Embed Size (px)
Citation preview

Case History WitH subspeCialty input
Dr sarah stewart (pediatrics, First-year resident)
The patient was a term, appropriate-for-gestational-age, male infant born via normal spontaneous vaginal delivery who presented at birth with a full-body rash. The rash appeared as diffuse discrete erythematous papules and plaques with occasional overlying fluid-filled vesicles and bullae, most prominent on the face and scalp but sparing mucous membranes, palms, and soles (Figs 1 and 2). He was well-appearing with normal vital signs, Apgar scores of 8 and 9, a birth weight of 3768 g, and an examination with results that were otherwise normal. His mother’s pregnancy was remarkable for presumed herpes zoster at 31 weeks that resolved with valacyclovir. She had a history of primary varicella-zoster at 2 years of age and 2 episodes of herpes zoster before this pregnancy. Labor and delivery were complicated by a prolonged rupture of membranes (20 hours) and meconium-stained fluid. Though maternal prenatal laboratory
tests were negative for infection, the patient’s mother received 3 doses of clindamycin because of a history of previous neonatal group B Streptococcus (GBS) infection. The patient’s father had a history of herpes labialis. The patient’s mother denied any history of herpes labialis or herpes genitalis.
The patient’s initial laboratory results at 2 hours of life included a white blood cell count of 24.4 K/µL (normal: 7.5–30.0 K/µL) with 74% neutrophils (normal: 32.0%–68.0%), 20% lymphocytes (normal: 24.0%–36.0%), 4% monocytes (normal: 0.0%–0.9%), 1% eosinophils (normal: 0.0%–2.0%), and 0% basophils (normal: 0.0%–1.0%); a C-reactive protein (CRP) level of 0.03 mg/dL (normal: 0.00–0.99 mg/dL); a blood glucose level of 32 mg/dL (normal: 45–110 mg/dL); an aspartate aminotransferase level of 68 IU/L (normal: 15–41 IU/L); an alanine transaminase level of 8 IU/L (normal: 11–63 IU/L); a total bilirubin level of 3.1 mg/dL (normal: 2.0–6.0 mg/dL); and an alkaline phosphatase level of 110 IU/L (normal: 30–300 IU/L). The remaining results of the
Well-Appearing Newborn With a Vesiculobullous Rash at BirthSarah E. Stewart, MD, a Jody L. Lin, MD, b Jennifer L. Everhart, MD, b Trung H. Pham, MD, PhD, c Ann L. Marqueling, MD, d, e Kerri E. Rieger, MD, PhD, d, f Sarah L. Hilgenberg, MDb
A term, appropriate-for-gestational-age, male infant born via normal spontaneous vaginal delivery presented at birth with a full-body erythematous, vesiculobullous rash. He was well-appearing with normal vital signs and hypoglycemia that quickly resolved. His father had a history of herpes labialis. His mother had an episode of herpes zoster during pregnancy and a prolonged rupture of membranes that was adequately treated. The patient underwent a sepsis workup, including 2 attempted but unsuccessful lumbar punctures, and was started on broad-spectrum antibiotics and acyclovir, given concerns about bacterial or viral infection. The rash evolved over the course of several days. Subsequent workup, with particular attention to his history and presentation, led to his diagnosis.
abstract
PEDIATRICS Volume 141, number 3, March 2018:e20170236 Diagnostic Dilemmas
to cite: Stewart SE, Lin JL, Everhart JL, et al. Well-Appearing Newborn With a Vesiculobullous Rash at Birth. Pediatrics. 2018;141(3):e20170236
Divisions of aGeneral Pediatrics, bPediatric Hospital Medicine, and cPediatric Infectious Diseases, Department of Pediatrics, Lucile Packard Children’s Hospital Stanford, Palo Alto, California; and Departments of dDermatology, ePediatrics, and fPathology, School of Medicine, Stanford University, Stanford, California
Dr Stewart contributed to the conception and design of the case presentation, drafted the initial manuscript, and reviewed and revised the manuscript; Drs Lin and Everhart contributed to the conception and design of the case presentation and reviewed and revised the manuscript; Drs Pham, Marqueling, and Reiger drafted their sections of the initial manuscript and reviewed and revised the manuscript; Dr Hilgenberg contributed to the conception and design of the case presentation, drafted portions of the initial manuscript, and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted.
Doi: https:// doi. org/ 10. 1542/ peds. 2017- 0236
Accepted for publication Jul 17, 2017
Address correspondence to Sarah E. Stewart, MD, Division of General Pediatrics, Department of Pediatrics, Lucile Packard Children’s Hospital, 725 Welch Rd, Mail Code 5906, Palo Alto, CA 94304. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2018 by the American Academy of Pediatrics
FinanCial DisClosure: Dr Lin received support from the KL2 Mentored Career Development Award of the Stanford Clinical and Translational Science Award to Spectrum (NIH KL2 TR 001083, UL1 TR 001085) and the Clinical Excellence Research Center; the other authors have indicated they have no financial relationships relevant to this article to disclose.
FunDinG: No external funding.
by guest on August 15, 2020www.aappublications.org/newsDownloaded from

complete blood cell (CBC) count and comprehensive metabolic panel were unremarkable.
Dr Hilgenberg, as a pediatric hospitalist assuming care of this infant after birth, what is your differential diagnosis?
Dr Hilgenberg (pediatric Hospitalist)
This infant’s presentation is most concerning for one of the following: (1) a congenital “TORCH” infection, which is an infection caused by toxoplasmosis, other pathogens (varicella-zoster virus [VZV], syphilis, enteroviruses, or parvovirus B19), rubella, cytomegalovirus, or herpes simplex virus (HSV)1; (2) bacterial sepsis, given the mother’s previous neonatal GBS infection with her last pregnancy2; and (3) a primary dermatologic condition such as epidermolysis bullosa (EB).
Dr stewart
How and when do TORCH infections typically present? What, if any, are their dermatologic manifestations, given that skin lesions are our patient’s only sign of illness?
Dr Hilgenberg
Interestingly, the majority of live-born infants with TORCH infections are asymptomatic at birth.3 When symptomatic, common features can include microcephaly, intrauterine growth restriction, jaundice,
hepatosplenomegaly, intracranial calcifications, and rash, as well as laboratory abnormalities. Despite these common features, some clinical manifestations are more suggestive of particular infections in the neonate.
For instance, congenital toxoplasmosis has 4 subtypes: subclinical, severe neonatal disease, mild or severe disease in the first few months of life, and sequelae or relapse of an undiagnosed, typically ocular, infection later in childhood. The minority of patients who are symptomatic at birth may present with the classic triad of chorioretinitis, hydrocephalus, and intracranial calcifications. Dermatologic features include a maculopapular, petechial, or purpuric rash.1, 3 Additional signs and symptoms include fever, seizures, generalized lymphadenopathy, thrombocytopenia, mononuclear
cerebrospinal fluid pleocytosis, or elevated cerebrospinal fluid protein. The incidence of congenital toxoplasmosis in the United States is 1 in 1000 to 1 in 10 000 newborns.4
Congenital syphilis is characterized as either early, presenting before 2 years of age but typically within the first 5 weeks of life, or late, presenting after 2 years of age. Differentiating findings among infants with early congenital syphilis include nasal discharge, maculopapular rash (particularly on the palms, soles, and diaper area), generalized lymphadenopathy, and skeletal abnormalities. Patients with late congenital syphilis present with physical anomalies, such as teeth or bony abnormalities, but rarely present with rash. The Centers for Disease Control and Prevention reports that the incidence of congenital syphilis in the United
STEWART et al2
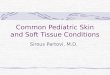
FiGure 1Patient on first day of life. Coalescing erythematous vesicles are seen on the face, and dull gray and erythematous patches and plaques are seen on the body and extremities. The mucous membranes, hands, and the soles of the feet are spared.
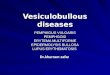
FiGure 2A, Lesions on the first day of life. B, New lesions on fingers on the fourth day of life. C, New lesions on cheeks on the fourth day of life. D, Lesions on the fifth day of life. The forehead vesicles became less raised and less erythematous. A few new lesions appeared on the scalp.
by guest on August 15, 2020www.aappublications.org/newsDownloaded from

States is 11.6 cases per 100 000 newborns.5
Congenital rubella syndrome can include sensorineural hearing loss, ocular disease (cataracts, congenital glaucoma), cardiac defects, bone disease, hemolytic anemia, thrombocytopenia, “blueberry muffin rash, ” or petechiae and purpura caused by dermal erythropoiesis.3 After the development of the rubella vaccine in 1969 and widespread use shortly thereafter, the incidence of congenital rubella in the United States is <1 case per year.6
Cytomegalovirus, the most common congenital viral infection in the United States, with an incidence of 0.5% to 1.0% in all newborns, causes symptoms at birth in 10% of infected infants.7 Differentiating clinical features may include sensorineural hearing loss, periventricular intracranial calcifications, chorioretinitis, seizures, thrombocytopenia, and rash with a petechial, morbilliform, or widespread erythematous, macular appearance.
Congenital HSV infection is relatively rare, with an incidence of 1 in 3000 to 1 in 20 000 newborns, and infants may exhibit the characteristic triad of skin findings (scarring, active lesions, hypo- and hyperpigmentation, aplasia cutis, and/or an erythematous macular exanthem), eye damage, and severe central nervous system (CNS) manifestations.8, 9 Most newborns with perinatally acquired HSV appear normal at birth and then present within the first 1 to 6 weeks of life with infection symptoms localized to the skin, eyes, and mouth (SEM), involving the CNS, or disseminated.
Congenital varicella may present with cicatricial skin lesions, which may be pigmented or depressed in a dermatomal distribution, ocular disease, limb abnormalities, and
cortical atrophy or seizures. If present, the rash in both HSV and VZV is vesicular in nature. The Centers for Disease Control and Prevention reports that the incidence of congenital varicella in the United States is 0.4% to 2.0% of newborns born to mothers with varicella in the first or second trimester. Neonatal varicella, a much more severe and often life-threatening condition, can occur when the mother develops varicella in the time period 5 days before the delivery through 2 days after delivery.10
Parvovirus B19 can present with ocular anomalies, hydrocephalus, musculoskeletal problems, hepatocellular damage, heart defects, and subcutaneous edema, as well as petechiae.3
Dr stewart
How does the rest of your differential diagnosis inform the next steps in this infant’s management?
Dr Hilgenberg
Bacterial sepsis, most commonly caused by GBS in the neonatal period, typically presents within the first 24 to 48 hours of life and is associated with low birth weight, hypothermia, lethargy, poor feeding, and an elevation of CRP levels. Respiratory distress and cardiac symptoms may be present if these organ systems are involved. Cutaneous manifestations are less common, but they can occur.11
The fact that our patient is overall well-appearing and well-developed with normal vital signs and without significant laboratory abnormalities argues against a congenital TORCH infection or bacterial sepsis. His rash is not typical of those seen in toxoplasmosis, syphilis, rubella, cytomegalovirus, or parvovirus B19. Therefore, I would send blood and lesion cultures to test for bacteria and HSV/VZV polymerase chain reactions (PCRs). Though the patient appears hemodynamically
stable, meningitis is a potentially devastating consequence of TORCH infections and bacterial sepsis, so lumbar puncture should be considered. I would be inclined to start empirical treatment with broad-spectrum antibiotics for possible bacterial sepsis and antiviral agents for possible HSV or VZV. Lastly, I would consider a dermatology consultation, depending on how the clinical course evolves.
Dr stewart
The patient underwent a sepsis workup. Lumbar puncture was attempted and unsuccessful. A lesion bacterial culture and serum and lesion HSV/VZV PCRs were obtained. The patient was started on intravenous ampicillin, gentamicin, and acyclovir. He was feeding, urinating, and stooling normally with a continued overall well appearance.
Dr Pham, as a pediatric infectious disease specialist, what are you most concerned about, given this patient’s presentation and history? Are there other studies you would recommend?
Dr pham (pediatric infectious Disease)
The patient has been well-appearing and neurologically appropriate with normal vital signs despite the extensive rash. His CBC panel, CRP test, liver function test (LFT), and blood culture results are reassuring to date. In terms of infectious etiologies, the differential diagnosis for a diffuse vesiculobullous rash in newborns, as seen in this patient, would include viral infections such as HSV and VZV, staphylococcal and streptococcal skin infections, listeriosis, congenital candidiasis, and congenital syphilis.12
Neonatal HSV infection seems unlikely, given how early the lesions appeared (at birth) and given his lack
PEDIATRICS Volume 141, number 3, March 2018 3 by guest on August 15, 2020www.aappublications.org/newsDownloaded from

of systemic symptoms with this level of cutaneous severity. Approximately 85% of HSV infections in newborns are transmitted intrapartum, and 10% are transmitted postnatally.13 Congenital or intrauterine HSV infection is very rare, accounting for only ∼5% of neonatal cases, and is often accompanied by congenital malformations, which our patient does not appear to have.13, 14 As Dr Hilgenberg pointed out, clinical manifestations of neonatal HSV infections usually fall into 3 disease types: SEM disease, CNS disease, and disseminated disease. SEM disease accounts for 45% of cases and typically presents at 10 to 14 days of life.15– 17 Skin manifestations typically include small clustered vesicles with surrounding erythema that mature into pustules and then erosions with overlying eschar formation over 1 to 3 days. Lesions begin at the site of inoculation, most commonly at sites of skin injury or prolonged contact with the cervix, and have the potential to spread locally or disseminate more broadly. In contrast, congenital HSV commonly presents with vesicles at birth. Cutaneous scars often are also present.18 CNS disease represents 30% of cases, with onset at ∼16 to 19 days. Disseminated disease, accounting for the remaining 25%, usually presents at 7 to 12 days, with many cases at <7 days.17 However, newborns with disseminated HSV infections are often critically ill, and 60% to 75% have CNS involvement.13, 17
VZV is also unlikely because the patient’s mother has a history of primary varicella in early childhood, corroborated by her history of subsequent episodes of zoster. Thus, her dermatomal eruption during pregnancy should reflect a localized reactivation of VZV rather than a primary varicella infection, which would have put the infant at risk for congenital or neonatal VZV transmission. Viremia from
VZV reactivation has only been reported on rare occasions in immunocompromised individuals who have disseminated disease. Evidence linking zoster during pregnancy with congenital varicella is lacking.19, 20
Staphylococcal and streptococcal skin infection, listeriosis, and congenital candidiasis are possible; however, given the extensive skin manifestation, it would be unusual to have such a well-appearing infant with normal vital signs and benign laboratory results. Lastly, congenital syphilis is also less likely, because the maternal syphilis screen during pregnancy had negative results and because the infant, apart from the rash, has no other clinical manifestations suggestive of syphilis.
In terms of management, empirical coverage with acyclovir, principally for HSV at this point, is prudent while the patient is being worked up for neonatal HSV.9 However, our suspicion of HSV, particularly of CNS and disseminated disease, is low. Thus, we do not recommend repeating lumbar puncture at this point. We agree with obtaining HSV and VZV PCRs from blood and HSV PCRs from the conjunctivae, nares, oropharynx, and rectum. In addition, we recommend that HSV/VZV PCRs, a Gram-stain, a bacterial culture, a potassium hydroxide stain, and a fungal culture be obtained from the lesions. An ophthalmology exam to complete the workup for TORCH infections, including neonatal HSV disease, should also be performed. The patient has been on ampicillin and gentamicin, empirically, for bacterial sepsis. Given the lack of signs and symptoms suggestive of sepsis, it would be reasonable to discontinue empirical antibiotics if the blood culture is negative for bacteria at 48 hours. Lastly, it is important to consider noninfectious etiologies for this rash, such as primary dermatologic conditions.
Dr stewart
Dr Pham, would you recommend starting varicella-zoster immune globulin (VariZIG) for possible varicella?
Dr pham
We would not recommend VariZIG at this point. Based on maternal history and timing of clinical presentation, our suspicion of primary varicella in this infant is low. Required criteria for VariZIG administration are significant exposure to varicella (such as being an exposed newborn) and inclusion in one of the following populations: (1) immunocompromised children, (2) pregnant women without evidence of immunity, (3) newborns whose mothers had an onset of chickenpox between 5 days before delivery and 48 hours after delivery (VariZIG is not indicated if the mother has zoster), (4) hospitalized premature infants of ≥28 weeks’ gestation whose mothers lack immunity against VZV, and (5) hospitalized premature infants of <28 weeks’ gestation or with a birth weight of 1000 g or less, regardless of maternal immunity.18, 21
Dr stewart
A pediatric ophthalmologist was consulted and found no evidence of conjunctivitis, keratitis, cataracts, optic nerve swelling, chorioretinitis, or uveitis. Over the next 72 hours, new similar lesions appeared on the infant’s face, scalp, hands, and feet. The older lesions became dull and flat. A pediatric dermatologist was consulted.
Dr Marqueling, as a pediatric dermatologist, what is your differential diagnosis for this rash?
Dr Marqueling (pediatric Dermatology)
In addition to the infectious disease etiologies, bullous diseases presenting in the neonatal period should be
STEWART et al4 by guest on August 15, 2020www.aappublications.org/newsDownloaded from

considered. In particular, I am concerned about bullous mastocytosis, given the vesicles and small bullae with overlying erythematous and edematous papules and plaques and the questionably present Darier’s sign on my examination. Bullous lesions in cutaneous mastocytosis usually develop within erythematous papules or plaques on involved skin. Other conditions I would include in my differential diagnosis, though extremely uncommon, are chronic bullous disease of childhood (linear immunoglobulin A disease), EB (including bullous dermolysis of the newborn), and epidermolytic ichthyosis. Chronic bullous disease of childhood is a rare autoimmune bullous disease that typically presents at 1 to 6 years of age with widespread, tense, bullae-forming rosettes. Rare reports of neonatal presentation with bullae at birth have been reported.22 EB is a group of inherited disorders characterized by skin fragility. Although severity later in life varies by type of EB, neonatal presentation may be similar in all types, presenting with generalized mechanically-induced blisters and erosions. Additional features may include absent or dystrophic nails and cutaneous localized absences of skin (large ulcers on the lower extremities, each with well-demarcated edges and a red, shiny base). Epidermolytic ichthyosis may present in ways that are nearly indistinguishable from EB, with spontaneous or mechanically-induced bullae as the most prominent feature. Features that may help to differentiate the 2 conditions include a thickened, red, and macerated base with bullae or raw denuded areas. Incontinentia pigmenti also crossed my mind, but as this is X-linked dominant trait, it is usually not compatible with life in male fetuses.23, 24
Dr stewart
You mention Darier’s sign. What is this, and what implication does
this possible finding have for our patient?
Dr Marqueling
Darier’s sign is said to be present when the skin urticates, becoming edematous and red, similar to a hive, after stroking it with a blunt object. It is caused by the release of histamine from mast cells and is seen in conditions such as mastocytosis.
Dr stewart
Do you have additional recommendations regarding diagnostic workup, given your concerns and exam findings?
Dr Marqueling
I would follow-up on blood and lesion cultures and PCRs and continue acyclovir until viral PCR results returned. Given my concern for possible bullous mastocytosis or a neonatal blistering disorder, I recommend a skin biopsy.
Dr stewart
After 48 hours, all cultures and PCRs were negative for infection, so anti-infectives were discontinued. A skin biopsy was performed. Dr Reiger, can you describe your findings?
Dr rieger (Dermatopathologist)
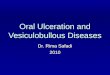
A skin biopsy showed an infiltrate of monomorphic cuboidal and fusiform cells in the upper third of the dermis (Fig 3). There was a mild superficial dermal edema, but there was no evidence of a subepidermal split. The cells in the infiltrate contained small central nuclei and lightly granular amphophilic cytoplasm, and they stained positive for CD117 and the mast cell tryptase, confirming the diagnosis of cutaneous mastocytosis. The mast cells did not express CD25. The expression of CD25 on cutaneous mast cells from adult patients with urticaria pigmentosa has been shown to be
predictive of systemic mastocytosis, although this has not been studied in the pediatric population.25 Regarding the other diagnoses on the differential, no viral cytopathic changes were identified, and an immunostain for HSV had negative results, providing no support for a herpetic infection. No neutrophilic infiltrate or subepidermal split were identified to support chronic bullous disease of childhood. No blister was identified to support an inherited blistering disease. Thus, overall, this skin biopsy was compatible with cutaneous mastocytosis.
Dr Marqueling, what is mastocytosis?
Dr Marqueling
The mastocytoses are disorders characterized by mast cell accumulation in tissues throughout the body. They are caused by a mutation in the c-tyrosine-kinase gene. It is estimated that <200 000 people total in the United States are affected.26 Severity ranges from cutaneous to systemic disease.27 Cutaneous mastocytosis accounts for ∼50% of cases, occurs primarily in children, and presents most often shortly after birth, with 80% of cases occurring before age 2 and 50% of cases resolving by adolescence.26, 28 The most common form is a solitary mastocytoma, presenting as a single tan to brown papule or small plaque. Infants with multiple lesions, ranging from a few to a couple hundred, are diagnosed with urticaria pigmentosa. In the most severe form, diffuse cutaneous mastocytosis, patients have nearly confluent erythema with a rough peau d’orange texture. When mast cells are stimulated, they may degranulate and release histamine, causing lesions of mastocytosis to become raised, or in some cases, to blister. A definitive diagnosis is made by confirming the presence of an accumulation of mast cells on skin biopsy.28 Darier’s sign, as described above, is common.27 Serum tryptase,
PEDIATRICS Volume 141, number 3, March 2018 5 by guest on August 15, 2020www.aappublications.org/newsDownloaded from

a marker of overall mast cell burden, is often elevated in more widespread cases.
Dr stewart
Given the extent of our patient’s cutaneous involvement, are you concerned about systemic involvement? If so, what studies and treatment might be indicated?
Dr Marqueling
Although the bullous presentation is striking, the number and relatively discrete nature of his plaques places him into the category of urticaria pigmentosa, as opposed to the more severe diffuse cutaneous mastocytosis. With the more common forms of childhood mastocytosis, solitary mastocytoma and urticaria pigmentosa, there is rarely systemic involvement. Unlike adult-onset mastocytosis, internal organ involvement is rare but can be severe when present.
Although the patient has had no diarrhea and no evidence of hepatosplenomegaly, a liver ultrasound would be prudent. I also recommend a CBC count to evaluate for bone marrow involvement. Finally, I would obtain a serum tryptase level, which is more likely to be elevated in patients with systemic disease. If lymphadenopathy, hepatosplenomegaly, or ill-appearance are present, evaluation for systemic mastocytosis should include a CBC panel, LFTs, and, potentially, an abdominal ultrasound, a bone scan, and a bone marrow biopsy. A CBC panel, LFTs, and abdominal ultrasound were conducted for this patient and yielded normal results. The authors of a 20-year retrospective study have suggested that the results of a bone marrow biopsy, if normal, were predictive of resolution of pediatric mastocytosis if presenting before the age of 2 and, if abnormal, might predict progression to ongoing systemic mastocytosis.29 A bone
marrow biopsy would not change the treatment of this patient at this time because he currently has no signs of systemic involvement, so I recommend deferring it. Treatment of systemic mastocytosis includes biologics such as interferon-α-2b and tyrosine-kinase inhibitors and should be started at signs of systemic involvement.30
Dr stewart
What do you recommend for our patient’s management now that we have a diagnosis?
Dr Marqueling
In terms of treatment, I recommend starting the histamine receptor blockers cetirizine (an oral histamine 1 receptor antagonist with a long track record of safety in infants) and ranitidine (an oral histamine 2 receptor antagonist, which also protects against gastric hypersecretion because of the increased number of mast cells in the stomach).31 For topical treatment, I recommend topical cromolyn, a mast cell stabilizer, for existing closed lesions to try to prevent formation of urticarial lesions and bullae. I also recommend mupirocin 2% ointment, a topical antibiotic, for open and exposed lesions, and triamcinolone 0.1% ointment, a topical corticosteroid, to decrease skin inflammation. Patients should have ready access to injectable epinephrine because of the increased risk of anaphylaxis; parents should be educated on when and how to use it.
It is common for mastocytosis to involute in childhood, but some cases persist until puberty. We discussed this entity at length with the patient’s parents, and discussed the potential triggers and/or mast cell degranulators that should be avoided, such as physical stimuli (friction, pressure, and scratching lesions), medications (nonsteroidal anti-inflammatory drugs, opiates,
STEWART et al6
FiGure 3A punch biopsy showed an infiltrate filling the upper third of the dermis. The infiltrate was composed of monomorphic spindled and cuboidal cells with small central nuclei and lightly granular amphophilic cytoplasm. A, Hematoxylin and eosin stain (original magnification ×4). B, Hematoxylin and eosin stain (original magnification ×40). C, Mast cell marker CD117 (original magnification ×10). D, Mast cell tryptase (original magnification ×10).
by guest on August 15, 2020www.aappublications.org/newsDownloaded from

codeine, and polymyxin), and foods (citrus, strawberries, tomatoes, spinach, specific cheeses, egg whites, and certain fish).
Dr stewart
Dr Marqueling’s treatment recommendations were initiated, and the patient was discharged from the hospital. How is the patient doing now?
Dr Hilgenberg
At 2 years of age, he is doing well. He had 1 visit to the emergency department at 5 months of age for hematemesis and melena presumed to be caused by Mallory Weiss tears
secondary to gastric hypersecretion. Bleeding resolved with omeprazole, and he is now maintained on ranitidine and cromolyn sodium. His lesions are now primarily hyperpigmented with almost complete resolution of blistering. For the lesions, he receives topical cromolyn daily and topical steroids as needed. He has an epinephrine autoinjector with him at all times but has never needed to use it. Because his laboratory work remains normal, indicating there is no systemic involvement, he has not had a bone marrow biopsy to evaluate for hematologic involvement. He continues to grow and develop normally.
PEDIATRICS Volume 141, number 3, March 2018 7
potential ConFliCt oF interest: The authors have indicated they have no potential conflicts of interest to disclose.
abbreviations
CBC: complete blood cellCNS: central nervous systemCRP: C-reactive proteinEB: epidermolysis bullosaGBS: group B StreptococcusHSV: herpes simplex virusLFT: liver function testPCR: polymerase chain reactionSEM: skin, eyes, and mouthTORCH: toxoplasmosis, other,
rubella, cytomegalovi-rus, or herpes
VariZIG: varicella-zoster immune globulin
VZV: varicella-zoster virus
reFerenCes
1. Del Pizzo J. Focus on diagnosis: congenital infections (TORCH). Pediatr Rev. 2011;32(12):537–542
2. Polin RA; Committee on Fetus and Newborn. Management of neonates with suspected or proven early-onset bacterial sepsis. Pediatrics. 2012;129(5):1006–1015
3. Neu N, Duchon J, Zachariah P. TORCH infections. Clin Perinatol. 2015;42(1):77–103, viii
4. American Academy of Pediatrics. Toxoplasma gondii infections. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book: 2015 Report of the Committee on Infectious Diseases. Elk Grove Village, IL: American Academy of Pediatrics; 2015:787–796
5. Bowen V, Su J, Torrone E, Kidd S, Weinstock H. Increase in incidence of congenital syphilis - United States, 2012-2014. MMWR Morb Mortal Wkly Rep. 2015;64(44):1241–1245
6. Lanzieri T, Redd S, Abernathy E, Icenogle J; Centers for Disease Control and Prevention. Congenital Rubella Syndrome. In: Manual for the Surveillance of Vaccine-Preventable Diseases. Available at: https:// www. cdc. gov/ vaccines/ pubs/ surv- manual/ chpt15- crs. html. Accessed January 3, 2017
7. American Academy of Pediatrics. Cytomegalovirus. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book: 2015 Report of the Committee of Infectious Diseases. Elk Grove Village, IL: American Academy of Pediatrics; 2015:317–322
8. Kimberlin DW. Neonatal herpes simplex infection. Clin Microbiol Rev. 2004;17(1):1–13
9. American Academy of Pediatrics. Herpes simplex. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book: 2015 Report of the Committee on Infectious Diseases. Elk Grove Village, IL: American Academy of Pediatrics; 2015:432–445
10. Lopez A, Leung J, Schmid S, Marin M; Centers for Disease Control and Prevention. Varicella. In: Manual for the Surveillance of Vaccine-Preventable Diseases. Available at: https:// www. cdc. gov/ vaccines/ pubs/ surv- manual/ chpt17- varicella. html. Accessed January 3, 2017
11. Verani JR, McGee L, Schrag SJ; Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC). Prevention of perinatal group B streptococcal disease--revised
guidelines from CDC, 2010. MMWR Recomm Rep. 2010;59(RR-10):1–36
12. Hussain S, Venepally M, Treat JR. Vesicles and pustules in the neonate. Semin Perinatol. 2013;37(1):8–15
13. Wilson CB, Nizet V, Maldonado YA, Remington JS, Klein JO. Remington and Klein’s Infectious Diseases of the Fetus and Newborn Infant. 8th ed. Philadelphia, PA: Saunders; 2016
14. Baldwin S, Whitley RJ. Intrauterine herpes simplex virus infection. Teratology. 1989;39(1):1–10
15. Kimberlin D, Lin C, Jacobs RF, et al. Natural history of neonatal herpes simplex virus infections in the acyclovir era. Pediatrics. 2001;108(2):223–229
16. Corey L, Wald A. Maternal and neonatal herpes simplex virus infections. N Eng J Med. 2009;361(14):1376–1385
17. Curfman AL, Glissmeyer EW, Ahmad FA, et al. Initial presentation of neonatal herpes simplex virus infection. J Pediatr. 2016;172:121–126.e1
18. Friedlander S, Bradley J. Viral Infections. In: Eichenfield L, Frieden I, Esterly N, eds. Neonatal Dermatology, 2nd ed. Philadelphia, PA: Saunders; 2008:193–212
by guest on August 15, 2020www.aappublications.org/newsDownloaded from

19. Feldman S, Chaudary S, Ossi M, Epp E. A viremic phase for herpes zoster in children with cancer. J Pediatr. 1977;91(4):597–600
20. Enders G, Miller E, Cradock-Watson J, Bolley I, Ridehalgh M. Consequences of varicella and herpes zoster in pregnancy: prospective study of 1739 cases. Lancet. 1994;343(8912):1548–1551
21. American Academy of Pediatrics. Varicella-zoster virus infections. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book: 2015 Report of the Committee of Infectious Diseases. Elk Grove Village, IL: American Academy of Pediatrics; 2015:846–860
22. Hruza LL, Mallory SB, Fitzgibbons J, Mallory GB Jr. Linear IgA bullous dermatosis in a neonate. Pediatr Dermatol. 1993;10(2):171–176
23. Howard R, Frieden I. Vesicles, Pustules, Bullae, Erosions and Ulcerations.
In: Eichenfield L, Frieden I, Esterly N, eds. Neonatal Dermatology, 2nd ed. Philadelphia, PA: Saunders; 2008:131–158
24. Bruckner A. Epidermolysis Bullosa. In: Eichenfield L, Frieden I, Esterly N, eds. Neonatal Dermatology, 2nd ed. Philadelphia, PA: Saunders; 2008:159–172
25. Hollmann TJ, Brenn T, Hornick JL. CD25 expression on cutaneous mast cells from adult patients presenting with urticaria pigmentosa is predictive of systemic mastocytosis. Am J Surg Pathol. 2008;32(1): 139–145
26. Brockow K. Epidemiology, prognosis, and risk factors in mastocytosis. Immunol Allergy Clin North Am. 2014;34(2):283–295
27. Lazar A, Murphy G. The Skin. In: Kumar V, Abbas A, Aster J, Fausto N, eds. Robbins & Cotran Pathologic Basis
of Disease, 8th ed. Philadelphia, PA: Saunders; 2009:2293–2296
28. Tharp M. Mastocytosis. In: Bolognia J, Jorizzo J, Schaffer J, eds. Dermatology, 3rd ed. Amsterdam, Netherlands: Elsevier Limited; 2012:1993–2002
29. Uzzaman A, Maric I, Noel P, Kettelhut BV, Metcalfe DD, Carter MC. Pediatric-onset mastocytosis: a long term clinical follow-up and correlation with bone marrow histopathology. Pediatr Blood Cancer. 2009;53(4):629–634
30. Heide R, Beishuizen A, De Groot H, et al; Dutch National Mastocytosis Work Group. Mastocytosis in children: a protocol for management. Pediatr Dermatol. 2008;25(4):493–500
31. Simons FE, Silas P, Portnoy JM, et al. Safety of cetirizine in infants 6 to 11 months of age: a randomized, double-blind, placebo-controlled study. J Allergy Clin Immunol. 2003;111(6):1244–1248
STEWART et al8 by guest on August 15, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2017-0236 originally published online February 6, 2018; 2018;141;Pediatrics
Marqueling, Kerri E. Rieger and Sarah L. HilgenbergSarah E. Stewart, Jody L. Lin, Jennifer L. Everhart, Trung H. Pham, Ann L.
Well-Appearing Newborn With a Vesiculobullous Rash at Birth
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/141/3/e20170236including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/141/3/e20170236#BIBLThis article cites 19 articles, 4 of which you can access for free at:
Subspecialty Collections
bhttp://www.aappublications.org/cgi/collection/infectious_diseases_suInfectious Diseasehttp://www.aappublications.org/cgi/collection/dermatology_subDermatologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on August 15, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2017-0236 originally published online February 6, 2018; 2018;141;Pediatrics
Marqueling, Kerri E. Rieger and Sarah L. HilgenbergSarah E. Stewart, Jody L. Lin, Jennifer L. Everhart, Trung H. Pham, Ann L.
Well-Appearing Newborn With a Vesiculobullous Rash at Birth
http://pediatrics.aappublications.org/content/141/3/e20170236located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2018has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on August 15, 2020www.aappublications.org/newsDownloaded from