Embed Size (px)
Citation preview
West Virginia-ACC
Poster Competition
Abstracts
April 8, 2017
CV Team Research
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Nursing Knowledge of Heart Failure
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Background: Heart failure is a constellation of signs and symptoms reflecting a physiologic change in the heartsability to keep up with demand. Heart failure is considered a global pandemic and is a complex disease thatoftentimes is progressive. Heart failure is often associated with underlying coronary atherosclerosis, and itsassociated risks, including hypertension, diabetes mellitus, metabolic syndrome and dyslipidemia. To slow theprogression and improve quality of life patients should be educated about the disease and in most health caresettings nurses provide this education. However, nurses may lack sufficient knowledge of the processes that lead toheart failure.Objective: The purpose of this study was to determine the level of understanding nurses possess regarding heartfailure, and whether additional evidence-based education regarding heart failure, sufficiently improves the nurses’knowledge of heart failure.Methods: A pre/posttest design using a convenience sample of nurses at Marshall Health was used in this study.All nurses at Marshall Health cardiology and internal medicine were included without exclusion of hours worked ornursing degree. By using Rogers Diffusion of Innovations theory, nurses received heart failure education consistingof a video approximately 60 minutes long created by Qualidigm. Participants took a pretest just prior to theeducation video and one month later a posttest.Results: The results showed that heart failure knowledge did increase from pre to posttest, however it was notsignificant (p= 0.2).
West Virginia-ACC Poster Competition Abstract
Authors:
Beth Ann White DNP, Marilyn E. Smith PhD, Mark Studeny MD, and Teresa Ritchie DNP
C
Author to Receive Correspondence - Contact Information
Full Name: White Beth ALast First M.I.
Address: 4302 Staunton AveStreet Address Apartment/Unit
#Charleston WV 25304
City State ZIP CodeWork Phone: 304-638-2911 Alternate Phone: 304-638-2911
E-mail Address: [email protected]
TrainingProgram: WVU
__X_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.

FIT Research
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Battery longevity from cardiac resynchronization therapy defibrillators: differences between manufacturers anddiscrepancies with published product performance reports.
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Objective:
Cardiac resynchronization therapy (CRT) is an important treatment for heart failure that requires constant ventricular pacing,placing a high-energy burden on CRT defibrillators (CRT-D). Longer battery life reduces the need for device changes andassociated complications, thereby affecting patient outcomes and cost of care. We therefore investigated the time to batterydepletion of CRT-D from different manufacturers and compared these results with manufacturers' published productperformance reports (PPRs).
METHODS AND RESULTS:
All CRT-D recipients at our institution between January 2008 and December 2010 were included in this study cohort. Thepatients were followed up to the endpoint of battery depletion and were otherwise censored at the time of death, last follow-up,or device removal for any reason other than battery depletion. A total of 621 patients [173 Boston Scientific (BSC), 391Medtronic (MDT), and 57 St. Jude Medical (SJM)] were followed up for a median of 3.7 (IQR 1.6-5.0) years, during which time253 (41%) devices were replaced for battery depletion. Compared with MDT devices, battery depletion was 85 and 54% lesslikely to happen with BSC and SJM devices, respectively (P < 0.001 for pairwise comparisons). Product performance reportsfrom all manufacturers significantly overestimated battery longevity by more than 20% 6 years after device implantation.
CONCLUSIONS:
Large differences in CRT-D battery longevity exist between manufacturers. Industry-published PPRs significantly overestimatedevice longevity. These data have important implications to patients, healthcare professionals, hospitals, and third-partypayers.
West Virginia-ACC Poster Competition Abstract
Authors:
Mian Bilal Alam, MD. PGY IV Cardiology Fellow – Marshall University, Joan Edwards school of medicine. Huntington. WVSamir Saba, MD. Associate Professor of Medicine, Chief of Cardiac Electrophysiology, University of Pittsburgh Medical Centre. Pittsburgh,PA.
C
Author to Receive Correspondence - Contact Information
Full Name: ALAM MIAN BILALLast First M.I.
Address: 30 PERSIMMON LNStreet Address Apartment/Unit
#HUNTINGTON WV 25701
City State ZIP CodeWork Phone: Alternate Phone: 720 975 3364
E-mail Address: [email protected]
TrainingProgram: PGY IV – CARDIOLOGY, Marshall University – Huntington WV.
I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC Annual Meeting.I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Outcomes of Transcatheter and Surgical Aortic Valve Replacement in Patients on Maintenance Dialysis: Insight from TheNationwide Inpatient Sample
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Background: Surgical aortic valve replacement (SAVR) for aortic stenosis in dialysis patients has been associated withsignificant mortality. The introduction of transcatheter aortic valve replacement (TAVR) expanded definitive therapy of aorticstenosis to many high-risk patients, but it has not been fully evaluated in the dialysis population.
Objective: We aim to perform a comparative analysis of SAVR and TAVR in dialysis patients using a contemporary nationwidedatabase. Design, Setting, and Participants: This study analyzed all patients receiving maintenance dialysis with severe aorticstenosis who underwent SAVR or TAVR in a nationwide inpatient database from January 1, 2005, through December 31,2014.
Methods: The trends of transcatheter and surgical aortic valve replacement in patients on dialysis during the 10-year studyperiod were assessed. In-hospital mortality, rates of major adverse events, hospital length of stay, cost of care andintermediate care facility utilization were compared between dialysis patients who underwent SAVR and those who underwentTAVR using both unadjusted and propensity-matched data.
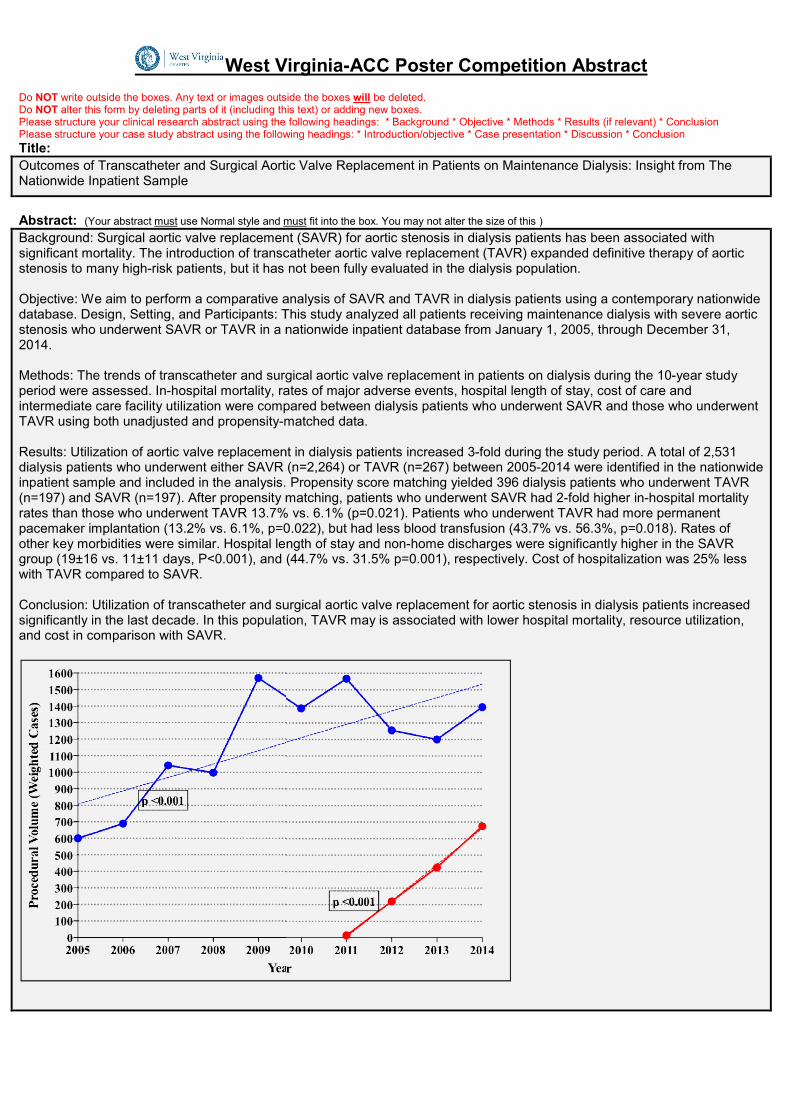
Results: Utilization of aortic valve replacement in dialysis patients increased 3-fold during the study period. A total of 2,531dialysis patients who underwent either SAVR (n=2,264) or TAVR (n=267) between 2005-2014 were identified in the nationwideinpatient sample and included in the analysis. Propensity score matching yielded 396 dialysis patients who underwent TAVR(n=197) and SAVR (n=197). After propensity matching, patients who underwent SAVR had 2-fold higher in-hospital mortalityrates than those who underwent TAVR 13.7% vs. 6.1% (p=0.021). Patients who underwent TAVR had more permanentpacemaker implantation (13.2% vs. 6.1%, p=0.022), but had less blood transfusion (43.7% vs. 56.3%, p=0.018). Rates ofother key morbidities were similar. Hospital length of stay and non-home discharges were significantly higher in the SAVRgroup (19±16 vs. 11±11 days, P<0.001), and (44.7% vs. 31.5% p=0.001), respectively. Cost of hospitalization was 25% lesswith TAVR compared to SAVR.
Conclusion: Utilization of transcatheter and surgical aortic valve replacement for aortic stenosis in dialysis patients increasedsignificantly in the last decade. In this population, TAVR may is associated with lower hospital mortality, resource utilization,and cost in comparison with SAVR.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Outcomes of Transcatheter and Surgical Aortic Valve Replacement in Patients on Maintenance Dialysis: Insight from TheNationwide Inpatient Sample
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Background: Surgical aortic valve replacement (SAVR) for aortic stenosis in dialysis patients has been associated withsignificant mortality. The introduction of transcatheter aortic valve replacement (TAVR) expanded definitive therapy of aorticstenosis to many high-risk patients, but it has not been fully evaluated in the dialysis population.
Objective: We aim to perform a comparative analysis of SAVR and TAVR in dialysis patients using a contemporary nationwidedatabase. Design, Setting, and Participants: This study analyzed all patients receiving maintenance dialysis with severe aorticstenosis who underwent SAVR or TAVR in a nationwide inpatient database from January 1, 2005, through December 31,2014.
Methods: The trends of transcatheter and surgical aortic valve replacement in patients on dialysis during the 10-year studyperiod were assessed. In-hospital mortality, rates of major adverse events, hospital length of stay, cost of care andintermediate care facility utilization were compared between dialysis patients who underwent SAVR and those who underwentTAVR using both unadjusted and propensity-matched data.
Results: Utilization of aortic valve replacement in dialysis patients increased 3-fold during the study period. A total of 2,531dialysis patients who underwent either SAVR (n=2,264) or TAVR (n=267) between 2005-2014 were identified in the nationwideinpatient sample and included in the analysis. Propensity score matching yielded 396 dialysis patients who underwent TAVR(n=197) and SAVR (n=197). After propensity matching, patients who underwent SAVR had 2-fold higher in-hospital mortalityrates than those who underwent TAVR 13.7% vs. 6.1% (p=0.021). Patients who underwent TAVR had more permanentpacemaker implantation (13.2% vs. 6.1%, p=0.022), but had less blood transfusion (43.7% vs. 56.3%, p=0.018). Rates ofother key morbidities were similar. Hospital length of stay and non-home discharges were significantly higher in the SAVRgroup (19±16 vs. 11±11 days, P<0.001), and (44.7% vs. 31.5% p=0.001), respectively. Cost of hospitalization was 25% lesswith TAVR compared to SAVR.
Conclusion: Utilization of transcatheter and surgical aortic valve replacement for aortic stenosis in dialysis patients increasedsignificantly in the last decade. In this population, TAVR may is associated with lower hospital mortality, resource utilization,and cost in comparison with SAVR.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Outcomes of Transcatheter and Surgical Aortic Valve Replacement in Patients on Maintenance Dialysis: Insight from TheNationwide Inpatient Sample
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Background: Surgical aortic valve replacement (SAVR) for aortic stenosis in dialysis patients has been associated withsignificant mortality. The introduction of transcatheter aortic valve replacement (TAVR) expanded definitive therapy of aorticstenosis to many high-risk patients, but it has not been fully evaluated in the dialysis population.
Objective: We aim to perform a comparative analysis of SAVR and TAVR in dialysis patients using a contemporary nationwidedatabase. Design, Setting, and Participants: This study analyzed all patients receiving maintenance dialysis with severe aorticstenosis who underwent SAVR or TAVR in a nationwide inpatient database from January 1, 2005, through December 31,2014.
Methods: The trends of transcatheter and surgical aortic valve replacement in patients on dialysis during the 10-year studyperiod were assessed. In-hospital mortality, rates of major adverse events, hospital length of stay, cost of care andintermediate care facility utilization were compared between dialysis patients who underwent SAVR and those who underwentTAVR using both unadjusted and propensity-matched data.
Results: Utilization of aortic valve replacement in dialysis patients increased 3-fold during the study period. A total of 2,531dialysis patients who underwent either SAVR (n=2,264) or TAVR (n=267) between 2005-2014 were identified in the nationwideinpatient sample and included in the analysis. Propensity score matching yielded 396 dialysis patients who underwent TAVR(n=197) and SAVR (n=197). After propensity matching, patients who underwent SAVR had 2-fold higher in-hospital mortalityrates than those who underwent TAVR 13.7% vs. 6.1% (p=0.021). Patients who underwent TAVR had more permanentpacemaker implantation (13.2% vs. 6.1%, p=0.022), but had less blood transfusion (43.7% vs. 56.3%, p=0.018). Rates ofother key morbidities were similar. Hospital length of stay and non-home discharges were significantly higher in the SAVRgroup (19±16 vs. 11±11 days, P<0.001), and (44.7% vs. 31.5% p=0.001), respectively. Cost of hospitalization was 25% lesswith TAVR compared to SAVR.
Conclusion: Utilization of transcatheter and surgical aortic valve replacement for aortic stenosis in dialysis patients increasedsignificantly in the last decade. In this population, TAVR may is associated with lower hospital mortality, resource utilization,and cost in comparison with SAVR.
West Virginia-ACC Poster Competition Abstract
Authors:
Fahad Alqahtani MD, Sami Aljohani MD, Khaled Boobes MD, Elad Maor MD, PhD, Assem Sherieh MD, Charanjit S Rihal MD,David R Holmes MD, Mohamad Alkhouli MD
C
Author to Receive Correspondence - Contact Information
Full Name: Alqahtani Fahad SLast First M.I.
Address: 1 medical center drive 3ed floorStreet Address Apartment/Unit
#Morgantwon WV 26501
City State ZIP CodeWork Phone: 304-598-4000 Alternate Phone: 202-2860814
E-mail Address: [email protected]
TrainingProgram: WVU cardiovascular fellowship program-Morgantown
___I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Utilization of radionuclide myocardial perfusion imaging for the evaluation of chest pain in a population of the state of WestVirginia: assessment with the ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 Multimodality AppropriateUse Criteria for the Detection and Risk Assessment of Stable Ischemic Heart Disease
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction, Objective and Design:Radionuclide myocardial perfusion imaging (RMPI) is ubiquitous in diagnosing coronary artery disease (CAD), hence cost-effective use is extremely important. Appropriate Use Criteria (AUC) for Cardiac Radionuclide Imaging (CRI) were firstdeveloped on 2009 and later revised on 2013 to classify their appropriateness of use based on a pre-test risk assessment forcoronary heart disease (CHD) risk in asymptomatic individuals and on the pre-test probability of CAD in symptomatic patients.Multiple studies have evidenced that there exists heterogeneity of AUC patterns and outcomes depending on thecharacteristics of the scenario where the CRI is used.We sought to evaluate physicians’ use of CRI according to the updated AUC in order to determine utilization patterns ofmyocardial perfusion imaging for the evaluation of non-acute chest pain/angina equivalent in a outpatient cohort of patients inHuntington, WV. We expected to prove that percentage of appropriate RMPIs in our sample population approximates thenational average.This was a retrospective study including RMPIs performed at Erma Ora Byrd Clinical Center (BCC) for the evaluation of non-acute chest pain on 1/1/2014 - 3/31/2014. BCC is located in Huntington, WV. Outpatient RMPIs for Marshall Universityclinicians and private practitioners are performed there. We reviewed 167 RMPIs. Pertinent data were collected. Pretestprobability of CAD was calculated for each individual that was then used to determine study appropriateness.
Results and Discussion:Patients’ age was 61±13 years, 53 % were women. Forty-five percent had ASCVD, 71% HTN, 31% DM, 52% HLP and 22%tobacco use. Regadenoson was the stressor in 67.7%, the rest used treadmill exercise. Sixty-six percent were cardiologist-ordered. Rates of Appropriate, May-be-appropriate, Rarely-appropriate and unclassified studies were 91 %, 0 %, 5.4% and3.6%, respectively. Appropriateness rate compared with literature reviewed. Female young patients with low pre-testprobability of CAD were more likely to have Rarely appropriate than Appropriate studies (87.5% vs. 49%, p=0.034; age44.5±7.5 vs. 62.2±12.6, p=0.0001; respectively) coinciding with literature reviewed. Cardiologist-ordered studies were notmore likely Rarely appropriate than non-cardiologist-ordered (5.4% vs 3.65%, p=0.60306) contrasting with literature reviewed.Academical-ordered studies were not more likely Rarely appropriate than those from private counterparts (5.2% vs. 0%,p=0.42) coinciding with literature reviewed.
Conclusions and Relevance:Appropriateness rate in our study compares to the national/international average. Most Rarely appropriate studies wereobserved in younger, female patients with low probability of CAD which highlights an area of improvement when selectingappropriate diagnostic tools in this particular population. Physician’s specialty/academical status did not influenceappropriateness in our study. Additional research is needed in the general population since our patients come from anoutpatient setting which limits sample representativeness.
West Virginia-ACC Poster Competition Abstract
Authors:Eric Arguelles, MD; Warren Doyle, MD; Charles E. Meadows III, MD; Ellen A. Thompson, MD; Paulette S. Wehner, MD.Department of Cardiology, Joan C Edwards School of Medicine, Marshall University, Huntington, WV.
C
Author to Receive Correspondence - Contact Information
Full Name: Arguelles Eric N/ALast First M.I.
Address: 6213 Country Club Dr.Street Address Apartment/Unit
#Huntington WV 25705
City State ZIP CodeWork Phone: 7862736269 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: Marshall University Adult Cardiovascular Diseases.
_X__I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.

West Virginia-ACC Poster Competition AbstractPlease structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
Elevated Plasma Marinobufagenin, An Endogenous Cardiotonic Steroid, Is Associated With
Right Ventricular Dysfunction and Nitrative Stress in Heart Failure
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Background—Plasma levels of cardiotonic steroids are elevated in volume-expanded states, such aschronic kidney disease, but the role of these natriuretic hormones in subjects with heart failure (HF) isunclear. We sought to determine the prognostic role of the cardiotonic steroids marinobufagenin (MBG) inHF, particularly in relation to long-term outcomes.
Methods and Results—We first measured plasma MBG levels and performed comprehensive clinical,laboratory, and echocardiographic assessment in 245 patients with HF. All-cause mortality, cardiactransplantation, and HF hospitalization were tracked for 5 years. In our study cohort, median (interquartilerange) MBG was 583 (383–812) pM. Higher MBG was associated with higher myeloperoxidase (r=0.42,P<0.0001), B-type natriuretic peptide (r=0.25, P=0.001), and asymmetrical dimethylarginine (r=0.32,P<0.001). Elevated levels of MBG were associated with measures of worse right ventricular function (RVs′, r=−0.39, P<0.0001) and predicted increased risk of adverse clinical outcomes (MBG≥574 pmol/L:hazard ratio 1.58 [1.10–2.31], P=0.014) even after adjustment for age, sex, diabetes mellitus, and ischemicpathogenesis.
Conclusions—In the setting of HF, elevated plasma levels of MBG are associated with right ventriculardysfunction and predict worse long-term clinical outcomes in multivariable models adjusting forestablished clinical and biochemical risk factors. Infusion of MBG seems to directly contribute to increasednitrative stress and cardiac fibrosis.
West Virginia-ACC Poster Competition Abstract
Authors:
David J. Kennedy, PhD; Kevin Shrestha, MD; Brendan Sheehey, BS; Xinmin S. Li,PhD; Anuradha Guggilam, DVM, PhD; Yuping Wu, PhD; Michael Finucan, BS; AlaaGabi, MD; Charles M. Medert, BS; Kristen Westfall, MBA; Allen Borowski, RDCS;Olga Fedorova, PhD; Alexei Y. Bagrov, MD, PhD; W.H. Wilson Tang, MD
C
Author to Receive Correspondence - Contact Information
Full Name: Gabi AlaaLast First M.I.
Address: 1249 15TH StreetStreet Address Apartment/Unit
#Huntington WV 25701
City State ZIP CodeWork Phone: 3046381755 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: Marshall University
AG I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Racial Disparity in Aortic Valve Replacement Outcomes: Insight from National Inpatient Sample
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Racial disparity in Aortic Valve Replacement Outcomes:Insight from National Inpatient Sample
INTRODUCTIONS:Racial disparities exist in the management of many cardiovascular diseases including Aortic Valve Replacement (AVR). The incidence ofaortic valve stenosis is less common in African Americans (AA) (1), and AA undergo AVR less frequently than EA (2). The Society ofThoracic Surgeons’ risk (STS) score identifies the AA and Hispanic races as an independent risk factor for perioperative morbidity but notmortality in patients undergoing isolated AVR. We aim to investigate the effect of race on mortality and morbidity of AVR in a largecontemporary nationwide database.
METHODS: The 2004-2013 Nationwide Inpatient Sample was utilized to identify 108,673 patients who underwent isolated AVR usingICD-9 Codes. In-hospital outcomes of AA patients (n=5,921) and of Hispanics patients (n=6922) in comparison to propensity matchedcohorts of the Caucasian patient’s population (n=95.830). Propensity matched score analysis yielded a total of two pairs of matchinggroups (5806 patients in each of the two groups comparing EA and AAs; and 6897 patients in each of the two groups comparing the EAand the Hispanics).
RESULTS: In-hospital mortality was significantly higher in AA undergoing AVR compared with Caucasian patients (6.1% vs. 4.7%, OR1.21, CI 1.02-1.44, p=0.03). Key perioperative complications were not significantly different between the two groups (Figure 1). There wasno significant difference in in-hospital mortality between Hispanic patients in comparison with Caucasian patients undergoing AVR (4.5%vs. 4.1%, OR=1.04, CI=0.795-1.145, p=0.614).
DISCUSSION: The main finding in our study: African American race is an independent predictor of in-hospital mortality after isolatedAVR. Prior studies had concluded that race was not a significant predictor of operative mortality after isolated AVR or MVR (3,4). Inaddition, the current STS score calculator does not identify the AA race as an independent risk factor for perioperative mortality in patientsundergoing isolated AVR. This study is subject to the inherent limitations and biases of retrospective non-randomized studies. We believethat our study provides important insight and can serve as a seed to larger confirmatory studies.
CONCLUSION: In a large contemporary nationwide sample of patients undergoing AVR, African American but not Hispanic race was anindependent predictor of in-hospital mortality. These findings have important implications for preoperative risk stratification of AfricanAmerican and Hispanic patients being evaluated for aortic valve replacement.REFERENCES:1)Yeung, M; Kerrigan, J et al ;”Racial Differences in Rates of Aortic Valve Replacement in Patients With Severe Aortic Stenosis”; Am JCardiol 2013;112:991e9952) Patel, D; Green, K, et al; “Racial Differences in the Prevalence of Severe Aortic Stenosis”; J Am Heart Assoc. 2014;3:e000879 doi:10.1161/JAHA.114.0008793) Taylor, N; O’Brien, S, et al; “Relationship Between Race and Mortality and Morbidity After Valve Replacement Surgery”; (Circulation.2005;111:1305-1312)4) Stamou, S. C., Robich, M., et al; “Effects of gender and ethnicity on outcomes after aortic valve replacement”; J Thorac Cardiovasc Surg2012;144:486-92
West Virginia-ACC Poster Competition Abstract
Authors:
Ali Hama Amin, Vinay Badhwar, Fahad Alqahtani, Sami Aljohani, Zakieh Chaker, Ahmad Almustafa, Akram Kawsara, MohamadAlkhouli
C
Author to Receive Correspondence - Contact Information
Full Name: Hama Amin AliLast First M.I.
Address: 1 Medical Centre Dr.Street Address Apartment/Unit
#Morgantown WV 26508
City State ZIP CodeWork Phone: 3045984000 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: WVU Heart & Vascular Institute
__x_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.

West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Detectable subclinical myocardial necrosis is associated with cardiovascular risk in stable patientswith diabetes.
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
BACKGROUND:Detection of systemic levels of cardiac troponin is associated with the presence of ongoingmyocardial necrosis and fulfills the contemporary definition of myocardial infarction (MI) in thepresence of ischemic symptoms. However, a minimal increase in cardiac troponin levels belowthe diagnostic range often provides clinical challenges, particularly in stable ambulatory patientswithout overt signs and symptoms suggestive of underlying ischemia and normal renal function.As biochemical assays become more and more sensitive, the ability to detect minimal myocardialdamage may allow risk assessment in stable cardiac patients beyond the acute setting.OBJECTIVE:To investigate the relationship between different degrees of subclinical myocardial necrosis,glycemic control, and long-term adverse clinical outcomes within a stable patient population withdiabetes mellitus.METHODS:We examined 1,275 stable patients with diabetes mellitus undergoing elective diagnosticcoronary angiography with cardiac troponin I (cTnI) levels below the diagnostic cut-off for definingmyocardial infarction (MI) (<0.03 ng/mL). The relationship of subclinical myocardial necrosis(cTnI 0.009-0.029 ng/mL) with incident major adverse cardiovascular events (MACE; defined asany death, MI, or stroke) over 3 years of follow-up was examined.RESULTS:Subclinical myocardial necrosis was observed in 22% of patients. A strong association wasobserved between the magnitude of subclinical myocardial necrosis and risk of 3-year incidentMACE (hazard ratio, 1.98; 95% confidence interval, 1.48-2.65; P < 0.001) and remainedstatistically significant even after adjustment for traditional risk factors, high-sensitivity C-reactiveprotein, and creatinine clearance. Only a weak correlation was observed between the presenceof subclinical myocardial necrosis and either glycemic control (r = 0.06; P = 0.044 for hemoglobinA1c versus cTnI) or insulin resistance (r = 0.04; P = 0.094 for glucose-to-insulin ratio versuscTnI).CONCLUSIONS:The presence of detectable subclinical myocardial necrosis in stable patients with diabetesmellitus is associated with heightened long-term risk for MACE, independent of traditional risk factors and
glycemic control.
West Virginia-ACC Poster Competition AbstractAuthors:
Naveed Iqbal MD1, W. H .Wilson Tang MD2 ,Yuping Wu PhD3, Stanley L. Hazen MD PhD2.1 Department of Cardiovascular Medicine, Marshall University School of Medicine; and 2 Department of CellBiology, Lerner Research Institute, Cleveland Clinic; and 3 Department of Mathematics, Cleveland State University,Cleveland,Ohio.
C
Author to Receive Correspondence - Contact Information
Full Name: Iqbal Naveed SLast First M.I.
Address: 223 Riverview DriveStreet Address Apartment/Unit
#Barboursville WV 25504
City State ZIP CodeWork Phone: 312-339-0015 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: Marshall University School of Medicine
__X_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition Abstract Do NOT write outside the boxes. Any text or images outside the boxes will be deleted. Do NOT alter this form by deleting parts of it (including this text) or adding new boxes. Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * Conclusion Please structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * Conclusion
Title:
Outcomes of Transcatheter and Surgical Aortic Valve Replacement in Patients with Hepatic Cirrhosis: Insight from Nationwide Inpatient Sample
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
BACKGROUND: Patients with hepatic cirrhosis undergoing surgical aortic valve replacement (SAVR) have higher perioperative morbidity and mortality compared to non-cirrhotics. Whether transcather aortic vavle replacement (TAVR) provides a safer alternative treatment in this high-risk group is unknown. We aim to utilize a nationwide database to assess outcomes of TAVR vs. SAVR in patients with hepatic cirrhosis. METHODS: Using the Nationwide Inpatient Sample and ICD-9 codes, we identified patients with the diagnosis of hepatic cirrhosis (ICD-9 Codes: 571.2, 571.5) who underwent aortic valve replacement between 2004-2013. In-hospital outcomes were compared between two propensity matched cohorts of patients who underwent TAVR vs. SAVR. RESULTS: 909 patients with cirrhosis who underwent aortic valve replacement (8.4% TAVR, 91.6% SAVR). Propensity matching yielded 102 Patients (n=51 TAVR, n=51 SAVR). There was no significant difference in in-hospital mortality between the two groups. With the exception of blood transfusion, there was no also difference in perioperative complications, lengths of stay and hospital charges. CONCLUSION: In a contemporary nationwide sample, there was no significant difference in mortality and key comorbidities between TAVR and SAVR in patients with hepatic cirrhosis. However, this comparison is limited by the small sample size and the inclusion of early TAVR experience. Larger scale studies are needed for comparative effectiveness analysis of TAVR vs. SAVR in this patients with hepatic cirrhosis. KEYWORDS: Transcathter aortic valve replacement • surgical aortic valve replacement • cirrhosis • outcomes • national trend.
West Virginia-ACC Poster Competition Abstract Authors:
Mohammad Kawsara, MD. Ahmad Almustafa, MD. Fahad Alqahtani, MD. Sami Aljuhaini, MD. Ali Amin, MD. Mohamad Alkhouli, MD.
C
Author to Receive Correspondence - Contact Information
Full Name: KAWSARA MOHAMMAD AKRAM
Last First M.I.
Address: 1 Medical Center Dr
Street Address Apartment/Unit #
Morgantown WV 26506
City State ZIP Code
Work Phone: 304-993-5880 Alternate Phone:
E-mail Address: [email protected]
Training Program: WVU Heart and Vascular Institute
_yes__I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC Annual Meeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Functional Status Improvement in TAVR Patients by Lung Disease Severity
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Over the past decade transcatheter aortic valve replacement (TAVR) has emerged as an alternative to surgical replacement(SAVR) initially in high risk surgical patients. As devices and techniques improve and procedure experience grows, TAVR isnow a viable option for intermediate risk surgical patients and studies are now investigating low surgical risk patients. One ofthe most common co-morbidities deeming patients intermediate to high risk surgical candidates chronic lung disease (CLD).TAVR has been shown to decrease mortality in these patients, but patient functional status has not been evaluated based onlung disease severity. In our TAVR program at Marshall University, patient functional status was evaluated using the 5-meterwalk test (5MWT) and the Kansas City Cardiomyopathy Questionnaire (KCCQ-12) at baseline, 30 days and 1 year follow up.All patients were included in this study. This study aims to delineate the quality of life improvement based on lung diseaseseverity in patients undergoing TAVR at 30 days and 1 year. To date 73 patients had undergone TAVR procedure at ourinstitution. There were no differences in age, sex or New York Heart Association class between patients by severity of CLD.In regards to patient KCCQ scores, there were no statistical differences in improvement at 30 days (n=61) or 1 year (n=40).Interestingly, however, patients without CLD reported the lowest improvement based on their scores. The 5MWT times alsoshowed no statistical difference between CLD severity in our population at 30 days (n=22) or 1 year (n=14). We did note thatour no CLD patients actually had a worsening of their 5MWT time at 30 days and a <1% improvement at 1 year compared topatients with any degree of CLD which increased by > 20% at 30 days and > 15% at 1 year. Our results indicate that chroniclung disease severity likely has no significant effect on functional status outcomes following transcatheter aortic valvereplacement. This is promising to report as more and more patients will be eligible for transcatheter based approaches foraortic valve replacement in the future.
West Virginia-ACC Poster Competition Abstract
Authors:
Rick Schnatz DO, Elise Anderson DO, Mark Studeny MD, Daniel Snavely MD
C
Author to Receive Correspondence - Contact Information
Full Name: Schnatz Rick GLast First M.I.
Address: 125 Willowood CircleStreet Address Apartment/Unit
#Hurricane WV 25526
City State ZIP CodeWork Phone: 304-691-8500 Alternate Phone: 301-580-1935
E-mail Address: [email protected]
TrainingProgram: Marshall University Cardiology
__X_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
FIT Cases
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Late Manifestation of Eisenmenger Physiology After Atrial Septal Defect Closure
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction:We are presenting a complex of middle age woman with a late development of Eisenmenger physiology after percutaneousASD closure.Case presentation:55 year-old woman presented to cardiology clinic with dyspnea on exertion for 2 weeks. She has a history of diabetes II,hypertension and breast cancer treated with radiation and lumpectomy two years prior. She was afebrile, BP 120/82, HR 120,O2 sat 78% on room air. Lungs were clear to auscultation; no clubbing or cyanosis.Transthoracic echocardiogram showed preserved left ventricular systolic function, but a large right ventricle (RV), mild-moderately reduced RV function and a large right-to-left interatrial shunt. Subsequent outpatient transesophagealechocardiogram demonstrated a large secundum atrial septal defect (ASD) with an absent aortic rim, and a diameter of 1.2cm.Patient was admitted for acutely worsening dyspnea and hypoxia. Right heart catheterization with direct left atrial pressuremeasurement was performed and revealed a cardiac output of 3.2 liters/minute, mean right atrial pressure of 13mmHg, meanpulmonary arterial pressure (mPAP) of 40 mm Hg, pulmonary vascular resistance (PVR) of 14 wood unit and systemicvascular resistance (SVR) of 20 wood unit. Balloon occlusion test was performed to verify the patient’s tolerability of potentialASD closure. An 18mm Amplatzer sizing balloon was used to occlude the defect. Left atrial and pulmonary artery pressureswere measured simultaneously, and both remained unchanged during balloon occlusion of the defect for 20 minutes. At thesame time O2 saturation rose from 78% to 94% on room air. The defect was therefore closed with a 30mm Gore Cardioformseptal occluder device. The patient was discharged on post procedural day 2 without complications and with no O2requirements.36 hours after discharge, the patient returned to emergency department with two episodes of hypoxemia and seizure both ofwhich occurred shortly after vomiting. Computed tomography of the lungs excluded pulmonary embolism. Repeat cardiaccatheterization demonstrated stable position of the septal occluder device with no residual interatrial shunt. However,hemodynamic assessment revealed a depressed cardiac output at 2.3 liters/minute, mPAP 55mm Hg, PVR 31WU, SVR of 20wood unit and an oxygen saturation of 82% on room air suggesting the interval development of an Eisenmenger physiology.Pulmonary vasoreactivity was tested with continuous inhalation of 100% FiO2 and nitric oxide 20 parts per million (ppm);mPAP improved to 34mm Hg, PVR improved to 7.2WU and cardiac output increased to 3.2 liters/minute. Patient clinicallyimproved and was transitioned off Nitric Oxide to 40 mg of sildenafil TID and 10 mg of macitentan daily.Discussion/Conclusion:Temporary balloon occlusion test results should be interpreted with caution in patients with severe pulmonary hypertension asEisenmenger physiology can develop late after ASD closure despite no acute increase in PAP during balloon occlusion.
West Virginia-ACC Poster Competition Abstract
Authors:
Ali Hama Amin, Ashwin, Bhirud, Kishore Bingi, Sami Aljohani, Naser Moiduddin, Fahad Alqahtani, Mohamad Alkhouli
West Virginia University- Heart and Vascular Institute, Morgantown, WV, USA.
C
Author to Receive Correspondence - Contact Information
Full Name: Bhirud Ashwin RLast First M.I.
Address: 2213 Suncrest VillageStreet Address Apartment/Unit
#Morgantown WV 26505
City State ZIP CodeWork Phone: 7033281621 Alternate Phone: NA
E-mail Address: [email protected]
TrainingProgram: West Virginia University Fellowship in Cardiovascular Disease
_x_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Left ventricular diastolic collapse without hemodynamic compromise in a patient with large,Left pleural effusionAbstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction:Large pleural effusions are typically associated with dyspnea and potential respiratory compromise. With large pleuraleffusions, increased intrapleural pressure may be transmitted to the pericardial space, resulting in impaired cardiacfilling and reduced stroke volume.Cardiac tamponade is due to extrinsic cardiac compression, generally secondary to pericardial effusion. In rare cases,patients with pleural effusion can show similar signs and symptoms due to the transmission of the elevated pleuralpressure to the heart1.Left ventricular diastolic collapse is a rare phenomenon that is occasionally observed in patients with cardiac tamponade.We report a case of isolated left ventricular LV diastolic collapse due to compression by a large left pleural effusionwithout clinical hemodynamic compromise.Case report:56-year-old male presented to our institution with left flank pain, shortness of breath, and chest pain. The patient was nothypotensive, but had resting sinus tachycardia. Laboratory studies were remarkable for leukocytosis of 21,000.EKG showed sinus tachycardia. Chest x-ray showed large left-sided pleural effusion, and left lung infiltrates (figure 1). A2D echocardiogram was obtained and demonstrated a large left pleural effusion causing early to mid diastolic collapse ofthe Left ventricular (LV) posterior and lateral walls consistent with isolated chamber tamponade. (figure 2).LV septalmotion was normal. No Right ventricular, or right atrial collapse was seen. After draining of 1200cc of left pleural fluid,the left ventricular diastolic collapse disappeared (figure 3). Chest X-ray also demonstrated a decrease in the left pleuraleffusion (figure 4). There were no clinical signs of tamponade, and the patient remained hemodynamically stablethroughout hospitalization. The patient was diagnosed with empyema due to health care associated pneumonia.Discussion:The results of this case report would suggest that the pleural effusion was responsible for the echocardiographic findingof left ventricular diastolic collapse. Presence of LV diastolic collapse in patients without clinical evidence of cardiactamponade should alert physicians to look for pleural effusion. Echocardiographic reevaluation after thoracentesisshould precede pericardiocentesis.Isolated diastolic collapse of the right ventricle, and/or right atrium due to large pleural effusion has been reported inmany case reports2-4, but isolated LV diastolic in setting of large pleural effusion is even more rare3.References:1-Vaska K, Wann S, Sagar K, Klopfenstein S. Pleural effusion as a cause of right ventricular diastolic collapse. Circulation.1992;86: 609-172-Venkatesh G, Tomlinson CW, O'Sullivan T, McKelvie RS. Right ventricular diastolic collapse without hemodynamiccompromise in a patient with large, bilateral pleural effusions. J Am Soc Echocardiogr 1995 Jul-Aug;8(4):551-3.
3-Kisanuki A, Shono H, Kiyohnaga K, Kawatake M, Otsuji Y, Minogoe S, Nakao S, Nomoto K, Tanaka H: Two-dimensionalechocardiographic demonstration of left ventricular diastolic collapse due to compression by pleural effusion. Am Heart J1991; 4-1: 1173–1175
4-Wrisley D. Marked diastolic collapse of the right atrium without hemodynamic compromise caused by large pleuraleffusion. J Am Soc Echocardiogr 1994;7:87–8. doi:10.1016/S0894-7317(14)80424-0
LV
RV
West Virginia-ACC Poster Competition Abstract
Authors:
Majd Kanbour MD, Ibrahim Shahoub MD, Nathan Vaughan MD.
C
Author to Receive Correspondence - Contact Information
Full Name: Kanbour MajdLast First M.I.
Address: 1249 15TH Street suite 4000Street Address Apartment/Unit
#
Huntington WV 25701City State ZIP Code
Work Phone: 304-691-8534 Alternate Phone: 304-972-3359
E-mail Address: [email protected]
TrainingProgram: Marshall University
_x__I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Successful Retrieval of Coronary Stent Lodged in Ostial Portion of Existing Left Main Coronary Stent Scaffold
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction: This case will discuss dislodgement of a coronary stent during attempted PCI. Dislodgement of a coronary stentis a rare complication, but it’s occurence can carry significant morbidity. Some of the more severe complications includecerebrovascular embolization, peripheral embolization, and coronary embolization. Snare loop, grasping forceps, basketretrieval devices, and wire techniques have all been used to retrieve stents percutaneously. In this case we describe retrievalof a coronary stent which became lodged in the scaffold of a pre-existing left main coronary stent and extended into the aorticroot.
Case Description: 67 year old male admitted from the ED secondary to Unstable Angina. The patient had an extensivehistory including CABG in 2008 and multiple PCI’s. He is known to have an atretic LIMA – LAD, patent SVG – PDA, patentSVG – OM, CTO SVG – Diag, CTO SVG – additonal OM, stenting of LAD proximal to distal, PCI to proximal RamusIntermedius, and recent PCI to Left Main coronary artery. During the diagnostic LHC there was difficulty engaging the leftmain coronary artery due to the present stent. After completion of imaging, the JL4 catheter was exchanged for an XB 4.0guide. This allowed for better engagement and revealed a focal 80% non-high C ramus intermedius lesion just distal to apatent stent. This lesion had been present on the prior angiogram 3 months prior, but was not nearly as significant, so thedecision was made to do PCI. A run through wire was placed distally into this vessel. A 3.0/12mm Xience Alpine was placedacross the wire, but could not be passed beyond the ostial portion of the left main coronary artery. The balloon/stent wasremoved, however, upon evaluation only the balloon had been extracted. Multiple fluorscopic views were obtained revealingthe stent to be lodged in the ostium of the left main and extending into the aortic root. The decision was made forpercutaneous retrieval, so a 401 Hi-torque Whisper wire was insterted, followed by a 30mm Goose Neck Microsnare. Thestent was not grasped by the microsnare, so it was removed. The wire was then looped through the scaffolding of the stentand it was pulled to the level of the right common femoral artery (CFA). However, upon removal, the wire broke and thestent/wire remained in the right CFA. Access was obtained in the left CFA and a Ensnare18x30 was used to retrieve both thestent and wire. Follow up angiography was done and there was no evidence of vascular injury. Due to chronic kidney diseasewith a large dye load, the procedure was completed and medical management continued. The patient did well throughout thehospitalization and was discharged home.
Discussion: This case is a strong example of how a routine procedure has the potential to have severe complications. Thewire passed easily through the left main into the ramus intermedius. However, the balloon/stent would not. This is likely due tothe wire passing through the stent scaffolding and the larger balloon/stent getting stuck. In the past stent dislodgement wasmore commonly associated with manually crimped stents, which is not routinely done any longer and not done in this case.Generally, the stent comes off the balloon when it is being pulled back into the guider or when it is being removed after inabilityto be placed secondary to unfavorable anatomy and/or inability to reach the lesion. Due to stent being partially in the left mainand the majority in the aorta, it was difficult to get the snare in the proper orientation, which is likely why this was unsuccessful.The wire allowed a more direct approach, while quick circular maneuvering of the wire in the vicinity of the stent allowed it towind through the struts getting a stable hold and allowing it to be pulled back to the CFA. The wire likely broke due to multipleloops through the scaffolding and the increased force used for removal. The Ensnare easily grasped the stent/wire andremoved without complications. There are multiple methods of stent retrieval, both from coronary arteries and peripherally.However, in this case the options were limited due to the location of the stent. Once the stent was within the CFA, anotheroption could have been to compress the stent against the wall of the vessel, however, this was deemed the final option ifunable to be retrieved entirely.
Conclusion: Dislodging of a stent is a rare complicatoin of percutaneous coronary intervention and causes an increase inmorbidity. This case is a good example of a routine procedure having the potential for severe complications such as coronary,cerebrovascular, and peripheral embolization of the stent. The Gooseneck microsnare, Ensnare, and wire were all used duringthis case showing the difficulty of removing a dislodged stent, along with how it may require multiple techniques for successfulretrieval.
West Virginia-ACC Poster Competition Abstract
Authors:Jason P. Mader, DO; David Francke, MD; Haytham Aljoudi, MD; Rameez Sayyed, MD.
C
Author to Receive Correspondence - Contact Information
Full Name: Mader Jason PLast First M.I.
Address: 1249 15th Street Suite 4000Street Address Apartment/Unit
#Huntington WV 25705
City State ZIP CodeWork Phone: 3046911000 Alternate Phone: 3046339113
E-mail Address: [email protected]
TrainingProgram: Marshall University Cardiology
_X_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Inferior STEMI Complicated by Retroperitoneal Hemorrhage due to Ruptured AAA
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )When patients presents with life threatening conditions, a rapid cost-benefit analysis prioritizes care and commits treatment toa certain course that, in the case of ST Elevation Myocardial Infarction (STEMI) treated with drug-eluting stents (DES), couldbe fatal if there is any deviation. Antiplatelet therapy is vital and secondary concerns (i.e. bleeding diatheses) may acceptsuboptimal outcomes – in rare cases, another life-threatening condition may be unmasked, one which is directly threatened bythe treatment for the first. We present a case of STEMI with high clot burden treated with multiple DES, complicated byretroperitoneal hemorrhage due to a ruptured abdominal aortic aneurysm.
West Virginia-ACC Poster Competition Abstract
Authors:
Neasman III M.D., Farley ; Lester D.O, Melissa; Chowdhury M.D., Nepal
C
Author to neasReceive Correspondence - Contact Information
Full Name: Neasman III M.D/ Farley BerryLast First M.I.
Address: 1249 15th street Suite 4000Street Address Apartment/Unit
#Huntington wv 25701
City State ZIP CodeWork Phone: 304-691-8500 Alternate Phone: 956-343-0084
E-mail Address: [email protected]
TrainingProgram: Marshall University Cardiology
XI understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Huge True LV Aneurysm with Cardiac Tamponade: Atypical Presentation
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Objective:1. Recognize, Diagnose, and Manage Cardiac Tamponade2. Recognize and Manage the Myocardial Infarction Complication such as Left Ventricle Aneurysm
Case Presentation49 years old CM with unremarkable PMH, nonsmoker, presented to the ER for feeling fatigue, nonproductive cough, and URIsymptoms for the past month. He denied chest pain, fever, chill, shortness of breath. He had not seen a PCP for the past 12years. Patient reported that he had lost about 10-15lbs but felt that it was likely due to working on his house that he and hiswife bought about 2 months ago.VS: BP 153/111, HR 106, T98.1, RR18, SaO2 95%Neck: supple, +JVDHeart: tachycardia, regular rhythm, no murmursLung: CTA, non-labored, no wheezes or ralesExt: warm, pulse 2+, capillary refills <2sTTE –RV collapse during systole, LV aneurysmPatient underwent emergent pericardiocentesis, and LHC showed LV aneurysm and RCA disease. Patient is evaluated foraneurysmectomy
Discussion:The presentation of cardiac tamponade depends upon the length of time over which pericardial fluid accumulates (1).In acute cardiac tamponade, patient presents with chest pain, tachypnea, elevated jugular venous pressure, and hypotension.Echocardiography plays major roles in the identification of pericardial effusion and assessing its hemodynamic significance.Early cardiac tamponade with minimal or no evidence of hemodynamic compromise may be treated conservatively, withcareful hemodynamic monitoring, serial echocardiographic studies, avoidance of volume depletion, and therapy aimed at theunderlying cause of the pericardial effusion. Both percutaneous and surgical drainage are highly effective at removal of fluidand relief of symptoms associated with hemodynamic compromise. Pericardiocentesis is treatment of choice in most patients.
Left ventricular aneurysms (LVAs) is one of the complications of MI that can lead to serious morbidity (2). LVA is mostcommonly the result of MI, usually involving the anterior wall. The presence of an LVA may be suspected from the EKG, chestX-ray, and echocardiography. Echo is most often used in diagnose. Small to moderate size asymptomatic aneurysms can besafely treated medically with a five-year survival of up to 90%. Surgical repair of an LVA is very effective, and results in asignificant improvement in patient survival, symptoms and functional class compared to medical treatment.
West Virginia-ACC Poster Competition Abstract
Authors:
C
Author to Receive Correspondence - Contact Information
Full Name: Nguyen Ngoc MLast First M.I.
Address: 945 4th Ave 113Street Address Apartment/Unit
#Huntington WV 25701
City State ZIP CodeWork Phone: Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: Marshall
__yes_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:ACQUIRED GERBODE DEFECT INVOLVING THE MITRAL VALVE
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Background: Gerbode defect is a rare intracardiac shunt between the left ventricle and right atrium which can be congenital(type I defect) and in even rarer cases, can be acquired (type II defect), as a complication of endocarditis, myocardialinfarction, chest trauma, or post previous cardiac surgery. Cases secondary to endocarditis are commonly a result ofStaphylococcus aureus, involve the aortic or tricuspid valve, and mortality rates are as high as 13.6%. We present an acquiredGerbode, type II, defect due to mitral valve endocarditis, where the echocardiographic assessment was essential to thepatient’s management and survival. To our knowledge, this type of case has not been reported in the literature.
Case: 49-year-old male presented to an outlying hospital for second degree burns involving 18% of his total body surfacearea. He was transferred to our facility for further care and was treated with multiple debridements. The patient subsequentdeveloped endocarditis secondary to methicillin resistant Staphylococcus aureus (MRSA) and subsequent transesophagealechocardiogram revealed a large vegetation and perforation of the A3 leaftlet of the mitral valve, leading to subsequent severemitral regurgitation, with fistula formation to the right atrium, consistent with Gerbode defect. Due to hemodynamic instability,he was transferred to higher level of care for surgical repair of the Gerbode defect.
Discussion: We present a type II Gerbode defect, involving the mitral valve, which has not been previously described in theliterature. We hypothesize that the infection traveled from the anterior valve of the mitral leaflet and through the membranousportion of the interventricular septum, leading to a perforation, creating an intracardiac shunt. This theory was furthersupported by color flow on echocardiogram and confirms that mitral valve endocarditis can lead to a type II Gerbode defect.
West Virginia-ACC Poster Competition Abstract
Authors:
Shah, R., DO; Cansino, S., MD
C
Author to Receive Correspondence - Contact Information
Full Name: Shah Rani ALast First M.I.
Address: 1249 15th Street Suite 4000Street Address Apartment/Unit
#Huntington WV 25701
City State ZIP CodeWork Phone: 3046918534 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: Marshall University, Adult Cardiology Program
_X__I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
Is Eximer Coronary laser Atherectomy “ ECLA” is underutilizedvaluable tool !!
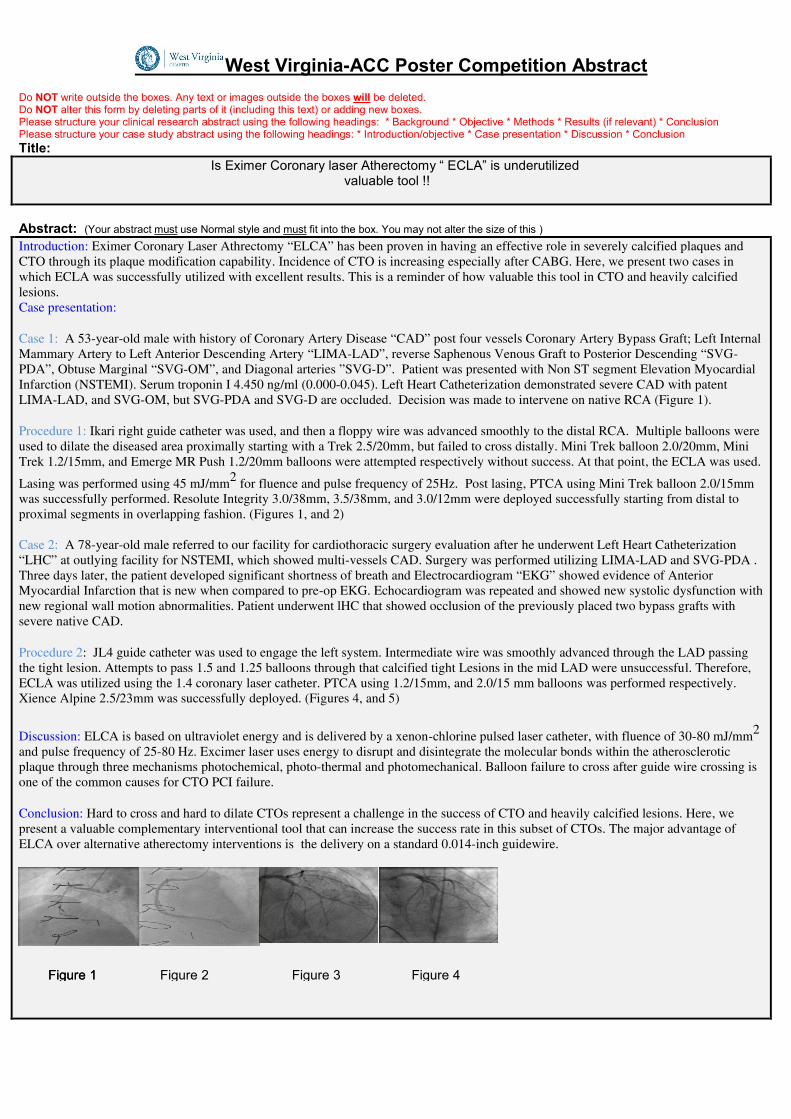
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction: Eximer Coronary Laser Athrectomy “ELCA” has been proven in having an effective role in severely calcified plaques andCTO through its plaque modification capability. Incidence of CTO is increasing especially after CABG. Here, we present two cases inwhich ECLA was successfully utilized with excellent results. This is a reminder of how valuable this tool in CTO and heavily calcifiedlesions.Case presentation:
Case 1: A 53-year-old male with history of Coronary Artery Disease “CAD” post four vessels Coronary Artery Bypass Graft; Left InternalMammary Artery to Left Anterior Descending Artery “LIMA-LAD”, reverse Saphenous Venous Graft to Posterior Descending “SVG-PDA”, Obtuse Marginal “SVG-OM”, and Diagonal arteries ”SVG-D”. Patient was presented with Non ST segment Elevation MyocardialInfarction (NSTEMI). Serum troponin I 4.450 ng/ml (0.000-0.045). Left Heart Catheterization demonstrated severe CAD with patentLIMA-LAD, and SVG-OM, but SVG-PDA and SVG-D are occluded. Decision was made to intervene on native RCA (Figure 1).
Procedure 1: Ikari right guide catheter was used, and then a floppy wire was advanced smoothly to the distal RCA. Multiple balloons wereused to dilate the diseased area proximally starting with a Trek 2.5/20mm, but failed to cross distally. Mini Trek balloon 2.0/20mm, MiniTrek 1.2/15mm, and Emerge MR Push 1.2/20mm balloons were attempted respectively without success. At that point, the ECLA was used.
Lasing was performed using 45 mJ/mm2 for fluence and pulse frequency of 25Hz. Post lasing, PTCA using Mini Trek balloon 2.0/15mmwas successfully performed. Resolute Integrity 3.0/38mm, 3.5/38mm, and 3.0/12mm were deployed successfully starting from distal toproximal segments in overlapping fashion. (Figures 1, and 2)
Case 2: A 78-year-old male referred to our facility for cardiothoracic surgery evaluation after he underwent Left Heart Catheterization“LHC” at outlying facility for NSTEMI, which showed multi-vessels CAD. Surgery was performed utilizing LIMA-LAD and SVG-PDA .Three days later, the patient developed significant shortness of breath and Electrocardiogram “EKG” showed evidence of AnteriorMyocardial Infarction that is new when compared to pre-op EKG. Echocardiogram was repeated and showed new systolic dysfunction withnew regional wall motion abnormalities. Patient underwent lHC that showed occlusion of the previously placed two bypass grafts withsevere native CAD.
Procedure 2: JL4 guide catheter was used to engage the left system. Intermediate wire was smoothly advanced through the LAD passingthe tight lesion. Attempts to pass 1.5 and 1.25 balloons through that calcified tight Lesions in the mid LAD were unsuccessful. Therefore,ECLA was utilized using the 1.4 coronary laser catheter. PTCA using 1.2/15mm, and 2.0/15 mm balloons was performed respectively.Xience Alpine 2.5/23mm was successfully deployed. (Figures 4, and 5)
Discussion: ELCA is based on ultraviolet energy and is delivered by a xenon-chlorine pulsed laser catheter, with fluence of 30-80 mJ/mm2
and pulse frequency of 25-80 Hz. Excimer laser uses energy to disrupt and disintegrate the molecular bonds within the atheroscleroticplaque through three mechanisms photochemical, photo-thermal and photomechanical. Balloon failure to cross after guide wire crossing isone of the common causes for CTO PCI failure.
Conclusion: Hard to cross and hard to dilate CTOs represent a challenge in the success of CTO and heavily calcified lesions. Here, wepresent a valuable complementary interventional tool that can increase the success rate in this subset of CTOs. The major advantage ofELCA over alternative atherectomy interventions is the delivery on a standard 0.014-inch guidewire.
Figure 1Figure 1 Figure 2 Figure 3 Figure 4
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
Is Eximer Coronary laser Atherectomy “ ECLA” is underutilizedvaluable tool !!
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction: Eximer Coronary Laser Athrectomy “ELCA” has been proven in having an effective role in severely calcified plaques andCTO through its plaque modification capability. Incidence of CTO is increasing especially after CABG. Here, we present two cases inwhich ECLA was successfully utilized with excellent results. This is a reminder of how valuable this tool in CTO and heavily calcifiedlesions.Case presentation:
Case 1: A 53-year-old male with history of Coronary Artery Disease “CAD” post four vessels Coronary Artery Bypass Graft; Left InternalMammary Artery to Left Anterior Descending Artery “LIMA-LAD”, reverse Saphenous Venous Graft to Posterior Descending “SVG-PDA”, Obtuse Marginal “SVG-OM”, and Diagonal arteries ”SVG-D”. Patient was presented with Non ST segment Elevation MyocardialInfarction (NSTEMI). Serum troponin I 4.450 ng/ml (0.000-0.045). Left Heart Catheterization demonstrated severe CAD with patentLIMA-LAD, and SVG-OM, but SVG-PDA and SVG-D are occluded. Decision was made to intervene on native RCA (Figure 1).
Procedure 1: Ikari right guide catheter was used, and then a floppy wire was advanced smoothly to the distal RCA. Multiple balloons wereused to dilate the diseased area proximally starting with a Trek 2.5/20mm, but failed to cross distally. Mini Trek balloon 2.0/20mm, MiniTrek 1.2/15mm, and Emerge MR Push 1.2/20mm balloons were attempted respectively without success. At that point, the ECLA was used.
Lasing was performed using 45 mJ/mm2 for fluence and pulse frequency of 25Hz. Post lasing, PTCA using Mini Trek balloon 2.0/15mmwas successfully performed. Resolute Integrity 3.0/38mm, 3.5/38mm, and 3.0/12mm were deployed successfully starting from distal toproximal segments in overlapping fashion. (Figures 1, and 2)
Case 2: A 78-year-old male referred to our facility for cardiothoracic surgery evaluation after he underwent Left Heart Catheterization“LHC” at outlying facility for NSTEMI, which showed multi-vessels CAD. Surgery was performed utilizing LIMA-LAD and SVG-PDA .Three days later, the patient developed significant shortness of breath and Electrocardiogram “EKG” showed evidence of AnteriorMyocardial Infarction that is new when compared to pre-op EKG. Echocardiogram was repeated and showed new systolic dysfunction withnew regional wall motion abnormalities. Patient underwent lHC that showed occlusion of the previously placed two bypass grafts withsevere native CAD.
Procedure 2: JL4 guide catheter was used to engage the left system. Intermediate wire was smoothly advanced through the LAD passingthe tight lesion. Attempts to pass 1.5 and 1.25 balloons through that calcified tight Lesions in the mid LAD were unsuccessful. Therefore,ECLA was utilized using the 1.4 coronary laser catheter. PTCA using 1.2/15mm, and 2.0/15 mm balloons was performed respectively.Xience Alpine 2.5/23mm was successfully deployed. (Figures 4, and 5)
Discussion: ELCA is based on ultraviolet energy and is delivered by a xenon-chlorine pulsed laser catheter, with fluence of 30-80 mJ/mm2
and pulse frequency of 25-80 Hz. Excimer laser uses energy to disrupt and disintegrate the molecular bonds within the atheroscleroticplaque through three mechanisms photochemical, photo-thermal and photomechanical. Balloon failure to cross after guide wire crossing isone of the common causes for CTO PCI failure.
Conclusion: Hard to cross and hard to dilate CTOs represent a challenge in the success of CTO and heavily calcified lesions. Here, wepresent a valuable complementary interventional tool that can increase the success rate in this subset of CTOs. The major advantage ofELCA over alternative atherectomy interventions is the delivery on a standard 0.014-inch guidewire.
Figure 1Figure 1 Figure 2 Figure 3 Figure 4
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
Is Eximer Coronary laser Atherectomy “ ECLA” is underutilizedvaluable tool !!
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction: Eximer Coronary Laser Athrectomy “ELCA” has been proven in having an effective role in severely calcified plaques andCTO through its plaque modification capability. Incidence of CTO is increasing especially after CABG. Here, we present two cases inwhich ECLA was successfully utilized with excellent results. This is a reminder of how valuable this tool in CTO and heavily calcifiedlesions.Case presentation:
Case 1: A 53-year-old male with history of Coronary Artery Disease “CAD” post four vessels Coronary Artery Bypass Graft; Left InternalMammary Artery to Left Anterior Descending Artery “LIMA-LAD”, reverse Saphenous Venous Graft to Posterior Descending “SVG-PDA”, Obtuse Marginal “SVG-OM”, and Diagonal arteries ”SVG-D”. Patient was presented with Non ST segment Elevation MyocardialInfarction (NSTEMI). Serum troponin I 4.450 ng/ml (0.000-0.045). Left Heart Catheterization demonstrated severe CAD with patentLIMA-LAD, and SVG-OM, but SVG-PDA and SVG-D are occluded. Decision was made to intervene on native RCA (Figure 1).
Procedure 1: Ikari right guide catheter was used, and then a floppy wire was advanced smoothly to the distal RCA. Multiple balloons wereused to dilate the diseased area proximally starting with a Trek 2.5/20mm, but failed to cross distally. Mini Trek balloon 2.0/20mm, MiniTrek 1.2/15mm, and Emerge MR Push 1.2/20mm balloons were attempted respectively without success. At that point, the ECLA was used.
Lasing was performed using 45 mJ/mm2 for fluence and pulse frequency of 25Hz. Post lasing, PTCA using Mini Trek balloon 2.0/15mmwas successfully performed. Resolute Integrity 3.0/38mm, 3.5/38mm, and 3.0/12mm were deployed successfully starting from distal toproximal segments in overlapping fashion. (Figures 1, and 2)
Case 2: A 78-year-old male referred to our facility for cardiothoracic surgery evaluation after he underwent Left Heart Catheterization“LHC” at outlying facility for NSTEMI, which showed multi-vessels CAD. Surgery was performed utilizing LIMA-LAD and SVG-PDA .Three days later, the patient developed significant shortness of breath and Electrocardiogram “EKG” showed evidence of AnteriorMyocardial Infarction that is new when compared to pre-op EKG. Echocardiogram was repeated and showed new systolic dysfunction withnew regional wall motion abnormalities. Patient underwent lHC that showed occlusion of the previously placed two bypass grafts withsevere native CAD.
Procedure 2: JL4 guide catheter was used to engage the left system. Intermediate wire was smoothly advanced through the LAD passingthe tight lesion. Attempts to pass 1.5 and 1.25 balloons through that calcified tight Lesions in the mid LAD were unsuccessful. Therefore,ECLA was utilized using the 1.4 coronary laser catheter. PTCA using 1.2/15mm, and 2.0/15 mm balloons was performed respectively.Xience Alpine 2.5/23mm was successfully deployed. (Figures 4, and 5)
Discussion: ELCA is based on ultraviolet energy and is delivered by a xenon-chlorine pulsed laser catheter, with fluence of 30-80 mJ/mm2
and pulse frequency of 25-80 Hz. Excimer laser uses energy to disrupt and disintegrate the molecular bonds within the atheroscleroticplaque through three mechanisms photochemical, photo-thermal and photomechanical. Balloon failure to cross after guide wire crossing isone of the common causes for CTO PCI failure.
Conclusion: Hard to cross and hard to dilate CTOs represent a challenge in the success of CTO and heavily calcified lesions. Here, wepresent a valuable complementary interventional tool that can increase the success rate in this subset of CTOs. The major advantage ofELCA over alternative atherectomy interventions is the delivery on a standard 0.014-inch guidewire.
Figure 1Figure 1 Figure 2 Figure 3 Figure 4
West Virginia-ACC Poster Competition Abstract
Authors:
Yousef, G.M., Elhamdani, M.
C
Author to Receive Correspondence - Contact Information
Full Name: Yousef George MLast First M.I.
Address: 1249 15th streetStreet Address Apartment/Unit
#Huntington WV 25701
City State ZIP CodeWork Phone: Alternate Phone: (304) 942-4688
E-mail Address: [email protected]
TrainingProgram: Marshall University
I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
Resident Cases
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Recognition and Treatment of Atrial Fibrillation Caused by an Accessory Pathway in a Middle Aged Patient.
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction:Atrial fibrillation (AF) is the most common cardiac arrhythmia in clinical practice. Hypertensive heart disease and coronaryartery disease remain the most common chronic underlying cardiac cases of AF. Potentially reversible risk factors of AF inyoung patients include acute alcohol intoxication (holiday heart), thyrotoxicosis, cardiothoracic and non cardiothoracic surgery.Autonomic dysfunction may play a role in the development of AF especially in the paroxysmal type. Evidence from previousstudies indicates that accessory pathway may play a major role in the development of AF. It also has been reported thatpatient with concealed accessory pathway as well as patient with Wolff Parkinson White disease could be expected to have anincidence of AF. Explanations for the occurrence of AF in these patients is not fully clear but a proposed mechanism is aretrograde conduction of the ventricular beat could degenerate into atrial fibrillation in the atrium.
Case presentation:48 years old white Caucasian male with history of coronary artery disease and multiple stents, history of AF status post fourelectrical cardioversions, on Rivaroxaban and Sotalol therapy. He presented with recurrent tachypalpitations associated withdizziness and lightheadedness. No chest pain or syncope. Social history is negative for any alcohol intake. Initial EKG showednarrow complex tachycardia, 172 beats per minute, short RP with inverted P waves in lead II. Physical exam showed stableblood pressure and respiratory rate. Cardiac exam showed tachycardia with regular heart rhythm, without murmurs, gallop orrubs. TSH was normal and troponin was negative. He received Digoxin intravenously in ER, tachycardia persisted but QRSbecame wide (aberrancy, no pre-excitation). Amiodarone was given IV for possible Ventricular Tachycardia, and he convertedto sinus rhythm. Since he is young and presented with a regular tachycardia, we suspected the presence of SVT as a cause ofAF. Electrophysiology study was done and revealed a left concealed accessory pathway, inducible OrthodromicReentry Tachycardia (ORT), and no pre-excitation. Radio-frequency ablation of the AP was successful and ORT was notinducible. The patient may not have to be on an anticoagulant and anti-arrhythmic agent anymore. We felt comfortablestopping Sotalol and Rivaroxaban. He was seen in follow up appointment and was doing well.
Discussion:AF in young patients can be trigged by multiple reversible causes, accessory pathway is an under estimated reversible causeof AF. Our patient was a middle aged man with resistant AF, was found to have accessory pathway after comprehensive EPstudy. Radio-frequency catheter ablation was a successful treatment to prevent atrial fibrillation recurrence and toget the patient off Xarelto and Sotalol.
Conclusion:We would like to emphasize the importance of recognition of concealed accessory pathway as a cause of reversible atrialfibrillation in young and middle aged patients. We can save these patients of being on lifelong anticoagulation and ant-arrhythmic treatment by managing them with radio-frequency ablation treatment.
West Virginia-ACC Poster Competition Abstract
Authors:
Abdelrahman Aljadi MD.Esam Baryun MD.
C
Author to Receive Correspondence - Contact Information
Full Name: Aljadi Abdelrahman MLast First M.I.
Address: 6419 Country Club DrStreet Address Apartment/Unit
#Huntington WV 25705
Work Phone: 8322584039 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: Marshall University School of Medicine.
_xx__I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Blue Toe Syndrome
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Intro: Blue Toe Syndrome is usually caused by embolic occlusion of distal arteries secondary to a proximal atherothromboticsource that is characterized by sudden appearance of cold, painful, discolored toes in the setting of palpable pulses onphysical exam. Bilateral lower extremity involvement usually indicates an embolic source that must be identified and treated toprevent devastating complications such as tissue loss or organ failure. The following is a case of a man who developed bluetoe syndrome and underwent successful repair of an ulcerated abdominal aortic aneurysm. It is known that microembolizationcan occur after an invasive vascular procedure (such as cardiac catheterization) or due to an aneurysm. The patient in thiscase had both.Case Presentation: A seventy-one year old white male with past medical history of hyperlipidemia, glaucoma, prior tobaccouse and coronary artery disease presented to an ambulatory care center complaining of toe discoloration and pain. His chiefcomplaint on presentation consisted of his right great and second toes “turning black” accompanied by severe pain, especiallywith ambulation. Onset of pain was shortly after his heart catheterization a month prior. He was evaluated, pertinent physicalexam noting bluish discoloration of the first and second digit of the right foot, with intact bilateral pulses. He was told he mayhave Raynaud’s phenomenon and was instructed to follow up with his primary care provider. When his symptoms did notimprove, he was evaluated by cardiology who ordered a computed tomography angiography of the abdomen with runoff whichrevealed a 3.8 cm infrarenal abdominal aortic aneurysm with ulcerated mural thrombus near the near the right renal artery .He was subsequently admitted to the hospital for further evaluation and aneurysm repair. On admission vital signs were withinnormal limits, physical exam revealed the feet were cool to touch with bilateral bluish discoloration of the toes and with livedoreticularis of the dorsum of feet.There were bilateral intact palpable dorsalis pedis and posterior tibialis pulses. Medications attime of admission included aspirin, plavix, lisinopril, amlodipine and metoprolol. Statin therapy was initiated. Labs onadmission demonstrated normal complete metabolic panel, normal complete blood count, and elevated total serum cholesterolof 282, triglycerides 224, high density lipoprotein 62, low density lipoprotein of 179. Ankle-brachial index was normal howevertoe-brachial index was severely abnormal further reflecting distal circulation pathology. The diagnosis of critical limb ischemiasecondary to an ulcerated aortic aneurysm with mural thrombus and distal embolization and bilateral blue toe syndrome wasmade. On admission, he had a normal skin perfusion test with the exception of severe right hallux disease and mild left halluxdisease. Patient was observed overnight with no further events, thena successful percutaneous endovascular aneurysmrepair.The patient tolerated the procedure well. Patient was started on a high dose statin regimen and on day of dischargehad marked improvement of his bilateral toe discoloration and improvement of pain symptoms that were further observed on a2 week office follow- up.Discussion: This case demonstrates the importance of having a high index of suspicion for embolic phenomenon after anyinvasive vascular procedure and the need to rule out such a diagnosis in a patient who presents with pain and discoloration ofa limb/digits before treating more benign conditions such as a vasospastic syndrome. Differential diagnosis for discolored toesincludes embolic, thrombotic and intramural pathologies - embolic and thrombotic being the most worrisome with devastatingconsequences. Intramural disease such as Raynaud’s and vasculitities usually present with similar discoloration that can betransient (i.e. depending on temperature) and usually present with other known connective tissue disorders. Cardiac sourcesof emboli should be considered as well. Embolic phenomenon after left heart catheterization is approximately 1.4% however,not all presented with cutaneous manifestations, most others presented with creatinine elevations at three weeks postprocedure. After the diagnosis is made, the goal of therapy for blue toe syndrome is to control the source of the embolization.Although our patient did demonstrate signs of blue toe syndrome shortly after his heart catherization, the ulcerative nature ofthe aneurysm and the presence of thrombus on the CT scan were in need of urgent repair to prevent further embolicphenomenon and reduce subsequent morbidity and mortality. Blue toe syndrome is characterized by sudden appearance ofcold, painful, discolored toes and/or livedo reticularis, purpura, cutaneous necrosis to multi-organ systemic disease (includingrenal failure and organ failure) in the setting of palpable pulses on physical exam. The mechanism of blue toe syndromeincludes occlusion of small distal arteries due to cholesterol crystals that dislodge from the aneurismal wall. While kidneyfailure, splenic and bowel ischemia are commonly associated with blue toe syndrome – up to 30-70% of cases, our patientwas fortunate to not have these complications. If a patient does have systemic complications from microembolization,mortality can be up to 70%.Conclusion: This case demonstrates the need for urgent diagnosis of embolic phenomenon before concluding on lessdevastating diagnoses such as Raynaud’s phenomenon. Heightened awareness of risk factors, lab findings and mostimportantly suspicious physical exam findings especially in patients with recent vascular interventions help avoid mis-diagnoses and can potentially be life-saving.
West Virginia-ACC Poster Competition Abstract
Authors:
Elise Anderson, DO, Navid Iqbal, MD, Mehair El-Hamdani, MD
C
Author to Receive Correspondence - Contact Information
Full Name: Anderson Elise SLast First M.I.
Address: 2125 Brooke StStreet Address Apartment/Unit
#Culloden WV 25510
City State ZIP CodeWork Phone: 3047105768 Alternate Phone: 304-710-5768
E-mail Address: [email protected]
TrainingProgram: Marshall University
__x_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
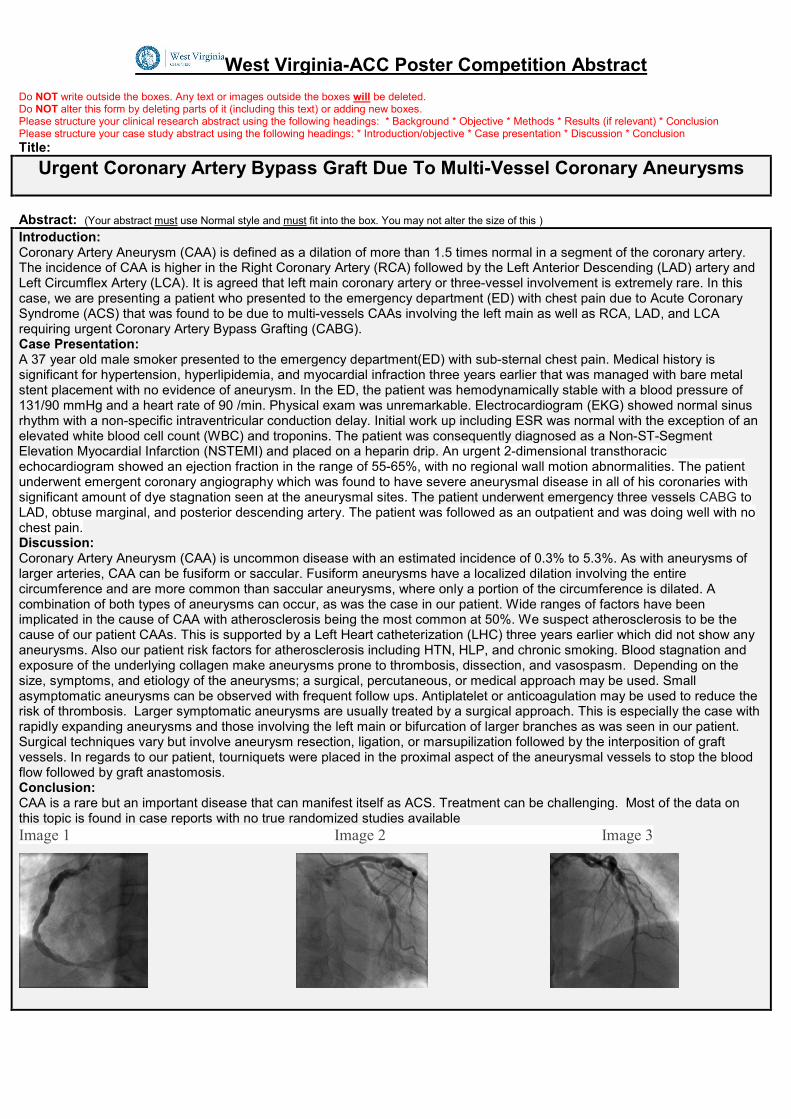
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
Urgent Coronary Artery Bypass Graft Due To Multi-Vessel Coronary Aneurysms
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction:Coronary Artery Aneurysm (CAA) is defined as a dilation of more than 1.5 times normal in a segment of the coronary artery.The incidence of CAA is higher in the Right Coronary Artery (RCA) followed by the Left Anterior Descending (LAD) artery andLeft Circumflex Artery (LCA). It is agreed that left main coronary artery or three-vessel involvement is extremely rare. In thiscase, we are presenting a patient who presented to the emergency department (ED) with chest pain due to Acute CoronarySyndrome (ACS) that was found to be due to multi-vessels CAAs involving the left main as well as RCA, LAD, and LCArequiring urgent Coronary Artery Bypass Grafting (CABG).Case Presentation:A 37 year old male smoker presented to the emergency department(ED) with sub-sternal chest pain. Medical history issignificant for hypertension, hyperlipidemia, and myocardial infraction three years earlier that was managed with bare metalstent placement with no evidence of aneurysm. In the ED, the patient was hemodynamically stable with a blood pressure of131/90 mmHg and a heart rate of 90 /min. Physical exam was unremarkable. Electrocardiogram (EKG) showed normal sinusrhythm with a non-specific intraventricular conduction delay. Initial work up including ESR was normal with the exception of anelevated white blood cell count (WBC) and troponins. The patient was consequently diagnosed as a Non-ST-SegmentElevation Myocardial Infarction (NSTEMI) and placed on a heparin drip. An urgent 2-dimensional transthoracicechocardiogram showed an ejection fraction in the range of 55-65%, with no regional wall motion abnormalities. The patientunderwent emergent coronary angiography which was found to have severe aneurysmal disease in all of his coronaries withsignificant amount of dye stagnation seen at the aneurysmal sites. The patient underwent emergency three vessels CABG toLAD, obtuse marginal, and posterior descending artery. The patient was followed as an outpatient and was doing well with nochest pain.Discussion:Coronary Artery Aneurysm (CAA) is uncommon disease with an estimated incidence of 0.3% to 5.3%. As with aneurysms oflarger arteries, CAA can be fusiform or saccular. Fusiform aneurysms have a localized dilation involving the entirecircumference and are more common than saccular aneurysms, where only a portion of the circumference is dilated. Acombination of both types of aneurysms can occur, as was the case in our patient. Wide ranges of factors have beenimplicated in the cause of CAA with atherosclerosis being the most common at 50%. We suspect atherosclerosis to be thecause of our patient CAAs. This is supported by a Left Heart catheterization (LHC) three years earlier which did not show anyaneurysms. Also our patient risk factors for atherosclerosis including HTN, HLP, and chronic smoking. Blood stagnation andexposure of the underlying collagen make aneurysms prone to thrombosis, dissection, and vasospasm. Depending on thesize, symptoms, and etiology of the aneurysms; a surgical, percutaneous, or medical approach may be used. Smallasymptomatic aneurysms can be observed with frequent follow ups. Antiplatelet or anticoagulation may be used to reduce therisk of thrombosis. Larger symptomatic aneurysms are usually treated by a surgical approach. This is especially the case withrapidly expanding aneurysms and those involving the left main or bifurcation of larger branches as was seen in our patient.Surgical techniques vary but involve aneurysm resection, ligation, or marsupilization followed by the interposition of graftvessels. In regards to our patient, tourniquets were placed in the proximal aspect of the aneurysmal vessels to stop the bloodflow followed by graft anastomosis.Conclusion:CAA is a rare but an important disease that can manifest itself as ACS. Treatment can be challenging. Most of the data onthis topic is found in case reports with no true randomized studies availableImage 1 Image 2 Image 3
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
Urgent Coronary Artery Bypass Graft Due To Multi-Vessel Coronary Aneurysms
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction:Coronary Artery Aneurysm (CAA) is defined as a dilation of more than 1.5 times normal in a segment of the coronary artery.The incidence of CAA is higher in the Right Coronary Artery (RCA) followed by the Left Anterior Descending (LAD) artery andLeft Circumflex Artery (LCA). It is agreed that left main coronary artery or three-vessel involvement is extremely rare. In thiscase, we are presenting a patient who presented to the emergency department (ED) with chest pain due to Acute CoronarySyndrome (ACS) that was found to be due to multi-vessels CAAs involving the left main as well as RCA, LAD, and LCArequiring urgent Coronary Artery Bypass Grafting (CABG).Case Presentation:A 37 year old male smoker presented to the emergency department(ED) with sub-sternal chest pain. Medical history issignificant for hypertension, hyperlipidemia, and myocardial infraction three years earlier that was managed with bare metalstent placement with no evidence of aneurysm. In the ED, the patient was hemodynamically stable with a blood pressure of131/90 mmHg and a heart rate of 90 /min. Physical exam was unremarkable. Electrocardiogram (EKG) showed normal sinusrhythm with a non-specific intraventricular conduction delay. Initial work up including ESR was normal with the exception of anelevated white blood cell count (WBC) and troponins. The patient was consequently diagnosed as a Non-ST-SegmentElevation Myocardial Infarction (NSTEMI) and placed on a heparin drip. An urgent 2-dimensional transthoracicechocardiogram showed an ejection fraction in the range of 55-65%, with no regional wall motion abnormalities. The patientunderwent emergent coronary angiography which was found to have severe aneurysmal disease in all of his coronaries withsignificant amount of dye stagnation seen at the aneurysmal sites. The patient underwent emergency three vessels CABG toLAD, obtuse marginal, and posterior descending artery. The patient was followed as an outpatient and was doing well with nochest pain.Discussion:Coronary Artery Aneurysm (CAA) is uncommon disease with an estimated incidence of 0.3% to 5.3%. As with aneurysms oflarger arteries, CAA can be fusiform or saccular. Fusiform aneurysms have a localized dilation involving the entirecircumference and are more common than saccular aneurysms, where only a portion of the circumference is dilated. Acombination of both types of aneurysms can occur, as was the case in our patient. Wide ranges of factors have beenimplicated in the cause of CAA with atherosclerosis being the most common at 50%. We suspect atherosclerosis to be thecause of our patient CAAs. This is supported by a Left Heart catheterization (LHC) three years earlier which did not show anyaneurysms. Also our patient risk factors for atherosclerosis including HTN, HLP, and chronic smoking. Blood stagnation andexposure of the underlying collagen make aneurysms prone to thrombosis, dissection, and vasospasm. Depending on thesize, symptoms, and etiology of the aneurysms; a surgical, percutaneous, or medical approach may be used. Smallasymptomatic aneurysms can be observed with frequent follow ups. Antiplatelet or anticoagulation may be used to reduce therisk of thrombosis. Larger symptomatic aneurysms are usually treated by a surgical approach. This is especially the case withrapidly expanding aneurysms and those involving the left main or bifurcation of larger branches as was seen in our patient.Surgical techniques vary but involve aneurysm resection, ligation, or marsupilization followed by the interposition of graftvessels. In regards to our patient, tourniquets were placed in the proximal aspect of the aneurysmal vessels to stop the bloodflow followed by graft anastomosis.Conclusion:CAA is a rare but an important disease that can manifest itself as ACS. Treatment can be challenging. Most of the data onthis topic is found in case reports with no true randomized studies availableImage 1 Image 2 Image 3
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
Urgent Coronary Artery Bypass Graft Due To Multi-Vessel Coronary Aneurysms
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction:Coronary Artery Aneurysm (CAA) is defined as a dilation of more than 1.5 times normal in a segment of the coronary artery.The incidence of CAA is higher in the Right Coronary Artery (RCA) followed by the Left Anterior Descending (LAD) artery andLeft Circumflex Artery (LCA). It is agreed that left main coronary artery or three-vessel involvement is extremely rare. In thiscase, we are presenting a patient who presented to the emergency department (ED) with chest pain due to Acute CoronarySyndrome (ACS) that was found to be due to multi-vessels CAAs involving the left main as well as RCA, LAD, and LCArequiring urgent Coronary Artery Bypass Grafting (CABG).Case Presentation:A 37 year old male smoker presented to the emergency department(ED) with sub-sternal chest pain. Medical history issignificant for hypertension, hyperlipidemia, and myocardial infraction three years earlier that was managed with bare metalstent placement with no evidence of aneurysm. In the ED, the patient was hemodynamically stable with a blood pressure of131/90 mmHg and a heart rate of 90 /min. Physical exam was unremarkable. Electrocardiogram (EKG) showed normal sinusrhythm with a non-specific intraventricular conduction delay. Initial work up including ESR was normal with the exception of anelevated white blood cell count (WBC) and troponins. The patient was consequently diagnosed as a Non-ST-SegmentElevation Myocardial Infarction (NSTEMI) and placed on a heparin drip. An urgent 2-dimensional transthoracicechocardiogram showed an ejection fraction in the range of 55-65%, with no regional wall motion abnormalities. The patientunderwent emergent coronary angiography which was found to have severe aneurysmal disease in all of his coronaries withsignificant amount of dye stagnation seen at the aneurysmal sites. The patient underwent emergency three vessels CABG toLAD, obtuse marginal, and posterior descending artery. The patient was followed as an outpatient and was doing well with nochest pain.Discussion:Coronary Artery Aneurysm (CAA) is uncommon disease with an estimated incidence of 0.3% to 5.3%. As with aneurysms oflarger arteries, CAA can be fusiform or saccular. Fusiform aneurysms have a localized dilation involving the entirecircumference and are more common than saccular aneurysms, where only a portion of the circumference is dilated. Acombination of both types of aneurysms can occur, as was the case in our patient. Wide ranges of factors have beenimplicated in the cause of CAA with atherosclerosis being the most common at 50%. We suspect atherosclerosis to be thecause of our patient CAAs. This is supported by a Left Heart catheterization (LHC) three years earlier which did not show anyaneurysms. Also our patient risk factors for atherosclerosis including HTN, HLP, and chronic smoking. Blood stagnation andexposure of the underlying collagen make aneurysms prone to thrombosis, dissection, and vasospasm. Depending on thesize, symptoms, and etiology of the aneurysms; a surgical, percutaneous, or medical approach may be used. Smallasymptomatic aneurysms can be observed with frequent follow ups. Antiplatelet or anticoagulation may be used to reduce therisk of thrombosis. Larger symptomatic aneurysms are usually treated by a surgical approach. This is especially the case withrapidly expanding aneurysms and those involving the left main or bifurcation of larger branches as was seen in our patient.Surgical techniques vary but involve aneurysm resection, ligation, or marsupilization followed by the interposition of graftvessels. In regards to our patient, tourniquets were placed in the proximal aspect of the aneurysmal vessels to stop the bloodflow followed by graft anastomosis.Conclusion:CAA is a rare but an important disease that can manifest itself as ACS. Treatment can be challenging. Most of the data onthis topic is found in case reports with no true randomized studies availableImage 1 Image 2 Image 3

West Virginia-ACC Poster Competition Abstract
Authors:
Obadah Aqtash1,MD; Ahmed Amro1,MD; Mian Alam2,MD; Rameez Sayed2 ,MD; Mark Studeny2 ,MD;
1- Department of Internal Medicine, Marshall University Joan C. Edwards School of Medicine, Huntington, WV, USA.2. Department of Cardiovascular Services. Marshall University Joan C. Edwards School of Medicine, Huntington, WV, USA.
C
Author to Receive Correspondence - Contact Information
Full Name: Aqtash Obadah SLast First M.I.
Address: 6709 Country Club Dr. 6709Street Address Apartment/Unit
#Huntington WV 25705
City State ZIP CodeWork Phone: 681-204-8668 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: Marshall University School Of Medicine
___I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
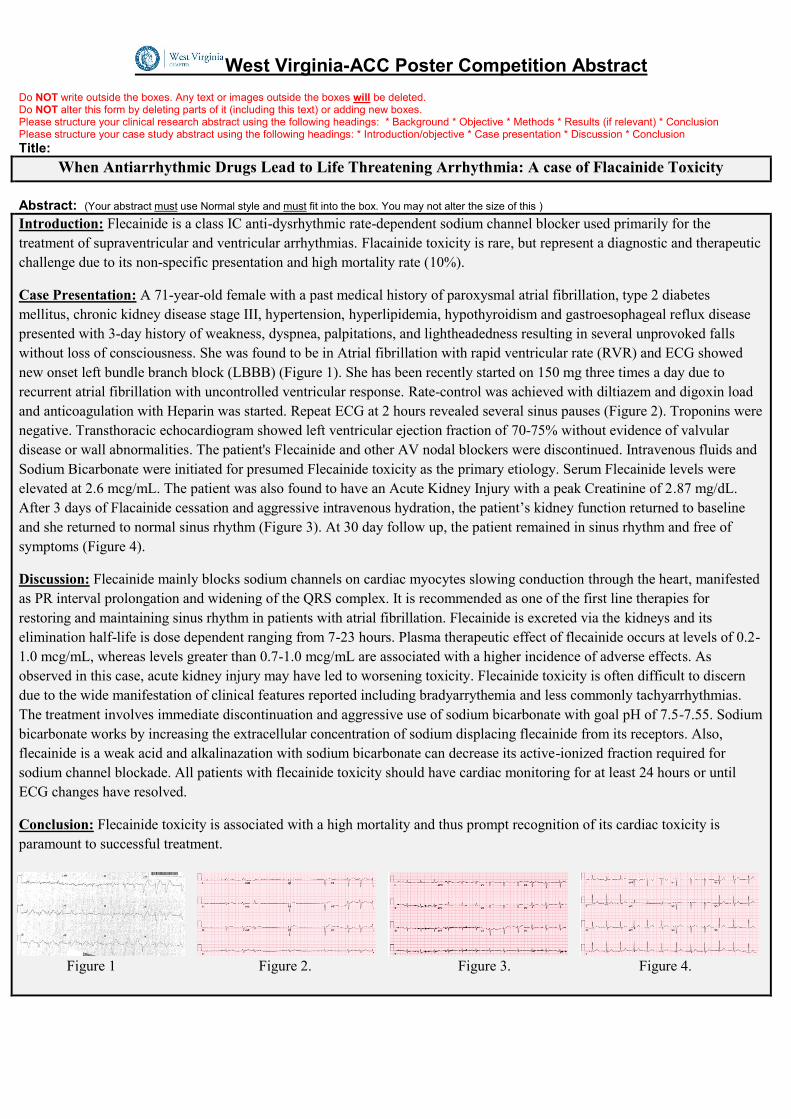
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
When Antiarrhythmic Drugs Lead to Life Threatening Arrhythmia: A case of Flacainide Toxicity
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Introduction: Flecainide is a class IC anti-dysrhythmic rate-dependent sodium channel blocker used primarily for thetreatment of supraventricular and ventricular arrhythmias. Flacainide toxicity is rare, but represent a diagnostic and therapeuticchallenge due to its non-specific presentation and high mortality rate (10%).
Case Presentation: A 71-year-old female with a past medical history of paroxysmal atrial fibrillation, type 2 diabetesmellitus, chronic kidney disease stage III, hypertension, hyperlipidemia, hypothyroidism and gastroesophageal reflux diseasepresented with 3-day history of weakness, dyspnea, palpitations, and lightheadedness resulting in several unprovoked fallswithout loss of consciousness. She was found to be in Atrial fibrillation with rapid ventricular rate (RVR) and ECG showednew onset left bundle branch block (LBBB) (Figure 1). She has been recently started on 150 mg three times a day due torecurrent atrial fibrillation with uncontrolled ventricular response. Rate-control was achieved with diltiazem and digoxin loadand anticoagulation with Heparin was started. Repeat ECG at 2 hours revealed several sinus pauses (Figure 2). Troponins werenegative. Transthoracic echocardiogram showed left ventricular ejection fraction of 70-75% without evidence of valvulardisease or wall abnormalities. The patient's Flecainide and other AV nodal blockers were discontinued. Intravenous fluids andSodium Bicarbonate were initiated for presumed Flecainide toxicity as the primary etiology. Serum Flecainide levels wereelevated at 2.6 mcg/mL. The patient was also found to have an Acute Kidney Injury with a peak Creatinine of 2.87 mg/dL.After 3 days of Flacainide cessation and aggressive intravenous hydration, the patient’s kidney function returned to baselineand she returned to normal sinus rhythm (Figure 3). At 30 day follow up, the patient remained in sinus rhythm and free ofsymptoms (Figure 4).
Discussion: Flecainide mainly blocks sodium channels on cardiac myocytes slowing conduction through the heart, manifestedas PR interval prolongation and widening of the QRS complex. It is recommended as one of the first line therapies forrestoring and maintaining sinus rhythm in patients with atrial fibrillation. Flecainide is excreted via the kidneys and itselimination half-life is dose dependent ranging from 7-23 hours. Plasma therapeutic effect of flecainide occurs at levels of 0.2-1.0 mcg/mL, whereas levels greater than 0.7-1.0 mcg/mL are associated with a higher incidence of adverse effects. Asobserved in this case, acute kidney injury may have led to worsening toxicity. Flecainide toxicity is often difficult to discerndue to the wide manifestation of clinical features reported including bradyarrythemia and less commonly tachyarrhythmias.The treatment involves immediate discontinuation and aggressive use of sodium bicarbonate with goal pH of 7.5-7.55. Sodiumbicarbonate works by increasing the extracellular concentration of sodium displacing flecainide from its receptors. Also,flecainide is a weak acid and alkalinazation with sodium bicarbonate can decrease its active-ionized fraction required forsodium channel blockade. All patients with flecainide toxicity should have cardiac monitoring for at least 24 hours or untilECG changes have resolved.
Conclusion: Flecainide toxicity is associated with a high mortality and thus prompt recognition of its cardiac toxicity isparamount to successful treatment.
Figure 1 Figure 2. Figure 3. Figure 4.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
When Antiarrhythmic Drugs Lead to Life Threatening Arrhythmia: A case of Flacainide Toxicity
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Introduction: Flecainide is a class IC anti-dysrhythmic rate-dependent sodium channel blocker used primarily for thetreatment of supraventricular and ventricular arrhythmias. Flacainide toxicity is rare, but represent a diagnostic and therapeuticchallenge due to its non-specific presentation and high mortality rate (10%).
Case Presentation: A 71-year-old female with a past medical history of paroxysmal atrial fibrillation, type 2 diabetesmellitus, chronic kidney disease stage III, hypertension, hyperlipidemia, hypothyroidism and gastroesophageal reflux diseasepresented with 3-day history of weakness, dyspnea, palpitations, and lightheadedness resulting in several unprovoked fallswithout loss of consciousness. She was found to be in Atrial fibrillation with rapid ventricular rate (RVR) and ECG showednew onset left bundle branch block (LBBB) (Figure 1). She has been recently started on 150 mg three times a day due torecurrent atrial fibrillation with uncontrolled ventricular response. Rate-control was achieved with diltiazem and digoxin loadand anticoagulation with Heparin was started. Repeat ECG at 2 hours revealed several sinus pauses (Figure 2). Troponins werenegative. Transthoracic echocardiogram showed left ventricular ejection fraction of 70-75% without evidence of valvulardisease or wall abnormalities. The patient's Flecainide and other AV nodal blockers were discontinued. Intravenous fluids andSodium Bicarbonate were initiated for presumed Flecainide toxicity as the primary etiology. Serum Flecainide levels wereelevated at 2.6 mcg/mL. The patient was also found to have an Acute Kidney Injury with a peak Creatinine of 2.87 mg/dL.After 3 days of Flacainide cessation and aggressive intravenous hydration, the patient’s kidney function returned to baselineand she returned to normal sinus rhythm (Figure 3). At 30 day follow up, the patient remained in sinus rhythm and free ofsymptoms (Figure 4).
Discussion: Flecainide mainly blocks sodium channels on cardiac myocytes slowing conduction through the heart, manifestedas PR interval prolongation and widening of the QRS complex. It is recommended as one of the first line therapies forrestoring and maintaining sinus rhythm in patients with atrial fibrillation. Flecainide is excreted via the kidneys and itselimination half-life is dose dependent ranging from 7-23 hours. Plasma therapeutic effect of flecainide occurs at levels of 0.2-1.0 mcg/mL, whereas levels greater than 0.7-1.0 mcg/mL are associated with a higher incidence of adverse effects. Asobserved in this case, acute kidney injury may have led to worsening toxicity. Flecainide toxicity is often difficult to discerndue to the wide manifestation of clinical features reported including bradyarrythemia and less commonly tachyarrhythmias.The treatment involves immediate discontinuation and aggressive use of sodium bicarbonate with goal pH of 7.5-7.55. Sodiumbicarbonate works by increasing the extracellular concentration of sodium displacing flecainide from its receptors. Also,flecainide is a weak acid and alkalinazation with sodium bicarbonate can decrease its active-ionized fraction required forsodium channel blockade. All patients with flecainide toxicity should have cardiac monitoring for at least 24 hours or untilECG changes have resolved.
Conclusion: Flecainide toxicity is associated with a high mortality and thus prompt recognition of its cardiac toxicity isparamount to successful treatment.
Figure 1 Figure 2. Figure 3. Figure 4.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:
When Antiarrhythmic Drugs Lead to Life Threatening Arrhythmia: A case of Flacainide Toxicity
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Introduction: Flecainide is a class IC anti-dysrhythmic rate-dependent sodium channel blocker used primarily for thetreatment of supraventricular and ventricular arrhythmias. Flacainide toxicity is rare, but represent a diagnostic and therapeuticchallenge due to its non-specific presentation and high mortality rate (10%).
Case Presentation: A 71-year-old female with a past medical history of paroxysmal atrial fibrillation, type 2 diabetesmellitus, chronic kidney disease stage III, hypertension, hyperlipidemia, hypothyroidism and gastroesophageal reflux diseasepresented with 3-day history of weakness, dyspnea, palpitations, and lightheadedness resulting in several unprovoked fallswithout loss of consciousness. She was found to be in Atrial fibrillation with rapid ventricular rate (RVR) and ECG showednew onset left bundle branch block (LBBB) (Figure 1). She has been recently started on 150 mg three times a day due torecurrent atrial fibrillation with uncontrolled ventricular response. Rate-control was achieved with diltiazem and digoxin loadand anticoagulation with Heparin was started. Repeat ECG at 2 hours revealed several sinus pauses (Figure 2). Troponins werenegative. Transthoracic echocardiogram showed left ventricular ejection fraction of 70-75% without evidence of valvulardisease or wall abnormalities. The patient's Flecainide and other AV nodal blockers were discontinued. Intravenous fluids andSodium Bicarbonate were initiated for presumed Flecainide toxicity as the primary etiology. Serum Flecainide levels wereelevated at 2.6 mcg/mL. The patient was also found to have an Acute Kidney Injury with a peak Creatinine of 2.87 mg/dL.After 3 days of Flacainide cessation and aggressive intravenous hydration, the patient’s kidney function returned to baselineand she returned to normal sinus rhythm (Figure 3). At 30 day follow up, the patient remained in sinus rhythm and free ofsymptoms (Figure 4).
Discussion: Flecainide mainly blocks sodium channels on cardiac myocytes slowing conduction through the heart, manifestedas PR interval prolongation and widening of the QRS complex. It is recommended as one of the first line therapies forrestoring and maintaining sinus rhythm in patients with atrial fibrillation. Flecainide is excreted via the kidneys and itselimination half-life is dose dependent ranging from 7-23 hours. Plasma therapeutic effect of flecainide occurs at levels of 0.2-1.0 mcg/mL, whereas levels greater than 0.7-1.0 mcg/mL are associated with a higher incidence of adverse effects. Asobserved in this case, acute kidney injury may have led to worsening toxicity. Flecainide toxicity is often difficult to discerndue to the wide manifestation of clinical features reported including bradyarrythemia and less commonly tachyarrhythmias.The treatment involves immediate discontinuation and aggressive use of sodium bicarbonate with goal pH of 7.5-7.55. Sodiumbicarbonate works by increasing the extracellular concentration of sodium displacing flecainide from its receptors. Also,flecainide is a weak acid and alkalinazation with sodium bicarbonate can decrease its active-ionized fraction required forsodium channel blockade. All patients with flecainide toxicity should have cardiac monitoring for at least 24 hours or untilECG changes have resolved.
Conclusion: Flecainide toxicity is associated with a high mortality and thus prompt recognition of its cardiac toxicity isparamount to successful treatment.
Figure 1 Figure 2. Figure 3. Figure 4.
West Virginia-ACC Poster Competition Abstract
Authors:
Zakeih Chaker MD, Fahad Alqahtani MD, Donald R Siddoway MD, Stephen Gnegy PA, Mohamad AdnanAlkhouli MD
C
Author to Receive Correspondence - Contact Information
Full Name: Chaker ZakeihLast First M.I.
Address: 1 Medical Center DriveStreet Address Apartment/Unit
#Morgantown WV 26505
City State ZIP CodeWork Phone: Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: WVU Internal Medicine Residency
_X__I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:A Pesky Bug Bite: Sarcoidosis Presenting with High Suspicion of Lyme Carditis
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Sarcoidosis is a multisystem granulomatous disease that most notably involves the lungs but can also significantly affect theheart among other extrapulmonary manifestations. Prompt suspicion and diagnosis of sarcoidosis induced cardiomyopathy isvital as common arrhythmias include complete heart block, ventricular tachycardia, and even sudden cardiac death. In thiscase, we present a patient with cardiac sarcoidosis initially presenting with suspicion of Lyme carditis due to her history ofpresent illness.A 34-year-old previously healthy woman presented to our emergency department with three episodes of dizziness withoutvertigo, tinnitus, and presyncope. Symptoms were associated with mild exertion such as walking up a flight of stairs and wereresolved after relaxing for about 10 minutes. She noted a heart rate of 32 beats per minute during her most recent episode,and described an engorged tick bite 2 months prior without developing rashes, fevers, myalgias, or arthralgias. Uponadmission, her initial EKG showed a 2:1 Mobitz type II AV block with transformation to a higher degree block on a successiveEKG. A chest radiograph and basic blood labs were unremarkable. Both the cardiology and infectious disease consultantswere concerned for early acute dissemintated Lyme disease, and a temporary transvenous pacemaker was placed.Parenteral ceftriaxone was started without resolution of arrhythmia. A transthoracic echocardiogram showed a pseudonormalleft ventricular filling pattern with abnormal relaxtion consistent with sarcoidosis or amyloidosis cardiomyopathy. The Lymeserology was negative and a CT scan of the chest showed revealed diffuse mediastinal, hilar, and paraesophagealadenopathy. Bronchoscopic biopsy showed non-necrotizing granulomatous inflammation confirming the diagnosis ofsarcoidosis.This case exemplifies the importance of evaluating a broad yet pertinent list of differential diagnoses especially when facingthe potential of fatal cardiac arrhythmias. Learning when to evaluate and treat less common pathologies fundamental to theart of medicine.
West Virginia-ACC Poster Competition Abstract
Authors:Peter Farjo MD; Sami Aljohani MD; Sameer Raina MD; Jason Moreland MD
C
Author to Receive Correspondence - Contact Information
Full Name: Farjo Peter DLast First M.I.
Address: 968 Northwestern Ave 5Street Address Apartment/Unit
#Morgantown WV 26505
City State ZIP CodeWork Phone: 7175864557 Alternate Phone: NA
E-mail Address: [email protected]
TrainingProgram: Categorical Internal Medicine at WVU School of Medicine
_X_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:3.4 CENTIMETER TRICUSPID VEGETATION IN A PATIENT PRESENTING WITHOUT FEVER OR LEUKOCYTOSIS ANDSUBSEQUENT RAPID DECOMPENSATION OF VALVULAR COMPETENCY
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )BACKGROUND: Appropriateness of surgical intervention in acute infectious tricuspid endocarditis is a controversial decisionearly in the course of infection. Surgical recommendations by the European Society of Cardiology revolve primarily aroundright sided heart failure, recurrent pulmonary emboli or failed treatment1. Even more restrictive recommendations are made bythe American Heart Association and American College of Cardiology2. Class IIB recommendations exist for earlier surgery,which may be inadequate given the high rates of mortality in vegetations sized greater than 10 mms2,3.
CASE: A 32 year old Caucasian male presented to the emergency department for dyspnea, cough and myalgias for six days.Past medical history was remarkable for intravenous drug abuse and pectus excavatum. At presentation, patient wastachycardic and tachypneic but afebrile. Laboratory results revealed profound thrombocytopenia but no leukocytosis orbandemia. CT angiography of the chest revealed cavitary pneumoniae in both lungs. Initial echocardiogram confirmed thediagnosis of tricuspid endocarditis with large vegetation measuring 3.2 by 2.3 cms upon the anterior leaflet and smallervegetation sized 1.5 by 0.9 cms attached to the valvular apparatus. Only mild tricuspid regurgitation was seen and leftventricular function was intact. Blood cultures confirmed methicillin sensitive Staphylococcus aureus bacteremia. It was agreedby infectious disease, cardiology, hospitalist and cardiothoracic surgery that medical management was appropriate. After 12days of appropriate antibiotic therapy, including 10 days of negative blood cultures, the patient developed large pulmonaryemboli and repeat echocardiogram confirmed fears that his tricuspid valve had become severely regurgitant and the largervegetation reduced by half, likely by embolization. Ejection fraction was now reduced to 45% with clinical findings consistentwith congestive heart failure. Patient was transferred to tertiary care facility for possible tricuspid valve replacement. To date,the patient remains intubated with plans for tracheostomy and possible valve replacement in the near future.
DISCUSSION: It is well established that prognosis in acute infective endocarditis is significantly worsened with vegetationssized greater than 10 mms, but the extent to which prognosis deteriorates with escalating size remains largely uncertain. Anincreasing number of cases appear in current literature with vegetations greater than 10 mms requiring emergent surgeriesbegging whether earlier surgical intervention would waylay such significant clinical deterioration3,4. Consideration for earlysurgery may be warranted in the setting of tricuspid vegetations with pulmonary emboli, heart failure and failure to eradicateinfection, a fact agreed upon by multiple professional societies 1,2. Even without these complications, however, early surgicalintervention may be important in large vegetations given the higher risk of these events.
CONCLUSION: Early surgery has been successful in patients with persistent infection and even ongoing intravenous drugabuse and perhaps should be considered more frequently, making surgical risk possibly less than risk of embolism andvalvular destruction 5,6,7. Ultimately the decision for early surgery must be based on clinical situation and should be based uponshared decision making between the cardiothoracic surgeon, cardiologist, and patient.
REFERENCES:1. The Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of
Cardiology. Guideline on the prevention, diagnosis, and treatment of infective endocarditis. European Heart Journal.2009;30:2369-2413. DOI:0.1093/eurheartj/ehp285.
2. Bach D. Timing of Surgery in Infective Endocarditis [Internet]. American College of Cardiology Foundation; 2016 January 8[cited 2017 February 18]. Available from: http://www.acc.org/latest-in-cardiology/ten-points-to-remember/2016/01/08/15/13/timing-of-surgery-in-infective-endocarditis/.
3. Leitman M, Dreznik Y, Tyomkin V, Fuchs T, Krakover R, Vered Z. Vegetation size in patients with infectiveendocarditis. European Journal Echocardiography. 2012;13(4):330-338.
4. Morokuma H, Minato N, Kamohara K, Minematsu N. Three Surgical Cases of Isolated Tricuspid Valve InfectiveEndocarditis. Ann Thorac Cardiovasc Surg. 2009 February 26;16(2):134-138.
5. Weymann A, Borst T, Popov A, Sabashnikov A, Bowles C, Schmack B, Veres G, Chaimow N, Simon AR, Karck M, SzaboG. Surgical treatment of infective endocarditis in active intravenous drug users: A justified procedure? Journal ofCardiothoracic Surgery. 2014 March 24;58(9). DOI:10.1186/1749-8090-9-58.
6. Furat C, Ilhan G, Bayar E, Ozpak B, Kara H, Yilmaz M. Isolated tricuspid valve infective endocarditis in young drugabusers. Therapeutic advances in cardiovascular disease. 2014;8(3):119-122.
7. Kang D, Kim Y, Kim S, Sun B, Kim D, Yun S, Song J, Choo S, Chung C, Song J, Lee, J, Sohn D. Early Surgery versusConventional Treatment for Infective Endocarditis. New England Journal of Medicine. 2012 June 28;366:2466-2473.
West Virginia-ACC Poster Competition Abstract
Authors:
Megan Hawkins, DO; Stanley Pamfilis, MD, FACC
C
Author to Receive Correspondence - Contact Information
Full Name: Hawkins Megan ELast First M.I.
Address: 822 Clifton StreetStreet Address Apartment/Unit
#Marietta OH 45750
City State ZIP CodeWork Phone: 405-209-5710 Alternate Phone: 304-424-2777
E-mail Address: [email protected]
TrainingProgram: Camden Clark Medical Center
_MH__I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Treatment of a Cardiac Arrhythmias with Electrical Cardioversion in Pregnancy
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Introduction
Physiological changes in pregnancy can result in tachyarrhythmia’s in previously asymptomatic WPWpatients. Sustained symptomatic arrhythmias can result in hemodynamic compromise in mother and fetus,therefore rapid intervention is crucial as in non-pregnant population. Electrical cardioversion (ECV) is utilized inlife-threatening situations when the patient is hemodynamically unstable. Literature review indicates there is nolarge-scale studies concerning the safety and efficacy of ECV in pregnant populations. This case report describesthe effective use of ECV during pregnancy.
Case presentation
A 26 y/o white female G1P0 at 33 weeks of gestation with past medical history significant forasymptomatic WPW syndrome. She presented with sudden onset of shortness of breath, sustained palpitations,dizziness and chest tightness. Her heart rate was 180-220 and blood pressure was 84/60mmHg with MAP of68mmhg. On physical examination, gravid uterus above umbilicus was noted. Initial serial EKGs showed widecomplex irregular tachyarrhythmia and A-fib with RVR. Her laboratory work up was normal. She was evaluated bya team of Cardiology, OB/GYN and Electrophysiologist. She underwent cardioversion with synchronized 150J DCshock under sedation without maternal or fetal complications. Post procedure EKG showed sinus rhythm withheart rate of 90, short PR interval and delta wave. She was admitted for observation overnight and she wasstarted on flecainide 50mg daily to prevent further tachyarrhythmias. On the following day, she was dischargedwithout additional sequalae with plans for post-partum ablation.
Discussion
WPW syndrome was first described by Wolf, Parkinson and White in 1930. It is a preexcitation syndromedue to anomalous pathway bypassing AV node. The overall incidence of arrhythmia resulting in WPW syndrome isreported up to 1% per year. However, the exact incidence of tachyarrhythmia’s in pregnant WPW syndromepatients is unknown. In 1961, Gleicher et al suggested that pregnancy may facilitate onset of tachyarrhythmias inpatients with asymptomatic preexcitation syndrome. Tachyarrhythmias in pregnancy can result in hemodynamiccompromise of fetus causing hydrops fetalis. It is also reported to cause premature delivery and intrauterinegrowth restriction. Therefore, rapid conversion to sinus rhythm is crucial for wellbeing of both mother and fetus.Trials of medical cardioversion were reported unsuccessful in the past and given the special circumstances in ourcase where the patient’s blood pressure was borderline low, a rapid management with electrical cardioversionunder sedation was considered.
Conclusion
Pregnancy predisposes tachyarrhythmias in previously asymptomatic WPW syndrome patients, andelectrical cardioversion can be considered safe and effective treatment.
West Virginia-ACC Poster Competition Abstract
Authors:
Hisham Hirzallah MD, Mial Bilal Alam MD, Ashwini Mallad MD, Rameez Sayyed MD
C
Author to Receive Correspondence - Contact Information
Full Name: Hirzallah Hisham Moh’d.HLast First M.I.
Address: 936 12th AVE 6Street Address Apartment/Unit
#Huntington WV 25701
City State ZIP CodeWork Phone: 304-942-1220 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: Marshall University, school of medicine
_HH__I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Seizure Like Activity and Recurrent Cardiac Arrests in a healthy 24-year-old. Loperamide abuse: A Case Report and LiteratureReview.Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction: Loperamide is a widely available over the counter (OTC) anti-motility agent. At recommended dose, it isrelatively safe in adults. However, at higher doses it can produce palliation for opiate withdrawal symptoms or even frankeuphoria, lending to its abuse potential and occasionally fatal cardiac dysrhythmia. We present an atypical case of loperamidetoxicity with seizure like activity and recurrent cardiac arrests, treated successfully with Isoproterenol.
Case Presentation: 24-year-old female with history of non-intravenous drug use transferred for seizure like activity. Herhospital stay was complicated with recurrent cardiac arrests, including first as pulseless electrical activity (n=1) andsubsequently with ventricular tachycardia (n=2). Patient was successfully resuscitated with standard ACLS protocol from eacharrest episodes (requiring one to two cycles of CPR). There was no evidence of neurological injury or prolonged mechanicalventilation requirement after each episode. Admission electrocardiogram (EKG) was remarkable for prolonged QTc at 645milliseconds. Blood work was unremarkable for any significant electrolyte imbalances and elevation of cardiac enzymes.Neurologic workup included negative CT brain, video electroencephalogram (EEG), and lumbar puncture. Cardiac CTangiography confirmed normal cardiac and coronary anatomy and transthoracic echocardiogram revealed normal structureand function. On detailed medication questionnaire, patient endorsed the use of loperamide (approximately 40-80 tablets aday) for opiate withdrawal palliation. In addition to aggressive electrolyte replacement, trial of IV Isoproterenol achievednormalization of QTc after three days. Considering stability of EKG over next few days, electrophysiology ruled out the needfor implantable cardiac defibrillator (ICD). Patient was extensively counseled on cessation of loperamide abuse and wasdischarged home.
Discussion: A food and drug administration (FDA) post-marketing surveillance study showed that the loperamide abuse is onthe rise with most intentional overdoses occurring after 2010. With opioid abuse reaching its epidemic level, the crux ofloperamide abuse is in the ever growing populous of addicted individuals seeking ways to self-medicate against opioidwithdrawal or to find the next high cheaply and without a prescription. Loperamide is a -opioid receptor agonist with poor oralbioavailability, limited GI absorption, and is metabolized by the liver. At super high doses, the drug is actively transportedthrough the blood brain barrier via an efflux transporter. Adverse effects include syncope, QT prolongation, ventriculararrhythmias, cardiac arrest, and death. While most commonly abused to for euphoria or withdrawal, our review of literatureidentified one case of a patient self-medicating irritable bowel syndrome and one older male using it for weight-gain. Ourpatient reported one year history of loperamide abuse taking 80-160 mg daily (10x daily recommended dose). She admitted toa previous ICU admission requiring intubation for a suicide attempt with loperamide, having taken over 400 mg. She wastreated successfully with isoproterenol infusion making it the second case reported, although, the optimal treatment strategy isnot well defined. Isolated case reports mention ICD implantation for recurrent cardiac arrests and cardiomyopathy with mixedresults. This, however, is high risk for concurrent IV drug use and concern of device infection. Furthermore, even in cases ofdocumented systolic dysfunction, abstinence from the offending agent resulted in return of normal systolic function – furtherlimiting indication for permanent ICD. The pro-arrhythmic mechanisms of loperamide induced dysrhythmia has been studiedusing cloned human cardiac sodium and potassium channels. Loperamide inhibits both the Nav1.5 sodium channel andespecially the human ether-a-go-go-related gene potassium channel. This study attributed the QRS prolongation to theinhibition of the sodium channel and further devolution into Torsades to the potassium channel inhibition.
Conclusion: Loperamide is a -opioid receptor agonist that is increasingly abused for treatment of opioid withdrawal andeuphoria. Because it is available without prescription, is not routinely tested for, and does not have a classic clinicalpresentation, diagnosis of loperamide overdose is difficult requiring heightened clinical suspicion. Despite an FDA warning,loperamide abuse is on the rise. Therefore, general population and clinicians should be more aware and attuned to thepotential of cardiac toxicity, QTc prolongation, and death from loperamide abuse. Further studies need to be done focused onelucidating optimal treatment strategies and improved initial diagnostics.
West Virginia-ACC Poster Competition Abstract
Authors:Abhinav Mittal, MD; Rahul Sangani, MD; Monica Cerone, MD; Robert Stansbury, MD
C
Author to Receive Correspondence - Contact Information
Full Name: Mittal, MD AbhinavLast First M.I.
Address: 139 Birds Eye View Dr.Street Address Apartment/Unit
#Morgantown WV 26501
City State ZIP CodeWork Phone: 304-598-4850 Alternate Phone: 724-413-5681
E-mail Address: [email protected]
TrainingProgram: West Virginia University, Department of Internal Medicine
_x_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Third degree atrioventricular block followed by syncope, labile blood pressure and orthostatic hypotension in patient withhistory of nasopharyngeal cancer: Baroreflex failure
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )Introduction:Baroreflex failure is an uncommon cause of syncope and labile blood pressures, but it can happen after neck radiation,cerebrovascular event, or post-surgical procedures involving the brainstem nuclei. It is challenging to diagnosis baroreflexfailure as most of the symptoms are similar to those of autonomic failure. Carotid sinus injury is the most common cause ofbaroreflex failure, but radiation related damage in the neck area can also lead to baroreflex failure. Here we are presenting acase of Baroreflex failure in a patient with history of nasopharyngeal cancer, status post neck radiation.Case Description:75-year-old man with past medical history of High blood pressure, hypothyroidism, diabetes, and nasopharyngeal cancerpresenting from an outside facility with complaints of symptoms including nausea, vomiting, syncope and was subsequentlyfound to have severe bradycardia with a third degree atrioventricular (AV) nodal block. He was given atropine and started on adopamine infusion. He was taking verapamil at home for his blood pressure and it was discontinued here due to AV block.The Electrophysiology team agreed with this and suggested that the 3rd degree AV block was due to Verapamil. A 30-dayevent monitor was ordered upon discharge with possible pacemaker placement in the future if the block continues. Hisbradycardia resolved after this, but the patient was noted to have labile blood pressure with systolic blood pressure rangingfrom 70 to 220 without medications. The patient was complaining about a headache, increased urination frequency andurgency with high blood pressure. He was started on tamsulosin but became hypotensive, so all of his anti-hypertensivemedications were discontinued. Even with this intervention, the patient continued to have episodes of labile blood pressure. Allof his laboratory tests and images results for labile blood pressure work up were negative here. The patient has a history ofnasopharyngeal cancer with radiation treatment. It was determined that his labile blood pressure was a result of baroreflexfailure secondary to radiation exposure. He was started on clonidine and was discharged with an event monitor. He was thenscheduled for a cardiology clinic follow up. During his follow up appointment, patient hadDiscussion:Baroreflex failure is a diagnosis of exclusion and based on clinical presentation, past medical history and labs results that failto identify an alternative diagnosis. There are many experimental methods which include vasoactive drugs, neck chambertechniques, and Valsalva manoeuvre which can be helpful to measure the baroreflex. Most of these are experimentaltechniques only. The patient with baroreflex failure can be managed conservatively with non-pharmacological methods suchas frequent blood pressure measurements, timed carbohydrate ingestion, measuring oral fluid intake, caffeine ingestion, andphysical exercises. Pharmacological treatment such as clonidine, a centrally acting alpha-2 agonist, has been shown todecrease the onset of hypertensive crisis and tachycardia by 81%. Fludrocortisone can help with orthostatic hypotension; lowdose benzodiazepines can help with suppressing sympathetic input.Conclusion:The patient with new episodes of labile blood pressure, syncope, and orthostatic blood pressure with normal laboratory testingand negative image findings may have baroreflex failure, especially in the setting of a history of carotid sinus injury or neckradiation. The Patient with baroreflex failure can benefit from frequent monitoring of blood pressure and centrally acting alpha2 agonists, such as clonidine. Baroreflex failure does not require any invasive intervention to control the symptoms.
West Virginia-ACC Poster Competition Abstract
Authors:
Kinjan P Patel MD, Hama Amin Ali MD, Lina Jacques MD, Abnash Jain MD
C
Author to Receive Correspondence - Contact Information
Full Name: Patel Kinjan PLast First M.I.
Address: 5203 Chestnut hill apartment 5203Street Address Apartment/Unit
#Morgantown WV 26505
City State ZIP CodeWork Phone: 2245724242 Alternate Phone: 8473388534
E-mail Address: [email protected]
TrainingProgram: WVU-Internal Medicine Program
__X_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Focal myocarditis presenting as Inferior wall STEMI
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Introduction: The leading cause of ST segment elevation is ST elevation myocardial infarction (STEMI), which is considered an emergency.However, Identification of mimickers, such as myocarditis, are vital as treatment differ in such cases. We are presenting a case of STelevation MI, initially thought to be STEMI, but later diagnosed as myocarditis.
Case report: A 19 years old gentleman no significant PMH presented to the ED with 1 hour of substernal 10/10 chest pain withoutradiation and no associated symptoms. Troponin at presentation was 64,759 (range 0 - 30 ng/L) and EKG showed ST elevation in inferiorleads with reciprocal changes, consistent with an inferior STEMI. . Urine drug screen was negative during admission exceptbenzodiazepine. Given these findings, the patient was taken to the Cath lab immediately, which revealed no evidence of CAD and an EF of~ 40%. The patient's chest pain resolved by the following morning, but ST elevation in inferior leads persisted and troponins continued torise for the next 2 days. Troponins peaked at 300,133. A TTE revealed mild diffuse hypokinesis, mild reduction in systolic function with anEF of 40-45% and normal diastolic function. Due to the focal changes on EKG with persistent ST elevations but no focal findings on LHC, aDx of acute myopericarditis was considered more likely than STEMI in this patient. Further history revealed that his mother had a similarchest pain and elevated biomarkers episode when she was in her early 20's, but she did not know her diagnosis at that time. The patientalso endorsed having a non-specific viral-type illness the week before. His major symptoms were generalized myalgia, weakness, lowgrade fever and fatigue. A CMR showed increased contrast in the sub-endocardium consistent with myocarditis. Patient was dischargedon ASA and metoprolol. Later, a follow up visit, patient revealed that he might have used cocaine prior to the event.
Discussion:
Myocarditis is an inflammatory condition mainly located in the myocardium. (1)(2)
Myocarditis prevalence and occurrence varies. There is no accurate data available for incidence and prevalenceavailable worldwide. In Australia, prevalence rate is 12% of young adults presenting with sudden death. In Japan, incidenceis around 0.11%. Nevertheless, Incidence of non-fatal myocarditis is likely higher than diagnosed, mostly due to thechallenges of establishing the diagnosis in standard clinical settings. (3)(4)(5).
The challenge involving of Myocarditis arises from etiology, clinical manifestation, establishing diagnosis andtreatment. Causes of myocarditis are numerous. Infectious such as viral. Systemic disorders such s cardiotoxic agents a suchas alcohol or cocaine. Pharmaceutical drugs such as lithium and vaccination have also been implicated. (1)(6). Clinicalmanifestation is heterogeneous, ranging from asymptomatic ECG abnormalities to cardiogenic shock with nonspecificsymptoms such as chest pain, dyspnea and palpitation often associated with prodromal flu like symptoms (6). Cardiac testssuch as ECG, troponin is nonspecific nor sensitive. ST elevation and elevated troponin have numerous causes ranging fromcardiac causes ranging such as cardiac contusion, aortic dissection to noncardiac causes such as pulmonary embolism andsepsis. (16-17) (18-19). The gold standard for diagnosis of myocarditis but routine biopsy not indicated in most cases (7).
Using Lake Louise CMR criteria for diagnosis clinically suspected myocarditis can help distinguishing ischemicfrom nonischemic cardiomyopathy. In suspected acute myocardial criteria, CMR diagnostic performance has sensitivity,81%; specificity, 71%; PPV, 90 %; NPV 55 %; and accuracy, 79% (9)
While PCI is most likely indicated, administration of TPA is likely detrimental in myocarditis cases. Hence physicianshould be aware of causes of ST-elevation with and without elevated troponin levels. It also guides the physician to initiatethe appropriate treatment including steroids, immunosuppressive therapy or IVIG when appropriate. (5)
West Virginia-ACC Poster Competition Abstract
Authors:Faisal Radwi, MDFahad Al-Qahtani, MDSameer Raina, MD
C
Author to Receive Correspondence - Contact Information
Full Name: Radwi FaisalLast First M.I.
Address: 108 suncrest terraceStreet Address Apartment/Unit
#Morgantown WV 26505
City State ZIP CodeWork Phone: 681-2143099 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: West Virginia University Internal Medicine Program.
_X__I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.
West Virginia-ACC Poster Competition AbstractDo NOT write outside the boxes. Any text or images outside the boxes will be deleted.Do NOT alter this form by deleting parts of it (including this text) or adding new boxes.Please structure your clinical research abstract using the following headings: * Background * Objective * Methods * Results (if relevant) * ConclusionPlease structure your case study abstract using the following headings: * Introduction/objective * Case presentation * Discussion * ConclusionTitle:Pericardial Cyst
Abstract: (Your abstract must use Normal style and must fit into the box. You may not alter the size of this )
Introduction:Pericardial cysts are considered to be a rare congenital abnormality with an estimated incidence of 1:100,000. We arereporting a case of a 58-year-old female with chest pain and non-productive cough, who was initially diagnosed withpericarditis and found to have a pericardial cyst.
Case presentation:A 58-year-old non-smoking female presented to the clinic with new onset very severe, non-exertional, retrosternal, stabbingchest pain, radiating to the back. It was associated with dry cough and intermittent lightheadedness. She denied anypalpitation, shortness of breath, diaphoresis, recent sick contacts or viral illness. Past medical, surgical history, and familyhistory were not significant. She denied neither smoker nor alcoholic. Vital signs on presentation were within normal limits.On exam; she was alert and oriented, no JVD or lower limb edema. Heart sounds were normal with regular rate, no murmur,but a mid-sternal pericardial friction rub was heard with the patient in the supine position. Lungs were clear bilaterally with nochest wall tenderness. EKG revealed normal sinus rhythm with a mild depressed PR interval in lead II and aVF. CompleteBlood Count (CBC) and Basic Metabolic Panel (BMP) were within normal limits. Troponins were negative. Therefore,Pulmonary embolism was entertained. D-dimer (0.613 ug/ml) and CRP (7.68 mg/l). Chest x ray was normal. ComputedTomography (CT) chest with intravenous contrast showed a (7.0 cm) right pericardiophrenic cyst and no evidence of apulmonary embolus. Echocardiography confirmed the diagnosis and revealed normal LV function and mild tricuspidregurgitation without evidence of pericardial effusion. Patient was evaluated by a thoracic surgeon and recommended tofollow up as outpatient. Patient’s pain dramatically improved on Ibuprofen.
Discussion:Pericardial cysts are rare benign congenital abnormalities that can be asymptomatic or present with dyspnea, chest pain,pericarditis, and hemorrhage into cyst, pericardial tamponade, atrial fibrillation, or a dry cough. Physicians should be awarethat these cysts, although probably present since birth, can be a cause of non-ischemic chest pain so that appropriate treatmentis initiated. Diagnosis of pericardial cyst requires obtaining Chest X-ray, Echocardiography and CT or MRI. A simple bedsideechocardiography can recognize the location of the cyst. Moreover, it helps to differentiating a mass from a cyst. Patient withpericardial cyst can be asymptomatic therefore; regular follow up and monitoring for possible symptoms should be done.However, for symptomatic patient treatment options include surgical removal, Video assisted thoracic surgery, orpercutaneous echocardiography guided aspiration.
Conclusion:We are presenting this case to alerts the practicing emergency medicine, internal medicine, and cardiologist physicians toconsider Pericardial cysts as one of the differential diagnosis of chest pain after excluding other common causes.
West Virginia-ACC Poster Competition Abstract
Authors:
Tashani, Mohamed, MD. Megri, Mohammed, MD. Karem, Emhemmid S, MD. Saunders, Elizabeth, MD
C
Author to Receive Correspondence - Contact Information
Full Name: Tashani MohamedLast First M.I.
Address: 21 Pyramid drive 519Street Address Apartment/Unit
#Huntington WV 25705
City State ZIP CodeWork Phone: 3046911086 Alternate Phone:
E-mail Address: [email protected]
TrainingProgram: Joan C. Edwards School of Medicine at Marshall University
__X_I understand that submission of an abstract constitutes a commitment to be present at the West Virginia-ACC AnnualMeeting. I understand that if I cannot be present that my poster will be withdrawn.





![VIRGINIA VIRGINIA ATHLETICS MEDIA RELATIONS 295 ......VIRGINIA 2017-18 SCHEDULE/RESULTS 19-1, 8-0 ACC DateOpponent past five seasons. TV Time/Result Nov. 10 [RV/RV] UNC GREENSBORO](https://img.pdfslide.net/doc/110x75/6043647c02d23659df0f1a6f/virginia-virginia-athletics-media-relations-295-virginia-2017-18-scheduleresults.jpg)











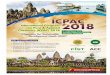
![2017-18 UNIVERSITY OF VIRGINIA MEN’S BASKETBALL • GAME …€¦ · VIRGINIA 2017-18 SCHEDULE/RESULTS 27-2, 16-1 ACC DateOpponent TV Time/Result Nov. 10 [RV/RV] UNC GREENSBORO](https://img.pdfslide.net/doc/110x75/605de35ff2e03627285f0087/2017-18-university-of-virginia-menas-basketball-a-game-virginia-2017-18-scheduleresults.jpg)







![Stratford University Tuition information poster [bs ba & bs acc]](https://img.pdfslide.net/doc/110x75/589bb2f01a28ab1d748b5fbf/stratford-university-tuition-information-poster-bs-ba-bs-acc.jpg)
