Embed Size (px)
Citation preview

Addiction (2000) 95 (Supplement 2), S129–S144
HUMAN MODELS IN CRAVING RESEARCH
What does cue-reactivity have to offerclinical research?
D. COLIN DRUMMOND
Department of Addictive Behaviour and Psychological Medicine, St George’s HospitalMedical School, University of London, London, UK
AbstractThis paper examines the application of the cue-reactivity paradigm as a means of studying alcohol dependencein clinical populations. Three main areas of application will be examined: cue-reactivity as a means ofunderstanding the nature of alcohol dependence; cue-reactivity as a predictor of relapse; and cue-reactivity asa method of studying treatment effects. The study of cue exposure and cue-reactivity has a long history butit is only relatively recently that the potential of cue-reactivity as a means of understanding and treatingaddictive behaviours has been studied in depth. The principal advantage of cue-reactivity over other existingparadigms to study addictive behaviour is in having a solid basis in widely studied general theories ofbehaviour. Cue-reactivity also provides a means of measuring and unpacking the concept of craving. Cravinghas long been believed to represent the underlying basis for addictive behaviour, and in the majority ofresearch studies craving has been conceptualized and measured in relatively simplistic ways. Craving hasgenerally been viewed as a unitary phenomenon and measured using self-reported questionnaires. Suchapproaches have had limited explanatory value, particularly in recent psychopharmacology research. Thereis clearly a need to develop new paradigms to study the effects of pharmacological agents aimed at attenuatingdrinking behaviour. It is in this area that cue-reactivity currently offers the greatest potential. In particular,the cue-reactivity paradigm draws an important distinction between cue mediated craving and withdrawalcraving. This can be viewed as similar to the distinction between generalised anxiety and anxiety provokedby phobic stimuli. However, while much is now known about the phenomenon of cue-reactivity, severalaspects require further elucidation and research investment.
IntroductionThe concept of alcohol craving has been viewedas an important feature of addiction to alcoholthroughout the history of the alcohol � eld.Lettsom (1787), for example, observed that tothe sufferer, alcohol:
“… becomes as necessary as food … neither
threats nor persuasions are powerful enough toovercome [the desire for alcohol], and themiserable sufferer is so infatuated, as in spiteof locks and keys, to bribe by high rewards thedependent nurse, privately to procure the fataldraught (p. 157).”
Similarly, Kerr, founder of the Society for the
Correspondence to: Dr D. Colin Drummond, Department of Addictive Behaviour and Psychological Medicine,St George’s Hospital Medical School, University of London, Level 6, Hunter Wing, Cranmer Terrace,London SW17 0RE, UK. E-mail: [email protected]
Submitted 1st September 1999; initial review completed 16th November 1999; � nal version accepted29th February 2000.
ISSN 0965–2140 print/ISSN 1360–0443 online/00/08S129–16 Ó Society for the Study of Addiction to Alcohol and Other Drugs
Carfax Publishing, Taylor & Francis Ltd

S130 D. Colin Drummond
Study and Cure of Inebriety, writing in 1889,referred to the abnormal desire for alcohol in theinebriate as “Pathological depravity of the appe-tite centre” (p. 221) and to “the dire drink crave,as in the punishment of Tantalus provokes thethirst it can never quench” (p. 247). Later,Jellinek (1960) viewed craving for alcohol as thekey underlying disorder in the Disease Conceptof Alcoholism, and as the basis for loss of con-trol. Craving (referred to as “the subjectiveawareness of the compulsion to drink”) was de-scribed by Edwards & Gross (1976) as one of theseven key elements of the Alcohol DependenceSyndrome, although they also point out that notall elements of the syndrome need necessarily bepresent simultaneously, leaving the interpret-ation of the signi� cance of craving (and otherelements) open to further elucidation.
However, the importance of craving as a cen-tral feature of addiction has been questioned.Mello (1972), for example, has argued that crav-ing represents super� uous tautology since it isusually de� ned by subsequent drinking behav-iour, and as such cannot be regarded as necess-arily causal. Similarly, Marlatt (1978)emphasizes that craving can be epiphenomenalor, more accurately, an explanation used by thedrinker to explain relapses. Further, the conceptof craving and the terminology used to describeit has come under criticism (Kozlowski &Wilkinson, 1987). In spite of Kozlowski &Wilkinson’s plea to tighten-up the technicalde� nition and use of the “craving” term, contro-versy and loose application of terminology con-tinues to reign. Notably in recent studies ofdrugs aimed at attenuating drinking behaviourthe term “craving” is seldom de� ned and is usedloosely and in different ways across studies. Fur-ther, the concepts of craving used implicitly orexplicitly in many such studies are not dissimilarto Jellinek’s concept of craving, which has beensubject to widespread criticism. Thus there isclearly a need to study and establish, or at leastto reach a consensus upon, the nature and rel-evance of craving.
There are two methods by which the natureand signi� cance of craving could be further elu-cidated, and both until now have received rela-tively scant attention in research. Other papers inthis supplement review the development ofde� nitions and subjective measures of craving(Sayette et al., 2000; Tiffany & Conklin, 2000).Both are necessary precursors to study the rel-
evance of craving in human addiction. Armedwith such measures one can then explore therelationship between craving and drinking be-haviour. The � rst area for research is to examinethe conditions under which craving, and relatedphenomena, are elicited. Also important is therelationship between craving and other elementsof the Dependence Syndrome such as with-drawal phenomena, relief drinking, salience, nar-rowing of repertoire and reinstatement. This hasreceived surprisingly little attention. This paperwill examine what is known about alcohol cuesand cue-reactivity, and the factors that mayin� uence cue-reactivity. The possible relation-ships between withdrawal, cue-reactivity andcraving will be explored. Finally, the potentialapplication of cue-reactivity as a means to studyalcohol dependence and relapse in humans willbe discussed.
Cues and cue-reactivityIn addition to noting the phenomenon of crav-ing, early observers of alcoholism (or inebriety)also had remarkably sophisticated concepts ofconditions in which craving and relapse occur(the terms “alcoholism” and “alcoholic” are usedthroughout as shorthand to denote “alcohol de-pendence” and individuals who are “alcohol-dependent”, respectively). Rush (1789), for ex-ample, noted that the environmental cues associ-ated with drinking could be dangerous foranyone “… who wishes to be cured of the habitsof intemperance” (p. 341). Rush also proposed aconcept of what is now termed conditioningtheory in relation to alcohol:
“Our knowledge of [the] principle of associ-ation upon the minds and conduct of menshould lead us to destroy … the in� uence of allthose circumstances, with which recollectionand desire of spirits are combined … and byrestraining them … from those places andcompanions, which suggested to them the ideaof ardent spirits, their habits of intemperancemay be completely destroyed (p. 340).”
Rush linked environmental cues both to the elic-itation of craving and to relapse. Wikler (1948)subsequently developed the theory that drugcues had an important role in the basis of mor-phine addiction in both animals and humansthrough what is now termed “cue-reactivity”.

Cue-reactivity and clinical research S131
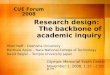
Figure 1. Models of relapse in addictive behaviour.
The principal distinction between this andalternative disease concepts of addiction (such asthat of Jellinek) is shown in Fig. 1. Within thedisease model, craving is a key manifestation (orsymptom) of the underlying disease of addiction,and craving, in turn, leads to relapse. It shouldalso be noted that Jellinek made a distinctionbetween craving arising during a period of absti-nence and craving occurring during binges. Thelatter form of craving is within this model“primed” by the ingestion of alcohol.
Within the cue-reactivity paradigm, cues pre-viously associated with drinking behaviour can,under certain conditions, elicit cue-reactivity,which can be symbolic expressive (e.g. craving,anxiety, pleasure), physiological (e.g. drug-like,withdrawal-like, appetitive), and behavioural(e.g. drink-seeking behaviour, consummatorybehaviour) (Drummond et al., 1995a). The cue-reactivity paradigm involves exposure to a cue orset of cues (e.g. the sight and smell of a favouritedrink) and observation and measurement of avariety of responses. Typically, symbolic express-ive reactivity will be measured by questionnairesdesigned to elicit subjective experiences. Physio-logical reactivity to alcohol cues has most oftenbeen measured in terms of changes in heart rate,skin conductance, skin temperature and sali-vation. More recently neuroimaging methodshave been used to study regional changes inbrain activity following cue exposure. Be-havioural cue-reactivity is the least studied, buthas included latency to drinking and speed ofdrinking test drinks of alcohol. A few studieshave examined how hard subjects work for al-cohol in an operant paradigm.
The three modalities of cue-reactivity shown
in Fig. 1 are conceptually distinct. However, inpractice they are often correlated (e.g. Glautier &Drummond, 1994), which may indicate a sharedunderlying causal mechanism. Tiffany (1995)has, however, drawn attention to the lack ofempirical support for a connection between sub-jective reports of craving and subsequent relapse.
The main attraction of the cue-reactivityparadigm for studying addiction and relapse isthat it allows the development of testable hy-potheses, and a means of studying addictiongrounded in widely studied general theories ofhuman behaviour. Such theories have also suc-cessfully been applied to the understanding andtreatment of other human behavioural disorderssuch as phobic anxiety and obsessive compulsivedisorder (Rachman & Hodgson, 1980; Marks,1987).
What are the cues?Reactivity to a wide variety of alcohol and drug-related cues has been studied in both humansand animals. A preliminary classi� cation of typesof cues provides four main categories: (1) extero-ceptive; (2) interoceptive; (3) temporal; and (4)cue relationships. Many of these cues have beendemonstrated to elicit cue-reactivity. Some re-main theoretical categories, but open to empiri-cal study.
The most commonly studied cues are extero-ceptive (sight, smell and taste), although in prac-tice these are dif� cult to present in isolation inthe experimental setting. Visual cues can includethe sight of a favourite drink, or can have morecomplex associations with drinking such as thesight of a bar, or billboard or television advertis-

S132 D. Colin Drummond
ing. Olfactory cues can include the smell ofalcohol or smells associated with drinking suchas certain foods or cigarette smoke. Interoceptivecues such as moods, cognitions and primingdoses of alcohol have also been studied. Therelationship between dreams and craving has notbeen studied formally, but could potentiallyin� uence cue-reactivity. Dreams about drugs areassociated with craving and relapse to drug use,possibly through a cue-reactivity mechanism(Christo & Franey, 1996).
In terms of temporal relationships, it is likelythat cues occurring more proximally to the inges-tion of alcohol will be more salient, and henceproduce greater reactivity, than cues more distal(and hence less predictive of alcohol delivery).For example, the smell, taste and sensation ofalcohol following ingestion are likely to be moresalient than talking or thinking about drinking.Indeed, our own research suggests that there aredifferences in reactivity between holding andlooking at alcoholic drinks compared to actuallytasting them, but this relationship is not as sim-ple as one of intensity (Glautier, Drummond &Remington, 1992). The time of day at whichcues are encountered is also likely to be relevantto the salience of a cue, although this has yet tobe studied. The time of day when alcohol ishabitually consumed may become an importantalcohol cue.
Finally, it is likely that there exist complexrelationships between cues. The context inwhich alcohol cues are presented can in� uencethe salience of cues and hence reactivity (e.g.Staiger & White, 1988). Further, alcoholics canreadily identify hierarchies of cues which presentgreater or lesser salience for them (Drummond& Glautier, 1994).
It is possible that inter-relationships exist be-tween cues in terms of their capacity to elicitcue-reactivity. Alcohol cues rarely occur in iso-lation. For example, the sight, smell and taste ofalcohol are dif� cult to separate experimentally orin the natural drinking environment. It may be,for example, that one cue, such as the sight of afavourite drink, has salience for an individualonly in a particular context, such as in the even-ing in the company of a drinking friend in afavourite pub. On the other hand, the samealcohol cue may have little salience � rst thing inthe morning, in a laboratory setting, in the pres-ence of a researcher. The interaction betweenco-occurring cues could be described as a “cue
cluster”, each cue within the cluster being anecessary but not suf� cient condition for drink-ing. Similarly, cues for an individual may occursequentially leading up to a drinking episode: a“cue chain”. For example, an of� ce worker leav-ing work on a Friday evening, walks home on aroute that passes his favourite pub, which hethen enters, lights a cigarette and orders a beer.In this example, each cue occurs sequentially,and each may in turn increase the salience of thesubsequent cue. It is possible in this situationthat if one of the cues is missing from the se-quence, the likelihood of drinking is reduced.For example, the favourite pub may be closed forrefurbishment, and even although all other cuesin the chain are present, drinking does not takeplace. The individual does not seek out analternative pub. The relationship between cuescould also be conceptualized as a cascade pro-cess in which each cue increases the likelihood ofencountering, and the salience of, the next cue: a“cue cascade”. Thus, in the of� ce worker exam-ple, leaving work feeling tired and stressed mayin� uence the choice of route home to includepassing a pub which holds greater salience forthe of� ce worker than other pubs. Once he hasentered the pub the likelihood of drinking al-cohol is increased by the presence of his friendswho apply social pressure on him to drink, andso forth. Thus there is likely to be a complexrelationship between cues that may be highlyspeci� c to the individual. However, again thisarea has received little research attention so far.A useful starting point might be to apply detailedqualitative analysis to the patterns and contextsof drinking, and to assess if these cue relation-ships, as opposed to the individual cues, havegreater predictive validity in respect of eitherrelapse to drinking or cue-reactivity.
What is cue-reactivity?In spite of the growth of research into cue-reac-tivity over the past 20 years there remains con-siderable controversy about what exactly is thenature of cue-reactivity. This research � eld hasbeen thoroughly reviewed elsewhere recently(Drummond, Cooper & Glautier, 1990; Drum-mond et al., 1995b; Glautier & Remington,1995). The three leading monistic models ofcue-reactivity are: (1) that cue-reactivity resem-bles unconditioned drug withdrawal (Wikler,1948); (2) cue-reactivity resembles uncondi-

Blood alcoholLevel
US
Withdrawalstate
UR
Sight & smell offavourite drink
CS
Conditioned withdrawal
CR
Cue-reactivity and clinical research S133
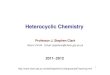
Figure 2. Conditioned learning in alcohol dependence. FromDrummond et al., 1990. US, Unconditioned stimulus; UR,Unconditioned response; CS, Conditioned stimulus; CR,
Conditioned response.
interpreting the research. In a review of thehuman cue-reactivity literature, Glautier et al.(1992) point out that some of the con� ictingconclusions can be explained by the mode ofpresentation of the cues. Studies in which drinkcues are presented but no alcohol is consumedtypically produce drug-opposite responses,whereas studies in which drinks were consumedtend to produce drug-like responses. However,this is not the sole explanation. Glautier & Rem-ington (1995) point out that it is extremelydif� cult to infer the direction of responses tocues since responses occur in multiple interactivephysiological response domains. For example,changes in heart rate in one direction are likely toaffect blood pressure, vascular tone, and henceskin temperature, such that erroneous inferencescan be made by studying one response measurein isolation. Further, they note that most of thestudies examined have not attempted to controlfor extra-experimental exposure to cues. Typi-cally this occurs in studies in which alcoholicsare compared to control subjects, ignoring thepossibility that alcoholics may differ from con-trols in many respects in addition to cue-reactivity.
One method of distinguishing between thethree models, empirically, is to design an exper-iment in which all extra-experimental effectshave been controlled for. One example of such astudy is that of Glautier, Drummond & Reming-ton (1994), in which social drinkers were intro-duced to novel stimuli which were, within theexperiment, associated with delivery of an al-coholic or a non-alcoholic drink over severalexposures. Subsequently, the effects of exposureto these stimuli without alcohol delivery werestudied. Differences in subjective, physiologicaland behavioural responses to these novel alcoholcues compared to neutral cues were found, sug-gesting that conditioning had taken place. Thepattern of responding appeared to support ageneralized arousal response rather than aspeci� c drug-like or drug-opposite response.Further studies are needed to examine the natureof such responses to novel stimuli, free fromextra-experimental effects in clinical alcoholicpopulations, providing appropriate ethical safe-guards of giving alcohol to alcoholic subjects canbe assured.
A recent meta-analysis of cue-reactivity exper-imental studies found similar pro� les across ad-dict groups, including smokers, drug addicts and
tioned drug effects (Stewart, de Wit & Eikel-boom, 1984); and (3) cue-reactivity opposes theunconditioned drug effect (Siegel, 1975). Allthree are described in terms of classical con-ditioning, cue-reactivity being a conditioned re-sponse (CR). However, it is important to notethat cue-reactivity need not be explained solelyin terms of conditioning, with cognitive theory asa leading alternative model (Marlatt, 1978).
Wikler (1948) viewed cue-reactivity as a stateresembling unconditioned drug withdrawal.Figure 2 shows a postulated mechanism for thedevelopment of withdrawal-like CRs to alcoholcues. During a drinking episode the alcoholic isexposed to cues such as the sight and smell offavourite drinks at a point in the drinking cyclewhen the blood alcohol level is falling or is at alow point (US), such as in the morning after adrinking binge. At this point the alcoholic is in astate of unconditioned alcohol withdrawal (UR).The cue becomes associated with withdrawaland hence, during a period of abstinence whenthe alcoholic is again exposed to the cues (CS),according to Wikler, a conditioned withdrawal-like reaction is elicited (CR).
Stewart et al. (1984), on the other hand, havepostulated that drug cues become associatedwith the pleasurable unconditioned effects ofdrugs and hence lead to drug-like CRs. Siegel’s(1975) model resembles that of Wikler. Thedifference is that Siegel hypothesized that the CRacts to oppose the unconditioned drug effectssuch that the CR is part of a homeostatic re-sponse, which leads to the development of drugtolerance. In this model the CR is effectively anopponent process (Solomon & Corbit, 1974).
There is empirical evidence to support allthree hypotheses, which presents a problem in

S134 D. Colin Drummond
alcoholics (Carter & Tiffany, 1999). Overall,subjective craving effects were greater thanphysiological effects. Across drug categories, in-creases in heart rate, sweat gland activity anddecreased skin temperature were found. Carterand Tiffany conclude that this pattern of re-sponding might indicate the induction of a con-ditioned incentive–motivational state, althoughalternative explanations could be advanced.
Overall, no clear conclusion can be made atpresent about the form of cue-reactivity, al-though it appears to be the case that whenextra-experimental factors and the mode of pres-entation of cues is controlled for, presentation ofcues without alcohol ingestion tends to lead todrug-opposite CRs, whereas ingestion tends tolead to drug-like CRs. Another observation isthat most studies have focused on physiologicalcue-reactivity. Where used, measures of cravingin such studies have tended to be single itemmeasures which examine craving intensity, buttell little about the affective valence of cue-reactivity (Tiffany, Carter & Singleton, 2000).Also, little attention has been paid to behaviouralcue-reactivity: do subjects consume more alcoholin the presence of cues, or indeed in the natural-istic drinking environment? There is some evi-dence that this is the case (e.g. Ludwig, Wikler &Stark, 1974), but the � eld is missing an oppor-tunity to make a real connection between cueexposure and actual drinking behaviour, ratherthan simply making inferences concerning likelybehavioural outcomes based on observed physio-logical responses (Meyer, 2000). Better mea-sures of craving are also likely to be of help.Future research on cue-reactivity will also needto apply greater care in design to take account ofthese factors as well as individual and contextualfactors, to which we now turn our attention.
Factors affecting cue-reactivityMany factors can in� uence cue-reactivity, someof which have been mentioned already. Thesecan usefully be grouped into 3 categories: (1) cuecharacteristics; (2) individual factors; and (3)contextual factors.
Cue characteristics are clearly important inboth the intensity and valence of cue-reactivity asdescribed in earlier sections. Further, as wouldbe predicted theoretically, in vivo cues tend tohave greater salience than imaginal cues, andinteroceptive cues such as the initial priming
effects of alcohol have been found to be moresalient than imaginal or visual cues. There is,however, a recent study which suggests thatimaginal cues may be as effective as in vivo cuesin eliciting cue-reactivity (Weinstein et al.,1998). Overall, cues that have had a greaterassociation with alcohol consumption are morelikely to be salient than those that have had alimited or no previous association.
There are also many individual factors thatcan in� uence cue-reactivity. These have recentlybeen reviewed by Rees & Heather (1995). Theclearest evidence for individual differences is indegree of alcohol dependence: dependence andcue-reactivity tend to be positively correlated(e.g. Kaplan, Meyer & Stoebel, 1983; Glautier &Drummond, 1994). These � ndings are in keep-ing with learning theory predictions, that individ-uals who are more alcohol dependent will havehad a greater level of prior exposure to alcoholand are likely to have engaged to a greater extentin withdrawal-relief drinking.
Although considerable research has been con-ducted into familial and personality factors thatmay predispose individuals to develop alcoholdependence, relatively little study has been madeof predisposition to development of cue-reactivity. It is possible that what may be inher-ited is a higher level of conditionability to alcoholcues. Newlin (1985), for example, found thatsons of alcoholic fathers had enhanced“antagonistic placebo responses” to alcohol cues,similar to those found in heavy drinkers. It ispossible that this mechanism is mediated byinherited differences in conditioned or uncondi-tioned tolerance. Also the effects of intra-uterinealcohol exposure on subsequent alcohol cue-re-activity has not been studied.
There is also evidence that introversion, neu-roticism and impulsivity are associated with en-hanced cue-reactivity (Powell et al., 1990;McCusker & Brown, 1991; Powell, Bradley &Gray, 1992). The relationship between personal-ity factors and cue-reactivity is a promising areafor future research. Similarly, little research ef-fort has been directed towards examining poten-tial links between psychiatric co-morbidity andcue-reactivity. It is possible that the mood-altering effects of alcohol may enhance thesalience of cues, particularly in anxiety and de-pressive disorders (Cooney et al., 1987; Greeley,Swift & Heather, 1992; Rohsenow et al., 1992).
In common with much of the alcohol research

Cue-reactivity and clinical research S135
� eld, cue-reactivity studies have tended to focuson males. There is some evidence of genderdifferences in alcohol cue-reactivity (Newlin,1989; Rubonis et al., 1994). More research isneeded to identify the contribution of gender todifferences in cue-reactivity.
Finally, contextual factors are likely to be im-portant in cue-reactivity. Context-speci� c expec-tancies have been found to be important both inrelation to perceived availability of alcohol incue-reactivity studies (Laberg, 1986) and in rela-tion to outcome and ef� cacy expectations(Cooney et al., 1987; Greeley et al., 1992;Rohsenow et al., 1992). Further, in interpretingstudies comparing alcoholics and controls,Drummond et al. (1990) have suggested that thedemand characteristics of the experiment mayin� uence cue-reactivity. It is suggested that ex-posure to alcohol cues will have particularsigni� cance for alcoholics attempting to abstainfrom alcohol compared with those who continueto drink.
In summary, future studies of cue-reactivityneed to pay greater attention to individual differ-ences in cue-reactivity and therefore will requiregreater sophistication in experimental design.
Cue-reactivity and relapseWhile study of factors that in� uence or predictcue-reactivity is important in its own right, ofgreater practical signi� cance is the relationshipbetween cue-reactivity and relapse in the clinicalsetting. Conditioning theory predicts that indi-viduals with a higher level of subjective (craving)and physiological reactivity to cues have a higherlikelihood of relapse to drinking. There is empiri-cal evidence to support this prediction in bothalcohol and smoking research.
Abrams et al. (1988) found that increased heartrate, urge reactivity and anxiety following ex-posure to smoking cues in abstinent smokerspredicted subsequent relapse. Rohsenow et al.(1994) found that cue-elicited salivation and at-tention to stimuli predicted relapse during follow-up. However, although the occurrence ofcue-elicited subjective urges to drink predictedthe intensity of urges during follow-up they werenot predictive of relapse. Drummond & Glautier(1994) also studied predictors of relapse as partof a cue exposure treatment study. We found thatcue-elicited skin conductance level and subjectivecraving predicted latency to relapse to heavy
drinking, reinstatement of dependence and quan-tity of alcohol consumed during 6-month follow-up in a group of severely dependent alcoholics.However, contrary to predictions, cue-reactivitydid not predict latency to initial lapse.
In summary, there is evidence from clinicalstudies conducted to date that cue-reactivity ispredictive of relapse and reinstatement of depen-dence. However, the relationship between reac-tivity and relapse is likely to be complex.
“Withdrawal craving” and cue-elicitedcravingAs described earlier, the role of craving in relapseto drug use has been questioned. One of theprincipal criticisms has been that there is littleempirical support for the relationship betweencraving and relapse. Tiffany (1990), for example,found little relationship between craving and druguse in reviewing experimental studies across awide range of drug types. Other research hasfound that addicts rarely spontaneously reportcraving as a reason for relapse (e.g. Marlatt &Gordon, 1980). These � ndings stand in contrastto the evidence that cue-reactivity, including sub-jective craving, does, to some extent, predictrelapse.
The discrepancy between these � ndings couldbe explained by the difference between what I willterm “withdrawal craving” and cue elicited crav-ing. The distinctions between these concepts areshown in Table 1. It should be remembered thatcraving has been conceptualized as one elementof the dependence syndrome. Craving is relatedto the severity of dependence and particularlyemerges as a feature of withdrawal (Edwards,1986). During alcohol withdrawal craving willincrease to reach a peak and gradually decay overtime, as do other symptoms of withdrawal. Allsuch symptoms, including craving, are rapidlyrelieved by intake of further alcohol. The severityand duration of such symptoms is related to thedegree of alcohol dependence, and some ele-ments of withdrawal, including craving, can per-sist for several weeks or months after the morevisible autonomic signs of tremor and withdrawalhave subsided. The extended experience of with-drawal is known as the Protracted WithdrawalSyndrome and includes autonomic arousal, agi-tation, tremor, anxiety, insomnia and electro-physiological abnormalities (Begleiter & Porjesz,1979; Kissin, 1979). Withdrawal craving could

S136 D. Colin Drummond
Table 1. Withdrawal craving and cue elicited craving
Withdrawal craving Cue elicited craving
Related to Severity of alcohol Cue-speci� c, butwithdrawal and enhanced by withdrawalprotracted withdrawal severity
Time–course Gradual peak and decay Brief response to cueduring withdrawal; exposure; minutes orweeks or months (tonic) hours (phasic)
Related to degree of Yes Yesdependence
Predictor of relapse During withdrawal only During withdrawal andprotracted period ofabstinence
Relationship to Unconditioned response Conditioned response toconditioning to alcohol cessation alcohol cues
therefore be de� ned as the subjective experienceof craving in the context of unconditioned al-cohol withdrawal. Withdrawal craving will varyduring a cycle, or repeated cycles, of drinkingand withdrawal. Within this conceptualization,while withdrawal craving may be related to theseverity and time–course of alcohol withdrawal,research is needed to establish whether this typeof craving is an element of unconditioned with-drawal, or if it is an empirically distinct phenom-enon. Either way, withdrawal craving can occurin environments that do not contain any alcohol-related cues, as well as those that do.
Cue-elicited craving, on the other hand oc-curs, by de� nition, only in the presence of al-cohol-related cues. Cues that can elicit this typeof craving may vary from one individual to an-other. The time–course of withdrawal cravingand cue-elicited craving are different. As with-drawal craving is related to the time–course ofalcohol withdrawal it will decay gradually overweeks and months following cessation of alcoholuse, and will be a tonic response. Cue-elicitedcraving, on the other hand, will only occur inresponse to cues and will be a short-lived, phasicresponse, lasting for a few minutes or hours atthe most. On the basis of existing knowledge,withdrawal craving is likely to represent an un-conditioned response to alcohol cessation,whereas cue-elicited craving is likely to be aconditioned response to alcohol cues. In thissense the distinction between withdrawal cravingand cue-elicited craving is akin to that betweengeneralized anxiety and phobic anxiety.
This distinction between withdrawal and cue-elicited craving is also similar to Isbell’s (1955)categories of “non-symbolic” physiological crav-ing and “symbolic” psychological craving. Isbellsuggested that non-symbolic craving was relatedto the withdrawal syndrome following a heavydrinking binge, whereas symbolic craving couldoccur during a period of sobriety or preceding arelapse. He also postulated that non-symboliccraving would be predominantly physiological,whereas symbolic craving would be principallypsychological. Ludwig (1988) subsequentlynoted that it would be dif� cult to separatephysiological and psychological aspects of crav-ing conceptually. Ludwig also proposed that thetwo types of craving are likely to be inter-related.
It is possible that cues are more salient, andproduce a greater level of reactivity, during with-drawal than during a prolonged period of absti-nence. The alcohol withdrawal syndrome andprotracted withdrawal are characterized by in-creased physiological reactivity generally. Therewould be good reason to assume that cue-reactivity (including cue-elicited craving) wouldbe enhanced during withdrawal also, when anindividual is likely to be more aroused. Thistheoretical relationship between withdrawal crav-ing and cue-elicited craving is illustrated in Fig.3. It will be seen that withdrawal craving followsa characteristic withdrawal peak and decaypro� le. Cues encountered during this period willelicit a higher level of craving, the extent ofwhich will be proportional to the backgroundwithdrawal craving level.

0Time since last drink
Cra
ving
inte
nsity
Withdrawal craving
Cue-elicited craving
Cue-reactivity and clinical research S137
Figure 3. Hypothetical relationship between cue elicited and withdrawal craving.
Both cue-elicited craving and withdrawal crav-ing will be correlated with the degree of depen-dence, perhaps for different reasons. Assuggested earlier, a more severely alcohol-depen-dent individual is likely to have more severeunconditioned withdrawal than a less dependentindividual. Withdrawal craving will be correlatedwith other withdrawal phenomena. Similarly, ifcue-elicited craving is a conditioned response, itis likely to be correlated with dependence be-cause of the greater conditioning history of themore dependent drinker.
To return to our earlier question of the prob-able predictive value of craving measures, whichtype of craving is more likely to be predictive ofsubsequent drinking behaviour? It could be ar-gued that cue-elicited craving is more likely topredict relapse to drinking than withdrawal crav-ing. Cue-elicited craving occurs in close proxim-ity to alcoholic drinks and cues which providethe context for relapse (e.g. pub settings, drink-ing friends, mood states). Cue-elicited craving istherefore more likely to occur shortly beforerelapse takes place. However, as withdrawalcraving theoretically increases cue-elicited crav-ing when cues are encountered, withdrawal crav-ing may in� uence the predictiveness ofcue-elicited craving, indirectly. After withdrawalhas subsided only cue-elicited craving is likely tobe of predictive value in subsequent relapse.
To what extent are these predictions borne outin practice? We know that severity of withdrawalsymptoms and degree of dependence are poor
predictors of relapse empirically (e.g. Drum-mond & Glautier, 1994). Withdrawal craving islikely to share similar characteristics to otherwithdrawal-related measures in relation to re-lapse. As Tiffany has shown (Tiffany & Conklin,2000), craving in general is a poor predictor ofrelapse. However, we also know that most re-lapses occur in the � rst 2 months after with-drawal of alcohol and the rate of relapsedecreases exponentially over time. This may berelated to the peak and decay of the backgroundlevel of withdrawal craving, which in turn mayincrease the salience of cues and severity ofcue-reactivity when cues are encountered.
Cue-elicited craving is predictive of relapse,but less so than autonomic cue-reactivity, al-though the two are correlated (Glautier &Drummond, 1994). It may be the case thatcue-elicited craving (and withdrawal craving) aresubject to many in� uences including the attribu-tional bias of the subject in labelling internalstates and the demand characteristics of the ex-perimental setting (Drummond et al., 1990). Ineffect, alcoholics may report craving subject towhat they want the researcher to hear. In ad-dition, there may be different physiological re-sponses and verbal reports, dependent on theavailability of alcohol in the cue exposure setting.Tiffany’s (1990) Cognitive Processing Model ofcue-reactivity postulates that craving will only beelicited when access to the drug or alcohol isimpeded during cue exposure. However, withinthis model physiological responses are predicted

S138 D. Colin Drummond
to occur whether access to the drug is impededor not (although physiological responding maydiffer according to these conditions). Therefore,although more research is needed to testTiffany’s model adequately it is likely thatphysiological cue-reactivity will be a better pre-dictor of relapse than cue-elicited craving alone(Carter & Tiffany, 1999). Thus, while the modeldescribed here relating to cue-elicited and with-drawal craving is similar to Isbell’s dichotomy,both may involve physiological and psychologicalelements in complex interplay.
In summary, the distinction between with-drawal craving and cue-elicited craving may ex-plain some of the limitations of craving measuresas predictors of relapse, particularly measures oftonic background craving (e.g. The ObsessiveCompulsive Drinking Scale: Anton, Moak &Latham, 1996). Future research needs to investi-gate the relationship between craving related tounconditioned withdrawal, cue-elicited craving,and relapse.
Cue-reactivity in developing new treatmenttechnologiesThere is a need to develop new and more effec-tive treatment methods for alcohol dependence.Brief interventions are relatively effective in re-ducing alcohol consumption in individuals withearly stage alcohol problems who have not yetdeveloped a signi� cant level of alcohol depen-dence (Bien, Miller & Tonigan, 1993). In pa-tients with more severe and established alcoholdependence the results of intervention are lessencouraging (Edwards, 1988). Until we have abetter understanding of the relapse process it willbe dif� cult to develop new treatment ap-proaches. This is where cue-reactivity offers itsgreatest potential.
Cue-reactivity is a useful method to measureand understand the effects of cue exposure treat-ment (Drummond & Glautier, 1994), althoughcue-reactivity is only a partial explanation of thepositive effects of cue exposure treatment. It islikely that cognitive concepts such as self-ef� cacy, situational con� dence and outcome ex-pectancies are also important mediators oftreatment response in cue exposure as well as inother treatment approaches. Nevertheless, cue-reactivity provides a means to study and re� necue exposure treatment techniques.
Another area in which cue-reactivity is likely to
� nd application is in the development of newdrug treatments which aim to reduce relapse orattenuate drinking behaviour. There is some evi-dence that naltrexone (a long-acting opioid an-tagonist) attenuates drinking behaviour in bothanimals and humans (O’Malley et al., 1992;Volpicelli et al., 1992; Froehlich & Li, 1993; deWaele et al., 1994; van Ree et al., 1994; Swift,1995). Naltrexone has recently been studied inthe context of cue-reactivity and a preliminarystudy has shown that naltrexone may reducecue-elicited urges to drink, and that this mayprovide some pointers as to its clinical effects(Monti et al., 1996). However, the precise mech-anism of naltrexone in alcohol dependence isunknown.
Of the recently developed drug therapies,acamprosate (a drug acting on the inhibitoryGABA system) shows particular promise, al-though its mechanism of action is still far fromclearly understood (Littleton, al Qatari & Little,1996). Acamprosate has been found to havesigni� cant clinical bene� ts in reducing alcoholconsumption and relapse across several clinicaltrials. However, one of the limitations of thedrug in routine practice is that it is not possibleat present to predict accurately which alcoholicsare most likely to bene� t from it. One possibleexplanation for the effect of acamprosate is thatit suppresses conditioned withdrawal-like re-sponses to alcohol cues (Littleton, 1995). It ispossible that responders to drug treatment ob-tain bene� t, compared with non-responders, byvirtue of individual differences in cue-reactivityand the effects of drug on cue-reactivity. It isequally possible that acamprosate has an effecton relapse through suppression of withdrawalsymptoms, including withdrawal craving, whichin turn results in lower levels of cue-reactivity, asproposed above. Benzodiazepines may have asimilar effect. These hypotheses could be readilytested experimentally.
In order to explore the possible role of suchdrug treatments in preventing relapse throughalterations in cue-reactivity, it is necessary todevelop more speci� c models of cue-reactivity inalcohol dependence. This enters the realm ofspeculation, but is a necessary exercise in gener-ating testable hypotheses.
Neuroadaptation and cue-reactivityConsiderable interest has focused so far on thedirectionality of cue-reactivity in alcohol depen-

Cue-reactivity and clinical research S139
Figure 4. Neuroadaptation and cue-reactivity in alcohol dependence: hypothesized effects on neurotransmission in opioidergicneurones. Section 1 shows the hypothesized effects of alcohol on opioidergic neurones that lead, over chronic alcohol exposure,to neuroadaptation. Initially (1a) the alcohol na õ ve system is in a steady state with a neutral hedonic effect (i.e. neither positivelyor negatively hedonic). With � rst alcohol exposure increased opioid neurotransmitter is released, resulting in a positively hedonicmood state (1b). Following chronic alcohol exposure (1c) the post-synaptic opioid receptor is downregulated due to exposureto high levels of opioid transmitter. Subjectively, a neutral hedonic state is experienced, indicative of the development of tolerance.Finally, during alcohol withdrawal, opioid release is reduced below the initial steady state level (1d). This, combined witha downregulated post-synaptic receptor, results in a negatively hedonic mood state. Section 2 shows the hypothesized effect ofalcohol cues on opioidergic neurones at various stages following abstinence from alcohol. If a cue is drug-like in its activityon the opioid system (CS 1 ), during withdrawal the increased opioid neurotransmitter release occasioned by the cue will resultin normalisation of hedonic tone (i.e. it will relieve a withdrawal-related negative hedonic state)(2a). During prolongedabstinence, after withdrawal has subsided, the same cue is hypothesized to produce a positive hedonic state (2b). This is becausethe cue increases opioid neurotransmitter release onto an upregulated (recovered) post-synaptic receptor. If, on the other hand,a cue is drug-opposite in activity on the opioid system (CS-), during withdrawal it will be expected to reduce opioid transmissioneven further than is already the case in the withdrawal state (2c). This will lead to worsening of the withdrawal-related negativehedonic state. Following a lengthy period of abstinence, the drug opposite cue will reduce opioid neurotransmission below thesteady state level (2d); but as the post synaptic receptor is upregulated, the effect of the cue will be less negatively hedonic than
it was during withdrawal.
dence. Cue-reactivity can be drug-like, with-drawal-like or drug-opposite. For the purpose ofthis discussion, we will assume that withdrawal-like and drug-opposite responses are synony-mous. Figure 4 presents a hypothesized model ofneuroadaptation and cue-reactivity in a neuro-transmitter system. This could be applied to anyneurotransmitter system but the opioid systemwill be used here as illustration. Followingchronic exposure to alcohol the opioid systemcan be hypothesized to undergo neuroadaptationwith downregulation of post-synaptic receptors.
This will lead to tolerance to the effects of al-cohol while drinking continues. When alcohol iswithdrawn, the decreased release of opioid neu-rotransmitter onto a downregulated post-synap-tic receptor will result in withdrawal, includingthe development of a negatively hedonic state(Nutt, 1999). With increasing duration of absti-nence, the post-synaptic receptor will graduallyupregulate, withdrawal will diminish and hedo-nic tone will return to a steady state (neutralhedonic state).
Section 2 in Fig. 4 shows the hypothesized

(a) Acute alcohol
Alcohol
Pos. hedonic
(b) Acute alcohol
Alcohol
Neutral
(c) CS + Neutral
(d) CS – Neg. hedonic
Naltrexone
Lengthyabstinence
Lengthyabstinence
Naltrexone
Naltrexone
Symbols and abbreviations used in Figures 4 and 5
CS + Cue producing drug-like responseCS – Cue producing drug-opposite response
Presynaptic neurone
Postsynaptic neurone: steady state
Postsynaptic neurone: downregulated
Steady state level of neuro-transmission
Reduced level of neuro-transmission
Considerably reduced level of neuro-transmission
Increased level of neuro-transmission
Neg. hedonic: Negatively hedonic mood state
Pos. hedonic: Positively hedonic mood state
S140 D. Colin Drummond
effect of exposure to alcohol cues at differentstages following withdrawal of alcohol. If a cueproduces a drug-like response (CS 1 ) in earlywithdrawal, this would lead to a neutral re-sponse. Although opioid release would increase,the receptor remains downregulated (less sensi-tive). However, after lengthy abstinence cue ex-posure would produce a positive hedonic(drug-like) effect because the receptor has re-turned to normal sensitivity. If, on the otherhand, a cue produces a drug-opposite response(CS-), in early withdrawal cue exposure wouldproduce a withdrawal-like hedonic response.Such a response would become gradually lessintense as the length of abstinence increasedbecause of receptor upregulation. Similarly, cueexposure in the presence of alcohol (i.e. alcoholintoxication) is likely to produce a different re-
sponse than cue exposure in the absence of drug.Thus, cue-reactivity varies within this model inrelation to duration of abstinence and the stageof the addiction-withdrawal cycle. This is inkeeping with the empirical human alcoholcue-reactivity research described earlier.
Cue-reactivity and opioid blockadeThe effect of cues at the neuronal level is notsimply idle speculation. It would be possible totest empirically both the mechanism of drugaction of opioid blockade on cue-reactivity, whileat the same time addressing the question of thedirectionality of cue-reactivity. It has been ob-served that alcohol induces activation of endor-phins in animals (Froehlich & Li, 1993; de Waeleet al., 1994). Further, opioid antagonists (nal-
Figure 5. Hypothesized effect of opioid blockade on alcohol cue-reactivity at a neuronal level. In the � rst part of the � gure(a) alcohol is applied to an alcohol na õ ve opioid neurone (as in 1b). This results in increased opioid neurotransmitter releaseand a positive hedonic state. As naltrexone provides opioid receptor blockade, it may block the positively hedonic effect ofalcohol-induced endogenous opioid release resulting in a neutral hedonic state (b). If a cue which is drug-like in effect on theopioid system is presented to an individual subject to opioid blockade induced by naltrexone, the positively hedonic effect ofthe cue is blocked by naltrexone, and a neutral hedonic state is maintained (c). If, on the other hand, a cue which is drugopposite in effect is presented to an opioid blockaded subject, the effect of the cue is to reduce opioid release and to produce a
negatively hedonic state similar to alcohol withdrawal (d).

Cue-reactivity and clinical research S141
trexone and nalmefene) can reduce alcohol con-sumption in both animals and humans(O’Malley et al., 1992; Volpicelli et al., 1992; vanRee et al., 1994; Swift, 1995). This has led to thehypothesis that opioid antagonists block thepositive hedonic effects of alcohol, thereby alter-ing alcohol cue-reactivity.
Figure 5 shows the hypothesized effects ofopioid blockade (in this case with naltrexone),depending on whether alcohol cue-reactivity isdrug-like or drug-opposite. As described above,alcohol is believed to increase release of endoge-nous opioids, which is positively hedonic,whereas naltrexone is hypothesized to block al-cohol-induced opioid release. If cue-reactivity isdrug-like (CS 1 ), naltrexone should block thepositive hedonic effects (or priming effect) ofcues, which would reduce the likelihood ofdrinking behaviour. If, on the other hand, cue-reactivity in opioid neurones is drug-opposite,cue exposure would lead to reduced opioid re-lapse and a negative hedonic state. It is possiblethat naltrexone would then intensify an alreadynegative hedonic state, perhaps increasing thelikelihood of drinking behaviour motivated byrelief of the negative state. Clearly the effects ofnaltrexone on alcohol cue-reactivity would alsodepend on the sensitivity of the receptors andhence would vary with duration of abstinence.Given that opioid antagonists tend to reducedrinking behaviour, suppression of a drug-likecue-reactivity appears more likely to be the case.Models such as those delineated above make itpossible to generate empirically testable hypoth-eses about the nature of cue-reactivity and aboutthe effects of a variety of different drugs ondifferent neurotransmitter systems. However, itmust be remembered that the effects of cues andpharmacological agents are likely to be highlycomplex at a neuronal level, given the knowninteractions between different neuronal systems.The opioid system, for example, interacts withthe dopamine system in a way that is likely to beimportant in drinking behaviour (Nutt, 1999).
ConclusionsThe concept of craving has been an enduringchimera throughout the history of the alcohol� eld. Despite problems of de� nition andmeasurement, it has its strong proponents andremains a phenomenon of clinical relevance, notleast to those who suffer from alcohol depen-
dence. The development of the cue-reactivityparadigm has added a further dimension to thestudy of craving and relapse. Cue-reactivity of-fers the opportunity to study the antecedents ofrelapse (including cue-elicited craving), and is amodel with a � rm basis in widely studied generaltheories of behaviour. The cue-reactivityparadigm also offers the opportunity to studycraving and relapse in parallel in human andanimal models.
The distinction between cue-elicited cravingand withdrawal craving, while important, doesnot negate the relevance of withdrawal craving.Withdrawal craving is likely to be relevant in thecontext of the protracted withdrawal syndrome,and may predict the intensity of cue-reactivity,although this has yet to be studied. Nevertheless,the distinction between cue-reactivity and with-drawal craving is important in adding greaterprecision to de� nitions and research study de-sign.
Other matters of importance to future researchare the factors that are known to in� uence cue-reactivity. There are several pointers from exist-ing research that should in� uence future studydesign, including the selection of appropriateexperimental controls. However, the study of cuecharacteristics, individual and contextual factorsin� uencing cue-reactivity would bene� t fromfurther research investment. In particular, thein� uence of psychiatric co-morbidity, which isknown to be of relevance in treatment and re-lapse, has not been studied so far to any greatextent in relation to cue-reactivity. More re-search investment in the study of individualizedand potentially complex interactions betweencues also deserves further investment in examin-ing conditions that may be more predictive ofrelapse than isolated laboratory-based cues, suchas the sight and smell of alcohol. Further, anopportunity is being missed to study the primingeffects of alcohol as a potentially more powerfulcue. However, this does not negate the value ofalso studying cue-reactivity that does not involvepriming doses of alcohol, as these cues may beimportant in the motivation to take the � rstdrink in the relapse process.
Cue-reactivity has value in studying the mech-anisms of psychotherapies, particularly cue-exposure treatment. However, cue-reactivity alsooffers a new method of studying the effects ofpharmacotherapies in alcohol dependence. In or-der to do so, more sophisticated models of cue-

S142 D. Colin Drummond
reactivity need to be developed and studied.Conversely, pharmacological agents with speci� cactions on neurotransmitter systems provide anopportunity to study the nature of cue-reactivityand its relevance to relapse.
In summary, the cue-reactivity paradigm con-tinues to offer new ways to study addictive be-haviour, and to contribute to the development ofnew treatment methods.
AcknowledgementsI am grateful to Drs Steve Glautier, CherryLowman and Raye Litten for comments on anearlier draft. I would also like to thank the Na-tional Institute of Alcohol Abuse and Alcoholismfor � nancial support in attending the workshopon Treatment and Alcohol Craving: Expandingthe Paradigm, in Washington, DC, 8–9 October1997, for which this paper was prepared.
ReferencesABRAMS, D. B., MONTI, P. M., CAREY, K. B., PINTO, R.
P. & JACOBUS, S. I. (1988) Reactivity to smokingcues and relapse: two studies of discriminant val-idity, Behavior Research and Therapy, 26, 225–233.
ANTON, R. F., MOAK, D. H. & LATHAM, P. K. (1996)The Obsessive Compulsive Drinking Scale: a newmethod of assessing outcome in alcoholism treat-ment studies, Archives of General Psychiatry, 53,225–231.
BEGLEITER, H. & PORJESZ, B. (1979) Persistence of a“subacute withdrawal syndrome” following chronicethanol intake, Drug and Alcohol Dependence, 4, 353–
357.BIEN, T. H., MILLER, W. R. & TONIGAN, J. S. (1993)
Brief interventions for alcohol problems: a review,Addiction, 88, 315–336.
CARTER, B. L. & TIFFANY, S. T. (1999) Meta-analysisof cue-reactivity in addiction research, Addiction, 94,327–340.
COONEY, N., GILLESPIE, R. A., BAKER, L. H. & KAPLAN,R. F. (1987) Cognitive changes after alcohol cueexposure, Journal of Consulting and Clinical Psy-chology, 55, 150–155.
CHRISTO, G. & FRANEY, C. (1996) Addicts’ drug-related dreams: their frequency and relationship tosix-month outcomes, Substance Use and Misuse, 31,1–15.
DOLINSKY Z. S. & BABOR T. F. (1997) Ethical, sci-enti� c and clinical issues in ethanol administrationresearch involving alcoholics as human subjects,Addiction, 92, 1087–1097.
DRUMMOND, D. C. & GLAUTIER, S. (1994) A con-trolled trial of cue exposure treatment in alcoholdependence, Journal of Consulting and Clinical Psy-chology, 62, 809–817.
DRUMMOND, D. C., COOPER, T. & GLAUTIER, S. P.
(1990) Conditioned learning in alcohol dependence:implications for cue exposure treatment, BritishJournal of Addiction, 85, 725–743.
DRUMMOND, D. C., TIFFANY, S., GLAUTIER, S. P. &REMINGTON, B. (1995a) Cue exposure in under-standing and treating addictive behaviours, in:DRUMMOND, D. C., TIFFANY, S. T., GLAUTIER S. P.& REMINGTON, B. (Eds) Addictive Behaviour: cueexposure theory and practice, pp. 1–17 (Chichester,John Wiley & Sons).
DRUMMOND, D. C., TIFFANY, S. T., GLAUTIER, S. P. &REMINGTON, B. (1995b) Addictive Behaviour: cue ex-posure theory and practice (Chichester, John Wiley &Sons).
EDWARDS, G. (1988) What treatments work for drink-ing problems? British Medical Journal, 296, 4–5.
EDWARDS, G. (1986) The alcohol dependence syn-drome: a concept as stimulus to enquiry, BritishJournal of Addiction, 81, 171–183.
EDWARDS, G. & GROSS, M. M. (1976) Alcohol de-pendence: provisional description of a clinicalsyndrome, British Medical Journal, 1, 1058–1061.
FROEHLICH, J. C. & LI, T. K. (1993) Recent de-velopments in alcoholism: opioid peptides, RecentDevelopments in Alcoholism, 11, 187–205.
GLAUTIER, S. P. & DRUMMOND, D. C. (1994) Alcoholdependence and cue-reactivity, Journal of Studies onAlcohol, 55, 224–229.
GLAUTIER, S. & REMINGTON, B. (1995) The form ofresponse to drug cues, in: DRUMMOND, D. C.,TIFFANY, S. T., GLAUTIER S. P. & REMINGTON, B.(Eds) Addictive Behaviour: cue exposure theory andpractice, pp. 21–46 (Chichester, John Wiley & Sons).
GLAUTIER, S., DRUMMOND, D. C. & REMINGTON,B. (1992) Different drink cues elicit differentphysiological responses in non-dependent drinkers,Psychopharmacology, 106, 550–554.
GLAUTIER, S., DRUMMOND, D. C. & REMINGTON, B.(1994) Alcohol as an unconditioned stimulus inhuman classical conditioning, Psychopharmacology,116, 360–368.
GREELEY, J., SWIFT, W. & HEATHER, N. (1992)Depressed affect as a predictor of desire for alcoholin current drinkers of alcohol, British Journal ofAddiction, 87, 1005–1012.
ISBELL, H. (1955) Craving for alcohol, QuarterlyJournal of Studies on Alcohol, 16, 38–42.
JELLINEK, E. M. (1960) The Disease Concept ofAlcoholism (New Haven, Hillhouse).
KAPLAN, R. F., MEYER, R. E. & STOEBEL, C. F. (1983)Alcohol dependence and responsivity to an ethanolstimulus as predictors of alcohol consumption,British Journal of Addiction, 78, 259–267.
KERR, N. (1889) Inebriety: its etiology, pathology, treat-ment and jurisprudence, chapter XIV, 2nd edn,pp. 243–266 (London, HK Lewis).
KISSIN, B. (1979) Biological investigations in alcoholresearch, Journal of Studies on Alcohol, 8 (Suppl.),146–181.
KOZLOWSKI, L. T. & WILKINSON, D. A. (1987) Use andmisuse of the concept of craving by alcohol, tobacco,and drug researchers, British Journal of Addiction, 82,31–36.

Cue-reactivity and clinical research S143
LABERG, J. C. (1986) Alcohol and expectancy: subjec-tive, psychophysiological and behavioural responsesto alcohol stimuli in severely, moderately and non-dependent drinkers, British Journal of Addiction, 81,797–808.
LETTSOM, J. C. (1787) Some remarks on the effectsof lignum quassiae amare, Memoires of the MedicalSociety of London, 1, 128–165.
LITTLETON, J. M. (1995) Acamprosate: how does itwork? Addiction, 90, 1179–1188.
LITTLETON, J., AL QATARI, M. & LITTLE, H. (1996)The neurobiology of craving: potential mechanismsfor acamprosate, in: SOYKA, M. (Ed.) Acamprosate inRelapse Prevention of Alcoholism, pp. 27–46 (Berlin,Springer).
LUDWIG, A. M. (1988) Understanding the Alcoholic’sMind: the nature of craving and how to control it(Oxford, Oxford University Press).
LUDWIG, A. M., WIKLER, A. & STARK, L. H. (1974)The � rst drink: psychobiological aspects of craving,Archives of General Psychiatry, 30, 539–547.
MARKS, I. M. (1987) Fears, Phobias and Rituals (NewYork, Oxford University Press).
MARLATT, G. A. (1978) Craving for alcohol, loss ofcontrol and relapse: a cognitive–behavioural analysis,in: NATHAN, P. E., MARLATT, G. A. & LOBERG,T. (Eds) Alcoholism: new directions in behaviouralresearch and treatment, pp 271–314 (New York,Plenum).
MARLATT, G. A. & GORDON, J. R. (1980) Determinantsof relapse: implications for the maintenance of be-havior change, in: DAVIDSON, P. O. & DAVIDSON, S.M. (Eds) Behavioral Medicine: changing healthlifestyles, pp. 410–452 (New York, Brunner-Mazel).
MCCUSKER, C. G. & BROWN, K. (1991) The cue-responsivity phenomenon in dependent drinkers:“personality” vulnerability and anxiety as interveningvariables, British Journal of Addiction, 86, 905–912.
MELLO, N. K. (1972) Behavioral studies of alcoholism,in: KISSEN, B. & BEGLEITER, H. (Eds) The Biology ofAlcoholism, Vol. 2. Physiology and behavior,pp. 219–291 (New York, Plenum).
MEYER, R. E. (2000) Craving: what can be done tobring the insights of neuroscience, behavioral scienceand clinical science into synchcrony, Addiction, 95(suppl. 2), S219–S227.
MONTI, P. M., ROHSENOW, D. J., SWIFT, R. M.,ABRAMS, D. B., COLBY, S. M., MUELLER, T. I.,BROWN, R. A. & GORDON, A. (1996) Effects of nal-trexone on urge to drink during alcohol cue ex-posure: preliminary results, Alcoholism Clinical andExperimental Research, 20, 92A (abstract).
NEWLIN, D. B. (1989) Placebo responding in the samedirection as alcohol in women, Alcoholism: Clinicaland Experimental Research, 13, 36–39.
NEWLIN, D. B. (1985) Offspring of alcoholics haveenhanced antagonistic placebo response, Journal ofStudies on Alcohol, 46, 490–494.
NUTT, D. (1999) Alcohol and the brain: pharmacolog-ical insights for psychiatrists, British Journal ofPsychiatry, 175, 114–119.
O’MALLEY, S. S., JAFFE, A. J., CHANG, G.,SCHOTTENFIELD , R. S., MEYER, R. E. &ROUNSAVILLE, B. (1992) Naltrexone and copingskills therapy for alcohol dependence: a controlledstudy, Archives of General Psychiatry, 49, 881–887.
POWELL, J., BRADLEY, B. & GRAY, J. A. (1992) Classicalconditioning and cognitive determinants of subjec-tive craving for opiates: an investigation of theirrelative contributions, British Journal of Addiction,87, 1133–1144.
POWELL, J, GRAY, J. A., BRADLEY, B. P., KASVIKIS, Y.,STRANG, J., BARRATT, L. & MARKS, I. (1990) Theeffects of exposure to drug related cues in detoxi� edopiate addicts: a theoretical review and some newdata, Addictive Behaviors, 8, 1–10.
RACHMAN, S. & HODGSON, R. (1980) Obsessionsand Compulsions (Englewood Cliffs, NJ, PrenticeHall).
VAN REE, J. M., KORNET, M. & GOOSEN, C. (1994)Neuropeptides and alcohol addiction in monkeys,EXS, 71, 165–174.
REES, V. W. & HEATHER, N. (1995) Individual differ-ences and cue-reactivity, in: DRUMMOND, D. C.,TIFFANY, S. T., GLAUTIER S. P. & REMINGTON, B.(Eds) Addictive Behaviour: cue exposure theory andpractice, pp. 99–118 (Chichester, John Wiley &Sons).
ROHSENOW, D. J., MONTI, P. M., ABRAMS, D. B.,RUBONIS, A. V., NIAURA, R. S., SIROTA, A. D. &COLBY, S. M. (1992) Cue elicited urge to drink andsalivation in alcoholics: relationship to individualdifferences, Advances in Behavior Research and Ther-apy, 14, 195–210.
ROHSENOW, D. J., MONTI, P. M., ABRAMS, D. B.,RUBONIS, A. V., NIAURA, R. S., COLBY, S. M.,WUNSHEL, S. M. & ABRAMS, D. B. (1994) Cue-reactivity as a predictor of drinking among malealcoholics, Journal of Consulting and ClinicalPsychology, 62, 620–626.
RUBONIS, A. V., COLBY S. M., MONTI, P. M.,ROHSENOW, D. J., GULLIVER, S. B. & SIROTA, A. D.(1994) Alcohol cue-reactivity and mood induction inmale and female alcoholics, Journal of Studies onAlcohol, 55, 487–494.
RUSH, B. (1789) An Inquiry Into the Effects of ArdentSpirits Upon the Human Body and Mind with anAccount of the Means of Preventing Them and of theRemedies for Curing Them, 8th edn, reprinted 1814(Brook� eld, Merriam).
SAYETTE, M. A., SHIFFMAN, S., TIFFANY, S. T.,NIAURA, R. S., MARTIN, C. S. & SHADEL, W. G.(2000) The measurement of drug craving, Addiction,95 (suppl. 2), S189–S210.
SIEGEL, S. (1975) Evidence from rats that morphinetolerance is a learned response, Journal of Compara-tive Physiological Psychology, 89, 498–506.
SOLOMON, R. L. & CORBIT, J. D. (1974) Opponentprocess theory of acquired motivation: I. Temporaldynamics of affect, Psychological Review, 81, 119–
145.STAIGER, P. K. & WHITE, J. M. (1988) Conditioned
alcohol-like and alcohol-opposite responses inhumans, Psychopharmacology, 95, 87–91.
STEWART, J., DE WIT, H. & EIKELBOOM, R. (1984) Roleof unconditioned and conditioned drug effects inthe self administration of opiates and stimulants,Psychological Review, 91, 251–268.
SWIFT, R. M. (1995) Effect of naltrexone on humanalcohol consumption, Journal of Clinical Psychiatry,56, 24–29.
TIFFANY, S. T. (1990) A cognitive model of drug urgesand drug-use behaviour: the role of automatic and

S144 D. Colin Drummond
non-automatic processes, Psychological Review, 97,147–168.
TIFFANY, S. (1995) The role of cognitive factors inreactivity to drug cues, in: DRUMMOND, D. C.,TIFFANY, S. T., GLAUTIER S. P. & REMINGTON, B.(Eds) Addictive Behaviour: cue exposure theory andpractice, pp. 137–65 (Chichester, John Wiley &Sons).
TIFFANY, S. T. & CONKLIN, C. A. (2000) A cognitiveprocessing model of alcohol craving and compulsivealcohol use, Addiction, 95 (suppl. 2), S145–S153.
TIFFANY, S. T., CARTER, B. L. & SINGLETON, E. G.(2000) Challenges in the manipulation, assessmentand interpretation of craving-relevant variables,Addiction, 95 (suppl. 2), S177–S187.
VOLPICELLI, J. R., ALTERMAN, A. I., HAYASHIDA, M. &O’BRIEN, C. P. (1992) Naltrexone in the treatment
of alcohol dependence, Archives of General Psy-chiatry, 49, 876–880.
DE WAELE, J. P., KIIANMAA, K. & GIANOULAKIS, C.(1994) Spontaneous and ethanol stimulated in vitrorelease of beta-endorphin by the hypothalamusof AA and ANA rats, Alcoholism: Clinical andExperimental Research, 18, 1468–1473.
WEINSTEIN, A., LINGFORD-HUGHES, A., MARTINEZ-RAGA, J. & MARSHALL, J. (1998) What makes al-cohol-dependent individuals early in abstinencecrave for alcohol: exposure to the drink, images ofdrinking, or remembrance of drinks—past?Alcoholism: Clinical and Experimental Research, 22,1376–1381.
WIKLER, A. (1948) Recent progress in research onthe neurophysiologic basis of morphine addiction,American Journal of Psychiatry, 105, 329–338.