Embed Size (px)
Citation preview

Welcome to the WJB Dorn
VA Medical Center
061118
Leadership
David L. Omura, DPT, MHA, MS
Medical Center Director
Jeff Soots
Associate Medical Center Director
Angelia Scott
Assistant Director
Bernard L. DeKoning, MD
Chief of Staff
Ruth Mustard, RN, MSN
Associate Director for Patient Care/Nursing Services

Mission and Vision
Our Mission: Veteran Focused, Performance Driven Health
Care
Our Vision: The Wm. Jennings Bryan Dorn VA Medical Center
will be recognized as a leading medical center in South
Carolina and one of the best in the Nation. We will be at the
forefront in areas of efficiency, innovation, quality, patient
centered care and employee satisfaction

Overview
• Opened in 1932
• 97 total acres
• 206-bed Medical center
• Over 83,000 Unique Patients
• Over 8,400 Women Veterans
• Over 1M outpatient visits
• 4,000 inpatient admissions
• Over 2650 FTEE
• FY18 Budget over $530M
• Over $114 M in new construction projects approved
• HEP C – More than 1400 veterans have been started on
treatment with a 98% cure rate and an emphasis on
outreach and rural areas
• State of the art Sim Center built in collaboration with the
University of South Carolina School of Medicine
Leading the Way

• Summer Student Program with over 70 graduates in
2018
• Affiliated with USC and more than 91 institutions of
higher education and 26 disciplines
• 152 Academic Affiliations, with over 800 annual trainee
rotations
Training Tomorrow’s Health Care Professionals
• Establishing a Community Care Network Transition Team to implement Mission Act requirements
• Columbia POCs
– Steve Garver, Chief (803)776-4000 x6604 [email protected]
– Walter Harper, Manager (803)776-4000 x7202 [email protected]
• Stopped sending referrals to HealthNet as of June 30, 2018.
Community Care

Community CareFY 18 Top 20 Community Care Authorizations Created
Category of Care # of Authorizations
NIC HOMEMAKER/HOME HEALTH AID 1348
DENTAL 1174
RADIOLOGY MAMMOGRAM 1026
INPATIENT 923
ER VISIT/URGENT CARE 648
NEUROSURGERY 624
OPHTHALMOLOGY 621
NEPHROLOGY 511
RADIATION THERAPY 417
UROLOGY 323
NIC SKILLED NURSING 302
PHYSICAL THERAPY 299
INTERVENTIONAL RADIOLOGY 290
ORTHOPEDIC 269
CHEMOTHERAPY 262
VASCULAR 259
VASCULAR TESTS, PROCEDURES, STUDIES 201
ALLERGY AND IMMUNOLOGY 185
ORTHOPEDIC TESTS, PROCEDURES, STUDIES 182

Spartanburg
5,464 Patients
97 MilesGreenville
18,389 Patients
115 Miles
Rock Hill
7,487 Patients
71 Miles
Florence
6,896 Patients
80 Miles
Sumter
5,004 Patients
44 Miles
Orangeburg
2,799 Patients
42 Miles
Dorn VA Medical Center
Columbia
Community Based Outpatient Clinics
(CBOCs)
Anderson
6,809 Patients
140 Miles
VHA Funding
• Appropriated Funds & General Post Funds
• Medical Services – clinical salaries, equipment, supplies,
medications, travel, care in the community
• Medical Support and Compliance – administrative salaries,
non-medical equipment, advertising costs
• Medical Facilities – engineering, environmental mgmt.,
safety, utilities, facility related equipment
• General post funds – donations for specific purposes or to
support Veteran needs
• Appropriations can be one-year (annual authority), multiple year
(specific period of time in excess of 1 fiscal year), No-year
authority (indefinite period of time)

Veterans Equitable Resource Allocation
(VERA) Funding
• VERA methodology funds each network and facility based on
the number of Veterans who use the healthcare systems
• Two categories – Basic and Complex care
• Basic care most recent three-year patient usage data
• Complex is one-year projected population based on five
year patient data
• VERA Research Support – funding for both basic & complex
due to research isn’t directly related to number of patients
FY 2018 M7 FY 2017 M7 Count Percentage
Non-Reliant 3,586 3,408 178 5.22%
Basic 68,828 68,664 164 0.24%
Complex 3,738 3,591 147 4.09%
Uniques 76,152 75,663 489 0.65%
544 COLUMBIA (SC)Unique Pats Difference

Expansions and New Facilities
Behavioral Health
Center of Excellence15,000 sq. ft.
100% designed, estimated
start January 2019 and
completion July 2020
Prosthetics Center16,500 sq. ft.
100% designed, estimated
start January 2019 and
completion by July 2020
Rehab Center15,000 sq. ft.
100% designed, estimated
start January 2019 and
completion by July 2020
Police Station6,500 sq. ft.
Construction began March
2018, estimated completion
February 2019
Parking Garage278 Spaces
Construction began
February 2018, estimated
completion July 2019
Fisher HouseCommunity fundraising in
progress
Perimeter Fence100% designed, estimated
start October 2019,
completion by October 2020
4 New CBOCs3 are 75% designed,
estimated start Q1 FY20
1 awaiting assignment from
Real Property
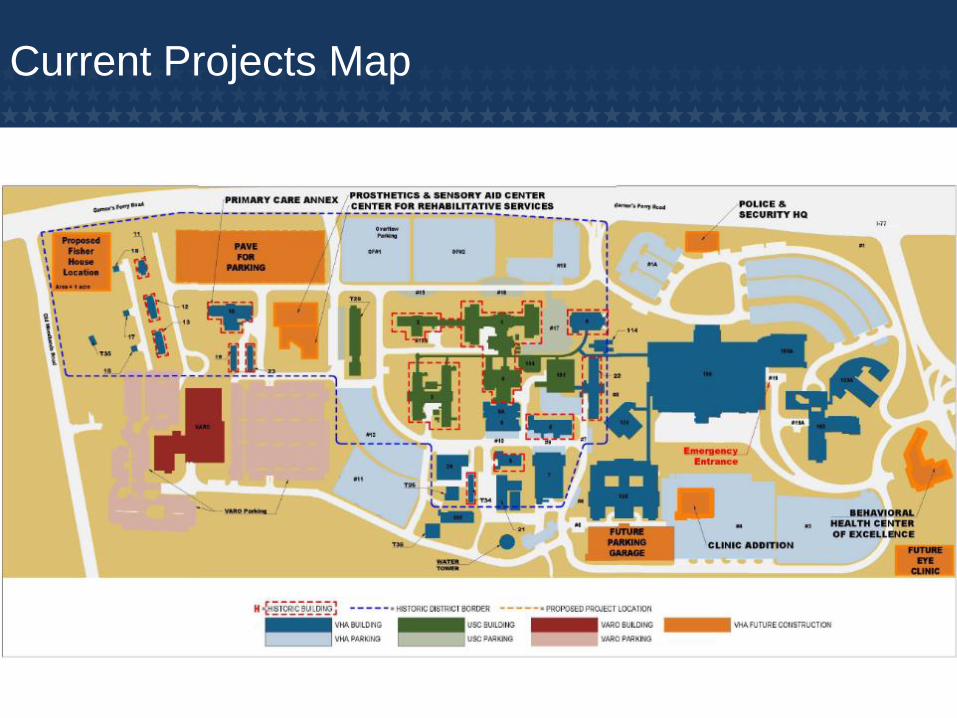
Current Projects Map

Q & A

Ralph H. Johnson VA Medical Center
• PFC Ralph H. Johnson, USMC was born January 11, 1949, in Charleston, South Carolina.
• Enlisted in the U.S. Marine Corps Reserve in March 1967, and was discharged to enlist in the Regular Marine Corps in July 1967.
• In January 1968, he arrived in the Republic of Vietnam. During combat in the early morning hours of March 5, 1968, a hand grenade landed in the three-man fighting hole occupied by Private Johnson and two fellow Marines. PFC Johnson willingly hurled himself upon the explosive device and was killed instantly.
• PFC Johnson was awarded the Congressional Medal of Honor posthumously.
• On September 5, 1991 the Charleston VA Medical Center was renamed the Ralph H. Johnson Department of Veterans Affairs Medical Center.
Ralph H. Johnson

Garett Schreier, MSN, RNAssociate Director of
Nursing and Patient Care Services
Scott Isaacks, FACHEMedical Center Director / Chief Executive Officer
Florence Hutchison, MD
Chief of Staff
Todd WilliamsAssistant Director
Felissa KoernigAssociate Director
Executive Leadership Team
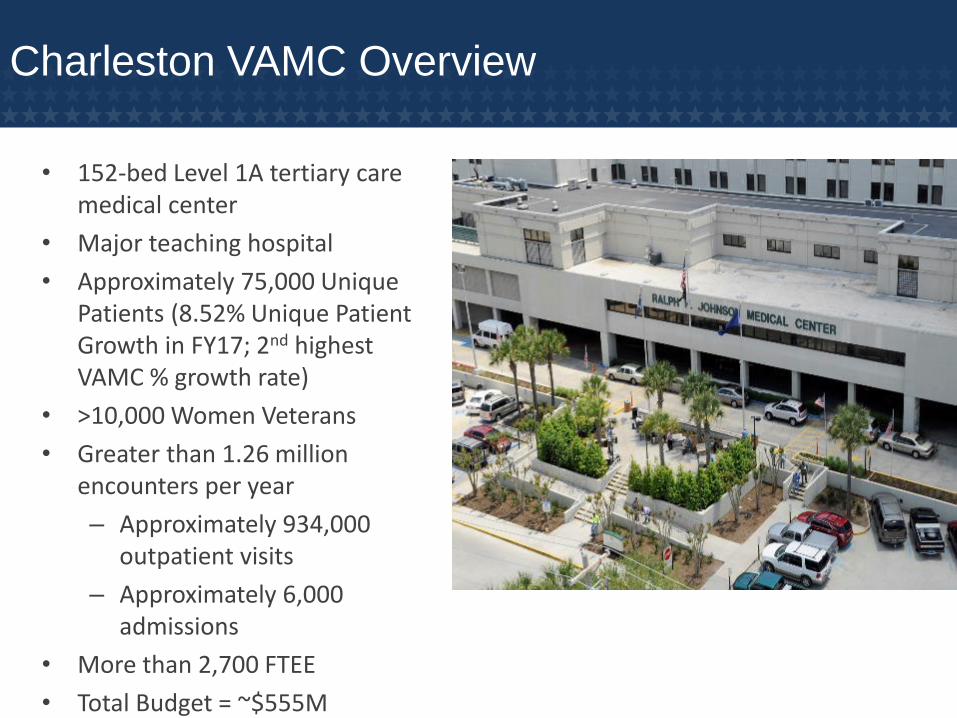
• 152-bed Level 1A tertiary care medical center
• Major teaching hospital
• Approximately 75,000 Unique Patients (8.52% Unique Patient Growth in FY17; 2nd highest VAMC % growth rate)
• >10,000 Women Veterans
• Greater than 1.26 million encounters per year
– Approximately 934,000 outpatient visits
– Approximately 6,000 admissions
• More than 2,700 FTEE
• Total Budget = ~$555M
Charleston VAMC Overview
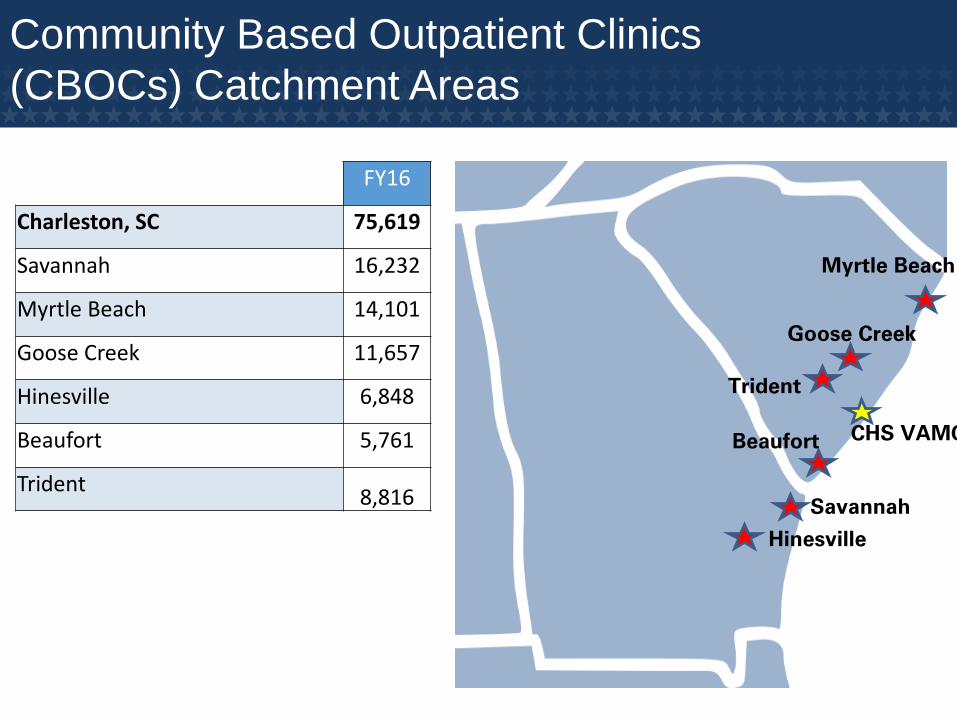
Community Based Outpatient Clinics
(CBOCs) Catchment Areas
Myrtle Beach
Trident
Goose Creek
Beaufort
Hinesville
Savannah
CHS VAMC
FY16
Charleston, SC 75,619
Savannah 16,232
Myrtle Beach 14,101
Goose Creek 11,657
Hinesville 6,848
Beaufort 5,761
Trident 8,816
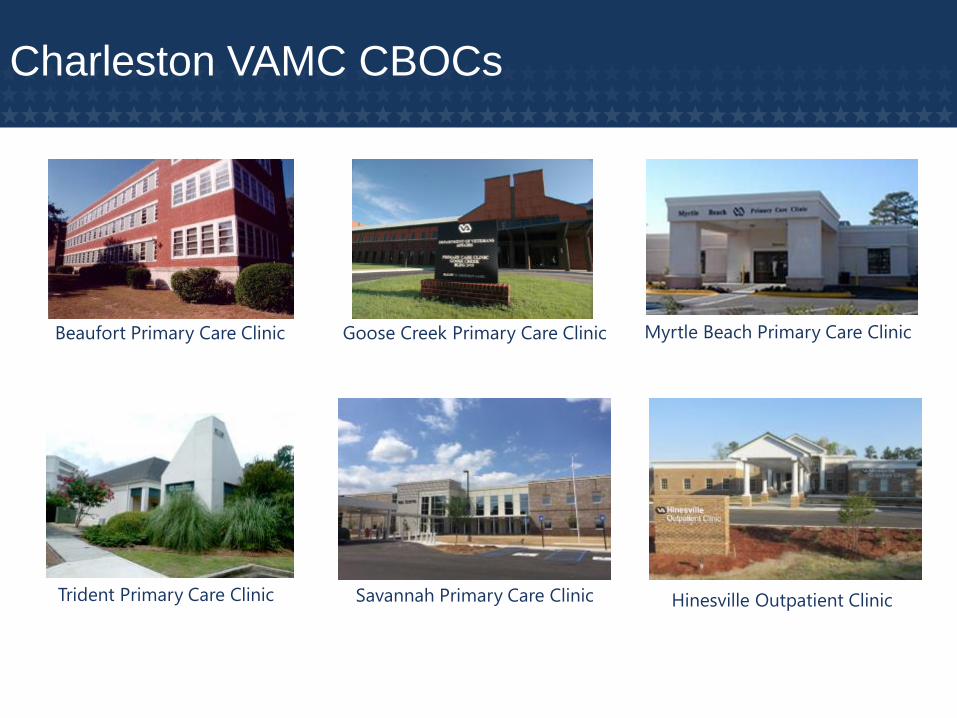
Beaufort Primary Care Clinic Myrtle Beach Primary Care Clinic
Savannah Primary Care Clinic
Goose Creek Primary Care Clinic
Trident Primary Care Clinic Hinesville Outpatient Clinic
Charleston VAMC CBOCs
• Primary Care• Specialty Care• Mental Health• Homeless Program• MHICM• Preventative Medicine • Residential Care• Geriatrics• Nursing Home Care
Unit
• Dental
• Rehab Medicine
• Primary Care
• Home Based Services
• Pharmacy / CMOP
• Prosthetics
• Caregiver Support
• Social Work
Wrap Around Services

• General Surgery• Cardio-thoracic Surgery• Vascular Surgery• Neurosurgery• Urology• Dermatology• Neurology• Gastroenterology• Hematology/Oncology• Bariatric Surgery• Ophthalmology• Podiatry• Orthopedics• Audiology
• Speech Pathology• Nephrology• Hemodialysis• Rehab Medicine• Cardiology• DaVinci Robot – VISN7 Referral
Center
Clinical Services

• Strategic Analytics for Improvement and Learning Value (SAIL)– 5 Star Rating in FY17 – 3rd consecutive year– Ended FY17
• Ranked 6th in overall quality compared to other VAMCs• Most efficient Level 1A VAMC in nation
• Growth– 8.52% unique patient growth in FY17– 2nd fastest growing VAMC in U.S. for % increase of unique
patients
• New Space Licensing Authority • SCHA Working Well Member • Outstanding Reviews
– Joint Commission, OIG/CAP, Research AAA LAC Accreditation Survey, Police OS&LE Survey, VA National Enforcement Office for Pathology and Laboratory Medicine, OIG IT Review
Leading the Way

• Nationally recognized PTSD program• Robotic & Bariatric Surgery Center of Excellence; Regional
referral center for Cochlear Implants, Robotic & Bariatric Surgery
• VA/DoD Sharing– 1 of 12 VA-DoD Joint Venture sites– Joint Incentive Fund (JIF) projects:
• Optometry Clinic• Ophthalmology• 2 Mobile MRIs• Physical Therapy• Dermatology
• Tele-Mental Health collaboration with Winn Army Community Hospital, Ft. Stewart, GA
Leading the Way
• Affiliated with MUSC and more than 40 institutions of higher education
• 105 FTEE resident positions in academic year 2017-2018
• Approved by VA Office of Academic Affiliations for Quality Residency Program
• Support 25 separate clinical postgraduate residency programs
• VA Nursing Academy Partnership with MUSC College of Nursing started 2008
• Post-Baccalaureate Nurse Residency program since 2012
• Mental Health Nurse Practitioner Residency program
• Dental Residency• PharmD Residency
Training Tomorrow’s Health Care Professionals
and Advancing Research

• Establishing a provider relations team.
– Kelly Keller, Claims Assistant currently works with the vendors on provider agreements(referred to as Care Plans under the Mission Act).
– Kelly Keller Contact Information
• (843) 789-6360
• Stopped sending referrals to HealthNet as of June 30, 2018.
Community Care
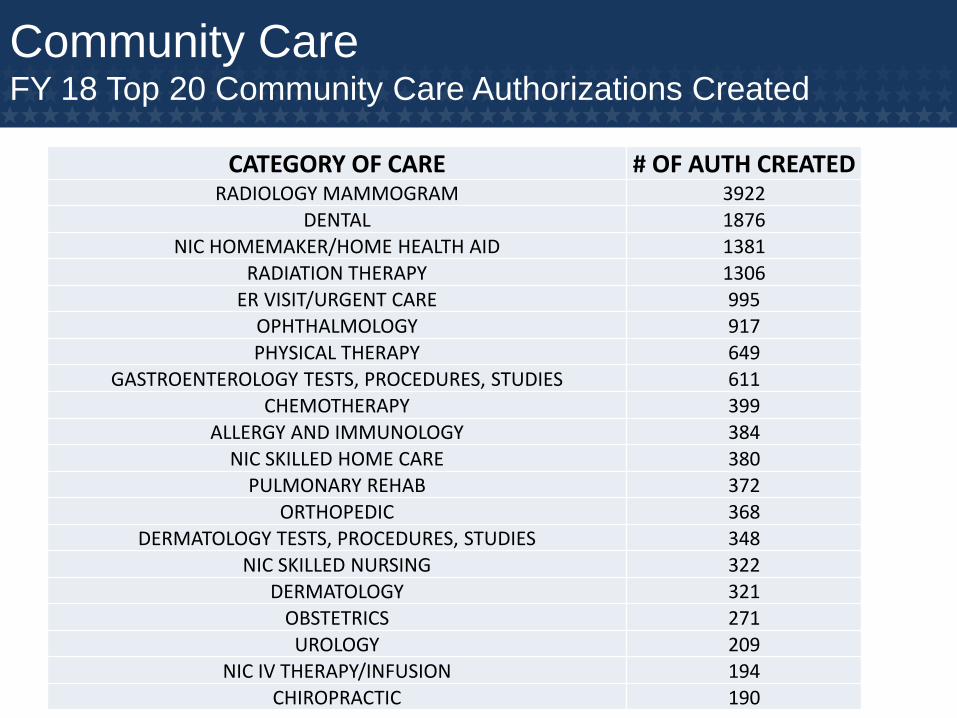
Community CareFY 18 Top 20 Community Care Authorizations Created
CATEGORY OF CARE # OF AUTH CREATED RADIOLOGY MAMMOGRAM 3922
DENTAL 1876NIC HOMEMAKER/HOME HEALTH AID 1381
RADIATION THERAPY 1306ER VISIT/URGENT CARE 995
OPHTHALMOLOGY 917PHYSICAL THERAPY 649
GASTROENTEROLOGY TESTS, PROCEDURES, STUDIES 611
CHEMOTHERAPY 399ALLERGY AND IMMUNOLOGY 384
NIC SKILLED HOME CARE 380PULMONARY REHAB 372
ORTHOPEDIC 368DERMATOLOGY TESTS, PROCEDURES, STUDIES 348
NIC SKILLED NURSING 322DERMATOLOGY 321
OBSTETRICS 271UROLOGY 209
NIC IV THERAPY/INFUSION 194
CHIROPRACTIC 190
Q & A
Data Management / Process Improvement
061118

• Accountable for long-term coordination of
care and health outcomes
• Responsible for population health
outcomes for all enrolled Veterans in SC
• Data-rich environment drives improvement
& “Analysis Paralysis”
• Population Statistics
• Data Systems- National, Regional, Local
• Return on Investment
(profit driven vs. 3 year capitated model)
• Department of Veterans Affairs strategies
drive local KPIs
Challenges Experienced by VA Hospitals:
Data Management / Process Improvement
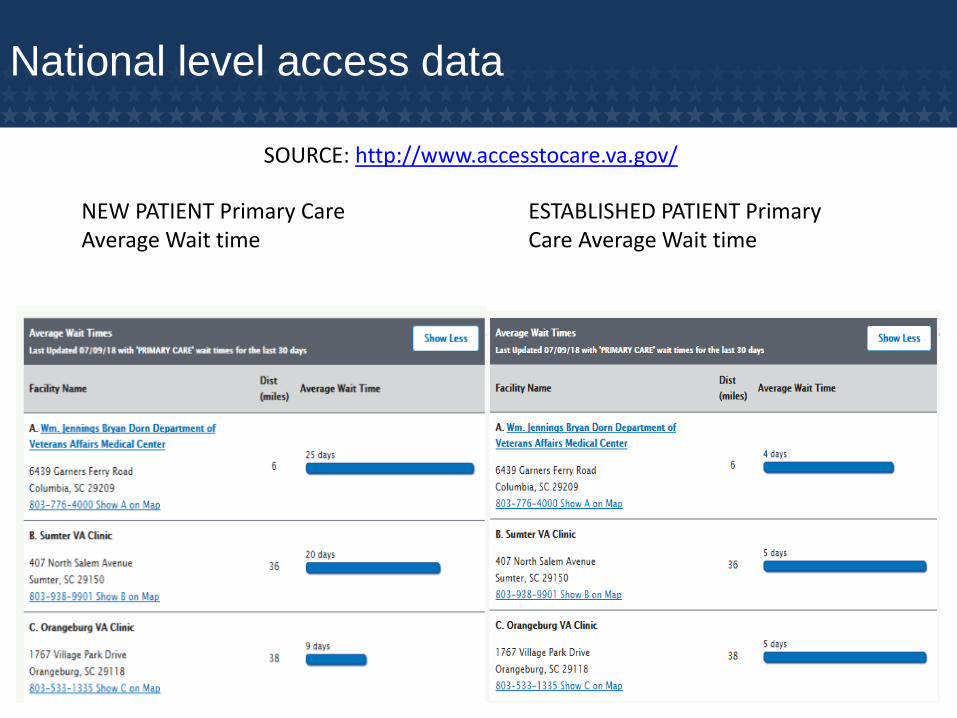
National level access data
ESTABLISHED PATIENT Primary Care Average Wait time
NEW PATIENT Primary Care Average Wait time
SOURCE: http://www.accesstocare.va.gov/
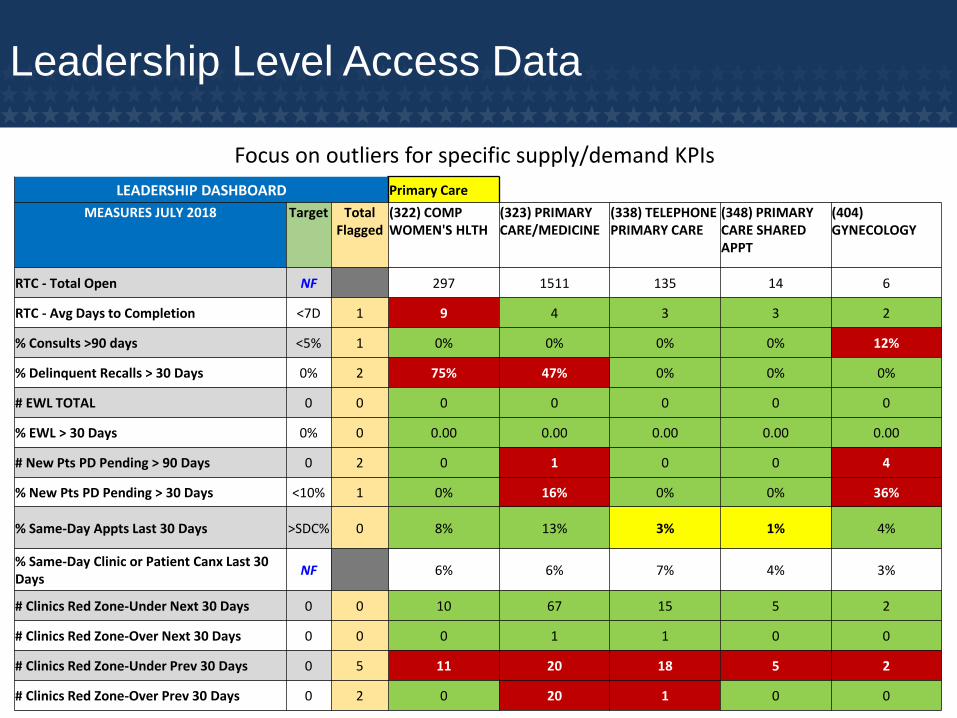
Focus on outliers for specific supply/demand KPIs
LEADERSHIP DASHBOARD Primary Care
MEASURES JULY 2018 Target Total Flagged
(322) COMP WOMEN'S HLTH
(323) PRIMARY CARE/MEDICINE
(338) TELEPHONE PRIMARY CARE
(348) PRIMARY CARE SHARED APPT
(404) GYNECOLOGY
RTC - Total Open NF 297 1511 135 14 6
RTC - Avg Days to Completion <7D 1 9 4 3 3 2
% Consults >90 days <5% 1 0% 0% 0% 0% 12%
% Delinquent Recalls > 30 Days 0% 2 75% 47% 0% 0% 0%
# EWL TOTAL 0 0 0 0 0 0 0
% EWL > 30 Days 0% 0 0.00 0.00 0.00 0.00 0.00
# New Pts PD Pending > 90 Days 0 2 0 1 0 0 4
% New Pts PD Pending > 30 Days <10% 1 0% 16% 0% 0% 36%
% Same-Day Appts Last 30 Days >SDC% 0 8% 13% 3% 1% 4%
% Same-Day Clinic or Patient Canx Last 30 Days
NF 6% 6% 7% 4% 3%
# Clinics Red Zone-Under Next 30 Days 0 0 10 67 15 5 2
# Clinics Red Zone-Over Next 30 Days 0 0 0 1 1 0 0
# Clinics Red Zone-Under Prev 30 Days 0 5 11 20 18 5 2
# Clinics Red Zone-Over Prev 30 Days 0 2 0 20 1 0 0
Leadership Level Access Data
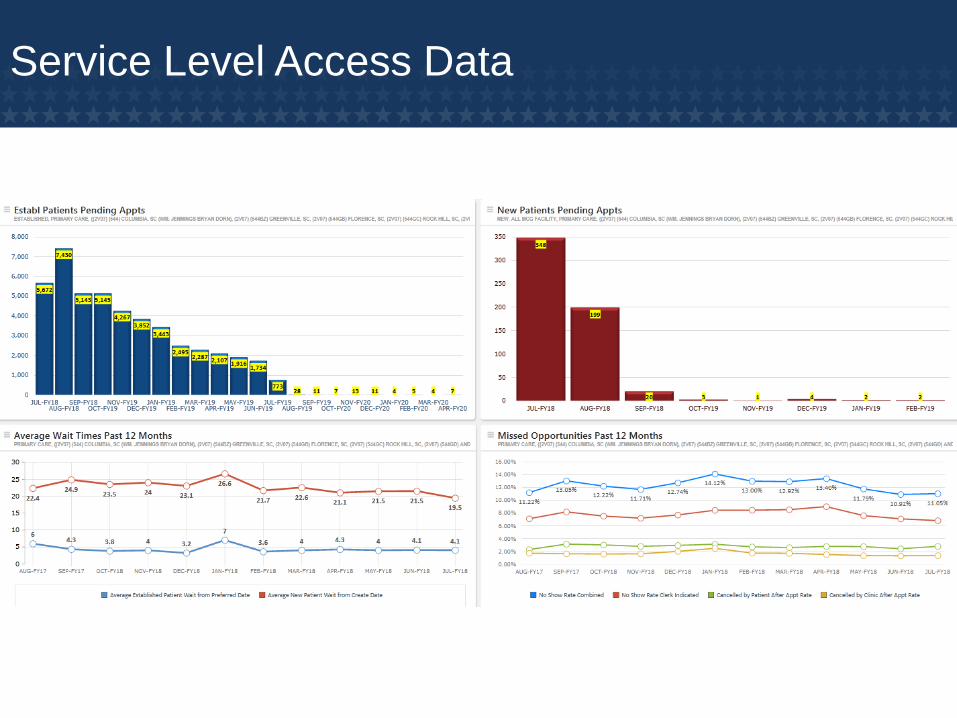
Service Level Access Data

Shared Data and Quality Management
https://www.medicare.gov/hospitalcompare/Data/About.html
Culture Transformation
Reframing the context of QM, Data Analytics, and Process Improvement
• Build
• Educate
• Engage
• Spread
• Sustain
Facilitating Improvement /Sustainable Outcomes
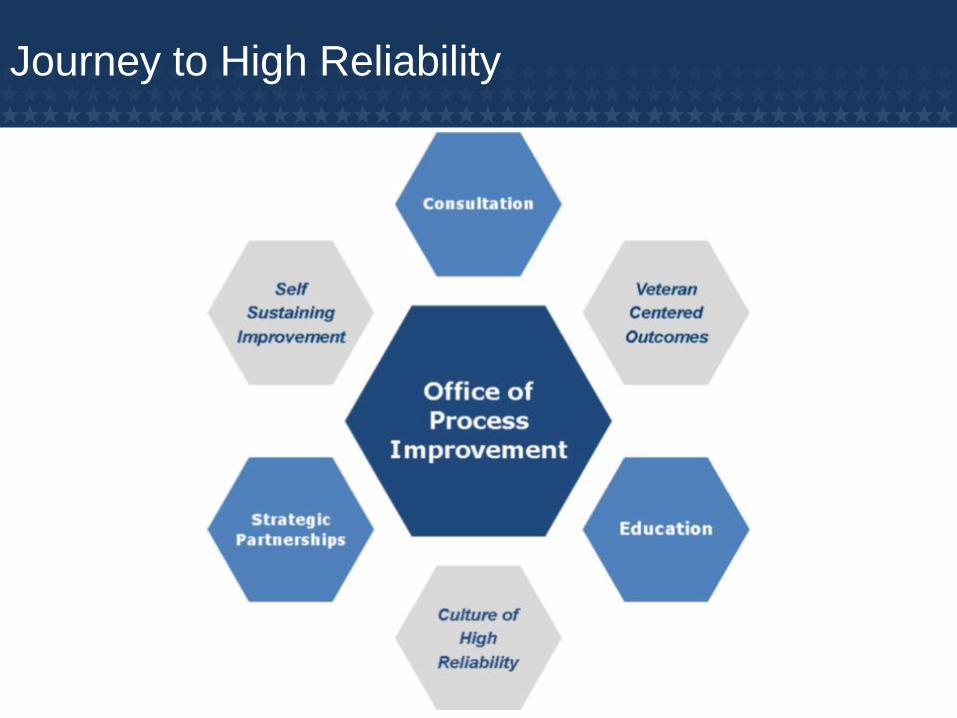
Journey to High Reliability

Summary
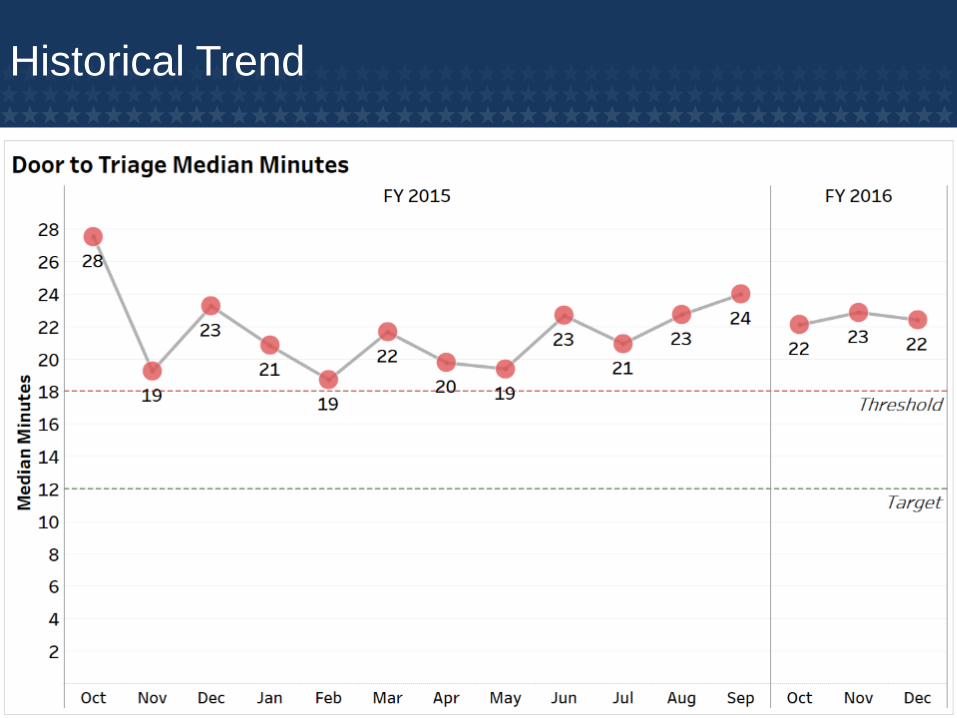
Historical Trend
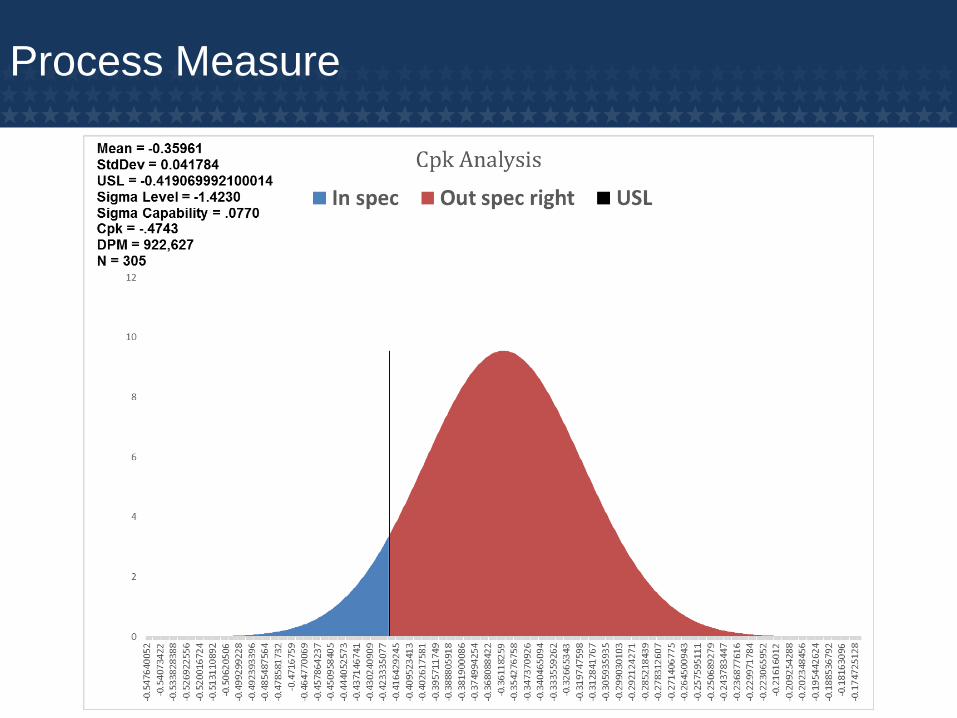
Process Measure
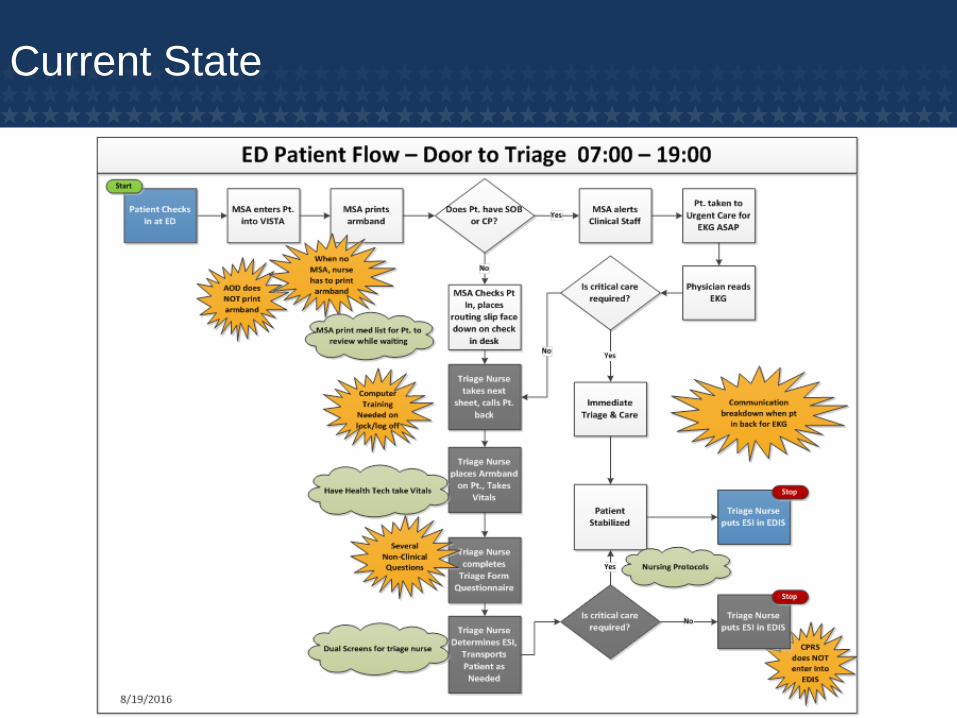
Current State
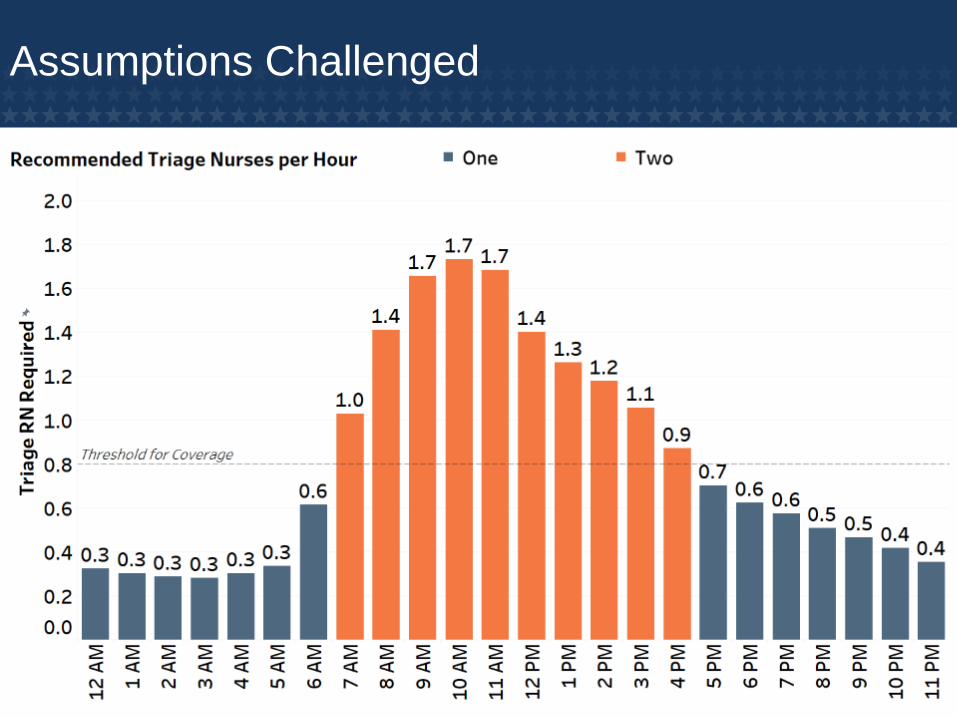
Assumptions Challenged

Identified Waste
• Triage Nurse Gathering Patients from Waiting
Area
• Triage Nurse Taking Patient Vital Signs
• Triage Nurse Transporting Patient to Lab and
Radiology
• Several Underutilized Health Technicians
Available
• No Process Standard Work
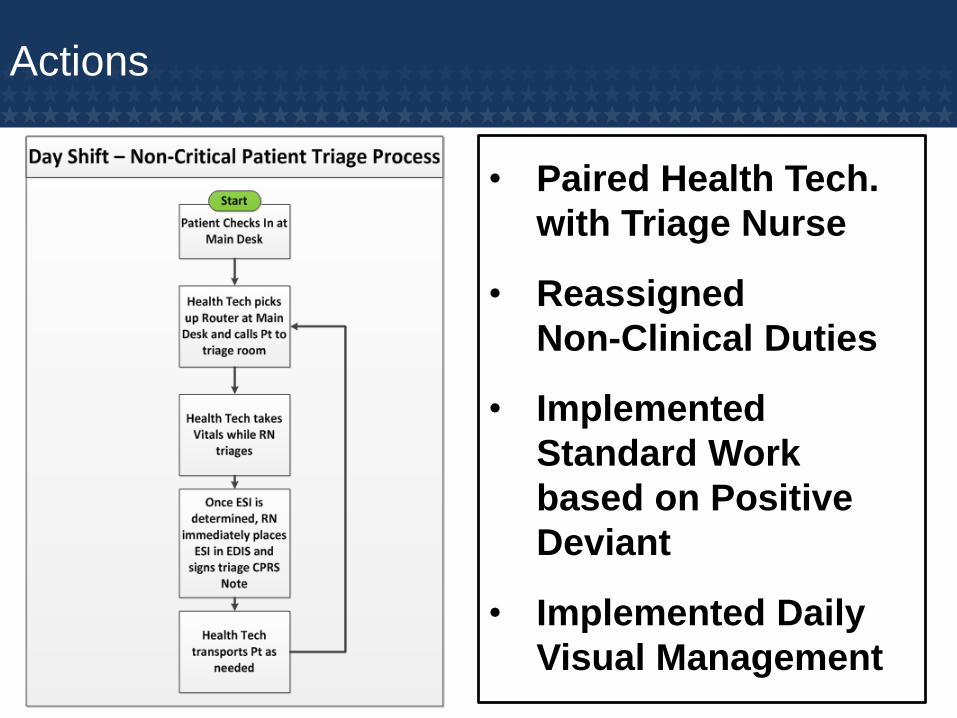
Actions
• Paired Health Tech.
with Triage Nurse
• Reassigned
Non-Clinical Duties
• Implemented
Standard Work
based on Positive
Deviant
• Implemented Daily
Visual Management
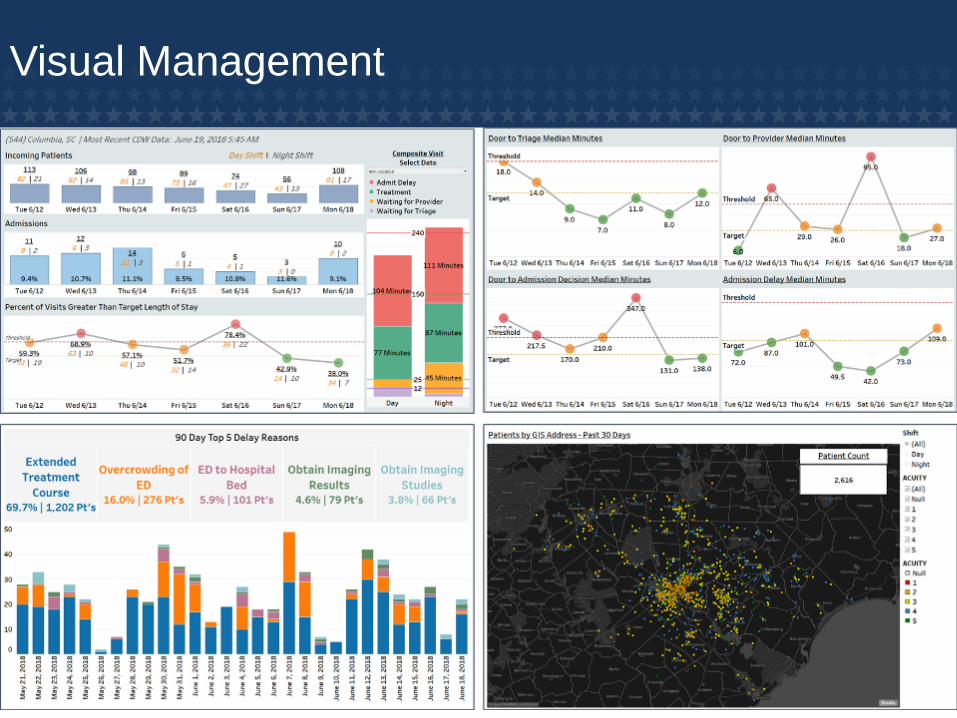
Visual Management
Visual Management
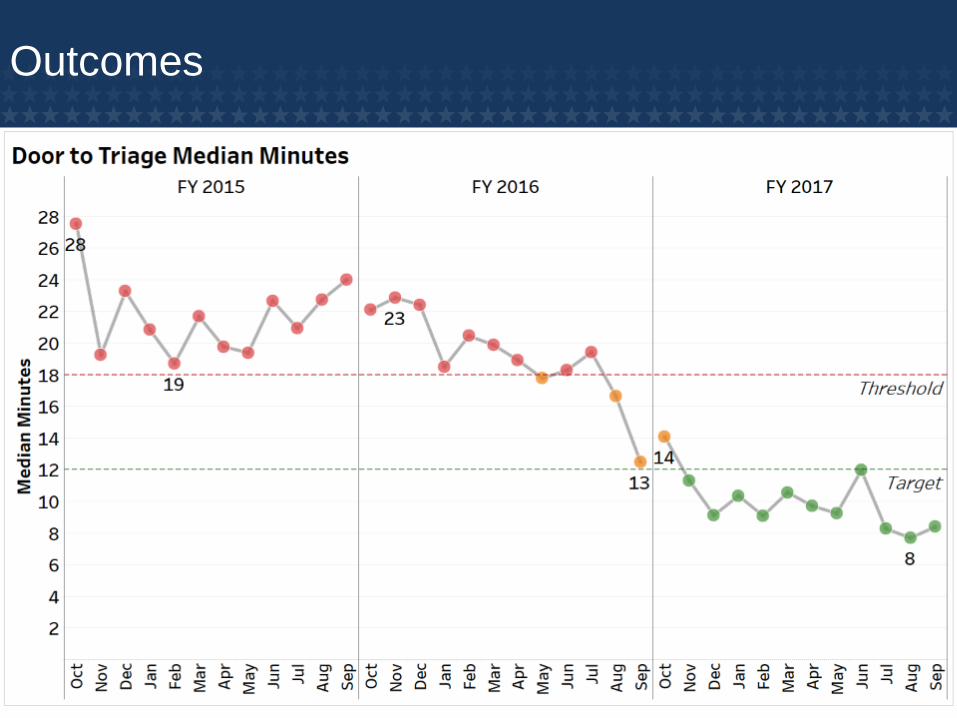
Outcomes

Outcomes (continued)

Outcomes (continued)
• 50% Decrease in
Defect Rate
• Increased
Process
Capability
• Increased
Process
Stability
Continuous Improvement
Updates Since Project Completion
• Sustained high performance in most Key
Performance Indicators for 12+ months
• Commenced new Process Improvement
Project February 2018 with focus on improving
care and resource utilization for non-emergent
patients
• Visual Management Tools have been spread to
15+ VHA facilities nationwide, with plans for
additional expansion

Q & A

Community Care Overview
061118
VA MISSION ACT OF 2018:
MODIFIES THE VETERANS COMMUNITY
CARE PROGRAM (FORMALLY CHOICE) TO
PROVIDE CARE IN THE COMMUNITY TO
VETERANS WHO ARE ENROLLED IN THE VA
HEALTHCARE SYSTEM OR OTHERWISE ENTITLED TO VA CARE.
53
54
VA Mission Act of 2018
• Consolidates seven VA community care programs into one
streamlined program.
• Removes arbitrary 30-day/40-mile barriers to veterans’ care in
the community.
– A veteran and the veteran’s referring clinician agree that furnishing care
or services in the community would be in the best medical interest of the
veteran.
– Whether the covered veteran faces an excessive driving distance,
geographical challenge, or environmental factor that impedes access.
– Whether a medical condition of the covered veteran affects his/her
ability to travel.
– Whether there is a compelling reason that the covered veteran needs to
receive care or services from a medical facility other than a VA medical
facility.
55
VA Mission Act of 2018
• Authorizes access to walk-in community clinics for enrolled veterans who have previously used VA healthcare services in the last two years.– Veterans would be entitled to two visits (annually) without a copayment
• Creates standards for timely payment to community care providers
• VA would be required to coordinate veterans’ care and would be required to:– Ensure the scheduling of medical appointments in a timely manner.
– Ensure continuity of care and services.
– Coordinate coverage for veterans who utilize care outside of a region from where they reside.
– Ensure veterans do not experience a lapse in health care services.

56
Community Care Network (CCN)
• The Community Care Network (CCN) is a set of contracts
awarded to as many as four private sector TPAs to develop and
administer regional networks of high-performing licensed
healthcare providers covering an established set of regional
boundaries aligned to state boundaries to provide local flexibility
and increased access to care. Each regional network will serve
as the contract vehicle for VA to purchase care in the community.
• CCN Regions are divided by state boundaries and were
established with the consideration of volume of Veterans enrolled
in the VA system and the number of community care referrals in
FY 15 by state

57
Community Care Network (CCN)
CCN deployment will be phased in across the awarded regions to ensure
operational capability prior to phasing-out other purchased care contracts

CCN Capabilities
Current State Eligibility Future
State • VA Determines eligibility• Contractor attains Veteran
opt-in
• VA determines eligibility• Clear Processes for exchanging
eligibility information between the contractor and VA
• VA sends out authorizations to the contractor who then sends them to providers
• VA sends referrals directly to providers, with copies sent to the contractor.
• All referrals include a SECO that relates to a specific number of visits and/or services related to a plan of care
• Contractor schedules appointments
• Use of contractor portal for medical documentation exchange
• Scheduling occurs locally • Veterans may schedule their own
appointment or get support form local staff.
• Direct health information sharing capability between VA and CCN providers
Referrals & Authorization
Care Coordination

CCN Capabilities
Current State Future State
• Adequacy measurements are region-based
• No high performing provider designation
• Poor visibility into network coverage gaps
• Adequacy measured at VAMC level• Accreditation standards and high
performing provider designation • Local VAMC participation in network
development effort• More CCN services offered than
PC3/Choice
• VA re-adjudicates claims• Providers are not paid timely
and strained provider relationships
• Lengthy reimbursement process
• VA will not re-adjudicate claims• Contractor pays provides• 98 percent of clean claims paid
within 30 days of receipt
• Contractor manages Veterans, providers and VA touchpoints
• Veteran customer service and experience is inconsistent
• VA will directly manage Veteran touchpoints
• Contractor supports VA staff and community provider touchpoints
Community Care Network
Provider Payments
Customer Service
VA’s Role
Eligibility and Enrollment
• VA will continue to determine Veteran eligibility under CCN as it does currently for PCCC and the VCP contracts. CCN contractors will be required to confirm eligibility as part of the new contract.
• VA will send Veteran records to the CCN contractors in each region. Enrollment updates will be sent subsequently if Veteran records or eligibility status changes.
Referrals and Authorizations
• Local VAMC staff will issue and send referrals/authorizations directly to providers in the CCN network.
• All CCN referrals/authorizations must include a specific Standardized Episode of Care (SEOC) that relates to a specific number of visits and/or services related to a plan of care.
VA’s Role
Care Coordination
• To better serve Veterans, scheduling will occur directly between
Veterans and their local VAMC.
Customer Experience
• VA staff will directly manage Veteran touchpoints for customer
service while the contractors will support VA staff and community
provider inquiries.
• VA staff will collaborate with CCN contractors to ensure customer
services processes between VA and community providers are
efficient, timely, and effective.
62
Providers
• Establishes a program to provide continuing medical education
credits for community care providers at no cost to them.
• Require VA to develop and administer a training program for VA
employees and contractors on how to administer non-VA health
care programs and the management of prescriptions for opioids.
• Allow VA to deny, suspend, or revoke the eligibility of a non-
Department health care provider to participate in the community
care program if that the provider was previously removed from
VA employment or had their medical license revoked.
• Authorizes VA to enter into Veterans Care Agreements (VCAs)
that are not subject to competition or other requirements
associated with federal contracts.
Payments• VA refers services to a network provider who renders the service and
invoices the CCN Region Contract
• CCN contractors will be responsible for processing, adjudicating, and paying claims received from community providers on behalf of VA. To address concerns over timely payments, each CCN contract has performance measures in place to ensure the contractors pay 98 percent of all clean claims (including resubmissions) within 30 days of receipt.
• The VA has mandated a 7 day payment period from Contractor to provider (within 7 business days)
• VA receives a copy of the Provider EDI invoice from the Contractor - VA pays Contractor based on invoice from Contractor
• Denied invoices by the VA will be sent back to CCN contractors with reason codes so they have the opportunity to correct and resubmit within 30 days for reimbursement. After initial reimbursement, VA will conduct post-payment analytics and validation to ensure prompt payments are being made.
• VA has full visibility into Contractor payment timeliness to each CCN Network Provider.
Records Management
• VA will share medical record information with non-VA entities.
• CCN requires VA to implement a process to make certain that community care providers have access to available and relevant medical history of the patient, including a list of all medication prescribed to the veteran as known by VA.
• Efforts are underway to ensure the CCN contracts for each region include a preferred method of exchange for medical documentation for authorizations and coordination of care. The process for receiving medical documentation will be finalized with the CCN contractors 90 days after award.
• Each CCN contractor is measured on their medical documentation submission timeframes.
Accountability
• Requires competency standards for non-VA providers treating
veterans.
• Requires VA to monitor network care and report to Congress on
the care provided to veterans.
• Requires VA to publish data on these quality measures on the
Hospital Compare website through the Centers for Medicare and
Medicaid.
– Satisfaction
– Timely care
– Effective care
– Safety (including complications, readmissions, and death)
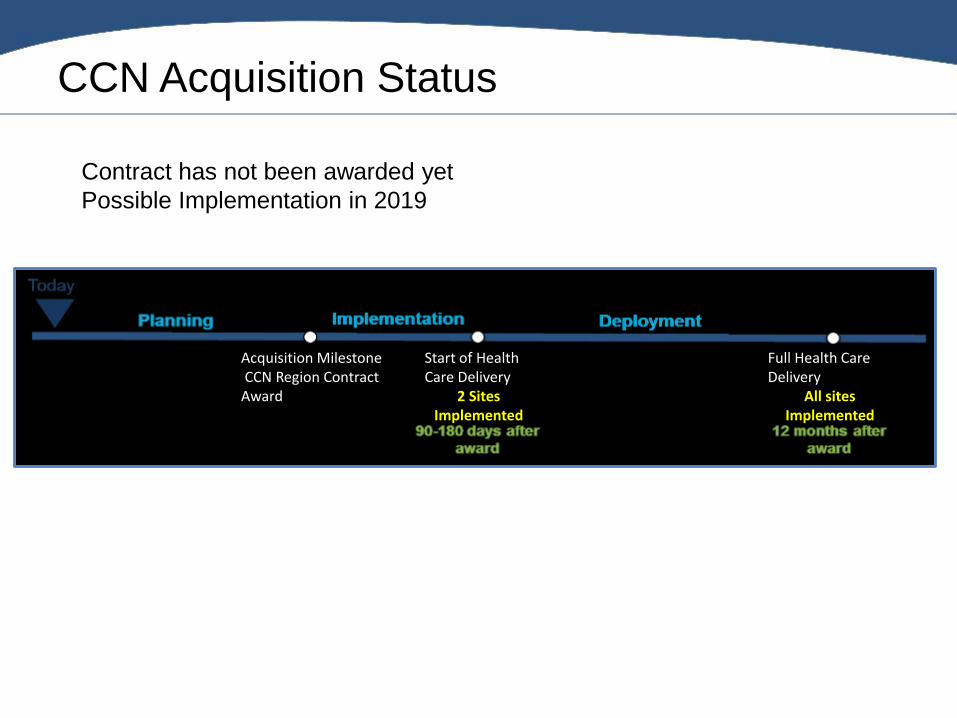
CCN Acquisition Status
Acquisition MilestoneCCN Region Contract
Award
Start of Health Care Delivery
2 Sites Implemented
Full Health Care Delivery
All sites Implemented
Contract has not been awarded yet
Possible Implementation in 2019
Q & A

VA Research Overview
Biomedical Laboratory Research &
Development Service (BLR&D):
• Pre-clinical and clinical, molecular, genomic, and physiological level in regard to diseases affecting Veterans.
• Includes research on animal models and human tissues, blood, or other biologic specimens.
• Some limited human studies
Clinical Service Research and
Development (CSR&D):
• Human Research Examples:
• interventional and effectiveness studies,
• Clinical, epidemiological and technological studies
Health Services Research and
Development Service (HSRD):
• Research at the interface of health care systems, patients and health care outcomes.
• All aspects of VA health care;
• Quality
• Access
• Patient outcomes
• Health care costs
Rehabilitation Research and Development Service (RR&D):
• Research evaluating:
• new technologies and therapies
• technology transfers
• final clinical application.
VA’s Office of Research and Development (ORD) is organized through
four services:
Post Traumatic Stress Disorder
(PTSD)
Traumatic Brain Injury
(TBI)
Suicide Prevention
Opioid Addiction
Women’s Health
Chronic Diseases
Veteran Homelessness
High Priority VA Research Topics

69%
3%
28% Department ofVeterans Affairs
NIH/ DOD
Private Industry
1.7 Million in Research
funding in FY 17
Funding Sources Key Partnerships
• USC School of Medicine
• USC College of Pharmacy
• Arnold School of Public Health
• Greenville Health System
• SCDHEC
• NCI
Active Research Studies
• Oncology
• Endocrinology
• PTSD
• Drug Trials
• Heart Failure
• MVP – how genes affect health and
illness
Million Veteran Program
(MVP)
• 50 VA Medical Centers serve
as MVP enrollment sites
• In SC, Dorn VAMC, Greenville,
Florence, & Rockhill enroll
• Nationally - over 650,000
Veterans enrolled
• Locally - 11,000 enrolled
WJB Dorn VA Research Overview

Shirley Buchanan Research Facility-
Facilitating collaborative efforts between researchers at
the Dorn VA and the USC School of Medicine
• State of the art facility with wet lab bench space
• Multi-photon confocal microscopy
• Surgical suites for rodent testing
• Equipment oversight from the USCSOM Instrumentation
Resource Facility
Research Facility

• Independent non-profit corporation established in 1997 to support activities in:– research – Education
• Provides Grants Management and Administrative services
• Markets Dorn's unique research capabilities and expertise to funding agencies (NIH, DoD, NCI, pharmaceutical and device companies)
• Seed Grants for pilot projects with funding potential
Dorn Research Institute (DRI)
WJB Dorn VA Research Contacts
– Dr. K. Sue Haddock, PhD, Associate Chief of Staff for
Research, [email protected]
– Andrew Barden, Administrative Officer,
– DRI Executive Director, Rebecca Parsons,
Interested in VA Research Opportunities?

Q & A

Columbia VAHCS Mental Health Service
061118
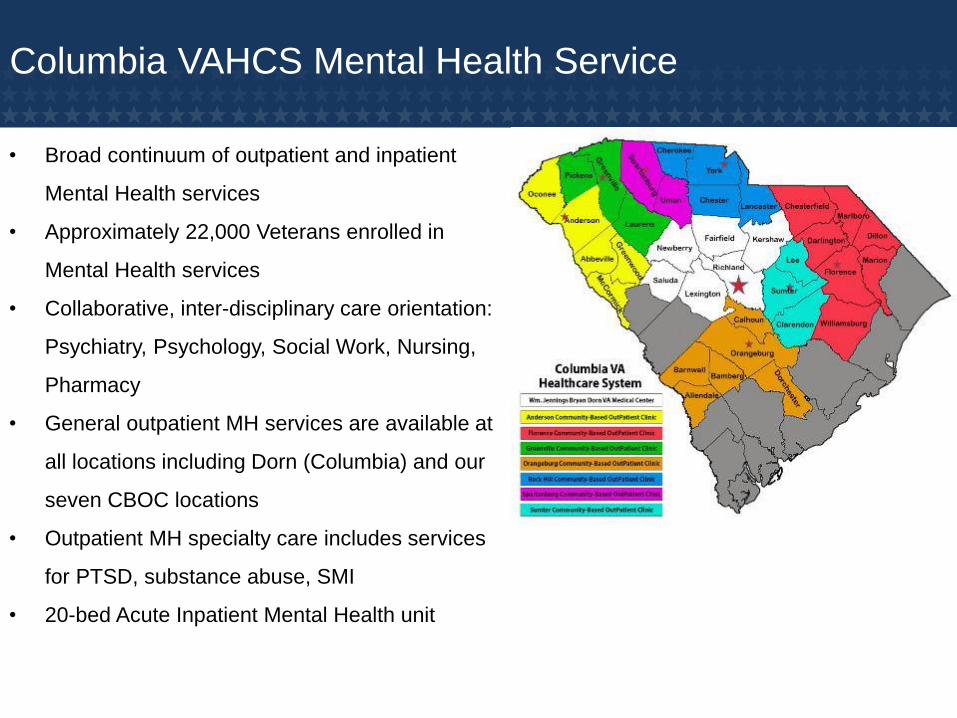
Columbia VAHCS Mental Health Service
• Broad continuum of outpatient and inpatient
Mental Health services
• Approximately 22,000 Veterans enrolled in
Mental Health services
• Collaborative, inter-disciplinary care orientation:
Psychiatry, Psychology, Social Work, Nursing,
Pharmacy
• General outpatient MH services are available at
all locations including Dorn (Columbia) and our
seven CBOC locations
• Outpatient MH specialty care includes services
for PTSD, substance abuse, SMI
• 20-bed Acute Inpatient Mental Health unit
Overview of Current Mental Health Services
• General Outpatient Mental Health
➢ Medication Management/Psychiatry
➢ Evidence-Based Psychotherapy Services
➢ Case Management
• Outpatient Geriatric Psychiatry
• Tele-Mental Health Services
• Primary Care/Mental Health Integration (PCMHI)
• Suicide Prevention Team
• H.O.M.E. Program
• Trauma Recovery Program (TRP) – PTSD Clinical Team
• Substance Abuse Treatment Program (SATP)
• Acute Inpatient Mental Health
• Serious Mental Illness (SMI) Services
➢ Psychosocial Rehabilitation & Recovery Center (PRRC)
➢ Mental Health Intensive Case Management (MHICM)

Future Expansion of Mental Health Services
• New Acute Inpatient Mental Health Unit in Building 100 3rd Tower – February 2019
• Possible expansion of inpatient MH services – 2019
• New Behavioral Health Center of Excellence – Construction 2020-2021
➢ Trauma Recovery Program
➢ Substance Abuse Treatment Program
➢ Psychosocial Rehabilitation & Recovery Center
➢ Mental Health Intensive Care
• Tele-Mental Health Expansion – 2018/2019
➢ Home-to-Home Evidence-Based Psychotherapy
• Couples Therapy Program – 2018/2019
• As new Community-Based Outpatient Clinics are constructed (Florence, Orangeburg,
Rock Hill, Sumter), Mental Health services will continue to grow including PCMHI,
Substance Abuse and PTSD

VHA Veteran Suicide Prevention Initiative
#BeThereWe can all play a role in preventing suicide, but many
people don’t know what they can do to support a Veteran or Servicemember in their life who is going
through a difficult time.
A simple act of kindness can help someone who feels alone.
Your actions could help save a life!
“No Veteran Left Behind” (video)
https://www.youtube.com/watch?v=i-xKK2HbmpI
Suicide Prevention is Everyone’s Business
#BeThere

Health Care for Homeless Veteran
Program (HCHV)
To reduce homelessness among Veterans by:
▪ Following the Housing First model of care.
▪ Conducting outreach to those who are the most
vulnerable who are not currently receiving services.
▪ Serving as the hub and entry point for housing and
other mental health and substance use services.
HCHV Goals

▪ Providing case management
▪ Linkage to permanent housing solutions
▪ Employment opportunities
▪ Health care
▪ Justice services
▪ Collaborating with community partners to
provide ongoing community based services that
will help maintain and sustain Veterans in
permanent housing.
HCHV Goals
• Health Care for Homeless Veterans Intake
• Community Employment Coordinator
• Compensated Work Therapy Program (CWT)
a. Supportive Employment (SE)
b. Community Based Employment Services (CBES)
• Grant and Per Diem Program (GPD)
• Housing and Urban Development/VA Supportive Housing
(HUD/VASH)
• Veterans Justice Outreach Program (VJO)
HCHV Programs
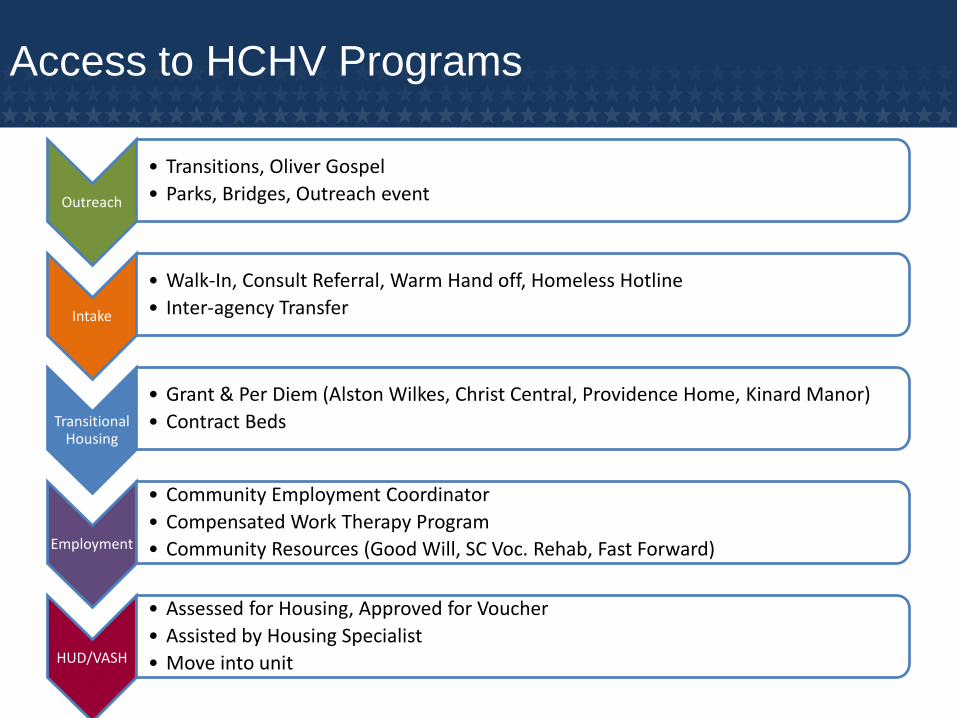
Outreach
• Transitions, Oliver Gospel
• Parks, Bridges, Outreach event
Intake
• Walk-In, Consult Referral, Warm Hand off, Homeless Hotline
• Inter-agency Transfer
Transitional Housing
• Grant & Per Diem (Alston Wilkes, Christ Central, Providence Home, Kinard Manor)
• Contract Beds
Employment
• Community Employment Coordinator
• Compensated Work Therapy Program
• Community Resources (Good Will, SC Voc. Rehab, Fast Forward)
HUD/VASH
• Assessed for Housing, Approved for Voucher
• Assisted by Housing Specialist
• Move into unit
Access to HCHV Programs

Veterans Justice Outreach Program
Justice Outreach
Veterans Justice Outreach
• Gain access to the jail system
• Identify Veterans and
Determine Eligibility
• Conduct outreach,
assessment, and case
management for Veterans in
local courts and jails
• Linkage to VA and Community
Services/Resources
Prison Re-Entry
Health Care Re-Entry
• Gain access to the prison
• Educate Veterans’ groups
about VA and VA services
• Identify Veterans and
Determine Eligibility
• Reentry Planning (6 mos.
pre-release)
• Linkage to VA and
Community Services
Health Care for Homeless Veterans
Program (HCHV)
• HUD/VASH maintains a lease up rate of 95% and have
100% of the allocated vouchers are in use.
• Grant and Per Diem (GPD) has 125 transitional Housing
Beds and 12 Contract Housing beds. The 2019 NOFA
expansion will include 45 GPD beds in the Upstate.
HCHV Program Accomplishments
• The VJO program has expanded to 4 Veteran Treatment
Courts (VTC’s) in Richland, Greenville, Spartanburg and
Greenwood. A VTC in Anderson will open in FY19.
• The Community Employment Coordinator has
successfully increased Veteran employment
opportunities and collaborates with over 125 community
employers.
HCHV Program Accomplishments

• Many homeless Veterans with debilitating physical and mental health issues are without hope. The HCHV, in collaboration with other government and community service providers, is changing the end of the story for Veterans who are homeless as well as those with serious mental illness and physical health issues.
Changing the end of the story
Q & A
Patient Safety: Responding to the Opioid Crisis
Ashleigh Powers, PharmD
PGY2 Ambulatory Care Pharmacy Resident
Ginger Ervin, PharmD
Associate Chief, Clinical Pharmacy Service
• Identify three primary campaigns enacted by the
Veteran’s Affairs Administration following introduction of
the Comprehensive Addiction and Recovery Act
• Select an appropriate tool for a primary care provider to
use in order to compile specified information on a patient
panel
• Compare opioid-alternative therapies for a patient with
chronic pain
93
Objectives
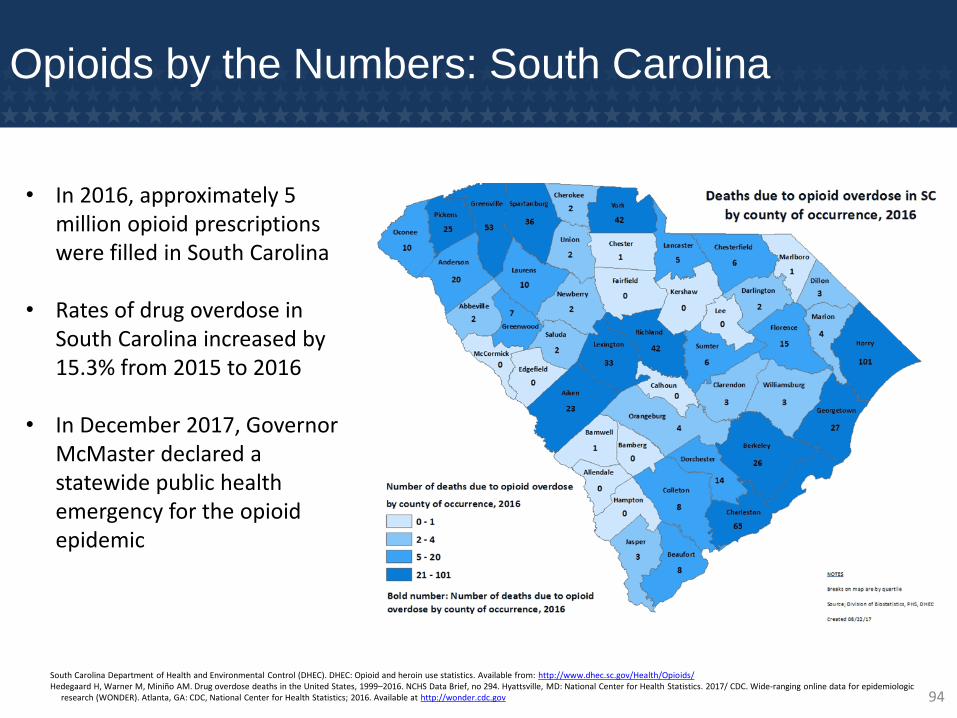
Opioids by the Numbers: South Carolina
• In 2016, approximately 5 million opioid prescriptions were filled in South Carolina
• Rates of drug overdose in South Carolina increased by 15.3% from 2015 to 2016
• In December 2017, Governor McMaster declared a statewide public health emergency for the opioid epidemic
South Carolina Department of Health and Environmental Control (DHEC). DHEC: Opioid and heroin use statistics. Available from: http://www.dhec.sc.gov/Health/Opioids/Hedegaard H, Warner M, Miniño AM. Drug overdose deaths in the United States, 1999–2016. NCHS Data Brief, no 294. Hyattsville, MD: National Center for Health Statistics. 2017/ CDC. Wide-ranging online data for epidemiologic
research (WONDER). Atlanta, GA: CDC, National Center for Health Statistics; 2016. Available at http://wonder.cdc.gov 94

Addressing the Opioid Epidemic in the VA:
Introduction of the CARA Law
• On July 22, 2016, the Comprehensive Addiction and Recovery Act (CARA) Law
was enacted by President Obama
• Six pillars of coordinated response: Prevention, Treatment, Recovery, Law
Enforcement, Criminal Justice Reform, and Overdose Reversal
• Title IX: Dedicated to Department of Veterans Affairs
Opioid Safety Initiative & Pain Management
(OSI)
Overdose Education & Naloxone Distribution
(OEND)
Opioid Use Disorder (OUD)
Three Primary Campaigns in CARA
95
\
Opioid Safety Initiative
(OSI)

Opioid Safety Initiative & Pain Management (OSI)
Goal: Reduce unsafe opioid pain medication prescribing
through utilization of:
VA Opioid Therapy Risk Reports
State Prescription Drug Monitoring Programs
Urine Drug Testing
Provider Education & Training
97

Tools for VA Providers: Opioid Therapy Risk
Report (OTRR)
• Provides a list of long term opioid patients by primary care team and provides clinical summary for each patient
• Additional information provided: concurrent high-risk disease states for opioid use disorder (PTSD, depression, substance use disorder, CKD, obstructive sleep apnea), any concurrent benzo, and next primary care appointment date & time 98

Tools for VA Providers: PDMP Report
• Tool for providers to assess patients who do not have an annual PDMP completed or recorded
• Can search by Provider, Medication Group, and Upcoming Appointment Date
• Additional information provided: opioid prescribers, benzodiazepine medications/prescribers,
other controlled medications/prescribers
99
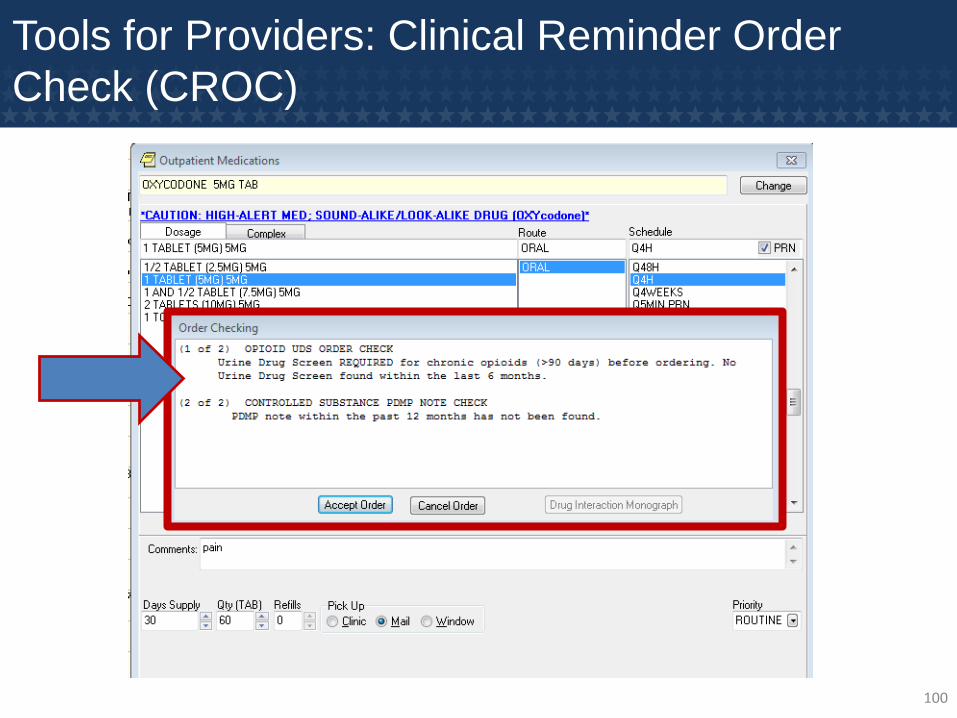
Tools for Providers: Clinical Reminder Order
Check (CROC)
100

OSI Provider Education & Training
• Addition of full-time Clinical Pharmacy Specialist
specializing in Pain Management
• Academic Detailing Campaign led by Clinical
Pharmacy Specialists
– Utilize one-on-one provider appointments to discuss
naloxone prescribing, opioid safety initiative, and risks
of long-term opioid therapy
• Provider education at Mental Health and Primary
Care huddles
101

\
Overdose Education &
Naloxone Distribution
(OEND)
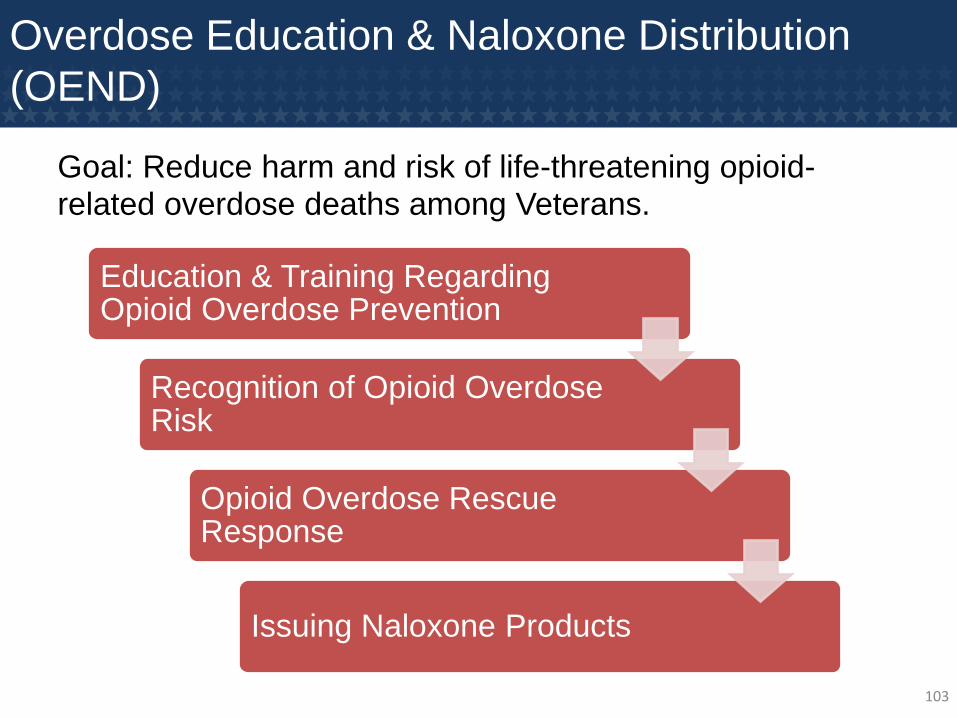
Overdose Education & Naloxone Distribution
(OEND)
Goal: Reduce harm and risk of life-threatening opioid-related overdose deaths among Veterans.
Education & Training Regarding Opioid Overdose Prevention
Recognition of Opioid Overdose Risk
Opioid Overdose Rescue Response
Issuing Naloxone Products
103

OEND Education & Training
• Targeted Academic Detailing Campaign by
Clinical Pharmacy Specialists
- Appropriate candidates for naloxone kits
- Appropriate use of naloxone kits
• Patient Education by Mental Health Clinical
Pharmacy Specialists
– 2015: Naloxone required restricted drug consult in
order to ensure each patient received appropriate
education regarding naloxone use
– 2016: Naloxone un-restricted in order to increase
accessibility to patients
104

Naloxone Provider Education: Academic Detailing
Naloxone rate of prescribing
was >3 times higher in
providers visited by
Academic Detailing vs. Non-
Detailed providers 1 year
after first OEND-related AD
visit, and was >7 times
greater at 2 years.
Average rate of increase in
naloxone prescribing was
7.1% greater in the AD-
exposed versus the AD-
unexposed providers (95%
CI: 2.0%, 12.5%)
Harvey M. Comprehensive Addiction and Recovery Act (CARA): ADS Updates. VHA PBM Academic Detailing Service. 2017 May.105

Naloxone Patient Education: Academic
Detailing Initiative
• Mailed brochure to all patients considered at high risk for opioid overdose
106
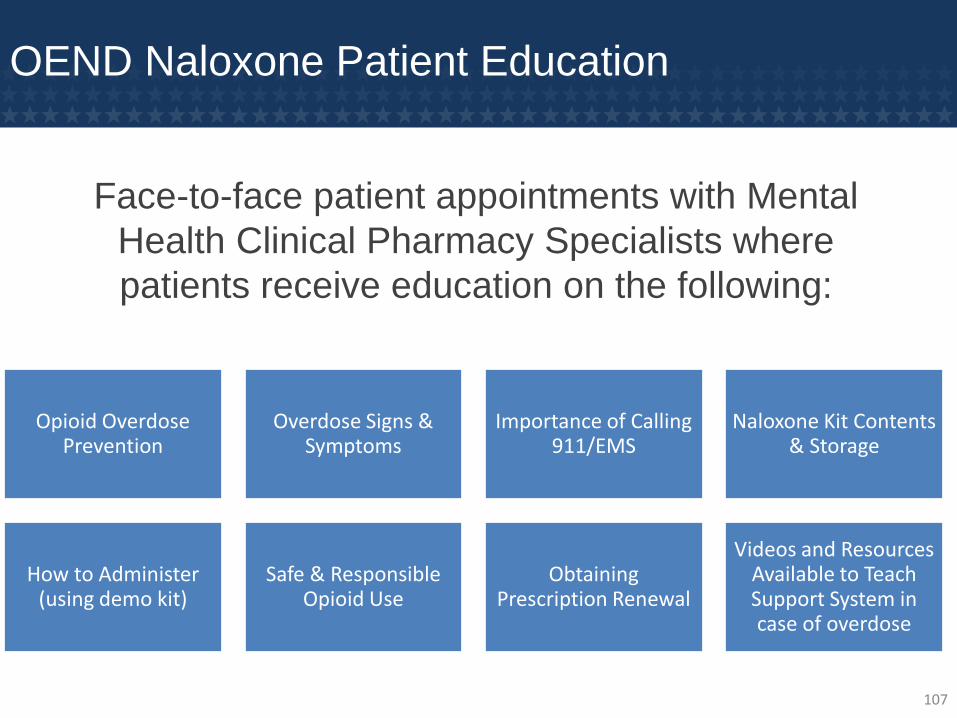
OEND Naloxone Patient Education
Face-to-face patient appointments with Mental
Health Clinical Pharmacy Specialists where
patients receive education on the following:
Opioid Overdose Prevention
Overdose Signs & Symptoms
Importance of Calling 911/EMS
Naloxone Kit Contents & Storage
How to Administer (using demo kit)
Safe & Responsible Opioid Use
Obtaining Prescription Renewal
Videos and Resources Available to Teach Support System in case of overdose
107
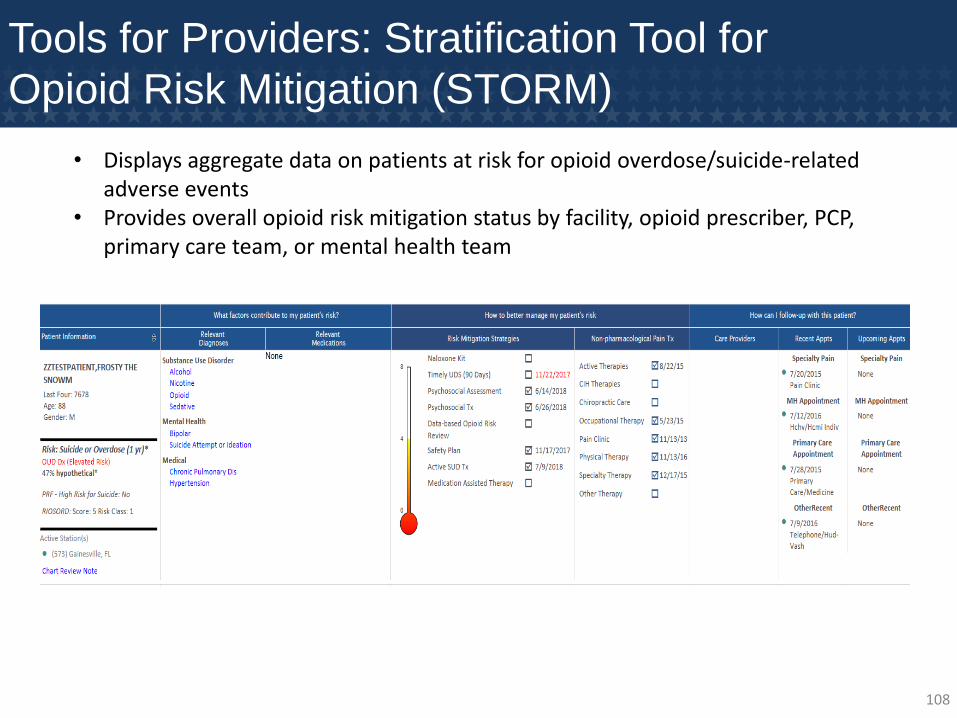
Tools for Providers: Stratification Tool for
Opioid Risk Mitigation (STORM)
• Displays aggregate data on patients at risk for opioid overdose/suicide-related adverse events
• Provides overall opioid risk mitigation status by facility, opioid prescriber, PCP, primary care team, or mental health team
108

\
Opioid Use Disorder
(OUD)
Opioid Use Disorder: Goals
Identify patients at high risk of opioid use disorder
Educate providers about proper diagnosis of opioid use disorder
Engage and treat Veterans diagnosed with opioid use disorder using pharmacotherapy or alternative treatments for chronic pain
110
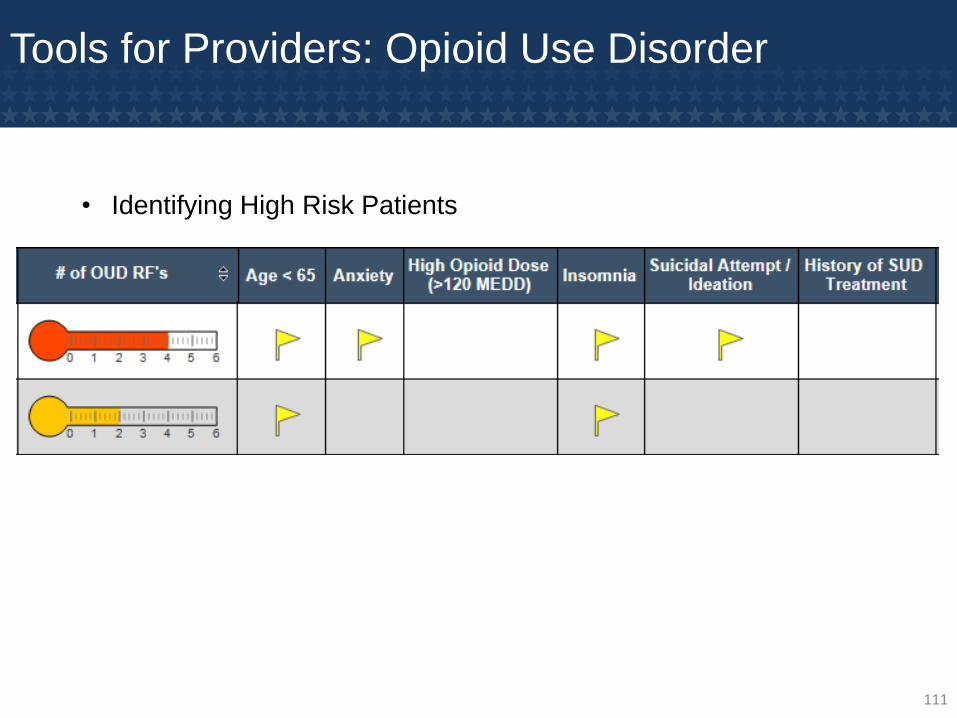
Tools for Providers: Opioid Use Disorder
• Identifying High Risk Patients
111
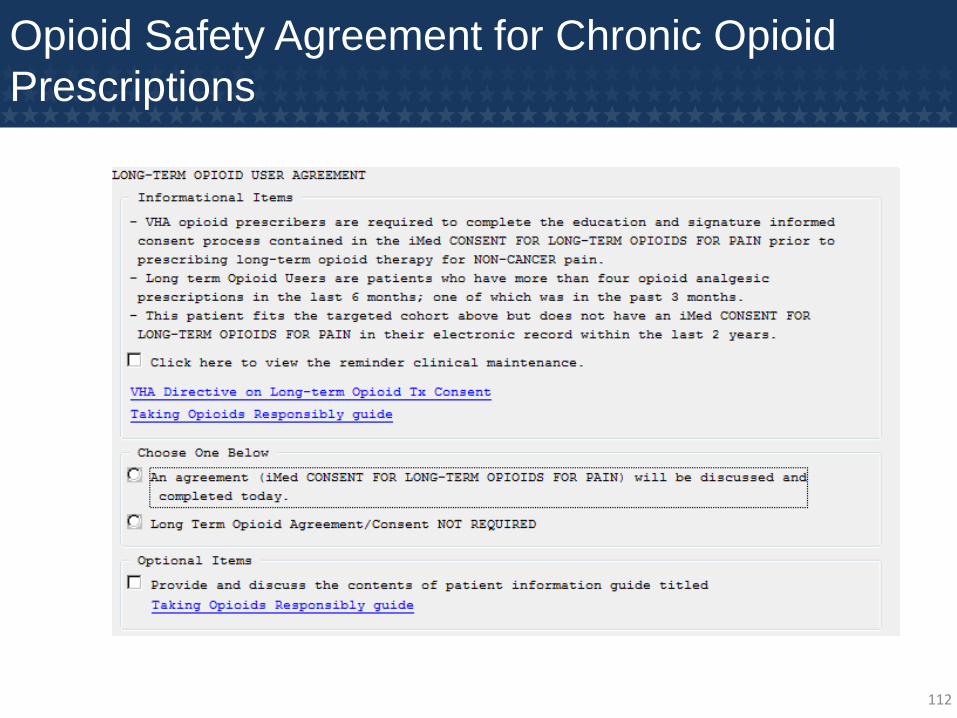
Opioid Safety Agreement for Chronic Opioid
Prescriptions
112
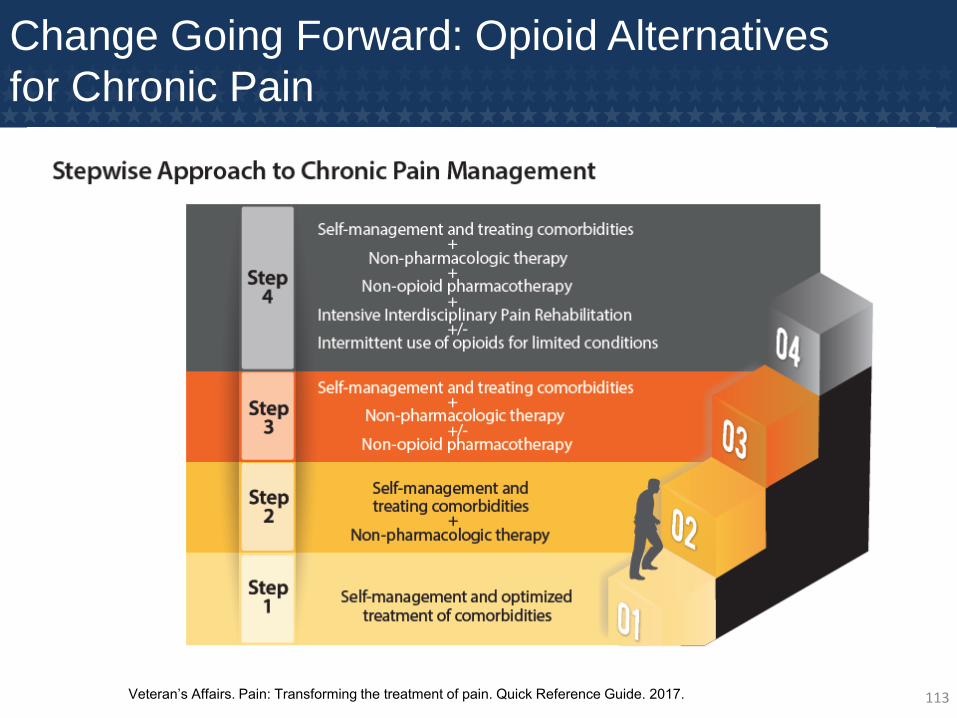
Change Going Forward: Opioid Alternatives
for Chronic Pain
Veteran’s Affairs. Pain: Transforming the treatment of pain. Quick Reference Guide. 2017. 113

Managing Chronic Pain: Complementary
Treatments
• Cognitive Behavioral Therapy
• Physical Therapy
• Yoga
• Tai Chi
• Mindfulness Meditation Group
• Hypnosis
• Biofeedback
• Battlefield Acupuncture
114
Conclusions
• Multiple tools available to providers to assist with identifying high-risk patients and educating patients on safe use of opioids– Potential limitations include time constraints with both
primary care providers and mental health providers given large patient panels
– Opportunity for team management approach
• Objectives going forward:– Marketing use of non-opioid therapy for chronic pain and
acute pain
– Increased patient education on risk of opioid overdose and role of naloxone
– Expanding scope of complementary treatments offered
115

\
Q & AAshleigh Powers, PharmD
PGY2 Ambulatory Care Pharmacy Resident
Ginger Ervin, PharmD
Associate Chief, Clinical Pharmacy Service

Primary Care
Panel Management and Oversight
061118

Primary Care: Overview
• Primary Care (Medical Center)
• Red, White, Blue, Palmetto, & Freedom Teams
• Women’s Clinic
• SCI
• Geri PACT
• Employee Health
• Community Based Care Service
• 4 Primary Care Community Based Outpatient Clinics (CBOCs)
Spartanburg, Florence, Sumter, & Orangeburg
• 2 Multi-Specialty CBOCs
Anderson & Greenville
• 1 Contract CBOC
Rock Hill
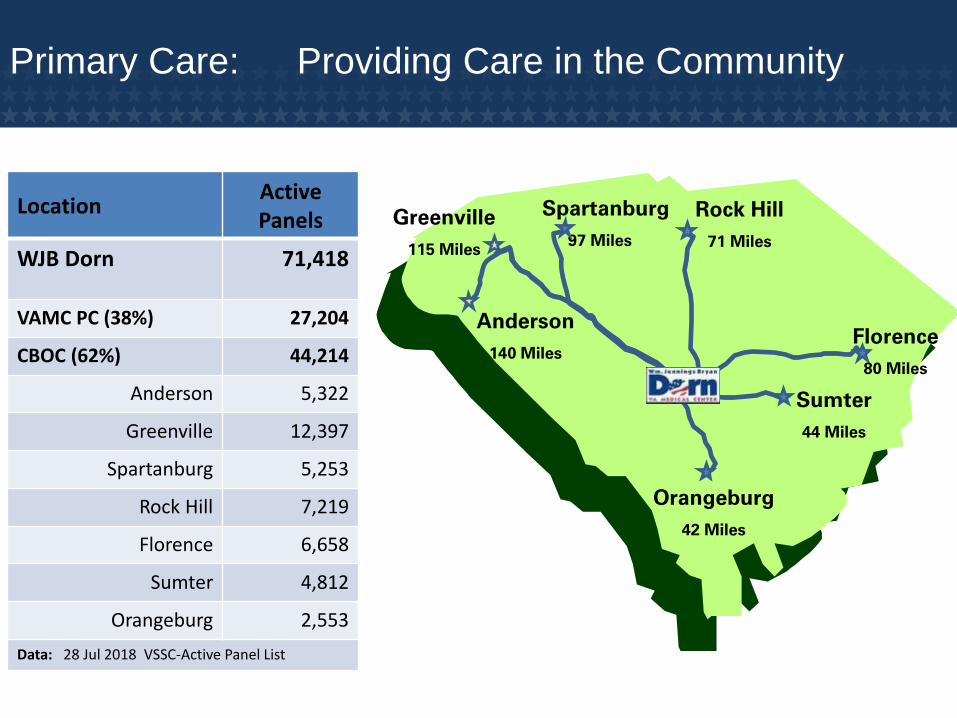
Primary Care: Providing Care in the Community
Orangeburg
42 Miles
Rock Hill
71 Miles
Anderson
140 Miles
Greenville
115 Miles
Spartanburg
97 Miles
Florence
80 Miles
Sumter
44 Miles
LocationActive Panels
WJB Dorn 71,418
VAMC PC (38%) 27,204
CBOC (62%) 44,214
Anderson 5,322
Greenville 12,397
Spartanburg 5,253
Rock Hill 7,219
Florence 6,658
Sumter 4,812
Orangeburg 2,553
Data: 28 Jul 2018 VSSC-Active Panel List

Primary Care: Catchment Areas
Anderson
Greenville
Spartanburg
Rock Hill
Florence
Sumter
Orangeburg
WJB Dorn VAMC

Primary Care: Patient Aligned Care Teams (PACT)
• Patient Centered
• Patient Driven
• Team approach
• Proactive not reactive
• Working at the top of your license and
competency
• Enhanced communication
• Collaboration
• Working smarter not harder
• Increased access for non face to face visits
(phone, secure messaging, mail)
ProviderRN Care Manager
Veteran LPN MSA
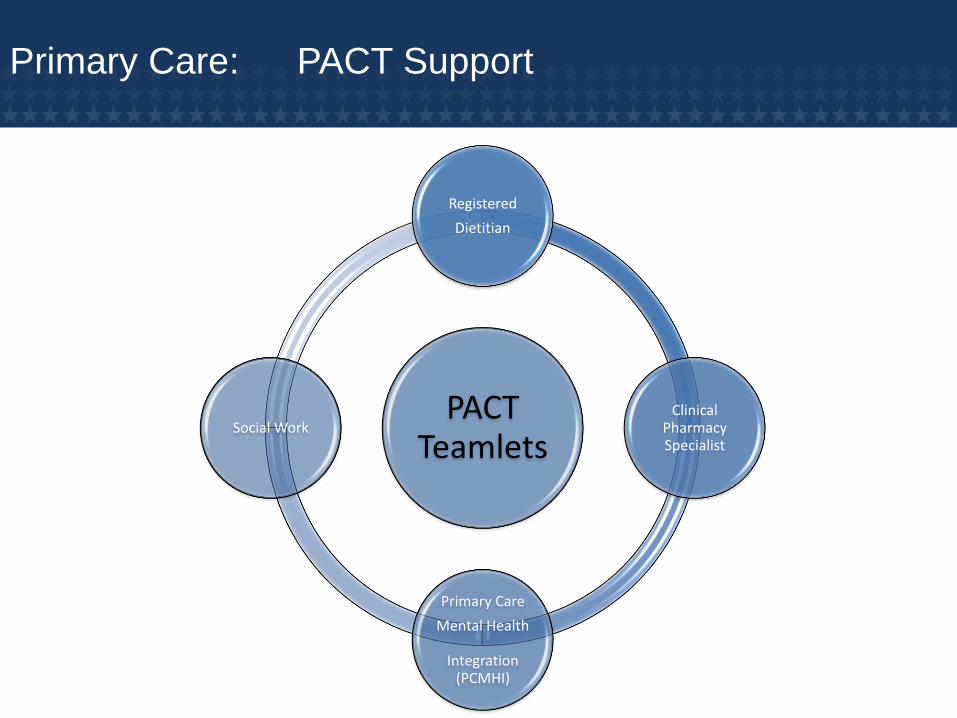
Primary Care: PACT Support
PACT Teamlets
Registered
Dietitian
Clinical Pharmacy Specialist
Primary Care
Mental Health
Integration (PCMHI)
Social Work
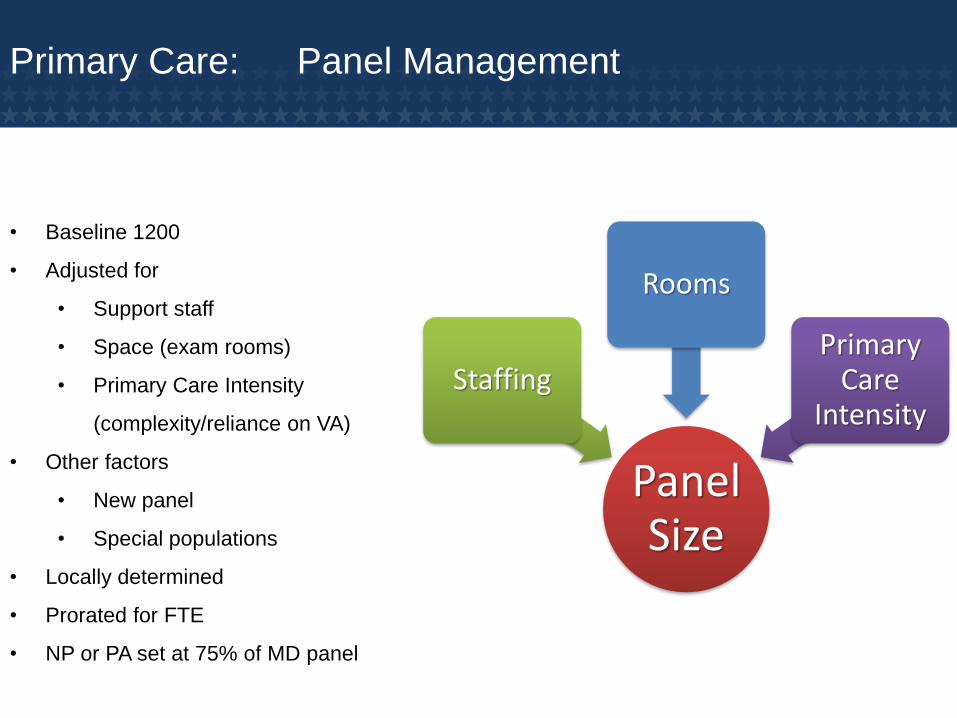
Primary Care: Panel Management
• Baseline 1200
• Adjusted for
• Support staff
• Space (exam rooms)
• Primary Care Intensity
(complexity/reliance on VA)
• Other factors
• New panel
• Special populations
• Locally determined
• Prorated for FTE
• NP or PA set at 75% of MD panel
Panel Size
Staffing
Rooms
Primary Care
Intensity

Primary Care: Primary Care Management Module
(PCMM)
• Patient assignments to Team
• Patient inactivation from Team
• Patient assignments to PCP/associate providers
• Preceptor : associate provider assignments
• Team membership
• PCP FTEE
Tracks and manages
Calculates actual panel size
Monitors panel capacity
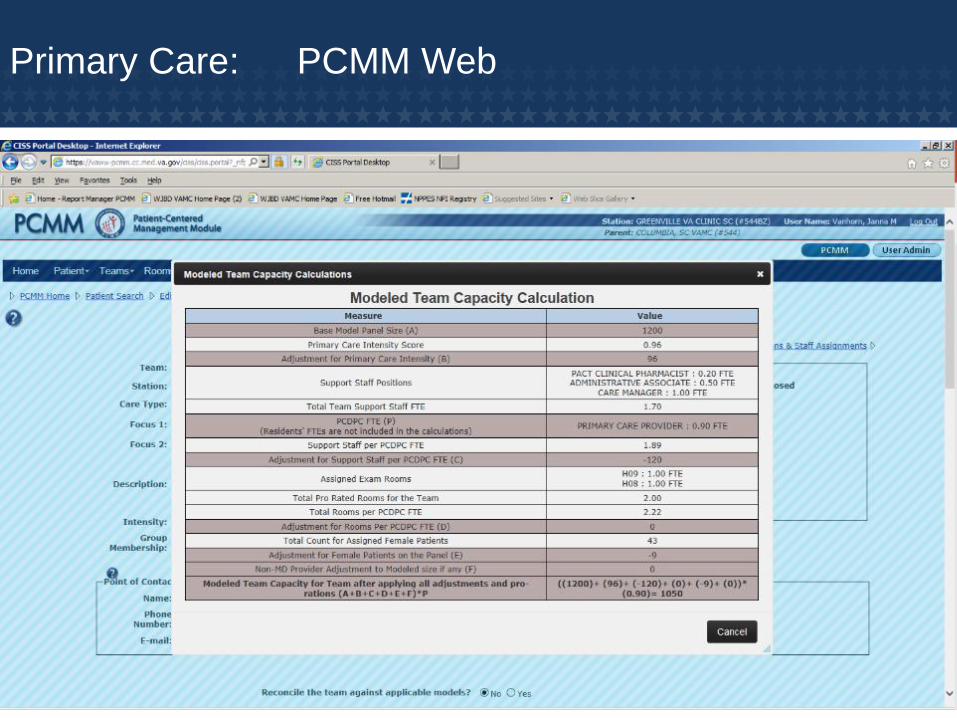
Primary Care: PCMM Web

Primary Care: ACCESS TO CARE
• Access to Care
0
5
10
15
20
25
30
WJB DornVAMC
Greenville VAClinic
Florence VAClinic
Rock Hill VAClinic
Anderson VAClinic
OrangeburgVA Clinic
Sumter VAClinic
SpartanburgVA Clinic
5 5 3 2 5 4 4
11
2426
19
11
18
21
Established Wait New Wait

Primary Care: Expansion
•Multi-Specialty CBOC (Approximately 77,000 GSF
•Opened: August 2013Greenville
•Multi-Specialty CBOC (Approximately 64,000 GSF)
•Opened: February 2016Anderson
•Replacement CBOC / New Construction Project
•Approximately 24,000 GSFOrangeburg
•Replacement CBOC / New Construction Project
•Approximately 29,000 GSFSumter
•Contract Transition / New Construction Project
•Approximately 29,000 GSFRock Hill
•Building 10 Reconstruction Project (20,000 GSF)
•Expansion/New Construction Project (6,000 GSF)Primary Care

Q & A
Comprehensive Emergency Management
061118
XXX
XXX
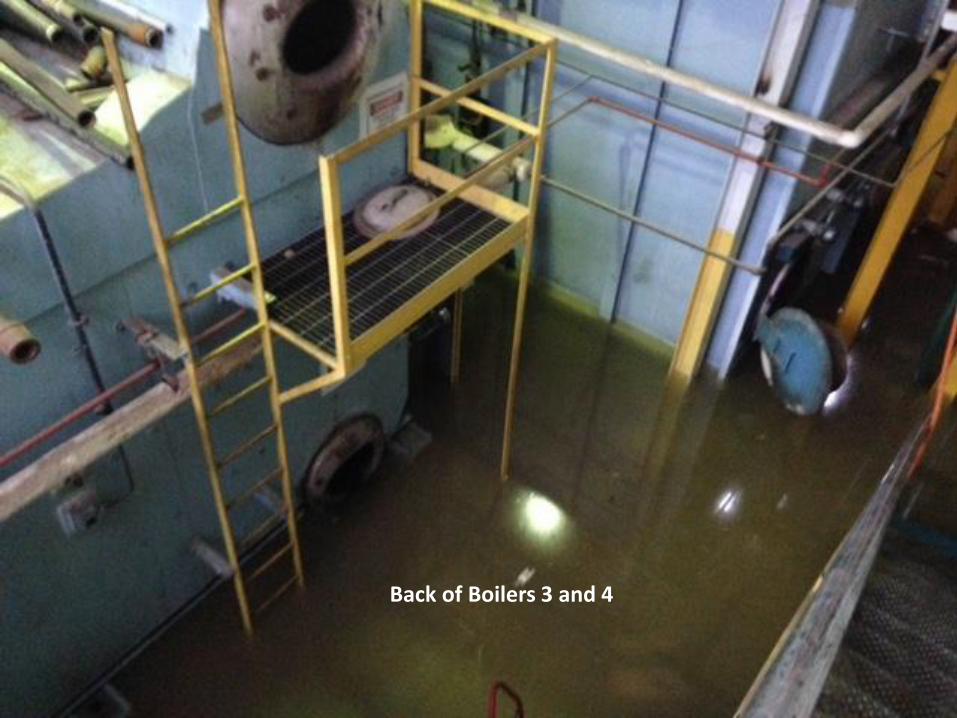
Back of Boilers 3 and 4

Pump Room Looking at Tunnels
Pump Room Looking at Feed Pumps
Back Stairwell


XXX
XXX
National Response Framework
The National Response Framework (NRF) is a guide to how the Nation responds to all
types of disasters and emergencies.
• It is built on scalable, flexible, and adaptable concepts identified in the National
Incident Management System (NIMS) to align key roles and responsibilities across
the Nation.
• This Framework describes specific authorities and best practices for managing
incidents that range from the serious but purely local to large-scale terrorist attacks
or catastrophic natural disasters.
• This Framework is always in effect, and elements can be implemented at any
time. The structures, roles, and responsibilities can be partially or fully implemented
in the context of a threat or hazard, anticipation of an event, or response to an
incident.
National Response Framework
• Selective implementation of Framework structures and procedures allows for a
scaled response, delivery of the specific resources and capabilities, and a level of
coordination appropriate to each incident.
• The Response mission area focuses on responding effectively to all types of
incidents that range from those that are adequately handled with local assets to
those of catastrophic proportion that require marshaling the capabilities of the entire
Nation.
• The objectives of the Response mission area define the capabilities necessary to
save lives, protect property and the environment, meet basic human needs, stabilize
the incident, restore basic services and community functionality, and establish a
safe and secure environment moving toward the transition to recovery.
National Response Framework
• The Response mission area includes 14 core capabilities:
o Planning
o Public information and warning
o Operational coordination
o Critical transportation
o Environmental response/health and
safety
o Fatality management services
o Infrastructure systems
o Mass search and rescue operations
o Operational communications
o Public health and medical services
o Mass care services
o On-scene security and protection
o Public and private services and
resources
o Situational assessment.

Emergency Support Functions (ESF) of the
National Response Framework
Major role in ESF #8—Public Health and Medical Services:
• Coordinates with participating NDMS hospitals to provide incident-related medical
care to authorized NDMS beneficiaries affected by a major disaster or emergency.
• Furnishes available VA hospital care and medical services to individuals
responding to, involved in, or otherwise affected by a major disaster or
emergency, including members of the Armed Forces on active duty.
• Designates and deploys available medical, surgical, mental health, and other
health service support assets.
• Provides a Medical Emergency Radiological Response Team
for technical consultation on the medical
management of injuries and illnesses due
to exposure to or contamination by ionizing radiation.
• Alerts VA FCCs (Federal Coordinating Centers)
to activate NDMS patient reception plans in a
phased, regional approach and when appropriate,
in a national approach.
Emergency Support Functions (ESF) of the
National Response Framework
In addition to ESF #8 the VA also has support responsibilities under the following
ESF annexs:
• ESF #3 – Public Works and Engineering
• Provide engineering personnel and support,
including design estimation and construction
supervision for repair, reconstruction, and
Restoration of eligible facilities.
• ESF #5 – Information And Planning
• Provides accurate and timely information
related to an actual or potential incident.
• Develops and executes plans related to
an actual or potential incident.
• Develops operational plans and procedures
to inform internal coordination and execution
of objectives and tasks set forth in the NRF
and Federal Interagency Operational Plans.
Emergency Support Functions of the National
Response Framework
• ESF #6 – Mass Care, Emergency Assistance, Housing, and Human Services
• May provide for food preparation and stockpiling in its facilities during the
incident, as well as facilities for mass sheltering.
• Provide medical supplies and services and medical workers to augment
health services personnel to support mass care operations.
• Administers the laws providing benefits and other services to veterans and
the dependents and beneficiaries of veterans.
• During incident operations, provide emergency healthcare services to veteran
beneficiaries in VA medical facilities,
to active duty military personnel, and
as resources permit, to civilians in
communities affected by national security
emergencies.
Emergency Support Functions of the National
Response Framework
• ESF #7 – Logistics Management and Resource Support
• Provide technical assistance to identify and procure medical supplies and
other medical services.
• Provide personnel knowledgeable in Federal procurement and distribution
operations.
• Provide computer support operations as appropriate.
• ESF #13 – Public Safety and Security
• Participate in the ESF #13 Stakeholder Committee and Advisory Board.
• Provide general and specialized resources to assist in the ESF #13
response.
• ESF #15 – External Affairs• Support the National Response Framework ESF #15 organization and staff.
Federal Response and Assistance under the
Stafford Act
• When an incident is anticipated to exceed
state resources or when the Federal
Government has unique capabilities needed
by states, the governor may request Federal
assistance. In such cases, the affected local
jurisdiction, the state and Federal
governments coordinate to provide the
necessary assistance. Assistance in the form
of funding, resources, and services may be
provided. Federal departments and agencies
respect the sovereignty and responsibilities of
local, state governments while rendering
assistance that supports the affected local or
state governments.
• Before requesting a declaration the situation
or disaster must be of such that an effective
response is beyond the capabilities of the
state and the affected local governments and
requires Federal assistance.
Federal Departments and Agencies Acting Under
Their Own Authorities
• Immediate lifesaving assistance to states, as well as other types of assistance, are
performed by Federal departments or agencies under their own authorities and
funding or through reciprocal mutual assistance agreements and do not require a
Stafford Act declaration (Humanitarian Support).
• The Dorn VA Medical Center participates with our state and local partners in
Emergency Management preparations and participates in exercises as members
of the Midlands Regional Healthcare Coalition and the South Carolina Hospital
Association.
Q & A

Closing Comments
061118