Embed Size (px)
Citation preview
What Happens to Children Who Lose Public Health Insurance?
Presented byJanet B. Mitchell, Ph.D.Susan G. Haber, Sc.D.Sonja Hoover, M.P.P.
RTI International
Presented atChildren’s Health Services Research Annual Meeting
June 25, 2005Boston, MA
411 Waverley Oaks Road ■ Suite 330 ■ Waltham, MA 02452-8414
High Rates of SCHIP Disenrollment
Little is known about what happens to those children.
Even less is known about what happens to children who leave premium assistance programs.
Do these programs provide bridge to non-subsidized private health insurance?
If not, what happens to these children?
Oregon’s Twin Programs
Oregon has two programs to provide health insurance for low-income children: SCHIP Family Health Insurance Assistance Program (FHIAP), a premium
assistance program
Eligibility requirements are identical: <= 170% of FPL
Allowed us to compare outcomes for children disenrolled from the two programs Why did they leave the program? Did children transition to private health insurance, or did they
become uninsured? Were they able to access health care services?
Program Overview
SCHIP
Medicaid “look alike”
No premiums or copayments
Only children are covered
FHIAP
Covers entire family
Subsidy used for ESI or individual market health insurance
Family pays 5%-30% of premium, depending on income
Family pays all plan coinsurance amounts
Data
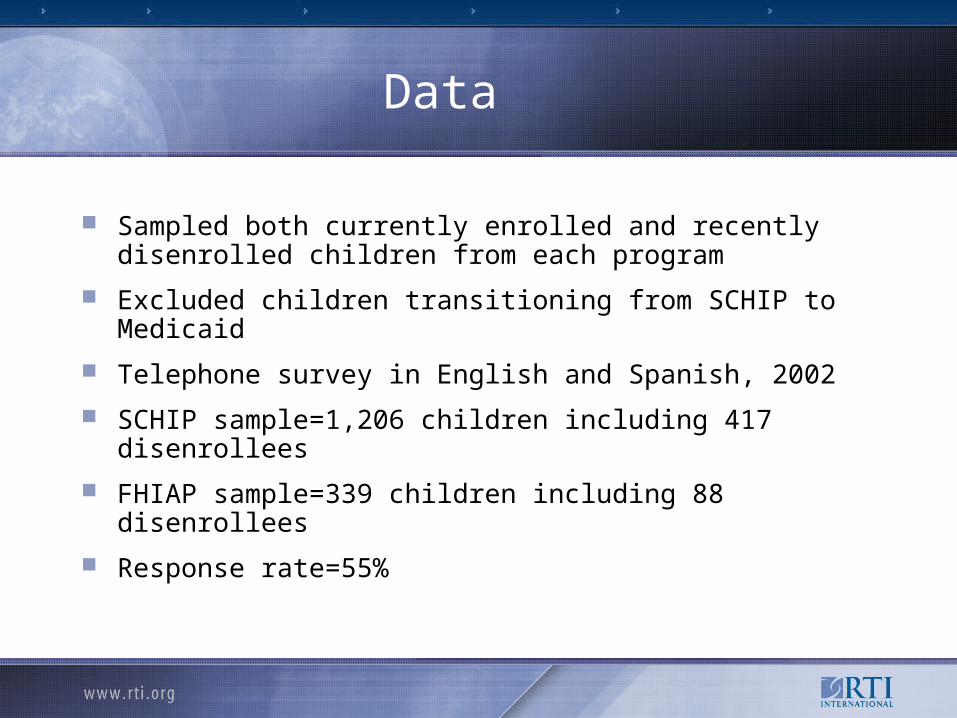
Sampled both currently enrolled and recently disenrolled children from each program
Excluded children transitioning from SCHIP to Medicaid
Telephone survey in English and Spanish, 2002
SCHIP sample=1,206 children including 417 disenrollees
FHIAP sample=339 children including 88 disenrollees
Response rate=55%
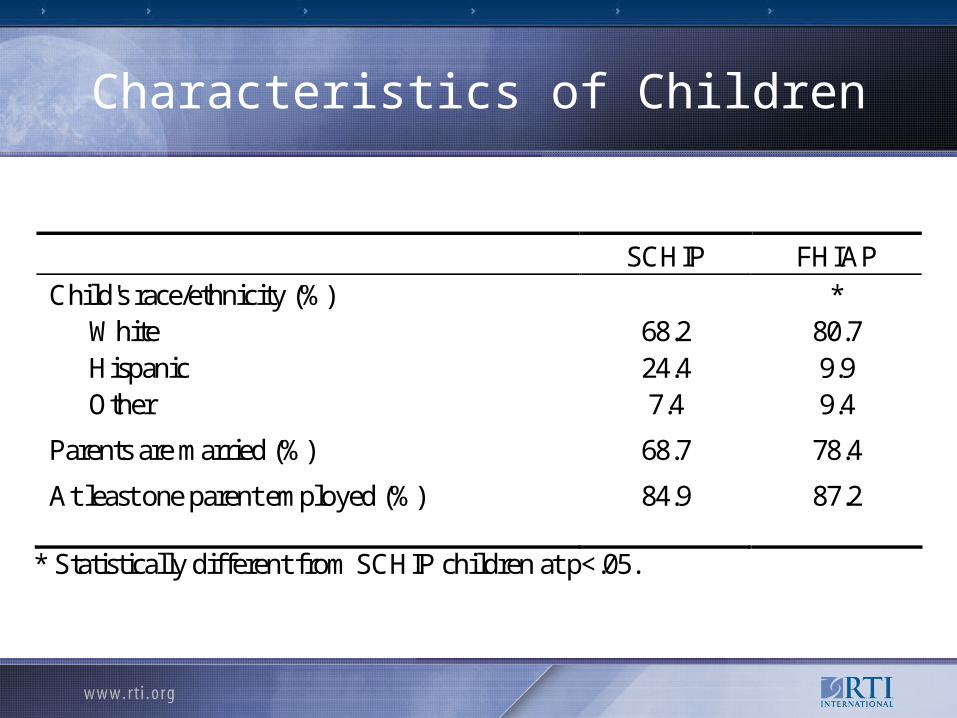
Characteristics of Children
SCHIP FHIAP Child's race/ethnicity (%) * White 68.2 80.7 Hispanic 24.4 9.9 Other 7.4 9.4
Parents are married (%) 68.7 78.4
At least one parent employed (%) 84.9 87.2
* Statistically different from SCHIP children at p<.05.
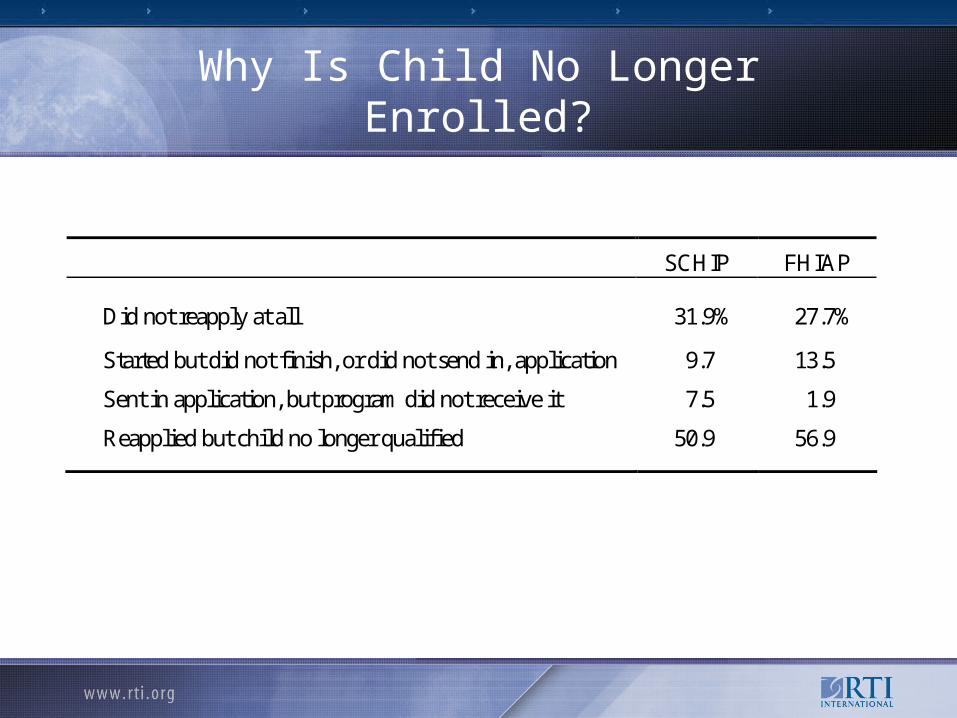
Why Is Child No Longer Enrolled?
SCHIP FHIAP
Did not reapply at all 31.9% 27.7%
Started but did not finish, or did not send in, application 9.7 13.5
Sent in application, but program did not receive it 7.5 1.9
Reapplied but child no longer qualified 50.9 56.9
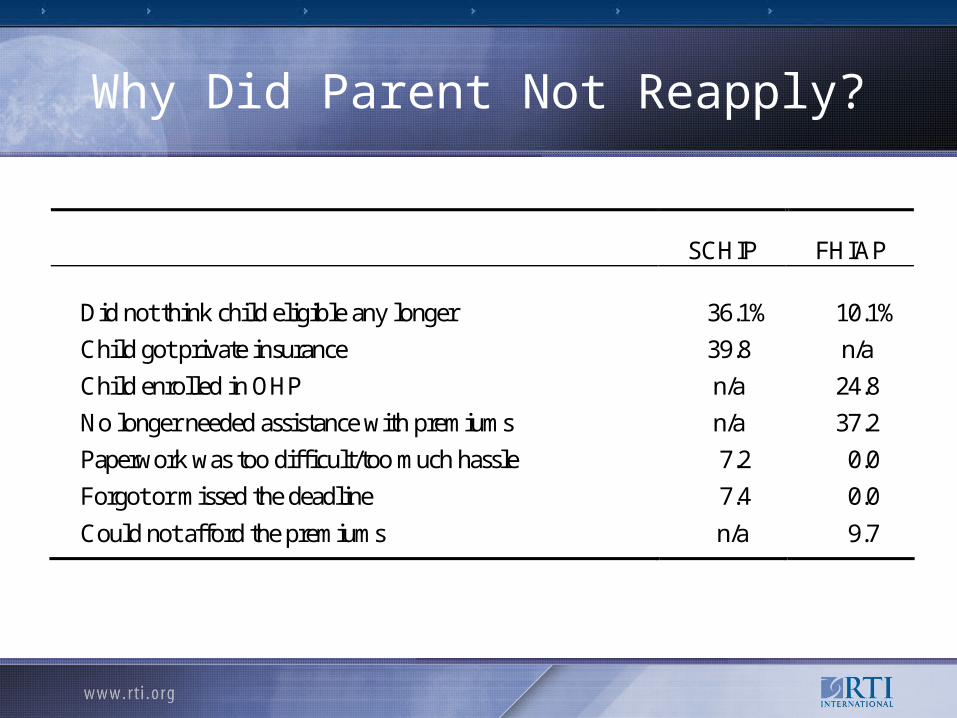
Why Did Parent Not Reapply?
SCHIP FHIAP
Did not think child eligible any longer 36.1% 10.1%
Child got private insurance 39.8 n/a
Child enrolled in OHP n/a 24.8
No longer needed assistance with premiums n/a 37.2
Paperwork was too difficult/too much hassle 7.2 0.0
Forgot or missed the deadline 7.4 0.0
Could not afford the premiums n/a 9.7
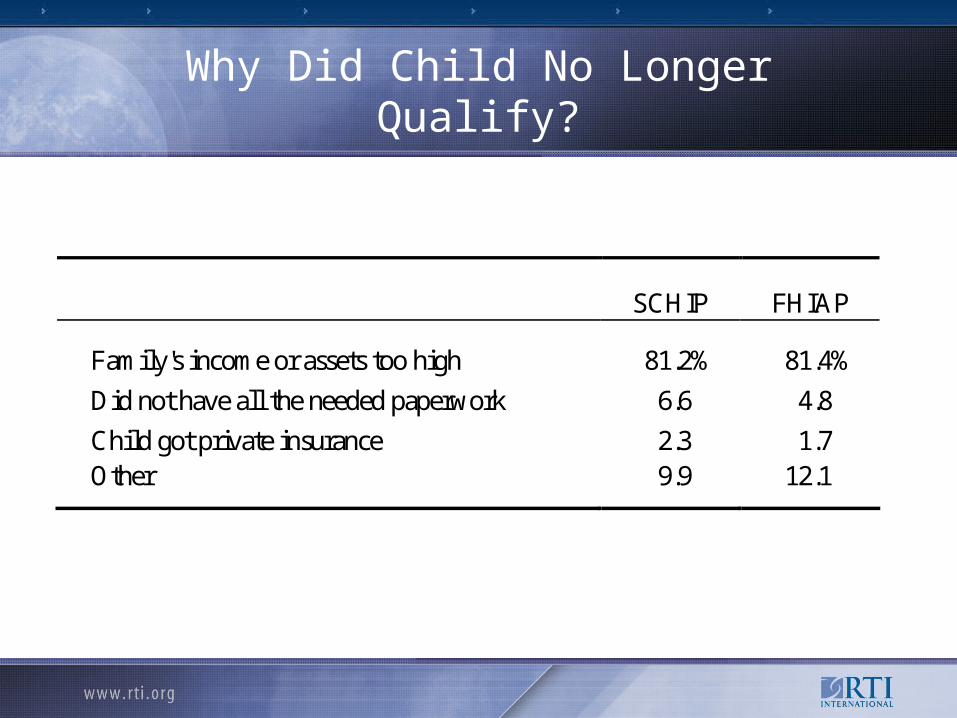
Why Did Child No Longer Qualify?
SCHIP FHIAP
Family's income or assets too high 81.2% 81.4%
Did not have all the needed paperwork 6.6 4.8
Child got private insurance 2.3 1.7 Other 9.9 12.1
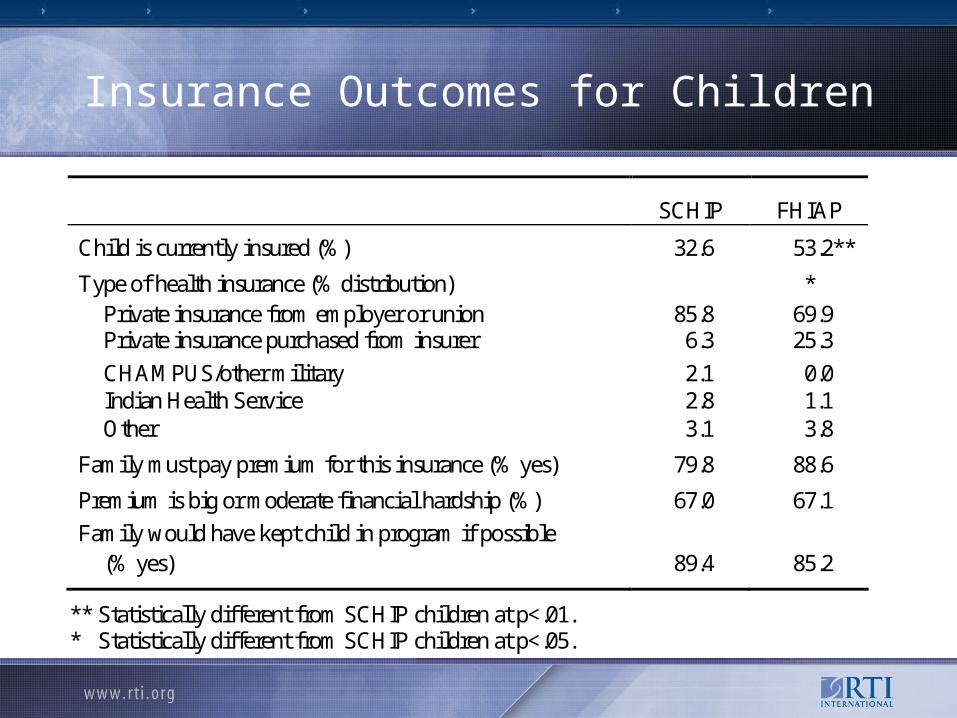
Insurance Outcomes for Children
SCHIP FHIAP
Child is currently insured (%) 32.6 53.2**
Type of health insurance (% distribution) * Private insurance from employer or union 85.8 69.9 Private insurance purchased from insurer 6.3 25.3
CHAMPUS/other military 2.1 0.0 Indian Health Service 2.8 1.1 Other 3.1 3.8
Family must pay premium for this insurance (% yes) 79.8 88.6
Premium is big or moderate financial hardship (%) 67.0 67.1
Family would have kept child in program if possible (% yes) 89.4 85.2
** Statistically different from SCHIP children at p<.01. * Statistically different from SCHIP children at p<.05.
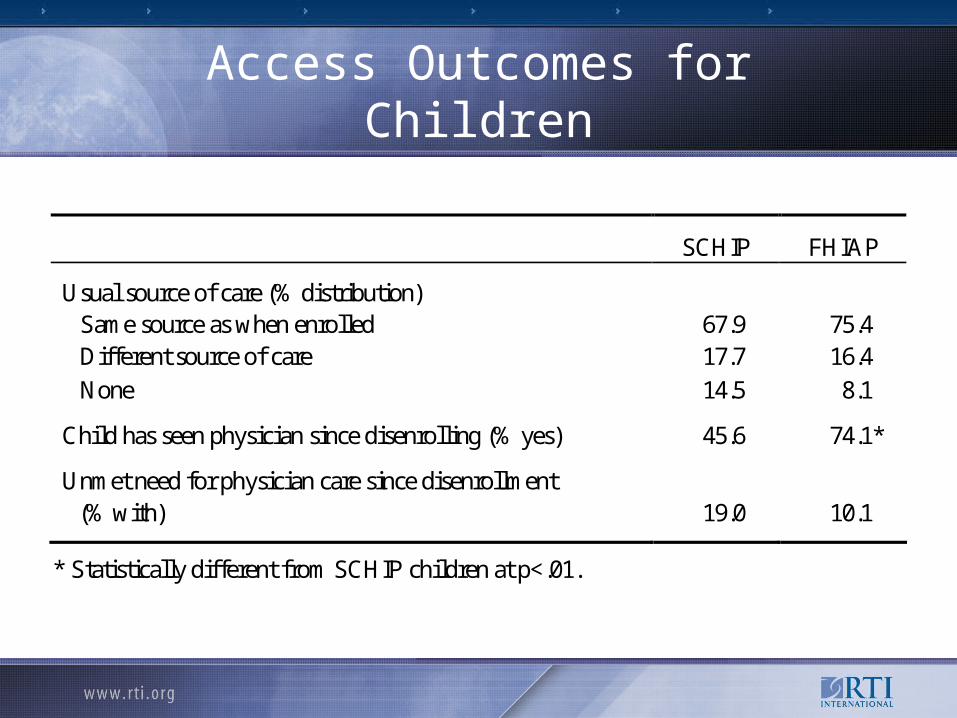
Access Outcomes for Children
SCHIP FHIAP
Usual source of care (% distribution) Same source as when enrolled 67.9 75.4 Different source of care 17.7 16.4
None 14.5 8.1
Child has seen physician since disenrolling (% yes) 45.6 74.1*
Unmet need for physician care since disenrollment (% with) 19.0 10.1
* Statistically different from SCHIP children at p<.01.
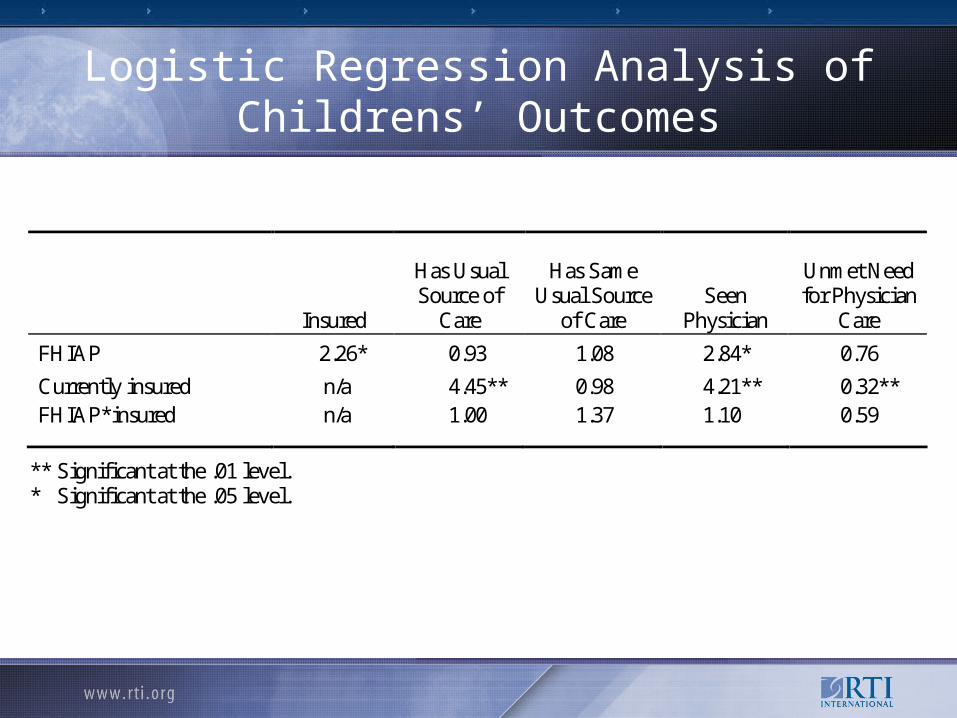
Logistic Regression Analysis of Childrens’ Outcomes
Insured
Has Usual Source of
Care
Has Same Usual Source
of Care Seen
Physician
Unmet Need for Physician
Care
FHIAP 2.26* 0.93 1.08 2.84* 0.76
Currently insured n/a 4.45** 0.98 4.21** 0.32** FHIAP*insured n/a 1.00 1.37 1.10 0.59
** Significant at the .01 level. * Significant at the .05 level.
Conclusions
Neither program provided a complete bridge to (non-subsidized) private health insurance.
While FHIAP disenrollees were more likely to be insured, absolute levels were low for both groups of children.
Loss of eligibility (real or perceived) was the primary reason for loss of public insurance coverage.
Becoming uninsured reduced access to care for all disenrolled children.
Policy Implications
Due to high premium costs and lack of access to ESI, many low-income working families are uninsured.
Policymakers may want to consider raising income eligibility ceiling for SCHIP and premium assistance programs.





























