Embed Size (px)
Citation preview

Caries Management by Risk Caries Management by Risk AssessmentAssessment ::
The Caries BalanceThe Caries Balance
John D.B. FeatherstoneJohn D.B. Featherstone
Professor and DeanProfessor and Dean
EE--mail [email protected] [email protected]
School of DentistrySchool of Dentistry
University of California San FranciscoUniversity of California San Francisco
DisclosureDisclosure
I have no personal financial interest in any I have no personal financial interest in any company relevant to this presentation. company relevant to this presentation.
I consult for, have consulted for, or have I consult for, have consulted for, or have done research funded or supported by:done research funded or supported by:
Arm and Hammer, Beecham, Cadbury, GSK, Arm and Hammer, Beecham, Cadbury, GSK,
KaVo, Novamin, Omnii Oral Pharmaceuticals, KaVo, Novamin, Omnii Oral Pharmaceuticals, Oral B, Philips Oralcare, Procter and Gamble, Oral B, Philips Oralcare, Procter and Gamble, 3M ESPE Preventive Care, Wrigley, and the 3M ESPE Preventive Care, Wrigley, and the
National Institutes of Health.National Institutes of Health.
Protective Factors
What is Dental Caries?What is Dental Caries?
�� Dental caries is tooth decay Dental caries is tooth decay
�� Specific bacteria (Streptococcus mutans, Specific bacteria (Streptococcus mutans, Streptococcus sobrinus, and lactobacilli) on Streptococcus sobrinus, and lactobacilli) on the tooth surface feed on carbohydrates and the tooth surface feed on carbohydrates and
make acids as waste productsmake acids as waste products
�� Acids travel into the tooth and dissolve Acids travel into the tooth and dissolve mineral mineral -- if mineral loss is not halted or if mineral loss is not halted or reversed a cavity is formedreversed a cavity is formed
�� Dental caries is a transmissible bacterial Dental caries is a transmissible bacterial
infectioninfection
Protective Factors
“White spot” lesion
Protective Factors
Frank occlusal
cavity

Protective Factors
Childhood
Caries
The Caries BalanceThe Caries BalanceProtective Factors
• Saliva flow and components
• Fluoride, Calcium, Phosphate:
remineralization
• Antibacterials:-
chlorhexidine, xylitol, new?
No CariesCaries
Pathological Factors
• Acid-producing bacteria
• Frequent eating/drinking of
fermentable carbohydrates
•Sub-normal saliva flow and
function
Featherstone, Community Dent Oral Epidem, 1999
Protective Factors
Stay in balance to survive
Pathological FactorsPathological Factors
�� Cariogenic bacteria: mutans streptococci Cariogenic bacteria: mutans streptococci ((S. mutans and S. sobrinus) S. mutans and S. sobrinus) and and lactobacillus specieslactobacillus species
�� Frequency of ingestion of fermentable Frequency of ingestion of fermentable carbohydrates: sucrose, glucose, carbohydrates: sucrose, glucose, fructose, cooked starchfructose, cooked starch
�� Reduced salivary function (medication Reduced salivary function (medication induced; radiation therapy; disease; induced; radiation therapy; disease; genetic)genetic)
Protective Factors
Acid producing bacteria are usually
less than 1 percent of the total flora in
the plaque
Scanning
Electron
Micrograph
of bacteria on
a tooth
surface

Streptococcus mutans culture showing active cell
division. S. sobrinus is similar. Sucrose leads to
extracellular polysaccharides that stick the
plaque together
Mutans StreptococciMutans Streptococci
This group of bacteria contains two primary species that appear in humans
�Streptococcus mutans - almost universal
�Streptococcus sobrinus - virulent, high risk
Both species produce acids and can live in
acid
Lactobacillus culture. Lactobacilli species produce
predominantly lactic acid from fermentable carbohydrates
What about
the clinical
relevance?
Does drilling
and filling
really fix
caries?
Clinical Study ResultsClinical Study ResultsNIH/NIDCR GrantNIH/NIDCR Grant
Caries Management By Risk Caries Management By Risk AssessmentAssessment19991999--2004 2004
Principal Investigator: Principal Investigator:
John Featherstone John Featherstone
CoCo--investigators: investigators:
Chuck Hoover, Stuart Gansky, Marcia RapozoChuck Hoover, Stuart Gansky, Marcia Rapozo--Hilo, Kim Tran, Hilo, Kim Tran, Joel White, Jane WeintraubJoel White, Jane Weintraub
Caries Management StudyCaries Management Study
S1
S3 S7S2
Baseline ObservationsSaliva SampleMS, LB and FRadiographs
DMFS1-7 cavities
Co
ntr
ol
Inte
rven
tio
n
Final ObservationsRadiographs
DMFS
Randomization
Restorations +Anti-bacterial
and Fluoride
Treatment
All Restorations
Complete
S2
S4-S6
Conventional Treatment Plan
Restorations
S3 S7
Final ObservationsRadiographs
DMFS
All Restorations
Complete
S4-S6
high low
2 Years
N=116
(CHX + F)
N=115

Decayed Surfaces vs. log MS and log LB
(Revised bacterial classifications 1-07)
High
Bacterial
Challenge
Baseline Bacterial
Levels vs Decay
Existing Cavity = High Risk
M ean (SE) logM S
0 1 2 3 4 5 6 70
1
2
3
4
5
Log MS Control
Log MS Intervention
Visit # - 6 month intervals
Chlorhexidine plus Fluoride
Restorations
Patients With Frank cavitiesPatients With Frank cavities
� One or more frank cavities indicates high risk for future new carious lesions
� Moderate to high levels of mutans streptococci
� Moderate to high levels of lactobacilli
� Patients have a high bacterial challenge that most likely can not be completely overcome by fluoride alone
�� Placing restorations does not reduce the Placing restorations does not reduce the bacterial loading in the rest of the mouthbacterial loading in the rest of the mouth
∆∆∆∆DMFS (SE)24% reduction (p=0.02)
Control Intervention0
1
2
3
4
5
Would you put a new roof on while the house is burning?
Placing a restoration does not significantly reduce the
bacterial loading in the remainder of the mouth.
Caries is a Transmissible Caries is a Transmissible Bacterial InfectionBacterial Infection
� Time for a paradigm shift
� Children infected by mother, caregiver, siblings
� Fluoride is effective only up to a point
� High bacterial challenge can not be completely overcome
� Placing “fillings” has little effect on cariogenic bacterial loading in the mouth
� Need to deal with the infection

First Colonizable Hard Surface. First Colonizable Hard Surface. Soft tissues can also be colonized Soft tissues can also be colonized
beforebefore teeth erupt.teeth erupt.
Pathological FactorsPathological Factors
�� Cariogenic bacteria: mutans streptococci Cariogenic bacteria: mutans streptococci ((S. mutans and S. sobrinus) S. mutans and S. sobrinus) and and lactobacillus specieslactobacillus species
�� Frequency of ingestion of fermentable Frequency of ingestion of fermentable carbohydrates: sucrose, glucose, carbohydrates: sucrose, glucose, fructose, cooked starchfructose, cooked starch
�� Reduced salivary function (medication Reduced salivary function (medication induced; radiation therapy; disease; induced; radiation therapy; disease; genetic)genetic)
+
Demineralization:-Step 1
Cariogenic
Bacteria
S. Mutans
S. Sobrinus
Lactobacilli
Fermentable
Carbohydrates
Sucrose
Glucose
Fructose
Cooked starch
Organic Acids
Which penetrate enamel and
dentin
Dissolve tooth mineral
Protective Factors
Cariogenic foods contain fermentable
carbohydrates such as sucrose,
glucose, fructose and cooked starch
NonNon--cariogenic Sweetenerscariogenic Sweeteners
�� SorbitolSorbitol
�� AspartameAspartame
�� SaccharinSaccharin
�� Sodium cyclamateSodium cyclamate
�� XylitolXylitol
Pathological FactorsPathological Factors
�� Cariogenic bacteria: mutans streptococci Cariogenic bacteria: mutans streptococci ((S. mutans and S. sobrinus) S. mutans and S. sobrinus) and and lactobacillus specieslactobacillus species
�� Frequency of ingestion of fermentable Frequency of ingestion of fermentable carbohydrates: sucrose, glucose, carbohydrates: sucrose, glucose, fructose, cooked starchfructose, cooked starch
�� Reduced salivary function (medication Reduced salivary function (medication induced; radiation therapy; disease; induced; radiation therapy; disease; genetic)genetic)

Male, 55 years old, before
radiation to the head and neck
for cancer treatment. Causes
saliva flow and function to be
cut by at least 90%
Same male, after radiation
to the head and neck. Six
months later, showing
rampant decay and massive
destruction of the teeth
Protective factorsProtective factors
�� Salivary components and flowSalivary components and flow
�� Fluoride, calcium and phosphate: Fluoride, calcium and phosphate: remineralizationremineralization
�� Antibacterials from extrinsic sourcesAntibacterials from extrinsic sources
Saliva Contains Numerous Saliva Contains Numerous Important ComponentsImportant Components
�� Calcium, phosphate and fluorideCalcium, phosphate and fluoride
�� Proteins and lipids that form the pellicle Proteins and lipids that form the pellicle that protects the tooth surfacethat protects the tooth surface
�� Proteins that keep calcium in solution Proteins that keep calcium in solution --they maintain supersaturationthey maintain supersaturation
�� Buffers: bicarbonate, phosphate, Buffers: bicarbonate, phosphate, peptidespeptides
�� Antibacterial substances & Antibacterial substances & immunoglobulinsimmunoglobulins
Protective factorsProtective factors
�� Salivary components and flowSalivary components and flow
�� Fluoride, calcium and phosphate: Fluoride, calcium and phosphate: remineralizationremineralization
�� Antibacterials from extrinsic sourcesAntibacterials from extrinsic sources
+
Demineralization:-Step 2
If fluoride is present in the If fluoride is present in the
solution between the solution between the
crystals it inhibits mineral crystals it inhibits mineral lossloss
Organic
Acids
Dental Mineral =
Carbonated
Hydroxyapatite
Acid soluble
Demineralization
Calcium and phosphate into
solution
Protective Factors
Scanning Electron Microscope image of
Normal Enamel Surface

Protective Factors
SEM of enamel
surface 60,000X,
showing crystal ends
Transmission Electron
Microscope image of enamel
cross-section at 60,000X
showing individual crystals
and the prism (rod) boundary
Protective Factors
Acid-damaged enamel crystals from a carious lesion at
3,000,000x showing rows of calcium atoms. Hexagonal
white patches (arrows) are where acid has dissolved
mineral from calcium deficient/carbonate rich regions.
Dissolved
regions
Water amongst
the crystals
Dr. Fluoride
protects against
mineral loss
Water
amongst
the
crystals
+
Remineralization/Tooth Repair
Fluoride speeds up remineralization ->
less soluble mineral
Calcium
in tooth
water
(from
saliva)
Phosphate
in tooth
water (from
saliva)
Remineralization
Builds on existing crystal remnants
New mineral less soluble
Fluoride helps
Dr. Fluoride speeds
up remineralization
and makes acid
resistant mineral
Demineralized surface blocks need to be replaced
with new calcium, phosphate and fluoride to make
a more acid resistant surface on the crystal

SEM in the body of a carious lesion (~ 30,000x)
showing remaining crystal remnants awaiting
remineralization
Sound enamel crystal (3,000,000x) dissected
from inner enamel showing carbonate rich acid
soluble regions (white patches).
Enamel crystal after remineralization with calcium,
phosphate and fluoride, showing a well-formed, low
solubility, fluorapatite-like veneer overlying the
original defective crystal
Calcium and phosphate are cemented in
place by fluoride providing a new stable wall
Enamel/dentin
crystal =
Carbonated apatite
Partly dissolved
crystal
Crystal
nucleus
ACID
Acid resistantAcid resistant
CaCa10 10 (PO(PO44))6 6 (F)(F)22 = =
fluorapatitefluorapatite--likelikecoating on crystalscoating on crystals
RemineralizationCalcium +
Phosphate
+ Fluoride
Fluoride works primarily via Fluoride works primarily via topical mechanismstopical mechanisms
�� Fluoride inhibits demineralization by Fluoride inhibits demineralization by adsorbing from solution onto tooth adsorbing from solution onto tooth mineral crystal surfacesmineral crystal surfaces
�� Fluoride enhances remineralization Fluoride enhances remineralization
by combining with calcium and by combining with calcium and phosphate to make a “fluorapatitephosphate to make a “fluorapatite--like” remineralized veneer like” remineralized veneer
Protective Factors
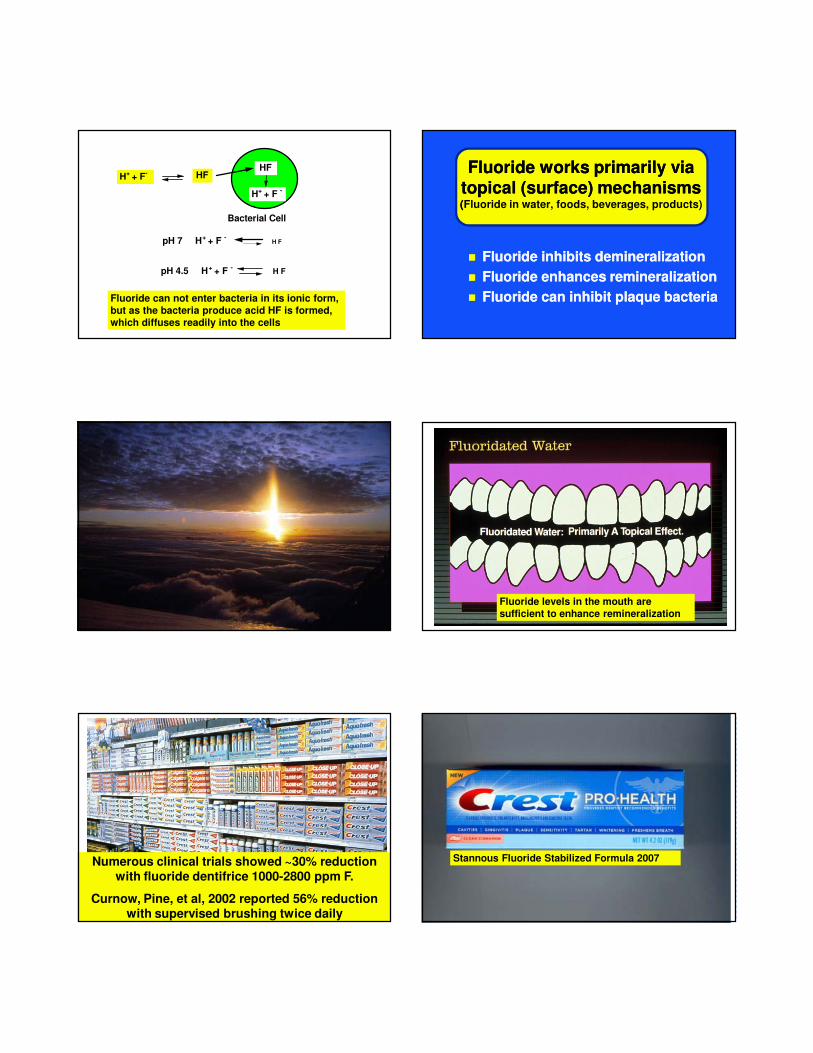
H+ + F- HF
HF
H+ + F -
Bacterial Cell
pH 7 H+ + F - H F
pH 4.5 H+ + F - H F
Fluoride can not enter bacteria in its ionic form,
but as the bacteria produce acid HF is formed,
which diffuses readily into the cells
�� Fluoride inhibits demineralizationFluoride inhibits demineralization
�� Fluoride enhances remineralizationFluoride enhances remineralization
�� Fluoride can inhibit plaque bacteriaFluoride can inhibit plaque bacteria
Fluoride works primarily via Fluoride works primarily via topical (surface) mechanismstopical (surface) mechanisms((Fluoride in water, foods, beverages, products)
Protective Factors
Fluoride levels in the mouth are
sufficient to enhance remineralization
Protective Factors
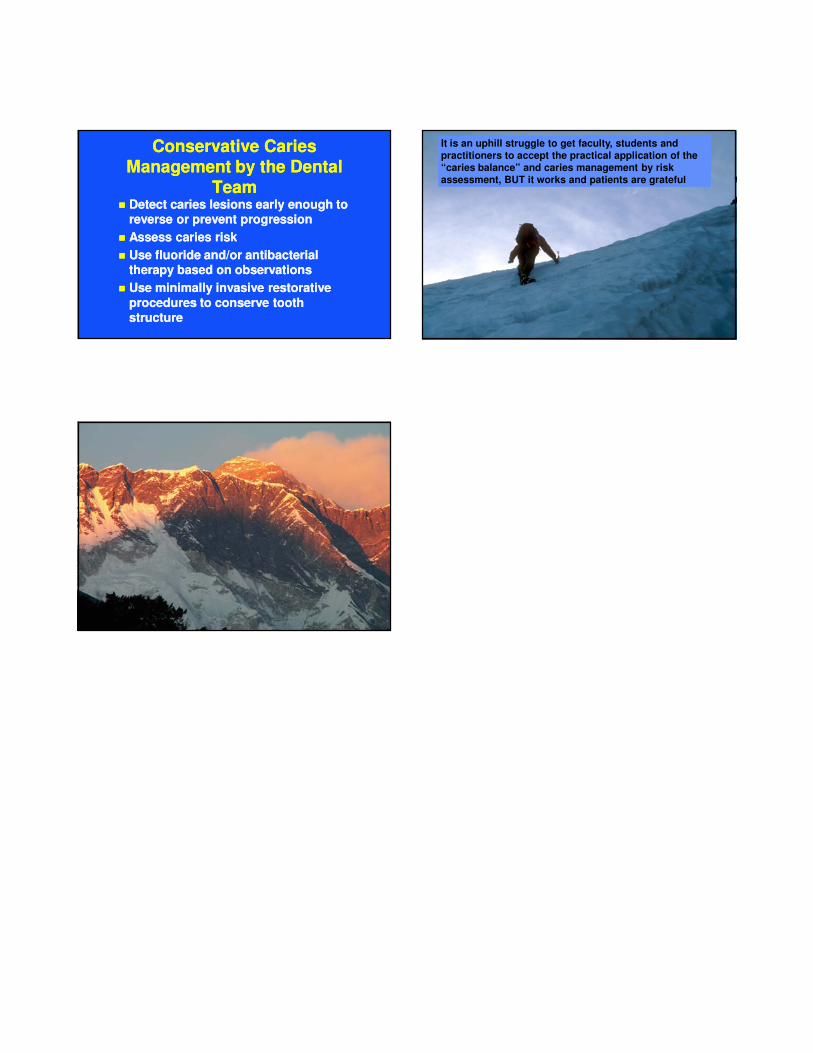
Numerous clinical trials showed ~30% reduction with fluoride dentifrice 1000-2800 ppm F.
Curnow, Pine, et al, 2002 reported 56% reduction with supervised brushing twice daily
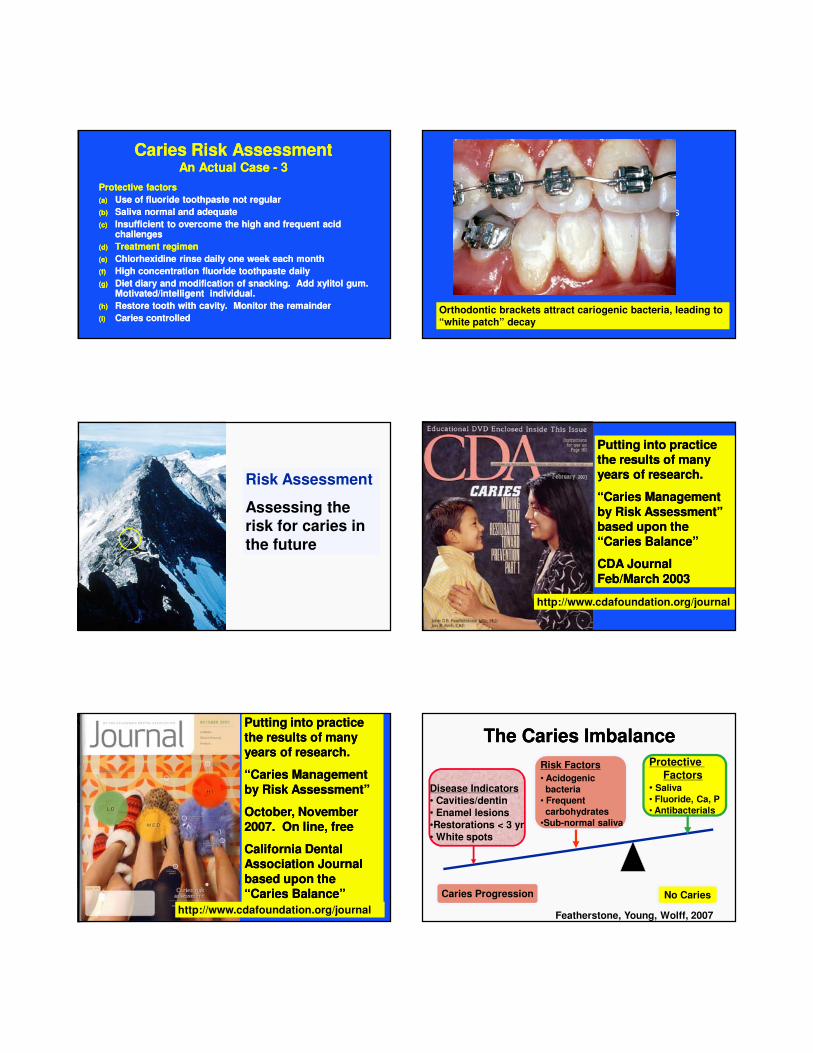
Orthodontic brackets attract cariogenic bacteria, leading to
“white patch” decay
Stannous Fluoride Stabilized Formula 2007

Over the counter fluoride rinses (0.05% NaF) are very effective in high caries risk patients when used once or twice daily for one minute, plus a
fluoride-containing dentifrice. O’Reilly and Featherstone, 1987
OfficeOffice--Applied Fluoride ProductsApplied Fluoride ProductsGel (Gel (>> 5,000 ppm F)5,000 ppm F)
and Fluoride Varnishand Fluoride Varnish�� Do not require continuing patient Do not require continuing patient
compliancecompliance
�� Forms slowly soluble calcium fluorideForms slowly soluble calcium fluoride--like like deposits in lesions and the plaquedeposits in lesions and the plaque
�� Gives slow release fluoride for several Gives slow release fluoride for several
weeksweeks
�� Three times a year for high risk patientsThree times a year for high risk patients
Evidence-based Clinical Recommendations:Professionally Applied Topical FluorideThe Council on Scientific Affairs, American
Dental AssociationMay, 2006
� Fluoride gel applied for 4 minutes or more is
effective� Fluoride varnish applied every 6 months is
effective
� Two or more applications of fluoride varnish per year are effective in high caries risk individuals
� Office topical applications no added benefit for low
risk individuals
Protective Factors
Weintraub et al, J Dent Res, 2006. Fluoride
varnish in infants (approx 2 years old at start)
Caries Incidence Infants Over 2 years
0 1 2 30
5
10
15
20
25
30
35
40
45
Fluoride Varnish Applications
Fluoride Varnish for High Risk of All Ages
White “Vanish” Varnish – 3M ESPE Prev Care
High fluoride concentration (5,000 High fluoride concentration (5,000 ppm F) toothpaste more effective ppm F) toothpaste more effective
than 1100 ppm F in high risk than 1100 ppm F in high risk individualsindividuals
Baysan A et al, Caries Res 2001. 5000 ppm F Baysan A et al, Caries Res 2001. 5000 ppm F toothpaste gave statistically significant extra toothpaste gave statistically significant extra reduction in root caries compared to 1100 reduction in root caries compared to 1100
ppm F toothpaste.ppm F toothpaste.
However, caries progression still occurred in However, caries progression still occurred in many subjects even with high concentration many subjects even with high concentration fluoride usefluoride use

High concentration fluoride products for high risk patients. Proven effective for root caries.
Conclusions Conclusions -- FluorideFluoride
�� The antiThe anti--caries effects of fluoride are caries effects of fluoride are primarily topical (surface) in plaqueprimarily topical (surface) in plaque
�� The systemic benefits of fluoride are The systemic benefits of fluoride are minimal minimal
�� Therapeutic levels of F can be achieved Therapeutic levels of F can be achieved
from drinking water and fluoride productsfrom drinking water and fluoride products
�� Fluoride therapy may not overcome a high Fluoride therapy may not overcome a high bacterial challengebacterial challenge
Calcium Phosphopeptide: Calcium Phosphopeptide: CPP/ACPCPP/ACP
Eric Reynolds Eric Reynolds -- Australia Australia
Background and mechanism
Laboratory studies: Three decades
Clinical Studies: clinical evidence
Representation of a proposed Representation of a proposed CPPCPP--ACP complexACP complex
Cross et al. 2007 Curr Pharm Des,
Conclusions Conclusions
�� Limited calcium and phosphate in Limited calcium and phosphate in individuals with reduced salivary function individuals with reduced salivary function is a common problemis a common problem
�� Calcium and phosphate delivery can be Calcium and phosphate delivery can be enhanced to improve remineralizationenhanced to improve remineralization
�� Great need for novel improved Great need for novel improved remineralization methods to better alter remineralization methods to better alter the “caries balance”, especially in the “caries balance”, especially in individuals with high bacterial challengeindividuals with high bacterial challenge
�� MI paste, MI Paste Plus (with fluoride)MI paste, MI Paste Plus (with fluoride)

The Caries BalanceThe Caries Balance
Protective Factors• Saliva flow and components
• Fluoride, calcium, phosphate:-
remineralization
• Antibacterials:- chlorhexidine,
xylitol, new?
No CariesCaries
Pathological Factors
• Acid-producing bacteria
• Frequent eating/drinking
of fermentable carbohydrates
• Sub-normal saliva flow and
function
Protective factorsProtective factors
�� Salivary components and flowSalivary components and flow
�� Fluoride, calcium and phosphate: Fluoride, calcium and phosphate: remineralizationremineralization
�� Antibacterials from extrinsic sourcesAntibacterials from extrinsic sources
Protective Factors
Biofilm Modification is necessary as part of our therapy for high bacterial challenge
individuals. Caries is a transmissible
bacterial infection
Caries is a Transmissible Caries is a Transmissible Bacterial InfectionBacterial Infection
�� Multiple acidMultiple acid--producing species of bacteria are producing species of bacteria are responsibleresponsible
�� Children are infected by mothers, careChildren are infected by mothers, care--givers, givers, siblings, playmates, through saliva transfer siblings, playmates, through saliva transfer
�� Babies and infants are most susceptible from birth Babies and infants are most susceptible from birth to about 4 years of ageto about 4 years of age
�� Children infected early have more cavities later in Children infected early have more cavities later in lifelife
�� Need to break the chain of infection and deal with Need to break the chain of infection and deal with the bacteriathe bacteria
Similarity of bacteriocins of Similarity of bacteriocins of S. S. mutansmutans from mother and infantfrom mother and infant
R.J. Berkowitz and H.V. Jordan
Archs. Oral Biol. 20:725-730, 1975
Demonstrated the likelihood of Demonstrated the likelihood of transmission from mother to childtransmission from mother to child
Oral colonization of S. mutans Oral colonization of S. mutans in Sixin Six--monthmonth--old Predentate old Predentate
InfantsInfants
A.K.L. Wan, W.K. Seow, et al.
J.Dent Res. 80:2060-2065,2001
� Showed that S.mutans colonized even before teeth erupted (50% of infants).
� Related to high S. mutans in mothers, increased frequency of sugar intake, breast feeding and habits with saliva transfer from mother to child
Chlorhexidine Gluconate 0.12%, 10 ml, daily for 1
week reduces MS markedly and LB somewhat after
restorations completed. Repeat every month.
�� Chlorhexidine was effective at reducing Chlorhexidine was effective at reducing the bacterial challenge in high caries risk the bacterial challenge in high caries risk individuals even when compliance was individuals even when compliance was problematicproblematic
�� Preferred regimen is once a day rinse for Preferred regimen is once a day rinse for one week every month for a yearone week every month for a year
�� Monitor success by bacterial testingMonitor success by bacterial testing
�� Ideally we need a better antibacterial Ideally we need a better antibacterial therapy therapy
�� Must combine with remin/fluorideMust combine with remin/fluoride
What about What about toddlers/preschoolers?toddlers/preschoolers?
�� No good antibacterial vehicle available for No good antibacterial vehicle available for
toddlers toddlers -- chlorhexidine has negativeschlorhexidine has negatives
�� Chewing xylitol gum inappropriate & mints Chewing xylitol gum inappropriate & mints
might be aspiratedmight be aspirated
�� Xylitol wipes? Xylitol wipes? -- Spiffies: Unpublished data Spiffies: Unpublished data show caries reduction over one year in infantsshow caries reduction over one year in infants
�� Enlist the mothers and caregiversEnlist the mothers and caregivers
XylitolXylitol
�� Xylitol is a 5 carbon “sugar alcohol”Xylitol is a 5 carbon “sugar alcohol”
�� It looks like sucrose and has about the same It looks like sucrose and has about the same sweetness by weightsweetness by weight
�� It is used in some foods, chewing gum, candies, It is used in some foods, chewing gum, candies, lozenges, and dental products as a sweetenerlozenges, and dental products as a sweetener
�� Cariogenic (caries causing) bacteria can not feed Cariogenic (caries causing) bacteria can not feed on iton it
�� Humans can feed on it and use it as an energy Humans can feed on it and use it as an energy source source
�� It inhibits the transfer of bacteria from person to It inhibits the transfer of bacteria from person to person by altering the way the bacteria stick to person by altering the way the bacteria stick to surfacessurfaces
Influence of maternal xylitol Influence of maternal xylitol consumption on acquisition of consumption on acquisition of
mutans streptococci by infantsmutans streptococci by infants
E. Soderling, P. Pienihakkinen, J. Tenovuo
J. Dent. Res. 79:882-887, 2000
Use of xylitol gum by mothers reduced Use of xylitol gum by mothers reduced colonization in infants.colonization in infants.
Xylitol was better than chlorhexidine varnish, which was better than fluoride varnish
Parallel study showed marked caries reductions Parallel study showed marked caries reductions after 5 years (10 year results still hold up)after 5 years (10 year results still hold up)
Treat the mother or Treat the mother or caregiver to reduce caries in caregiver to reduce caries in
the childthe child�� Mother or caregiver with active Mother or caregiver with active
caries must be taken care ofcaries must be taken care of
�� Chlorhexidine rinses during 3rd Chlorhexidine rinses during 3rd trimester continuing after birthtrimester continuing after birth
�� Fluoride therapy to control the decayFluoride therapy to control the decay
�� 44--5 g/day xylitol chewing gum for 5 5 g/day xylitol chewing gum for 5
minutes each time and/or mints.minutes each time and/or mints.

XylitolXylitol
�� Xylitol chewing gum use enhances Xylitol chewing gum use enhances remineralizationremineralization
�� It inhibits the transfer of bacteria from It inhibits the transfer of bacteria from person to person by altering the way the person to person by altering the way the bacteria stick to surfacesbacteria stick to surfaces
�� It inhibits future recolonizationIt inhibits future recolonization
Xylitol Gum, MintsXylitol Gum, Mints
XylitolXylitol
�� Noncariogenic sweetenerNoncariogenic sweetener
�� Inhibits transfer of bacteria Inhibits transfer of bacteria
from mother to childfrom mother to child
�� Can reduce loading of Can reduce loading of
cariogenic bacteria in the cariogenic bacteria in the mouthmouth
XylitolXylitolPeter Milgrom Peter Milgrom -- University University
of Washington of Washington
Caries response is dose dependent
Gummy bears successful as a delivery vehicle
A Few Xylitol Gum SourcesA Few Xylitol Gum Sources
�� Epic. http://www.epicdental.com/departments.aspEpic. http://www.epicdental.com/departments.asp
You can buy gums and mints from this company, including You can buy gums and mints from this company, including dispensers.dispensers.
�� Omni Preventive Care 3M ESPE. Office and home care Omni Preventive Care 3M ESPE. Office and home care products. products. http://solutions.3m.com/wps/portal/3M/en_US/preventivehttp://solutions.3m.com/wps/portal/3M/en_US/preventive--care/home/care/home/
�� Zellies. Ellie has the full range plus educational materials. Zellies. Ellie has the full range plus educational materials. http://www.zellies.comhttp://www.zellies.com
�� Spry is another company that markets gum and mints to Spry is another company that markets gum and mints to dental officesdental offices
http://www.homesteadmarket.com/xylitol_mints.htmlhttp://www.homesteadmarket.com/xylitol_mints.html
Use The Caries Use The Caries Balance to Balance to Assess the RiskAssess the Risk

The Caries BalanceThe Caries BalanceProtective Factors
• Saliva flow and components
• Fluoride, calcium, phosphate:
remineralization
• Antibacterials:-
chlorhexidine, xylitol, new?
No CariesCaries
Pathological Factors
• Acid-producing bacteria
• Frequent eating/drinking of
fermentable carbohydrates
•Sub-normal saliva flow and
function
Sometimes there is a
delicate balance
Caries Risk Assessment Caries Risk Assessment An Actual Case An Actual Case -- 11
21 year old female referred by general dentist
(a)(a) First cavity of her lifeFirst cavity of her life
(b)(b) Numerous interproximal lesions on radiographs, Numerous interproximal lesions on radiographs,
several into dentinseveral into dentin
(c)(c) Apparently good oral hygieneApparently good oral hygiene
(d)(d) College student living in an apartmentCollege student living in an apartment
(e)(e) White patches observed White patches observed -- Orthodontic treatment Orthodontic treatment
completed three years beforecompleted three years before
(f)(f) Did bacteria test Did bacteria test –– Ivoclar/Vivadent CRT Ivoclar/Vivadent CRT
Mixed saliva is added to
the two sided selective
media slide (mutans
streptococci and
lactobacilli)
Incubate for 72
hours and read
versus density
scale
Vivadent Test Strips. An actual case. Used to
measure mutans streptococci and lactobacilli
Caries Risk Assessment Caries Risk Assessment An Actual Case An Actual Case -- 22
Pathological factors
(a)(a) Mutans streptococci and lactobacilli very highMutans streptococci and lactobacilli very high
(b)(b) Frequent (greater than 3 times) between meal Frequent (greater than 3 times) between meal snacks of sugars/cooked starch snacks of sugars/cooked starch -- college student college student not eating regular mealsnot eating regular meals
(c)(c) No saliva reducing factors: 1) medications, 2) No saliva reducing factors: 1) medications, 2) radiation to the head and neck, 3) systemic radiation to the head and neck, 3) systemic reasonsreasons
(d)(d) Saliva flow normal (approximately 2.0 ml/min)Saliva flow normal (approximately 2.0 ml/min)
(e)(e) Previously appliances present Previously appliances present -- orthodontic orthodontic bracketsbrackets
Caries Risk Assessment Caries Risk Assessment An Actual Case An Actual Case -- 33
Protective factorsProtective factors
(a)(a) Use of fluoride toothpaste not regularUse of fluoride toothpaste not regular
(b)(b) Saliva normal and adequate Saliva normal and adequate
(c)(c) Insufficient to overcome the high and frequent acid Insufficient to overcome the high and frequent acid challengeschallenges
(d)(d) Treatment regimenTreatment regimen
(e)(e) Chlorhexidine rinse daily one week each monthChlorhexidine rinse daily one week each month
(f)(f) High concentration fluoride toothpaste dailyHigh concentration fluoride toothpaste daily
(g)(g) Diet diary and modification of snacking. Add xylitol gum. Diet diary and modification of snacking. Add xylitol gum. Motivated/intelligent individual.Motivated/intelligent individual.
(h)(h) Restore tooth with cavity. Monitor the remainderRestore tooth with cavity. Monitor the remainder
(i)(i) Caries controlled Caries controlled
Protective Factors
Orthodontic brackets attract cariogenic bacteria, leading to
“white patch” decay
Risk Assessment
Assessing the risk for caries in
the future
Putting into practice Putting into practice the results of many the results of many years of research. years of research.
“Caries Management “Caries Management
by Risk Assessment” by Risk Assessment” based upon the based upon the “Caries Balance”“Caries Balance”
CDA Journal CDA Journal
Feb/March 2003Feb/March 2003
http://www.cdafoundation.org/journal
Putting into practice Putting into practice the results of many the results of many years of research. years of research.
“Caries Management “Caries Management
by Risk Assessment”by Risk Assessment”
October, November October, November 2007. On line, free2007. On line, free
California Dental California Dental Association Journal Association Journal
based upon the based upon the “Caries Balance”“Caries Balance”
http://www.cdafoundation.org/journal
The Caries ImbalanceThe Caries Imbalance
Protective
Factors• Saliva
• Fluoride, Ca, P
• Antibacterials
No CariesCaries Progression
Risk Factors
• Acidogenic
bacteria
• Frequent
carbohydrates
•Sub-normal saliva
Disease Indicators
• Cavities/dentin
• Enamel lesions
•Restorations < 3 yr
• White spots
Featherstone, Young, Wolff, 2007

Barriers to CAMBRA ImplementationBarriers to CAMBRA Implementation
�� Up front cost to patientsUp front cost to patients
�� Lack of insurance coverageLack of insurance coverage
�� Practitioners and patients do not have Practitioners and patients do not have therapeutic measures in their mind as part of therapeutic measures in their mind as part of the treatment planthe treatment plan
�� Insufficient trainingInsufficient training
�� Lack of acceptance by traditionally trained Lack of acceptance by traditionally trained
clinicians clinicians -- afraid of the unknownafraid of the unknown
�� Lack of willingness to make the changeLack of willingness to make the change
Caries Risk assessment Caries Risk assessment (Age 6 years and older/adult) (Age 6 years and older/adult) -- 11
1. Disease Indicators = Clinical Observations1. Disease Indicators = Clinical Observations
(a)(a) Visible cavities present Visible cavities present
(b)(b) Caries restored in last 3 yearsCaries restored in last 3 years
(c)(c) Interproximal caries lesions/radiolucenciesInterproximal caries lesions/radiolucencies
(d)(d) White spots on enamel surfacesWhite spots on enamel surfaces
Any one of these signals a bacteria test for MS and Any one of these signals a bacteria test for MS and LBLB
These are all clinical observations that tell us These are all clinical observations that tell us nothing about the cause of the disease nothing about the cause of the disease -- they they indicate presence of diseaseindicate presence of disease
Caries Risk assessment Caries Risk assessment (Age 6 years and older/adult) (Age 6 years and older/adult) -- 22
2. Risk Factors (Biological determinants of caries risk)2. Risk Factors (Biological determinants of caries risk)
(a)(a) MS and LB medium or high MS and LB medium or high -- by cultureby culture
(b)(b) Visible heavy plaque on teethVisible heavy plaque on teeth
(c)(c) Frequent (greater than 3 times) between meal snacks of Frequent (greater than 3 times) between meal snacks of sugars/cooked starchsugars/cooked starch
(d)(d) Deep pits and fissuresDeep pits and fissures
(e)(e) Recreational drug useRecreational drug use
(f)(f) Inadequate saliva flow (less than 0.5 ml/min) Inadequate saliva flow (less than 0.5 ml/min)
(g)(g) Saliva reducing factors: 1) medications, 2) radiation to the Saliva reducing factors: 1) medications, 2) radiation to the head and neck, 3) systemic reasons, e.g. Sjogren’s head and neck, 3) systemic reasons, e.g. Sjogren’s syndromesyndrome
(h)(h) Exposed tooth rootsExposed tooth roots
(i)(i) Orthodontic appliances present Orthodontic appliances present
Caries Risk assessment Caries Risk assessment (Age 6 years and older/adult) (Age 6 years and older/adult) -- 33
3. Protective Factors3. Protective Factors
(a)(a) Lives/works/school in community with fluoridated waterLives/works/school in community with fluoridated water
(b)(b) Uses fluoride toothpaste once dailyUses fluoride toothpaste once daily
(c)(c) Use fluoride toothpaste at least twice dailyUse fluoride toothpaste at least twice daily
(d)(d) Uses fluoride rinse/gel dailyUses fluoride rinse/gel daily
(e)(e) Uses 5000 ppm F toothpaste dailyUses 5000 ppm F toothpaste daily
(f)(f) Fluoride varnish in last 6 monthsFluoride varnish in last 6 months
(g)(g) Office F topical in last 6 monthsOffice F topical in last 6 months
(h)(h) Chlorhexidine rinse prescribed/used daily for 1 week every Chlorhexidine rinse prescribed/used daily for 1 week every month last 6 monthsmonth last 6 months
(i)(i) Xylitol gum/candies 4 times daily last 6 monthsXylitol gum/candies 4 times daily last 6 months
(j)(j) Calcium/phosphate paste last 6 monthsCalcium/phosphate paste last 6 months
(k)(k) Saliva flow visibly adequate or > 1 ml/min by testSaliva flow visibly adequate or > 1 ml/min by test
Caries Risk AssessmentCaries Risk Assessment (Age 6years (Age 6years -- adult)adult)--5 5
4. Bacterial test for high risk individual as a baseline measure
5. Count the yes’s. Assess caries risk and circle risk as extreme, high, moderate or low
6. Treatment Plan
Includes home care, office preventive treatments and restorative work
7. Home Care Recommendations
8. Recall and Re-assessment of Caries Risk

Extreme Caries Risk IndividualsExtreme Caries Risk Individuals�� High Risk plus severe hyposalivation. Measure High Risk plus severe hyposalivation. Measure
saliva flow rate (less than 0.5 ml/minute)saliva flow rate (less than 0.5 ml/minute)
�� Same as for high risk individuals PLUS:Same as for high risk individuals PLUS:
�� Baking soda rinse 4x daily (2 teaspoons in 8 ounces Baking soda rinse 4x daily (2 teaspoons in 8 ounces water)water)
�� Consider fluoride trays for home use (1.1% neutral Consider fluoride trays for home use (1.1% neutral sodium fluoride gel) dailysodium fluoride gel) daily
�� Consider calcium phosphate home use gelConsider calcium phosphate home use gel
�� Recall 3 months and repeat F varnish etc.Recall 3 months and repeat F varnish etc.
Caries Risk (Age 6 yearsCaries Risk (Age 6 years--Adult):Adult):--Patient RecommendationsPatient Recommendations
�� Daily oral hygiene. Daily oral hygiene. FluorideFluoride--containing toothpastecontaining toothpaste
�� DietDiet. Limit between meal snacks, limit sodas.. Limit between meal snacks, limit sodas.
�� FluorideFluoride. Increase stepwise depending on risk level. . Increase stepwise depending on risk level.
(1) Toothpaste 2x daily, (2) F rinse (0.05% sodium fluoride) daily, (1) Toothpaste 2x daily, (2) F rinse (0.05% sodium fluoride) daily, (3) 5,000 ppm F dentifrice/gel nightly. Consider fluoride (3) 5,000 ppm F dentifrice/gel nightly. Consider fluoride varnish.varnish.
�� Sugar free gum/candy.Sugar free gum/candy. Xylitol containing gum/candy, 4x daily.Xylitol containing gum/candy, 4x daily.
�� Antibacterial rinseAntibacterial rinse. Chlorhexidine gluconate (0.12%) once . Chlorhexidine gluconate (0.12%) once daily for one week every month for 6 months. daily for one week every month for 6 months.
�� For Dry Mouth (EXTREME RISK)For Dry Mouth (EXTREME RISK). Baking soda toothpaste with . Baking soda toothpaste with fluoride, xylitol gum, rinse frequently with baking soda fluoride, xylitol gum, rinse frequently with baking soda suspension in water (2 teaspoons/250 ml water).suspension in water (2 teaspoons/250 ml water).
Caries Risk assessment Caries Risk assessment (Age 6 years and older/adult)(Age 6 years and older/adult)--44
�� TestsTests
(a)(a) Stimulated Stimulated saliva flow ratesaliva flow rate is measured by chewing is measured by chewing and spitting for 3and spitting for 3--5 minutes (timed). Amount (in ml) 5 minutes (timed). Amount (in ml) divided by time = rate (ml/min). Less than 0.7 divided by time = rate (ml/min). Less than 0.7 ml/min is low and , less than 0.5 ml/min is dry.ml/min is low and , less than 0.5 ml/min is dry.
(b)(b) Bacteria testing by the CRT (Caries Risk Test, from Bacteria testing by the CRT (Caries Risk Test, from Vivadent, Amherst, NY) or Dentocult Vivadent, Amherst, NY) or Dentocult (www.edgedental.com). Use selective media sticks (www.edgedental.com). Use selective media sticks for mutans streptococci and lactobacilli. Incubate for mutans streptococci and lactobacilli. Incubate 72 hours and read as low medium or high.72 hours and read as low medium or high.
(c)(c) Follow up with repeat tests at 3Follow up with repeat tests at 3--6 months until 6 months until stablestable
Vivadent Test Strips. Used to measure mutans
streptococci and lactobacilli bacterial challenge level.
HighLow
Mutans
streptococci
Lactobacilli
What is the Caries Risk of What is the Caries Risk of this Individual?this Individual?
15 year old female15 year old female�� No new caries lesions in the last 5 yearsNo new caries lesions in the last 5 years
�� No symptoms of salivary dysfunction No symptoms of salivary dysfunction (dry mouth), no medications with (dry mouth), no medications with salivary side effects salivary side effects
�� Assume low cariogenic bacteria levelsAssume low cariogenic bacteria levels
�� Not a frequent snackerNot a frequent snacker

Low Risk PatientLow Risk Patient
Protective Factors• No new caries in 5 years
• Saliva normal
• Fluoride, calcium, phosphate
- remineralization:-
• 2 x daily F toothpaste
• Antibacterials:- No need
No CariesCaries
Pathological Factors
• Low Acid-producing bacteria
• Saliva normal
• Carbohydrates o.k.
X
Therapy for Low Caries Risk Therapy for Low Caries Risk IndividualIndividual
15 year old female15 year old female
�� Maintain 2 x daily fluoride toothpaste brushing Maintain 2 x daily fluoride toothpaste brushing
and other habits. and other habits.
�� Recall 12 months.Recall 12 months.
The Caries BalanceThe Caries BalanceProtective Factors
• Saliva flow and components
• Remineralization:
•Fluoride, calcium, phosphate
• Antibacterials:-
chlorhexidine, xylitol, new?
No CariesCaries
Pathological Factors
• Acid-producing bacteria
• Frequent eating/drinking of
fermentable carbohydrates
•Sub-normal saliva flow and
function
What is the Caries Risk of this What is the Caries Risk of this Individual?Individual?
19 year old female19 year old female�� Several radiographic lesions into dentinSeveral radiographic lesions into dentin
�� Symptoms of salivary dysfunction (dry Symptoms of salivary dysfunction (dry mouth), taking antimouth), taking anti--anxiety medication, and anxiety medication, and major analgesic daily for three years.major analgesic daily for three years.
�� Risk assessment signals to do a bacteria test Risk assessment signals to do a bacteria test --
medium LB and medium MSmedium LB and medium MS
�� Admits to being a frequent snacker Admits to being a frequent snacker
High/Extreme Risk High/Extreme Risk PatientPatient
Protective Factors•Fluoride - remineralization
F Toothpaste once daily only
Minimal calcium, phosphate
• Antibacterials:- none used
No Caries
Caries
X

High Risk PatientHigh Risk PatientProtective Factors
• Office applied Topical Fluoride
• Chlorhexidine 10 ml daily one
week a month for 6 months
• Brush with high 5000 ppm F
toothpaste daily - enhance
remineralization
• Xylitol gum daily
•Consider MI paste
• Recall 3 or 6 months
No New Caries
CariesOn Hold
Caries risk assessment procedures and treatments for
children aged 0-5 years, can be
accessed in the October 2007 CDA JournalRamos-Gomez et al.,
www.cdafoundation.org/journal
1.1. Modification of the oral flora Modification of the oral flora
2.2. Patient educationPatient education
3.3. Remineralization of nonRemineralization of non--cavitated lesions of enamel cavitated lesions of enamel
and dentin and dentin
4.4. Minimal operative intervention of cavitated lesions Minimal operative intervention of cavitated lesions
5.5. Repair of defective restorationsRepair of defective restorations
FDI statement 2002FDI statement 2002
Minimal Intervention in the Management of Minimal Intervention in the Management of Dental CariesDental Caries
Minimally Invasive DentistryMinimally Invasive Dentistry
� The basic principle is to preserve as much of the natural tooth structure as possible while at the same time encouraging remineralization of early lesions to inhibit further progression.
� Maintaining a balance between caries pathological and protective factors is the key to success and the oral health of the patient
Featherstone, April, 2004
Conservative Caries Conservative Caries Management by the Dental Management by the Dental
TeamTeam�� Detect caries lesions early enough to Detect caries lesions early enough to
reverse or prevent progressionreverse or prevent progression
�� Assess caries risk Assess caries risk
�� Use fluoride and/or antibacterial Use fluoride and/or antibacterial therapy based on observationstherapy based on observations
�� Use minimally invasive restorative Use minimally invasive restorative
procedures to conserve tooth procedures to conserve tooth structurestructure
It is an uphill struggle to get faculty, students and
practitioners to accept the practical application of the
“caries balance” and caries management by risk
assessment, BUT it works and patients are grateful








