-
What do we know about RAVs today
Francesca Ceccherini-SilbersteinUniversità degli Studi di Roma
“Tor Vergata”
Cattedra di Virologia
Disclosures: Advisory/Consulting/Conferences/Grants: Gilead,
BMS, AbbVie, Roche Diagnostics, MSD, BMS, Janssen, Abbott
Molecular, ViiV
-
RASsResistance associatedsubstitutions
RAVsResistance associated variants
Pawlotsky JM, Gastroenterology 2016 and EASL 2016
-
1991 20010
20
40
60
80
100
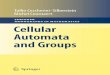
8-12
SV
R (%
)
15-20
38-43
25-30
50-60
1995 1998
Standard interferon (6 mos)[1]
Standardinterferon
(12-18 mos)[2,3]
Interferon/ribavirin
(6-12 mos)[3,4] PegIFNmonotherapy(6-12 mos)[5,6]
PegIFN/ribavirin(6-12 mos)[6,7]
2011-2013
70-80
PI + PegIFN/RBV(6-12 mos)[8-18]
1. Carithers RL Jr., et al. Hepatology. 1997;26(3 suppl
1):83S-88S. 2. Zeuzem S, et al. N Engl J Med. 2000;343:1666-1672.
3. Poynard T, et al. Lancet. 1998;352:1426-1432. 4. McHutchison JG,
et al. N Engl J Med. 1998;339:1485-1492. 5. Lindsay KL, et al.
Hepatology. 2001;34:395-403. 6. FriedMW, et al. N Engl J Med.
2002;347:975-982. 7. Manns MP, et al. Lancet. 2001;358:958-965. 8.
Poordad F, et al. N Engl J Med. 2011;364:1195-1206. 9. Jacobson IM,
et al. N Engl J Med. 2011;364:2405-2416. 10. Sherman KE, et al. N
Engl J Med. 2011;365:1014-1024. 11. Jacobson IM, et al.64th Annual
Meeting of the American Association for the Study of Liver
Diseases, 1-5 November 2013, Washington, DC. 12. Zeuzem S, et al.
Gastroeneterology 2014;146:430-41. 13. Lawitz E, et al.
Gastroenterology 2013;144:S-151. 14. Jensen D, et al. 64th Annual
Meeting of the AmericanAssociation for the Study of Liver Diseases,
1-5 November 2013, Washington, DC. 15. Jacobson I, et al. 64th
Annual Meeting of the American Association for the Study of Liver
Diseases, 1-5 November 2013, Washington, DC. 16. Marcellin P, et
al. Gastroenterology 2013;145:790-800e3. 17.Bronowicki JP, et al.
Antiviral Ther 2013;18:885-93. 18. Manns MP, et al. Hepatology
2012;56:884-93. 19. Hezode C, et al. Hepatology 2012;56:553A- 4A.
20. Dore G, et al. J Hepatol 2013;58:S570-1. 21. Lawitz E, et al.
Lancet Infect Dis 2013;13:401-8. 22. Kowdley KV, et al.
Lancet2013;381:2100-7. 23. Lawitz E, et al. 64th Annual Meeting of
the American Association for the Study of Liver Diseases.
Washington, DC, 1-5 November 2013. 24. Lawitz E, et al. N Engl J
Med 2013;368:1878-87. 25. Jacobson IM, et al. N Engl J Med
2013;368:1867-77. 26. Zeuzem S, et al. NEngl J Med
2014;370:1993-2001. 27. Osinusi A, et al. JAMA 2013;310:804-11. 28.
Jacobson IM, et al. 64th Annual Meeting of the American Association
for the Study of Liver Diseases. Washington, DC, 1-5 November 2013.
29. Sulkowski MS, et al. N Engl J Med 2014;370:211-21. 30. Zeuzem
S,et al. N Engl J Med 2014;370:1889-9. 31. Afdhal N, et al. N Engl
J Med 2014;370:1483-9. 32. Feld JJ, et al. N Engl J Med
2014;370:1594-603. 33. Zeuzem S, et al. N Engl J Med
2014;370:1604-14. 34. Ferenci P, et al. N Engl J Med
2014;370:1983-9. 35. Poordad F, et al. N Engl J
Med2014;370:1973-82. 36. Lawitz E, et al. 64th Annual Meeting of
the American Association for the Study of Liver Diseases,
Washington, DC, 1-5 November 2013. 37. Gane EJ, et al.
Gastroenterology 2014;146:736-43e1.
IFN-free DAA +/- RBV(3-6 mos) [24-37]
2012-2014
83-9689-100
1 DAA +PegIFN/RBV
(3-6-12 mos) [19-24]
1989HCV
identified
1992HCV
Blood Test
2005HCV in-vitro
Culture
1999HCV
Replicon
1974Mystery
virus
Changes in standard of care for HCV, and improvements in numbers
of sustained virological responses
-
hivforum.org
31%–33% nucleotide difference among the 7 known HCVgenotypes and
20%–25% among the nearly 67 HCV subtypes(Smith et al., 2014).
HCV genetic variability is higher than HIV’s and HBV’s
-
0% 25%Amino acid variability:
47% amino acids of HCV PROTEASE NS3 are conserved
among all HCV-genotypes
55% amino acids of HCVPOLYMERASE NS5B are conserved
among all HCV-genotypes
0% 25%Amino acid variability:
46% amino acids of HCVNS5A are conserved
among all HCV-genotypes
Cento et al., PLoS ONE 2012 Love et al., J Vir 2009 Di Maio et
al., AAC 2014
Today only few DAAs are pangenotypic…….
What about today in the era of new DAAs?Still genotype important
predictor for response?
(Grazoprevir) Daclatasvir Sofosbusvir
-
FROM CURRENT STATUS TO OPTIMIZATION OF HCV TREATMENT:
RECOMMENDATIONS FROM AN EXPERT PANEL
Craxi` A*, Perno CF*, Vigano` M, Ceccherini-Silberstein F, Petta
S, and The AdHoc (Advancing Hepatitis C for the Optimization of
Cure) Working Party: AlbertiA, Aghemo A, Andreone P, Andreoni M,
Bonora S, Brunetto MR, Bruno S, Caporaso N, Chirianni A, Ciancio A,
Degasperi E, Di PerriG, Fagiuoli S, Gaeta GB, Ferrari C, Pellicelli
A, Puoti M, Raimondo G, Taliani G, Villa E , Zignego AL Submitted
2016
HCV genotype dictates the choice of anti-HCV drugs
and can modulate the duration of treatment in infected
patients
with chronic hepatitis C
-
HIV versus HCVBaseline resistance testing
• HIV treatment failure expected at
-
First documentation of a transmission of an HCV DAA resistant
variant from a DAA treated patient to his sexual HIV-infected
partner
Patient A, a man chronically infected with HCV genotype 1a and
co-infected with HIV- 1, treated with pegIFN/RBV plus telaprevir in
July2012 with HCV breakthrough. HCV NS3 protease sequences
beforetreatment with telaprevir did not have anymajor substitution
associated with NS3 PIs.
Patient B, a man also HIV-1 infected and sexual partner of
patient A, diagnosed of acute HCV co-infection in January 2011,
with HCV genotype 1a. This patient refused therapy with pegIFN/RBV
during the acute phase of HCV infection.In April 2012 he entered a
clinical HCV trial and was treated for 24 weeks with pegIFN/RBV
plus Daclatasvir, with undetectable HCV RNA at week 24 and 36 after
the end of treatment. However, at week 48 after stopping therapy,
presented elevated transaminase and detectable HCV RNA, suggesting
a HCV re-infection. The patient denied any known riskfor HCV
infection except unprotected sexualintercourse with his partner
(patient A).After 12 weeks, patient B tested negative for HCV
infection.
108 and 28 individualNS3 protease clonesfrom patient A and B
early samples, respectively, weresequenced
Franco et al Gastroenterology May 2014
V36M substitution detectedin 9/20 clones in patient A (20 weeks
off therapy) and in all late sequencesfrom patient B.
-
Virological issues in the DAAs EraAfter treatment failure:
useful / recommended the
resistance test?
[…] Currently, there is no data to firmly supportretreatment
recommendations, which must be based onindirect evidence (HCV
genotype, known resistanceprofiles of the administered drugs,
number of drugs used,use of ribavirin, treatment duration). Whether
assessing thesequence of the target HCV genes (HCV resistance
testing)prior to retreatment is helpful to make a decision
remainsunknown, as well as which therapeutic decision should bemade
based on this result.
For patients with cirrhosis or other patients who
requireretreatment urgently, testing for RAVs that conferdecreased
susceptibility to NS3 protease inhibitors (eg,Q80K) and to NS5A
inhibitors should be performed usingcommercially available assays
prior to selecting the nextHCV treatment regimen.
-
Update of December 11, 2015
-
Role of RAVs after treatment failure to DAAs
FROM CURRENT STATUS TO OPTIMIZATION OF HCV TREATMENT:
RECOMMENDATIONS FROM AN EXPERT PANEL Craxi` A, et al Subitted
2016
Statements• Baseline resistance testing for RAVs before first
course with DAAs has limited clinical utility, unless if
recommended by specific drug labels.• In case of baseline presence
of NS5A RAVs or Q80K, the search of other baseline NS3 andNS5a RAVs
might be useful to personalize therapy, and should encourage the
use of at least2 active DAAs without resistance and/or longer
treatment duration and/or the addition ofRbv.• Resistance testing
after treatment failure in all 3 genes (NS3, NS5A, NS5B [for the
twodifferent classes of nucleoside and non- nucleoside inhibitors]
independently of the failure regimen) is strongly recommended in
order to optimize retreatment strategy*.• HCV sequencing can be
based on Sanger population method and should also confirm
theprevious genotype and subtype assignment.• According to
resistance results, current re-treatment strategies for patients
failing a firstcourse with DAAs should include at least 2 active
drug classes, with a preferential use ofone drug with high genetic
barrier to resistance, and with extended treatment durationsand
addition of Rbv, otherwise waiting for better future options.• If a
deferred treatment has been considered, and in case of presence of
RAVs at failure, inorder to assist the therapeutic choice when
starting a re-treatment, HCV sequencing shouldbe repeated (only in
the gene with previous RAVs) and should be better based on
deepsequencing.* NOTE: It would be desirable to preserve a sample
before starting treatment with DAA, because in case of failure and
presence of RAVs, the study of the baseline sample may help to
distinguish if the resistance occurred during failure or it was
already present as natural resistance before treatment. This
information may help to set to the best the next regimen.
-
Hepatitis C Virus Resistance to Direct-Acting Antiviral Drugs in
Interferon-Free Regimens
Pawlotsky JM: Gastroenterology 2016
-
Should we be worried about baseline RAVs?SVR rates to NS3
protease inhibitorplus NS5A inhibitor combinationregimens in HCV
genotype 1infected patients according to thepresence of baseline
RAVs.
SVR rates for NS3 protease inhibitorplus nucleos(t)ide NS5B
inhibitorcombination regimens in HCVgenotype 1 infected
patientsaccording to the presence of baselineRAVs.
SVR rates NS5A inhibitor plusnucleos(t)ide NS5B inhibitor
DAAcombination regimens in HCVgenotype 1 infected patientsaccording
to the presence ofbaseline RAVs.
Sarrazin C et al., J Hepatol 2015
-
Rong L et al., Sci Transl Med 2010
It has been predicted that every nucleoside of the 3.2 kb HBV
genome or the 10 kb HIV and HCV genomes theoretically can be
substituted every day within a given infected patient
Mutations occur frequently during the HCV replication
Smith et al., 2014
-
Overall prevalence of Q80K in G1 across different regions
6%
19%
All G1 G1a
Europe
34%
48%
All G1 G1a
North America
3%9%
All G1 G1a
South America
13.7% of patients (274/2007) all HCV G1 29.5% (269/911) of those
with HCV GT1a and 0.5% (5/1096) of those with HCV GT1b
Update from Sorbo MC et al., ICAR 2015
Sarrazin C et al., Antivir Res 2015
HCV GT-1a(N=267)
HCV GT-1b(N=352)
16.1%
1.1%
Jacobson et al. Presented at AASLD 2013Lenz et al. Presented at
AASLD 2013
Q80K: 34.7% in subtype 1a HCV German treatment-naïve pts
(N=170)
Dietz et al., PLoSOne 2016
Italy our data
-
The prevalence of pre-treatment NS5A RAVs in GT-1 is
differentacross different countries, ranging from 6% to 25%, and
differentaccording to subtype…..
The analysis of >3000 GT-1 NS5A sequences form 14 countries
showed a high prevalence of baseline Y93H mutation (associated with
resistance to daclatasvir 100 fold) in GT -1 b infected patients,
ranging from 7% to 15%.
Svarovskaia E.S., EASL 2015
-
The Italian experience: the prevalence of patients with at least
1 natural NS5A RAV
is different according to genotype and subtype
Cento V, 14th European Meeting on HIV & Hepatitis - 2016
M28V: 3.7%L31M: 4.3%Y93HC: 1000)
-
23/26 86/91 32/34 164/169 17/20 113/113 14/14 44/44
12 Weeks 12 Weeks 24 Weeks 24 WeeksSarrazin et al., EASL
2015
Impact of baseline NS5A RAVs can be reduced/eliminated by
changing the regimen (longer duration of treatment, inclusion
of
RBV) in patients with compensated cirrhosis treated with
Ledipasvir/Sofosbuvir
• 18% (94/511) cirrhotic patients had BL RAVs
Chart1
LDV/SOFLDV/SOF
LDV/SOF+RBVLDV/SOF+RBV
LDV/SOFLDV/SOF
LDV/SOF+RBVLDV/SOF+RBV
With RAVs
No RAVs
SVR12 (%)
88
95
94
97
85
100
100
100
Sheet1
With RAVsNo RAVs
LDV/SOF8895
LDV/SOF+RBV9497
LDV/SOF85100
LDV/SOF+RBV100100
-
LDV/SOF ± RBV: SVR12 in GT 1 Patients With Cirrhosis ± Baseline
NS5A RAVs
Sarrazin et al., EASL 2015
Different impact according to HCV-1 subtype……
-
… Even in GT 1 and GT 4 patients with advanced liver disease or
post liver transplant (SOLAR-1 and 2)
Charlton M et al., EASL 2016
Impact of baseline NS5A RAVs can be reduced/eliminated by longer
duration of treatment in patients
treated with Ledipasvir/Sofosbuvir
GT1 a (N=376) & GT1b (N=211) GT 4 (N=35)
Baseline NS5B RAVs did not impact SVR12 rates
At time of relapse, NS5A RAVs were detected in most (91%)
patients, whereas NS5B RAVs were uncommon (16%; no S282T, L159F and
V321A; E237G was detected in 3 patients)
-
Baseline resistance polymorphisms
• NS5A: -28, -30, -31, or -93 polymorphisms detected in 22 of
112 patients• 82% (18/22) SVR in patients with NS5A
polymorphisms
• 10/14 (71%) in cirrhosis cohort; 8/8 in post-transplant
cohort
• 90% (81/90) SVR12 in patients without NS5A polymorphisms•
39/45 (87%) in cirrhosis cohort; 42/45 in post-transplant
cohort
• No NS5B-S282 variants detected at baseline or failure
Daclatasvir + Sofosbuvir + Ribavirin Combination for HCV
Patients with Advanced Cirrhosis or Post-transplant Recurrence:
ALLY-1 Phase 3 Study
Poordad F et al EASL 2015
-
HCV resistance to the daclatasvir/sofosbuvir combination across
different HCV genotypes in the real life
Impact of preexisting HCV NS5A and/or NS5B resistance-associated
variants (RAVs) on treatment outcomes in a cohort of 177 patients
infected with HCV genotypes (GT) 1a (N=44), 1b (N=63), 3 (N=29) and
4 (N=41) receiving SOF plus DCV without ribavirin for 12 weeks.
44% of patients were cirrhotic.
Prior to treatment, NS5A RAVs were detected at a frequency of 9%
in GT1a-, 32% in GT1b-, 21% in GT3-and 10% in GT4-infected
patients. The most frequent RAVs were Y93H in GT1b (11%) and GT3
(3.5%). No NS5B S282T, L320F or V321A variants were detected, while
L159F was found in12% of GT1b patients at baseline Fourati S et
al., CROI 2016
-
Although the number of patients with baseline variants other
than Q80K was small, there was no difference in SVR24 rates among
GT1a-infected patients with any of these variants at baseline as
compared to
patients with the reference amino acid residue at the
corresponding position
Observed data SVR24 ratea in the presence of baseline
variants
Krishnan P et al., AAC 2015
-
Zeuzem S et al., Ann Intern Med. 2015
-
For HCV ……….already more than 100 RASs…
HCV DRAG, Forum for Collaborative HIV Research, Lontok et al
Hepatology 2015
1a – red 1b – blue 2 – brown 3a – green 4 – orange
Detection10%
-
Carefully…..Different WT codons in different HCV genotypes
/subtypes…..
Sorbo MC et al manuscript in preparation RAS from Lontok et al
2015
1a – red 1b – blue 2 – brown 3a – green 4 – orangeHCV-1b1:
D90208; HCV-1b2: AJ238799*; HCV-4a1:Y11604; HCV-4a2:NC_009825*
-
Carefully…..Different WT codons in different HCV genotypes
/subtypes…..
Sorbo MC et al manuscript in preparation
1a – red 1b – blue 2 – brown 3a – green 4 – orange
RAS from Lontok et al 2015
HCV-1b1: D90208; HCV-1b2: AJ238799*; HCV-4a1:Y11604;
HCV-4a2:NC_009825*
-
Not all RASs are Equal…..Fold-change in EC50 1a 1b
Position M28T Q30R L31M/V Y93H/N L31V Y93H/N
Ledipasvir 20x >100x >100x/>100x>1,000x/>10,000
20X >100x/?
Ombitasvir >1000x >100x10,000x/
>10,000x 100x
Daclatasvir >100x >1000x
>100x/>1000x>1,000x/>10,000x 100x>10x
>1,000x/
>1,000x 100x/-->100x
Velpatasvir
-
Huang et al., CROI 2016
Open and filled symbols depict viruses with or without mixtures,
respectively
-
Beware of HCV-genotype for NS5A resistance ...
Nakamoto S., WJG 2014
-
SVR rates were reduced in GT-3 patients with natural NS5A
RAVs treated with grazoprevir, MK-3682 (NS5B), and MK-8408 (NS5A
inhibitor) for 8
weeks
Gane EJ, AASLD 2015
ASTRAL-3: phase 3 studyof SOF + VEL for 12 weeks
in GT 3 patients
SVR12 84% (21/25) in patients
with Y93H
Mangia A, AASLD 2015
-
SVR rates were reduced in GT-3 patients with natural NS5A
RAVs treated with grazoprevir, MK-3682 (NS5B), and MK-8408 (NS5A
inhibitor) for 8
weeks
Gane EJ, AASLD 2015
ASTRAL-3: phase 3 studyof SOF + VEL for 12 weeks
in GT 3 patients
SVR12 84% (21/25) in patients
with Y93H
Mangia A, AASLD 2015
Better results if longer duration of treatment and/or inclusion
of RBV?
-
Kwo PY, EASL 2016
SVR rates were NOT reduced in GT-3 non-cirrhotic patients
with natural NS5A RAVstreated with ABT-493 + ABT-530
co-administered for 8 weeks
Muir AJ, EASL 2016
100 % SVR in GT-3 cirrhotic treatment-naïve patients treated
with ABT-493 + ABT-530 with/without RBV for 12 weeks
-
GT1a 24 (20.0)GT1b 44 (36.7)GT2c 6 (5.0)GT3a 24 (20.0)
GT4 (a-d-n-r) 22 (18.3)
0102030405060708090
100
Suboptimal/not recommended (N=70) Recommended (N=50)
Relapse (N=97) Breakthrough (N=14) Non responder (N=9)
75.7%
12.9% 11.4%
88.0%
10.0%2.0%
In a real life italian setting a total of 120 patients whofailed
a DAA-regimen were analyzed (cirrhotics 74%)
Di Maio VC et al., EASL 2016Di Maio VC et al., 14th European
Meeting on HIV & Hepatitis - 2016
Prev
alen
ce o
f pat
ient
s inc
lude
din
the
anal
ysis
(%)
• SOF+RBV (N=46, HCV-1,3,4)• SMV+DCV+/-RBV (N=8)• SOF+PegIFN+RBV
(N=6)• 3D+/-RBV (N=1 HCV-2, N=2 HCV-3)• Other (N=7)
• SMV+SOF+/-RBV (N=33)• 3D+/-RBV (N=4, HCV-1a,1b)• DCV+SOF+/-RBV
(N=4)• LDV+SOF+/-RBV (N=4)• SOF+RBV (N=5, HCV-2)
-
Day 0 4w 8w
1
2
3
4
5
6
7
Relapser to SOCHCV genotype: 1a Sex: M CirrhosisAge:
53ID_1497HC
V-RN
A (lo
g IU
/ml)
LLOQ (12 IU/ml)
Paritaprevir/ritonavir+Ombitasvir+Dasabuvir+RBV
On September 2015 the HCV genotype determination wasrepeated
with a commercial assay:HCV genotype 3a
A NS3, NS5A and NS5B genotypic resistance test was performed in
our laboratory…
A Clinical case of a patient with cirrhosis starting in August
2015 3D+RBV
-
Day 0 4w 8w
1
2
3
4
5
6
7
HCV-
RNA
(log
IU/m
l)
LLOQ (12 IU/ml)
GRT 8 weeksBy phylogenetic analysis a HCV- 3a infection was
confirmedNS3 Resistance Mutations: NoneNS5A Resistance Mutations:
Y93HNS5B Resistance Mutations: None
Relapser to SOCHCV genotype: 3a Sex: M CirrhosisAge:
53ID_1497
Paritaprevir/ritonavir+Ombitasvir+Dasabuvir+RBV
A Clinical case of a patient with cirrhosis starting in August
2015 3D+RBV
-
Day 0 4w 8w
1
2
3
4
5
6
7
HCV-
RNA
(log
IU/m
l)
LLOQ (12 IU/ml)
GRT 8 weeksBy phylogenetic analysis a HCV- 3a infection was
confirmedNS3 Resistance Mutations: NoneNS5A Resistance Mutations:
Y93HNS5B Resistance Mutations: None
SOF Interruption
DCV Start
In vitro daclatasvir resistance profile
0
2000
4000
6000
8000
M28
TQ
30H
Q30
RL3
1ML3
1VY9
3CL3
1VY9
3HL3
1M-Y
93H
F28S
L31M
C92R
Y93H
A30K
L31F
Y93H
R30G
R30H
R30S
L30H
Y93H
Y93R
Fold
resi
stan
ceGT 1a1 GT 45GT 23GT 1b2 GT 34
Natural RAS Y93H:2% in 93 GT-3 patientsCento V, 14th European
Meeting on HIV & Hepatitis - 2016
Relapser to SOCHCV genotype: 3a Sex: M CirrhosisAge:
53ID_1497
Paritaprevir/ritonavir+Ombitasvir+Dasabuvir+RBV
A Clinical case of a patient with cirrhosis starting in August
2015 3D+RBV
-
Documento di indirizzo dell’Associazione Italiana per lo Studio
del Fegatoper l’uso razionale di antivirali diretti di seconda
generazione nelle categorie di pazienti
affetti da epatite C cronica ammesse alla rimborsabilità in
Italia
Aggiornamento del 15 Dicembre 2015
-
EUROPEAN RAVS DATABASE: FREQUENCY AND CHARACTERISTICS OF RAVS IN
TREATMENT-NAÏVE AND DAA-EXPERIENCED PATIENTS
Susser & Dietz et al., EASL 2016
-
Do DAA resistance mutations “disappear” following
discontinuation of therapy?
-
In the majority of patients PR RAVs disappear….
Lentz O, et al. EASL 2014
Simeprevir
Krishnan P et al. EASL 2015
Paritaprevir/r
-
Post-treatment 24 Weeks
Post-treatment 48 Weeks
NS3/4A (any) 31/67 (46%) 5/57 (9%)NS5A (any) 68/70 (97%) 49/51
(96%)NS5B (non-nuc) 33/44 (75%) 20/35 (57%)
Persistence of NS5a Resistance Associated Variants Following
Ombitasvir/Paritaprevir/r +
Dasabuvir Treatment• Pooled patients with virologic failure from
all clinical trials
(n=2510)• 67 patients with HCV genotype 1a • 7 patients with HCV
genotype 1b (no long-term follow-up
reported)
Krishnan et al., Abstract #O057, EASL 2015
-
The absence (by Sanger sequencing) or low prevalence of RAVs
does not always means low amount of circulating
resistant virus
WT R155 (65.5%)
WT= wild-type
PT 13PT 11
WT R155 (96.3%)
R155K (35.5%)
R155K (3.7%)
Mutational Load of R155K: 77,966 IU/ml
Mutational Load of R155K: 594,022 IU/ml
HCV-RNA : 1,671,926 IU/ml HCV-RNA: 2,090,903 IU/ml
Mutational Load of R155K: 44,167 IU/ml
WT R155 (96.0%)
R155K (4.0%)
HCV-RNA: 1,104,189 IU/ml
At 100 weeks of therapy interruption At 62 weeks of therapy
interruption
PT 211
Three HCV-1a infected patients, all failing TVR-containing
regimen with RAVs, still showed the R155K after 60-100 weeks of
therapy interruption.
Di Maio VC, EASL 2015
-
SVR12 Rates With Retreatment of G1 SMV/SOF Failures: Real-World
Database
Simeprevir + sofosbuvir failures (n=27)
No RAVs: 18% NS3/NS5B: 52%/15% NS3 plus:
• NS5A: 4%• NS5B: 7%
Retreatment regimens Ledipasvir/sofosbuvir + RBV
12/24 weeks (n=10/13) Ombitasvir/paritaprevir/r +
dasabuvir + RBV 12/24 weeks (n=3/1)
0
20
40
60
80
100
SVR
12 (%
)
100% 100%
12 Weeks(n=10)
Interim SVR12 Rates (ITT)
93%
24 Weeks(n=13)
12 Weeks(n=3)
LDV/SOF + RBV OMB/PTV/r + DAS + RBV
Vermehren J, et al. EASL 2016
-
SVR12 Rates With Retreatment of Prior SOF/LDV or DCV DAA
Failures:
Real-World Study RAVs identified in sofosbuvir plus
daclatasvir or ledipasvir failures (n=22) No RAVs: 5% NS5A: 77%
NS5A plus either NS3 (5%), NS5B
(9%) or NS3 + NS5B (5%) Retreatment regimens
Simeprevir + sofosbuvir + RBV 12/24 weeks (n=6/11)
Ombitasvir/paritaprevir/r + dasabuvir + RBV 12/24 weeks
(n=4/1)
0
20
40
60
80
100
SVR
12 (%
)
100%
75%
12 Weeks(n=6)
Interim SVR12 Rates (ITT)100%
24 Weeks(n=11)
12 Weeks(n=4)
SIM + SOF + RBV OMB/PTV/r + DAS + RBV
Vermehren J, et al. EASL 2016
-
Lawitz E. et al., EASL 2015Hadas Dvory-Sobol IWDR Berlin, June
2014
Presence of NS5A RAVs is Associated with Retreatment Failure
SOF/LDV
12 240
N=41 SVR12
weeks
Failed SOF/LDV 8-12 wks (SVR>94%)Regimen SVR: 70%Cirrhosis:
46% BL NS5A RAVs: 73%
-
Lawitz E. et al., EASL 2015Hadas Dvory-Sobol IWDR Berlin, June
2014
Prior to re-treatno NS5B RAVs(S282T, L159F, V321A)At second VF 4
of 12 (33%) patients had NS5B RAVs:S282T (n=2)L159F (n=1)S282T +
L159F (n=1)
Presence of NS5A RAVs is Associated with Retreatment Failure
SOF/LDV
12 240
N=41 SVR12
weeks
Failed SOF/LDV 8-12 wks (SVR>94%)Regimen SVR: 70%Cirrhosis:
46% BL NS5A RAVs: 73%
-
Retreatment of LDV/SOF Failuresin absence of cirrhosis
Wilson E. et al Clin Infect Dis 2016
SOF/LDV12 240
N=34* SVR12
weeks
2 non-VF excludedBL Y93H/N: 8/32
* Failed: 4wks LDV/SOF + 9451
+/- 9669 (SVR=20-40%)Cirrhosis: 0% (97% F0-2) BL NS5A RAVs:
85%
SVR: 97%
Thirty-two of 34 enrolled participants completed therapy
97 100 96
0
20
40
60
80
100
Combined
31/32 5/526/27
SV
R12
(%)
No RAVs
RAVs
1 Relapse GT1b:BL NS5A: L31M + Y93H >1000x FC in LDV EC50At
Failure: L31M + Y93H + NS5B S282T (17.8%)
-
Hezode C et al EASL 2016
-
Poordad F et al., AASLD 2015
QUARTZ-I: Retreatment of HCV Genotype 1 DAA-failures with
Ombitasvir/Paritaprevir/r, Dasabuvir, and Sofosbuvir
17/22 patients had at BL >1 RAV in 1 of the 3 DAA targets;7
patients had RAVs (other than NS3 Q80K) in 2 targets:2 patients had
RAVs in all 3 targets.
• 22 DAA-treated patients 14/20 1a failed 3D
regimen No LDV/SOF
failures
Single treatment failure had no RAVs detected
-
Retreatment may require «unconventional» approaches with
multiple DAAsC-SWIFT retreatment Part B
HCV GT1-infected patients who failed 4, 6, or 8 weeks of
EBR/GZR+ SOF in Part A were offered retreatment with EBR/GZR + SOF
+RBV for 12 weeks
Lawitz E., AASLD 2015, Poster #LB-12
-
SOF/VEL + RBV for 24 weeks may be an effective retreatment
strategy for patients who
have failed NS5A-based HCV treatment
• 11/13 GT 3 patients with RAVs had Y93H; 9 (82%) achieved
SVR12• 5 patients had 2 NS5A RAVs; all 5 achieved SVR12• 3 patients
had NS3 RAVs; all 3 achieved SVR12
GT 2 (n=13*)GT 1 (n=34) GT 3 (n=16)
100% SVR 100% SVR100% SVR
38%No RAVs
5/13
62%RAVs8/13
82%No RAVs
28/34
18%RAVs6/34
19%No RAVs
3/16
81%RAVs13/16
100% SVR
77% SVR
10/133/38/85/56/6
96% SVR
27/28
Gane EJ et al., EASL 2016
-
Considerations in DAA Treatment Failure
Was initial therapy sub-optimal?Drug comboDurationRBV use
Indications of other problems on treatment?Adherence?
Significant drug interactions?
Are there other baseline host/disease factors that may have
contributed?Cirrhosis, especially decompensation IL28B, age,
treatment experience, baseline RASs
By Courtesy of N Terrault 2016
-
The role of NS5B resistance test for patients who failed a
Sofosbuvir containing regimen is not yet defined
Svarovskaia et al, JID 2015
n=901* with deep sequencing
n =12,012 in SOF or LDV/SOF clinical studiesn=1025 with
virologic failure
1% 282T SOF virologic failures Gane et al AASLD 2015
Zhdanov K., APASL 2015
Buti M et al J Hepatology 2015
-
DAA target Regimen HCV-geno/subtypeBaseline RASs Failure
RASs
NS3 NS5A NS5B NS3 NS5A NS5B
NS3+NS5B
SMV+SOF 1b V55A L159F+C316NSMV+SOF 1b Q80Q/R
L159F+C316N+S556GSMV+SOF 1b D168D/V L31M+Y93H L159F+C316NSMV+SOF 1b
Q80Q/R Y93H/Y L159F+C316N
SMV+SOF+RBV 1b D168D/V L159F+C316NNS5A+NS5B LDV+SOF+RBV 1b Y93H
L159F+C316N
NS5B
SOF+RBV 1b L159F+C316N L159F+C316NSOF+RBV 1b L159F+C316N
L159F+C316NSOF+RBV 1b R30H+Y93H L159F+C316N+S556GSOF+RBV 1b
L159FSOF+RBV 3a L159L/FSOF+RBV 3a L159FSOF+RBV 3a L159F
SOF+PegINF+RBV 1b L159F+C316NSOF+PegINF+RBV 1b
L159F+C316N+S556S/GSOF+PegINF+RBV 1b
L159F+C316N+S556GSOF+PegINF+RBV 1b L159F+C316N
DAA, Direct Acting Antivirals; RASs, Resistance Associated
Substitutions
3/20 (15%) HCV-3a infected patients who failed a
Sofosbuvircontaining regimen showed L159F RAS at virological
failure
Baseline resistance test not available
Di Maio VC et al., EASL 2016Di Maio VC et al., 14th European
Meeting on HIV & Hepatitis - 2016
-
Sex: MALE Country of Origin: ITALYAge: 41 year
Liver status: OLT in 2007HCV genotype: 4d
Outcome to previous pegIFN+RBV treatment: Null responder
The oral combination of daclatasvir + simeprevir was chosen as a
new treatment in 2014.
Clinical case
-
Day 0 Day1 Day2 1w 2w 4w 6w 7w 2w
1
2
3
4
5
6
7
Null Responder to SOCHCV genotype: 4d Age: 41 Sex: MID_451 OLT
in 2007
HCV-
RNA
(log
IU/m
l) Daclatasvir+Simeprevir Interruption
LLOQ (15 IU/ml)
GRT 2 weeks after therapy interruptionNS3 Resistance Mutations:
A156G, D168ENS5A Resistance Mutations: L28V, R30S
-
Day 0 Day1 Day2 1w 2w 4w 6w 7w 2w
1
2
3
4
5
6
7
Null Responder to SOCHCV genotype: 4d Age: 41 Sex: MID_451 OLT
in 2007
HCV-
RNA
(log
IU/m
l) Daclatasvir+Simeprevir Interruption
GRT Day 0NS3 Resistance Mutations: D168ENS5A Resistance
Mutations: R30S
LLOQ (15 IU/ml)
GRT 2 weeks after therapy interruptionNS3 Resistance Mutations:
A156G, D168ENS5A Resistance Mutations: L28V, R30S
-
1w 2w 3w 4w 5w 7w 9w 10w 12w 14w 19w 4w
1
2
3
4
5
6
7
0d 1d 2d
HCV-
RNA
(log
IU/m
l)
LLOQ (15 IU/ml)
Sofosbuvir+Ribavirin
HCV genotype: 4d Age: 41 Sex: MID_451 OLT in 2007
GRT 4 weeks after therapy interruptionNS3 Resistance Mutations:
D168ENS5A Resistance Mutation: R30SNS5B Resistance Mutations:
None
Days Weeks
Breakthrough to DCV+SMV
-
Day 0 2w 4w 6w 8w 12w 16w 20w 24w 4w 11w
1
2
3
4
5
6
7
HCV-
RNA
(log
IU/m
l) Ledipasvir+Sofosbuvir+Ribavirin
LLOQ (15 IU/ml)
after EOT
GRT 11 weeks after therapy interruptionNS3 Resistance Mutations:
D168ENS5A Resistance Mutations: R30SNS5B Resistance Mutations:
None
HCV genotype: 4d Age: 41 Sex: MID_451 Breakthrough to
SOF+RBV
-
Day 0 2w 4w 6w 8w 12w 16w 20w 24w 4w 11w
1
2
3
4
5
6
7
HCV-
RNA
(log
IU/m
l) Ledipasvir+Sofosbuvir+Ribavirin
LLOQ (15 IU/ml)
after EOT
GRT 11 weeks after SOF+LDV+RBV interruptionNS3 Resistance
Mutations: D168ENS5A Resistance Mutations: R30SNS5B Resistance
Mutations: None
GRT Day 0 (2014)NS53 Resistance Mutations: D168ENS5A Resistance
Mutations: R30S
HCV genotype: 4d Age: 41 Sex: M
Second OLT in 2016 Breakthrough to SOF+RBV
GRT 2 weeks after DCV+SMV interruptionNS3 Resistance Mutations:
A156G, D168ENS5A Resistance Mutations: L28V, R30S
Breakthrough to DCV+SMVNull Responder to SOC
Relapse to SOF+LDV+RBV
-
Treatment should be individualized
From Sarrazin C et al., J Hepatol 2015
Both in terms of treatment duration,number of effective drugsand
screening after SVR
-
DAA failure
Genotypic resistance testingNS3+NS5A+NS5B
No NS5A RAVs
SOF/LDV + RBVSOF + DCV + RBV
24 weeksNo Q80K
SOF + SIM + RBV 24 weeks
NS5A RAVs(Q30, L31, H58, Y93)
SOF + SIM + RBV 24 weeks
(even if Q80K)
NS5A and NS3 RAVs
(R155, A156, D168)
Desperationtime
3D + SOFSOF + SIM + DCV + RBVSOF +LDV/DCV + RBV
SOF + pegIFN + RBV12/24 weeks
Investigational triple regimens
Modified by Wyles D, AASLD 2015
Retreatment may require «unconventional» approaches with
multiple DAAs
-
Conclusions• Although systematic HCV resistance testing prior to
start DAA
treatment is NOT recommended (exception: NS3-Q80K, soon
NS5A-test for elbasvir), it is indeed currently considered (helpful
to store a sample in difficult patients).
• SVR rates are high with new IFN-free regimens (in both mono
and co-infected HIV populations). However, failures can occur,
particularly when treatment is suboptimal.
• At failure: the resistance test should be performed in all 3
genes NS3 + NS5A + NS5B.
• Retreatment options exist, today particularly based on
sofosbuvir in combination with one or two other DAAs (better with
RBV and longer duration).
• However, the frequent finding at failure of major RAVs
involving ≥2 DAAs-targets may advocate also for unconventional,
resistance-based regimens.
-
Thanks for your attention
What do we know about RAVs todayRASs�Resistance associated
substitutionsDianummer 3HCV genetic variability is higher than
HIV’s and HBV’sDianummer 5HCV genotype dictates the choice of
anti-HCV drugs �and can modulate the duration of treatment in
infected patients with chronic hepatitis C��HIV versus HCV�Baseline
resistance testingDianummer 8Virological issues in the DAAs
EraDianummer 10Dianummer 11Dianummer 12Dianummer 13Should we be
worried about baseline RAVs?Dianummer 15Overall prevalence of Q80K
in G1 across different regionsThe prevalence of pre-treatment NS5A
RAVs in GT-1 is different across different countries, ranging from
6% to 25%, and different according to subtype…..�Dianummer 18Impact
of baseline NS5A RAVs can be reduced/eliminated by changing the
regimen (longer duration of treatment, inclusion of RBV) in
patients with compensated cirrhosis �treated with
Ledipasvir/SofosbuvirLDV/SOF ± RBV: SVR12 in GT 1 Patients With
Cirrhosis ± Baseline NS5A RAVs… Even in GT 1 and GT 4 patients with
advanced liver disease or post liver transplant (SOLAR-1 and
2)Dianummer 22Dianummer 23Dianummer 24Dianummer 25Dianummer
26Dianummer 27Dianummer 28Dianummer 29Not all RASs are
Equal…..�Dianummer 31Beware of HCV-genotype for NS5A resistance
...SVR rates were reduced in GT-3 patients with natural NS5A RAVs
treated with grazoprevir, MK-3682 (NS5B), and MK-8408 (NS5A
inhibitor) for 8 weeksSVR rates were reduced in GT-3 patients with
natural NS5A RAVs treated with grazoprevir, MK-3682 (NS5B), and
MK-8408 (NS5A inhibitor) for 8 weeksSVR rates were NOT reduced in
GT-3 non-cirrhotic patients �with natural NS5A RAVs �treated with
ABT-493 + ABT-530 co-administered for 8 weeks �Dianummer
36Dianummer 37Dianummer 38Dianummer 39Dianummer 40Dianummer
41Dianummer 42In the majority of patients PR RAVs
disappear….Persistence of NS5a Resistance Associated Variants
Following Ombitasvir/Paritaprevir/r + Dasabuvir TreatmentDianummer
46SVR12 Rates With Retreatment of G1 �SMV/SOF Failures: Real-World
DatabaseSVR12 Rates With Retreatment �of Prior SOF/LDV or DCV DAA
Failures: �Real-World StudyDianummer 49Dianummer 50Retreatment of
LDV/SOF Failures�in absence of cirrhosisDianummer 53Dianummer
54Retreatment may require «unconventional» approaches with multiple
DAAs�C-SWIFT retreatment Part BSOF/VEL + RBV for 24 weeks may be an
effective retreatment strategy for patients who have failed
NS5A-based HCV treatmentConsiderations in DAA Treatment FailureThe
role of NS5B resistance test for patients who failed a Sofosbuvir
containing regimen �is not yet definedDianummer 59Clinical case
�Dianummer 61Dianummer 62Dianummer 63Dianummer 64Dianummer
65Treatment should be individualizedRetreatment may require
«unconventional» approaches with multiple DAAs�ConclusionsDianummer
69
![Network Video Recorder - ANNKE | [Official] Annke-Easy & Affordable Security Camera ... · PDF file · 2016-09-14EU Conformity Statement ... Searching and playing back record files](https://img.pdfslide.net/doc/110x75/5ab11eac7f8b9a284c8c0eb3/network-video-recorder-annke-official-annke-easy-affordable-security-camera.jpg)