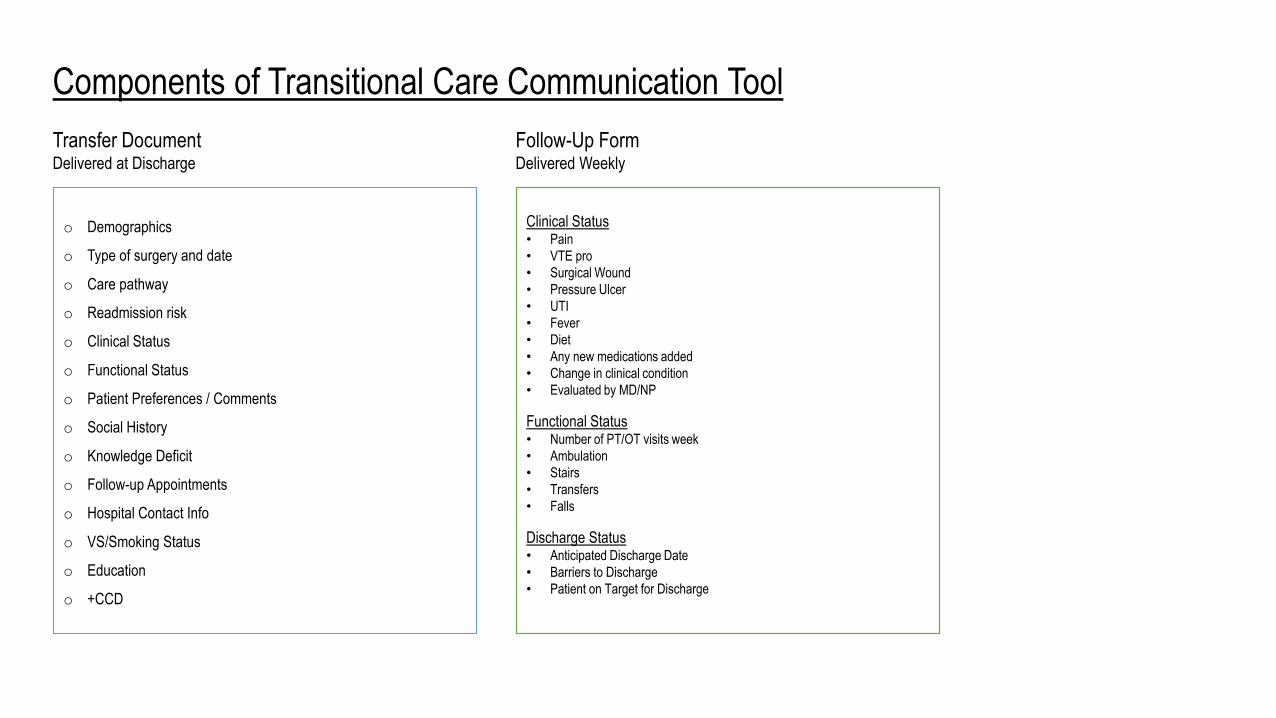
Components of Transitional Care Communication Tool
Transfer DocumentDelivered at Discharge
o Demographics
o Type of surgery and date
o Care pathway
o Readmission risk
o Clinical Status
o Functional Status
o Patient Preferences / Comments
o Social History
o Knowledge Deficit
o Follow-up Appointments
o Hospital Contact Info
o VS/Smoking Status
o Education
o +CCD
Clinical Status• Pain
• VTE pro
• Surgical Wound
• Pressure Ulcer
• UTI
• Fever
• Diet
• Any new medications added
• Change in clinical condition
• Evaluated by MD/NP
Functional Status• Number of PT/OT visits week
• Ambulation
• Stairs
• Transfers
• Falls
Discharge Status• Anticipated Discharge Date
• Barriers to Discharge
• Patient on Target for Discharge
Follow-Up FormDelivered Weekly
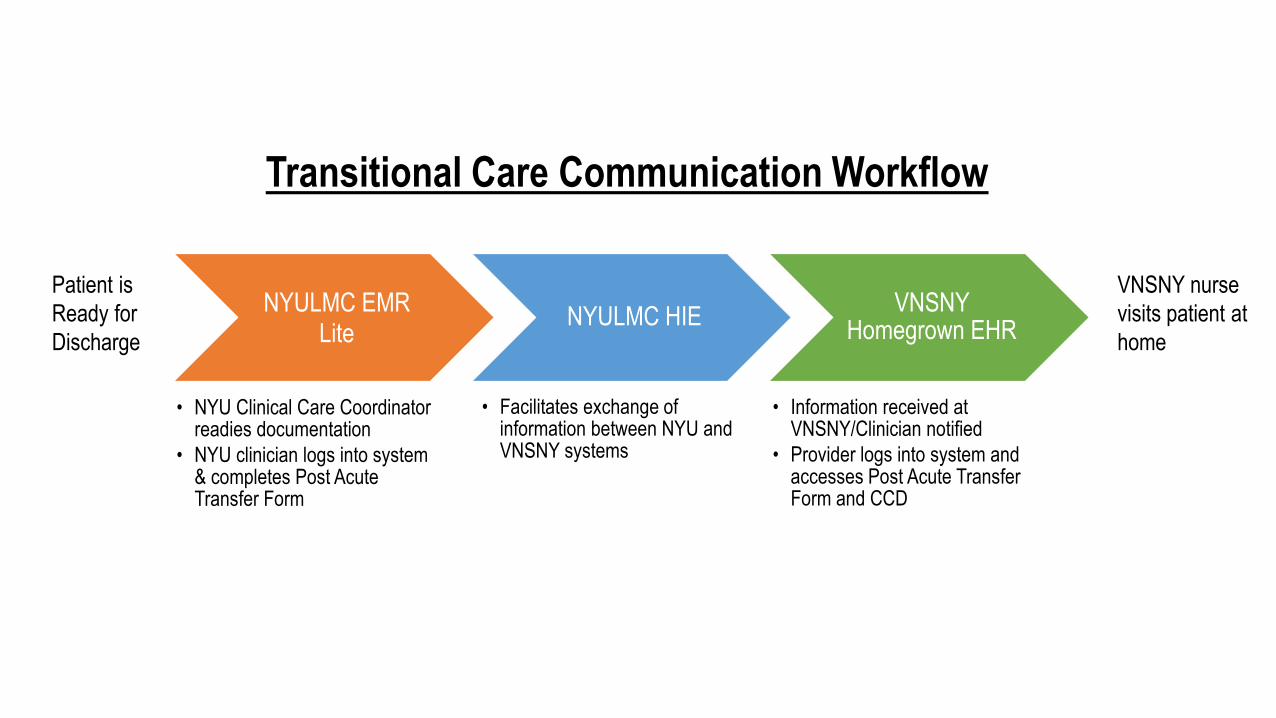
NYULMC EMR Lite
• NYU Clinical Care Coordinator readies documentation
• NYU clinician logs into system & completes Post Acute Transfer Form
NYULMC HIE
• Facilitates exchange of information between NYU and VNSNY systems
VNSNY Homegrown EHR
• Information received at VNSNY/Clinician notified
• Provider logs into system and accesses Post Acute Transfer Form and CCD
Transitional Care Communication Workflow
Patient is
Ready for
Discharge
VNSNY nurse
visits patient at
home
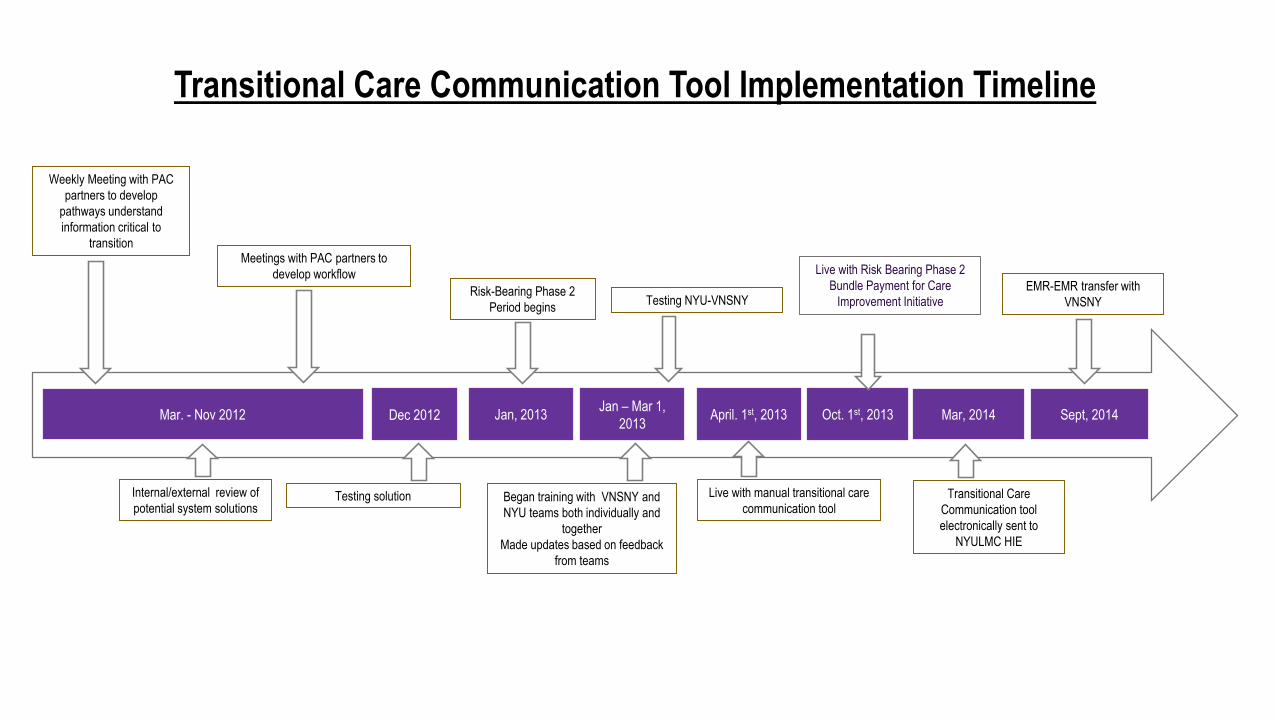
Weekly Meeting with PAC
partners to develop
pathways understand
information critical to
transition
Testing NYU-VNSNY
Mar. - Nov 2012 April. 1st, 2013 Sept, 2014
EMR-EMR transfer with
VNSNYRisk-Bearing Phase 2
Period begins
Oct. 1st, 2013
Live with manual transitional care
communication tool
Mar, 2014
Transitional Care
Communication tool
electronically sent to
NYULMC HIE
Internal/external review of
potential system solutions
Meetings with PAC partners to
develop workflow
Testing solution
Dec 2012 Jan, 2013
Began training with VNSNY and
NYU teams both individually and
together
Made updates based on feedback
from teams
Live with Risk Bearing Phase 2
Bundle Payment for Care
Improvement Initiative
Transitional Care Communication Tool Implementation Timeline
Jan – Mar 1,
2013
We have exchanged over
7,000 forms with VNSNY
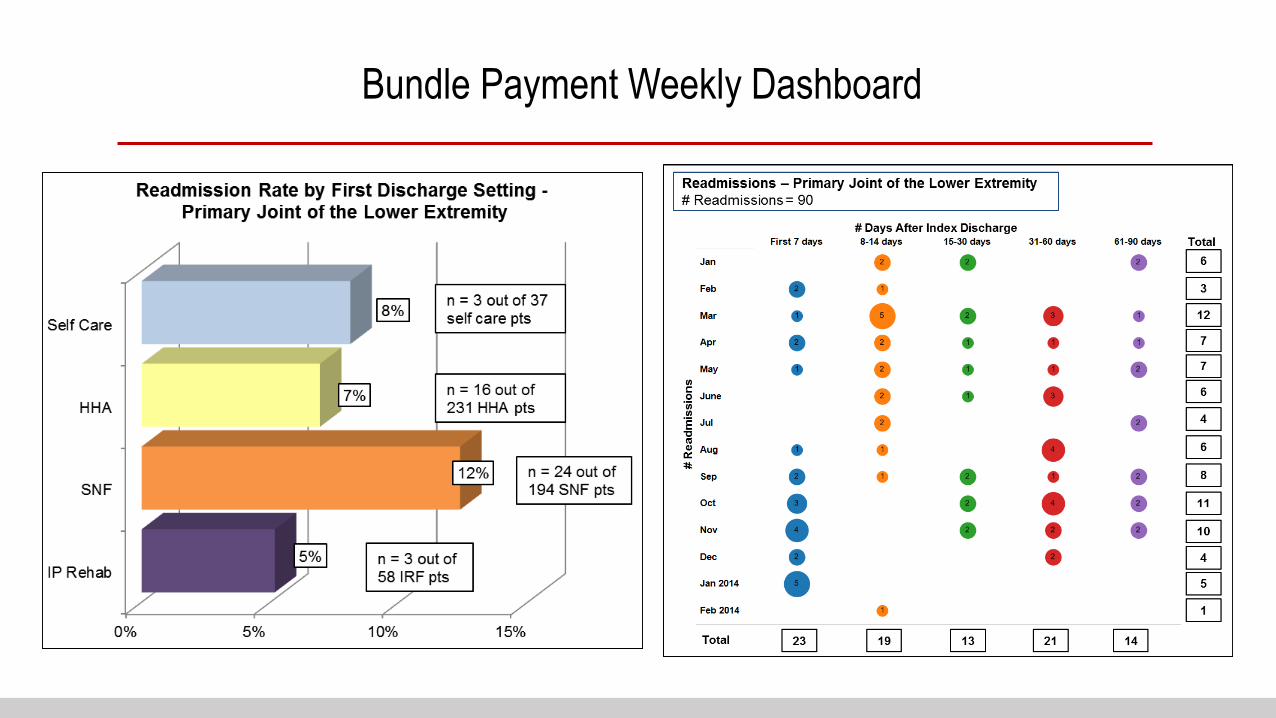
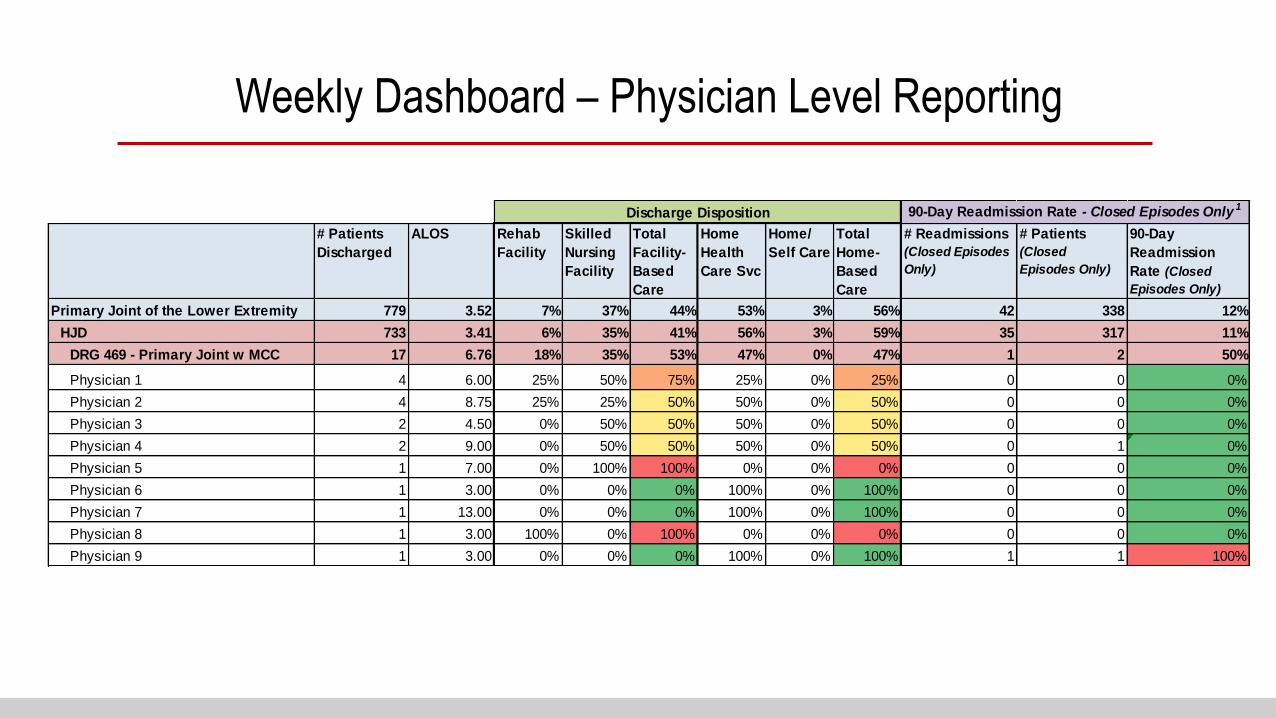
Bundle Payment Weekly Dashboard
# Patients
Discharged
ALOS Rehab
Facility
Skilled
Nursing
Facility
Total
Facility-
Based
Care
Home
Health
Care Svc
Home/
Self Care
Total
Home-
Based
Care
# Readmissions
(Closed Episodes
Only)
# Patients
(Closed
Episodes Only)
90-Day
Readmission
Rate (Closed
Episodes Only)
Primary Joint of the Lower Extremity 779 3.52 7% 37% 44% 53% 3% 56% 42 338 12%
HJD 733 3.41 6% 35% 41% 56% 3% 59% 35 317 11%
DRG 469 - Primary Joint w MCC 17 6.76 18% 35% 53% 47% 0% 47% 1 2 50%
Physician 1 4 6.00 25% 50% 75% 25% 0% 25% 0 0 0%
Physician 2 4 8.75 25% 25% 50% 50% 0% 50% 0 0 0%
Physician 3 2 4.50 0% 50% 50% 50% 0% 50% 0 0 0%
Physician 4 2 9.00 0% 50% 50% 50% 0% 50% 0 1 0%
Physician 5 1 7.00 0% 100% 100% 0% 0% 0% 0 0 0%
Physician 6 1 3.00 0% 0% 0% 100% 0% 100% 0 0 0%
Physician 7 1 13.00 0% 0% 0% 100% 0% 100% 0 0 0%
Physician 8 1 3.00 100% 0% 100% 0% 0% 0% 0 0 0%
Physician 9 1 3.00 0% 0% 0% 100% 0% 100% 1 1 100%
90-Day Readmission Rate - Closed Episodes Only 1Discharge Disposition
Weekly Dashboard – Physician Level Reporting
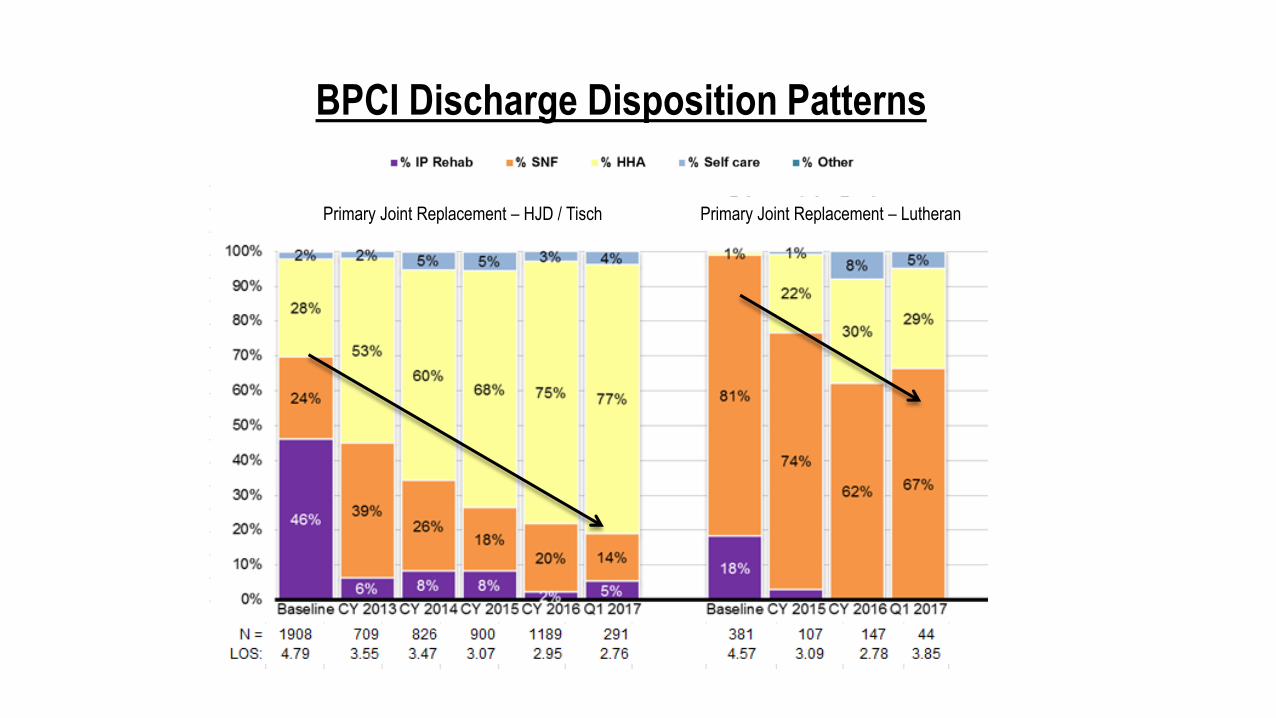
BPCI Discharge Disposition Patterns
Primary Joint Replacement – HJD / Tisch Primary Joint Replacement – Lutheran
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
Baseline CY 2013 CY 2014 CY 2015 CY 2016 CY 2017
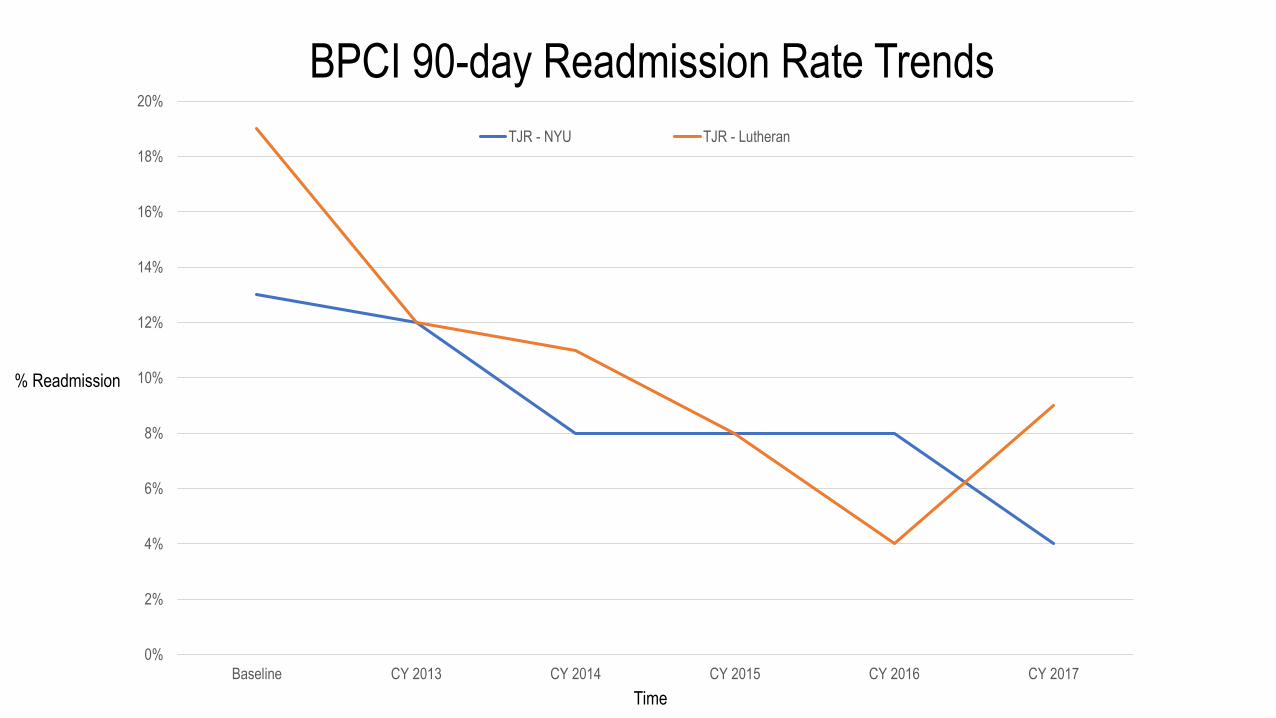
BPCI 90-day Readmission Rate Trends
TJR - NYU TJR - Lutheran
% Readmission
Time
0
2
4
6
8
10
12
Baseline CY 2013 CY 2014 CY 2015 CY 2016 CY 2017
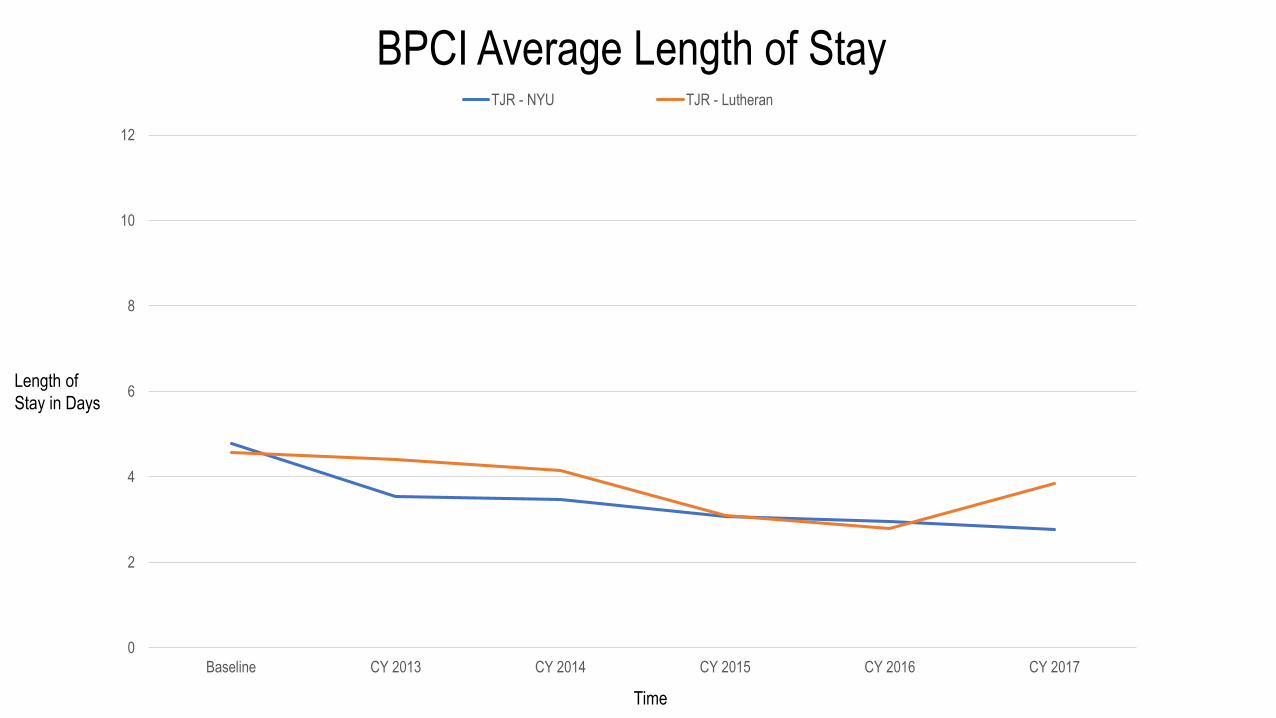
BPCI Average Length of StayTJR - NYU TJR - Lutheran
Time
Length of
Stay in Days

Lessons Learned
- Concept of bundle payment is still very new
- Continuous engagement requires reminders – re-education around reports, and data, new goals and targets, and regular discussion of performance
- Data is consumed and understood differently by different groups
- Leverage IT platforms (EMR, HIE, analytics) to identify population of interest at preadmission and during inpatient stay
- Early identification of BPCI patients is critical to success
- Place focused information in the hands of clinicians on a timely basis in order to facilitate care redesign
- Develop tools to risk stratify patients to allow targeted clinical intervention
- Developed and tested Care Coordination workflow manually
- Advance clinical and technical relationships with post acute partners to expand influence with care delivery

Questions

In Summary
VBM
Pathways
Paperless
Registration
Total Joint
Arthroplasty
Bundled Payment
Care Initiative
BPCI Discharge Disposition Patterns
Primary Joint Replacement – HJD / Tisch Primary Joint Replacement – Lutheran

Thank you
for your consideration.