Embed Size (px)
Citation preview

© 2001 Wiley-Liss, Inc.
Seminars in Surgical Oncology 2001; 20:181–186
What Every Surgical Oncologist Should KnowAbout Digital Mammography
ETTA D. PISANO, MD,1* CHERIE KUZMIAK, DO,1 MARCIA KOOMEN, MD,1
AND WILLIAM CANCE, MD2
1Department of Radiology and UNC-Lineberger Comprehensive Cancer Center,University of North Carolina, Chapel Hill, North Carolina
2Department of Surgery and UNC-Lineberger Comprehensive Cancer Center,University of North Carolina, Chapel Hill, North Carolina
This article reviews the available information on digital mammography for surgeons whocare for patients with breast cancer. The limitations of the current film-based technology andwhy digital mammography promises to improve breast cancer detection and breast lesiondiagnosis are described. The basics of digital imaging technology are reviewed, including adescription of image contrast and spatial resolution and its variance from currently availableclinical digital mammography systems. The results of clinical trials completed to date arereported. An upcoming large screening trial for digital mammography, sponsored by the Na-tional Cancer Institute, is described. Future technological developments, including improve-ments in softcopy display, image processing, computer-aided detection and diagnosis (CADD),tomosynthesis, and digital subtraction mammography (DSM), are briefly discussed. Semin.Surg. Oncol. 20:181–186, 2001.© 2001 Wiley-Liss, Inc.
KEY WORDS: digital mamography; computer-aided diagnosis/detection; softcopy display
INTRODUCTION
Film is an extremely useful medium that has been opti-mized over the past 40 years for mammographic imageacquisition, storage, and display. Because film serves threeroles, compromises have been made in achieving each ofthem. Since breast cancers are often quite similar in radio-graphic density to surrounding normal dense breast tissue,many lesions go undetected until they become palpable.From a physics perspective, digital mammography holdspromise for improved breast cancer detection and breastlesion characterization at a lower radiation dose to the pa-tient, primarily because of increased efficiency in the de-tection and depiction of the x-ray photons and low systemnoise [1,2]. In addition, digital detectors have a linear re-sponse to the number of photons they detect over a widerange of values. That is, the more photons detected by thesystem, the darker the images become. This allows forbetter penetration of the more dense parts of the breasts,areas in which breast cancers can be obscured by overly-ing breast tissue [2].
One of the advantages of digital mammograms is thatthey can be manipulated once they are acquired in muchthe same way as digital photographs. For a standard pho-tograph, as with a film mammogram, there is no way toadjust the contrast or density after it is acquired. Digital
images, however, can be adjusted to allow visualization orconspicuity of subtle details such as the spiculations at themargin of a small invasive breast cancer, or the granularcalcifications seen with a low-grade ductal carcinoma insitu. With film mammography, bad images cannot be re-adjusted or corrected. Therefore, patients must undergoadditional exposure to radiation to acquire images of ap-propriate quality if the first set is not diagnostic. Radiolo-gists and clinicians can examine the images with amagnifier or at a brighter viewbox, but the display of theimages is essentially fixed forever once those images areacquired. What you see is what you get [1,2].
In digital mammography systems, the process of detec-tion of photons is separated from the process of displayingthe image. Two separate media are used for each process.Yet a third medium is used for image storage. Each part ofthe imaging chain can be optimized separately. After theimages are acquired, the raw image data can be manipu-lated or processed, either by a computer or a human reader.
*Correspondence to: Etta D. Pisano, M.D., CB 7510, Room 503 OldInfirmary Building, UNC School of Medicine, 101 Manning Drive,Chapel Hill, NC 27599-7510. Fax: (919) 966-0817.E-mail: [email protected]

182 Pisano et al.
Computer-assisted detection and diagnosis (CADD) soft-ware to assist in image interpretation can be readily ap-plied to the raw digital data.
BASICS OF DIGITALMAMMOGRAPHY TECHNOLOGY
There are currently four digital mammography unitsavailable for clinical imaging, manufactured by GeneralElectric (GE) Medical Systems (Milwaukee, WI); FischerImaging Corporation (Denver, CO); Fuji Photo Film Com-pany, Ltd (Tokyo, Japan); and Lorad, a subsidiary ofHologic, Inc. (Bedford, MA). As of May 10, 2001, onlythe GE Senographe 2000D is approved for the imaging ofpatients by the United States Food and Drug Administra-tion (FDA). The other units are currently undergoing clini-cal testing for FDA pre-market approval (PMA). Inaddition, there are several digital mammography units thatare undergoing preclinical testing [1,2].
The spatial resolution of a digital image can be definedby the size of the real-world object that can be depicted byeach pixel. For mammography, this pixel size is usuallygiven in square microns, with that number defining thelength of each edge of the space depicted by each squarepixel. With fewer microns per pixel, the spatial resolutionof the detector is better. For example, the GE Senographe2000D has 100 µ2 pixels, while the Lorad Digital Mam-mography System has 41 µ2 pixels. Consequently, eachpixel in the image created by the GE unit depicts 100 µ2 of
the woman’s breast while the pixels in the Lorad image ofthe same woman’s breast depicts 41 µ2. Clearly, there aremany more pixels in the Lorad images than in the GE im-ages. So, while there undoubtedly is more informationavailable in the raw Lorad image data, the storage, trans-mission, and display of all those bits on the same imagecan be pretty challenging! The Fuji and Fischer systemshave 50 and 54 µ2 pixels, respectively.
The amount of contrast information available in theimage is defined by the bit depth per pixel [2]. The bitdepth is usually expressed as a whole number. That num-ber represents the power of 2 that equals the number ofgray levels available for display in that image. That is, ifan image has a bit depth of 8, there are 2 to the 8th power,or 256, gray levels available for display. This means thatthe range of x-ray photons that are absorbed by the detec-tor can be mapped out across 256 different gray values.So, the area of the detector that absorbs the most photonswill be translated into the darkest of those gray levels, andthe area of the detector that absorbs the fewest photonswill be translated into the lightest of those gray levels. Ofcourse, the areas detecting the intermediate numbers ofphotons will be mapped using the intermediate gray levelsthat are available. Images with higher numbers for bit depthhave better contrast by virtue of having more gray levelsavailable to spread across the range of numbers of detectedphotons [2]. For the existing systems, the bit depths are 10for Fuji, 12 for Fischer, and 14 for GE and Lorad.
Table I summarizes the technical parameters for the sys-tems. From this table, one can conclude that GE has in-vested computer data storage for greater contrast resolution
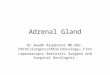
Fig. 1. This Fischer SenoScan™ digital mammogram, displayed atfull spatial resolution, reveals a cluster of calcifications that proved tobe a fibroadenoma at biopsy. Note how the calcifications have a pop-corn-like appearance and are relatively coarse. No branching or castingthat would be more typical of malignant calcifications is demonstrated.
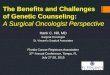
Fig. 2. This Fischer SenoScan™ digital mammogram shows a clusterof calcifications that proved to be a comedo-type ductal carcinoma insitu. The calcifications are quite variable in size, shape, and density,with linear forms. The appearance is quite typical for malignant calcifi-cations.

Digital Mammography 183
while Fuji and Fischer use the data for better spatial reso-lution, and Lorad stores both. The price of this decision ispaid in the size of the files to be manipulated, stored, re-trieved, and transmitted.
While it might seem obvious that more information ineither contrast or spatial resolution is better for breast can-cer detection, this is not necessarily the case. It may bethat a large improvement in contrast allows for earlier breastcancer detection than a large improvement in spatial reso-lution. It is possible that higher spatial resolution trans-lates into more false positives. Future clinical studies usingall of the available units will determine which factor ismost important in the clinic. Given that breast cancer isusually a low-contrast lesion which presents when it ismillimeters and not microns in size (even when micro-calcifications are involved), better image contrast may bemore important than better ability to detect small objectsin the image for most breast cancers. It is possible that theimprovement in calcification detection with smaller pixelsizes may cause more false-positive mammograms, lead-ing to more unnecessary biopsies, with all the attendantmorbidity and costs those entail.
The amount of information in the virtual image—thatis, the version in the computer itself—is only valuable ifall of it can be displayed and interpreted. If the 14-bit im-age with its 16,384 gray levels is displayed on an 8-, 10-,or 12-bit monitor, the image contrast available in the ac-tual viewed image is reduced commensurately. Laser-printed images, while they are static and cannot bemanipulated readily, have the advantage of making the fullrange of image contrast available to the viewer, since theycan be set up to print at the full 14 bits of contrast resolu-tion available in the virtual image.
Therefore, until large clinical studies are completed uti-lizing all of the available systems for breast cancer screen-ing and breast lesion characterization, it is impossible todeduce from first principals which system has the highestprobability of improving breast cancer detection and breastlesion characterization. The effect on breast cancer mor-tality is even more difficult to determine until more largeclinical trials are completed.
AVAILABLE CLINICAL DATA ONDIGITAL MAMMOGRAPHY
To date, there has only been one large screening trial toevaluate digital mammography, sponsored by the UnitedStates Department of Defense (DOD). This trial involvedtwo centers, the University of Colorado and the Univer-sity of Massachusetts, and utilized only a prototype GESenographe 2000D system at both sites. The preliminaryresults have been published [3], but more complete resultswith further follow-up were reported at the RadiologicalSociety of North America meeting late in 2000 [4].
This large screening trial enrolled 4,521 asymptomaticwomen who underwent both digital and screen-film mam-mography. All 6,768 examinations were interpreted inde-pendently, with patients recalled for additional testing ifeither test was positive. Breast cancer status was deter-mined by the results of biopsies for 183 lesions, and by ayear of clinical follow-up for those patients who did notundergo biopsy [4].
This study demonstrated a statistically significant re-duction in recall rates for digital mammography (11.9%)vs. screen-film mammography (15.0%). In addition, therewere statistically significantly fewer biopsies caused bythe digital studies than by the traditional mammograms.As for breast cancer detection, there was no statistical dif-ference in the number of cancers detected using digital andscreen-film mammography in this large asymptomaticpopulation, with 51 cancers detected overall, and a trendtowards traditional mammography finding more cancers[4]. The power of the study to find a small difference inbreast cancer detection was somewhat limited by the rela-tively small number of patients enrolled, and larger stud-ies will be needed to determine what the real rate of cancerdetection is with this new technology. In addition, theseresults apply only to the GE unit, since no patients wereimaged with the other machines.
The National Cancer Institute (NCI) recently awardedfunding to the American College of Radiology ImagingNetwork (ACRIN) to run a larger screening trial involv-ing all four available digital mammography devices. TheDigital Mammographic Imaging Screening Trial (D-MIST)is expected to enroll 49,500 asymptomatic women at 19centers in the U.S. and Canada over a 1.5-year period start-ing in July 2001. The centers involved, the types of equip-ment, and the principal investigators at each site are listedin Table II. The size of the trial is significantly larger thanthe DOD study in order to detect small differences in di-agnostic accuracy between digital and screen-film mam-mography, especially in the sensitivity of the test for theearly detection of breast cancer.
There has been one other large pilot study of diagnosticdigital mammography, performed by the International Digi-tal Mammography Development Group (IDMDG), andfunded by the Office of Women’s Health (OWH) in the
TABLE I. Technical Parameters for Digital MammographySystems
Total image size Spatial resolution Contrast(megabytes per (square microns resolution
Machine type image) per pixel) (bit depth)
Fischer SenoScan 29 54 12Fuji Computed 30 50 10
RadiographyGE Senographe 8 100 14
2000DLorad Digital 61 41 14
Mammography

184 Pisano et al.
Department of Health and Human Services. The IDMDGstudy enrolled 210 women at eight centers and utilizedprototype Fischer, GE, and Lorad equipment. Group Aconsisted of all consecutive women with mammo-graphically dense breasts who presented to the participat-ing mammography clinics for diagnostic mammographyand who underwent breast biopsy within the 12 weeks af-ter the eligibility mammogram. Women with palpable and/or nonpalpable lesions were included in this group. GroupB consisted of a random sample of women with mammo-graphically dense breasts who presented to the participat-ing mammography clinics for diagnostic mammography,and who had benign or negative findings at mammogra-phy. Eighteen radiologist readers interpreted these images.The results are currently under analysis. A larger studysponsored by the DOD, with the same design and a targetenrollment of 1,000 patients, is under way and should becompleted in 2002.
Finally, the cost-effectiveness of this new technologymust be assessed [5]. This evaluation is planned as part ofthe large ACRIN screening trial. Digital mammographywill almost certainly cost more than screen-film mammog-raphy, for both providers and patients. Consequently, itmust perform better than the current technology if it is tobecome more widely available. If it proves to be merelyequivalent in diagnostic accuracy to traditional methods,
it is unlikely to be utilized despite other advantages it mightprovide.
FUTURE DEVELOPMENTSSoftcopy Display
Digital mammograms can be presented on laser-printedfilm or on a computer workstation, also known as asoftcopy display system. The latter has traditionally uti-lized cathode ray tube (CRT) monitors. Laser printers pro-vide spatial resolutions comparable to traditionalmammography, with the reproduced size set to match theacquisition resolutions of current detectors, down to 41 µ2
pixels. In addition, image contrast is similar to that of mam-mography film. With this method of display, radiologistsand clinicians can hang and interpret the images the sameway they always have.
Of course, the cost of digital mammograms is higher ifthey are printed, because of the required hardware and thefilm itself, as well as the time it takes for a person to movethe image to the printer and the printed image to the reader.Film also has the disadvantage of inflexibility. There isonly one presentation format available for interpretation.If more than one version of each image is desired by thereader, there will be additional costs. Printing multipleversions of the same image is also very impractical.
Currently, only CRT technology supports the require-ments of softcopy display for digital mammography. Theexisting monitors do not have the same brightness or spa-tial resolution as viewboxes. Of the available digital mam-mography systems, only those obtained using the GEsystem can be completely displayed on the monitors at fullspatial resolution. Images from the other systems can onlybe partially shown on the monitors at full spatial resolu-tion. There are, however, technical corrections for both ofthese problems. “Roam and zoom” can be used to viewthe whole image at full spatial resolution. This tool mustbe fast and easy to use if it is to be useful to readers. Ascurrently implemented by Fischer, using this software al-lows the reader to view the image in much the same wayas when viewing traditional images with a magnifyingglass. High-brightness monitors are in development [6].Furthermore, the brightness difference may not be thatimportant. Studies [7,8] have demonstrated that the dis-play luminance available through CRT monitors does notworsen detection of lesions visible on mammograms com-pared to that available with viewboxes.
The most important feature available with softcopy dis-play is its flexibility. This allows the application of imageprocessing software nearly instantaneously. In the future,it is likely that processing specific to the visible lesion typeor mammographic task (screening vs. diagnosis) will beapplied to the images, perhaps automatically by the com-puter or at the request of the user. Image processing mighteven be automatically applied based on the individual fea-
TABLE II. ACRIN Sites, Machine Types and PrincipalInvestigators
Center Machine type Principal investigator
Beth Israel-Deaconess Fischer Janet Baum, M.D.LaGrange Diagnostics Fischer Carl Vyborny, M.D.
(IL)Memorial Sloan Kettering Fischer Michael Cohen, M.D.University of North Fischer Etta Pisano, M.D.
CarolinaWashington Radiology Fischer Leonard Glassman, M.D.
(DC)Mount Sinai (NY) Fuji Stephen Feig, M.D.University of Fuji Karen Lindfors, M.D.
California-DavisUniversity of Fuji Lawrence Bassett, M.D.
California-Los AngelesUniversity of North Fuji Etta Pisano, M.D.
CarolinaUniversity of Washington Fuji Anne Freitas, M.D.Northwestern University General Electric Edward Hendrick, Ph.D.University of Colorado General Electric John Lewin, M.D.University of General Electric Carl D’Orsi, M.D.
MassachusettsUniversity of General Electric Emily Conant, M.D.
PennsylvaniaUniversity of Toronto General Electric Martin Yaffe, Ph.D.Columbia University Lorad Suzanne Smith, M.D.Good Samaritan (NY) Lorad Melinda Staiger, M.D.Johns Hopkins Lorad Laurie Fajardo, M.D.Thomas Jefferson Lorad Catherine Piccoli, M.D.

Digital Mammography 185
tures of each patient’s breasts [9]. Of course, tools are avail-able already that allow on-line adjustment of the image sothe radiologist can better evaluate questionable areas inthe image. This might lead to fewer patient call-backs andbiopsies, as occurred in the large DOD screening trial, inwhich all images were interpreted in softcopy format [4].
While softcopy display holds great promise, the currentlyavailable products are not ideal. They are not fast or user-friendly enough. It is difficult to compare new digital ex-aminations to old film or digital examinations. It is notalways possible to import examinations from other ven-dors for display on the current monitor systems.
Image Processing
A recent IDMDG preference study suggested that dif-ferent clinical tasks, screening, and diagnosis, and differ-ent lesion types, calcifications and masses, will requiredifferent image presentations for optimal radiologist in-terpretation performance. In addition, radiologists preferdifferent image processing for each task and lesion typefor each machine type (Fischer vs. GE vs. Trex) [10].
This study used 28 Fischer, GE, and Lorad digitalmammograms, most with findings that had undergone bi-opsy, and all with at least one finding that was presumedbenign by virtue of stability. Twelve radiologists reviewedeight different versions of these same cases and ranked theimages according to their ability to depict the features ofthe lesion that best revealed the known diagnosis.
The results suggested that multiple presentations shouldbe utilized to gain the most information from digital mam-mography. In fact, at least three different presentations maybe useful for the same case. That is, radiologists interpret-ing mammograms may routinely want to view the imagesin a screening version, in a version suitable for the evalu-ation of calcifications, and in a version suitable for theevaluation of masses (Figs. 1,2) [10].
Given these results and others [11–13], the diagnosticaccuracy of digital mammography will likely depend bothon the type of machine utilized and on the processing meth-ods available for image display. If poor image processingselections are made, diagnostic accuracy might be dam-aged rather than improved with this new technology. Con-sequently, each company will have to determine whichsoftware algorithms to use to obtain the most clinicallyuseful information for patients.
CADD
CADD uses software to assist radiologists in interpret-ing mammograms. These programs have been applied todigitized patient images for traditional screen-film mam-mography. Available clinical data have definitively dem-onstrated that the diagnostic accuracy of radiologistsinterpreting screen-film mammograms can be improvedthrough the use of these programs, without a significant
effect on the number of patients recalled for additionalstudies [14–21].
As one might expect, a lot of work must be done to adaptthese methods to digital mammography. Of course, digitalmammograms will not have to be digitized to be evaluatedusing this “second opinion” software. Large numbers ofabnormal and normal digital mammograms are needed totrain the computer in how to distinguish abnormal areasfrom normal background and image noise. These cases willbe acquired by the CADD and digital mammography com-panies over the next few years. Each manufacturer is likelyto use its own CADD software, given that the image noiseis quite different across the different detector systems.
Fuji has already developed and tested a CADD productfor digital mammography, utilizing cases acquired in Ja-pan. Results with this system [22–24], evaluating 1,212digital mammograms with 240 cancers, revealed a 90.5%sensitivity with 1.3 false positives per image. Further test-ing of this product in North America is planned for thenear future.
Tomosynthesis and DSM
Tomosynthesis is an application being developed by GE.This technology provides precise motorized x-ray tubemotion that allows the acquisition of multiple images fo-cused at different levels within the breast. The planes aboveand below those levels are blurred, similar to the types ofimages provided by linear tomography. The entire imageset is then reconstructed in three dimensions. GE’stomosynthesis system, currently being tested as a proto-type at Massachusetts General Hospital, uses 7 to 10 im-age angles, with all images acquired at the same totalpatient dose as two-view conventional mammography. Ofcourse, with the blurring of the overlying image informa-tion, one would expect greater lesion surface character-ization and visualization of associated features, just as withother tomographic methods. Preliminary specimen imageshave been published and are quite promising [25]. A clini-cal trial of tomosynthesis, enrolling 400 patients recom-mended to undergo biopsy, is currently under way, fundedby the DOD.
DSM refers to the use of intravenous contrast in pa-tients undergoing digital mammography, with theprecontrast image electronically subtracted from thepostcontrast image. It is believed that this may be of valuein visualizing breast cancer better, particularly in gaugingthe extent of disease in patients at high risk for multicen-tricity, because of the increased vascularity of malignantlesions compared to normal breast tissue. Presumably, digi-tal mammography ought to allow detection of subtle dif-ferences in contrast uptake by tumors. This might beespecially useful in women with dense breasts, and in thosewith invasive lobular carcinoma, lesions that are especiallydifficult to fully characterize using traditional technology.

186 Pisano et al.
Images of small capillary beds in an in vivo rabbit modelutilizing the GE digital mammography detector systemhave been published [26].
SUMMARY
Digital mammography may ultimately improve breastcancer detection and diagnosis, but at this point there isinsufficient evidence to justify replacement of all tradi-tional film mammography systems, given the reduction inbreast cancer mortality that can be achieved with the stan-dard technology [27–29]. D-MIST, a large NCI screeningtrial getting under way in July 2001, will provide data re-garding the performance of this technology, and its cost-effectiveness. In addition, there is need for improvementin available image display methods. Clinical softcopyworkstations are somewhat difficult to use at present, andimage processing has not yet been optimized for eachmachine or for each clinical task. Future development ofadvanced digital mammography applications, such astomosynthesis and DSM, might allow for new ways ofimaging the breast that hold great promise for better pa-tient care.
REFERENCES1. Pisano ED, Yaffe M: Digital mammography. Breast Dis 1998;
10(3,4):127–136.2. Feig SA, Yaffe MJ. Current status of digital mammography. Semin
US CT MRI 1996;17(5):424–443.3. Lewin JM, Hendrick RE, D’Orsi CJ, et al: Comparison of full-field
digital mammography with screen-film mammography for cancerdetection: results of 4,945 paired examinations. Radiology2001;218(3):873–880.
4. Lewin JM, Hendrick RE, D’Orsi CJ, et al: Clinical evaluation of afull field digital mammography in a screening setting [Abstract].Radiology 2000;217(P):199.
5. Nields MW, Galaty Jr RR: Digital mammography: a model for as-sessing cost- effectiveness. Acad Radiol 1998;5 Suppl 2:S310–S313.
6. Report of the Joint Working Group on Telemammography/Teleradiology and Information Management. Washington, DC. AcadRadiol 1999;6 Suppl 7:S303–S324.
7. Hemminger BM, Dillon AW, Pisano ED, et al: Effect of displayluminance on the feature detection rates of masses in mammograms.Med Phys 1999;26(11):2266–2272.
8. Roehrig H, Krupinski E: Image quality of CRT displays and theeffect of brightness of diagnosis of mammograms. J Digit Imaging1998;11(3 Suppl 1):187–188.
9. Pisano ED, Cole EB, Hemminger BM, et al: Image processing al-gorithms for digital mammography: a pictorial essay. RadioGraphics2000;20:1479–1491.
10. Pisano ED, Cole EB, Major S, et al: Radiologists’ preferencesfor digital mammographic display. Radiology 2000:216(3):820–830.
11. Higashida Y, Morida N, Morita K, et al: Detection of subtle
microcalcifications: comparison of computed radiography andscreen-film mammography. Radiology 1992;183:483–486. 12.
12. Cowen AR, Brettle DS, Coleman NJ, et al: A preliminary investiga-tion of the imaging performance of photostimulable phosphor com-puted radiography using a new design of mammographic qualitycontrol test object. Br J Radiol 1992;65:528–535.
13. Oestmann JW, Kopans D, Hall DA, et al: A comparison of digitizedstorage phosphors and conventional mammography in the detec-tion of malignant microcalcifications. Invest Radiol 1988;23:725–728.
14. Burhenne LJ, Wood SA, D’Orsi CJ, et al: Potential contribution ofcomputer aided detection to screening mammography. Radiology2000;215:554–562.
15. Chan HP, Doi K, Galhorta S, et al: Image feature analysis and com-puter-aided diagnosis in digital radiography: automated detectionof microcalcifications in mammography. Med Phys 1987;14(4):538–547.
16. Chan HP, Vyborny CJ, MacMahon H, et al: Digital mammographyROC studies of the effects of pixel size and unsharp-mask filteringon the detection of subtle microcalcifications. Invest Radiol1987;22:581–589.
17. Yin F, Giger M, Doi K, et al: Computerized detection of masses indigital mammograms: analysis of bilateral subtraction images. MedPhys 1991;18(5):955–963.
18. Yin F, Giger ML, Doi K, et al: Comparison of bilateral-subtractionand single-image processing techniques in the computerized detec-tion of mammographic masses. Invest Radiol 1992;28(6):473–481.
19. Nishikawa RM, Giger ML, Doi K, et al: Computer-aided detectionof clustered microcalcifications using digital mammograms. MedBiol Engin Comput 1995;33:174–178.
20. Karssemeijer N, Te Brake GM: Detection of stellate distortions inmammograms. IEEE Trans Med Imaging 1996;15:611–619.
21. Roehrig J, Doi T, Hasegawa A, et al: Clinical results with R2imagechecker system. In Karresmeijer N, et al. (eds): “Digital mam-mography—Nijmegen, 1998.” Dordrecht: Kluwer Academic Pub-lishers; 1998; p. 395–400.
22. Kobatake H, Takeo H, Nawano S: Tumor detection system for full-field digital mammography [Abstract]. Proc SPIE Med Imaging 19973659.
23. Kobatake H, Takeo H, Nawano S: Tumor detection system for full-field digital mammography. In Karresmeijer N, et al. (eds): “Digi-tal mammography—Nijmegen, 1998.” Dordrecht: Kluwer AcademicPublishers; 1998; p. 87–94.
24. Kobatake H, Takeo H, Nawano S: Microcalcification detection sys-tem for full digital mammography. In Karresmeijer N, et al. (eds):“Digital mammography—Nijmegen, 1998.” Dordrecht: KluwerAcademic Publishers; 1998; p. 201–204.
25. Niklason LT, Christian BT, Niklason LE, et al: Digital tomosynthesisin breast imaging. Radiology 1997;205(2):399–406.
26. Niklason LT, Kopans D, Hamberg M: Breast imaging: tomosynthesisand digital subtraction mammography. Breast Dis 1998;10(3,4):151–164.
27. Nystrom L, Rutqvist LE, Wall S, et al: Breast cancer screening withmammography: overview of Swedish randomized trials. Lancet1993;342(8851):973-978.
28. Hendrick RE, Smith RA, Rutledge JH, et al: Benefit of screeningmammography in women ages 40–49: a new meta-analysis of ran-domized controlled trials. J Natl Cancer Inst Monogr 1997;22:87–92.
29. Tabar L, Vitak B, Chen H-H T, et al: Beyond randomized controlledtrials. Organized mammographic screening substantially reducesbreast carcinoma mortality. Cancer 2001;91(9):1724–1731.